Embed Size (px)
Citation preview

Roland 1
Diseases of the EACDiseases of the EACPETER ROLAND, MDPETER ROLAND, MD
BRANDON ISAACSON, MDBRANDON ISAACSON, MD
UT SOUTHWESTERNUT SOUTHWESTERNUT SOUTHWESTERNUT SOUTHWESTERN
DALLAS TXDALLAS TX
DisclosuresDisclosures
Consultant to Alcon LabsConsultant to Alcon Labs RolandRoland Consultant to Alcon Labs Consultant to Alcon Labs –– RolandRoland
Course Instructor Medtronic Midas Course Instructor Medtronic Midas Rex Institute Rex Institute -- IsaacsonIsaacson

Roland 2
Excess cerumenExcess cerumen
Adults 3Adults 3 10 %10 % 5 di N 50005 di N 5000 Adults 3Adults 3--10 % 10 % 5 studies N=50005 studies N=5000
Children 10% Children 10% 2 studies N=5732 studies N=573
Geriatric 34% Geriatric 34% 11 studies N=104studies N=104
Institutionalized 22Institutionalized 22-- 36% 36% 4 studies N=5754 studies N=575
Cerumen removalCerumen removal
CerumenolyticsCerumenolytics CerumenolyticsCerumenolytics Peroxide basedPeroxide based
Cerumenex®Cerumenex®
NaHCO3NaHCO3
OtherOther
MechanicalMechanical MechanicalMechanical
IrrigationIrrigation SyringeSyringe
Water picWater pic

Roland 3
Ear candlesEar candles
Ear candles -- Sealy 1996Ear candles -- Sealy 1996
No neg pressureNo neg pressure No neg pressureNo neg pressure
Burnt paraffinBurnt paraffin
Injuries Injuries (n=122)(n=122):: 13 burns13 burns
7 paraffin occlusions7 paraffin occlusions
2 TM f2 TM f 2 TM perfs2 TM perfs
3 otitis externa3 otitis externa
6 CHL6 CHL

Roland 4
Cerumen management clinical practice guidelineCerumen management clinical practice guideline Why?Why? Why?Why?
Strong recommendationsStrong recommendationsRx if 1) symptomatic 2) prevents a Rx if 1) symptomatic 2) prevents a
needed examneeded exam
RecommendationRecommendationAssess for modifying factorsAssess for modifying factors
Assess HA pts regularlyAssess HA pts regularly
Cerumen management clinical practice guidelineCerumen management clinical practice guideline OptionOption OptionOptionMay observe nonMay observe non--impacted cerumenimpacted cerumen
May use cerumenolytics, irrigation, or May use cerumenolytics, irrigation, or manual removalmanual removal
Carefully assess those who may not be Carefully assess those who may not be able to express symptomsable to express symptoms
Council pts on preventionCouncil pts on prevention

Roland 5
FurunculosisFurunculosis
Lateral 1/3Lateral 1/3 Lateral 1/3Lateral 1/3
Staph aureusStaph aureus
Systemic antibiotics with Systemic antibiotics with good gram + coveragegood gram + coverage Cephalosprin, clinda.,Cephalosprin, clinda.,
I&DI&D I&DI&D
External OtitisExternal Otitis
Inflammation of the EACInflammation of the EAC Inflammation of the EACInflammation of the EACAllergicAllergicIrritativeIrritativeBacterialBacterialFungalFungalViralViralViralViralPrimary DermatitisPrimary Dermatitis
Acute or ChronicAcute or Chronic

Roland 6
Fungal External OtitisFungal External Otitis
Uncommon as aUncommon as a Uncommon as a Uncommon as a primary disease. primary disease. Fungal organisms may Fungal organisms may grow on desquamated grow on desquamated epithelium or cerumen epithelium or cerumen as simple saprophytesas simple saprophytes
True fungal otitis isTrue fungal otitis isTrue fungal otitis is True fungal otitis is almost always either almost always either Aspergillus or Candida Aspergillus or Candida SpeciesSpecies
Treatment of Fungal OtitisTreatment of Fungal Otitis
Mechanical debridementMechanical debridement Mechanical debridementMechanical debridement
Usually responds to reUsually responds to re--acidification acidification &/or the use of topical anti&/or the use of topical anti--septics septics (Gentian violet, mercurochrome, )(Gentian violet, mercurochrome, )
Only rarely will antifungal antibiotics Only rarely will antifungal antibiotics y y gy y gbe requiredbe required
Lucente et al: The External Ear

Roland 7
Acute Bacterial Otitis ExternaAcute Bacterial Otitis Externa
AOE; PathognesisAOE; Pathognesis
Temp and humidityTemp and humidity Temp and humidityTemp and humidity
SeasonalSeasonal
pHpH
DermatitisDermatitis
TT TraumaTrauma
Fabricant et al. Arch Otorhinolaryngol: 201-9, 1949.

Roland 8
History1,2
• PAIN
Diagnosis of Bacterial Diagnosis of Bacterial Acute Otitis ExternaAcute Otitis Externa
PAIN• Itching• Hearing loss
Physical examination• Swollen external auditory canal1
• Erythema (variable)2
• Watery, scant exudate2
• Tenderness/PAIN2
1. Marple BF, et al. In: Roland PS, et al, eds. Hearing Loss. 1997:133-154.2. Roland PS. Curr Infect Dis Rep. 2000;2:160-167.
Photo courtesy of Michael Hawke, MD.
Organisms (%) Recovered During a Series of Clinical Trials
Microbiology of Acute Otitis Externa
Gram-positives
45.3%45.3% Gram-negatives
52.9%52.9%
Gram-positivesStaphylococcus sp 27.4%Coryneforms 12.1%
Streptococcus + Enterococcus 3.9%
Bacillus + P ib ill 1 5%
Gram-negativesPseudomonas
aeruginosa 37.7%Enterobacteriaceae +
Vibrionaceae 8.5%
Nonfermentative
1. Roland P, Stroman D. Laryngoscope. 2002;112:1166-1177.
52.9%52.9%
Fungi and Yeast1.7%
Paenibacillus 1.5%
Micrococcus 0.24%
Actinomycetes 0.14%
Gram-negatives 3.9%
Other Pseudomonads 2.3%
Other Gram-negatives 0.45%

Roland 9
AOE: TreatmentAOE: Treatment
Removal of debrisRemoval of debris Removal of debris Removal of debris
ReRe--acidification acidification
Assure delivery (remove debris or an Assure delivery (remove debris or an otowick)otowick)
AppropriateAppropriate topicaltopical antimicrobialantimicrobial Appropriate Appropriate topicaltopical antimicrobialantimicrobial
Appropriate pain managementAppropriate pain management
Systemic antibiotics are rarely requiredSystemic antibiotics are rarely required
AdvantagesAdvantages
DDelivery of high concentration (0 3%)elivery of high concentration (0 3%)DDelivery of high concentration (0.3%)elivery of high concentration (0.3%)33--5 GTTS dose is only 905 GTTS dose is only 90g g -- 150mcg 150mcg
but at a concentration of but at a concentration of 3000mcg/ml3000mcg/mlwhich exceeds the MIC of any known which exceeds the MIC of any known relevant pathogen.relevant pathogen.
MMinimal systemic effectinimal systemic effect
LLow costow cost
Alter local microAlter local micro--environmentenvironment

Roland 10
DisadvantagesDisadvantages
Local discomfortLocal discomfort Local discomfortLocal discomfort pHpH
alcoholalcohol
temperaturetemperature
Require direct contactRequire direct contact
Topical sensitizationTopical sensitizationTopical sensitizationTopical sensitization
Alter microAlter micro--environment environment
Minimal systemic effectMinimal systemic effect
Practical irrelevance of Practical irrelevance of ““MICMIC””MICMIC
therefore,
li i l i i i i i lli i l i i i i i lclinical sensitivities are meaninglessclinical sensitivities are meaningless&&
changing topical antibiotics is irrationalchanging topical antibiotics is irrational

Roland 11
HypersensitivityHypersensitivity
WARNING:WARNING: THETHE WARNING:WARNING: THE THE MANIFESTATION OF MANIFESTATION OF SENSITIZATION TO SENSITIZATION TO
NEOMYCIN IS NEOMYCIN IS USUALLY A USUALLY A LOW LOW
GRADEGRADE REDDENING REDDENING WITH SWELLING, DRY WITH SWELLING, DRY
SCALING AND SCALING AND ITCHING; ITCHING; IT MAY IT MAY
SIMPLY MANIFEST AS SIMPLY MANIFEST AS FAILURE TOFAILURE TO HEALHEAL
Rosenfeld et al OTO-HNS May 2006

Roland 12
Strong RecommendationStrong Recommendation
M t f AOE h ld i l dM t f AOE h ld i l dManagement of AOE should include Management of AOE should include assessment of pain and a assessment of pain and a
recommendation for analgesic recommendation for analgesic treatment based on the severity of treatment based on the severity of
painpain
RecommendationsRecommendations
1) Distinguish diffuse AOE from 1) Distinguish diffuse AOE from other causesother causes
2) Assess the patient for factors that 2) Assess the patient for factors that modify treatmentmodify treatment
Nonintact TM TT diabetesNonintact TM TT diabetesNonintact TM, TT, diabetes, Nonintact TM, TT, diabetes, immunocomprimised state, prior immunocomprimised state, prior
radiation therapyradiation therapy
3) Use topical therapy for initial 3) Use topical therapy for initial managementmanagement

Roland 13
RecommendationsRecommendations
4) The choice of topical agent should be 4) The choice of topical agent should be ) p g) p gbased on:based on:
EfficacyEfficacyLow incidents of adverse eventsLow incidents of adverse events
Likelihood of adherenceLikelihood of adherenceCostCost
5) Clinicians should inform pts how to5) Clinicians should inform pts how to5) Clinicians should inform pts how to 5) Clinicians should inform pts how to administer the dropsadminister the drops
RecommendationsRecommendations
6) When the TM is nonintact, a non6) When the TM is nonintact, a non--6) When the TM is nonintact, a non6) When the TM is nonintact, a nonototoxic topical preparation should be ototoxic topical preparation should be
prescribedprescribed
7) If the patient fails to respond within 7) If the patient fails to respond within 48 to 72hrs the clinician should reassess48 to 72hrs the clinician should reassess48 to 72hrs, the clinician should reassess 48 to 72hrs, the clinician should reassess
the ptthe pt..

Roland 14
Pay for performancePay for performance
Assess for pain at every visitAssess for pain at every visit Assess for pain at every visitAssess for pain at every visit
Prescribe a topicalPrescribe a topical
Do Do notnot prescribe a systemicprescribe a systemic
Canal CholesteatomaCanal Cholesteatoma
UnilateralUnilateral Multiple etiologiesMultiple etiologies UnilateralUnilateral
Not associated with Not associated with systemic diseasesystemic disease
OlderOlder
Rx: medical or Rx: medical or i li l
Multiple etiologiesMultiple etiologies congenitalcongenital
Post traumaticPost traumatic
Post obstructivePost obstructive
Post inflammatoryPost inflammatory
SpontaneousSpontaneoussurgicalsurgical SpontaneousSpontaneous
IatrogenicIatrogenic

Roland 15
Keratosis ObturansKeratosis Obturans BilateralBilateral SymptomsSymptoms
Associated w Associated w sinusitis & sinusitis & bronchiectasisbronchiectasis
Rx: regular office Rx: regular office debridementdebridement
CHLCHL
Otorrhea rareOtorrhea rare
Pain Pain
1st and 2nd decades1st and 2nd decades
Keratosis CholesteatomaKeratosis Cholesteatoma

Roland 16
Keratosis CholesteatomaKeratosis Cholesteatoma
Keratosis CholesteatomaKeratosis Cholesteatoma

Roland 17
ExostosisExostosis Suture linesSuture lines
17.5 C canal 17.5 C canal erythemaerythema
73% surfers73% surfers
Lateral to isthmusLateral to isthmus
OsteomaOsteoma
True neoplasmTrue neoplasm True neoplasmTrue neoplasm
SingleSingle
UnilateralUnilateral

Roland 18
Exostosis OsteomaExostosis Osteoma ReactiveReactive NeoplasticNeoplastic ReactiveReactive
Non occlusiveNon occlusive
BilateralBilateral
MultipleMultiple
Sessile Sessile
NeoplasticNeoplastic
OcclusiveOcclusive
UnilateralUnilateral
SingleSingle
PeduculatedPeduculated
Lamellar boneLamellar bone Trabecular boneTrabecular bone
Exostosis OsteomaExostosis Osteoma

Roland 19
Surgical TechniqueSurgical Technique
Skin flapsSkin flaps Skin flapsSkin flaps
ChiselChisel
DrillDrill
Facial Nerve!Facial Nerve! 14% Of FN 14% Of FN
l il iparalysis paralysis (Green)(Green)
Monitor?Monitor?
Granular MyringitisGranular Myringitis
DefinitionDefinitionDeDe –– epithelializationepithelializationDe De epithelialization epithelialization
of the tympanic of the tympanic membranemembrane
Granulation tissueGranulation tissueNormal middle earNormal middle ear
EtiologyEtiology Trauma, InfectionTrauma, Infection au a, ect oau a, ect o Impaired migration Impaired migration
provokes infection and provokes infection and induces trauma in the induces trauma in the lamina proprialamina propria

Roland 20
Granular myringitisGranular myringitis
SymptomsSymptomsy py p Otorrhea (most common), aural fullness, subjective Otorrhea (most common), aural fullness, subjective
hearing loss, otalgia, tinnitus, aural pruritus.hearing loss, otalgia, tinnitus, aural pruritus. Physical examPhysical exam
Focal versus diffuseFocal versus diffuse Ulceration versus polypoid massUlceration versus polypoid mass Purulent discharge versus crustingPurulent discharge versus crusting
PerforationPerforation PerforationPerforation May occur as a result of diseaseMay occur as a result of disease Disease may occur in the setting of a prior Disease may occur in the setting of a prior
perforationperforation
Granular myringitisGranular myringitis Grade IGrade I
Focal disease of tympanic Focal disease of tympanic membrane +/membrane +/ ear canal skinear canal skinmembrane +/membrane +/-- ear canal skinear canal skin
Shallow ulceration +/Shallow ulceration +/--crustingcrusting
Grade IIGrade II Focal polypoid granulationFocal polypoid granulation Purulent possible foul Purulent possible foul
smelling otorrheasmelling otorrhea Grade IIIGrade III
Diffuse tympanic membraneDiffuse tympanic membrane Diffuse tympanic membrane Diffuse tympanic membrane involvementinvolvement
Grade IVGrade IV Diffuse involvement with Diffuse involvement with
granulation tissue including granulation tissue including canalcanal
Wolf M, Primov-Fever A, Barshack I, Polack-Charcon S, Kronenberg J. Granular Myringitis: Incidence and Clinical Characteristics. Otology & Neurotology 2006;27:1094-7. Blevins: Otol & Neurotol 2001 El-Seifi: AJO 2000
Roland 21
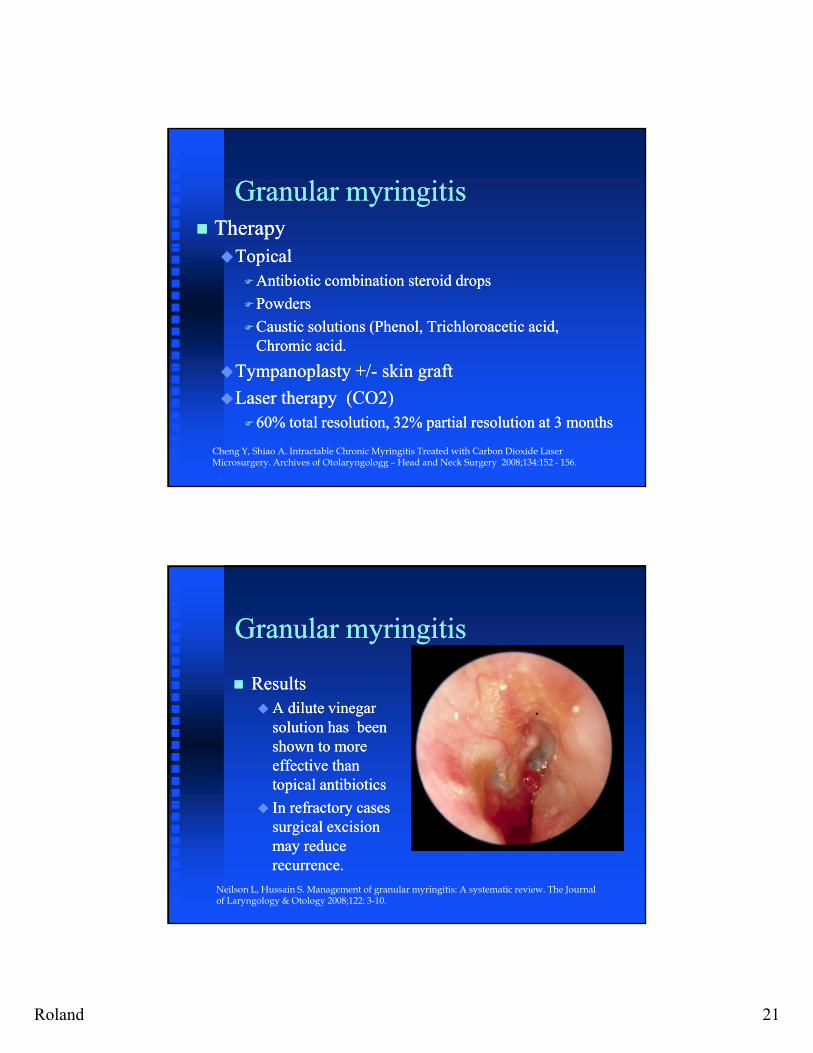
Granular myringitisGranular myringitis TherapyTherapyTopicalTopical
Antibiotic combination steroid dropsAntibiotic combination steroid drops
PowdersPowders
Caustic solutions (Phenol, Trichloroacetic acid, Caustic solutions (Phenol, Trichloroacetic acid, Chromic acid.Chromic acid.
T l t +/T l t +/ ki ftki ftTympanoplasty +/Tympanoplasty +/-- skin graftskin graft
Laser therapy (CO2)Laser therapy (CO2)60% total resolution, 32% partial resolution at 3 months60% total resolution, 32% partial resolution at 3 months
Cheng Y, Shiao A. Intractable Chronic Myringitis Treated with Carbon Dioxide Laser Microsurgery. Archives of Otolaryngologg – Head and Neck Surgery 2008;134:152 - 156.
Granular myringitisGranular myringitis
ResultsResults ResultsResultsA dilute vinegar A dilute vinegar
solution has been solution has been shown to more shown to more effective than effective than topical antibioticstopical antibiotics
I f tI f t In refractory cases In refractory cases surgical excision surgical excision may reduce may reduce recurrence.recurrence.
Neilson L, Hussain S. Management of granular myringitis: A systematic review. The Journal of Laryngology & Otology 2008;122: 3-10.

Roland 22
Malignant otitis externaMalignant otitis externa
PresentationPresentationi ii i Severe, unremitting Severe, unremitting
otalgia (worse at night), otalgia (worse at night), fullness, otorrhea, fullness, otorrhea, hearing loss, headache, hearing loss, headache, trismus, TMJ paintrismus, TMJ pain
ExamExam Granulation and Granulation and
exposed bone at BC exposed bone at BC junctionjunction
Facial nerve (25%) Facial nerve (25%) ( )( )most commonly most commonly affected cranial nerve, affected cranial nerve, followed by jugular followed by jugular foramen.foramen.
43% will present with 43% will present with cranial nerve cranial nerve involvementinvolvement
Moffat Axon Laryngoscope 2007
Malignant otitis externaMalignant otitis externa
Risk factorsRisk factors Risk factorsRisk factorsDiabetes mellitus 65% or as high as 90 to Diabetes mellitus 65% or as high as 90 to
100% of patients (Franco100% of patients (Franco--vidal O&N vidal O&N 2007)2007)
HIV/AIDSHIV/AIDS
ChemotherapyChemotherapy
Leukemia/lymphomaLeukemia/lymphoma
SplenectomySplenectomy
TransplantTransplant

Roland 23
Malignant Otitis externaMalignant Otitis externa
HIVHIV HIVHIVPatients are youngerPatients are younger
Suspect in patients with otitis externa Suspect in patients with otitis externa which does not improvewhich does not improve
May not to have granulation tissue in May not to have granulation tissue in EACEAC
Fungal infections more commonFungal infections more common
Pseudomonas when CD4 is less than 100 Pseudomonas when CD4 is less than 100
Aspergillus when CD4 less than 50 Aspergillus when CD4 less than 50
Malignant otitis externaMalignant otitis externa
Differential diagnosisDifferential diagnosis Differential diagnosisDifferential diagnosisCarcinoma of EACCarcinoma of EAC
Biopsy granulation if persistentBiopsy granulation if persistent
Granulomatous diseasesGranulomatous diseases
PagetPaget’’s diseases disease
Nasopharynx malignanciesNasopharynx malignancies
Clival lesionsClival lesions
Fibrous dysplasiaFibrous dysplasia

Roland 24
Malignant otitis externaMalignant otitis externa
PathophysiologyPathophysiology elderly moreelderly more Pathophysiology Pathophysiology –– elderly more elderly more susceptiblesusceptibleEndarteritis, microangiopathy, small Endarteritis, microangiopathy, small
vessel obliterationvessel obliteration
Pseudomonas can invade vessel wall Pseudomonas can invade vessel wall li i d h b ili i d h b icause vasculitis and thrombosiscause vasculitis and thrombosis
Poor chemotaxis and phagocytosisPoor chemotaxis and phagocytosis
Higher cerumen pH in diabetes and malesHigher cerumen pH in diabetes and males
Infection spreads through Haversion Infection spreads through Haversion system not air cells.system not air cells.
MOE stagingMOE staging
STAGE ISTAGE I: infection of canal and: infection of canal and STAGE ISTAGE I: infection of canal and : infection of canal and contiguous soft tissue w/wo CN VII contiguous soft tissue w/wo CN VII involvementinvolvement
STAGE IISTAGE II: Extension to include : Extension to include osteitis of skull base and multiple osteitis of skull base and multiple
Roland 48
cranial nervescranial nerves
STAGE IIISTAGE III: Intracranial : Intracranial complicationscomplications

Roland 25
Malignant otitis externaMalignant otitis externa
DiagnosisDiagnosisCTCTCT CT
Sensitive for bone erosion Sensitive for bone erosion
Permanent.Permanent.
No ideal for f/u No ideal for f/u
MRI MRI Sh d d i lSh d d i lShows marrow and dura involvementShows marrow and dura involvement
Enhancement may be prolonged Enhancement may be prolonged –– not ideal not ideal for f/ufor f/u
Poor at showing bone erosion Poor at showing bone erosion
Not an ideal initial study.Not an ideal initial study.
Malignant Otitis externaMalignant Otitis externa
DiagnosisDiagnosis Technetium Tc 99m Technetium Tc 99m
methylene diphosphonate methylene diphosphonate (MDP) (MDP) Positive in nearly Positive in nearly
100% of MOE100% of MOE Concentrates in areas Concentrates in areas
of osteoblastic activityof osteoblastic activity Better for initial Better for initial
diagnosisdiagnosis Increase sensitivity by Increase sensitivity by y yy y
identifying increase identifying increase uptake 4 to 24 hours uptake 4 to 24 hours after injection. after injection.
Positive in cancersPositive in cancers Remains positiveRemains positive

Roland 26
Malignant Otitis externaMalignant Otitis externa
DiagnosisDiagnosis DiagnosisDiagnosisGallium Ga 67Gallium Ga 67
Concentrates in areas with active inflammationConcentrates in areas with active inflammation
Attaches to lactoferrin (large quantities in leukocytes)Attaches to lactoferrin (large quantities in leukocytes)
Binds directly to bacteria and transferrinBinds directly to bacteria and transferrin
Resolves with resolution of infectionResolves with resolution of infection
Can repeat every 4 weeksCan repeat every 4 weeks
Follow with Gallium 67 and ESRFollow with Gallium 67 and ESR Stop therapy when these both normalizeStop therapy when these both normalize
Can recur up to year laterCan recur up to year later
Malignant Otitis ExternaMalignant Otitis Externa
Diagnostic work upDiagnostic work up Diagnostic work upDiagnostic work upBiopsy granulation tissueBiopsy granulation tissue
Culture (aerobe, anaerobe, fungal and Culture (aerobe, anaerobe, fungal and sensitivities)sensitivities) Initiate empiric therapy while awaiting Initiate empiric therapy while awaiting
culturesculturesculturescultures
Silver stain to ID fungal elementsSilver stain to ID fungal elements

Roland 27
Malignant Otitis externaMalignant Otitis externa
Bacterial pathogensBacterial pathogens Bacterial pathogensBacterial pathogensPseudomonas aeruginosaPseudomonas aeruginosa most commonmost common
33% resistance to Cipro in one series (Bernholz & 33% resistance to Cipro in one series (Bernholz & Harell Lscope 2002Harell Lscope 2002
Other organisms: Other organisms: Staphylococcus aureus, Staphylococcus aureus, S epidermidis, Proteus mirabilis, S epidermidis, Proteus mirabilis, p , ,p , ,Klebsiella oxytoca, P cepaciaKlebsiella oxytoca, P cepacia
Aspergillus fumigatusAspergillus fumigatus is the most is the most common fungal agentcommon fungal agent Unresponsive to antibioticsUnresponsive to antibiotics
Negative culturesNegative cultures
Malignant Otitis externaMalignant Otitis externa
Oral versus intravenous antibioticsOral versus intravenous antibioticsO ve sus ve ous b o csO ve sus ve ous b o cs Single versus double coverageSingle versus double coverage Duration of treatment 6 to 8 weeksDuration of treatment 6 to 8 weeks Oral Cipro 750 mg BID is acceptableOral Cipro 750 mg BID is acceptable May add RifampinMay add Rifampin Can use antipseudomonal PCN with concurrent Can use antipseudomonal PCN with concurrent
aminoglycoside in resistant and complicated casesaminoglycoside in resistant and complicated casesaminoglycoside in resistant and complicated casesaminoglycoside in resistant and complicated cases Culture negative (Djalilian HR O&N 2006)Culture negative (Djalilian HR O&N 2006)
Ceftazidime IV + Oral Cipro 750mg BID, topical Ceftazidime IV + Oral Cipro 750mg BID, topical aminoglycoside steroid dropsaminoglycoside steroid drops
Use aztreonam for PCN allergic patientsUse aztreonam for PCN allergic patients

Roland 28
Malignant Otitis externaMalignant Otitis externa
Amphotericin B for fungal MOEAmphotericin B for fungal MOE Amphotericin B for fungal MOEAmphotericin B for fungal MOELiposomal Amphotericin B is less toxic Liposomal Amphotericin B is less toxic
with equal efficacy. with equal efficacy.
Oral itraconazole after amphotericin Oral itraconazole after amphotericin has also been used successfully.has also been used successfully.
Malignant Otitis externaMalignant Otitis externa
Is there a role for hyperbaric oxygen?Is there a role for hyperbaric oxygen?
Increases the partial pressure of oxygen Increases the partial pressure of oxygen improving hypoxia and allowing greater improving hypoxia and allowing greater oxidative killing of bacteriaoxidative killing of bacteria
One series 7 of 8 patients recoveredOne series 7 of 8 patients recovered
No evidence to support its use by Cochrane No evidence to support its use by Cochrane reviewreview
Limited role for surgeryLimited role for surgeryg yg y
Debridement of bone sequestrum and Debridement of bone sequestrum and granulation granulation
Biopsy Biopsy
Duration of treatment is typically 6 weekDuration of treatment is typically 6 weekss

Roland 29
Malignant Otitis externaMalignant Otitis externa PrognosisPrognosis
li d dli d dMortality decreased 50% to 0 to 15%.Mortality decreased 50% to 0 to 15%.
Aspergillus, dural involvement are poor prognostic Aspergillus, dural involvement are poor prognostic factorsfactors
Facial nerve palsy can recover but incompleteFacial nerve palsy can recover but incomplete
Lower cranial nerve palsies can completely Lower cranial nerve palsies can completely recover.recover.
MOE oral quinolonesMOE oral quinolones
GiamarellouGiamarellou GiamarellouGiamarellou159 patients159 patients
Ciprofloxacin 88/101Ciprofloxacin 88/101
Ofloxacin 38/46 (5 resistant)Ofloxacin 38/46 (5 resistant)
58

Roland 30
Chronic External OtitisChronic External OtitisChronic External OtitisChronic External Otitis
A low grade diffuse infection of theA low grade diffuse infection of the A low grade, diffuse infection of the A low grade, diffuse infection of the external canal that persist for months external canal that persist for months or yearsor years
It is characterized clinically by It is characterized clinically by pruritits, scanty otorrhea and pruritits, scanty otorrhea and
59
progressive narrowing of the lumen of progressive narrowing of the lumen of the EAC. the EAC.
Duration exceeds 4 weeks or more Duration exceeds 4 weeks or more than 4 infections in one year.than 4 infections in one year.
PathologyPathologyPathologyPathology Mild to moderate Mild to moderate
ddedemaedema
Chronic Chronic inflammatory cell inflammatory cell infiltrateinfiltrateOften focalOften focal
60
Often focalOften focal
Microabscess Microabscess formationformation
Areas of calcificationAreas of calcification

Roland 31
PathologyPathologyPathologyPathology Progressive Progressive
b ith li l fib ib ith li l fib isubepithelial fibrosis subepithelial fibrosis leading to stenosisleading to stenosisPost inflammatory Post inflammatory
medial canal fibrosismedial canal fibrosis
61
PathologyPathologyPathologyPathology
62

Roland 32
Clinical PresentationClinical PresentationClinical PresentationClinical Presentation Hearing loss is a Hearing loss is a
more commonmore commonmore common more common presenting presenting symptom than symptom than otorrheaotorrhea
Females 2:1Females 2:1 Exacerbated by Exacerbated by
hearing aidshearing aids
63
Often starts in Often starts in anterior sulcus anterior sulcus
Bilateral in 50%Bilateral in 50%
Physical examinationPhysical examination
Absent cerumenAbsent cerumen Absent cerumenAbsent cerumen Raw epithelial Raw epithelial
surfacesurface——erythemaerythema ElephantiasisElephantiasis Scant, milky Scant, milky
otorrheaotorrhea
64
ShinnyShinny Narrowing of the Narrowing of the
lumenlumen

Roland 33
InfectiousInfectious
BacterialBacterial BacterialBacterialGram negative, especially Pseudomonas Gram negative, especially Pseudomonas StaphyloccusStaphyloccus
MycoticMycoticNot common pathogens in AOE but role Not common pathogens in AOE but role
in COE unclearin COE unclear probably greaterprobably greater
65
in COE unclearin COE unclear------probably greaterprobably greaterAspergillus & CandidaAspergillus & CandidaSlow growing fungi may be missedSlow growing fungi may be missed““IdId”” reactionsreactions
DermatologicalDermatological
Seborrheic dermatitisSeborrheic dermatitis Seborrheic dermatitisSeborrheic dermatitis fam history, scalp (fam history, scalp (““dandruffdandruff””), ),
flexures (retroflexures (retro--auricular) auricular)
PsoriasisPsoriasisOccasionally is isolated to earsOccasionally is isolated to ears
66
May develop from seborrheaMay develop from seborrhea
NeurodermatitisNeurodermatitis

Roland 34
SensitizationSensitization
1st case1st case of contact allergy of contact allergy to Neomycin was reportedto Neomycin was reportedto Neomycin was reported to Neomycin was reported in l952 by Baer and in l952 by Baer and Ludwig in a pt with Ludwig in a pt with chronic OE!chronic OE!
Cross reactivityCross reactivitybetween Neomycin and between Neomycin and other Aminoglycosides is other Aminoglycosides is common. Cf tobra in the common. Cf tobra in the NetherlandsNetherlands
The reaction time of the The reaction time of the aminoglycosides in patch aminoglycosides in patch testing almost always testing almost always exceeds 3 days andexceeds 3 days and
67
exceeds 3 days and exceeds 3 days and often takes 7 daysoften takes 7 days
The routine use of The routine use of Neomycin is not Neomycin is not recommended because of recommended because of the high risk of the high risk of sensitizationsensitization
HypersensitivityHypersensitivity
WARNING:WARNING: THETHE WARNING:WARNING: THE THE MANIFESTATION OF MANIFESTATION OF SENSITIZATION TO SENSITIZATION TO
NEOMYCIN IS NEOMYCIN IS USUALLY A USUALLY A LOW LOW
GRADEGRADE REDDENING REDDENING WITH SWELLING, DRY WITH SWELLING, DRY
SCALING ANDSCALING AND
68
SCALING AND SCALING AND ITCHING; ITCHING; IT MAY IT MAY
SIMPLY MANIFEST AS SIMPLY MANIFEST AS FAILURE TOFAILURE TO HEALHEAL
Roland 35
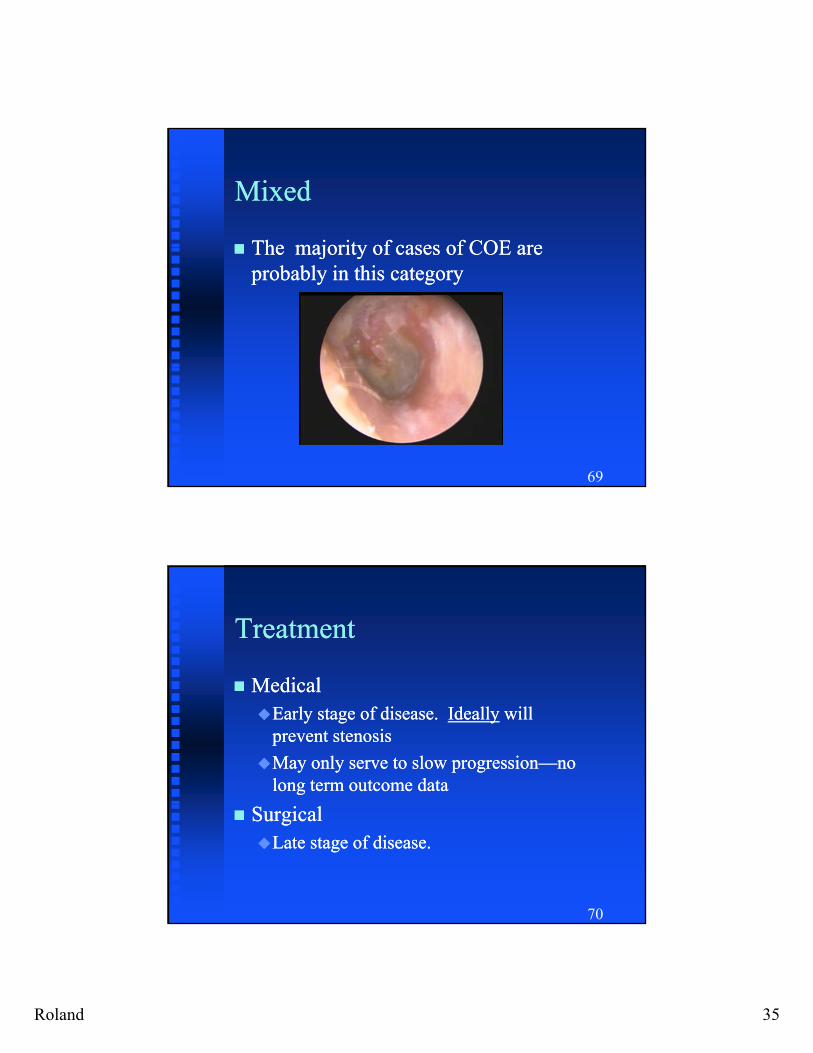
MixedMixed
The majority of cases of COE areThe majority of cases of COE are The majority of cases of COE are The majority of cases of COE are probably in this categoryprobably in this category
69
TreatmentTreatment
MedicalMedical MedicalMedicalEarly stage of disease. Early stage of disease. IdeallyIdeally will will
prevent stenosisprevent stenosis
May only serve to slow progressionMay only serve to slow progression——no no long term outcome datalong term outcome data
70
SurgicalSurgicalLate stage of disease. Late stage of disease.

Roland 36
Medical TherapyMedical Therapy SteroidsSteroids: drops, creams, : drops, creams,
injections?injections?injections?injections?
Single agents. Single agents. ophthalmic drops or ophthalmic drops or dermatologic creamsdermatologic creams
Combination agentsCombination agents
Topical TacrolimusTopical Tacrolimus
Caffer P, et al. Tacrolimus: A New Option in Therapy-Resistant Chronic Otitis Externa. Laryngoscope 2007;117:1046 – 52. 71
More effective in dry More effective in dry rather than wet casesrather than wet cases
Complete resolution in Complete resolution in 46% patients.46% patients.
Medical TherapyMedical Therapy
AntibioticsAntibiotics AntibioticsAntibioticsUse sparinglyUse sparinglyQuinolone drops Quinolone drops PowdersPowders----last last
longer & can longer & can include multiple include multiple
72
ppagentsagents
CultureCulture
““No TouchNo Touch”” aural aural toilettoilet

Roland 37
Surgical TherapySurgical Therapy
73
Local flapsLocal flaps
PrePre conchal post auricularconchal post auricular PrePre--conchal, post auricular conchal, post auricular Tendency to contract may help pull canal Tendency to contract may help pull canal
openopen
Decreased scarring because Decreased scarring because vascularityvascularity
Hard to get enough length Hard to get enough length
74
BulkyBulky

Roland 38
FTSG vs. STSGFTSG vs. STSG Greater resistance Greater resistance
to traumato trauma Most commonly Most commonly ddto traumato trauma
Glandular elements Glandular elements provide lubricationprovide lubrication
Less likely to Less likely to contractcontract
usedused
Easiest to obtainEasiest to obtain
Less reLess re--stenosis?stenosis?
75
contractcontract
Successful operationsSuccessful operations
Completely remove cicatrixCompletely remove cicatrix Completely remove cicatrixCompletely remove cicatrix
Include a canalplastyInclude a canalplasty
Resurface the bony canal with skin Resurface the bony canal with skin
76

Roland 39
Surgical resultsSurgical results ≈ 80% patent canal but ≈ 80% patent canal but
l tl trecurrences occur late recurrences occur late earliest @ 3yrs in earliest @ 3yrs in
SlatterySlattery’’s seriess series
Hearing improvements Hearing improvements range from 10dB to range from 10dB to
77
gg50dB 50dB 61% with closure of the 61% with closure of the
airair--bone ABG to 20 dB bone ABG to 20 dB (Beckers (Beckers ---- 53 pts)53 pts)





























