Embed Size (px)
Citation preview

•1
Pediatrics
Abusive Head Trauma:Differential Diagnosis
Christopher S. Greeley, MD, MSChief, Section of Public Health PediatricsTexas Children’s HospitalProfessor of PediatricsVice‐Chair of Community HealthBaylor College of Medicine
Pediatrics
•I have no personal, professional or financial relationships to declare
Disclosure
Pediatrics David, Ped Rad 2008 Pediatrics
Differential Diagnosis of SDH
•Accidental trauma•Headbanging•Breakdancing•Roller coaster rides•Lumbar puncture•Spinal anesthesia•Epidural anesthesia•Myelography•Ventricular shunt•Craniotomy
•Intrauterine trauma•Idiopathic intrauterine SDH•Intrauterine ITP•Pre-eclampsia•Birth Trauma•Glutaric aciduria•Galactosemia•Pyruvate carboxylase def•AVM, aneurysm•Arachnoid cysts
Hymel, Jenny: Child Maltreatment 2002

•2
Pediatrics
Differential Diagnosis of SDH
•Osteogenesis imperfecta•Sickle cell anemia•Allagille syndrome•Ehlers-Danlos syndrome•Menkes kinky hair disease•Polycystic kidney•Meningeal carcinomatosis•Leukemia, lymphoma•Brain tumors•Lupus
•Anticoagulation disorders•Liver failure•Hemophilia A and B•Factor V deficiency•Factor XII deficiency•Factor XIII deficiency•TTP•Hemorrhagic disease of newborn
•DIC
Hymel, Jenny: Child Maltreatment 2002Pediatrics
Differential Diagnosis of SDH
•Acquired clotting factor inhibitors
•Alpha 1 antitrypsin def•H flu meningitis•Strep pneumonia meningitis
•Kawasaki disease•Endocarditis with septic emboli
•Sinus infection with intracranial complication
•Malaria•Herpes simplex encephalitis
•Congenital toxoplasmosis•Lead poisoning•Cocaine ingestion•Hemodialysis•Moya Moya disease•Bone marrow transplant•Spontaneous intracranial hypotension
Hymel, Jenny: Child Maltreatment 2002
Pediatrics Levin, Ped Clin Nor Amer, 2009 Pediatrics
•A single case report?•A case series in adults?•A case series in children?•Historical “validation”•Expert opinion?
What Constitutes a “Mimic”

•3
Pediatrics
•Accidents/trauma•Benign Expansion of the Subarachnoid Spaces (BESS)•Bleeding disorders•Glutaric Aciduria•Menkes Disease•Scurvy•Birth•Hypoxia/choking
Outline
Pediatrics
•Provide clinical context for additional considerations in the evaluation of suspected AHT
•Will not be able to address all possibilities
Purpose
Pediatrics Pediatrics
Accidents
Pediatrics
•Several series compare outcomes from AHT and accidental injuries (including many with falls)
‐ Billmire (Pediatrics, 1984)‐ Duhaime (Pediatrics, 1992)‐ Goldstein (Crit Care Med, 1993)‐ Ewing-Cobbs (Pediatrics, 1998)‐ Reece/Sege (Arch Pediatr Adolesc Med, 2000)‐ Ewing-Cobbs (Child’s Nerv Syst, 2000)‐ DiScala (Arch Pediatr Adolesc Med, 2000)‐ Kelly (New Zealand Med J, 2004)‐ Bechtel (Pediatrics, 2004)‐ Tung (Pediatrics, 2006)‐ Myhre (Acta Paediatrica, 2007)
Accidental Injuries

•4
Pediatrics Pediatrics
Accidental Injuries
Pediatrics Pediatrics
Systematic Review
Maguire et al, Arch Dis Child, 2009
N=1655 children(779 AHT)
Pediatrics
•In a child with Intracranial hemorrhage:‐Apnea has PPV .93, OR 17.06
•(CI 5.018 to 58.011)‐RH has PPV .71, OR 3.50
•(CI 1.088 to 11.280)‐Rib fractures have PPV .73, OR 3.03 (NS)
•CI (0.716 to 12.799); few in sample
Significant Findings
Maguire et al, Arch Dis Child, 2009 Pediatrics
•Prospective study of 45 confessed AHT vs39 publicly witnessed accidental injuries
‐ ICP, seizures, coma more frequent‐SDH, mixed SDH, ischemia more frequent‐Extracranial fractures more frequent‐RH more frequent (85% vs 15%)‐Mortality greater (22% vs 5%)‐Scalp swelling, skull fracture less frequent‐Radiographic evidence of impact less frequent (22% vs 67%)
Confessed AHT vs Accidents
Vinchon, Childs Nerv Syst 2010

•5
Pediatrics
Sensitivity Specificity + Predictive value
- Predictive value
Chi Square
Brain ischemia
0.267 0.971 0.921 0.505 < 0.01
SDH 0.822 0.552 0.685 0.724 <0.001
Severe RH 0.556 0.974 0.961 0.655 <0.001
Absent scalp swelling
0.978 0.769 0.830 0.968 <0.001
SDH, RH,NO scalp swelling
0.244 1.00 1.00 0.534 <0.001
Confessed AHT vs Accidents
Vinchon, Childs Nerv Syst 2010
Pediatrics
•EDH more common in accidental•SDH more common in AHT •Skull fractures, subarachnoid hemorrhage, contusions not more frequent in AHT•Retinal hemorrhages more common in AHT
‐Especially those that extend to periphery, cover macula, subretinal or multilayered, retinoschisis
AHT vs Accidental Injuries
Pediatrics
•20 published studies (1969-1994) representing 1902 pediatric falls
‐18 of 23 deaths resulted from falls of more than 3 stories in height
•Helfer et al. (1977), Nimityongskul & Anderson (1987), Kravitz et al. (1969), Williams (1991), Lyons & Oates (1993), Selbst et al (1990), Levitt & McCormick (unpublished), Chadwick et al. (1991), Mayr et al. (1994 & 1999), Tarantino et al (1999), Gruskin & Schutzman (1999), Joffe & Ludwig (1988), Chiavello et al. (1994), Smith et al. (1997), Rivara et al. (1993), Barlow et al. (1983), Smith et al. (1975), Musemeche et al. (1991), Lehman & Schonfeld (1993), Annobil et al. (1995)
Can Falls Kill Young Children?
Pediatrics
•Helfer et al, Pediatrics, 1977‐Hospital witnessed group‐Fell off of beds, cribs or changing tables
•85 kids, 1 skull fracture•“No serious sequellae”
Short Falls Are Safe
•6
Pediatrics
•“Falling Out of Bed: A Relatively Benign
Occurrence”‐207 Children, <6 years, height <41-54 inches‐29 contusions, 1 skull fx, 1 clavicle fx‐“No serious, multiple, visceral or life-threatening injuries.”
Short Falls Are Safe
Lyon & Oates, Pediatrics, 1993 Pediatrics
•75,000 consumer safety protection records•18 deaths from falls
‐2-10 feet‐1-13 years old
Pediatrics Plunkett, Am J For Med & Path, 2001
Pediatrics Plunkett, Am J For Med & Path, 2001
*N.B. None had lucid interval >10 minutes, SDH and RH
*N.B. Did not contain any infants[9/18 were >4 years old]

•7
Pediatrics Pediatrics
•MMWR (CDC) database for 2001•55 fatal falls for 0-4 (20 million children)
‐1,039,275 non fatal falls‐Height of fall not identified‐Age not broken down more than “0-4”
Can Falls Kill Young Children?
Pediatrics CDC, MMWR, 2004 Pediatrics
•Estimates toddlers fall 3-5 times per week
‐200 per year
•3.2 billion fall per year (USA)‐For 0-4 year olds‐Rate of falls for <0 yr would be lower
•1 death for every 58 million falls
Can Falls Kill Young Children?

•8
Pediatrics Pediatrics
Pediatrics Pediatrics

•9
Pediatrics
(Avon Longitudinal Study of Parents and Children)
Pediatrics
•Survey of 14,009 children•Survey at 6 months
‐Asked about household injuries
•3357 (24%) falls reported‐76% reported only one fall‐Bed 33%, Sofa 20%
•437 (13%, 3%) had an injury‐375 (97%) were to the head‐21 (<1%) were serious; contusion‐3 had skull fractures‐No deaths
Pediatrics
•19 cases of reported short fall deaths (< 6 ft)
‐None witnessed
•14 (74%) had clear evidence of homicide•3 (15.5%) indeterminate•2 (10.5%) ‘genuinely’ accidental falls
‐21 mo fell 5-6 ft from top bunk, SDH/edema‐17 mo fell backward 2-3 ft from rocking chair, SDH, SAH, parietal contusion
Evaluation of Lethal Falls
Reiber, Am J Forens Med Pathol (1993)
Pediatrics
•Review of 26 studies of accidental falls•Life threatening injuries extremely uncommon in falls < 4 ft (think epidural hematoma)
‐Odds of death in aggregate 23/1,902•18 from falls > 3 stories
‐Risk of fatality otherwise 5/1,902 = 0.26%•Most injuries involve skull fractures, epidural hemorrhage, SAH, small contusions
‐SDH rare but does occur•Generally small, focal and underlying skull fx or STS
The Benignity of Short Falls
Dias MS, Neurosurg Clin N Am (2002)
•10
Pediatrics
•Yes, rarely, short falls kill young children‐Adults falling down stairs while carrying an infant‐Children in walkers falling down stairs‐Bunk bed falls‐Playground falls from swings
•Often with medical complications‐Stroke, hyponatremia, surgical mass
Can Short Falls Kill Young Children?
Pediatrics
•If they include the following‐Epidural hematoma‐Focal subdural hematomas acting with mass effect
‐Cervical spine fractures
•? mimic of Abusive Head Trauma
Can Short Falls Kill Young Children?
Pediatrics
•Babies fall•They hit their heads•Death from falls are exceedingly rare
‐But can happen
Take Homes
Pediatrics Pediatrics
Benign Expansion of theSubarachnoid Spaces (BESS)

•11
Pediatrics
•Many terms‐External hydrocephalus*‐Benign Subdural Collections‐Benign Extracerebral Fluid Collections†‐Psuedohydrocephalus-megalocephaly #
•Collection of CSF in the arachnoid space
‐“Real” vs. “potential” vs. “pathologic” spaces
Benign Expansion of theSubarachnoid Spaces (BESS)
*Dandy & Blackfan, AJDC, 1914 † Hamza, Ped Neuro, 1986
# Sahar, 1978
Pediatrics
•Common features‐Frontal subarachnoid collection (? how big)‐Prominent interhemishperic fissure‐Hypodense on CT
•Little or no ventriculomegaly
•All other growth parameters are normal•Usually has a family history (80-90%)
‐Some have persistent ↑OFC
Benign Expansion of theSubarachnoid Spaces (BESS)
Pediatrics
•Head circumference rises predictably and smoothly
•2/3 boys•50% with FH of macrocephaly
•Many have occipital plagiocephaly
•Developmentally normal except gross motor
•Characteristic CT appearance
Benign Expansion of theSubarachnoid Spaces (BESS)
Dias, Peds Clinics North Am (1998)
Pediatrics
•Enlarged CSF spaces•Isodense to CSF in ventricle
•Enhanced CT shows vessels crossing subarachnoid space
•Ventricular enlargement in about half
•Occipital plagiocephaly
Benign Expansion of theSubarachnoid Spaces (BESS)

•12
Pediatrics
•15 infants, had serial head CT‐Normal development, macrocrania, BESS‐IV contrast did not outline a membrane
•Follow-up in 6 to 36 months•Older children had OFC return to “normal”
‐Usually by 36 months
Benign Expansion of theSubarachnoid Spaces (BESS)
Carolan et al, Ped Neurosci 1986Pediatrics
•67 infants with widened subarachnoid space•22% had macrocrania
•Usually requires no therapy•? Due to defect in CSF absorption•Theoretically predisposes to SDH
‐Stretching of the cortical bridging veins
Benign Expansion of theSubarachnoid Spaces (BESS)
Odita, Child’s Nerv Sys, 1992
Pediatrics
BESS
Pediatrics
Chronic Subdural Hemorrhage

•13
Pediatrics
•Described in contrasted CT and MRI•Used to distinguish BESS (arachnoid) from CSH•Superficial cortical veins seen crossing the arachnoid space
‐Not seen crossing subdural collections
“Cortical Vein Sign”
McCluney et al, AJNR, 1992
Pediatrics
“Cortical Vein Sign”
McCluney et al, AJNR, 1992
Pediatrics Pediatrics
Ultrasound
Amodio et al, Ped Rad 2005Pediatrics Pediatrics
Ultrasound (venous waveform)
Amodio et al, Ped Rad 2005

•14
Pediatrics
•“Usually” arachnoid in location•Similar finding may be seen in CSH•Origin unclear
‐Persistent cortical vein‐Vascular channel from neomembrane
Cortical Bridging Vein
Pediatrics
MRI
Amodio et al, Ped Rad 2005
Pediatrics
MRI
Amodio et al, Ped Rad 2005Pediatrics
•15
Pediatrics
•Retrospective review, EHR, large practice network•All children <2 yrs with
‐2 visits, HC measurement
•Excluded‐Predisposing CNS disease, clear history of trauma
•Diagnosed with BESS on neuroimaging‐For macrocephaly or increased HC
Methods
McKeag et al, J Nsgy Peds, 2013Pediatrics
•CT or MRI of head‐No US
•All EHR reviewed•Those with intracranial bleeding on imaging
‐had a CPT review‐Had neuroimaging reviewed
Methods
McKeag et al, J Nsgy Peds, 2013
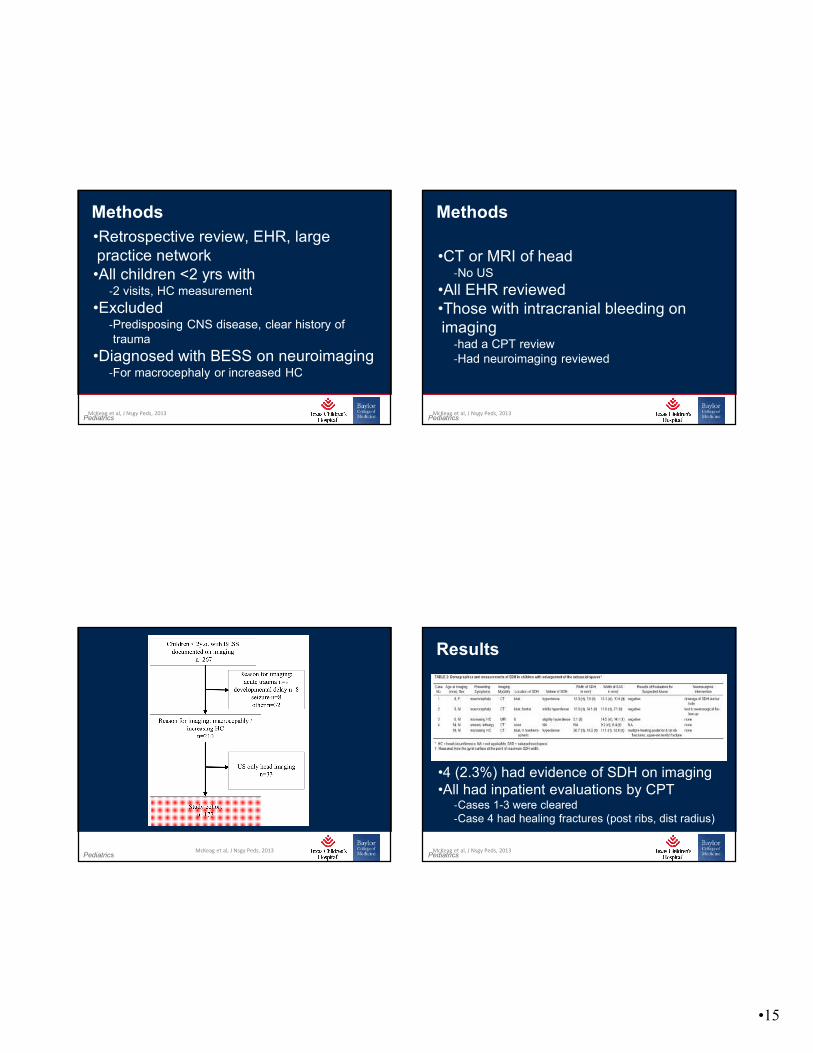
Pediatrics McKeag et al, J Nsgy Peds, 2013
Pediatrics
•4 (2.3%) had evidence of SDH on imaging•All had inpatient evaluations by CPT
‐Cases 1-3 were cleared‐Case 4 had healing fractures (post ribs, dist radius)
Results
McKeag et al, J Nsgy Peds, 2013

•16
Pediatrics
•8/177 (4.5%) had history of trauma‐1 week – 3 months prior
•1 of the 8 had SDH on neuroimaging‐Case 4 described earlier
Results
McKeag et al, J Nsgy Peds, 2013Pediatrics
•1 in 4 with BESS and SDH had concerns for CAN•“Thus, screening for occult injuries, including skeletal survey and ophthalmological evaluation, is needed in children with an SDH regardless of the presence of enlarged extraaxial spaces.”•Unclear causation (which came first)
Discussion
McKeag et al, J Nsgy Peds, 2013
Pediatrics
Fingarson, A. K., et al. (2016). "Enlarged subarachnoid spaces and intracranial hemorrhage in children with accidental head trauma."
J Neurosurg Pediatr: 1‐5. Pediatrics
•Purpose: do children with BEH have an increased risk of SDH with minor head trauma
Background
Fingarson, A. K., et al. (2016). "Enlarged subarachnoid spaces and intracranial hemorrhage in children with accidental head trauma."
J Neurosurg Pediatr: 1‐5.

•17
Pediatrics
•Retrospective, EHR review, 1-24 months old, June 2006-July 2012•Head CT for a fall < 6 feet•Also EPIC search for broad injury codes
‐Exclude prior injury, underlying neurological disease, or abuse diagnosis
•Images were of good quality, 2 masked neuroradiologists
‐Measured the EAS in standard fashion; defined as >4mm
‐All hemorrhages were described
Methods
Fingarson, A. K., et al. (2016). "Enlarged subarachnoid spaces and intracranial hemorrhage in children with accidental head trauma."
J Neurosurg Pediatr: 1‐5. Pediatrics
Results
Fingarson, A. K., et al. (2016). "Enlarged subarachnoid spaces and intracranial hemorrhage in children with accidental head trauma."
J Neurosurg Pediatr: 1‐5.
Pediatrics
Results
Fingarson, A. K., et al. (2016). "Enlarged subarachnoid spaces and intracranial hemorrhage in children with accidental head trauma."
J Neurosurg Pediatr: 1‐5. Pediatrics
•“There was no difference in the rate of ICH in children who fell less than 3 feet versus 3–6 feet.”
Results
Fingarson, A. K., et al. (2016). "Enlarged subarachnoid spaces and intracranial hemorrhage in children with accidental head trauma."
J Neurosurg Pediatr: 1‐5.

•18
Pediatrics
•BEH was not associated with SDH after minor trauma•BEH was associated with overall increased ICH
‐Specifically SAH/SPH, and multiple ICHs
Discussion
Fingarson, A. K., et al. (2016). "Enlarged subarachnoid spaces and intracranial hemorrhage in children with accidental head trauma."
J Neurosurg Pediatr: 1‐5. Pediatrics
Tucker, J., et al. (2016). "Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections”
J Neurosurg Pediatr: (18)1: 16‐20
Pediatrics
•Purpose: determine the frequency of BESS, hydrocephalus and subdural collections in children with macrocephaly
‐And to determine the prevalence of subdural collections in children with BESS
Background
Tucker, J., et al. (2016). "Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections”
J Neurosurg Pediatr: (18)1: 16‐20 Pediatrics
•Radiology reports searched for “macrocephaly”‐Single institution, May 2009-May 2015, CT or MRI or US‐Children younger than 2 years old‐Excluded with history of trauma or abuse
•All images reviewed by single neurosurgeon•Standardized subarachnoid measurements made
‐BESS graded 0-2 based on size (<5 mm, 5-9 mm, 10 mm)
Methods
Tucker, J., et al. (2016). "Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections”
J Neurosurg Pediatr: (18)1: 16‐20

•19
Pediatrics
•538 studies were included‐311/538 (57.8%) had BESS‐265/538 (49.2%) had BESS grade 1‐46/538 (8.6%) had BESS grade 2
•21/538 (3.9%) had incidental SDH‐18/21 in children with BESS 1 or 2
Results
Tucker, J., et al. (2016). "Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections”
J Neurosurg Pediatr: (18)1: 16‐20 Pediatrics
Results
Tucker, J., et al. (2016). "Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections”
J Neurosurg Pediatr: (18)1: 16‐20
Pediatrics
•Goal to look at findings in children with macrocephaly•These results may not be generalizable
‐Institution specific care
•Increasing degrees of BESS associated with increasing prevalence of subdural collections
Discussion
Tucker, J., et al. (2016). "Macrocephaly in infancy: benign enlargement of the subarachnoid spaces and subdural collections”
J Neurosurg Pediatr: (18)1: 16‐20 Pediatrics
To state that in children with external hydrocephalus a subdural hematoma can result from minor trauma is potentially to allow inflicted injury to be seen as accidental. Unfortunately, to fail to recognize that minor trauma can cause a subdural hematoma in children with external hydrocephalus is potentially to allow accidental injury to be seen as inflicted.
Pittman
Pittman, Pediatric Neurosurgey 2003

•20
Pediatrics
It is my opinion that, in the absence of other evidence of inflicted injury, the presence of a subdural hematoma in a child with external hydrocephalus is, by itself, insufficient to prove abuse.
Pittman
Pittman, Pediatric Neurosurgey 2003Pediatrics
My Take
•The issue of “BESS” is quite complicated‐Many different terms
•Differentiating “Chronic” SDH from “BESS” on CT alone is challenging•Significant surveillance bias•Unlikely that BESS represents a significant risk of developing a SDH from trivial trauma
Pediatrics Pediatrics
Bleeding Disorders
Pediatrics
•Multiple case reports•Diagnosis based upon history and physical examination
‐Family history
•Targeted testing
Bleeding Disorders

•21
Pediatrics
•Bleeding Disorders‐Vitamin K Deficiency Bleeding (VKDB)‐Von Willebrand Disease‐Hemophilia A (FVIII deficiency)‐[Factor XIII deficiency]
•Trauma Related Coagulopathy
Bleeding Disorders
Pediatrics
•Needed for the production of clotting factors
‐Hemorrhagic Disease of the Newborn‐Vitamin K Deficiency Bleeding (VKDB)
•Three historic forms‐Early (<24 hours)‐Classic (1-7 days)‐Late (2-12 weeks)
Vitamin K Deficiency
Pediatrics
•Usually present as neonate‐Maternal VKD‐No later than 12 weeks
•Breast Feeding increases risk of VKD•Medical Conditions can impair VK absorption
‐Biliary atresia‐Alagille’s Syndrome‐CF‐Intestinal Malabsorption
Vitamin K Deficiency
Pediatrics
•Clinical features‐RH‐ICH, usually SAH‐No fractures, no retinoschisis/retinal folds
•Elevated PT and aPTT‐Elevated PIVKA-II
•Not been reported with normal studies
Vitamin K Deficiency Bleeding

•22
Pediatrics Pediatrics, 1995
PT 19PTT 47
Pediatrics Pediatrics, 1995
Pediatrics J Emergency Medicine, 2005
PT 130PTT 96
Pediatrics J Emergency Medicine, 2005

•23
Pediatrics
•Coagulation should be tested for in all children with intracranial bleeding•Read:
‐Shearer MJ, Vitamin K deficiency bleeding (VKDB) in early infancy. Blood Reviews Vol 23, Iss 2, 2009, pp 49-59
Vitamin K Deficiency Bleeding
Pediatrics
•Traumatic Brain Injury‐Coagulation abnormalities in 1/3 of TBI‐In children as high as ¾ of TBI
Trauma Related Coagulopathy
Pediatrics
Trauma Related Coagulopathy
Stein & Smith, Neurocrit Care, 2004Pediatrics
Talving P et al, Journal of Trauma‐Injury Infection & Critical Care:November 2011 ‐ Volume 71 ‐ Issue 5 ‐ pp 1205‐1210

•24
Pediatrics
•Coagulopathy defined (and/or)‐Plts <100,000‐INR >1.2‐aPTT>36 sec
•Primary outcome = coagulopathy developed•Secondary outcomes = various clinical measures, mortality
Methods
Talving P et al, Journal of Trauma 2011 Pediatrics Pediatrics
Results
Talving P et al, Journal of Trauma 2011
320 kids88% blunt injury
43% (137/320) developedcoagulopathy
Pediatrics Pediatrics
Results
Talving P et al, Journal of Trauma 2011
“With increasinghead AIS, the incidence of coagulopathy increased in astepwise fashion”
Pediatrics Pediatrics
Results
Talving P et al, Journal of Trauma 2011

•25
Pediatrics Talving P et al, Journal of Trauma
2011 Pediatrics
•7 month old, fall down stairs•PT 17.6•PTT >200•Plt Count 247,000
Pediatrics Lantz and Couture, 2011
Pediatrics Lantz and Couture, 2011

•26
Pediatrics Talving P et al, Journal of Trauma
2011 Pediatrics
•Modest coagulopathy can develop in children with severe TBI•The more severe the injury the greater the odds of developing coagulopathy•Profound coagulopathy would be unexpected
‐Think underlying bleeding disorder
Conclusions
Pediatrics
•CBC, with platelet count•Review of peripheral smear
‐Platelet size and form
•aPTT•PT (INR)•[PIVKA-II level]
First Line Testing
Pediatrics
•“Prothrombin/Protein Induced by Vitamin K Absence/Antagonism”
‐Vitamin k absence produces a spectrum of undercarboxylated or partially carboxylatedmolecules (thrombin precursors/FII)
•20% have elevation in cord blood‐Mothers with poor nutrition
PIVKA II

•27
Pediatrics
•Independent from PT•Can have elevated PT with normal PIVKA
‐From non-VKDB causes
•“In overt VKDB, PIVKA-II is always present at extremely high levels and, with a half-life of ~60 h, can still be detected in samples collected days and even weeks after vitamin K and/or blood products have been given to correct coagulopathy.”
PIVKA II
Clarke and Shearer, Arch Dis Child 2007 Pediatrics
•Specific Factor Levels‐Factor XIII activity
•vWF antigen level•vWF ristocetin cofactor assay (vWF:RCo)•Platelet function (i.e. PFA-100)•Thrombin Time•Fibrinogen assay
Second Line Testing
Pediatrics
Anderst et al, Pediatrics, 2013Pediatrics Pediatrics
Glutaric Aciduria
•28
Pediatrics
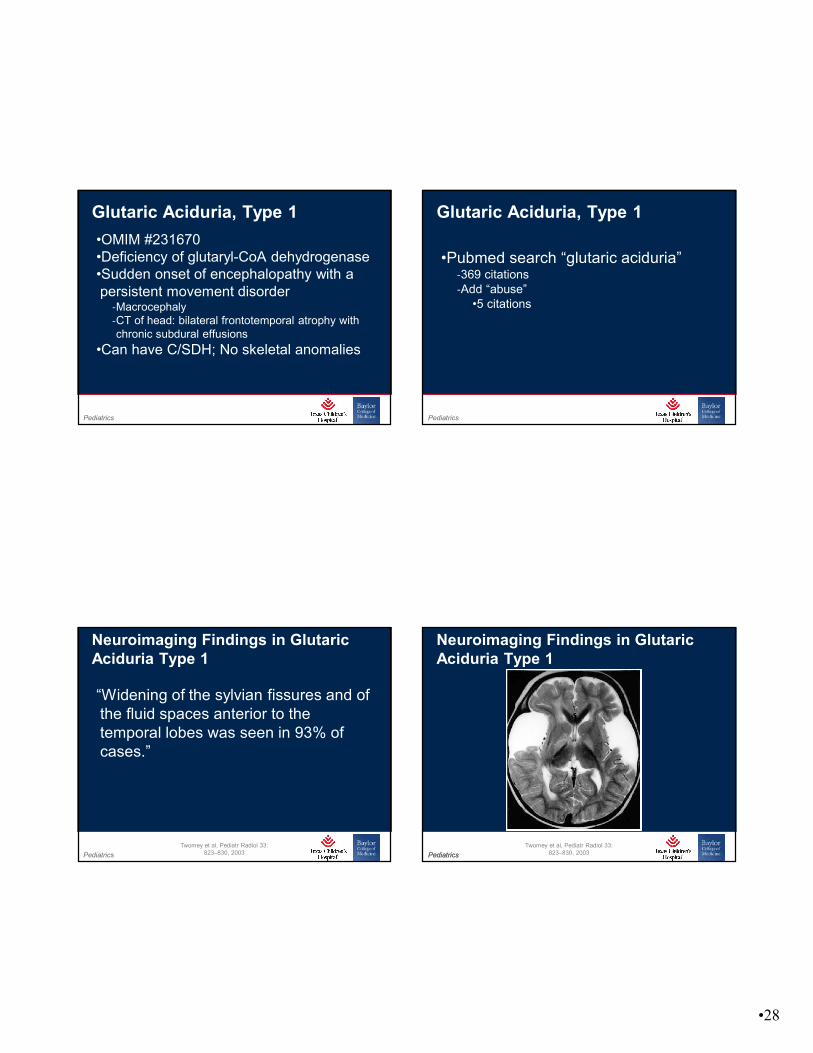
•OMIM #231670•Deficiency of glutaryl-CoA dehydrogenase•Sudden onset of encephalopathy with a persistent movement disorder
‐Macrocephaly‐CT of head: bilateral frontotemporal atrophy with chronic subdural effusions
•Can have C/SDH; No skeletal anomalies
Glutaric Aciduria, Type 1
Pediatrics
•Pubmed search “glutaric aciduria”‐369 citations‐Add “abuse”
•5 citations
Glutaric Aciduria, Type 1
Pediatrics
“Widening of the sylvian fissures and of the fluid spaces anterior to the temporal lobes was seen in 93% of cases.”
Neuroimaging Findings in GlutaricAciduria Type 1
Twomey et al, Pediatr Radiol 33: 823–830, 2003 Pediatrics Pediatrics
Neuroimaging Findings in GlutaricAciduria Type 1
Twomey et al, Pediatr Radiol 33: 823–830, 2003

•29
Pediatrics Pediatrics
Hedlund & Frasier, For Sci Med Path 2009
Glutaric Aciduria, Type 1
Pediatrics
•Diagnosis:‐Urine Organic Acids‐Plasma glutarylcarnitine‐Glutaryl-CoA dehydrogenase activity in leukocytes or cultured fibroblasts
Glutaric Aciduria, Type 1
Pediatrics
•6 month old, macrocephaly, subdural effusions
‐Evaluated for abuse
•Noted to have RH and chronic SDH•Skeletal survey negative•“high levels of glutaric and 3-hydroxyglutaric acid.”
Intraretinal Hemorrhages AndChronic Subdural Effusions
Gago et al, Retina, 2003
Pediatrics Gago et al, Retina, 2003

•30
Pediatrics Gago et al, Retina, 2003
Pediatrics Gago et al, Retina, 2003
Pediatrics
•Reviewed published literature in which SDH was present in children with GA-1
Pediatrics Vester et al, For Sci Med Path, 2015
•31
Pediatrics Vester et al, For Sci Med Path, 2015 Pediatrics Vester et al, For Sci Med Path, 2015
Pediatrics Pediatrics
Menkes
Pediatrics
•Lethal X-Linked Recessive •Low Copper, Low ceruloplasmin
‐Decreased activity of Cu+2 containing enzymes
•OMIM #309400, •1 in ~250,000 births•Heterogenous clinical course
‐Most are “classic” MD
•Present with seizures (2-3months)‐Developmental delay
Menkes “Kinky” Hair Syndrome

•32
Pediatrics
•Fetal hair unaffected‐Becomes “kinky” (steel wool) by 2-3 months
•Wormian bones, osteopenia, metaphyseal widening, ?rib fractures•Neurologic deterioration, intra-cranial bleeding, Cerebral atrophy•Vascular tortuosity
‐Intracranial, visceral hemorrhages
Menkes Disease
Pediatrics
Tümer and Møller, Eur J Human Gen, 2009
Pediatrics
Tümer and Møller, Eur J Human Gen, 2009 Pediatrics Pediatrics
Menkes Disease

•33
Pediatrics Pediatrics
Menkes Disease
Pediatrics
Menkes Disease
Bacopoulou, Arch Dis Child. 91(11): 919, 2006
Pediatrics
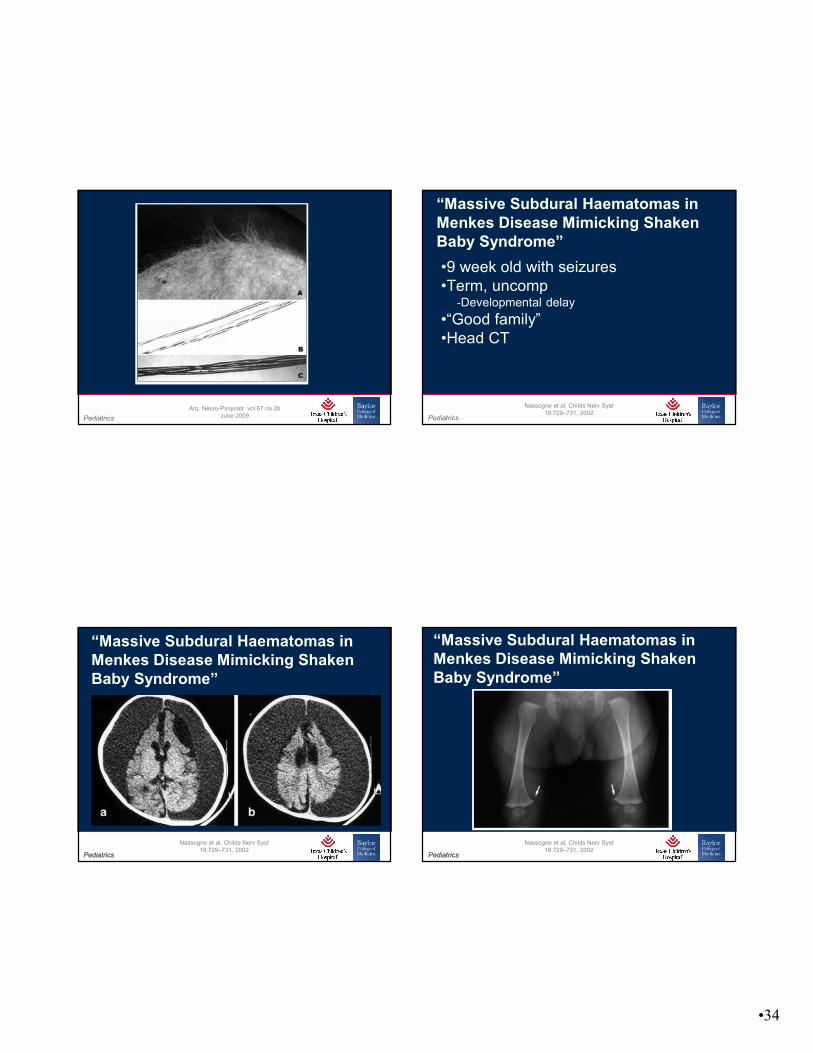
•9 month old with seizures•Term, uncomp
‐Developmental delay
•“Good family”•Head CT
“Menkes Disease as a Differential Diagnosis of Child Abuse”
Arq. Neuro-Psiquiatr. vol.67 no.2b June 2009 Pediatrics
Arq. Neuro-Psiquiatr. vol.67 no.2b June 2009
•34
Pediatrics
Arq. Neuro-Psiquiatr. vol.67 no.2b June 2009 Pediatrics
•9 week old with seizures•Term, uncomp
‐Developmental delay
•“Good family”•Head CT
“Massive Subdural Haematomas in Menkes Disease Mimicking Shaken Baby Syndrome”
Nassogne et al, Childs Nerv Syst18:729–731, 2002
Pediatrics Pediatrics
“Massive Subdural Haematomas in Menkes Disease Mimicking Shaken Baby Syndrome”
Nassogne et al, Childs Nerv Syst 18:729–731, 2002
Pediatrics Pediatrics
“Massive Subdural Haematomas in Menkes Disease Mimicking Shaken Baby Syndrome”
Nassogne et al, Childs Nerv Syst 18:729–731, 2002

•35
Pediatrics Pediatrics
“Massive Subdural Haematomas in Menkes Disease Mimicking Shaken Baby Syndrome”
Nassogne et al, Childs Nerv Syst 18:729–731, 2002
Pediatrics
•Serum ceruloplasmin .01 μmol/l‐Normal > 1.54 μmol/l
•Dynamic Copper studies were abnormal
“Massive Subdural Haematomas in Menkes Disease Mimicking Shaken Baby Syndrome”
Nassogne et al, Childs Nerv Syst 18:729–731, 2002
Pediatrics
•Retinal hemorrhages have not been described in “classic” Menkes Disease
•Gasch AT, Caruso RC, Kaler SG, et al., Menkes’ Syndrome: ophthalmologic findings. Ophthalmology 2002; 109: 1477-1483
Menkes Disease
Pediatrics Pediatrics
Scurvy

•36
Pediatrics
•Ascorbic Acid‐Needed to convert procollagen to collagen‐Capillary fragility
•Deficiency called Scurvy (Barlow’s)‐Infantile scurvy rarely seen after 1950’s‐Not seen before 3 months, rare by 7 months‐Tender limbs, fussiness, weight loss, bruising‐Xray changes
Vitamin C
Pediatrics
•Hemorrhage common‐Subperiosteal, intracranial, mucosal‐*“The central nervous system is often spared, notwithstanding extensive bleeding elsewhere”
•Conjunctival hemorrhage most common eye findings
‐Orbital hemorrhage common as well‐(Retinal hemorrhages not reported)
Scurvy
*Hess, Scurvy Past, Present and Future, 1920
Pediatrics CDC, Public Health Image Library Pediatrics CDC, Public Health Image Library

•37
Pediatrics
J New Zealand Med Ass, Vol 120 No 1262, 2007 Pediatrics
Pediatrics Pediatrics
Scurvy
Pediatrics Pediatrics
Scurvy

•38
Pediatrics
•Median age of presentation 29 months*•May result in bleeding
‐Normal coagulation studies
•No reliable testing in infants•Cited as cause of:
‐Fractures‐Retinal hemorrhages‐SDH
Infantile Scurvy
*Ratanachu-Ek S, et al. J Med AssocThai.2003;86 Suppl 3:S734-40
Pediatrics
•Barlow’s disease‐Medical Hypotheses (2002) 59(1), 52–56
•Elevated blood histamine caused byvaccinations and Vitamin C deficiency may mimic the shaken baby syndrome
‐Medical Hypotheses (2004) 62, 533–536
Clemetson
Pediatrics
•Low ascorbic acid‐Either results in or causes
•Elevated histamine (histaminemia)‐Histamine increases with vaccinations‐“causes separation of the endothelial cells from one another in scurvy”
‐“this causes the capillary fragility and the bleeding of scurvy.”
Premise
Pediatrics
•“so it seems that histaminemia is the crucial factor causing bleeding in scurvy and may be responsible for the fragility of the bridging veins and venules between the brain and the dura mater, as well as the retinal petechiae.”
Clemetson, Med Hypoth, 2004

•39
Pediatrics
“Since histamine is well recognized as a cause of capillary fragility and may well be involved in the association between retinal petechiae and subdural hemorrhage in infants, we must consider any other causes of histaminemia besides vitamin C deficiency.”
Clemetson, Med Hypoth, 2004 Pediatrics
•Literature review (medline, 1966-2003)•‘vitamin C’ combined with ‘haemorrhage’, ‘cerebral hemorrhage’, or ‘subdural hemorrhage’
‐27,838 articles
•“From the available information in the literature, there is no convincing evidence to conclude that vitamin C deficiency can be considered to be a cause of SBS.”
Could Vitamin C Deficiency have a Role in Shaken Baby Syndrome?
Fung & Nelson, Pediatrics International (2004) 46; 753-755
Pediatrics
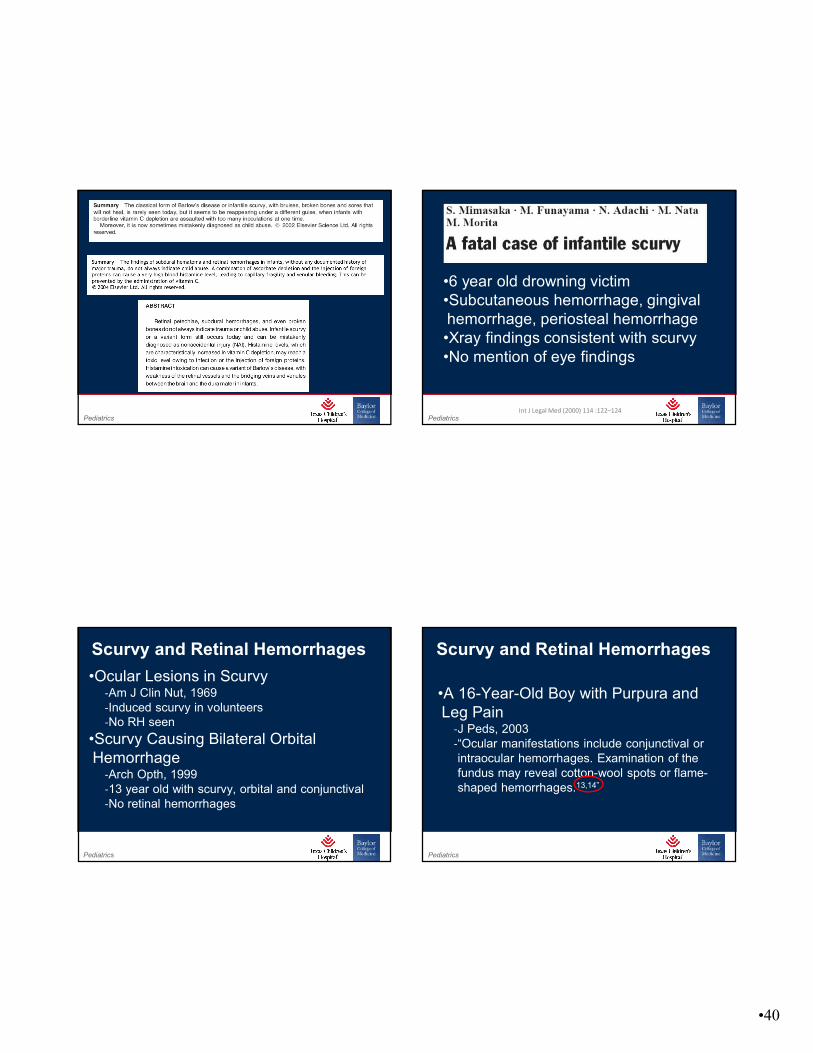
•Moreover, the clinical presentation of infantile scurvy resembles child abuse. Indeed, they share several features, such as mucosal and skin bleeding, retinal hemorrhage, subdural hematomas, and bony fractures and deformations. As a result of the serious medico-legal impact of this situation, a diagnosis of scurvy must be kept in mind when evaluating a suspected abused child.3,18,31
International Journal of Dermatology 2007 Pediatrics
•Moreover, the clinical presentation of infantile scurvy resembles child abuse. Indeed, they share several features, such as mucosal and skin bleeding, retinal hemorrhage, subdural hematomas, and bony fractures and deformations. As a result of the serious medico-legal impact of this situation, a diagnosis of scurvy must be kept in mind when evaluating a suspected abused child.3,18,31
International Journal of Dermatology 2007
•40
Pediatrics Pediatrics
•6 year old drowning victim•Subcutaneous hemorrhage, gingival hemorrhage, periosteal hemorrhage•Xray findings consistent with scurvy•No mention of eye findings
Int J Legal Med (2000) 114 :122–124
Pediatrics
•Ocular Lesions in Scurvy‐Am J Clin Nut, 1969‐Induced scurvy in volunteers‐No RH seen
•Scurvy Causing Bilateral Orbital Hemorrhage
‐Arch Opth, 1999‐13 year old with scurvy, orbital and conjunctival‐No retinal hemorrhages
Scurvy and Retinal Hemorrhages
Pediatrics
•A 16-Year-Old Boy with Purpura and Leg Pain
‐J Peds, 2003‐“Ocular manifestations include conjunctival or intraocular hemorrhages. Examination of the fundus may reveal cotton-wool spots or flame-shaped hemorrhages.13,14”
Scurvy and Retinal Hemorrhages

•41
Pediatrics
•Retinal Hemorrhages Due to Scurvy‐(Letter) Postgrad Med, 1990‐48 year old alcoholic (bread and water diet)‐Joint, skin, and retinal hemorrhages‐“We know of no other reports of retinal hemorrhages”
•Retinal Changes in Scurvy‐(Letter) Eye, 1994‐48 year old alcoholic (pastries and cigarettes)‐Teeth falling out, petechiae, muscle wasting‐“Flame hemorrhage and soft exudate”
Scurvy and Retinal Hemorrhages
Pediatrics
Verma et al, Pediatr Radiol (2007) 37:937–939
Unilateral Proptosis and Extradural Hematoma in a Child with Scurvy
•3 year old unable to walk for 2 weeks•“His diet had consisted of diluted cow’s milk and rice since late infancy and lacked fruit and vegetables.”•“extremely irritable and was undernourished”•Left eye proptotic, right eye normal•Swollen right thigh
Pediatrics
Verma et al, Pediatr Radiol (2007) 37:937–939 Pediatrics
Verma et al, Pediatr Radiol (2007) 37:937–939

•42
Pediatrics
Verma et al, Pediatr Radiol (2007) 37:937–939 Pediatrics
Verma et al, Pediatr Radiol (2007) 37:937–939
Unilateral Proptosis and Extradural Hematoma in a Child with Scurvy
•Right eye exam normal•Left eye
‐“The left eye was proptotic with ulceration and displayed seropurulent discharge and no perception of light.”
‐“(on MRI) There was a subperiosteal hematoma in the left orbit along with subretinal hemorrhage and retinal detachment.”
•This is the only report in a child
Pediatrics
•No reported cases of an infant‐With SDH, rib fractures alone‐All affected infants have periosteal hemorrhage, mucosal bleeding, cutaneous bleeding
‐Retinal hemorrhages not described in scurvy
Mimic?
Pediatrics Pediatrics
Birth
•43
Pediatrics Pediatrics
Birth
Thus, already at birth, man is shown that nature is not always his friend!
Schwartz,Birth Injuries of the Newborn, 1956,1961
Birth is a brutal process.
Birth, a process obeying the laws of hydrodynamics.
Pediatrics
•7.4 injuries per 1,000 births*•Cause of 2% of neonatal death (USA)
‐7.5 deaths per 100,000 births*
•Cephalohematomas, clavicle fx, subgaleal hemorrhage, humeral fx, femur fx
Birth Injuries
*AHRQ, 2008
Pediatrics
•Rib fractures•? Silent SDH/brain injury•? Retinal hemorrhages
Birth Injuries
Pediatrics
•111 asymptomatic normal term infants•MRI within 48hrs, no ophtho
‐Followed with serial MRI until normal
•9 had SDH (.08: .04-.15)•All resolved by 4 weeks (.01: .00-.03)
Frequency and Natural History of Subdural Haemorrhages inBabies and Relation to Obstetric Factors
Whitby et al, Lancet, 2004

•44
Pediatrics
•[retrospective; nested cohort study; maternal schizophrenia]•3T MRI on 88 (between 1-5 weeks)•17 had ICH (.20: .12-.29)
‐All asymptomatic
•No further imaging was performed
Intracranial Hemorrhage inAsymptomatic Neonates
Looney et al, Radiology, 2007
Pediatrics
•101 term; normal examination‐MRI within 72 hours‐Each study reviewed by 2 Ped Rad
•(+) SDH ‐MR imaging and US examinations at 3–7 days, 2 weeks, 1 month, and 3 months or until the MR imaging and US findings were negative.
Prevalence and Evolution of Intracranial Hemorrhage in Asymptomatic Term Infants
Rooks et al, Am J Neurorad, 2008
Pediatrics
•46 (46%: .36-.55) had (+SDH) studies‐Confirmed on follow-up imaging‐3 had positive which resolved (?false positive)
•None had SAH, EDH, Intraparenchymal
‐.01 (.00-.03)
•18 of 46 had follow-up imaging
Prevalence and Evolution of Intracranial Hemorrhage in Asymptomatic Term Infants
Rooks et al, Am J Neurorad, 2008Pediatrics
•1 of 16 had SDH at 1 month‐.11 (<.001-.303)‐Resolved by 3 months
•0 of 18 had SDH at 3 months‐.05 (.00-.16)
•0/73 (.0133: .000-.043)
•43 had normal gross motor exam at 2 years
Prevalence and Evolution of Intracranial Hemorrhage in Asymptomatic Term Infants
Rooks et al, Am J Neurorad, 2008

•45
Pediatrics Rooks et al, Am J Neurorad, 2008
Pediatrics
•Rooks & Whitby‐Birth SDH 55/212 (.26: .20-.32)‐One Month SDH 1/182(.01: <.00-.03)
•Add in Looney‐“Birth” SDH 72/300 (.24: .20-.29)
•None were noted to be symptomatic
Data Combination
Pediatrics
•149 term newborns‐Examined within 30 hours‐If (+) RH, re-examined every 2 weeks
•50/149 (34%: .26-.41); 76 eyes‐26/50 bilateral (52%); 26% of total eyes
•50 (+) “eyes” followed-up @ 2 weeks‐7 (+) RH (14%: .07-.27)
Incidence and Rate of Disappearance of Retinal Hemorrhage in Newborns
Emerson et al, Ophthalmology;108:36–39, 2001
Pediatrics
•5 of 7 eyes re-examined at 4 weeks‐1 (+) RH (.04: <.00-.12)
•This “eye” was (-) at 6 weeks‐.02: .00-.06
Incidence and Rate of Disappearance of Retinal Hemorrhage in Newborns
Emerson et al, Ophthalmology;108:36–39, 2001

•46
Pediatrics
•53 term infants‐Direct ophtholmoscopy and Retcam if (+)‐Between 1-4 days of life‐(+) RH were re-examined weekly
•18/53 (+) RH: .35 (.23-.47)‐14 bilateral‐All intraretinal
•0/53 had non-intraretinal (.02: .00-.06)
Incidence, Distribution, and Duration ofBirth-Related Retinal Hemorrhages
Hughes et al, J AAPOS;10:102-106, 2006 Pediatrics
•At ~1 week (18 scheduled for re-exam)‐5 (+) RH‐9 (-) RH‐4 lost
•5/49 (+) RH .12 (.04-.22)
Incidence, Distribution, and Duration ofBirth-Related Retinal Hemorrhages
Hughes et al, J AAPOS;10:102-106, 2006
Pediatrics
•At 4 weeks 2 (+) RH ‐.06: .00-.14
•At 8 weeks (58 days) 1 (+) RH ‐.04: <.00-.12
Incidence, Distribution, and Duration ofBirth-Related Retinal Hemorrhages
Hughes et al, J AAPOS;10:102-106, 2006 Pediatrics
•Birth (+) RH‐68/202 (.34: .28-.40)
•At 1 month (+) RH‐3/174 (.02: .00-.05)
Combined Data

•47
Pediatrics
•Retinal hemorrhages in up to 40% of newborn infants (multiple studies)
‐More common after vaginal and assisted deliveries
‐Most common at posterior pole, intraretinaldot/blot hemorrhages
‐Incidence declines rapidly within 72 hours‐Gone by 4-6 post-natal weeks
Retinal Birth Trauma
Pediatrics Pediatrics
Hypoxia
Pediatrics
•Two main themes‐Hypoxia (“Geddes I, II, III” or “Unified Theory”)‐Dysphagia (Geddes and Talbert)
Geddes et al.
Pediatrics
•Infants brains were examined for neuronal injury
‐Using special stains

•48
Pediatrics
Methodology
Geddes I
38/53 or 72%
•53 “well-documented cases of inflicted head injury”
‐Confession by perpetrator (7)‐Criminal conviction of non-accidental head injury with extracranial injuries (19)
‐Head injury with extracranial injuries but no conviction (8)
‐Criminal conviction without extracranial injuries (12)‐Discrepancy between injury and history provided (7)
Pediatrics
Microscopic Results
•Three types of axon damage studied‐vascular-ischemic axonal injury‐focal traumatic axonal injury (TAI)‐diffuse (traumatic) axonal injury (DAI)
•Most common finding is “global neuronal hypoxia-ischemia” (84% infants,63% children)
‐“a geographic pattern of white-matter immunoreactivity, which was usually widespread and related to vessels.”
Geddes I
Pediatrics
Results
•Apnea was more common in infants•Most common finding is “global neuronal hypoxia-ischemia”
Geddes IPediatrics
•37 infants from Geddes I•14 additional infants as control
‐7 SIDS, 5 RTI, 1 perinatal asphyxia, 1 AGE

•49
Pediatrics
Results•68% (25/37) cases were βAPP (+)
‐Including 11/14 who were “found dead”‐13/25 were “largely vascular in nature”‐5 had injury to only corpus callosum or central white matter
‐2 had DAI‐8 βAPP (+) localized to corticospinal bundles
•14% (2/14) controls “vascular axonal damage”
Geddes IIPediatrics Pediatrics
Discussion
Geddes II
Pediatrics
•50 fetal or infant deaths‐All no traumatic deaths
•3 infants with inflicted head injury•To study the dural haemorrhage pattern
Pediatrics
•17 intrauterine deaths•3 spontaneous abortions•16 perinatal deaths (<7 days)•5 neonatal deaths (<30 days)•9 infant deaths
50 Cases
Geddes III

•50
Pediatrics
Results
•1 child had macroscopic subdural blood‐25 week delivery, Chorioamnionitis, GNR sepsis
•“The only significant pathology was bleeding inside the strips of dura(intradural hemorrhage)” (72%, 36/50)
‐All was fresh blood
•Eyes/orbits were not examined
Geddes IIIPediatrics
Geddes III
Pediatrics Geddes III
Pediatrics Geddes III

•51
Pediatrics Geddes III
Pediatrics Geddes III
Pediatrics
•AHT does not result in the histologicfindings associated with trauma (βAPP~DAI)
‐The histologic findings in AHT are similar to those seen in hypoxia
•Hypoxia is the sole trigger of intraduralbleeding
‐This is a precursor for SDH (and RH)
Geddes et al.
Pediatrics
My Comments
•If SDH can be identified in this cohort, why was it not more frequently seen?•Unclear what an IDH means?
‐Assumption is that it is a pre-SDH

•52
Pediatrics
Dural Hemorrhage in Newborns
•Has been described for decades‐Perhaps centuries
•Schwartz, Birth Injuries in Newborns (1961)
‐“hemorrhage affects the dural reduplications (falx and tentorium) rather frequently” (p.38)
Geddes III
Pediatrics
Pediatrics Huang and Castillo, Radiographics
2008 Pediatrics Huang and Castillo, Radiographics
2008
Does not mention:Subdural HemorrhageIntradural hemorrhage

•53
Pediatrics
•Pure hypoxia•Appropriate ages•Common event•Timing is quite clear•Fatal and non-fatal
(Near-) Drowning
Pediatrics
Pediatrics Rafaat et al, Ped Crit Care Med, 2008
Pediatrics Rafaat et al, Ped Crit Care Med, 2008

•54
Pediatrics Rafaat et al, Ped Crit Care Med, 2008
0/156 patients = .0063 (95% CI: .0205 to .0000)
Pediatrics Pediatrics
Its Dysphagic Choking
Pediatrics
•Mathematical software model (CALEB)‐3 month old ‐600 physiologic (fetal) variables
Pediatrics Geddes & Talbert, 2006

•55
Pediatrics Geddes & Talbert, 2006
Pediatrics Geddes & Talbert, 2006
Pediatrics
Barnes et al. Sem Ped Neuro 2010
Pediatrics
•4.5 month old male infant•Fed on bottle, propped on chest•Father left room then returned•Baby blue and chocking•Attempted airway clearing then back blows•Blew into mouth, “saw baby’s stomach swell”•“Pumped on chest” then called EMS/911
Case Information
Barnes et al. Sem Ped Neuro 2010

•56
Pediatrics
•Ran next door to seek help•EMS arrived, baby apneic and pulseless•Resuscitation successful
‐Pulseless for 30minutes‐Hypoxic for >40 minutes
•Transported to ED
Case Information
Barnes et al. Sem Ped Neuro 2010Pediatrics
Barnes et al. Sem Ped Neuro 2010
Pediatrics
Barnes et al. Sem Ped Neuro 2010
Pediatrics
Barnes et al. Sem Ped Neuro 2010

•57
Pediatrics Pediatrics
Barnes et al. Sem Ped Neuro 2010
Case Interpretation
Pediatrics Pediatrics
Barnes et al. Sem Ped Neuro 2010
Case Interpretation
Pediatrics
•Infant suffered acute dysphagia (choking) and this alone was the cause of the death
‐Cause of RH and SDH
•Two proposed mechanisms (not exclusive)
‐Dysphagia causing increased venous pressure‐Choking causing hypoxia make it worse
Author’s Conclusion
Pediatrics
•Went to trial, father convicted‐Appealed and upheld‐The authors were the 4 defense experts for this trial
•There was a healing rib fracture as well‐Known by the authors
Not Included

•58
Pediatrics
Greeley, Seminars Ped Neuro 2010
Pediatrics
Pediatrics
•“This is a case study issue the purpose is to …present an alternative interpretation of the findings or features of the case.”•“This is not the presentation of research data and thus the requirement to present all of the data is not appropriate…”
Editorial Response
Pediatrics
•“In this instance the case is not identified in the report so the material presented is done so in the context of offering an alternative explanation for the findings in the patient. This does not require that all the ‘facts’ be presented or even that the presentation stick to the facts of the case at all as it represents, primarily, a vehicle for the presentation of the alternative theory.”
Editorial Response

•59
Pediatrics Pediatrics Geddes & Talbert, 2006
Pediatrics Radiologic Clinics of North America,
2011 Pediatrics http://www.healthsentinel.com/

•60
Pediatrics
James D. Cherry. Clinical Infectious Diseases, Vol. 28, Supplement 2. Pertussis in Adults: Epidemiology,Signs, Symptoms, and Implications for Vaccination (Jun., 1999), pp. S107‐S111
Pediatrics Geddes & Talbert, 2006
Pediatrics Marshall, Glasgow Med J, 1885, 23:24‐7
Pediatrics Marshall, Glasgow Med J, 1885, 23:24‐7

•61
Pediatrics Geddes & Talbert, 2006
Pediatrics
AAP Pertussis Reference•Pertussis (Whooping Cough) A 4-week-old neonate who was discharged from the hospital nursery to the home where a sibling had pertussis. The neonate died of pertussis pneumonia with hyperaeration complicated by Staphylococcus aureus pneumonia and subdural hemorrhages secondary to severe, paroxysmal coughing.•http://aapredbook.aappublications.org/cgi/content/full/2009/1/3.98/099_08
Pediatrics
Image 099_08 @ http://aapredbook.aappublications.org/visual/
Pediatrics
“Subdural bleeding secondary to whooping cough in the same patient as in image 099_08”

•62
Pediatrics Geddes & Talbert, 2006
Pediatrics
Pediatrics Pediatrics
•The clinical history is the single best guide as to the cause of the SDH•Context and associated findings are vital
‐Story that doesn’t make sense with your experience‐Traumatic findings without history of trauma‐Findings out of proportion to trauma history‐Seizures, apnea, retinal hemorrhages, bruising, long bone and rib fractures provide increasing specificity
Take Home Messages

•63
Pediatrics
•Keep an open mind, create a differential‐Coagulation studies should be performed on all children with a SDH
‐Look at pattern of head growth since birth‐Look for other evidence of genetic disease‐Other findings on neuroimaging
•Other conditions are usually self-evident•Further work-up should be predicated on suspicion on initial evaluation and studies
Take Home Messages
Pediatrics
•Teamwork is vital!•Child abuse evaluations benefit from multi-specialty input from experienced providers
‐Pediatric or retinal ophthalmologist‐Pediatric neurosurgeon‐Pediatric orthopedist, pediatric trauma surgeon‐Pediatric neuroradiologist‐Child Abuse Pediatrician
Take Home Messages