Embed Size (px)
Citation preview

MOKHTAR BASSIOUNI, M. D.MOKHTAR BASSIOUNI, M. D.
PROFESSOR OF OTOLARYNGOLOGYPROFESSOR OF OTOLARYNGOLOGYPROFESSOR OF OTOLARYNGOLOGYPROFESSOR OF OTOLARYNGOLOGY
UNIVERSITY OF ALEXANDRIAUNIVERSITY OF ALEXANDRIA
www.alexear.com

Tonsillo-pharyngitisTonsillo-pharyngitis
Clinical Aspects & ControversiesClinical Aspects & ControversiesClinical Aspects & ControversiesClinical Aspects & Controversies
E id i lE id i lEpidemiologyEpidemiology
Prevalence:N l ll hild i t l t 1
Prevalence:N l ll hild i t l t 1• Nearly all children experience at least 1episode of tonsillitis.
• Nearly all children experience at least 1episode of tonsillitis.
• Adeno-tonsillectomy is one of the most common surgical procedures performed in
• Adeno-tonsillectomy is one of the most common surgical procedures performed incommon surgical procedures performed in children in the US today with an annual
dit f $500 illi
common surgical procedures performed in children in the US today with an annual
dit f $500 illiexpenditure of $500 million. expenditure of $500 million.

DemographicsDemographics
Age Occurrence: Age Occurrence: • Tonsillitis is infrequent in the first 2
years of life, and most common in• Tonsillitis is infrequent in the first 2
years of life, and most common inyears of life, and most common in school-age children. years of life, and most common in school-age children.
MicrobiologyMicrobiology
• Most cases of pharyngitis and tonsillitis i l 90% f h i i i d l
• Most cases of pharyngitis and tonsillitis i l 90% f h i i i d lare viral: 90% of pharyngitis in adults
and 60% to 75% in children are caused are viral: 90% of pharyngitis in adults and 60% to 75% in children are caused by viruses.by viruses.

MicrobiologyMicrobiology
Viral Causes of Tonsillo-pharyngitis in Children• Common:Viral Causes of Tonsillo-pharyngitis in Children
• Common:• Common:• Adenoviruses, types 1, 2, 3, and 5.
L C
• Common:• Adenoviruses, types 1, 2, 3, and 5.
L C• Less Common:• Enteroviruses, Epstein-Barr virus, Herpes
i l i I fl i P i fl
• Less Common:• Enteroviruses, Epstein-Barr virus, Herpes
i l i I fl i P i flsimplex virus, Influenza viruses, Parainfluenza viruses Respiratory syncytial virus. I f
simplex virus, Influenza viruses, Parainfluenza viruses Respiratory syncytial virus. I f• Infrequent:
• Coronaviruses, Rhinoviruses.• Infrequent: • Coronaviruses, Rhinoviruses.
MicrobiologyMicrobiologyMicrobiologyMicrobiologyBacterial Pathogens in Tonsillo-pharyngitisBacterial Pathogens in Tonsillo-pharyngitisBacterial Pathogens in Tonsillo pharyngitis
Acute tonsillitis: the commonest is group A b-hemolytic i (GABHS ) i l d i 30 36 8% f hild
Bacterial Pathogens in Tonsillo pharyngitis
Acute tonsillitis: the commonest is group A b-hemolytic i (GABHS ) i l d i 30 36 8% f hildstreptococci (GABHS ); isolated in 30-36.8% of children.
Recurrent tonsillitis:
streptococci (GABHS ); isolated in 30-36.8% of children.
Recurrent tonsillitis:Recurrent tonsillitis: Aerobic: Streptococcus pneumoniae, Staphylococcus aureus, and Haemophilus influenzae.Anaerobic : Bacteroides fragilis
Recurrent tonsillitis: Aerobic: Streptococcus pneumoniae, Staphylococcus aureus, and Haemophilus influenzae.Anaerobic : Bacteroides fragilisAnaerobic : Bacteroides fragilis.
Hypertrophic tonsils: H influenzae.
Anaerobic : Bacteroides fragilis.
Hypertrophic tonsils: H influenzae.
Chronic tonsillitis: A polymicrobial bacterial population including: Staphylococcus aureus Moraxella catarrhalis andChronic tonsillitis: A polymicrobial bacterial population including: Staphylococcus aureus Moraxella catarrhalis andincluding: Staphylococcus aureus, Moraxella catarrhalis, and Hemophilus influenzae.including: Staphylococcus aureus, Moraxella catarrhalis, and Hemophilus influenzae.

• In polymicrobial infections beta-lactamase d i i G A
• In polymicrobial infections beta-lactamase d i i G Aproducing organisms can protect Group A
strep from eradication with penicillins.producing organisms can protect Group A strep from eradication with penicillins.
Some ClinicalSome ClinicalSome Clinical PresentationsSome Clinical Presentations
• Acute Follicular Tonsillitis.• Acute Follicular Tonsillitis.
• Chronic Tonsillitis.
• Obstructive Tonsillar Hyperplasia
• Chronic Tonsillitis.
• Obstructive Tonsillar Hyperplasia• Obstructive Tonsillar Hyperplasia.
• Unilateral Tonsillar Enlargement.
• Obstructive Tonsillar Hyperplasia.
• Unilateral Tonsillar Enlargement.
• Infectious Mononucleosis.
P it ill Ab
• Infectious Mononucleosis.
P it ill Ab• Peritonsillar Abscess.
• Thrush Tonsillitis.
• Peritonsillar Abscess.
• Thrush Tonsillitis.

Acute Follicular TonsillitisAcute Follicular Tonsillitis
• Signs and symptoms:• Signs and symptoms:
– Fever.
Sore throat
– Fever.
Sore throat– Sore throat.
– Dysphagia.
– Sore throat.
– Dysphagia.
– Enlarged tender cervical lymphadenopathy.
– Erythematous tonsils with exudates.
– Enlarged tender cervical lymphadenopathy.
– Erythematous tonsils with exudates.yy
Chronic TonsillitisChronic Tonsillitis
• Tonsils are unequal• Tonsils are unequal
in size.
• Irregular cryptal pattern
in size.
• Irregular cryptal pattern• Irregular cryptal pattern
• Malodorous breath.
• Irregular cryptal pattern
• Malodorous breath.
• Peritonsillar erythema.
• Persistent enlarged firm cervical (JD)
• Peritonsillar erythema.
• Persistent enlarged firm cervical (JD)• Persistent enlarged firm cervical (JD) lymphadenopathy.
• Persistent enlarged firm cervical (JD) lymphadenopathy.

Unilateral TonsillarUnilateral TonsillarUnilateral TonsillarUnilateral TonsillarUnilateral Tonsillar Unilateral Tonsillar EnlargementEnlargement
Unilateral Tonsillar Unilateral Tonsillar EnlargementEnlargementEnlargementEnlargementEnlargementEnlargement
Non-neoplastic Non-neoplastic
NeoplasticNeoplastic
Peritonsillar Abscess

InfectiousInfectiousInfectiousmononucleosis
Infectiousmononucleosis
White membrane covering b h ilone or both tonsils
Positive Paul-Bunnell bloodPositive Paul-Bunnell blood test
Atypical mononuclear whitecells are increased on the bl d filblood film.
Huge CLNsHuge CLNs

Obstructive TonsillarObstructive TonsillarObstructive Tonsillar Hyperplasia
Obstructive Tonsillar HyperplasiaHyperplasiaHyperplasia
• Snoring and Sleep • Snoring and Sleep g pApnoea (OSA).
• Muffled voice.
g pApnoea (OSA).
• Muffled voice.• Dysphagia.• Kissing tonsils.• Dysphagia.• Kissing tonsils.Kissing tonsils.Kissing tonsils.
Beware of the gag reflexg g

CandidiasisCandidiasis

Management ofManagement ofManagement of Pharyngo-tonsillitis
Management of Pharyngo-tonsillitisy gy g
• Investigations• Investigations
• Treatment of Acute attacks• Treatment of Acute attacks
• Treatment of recurrent attacks• Treatment of recurrent attacks
• Prophylactic treatment
• Surgery
• Prophylactic treatment
• Surgery• Surgery• Surgery
InvestigationsInvestigations
• ESR • ESR
• ASOT
• CRP
• ASOT
• CRP• CRP
• Throat swab / C&S.
• CRP
• Throat swab / C&S.

Treatment of Acute attacksTreatment of Acute attacksTreatment of Acute attacksTreatment of Acute attacks
• Penicillin• Penicillin
• Amoxycillin• Amoxycillin
• Usually the causative organism is non- B • Usually the causative organism is non- B lactamase-producing Streptococcus and will respond well to penicillins.lactamase-producing Streptococcus and will respond well to penicillins.p pp p
Treatment of Recurrent attacksTreatment of Recurrent attacksTreatment of Recurrent attacksTreatment of Recurrent attacks
•Usually, Recurrent tonsillitis is a polymicrobial infection in which beta-lactamase producinginfection, in which beta-lactamase producing organisms coexist and can protect Group A streptococci from eradication with penicillinsstreptococci from eradication with penicillins.
•Streptococcus pneumoniae Staphylococcus aureusStreptococcus pneumoniae, Staphylococcus aureus, and Haemophilus influenzae are the most common bacteria isolated in recurrent tonsillitis. These are
ll i h d bgenerally more resistant pathogens and are better faced with Beta-Lactamase stable antibiotics .

Treatment of Recurrent attacksTreatment of Recurrent attacksTreatment of Recurrent attacksTreatment of Recurrent attacks
•CombinationsAmpicillin-sulbactam A i illi l l tAmoxicillin-clavulanate •Second-generation cephalosporinsCefdinir (Cefdin)Cefdinir (Cefdin)Cefprozil •Third-generation cephalosporinsThird generation cephalosporinsCefixime Ceftriaxone •Macrolide/azalideAzithromycin Clarithromycin
VaccinationVaccination
• Pneumococcal conjugate vaccine• Pneumococcal conjugate vaccine
• H influenzae vaccine
• Flu vaccine
• H influenzae vaccine
• Flu vaccine
• Oral bacterial vaccine (Buccaline, bronchovaxom)
(
• Oral bacterial vaccine (Buccaline, bronchovaxom)
(• Immune-stimulant: (Echinacea)• Immune-stimulant: (Echinacea)

Indications for Indications for Indications for Indications for TonsillectomyTonsillectomyTonsillectomyTonsillectomy
AAO-HNS / Guidelines for Tonsillectomy1995 :• 3 or more episodes/yearAAO-HNS / Guidelines for Tonsillectomy1995 :• 3 or more episodes/year• Hypertrophy causing dental malocclusion.• Hypertrophy causing upper airway obstruction, severe
d sphagia sleep disorder cardiop lmonar
• Hypertrophy causing dental malocclusion.• Hypertrophy causing upper airway obstruction, severe
d sphagia sleep disorder cardiop lmonardysphagia, sleep disorder, cardiopulmonary complications
• One attack of quinsy.
dysphagia, sleep disorder, cardiopulmonary complications
• One attack of quinsy.One attack of quinsy.• Halitosis, not responsive to medical therapy• UTE, suspicious for malignancy
One attack of quinsy.• Halitosis, not responsive to medical therapy• UTE, suspicious for malignancy, p g y• Chronic or recurrent tonsillitis associated with
streptococcal carrier state .
, p g y• Chronic or recurrent tonsillitis associated with
streptococcal carrier state .• Individual considerations• Individual considerations
Other Indications Other Indications Other Indications Other Indications for Tonsillectomyfor Tonsillectomyfor Tonsillectomyfor Tonsillectomy
Marshall’s syndrome or PFAPA syndrome
(periodic fever aphthous stomatitis
Marshall’s syndrome or PFAPA syndrome
(periodic fever aphthous stomatitis(periodic fever, aphthous stomatitis,pharyngitis, cervical adenitis)
(periodic fever, aphthous stomatitis,pharyngitis, cervical adenitis)

Tonsillectomy and AllergyTonsillectomy and AllergyTonsillectomy and AllergyTonsillectomy and Allergy
• Does tonsillectomy potentiates the severity • Does tonsillectomy potentiates the severity y p yof bronchial asthma?
y p yof bronchial asthma?
• Does bronchial asthma constitute an• Does bronchial asthma constitute an• Does bronchial asthma constitute an absolute/relative/or no contraindication to t ill t ?
• Does bronchial asthma constitute an absolute/relative/or no contraindication to t ill t ?tonsillectomy? tonsillectomy?

•In a non-asthmatic atopic patient, does tonsillectomy increases the probability of o s ec o y c e ses e p ob b y odeveloping asthma?
[T ill i[T ill i[Tonsillectomy in recent references]
[Tonsillectomy in recent references]f ]f ]
• Tonsillectomy has no general immune consequences. y g q
• Pre-existing allergy or asthma is not a contraindication to tonsillectomy.contraindication to tonsillectomy.
• Tonsillectomy doesn’t have a deleterious impact on allergic childrenallergic children.

• Any role for ASOT in dictating indications for tonsillectomy?
• Any role for ASOT in dictating indications for tonsillectomy? yy
• Does a very high ASOT, necessitates any • Does a very high ASOT, necessitates any y g , ytreatment at all?
y g , ytreatment at all?

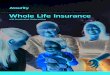
TitreTitre
300350400450
ASOT
100150200250300
050
ction 1 2 3 4 5 6 7 8 9 10
MonthMonthOnse
t of I
nfect
O
D i i f il hi f h i hD i i f il hi f h i h• Does a positive family history of rheumatic heart disease affects your decision about performing a tonsillectomy?
• Does a positive family history of rheumatic heart disease affects your decision about performing a tonsillectomy?tonsillectomy? tonsillectomy?

Is a throat swab a Is a throat swab a good diagnostic
t t?good diagnostic
t t?test?test?
• The throat swab is currently recommended as a diagnostic• The throat swab is currently recommended as a diagnostic• The throat swab is currently recommended as a diagnostic aid in patients with sore throat.The quoted sensitivity is (26-30%) and specificity (73-80%)
• The throat swab is currently recommended as a diagnostic aid in patients with sore throat.The quoted sensitivity is (26-30%) and specificity (73-80%)
• This low predictive value of throat swabs is probably due to a high symptomless carriage rate of group A ß haemolytic streptococcus (ranging from 6% to 40% ).
• This low predictive value of throat swabs is probably due to a high symptomless carriage rate of group A ß haemolytic streptococcus (ranging from 6% to 40% ). y p ( g g )
• In approximately one-third of patients with pharyngitis or tonsillitis, even with elaborate culture techniques no microbiologic etiology can be detected
y p ( g g )• In approximately one-third of patients with pharyngitis or
tonsillitis, even with elaborate culture techniques no microbiologic etiology can be detectedmicrobiologic etiology can be detected.
• Furthermore, non-pathogenic resident flora frequentlycontaminate the microbiological specimen, making the res lts of laborator c lt re reports of do btf l clinical
microbiologic etiology can be detected. • Furthermore, non-pathogenic resident flora frequently
contaminate the microbiological specimen, making the res lts of laborator c lt re reports of do btf l clinicalresults of laboratory culture reports of doubtful clinical value results of laboratory culture reports of doubtful clinical value
Indications for Indications for Indications for Indications for TonsillectomyTonsillectomyTonsillectomyTonsillectomy
AAO-HNS:• 3 or more episodes/yearAAO-HNS:• 3 or more episodes/year• Hypertrophy causing dental malocclusion.• Hypertrophy causing upper airway obstruction,
d h i l di d di l
• Hypertrophy causing dental malocclusion.• Hypertrophy causing upper airway obstruction,
d h i l di d di lsevere dysphagia, sleep disorder, cardiopulmonary complications
• One attack of quinsy
severe dysphagia, sleep disorder, cardiopulmonary complications
• One attack of quinsy• One attack of quinsy.• Halitosis, not responsive to medical therapy• UTE suspicious for malignancy
• One attack of quinsy.• Halitosis, not responsive to medical therapy• UTE suspicious for malignancy• UTE, suspicious for malignancy• Chronic or recurrent tonsillitis associated with
streptococcal carrier state .
• UTE, suspicious for malignancy• Chronic or recurrent tonsillitis associated with
streptococcal carrier state .p• Individual considerations
p• Individual considerations

• Does prophylactic antibiotics have a role in the • Does prophylactic antibiotics have a role in the management of tonsillo-pharyngitis?management of tonsillo-pharyngitis?
Potential Indications ofPotential Indications ofPotential Indications of Prophylactic AntibioticsPotential Indications of Prophylactic Antibioticsp yp y
• Recurrent tonsillo-pharyngitis.Hi h ASOT
• Recurrent tonsillo-pharyngitis.Hi h ASOT• High ASOT.
• Rheumatic fever.• High ASOT.• Rheumatic fever.• Conservative trial to preserve the tonsils
before surgery is stated.• Conservative trial to preserve the tonsils
before surgery is stated.before surgery is stated.• Adeno-tonsillar hyperplasia may
respond to one month of therapy with
before surgery is stated.• Adeno-tonsillar hyperplasia may
respond to one month of therapy withrespond to one month of therapy with beta-lactamase resistant antibioticsrespond to one month of therapy with beta-lactamase resistant antibiotics

Prophylactic AntibioticsProphylactic Antibiotics
• Long-acting penicillin• Long-acting penicillin
• Amoxycillin (20 mg/kg/day given either as a single dose )
• Amoxycillin (20 mg/kg/day given either as a single dose )g )
• Azithromycin (10 mg/kg given weekly)
g )
• Azithromycin (10 mg/kg given weekly)
• Trimethoprim/sulfamethoxazole (6.8/34 mg/kg/day divided into two daily doses)
• Trimethoprim/sulfamethoxazole (6.8/34 mg/kg/day divided into two daily doses) g g y y )g g y y )
Case StudyCase Study
• A 3 y boy presents to your office whose l i h h l dl d
• A 3 y boy presents to your office whose l i h h l dl dparents complain that he snores loudly and
stops breathing sometimes while sleeping. parents complain that he snores loudly and stops breathing sometimes while sleeping. The child’s pediatrician told the parents that his tonsils were “big” and that the child isThe child’s pediatrician told the parents that his tonsils were “big” and that the child ishis tonsils were big and that the child is under weight for his agehis tonsils were big and that the child is under weight for his age

• Also has dysphagia and daytime somnolence
• Also has dysphagia and daytime somnolencesomnolence
• Apneic spells last >10 secondssomnolence
• Apneic spells last >10 seconds• PMH:
– otherwise healthy• PMH:
– otherwise healthyotherwise healthy– Tonsillitis: Seldom
otherwise healthy– Tonsillitis: Seldom
• No allergies• No allergies
• PE:• PE:• PE:– Dark circles under eyes
• PE:– Dark circles under eyes
– Breathing with mouth open
– Small amount of clear
– Breathing with mouth open
– Small amount of clear rhinorrhea
– Tonsils are almost touching
rhinorrhea
– Tonsils are almost touchingTonsils are almost touching in the midlineTonsils are almost touching in the midline

DiagnosisDiagnosis
• Adenotonsillar hypertrophy.• Adenotonsillar hypertrophy.
• OSA.• OSA.
ManagementManagement
• Any role for conservative therapy?• Any role for conservative therapy?

Surgical choiceSurgical choice
• TonsillectomyAd ill
• TonsillectomyAd ill• Adeno-tonsillectomy
• Unilateral tonsillectomy• Adeno-tonsillectomy• Unilateral tonsillectomyy• Tonsillotomy
y• Tonsillotomy