Embed Size (px)
Citation preview
Case report
Page 1 of 4
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
For citation purposes: Konstantinidou AE, Souka A, Sofocleous C, Paraskevakou H. Osteogenesis imperfecta type II: postmortem histological diagnosis on curettage material. OA Case Reports 2013 Aug 08;2(7):67. Co
mpe
ting
inte
rest
s: n
one
decl
ared
. Con
flict
of i
nter
ests
: non
e de
clar
ed.
All a
utho
rs c
ontr
ibut
ed to
the
conc
eptio
n, d
esig
n, a
nd p
repa
ratio
n of
the
man
uscr
ipt,
as w
ell a
s rea
d an
d ap
prov
ed th
e fin
al m
anus
crip
t.Al
l aut
hors
abi
de b
y th
e As
soci
ation
for M
edic
al E
thic
s (AM
E) e
thic
al ru
les o
f disc
losu
re.
Osteogenesis imperfecta type II: postmortem histological diagnosis on curettage material
AE Konstantinidou1*, A Souka2, C Sofocleous3, H Paraskevakou1
manifestations that are regarded nontypical for the full-blown disease.Case reportA 35-year-old G2P1 Caucasian woman had her first-trimester ultra-sound evaluation. The histological picture was typical of osteogenesis imperfecta type II/III. The combina-tion of severe distortion of the limb bones with rib and limb fractures, in association with the above histopa-thology, permitted the diagnosis of osteogenesis imperfecta type II. The parents were referred for genetic counselling and molecular confirma-tion of COL1A1 or COL1A2 mutations.ConclusionThis report underscores the utility of histological diagnosis in certain skel-etal dysplasias, even in the absence of reliable postmortem radiographic con-trol, as is the case with curettage mate-rial in early termination of pregnancy.
IntroductionOsteogenesis imperfecta (OI) is a genetic skeletal disorder character-ised by decreased bone density and susceptibility to bone fractures, due to a genetic defect of mesoderm. Severity of the disease ranges from subtle to severe congenital and peri-natally lethal types. Since the mile-stone of ‘Sillence classification’ into four types1, OI classification has now been expanded to seven types, accepted by most experts in the field2. The congenital forms com prise types II and III, while type II represents one of the more common lethal skeletal dysplasias that manifest prenatally and are therefore seen in the post-mortem examination of the foetus2–5.
In the past five years, it has become clear that OI comprises a group of heterogeneous disorders,
with an estimated 90% of cases due to a causative dominant variant in the COL1A1 or COL1A2 genes, and with the remaining 10% due to caus-ative recessive variants in various genes known so far, or in other cur-rently unknown genes6.
OI can be prenatally suspected at the second trimester of gestation, usu-ally during the routine morphology scan. Prenatal ultrasound may detect rhizomelic shortening and bowing of long bones, hypoechogenicity of the skull and fractures. However, the accurate diagnosis and classification to subtypes is based on the postmor-tem radiography. Histology of the bone and cartilage is also typical and indis-tinguishable in OI types II and III. To date, it is not possible to discriminate the dominant from the recessive types based on radiography and histology6,7.
In this report, we describe the postmortem diagnosis of OI type II at 14 weeks of gestation, based on the histological examination of curettage material. Early ultrasound signs are described and discussed.
Case reportA 35-year-old G2P1 Caucasian woman had her first-trimester ultra-sound evaluation. Her husband was 41 years old. She and her husband were nonconsanguineous, and there was no family history of congeni-tal malformations. She had a body weight of 89 kg and a body height of 162 cm. Two years before, the mother had delivered a healthy male baby with a body weight of 4400 g without any skeletal dysplasia.
Prenatal ultrasound at 13 weeks and five days of gestation revealed an increased nuchal translucency thick-ness of 4.0 mm, incipient generalised
Abstract IntroductionOsteogenesis imperfecta type II is one of the more common lethal skeletal dysplasias with prenatal onset. The prenatal ultrasound scan may suggest the presence of severe short limb skeletal dysplasias and can accurately predict lethality, but the final diagnosis, typing and subtyping of the specific genetic skeletal disorder are mainly based on the postmortem radiography. Histopathology of the bone and car-tilage can be contributory in vari-ous skeletal dysplasias, and, in the case of osteogenesis imperfecta can be diagnostic. We describe a case of osteogenesis imperfecta type II diagnosed in a 14-week gestation foetus on the basis of the typical histopathological findings on curet-tage material. This report highlights the utility of histological diagnosis in certain skeletal dysplasias, even in the absence of reliable postmor-tem radiographic control, as is the case with curettage material in early termination of pregnancy. In addi-tion, we document the presence of limb and rib fractures as early as the 14th week of gestation, and confirm that osteogenesis imperfecta type II can present in the first-trimester ultrasound scan with increased nuchal translucency, ventriculo-megaly and generalised oedema,
*Corresponding authorEmail: [email protected] 1st Department of Pathology, Medical School,
University of Athens, Greece2 3rd Department of Obstetrics and Gynecology,
Attikon Hospital, University of Athens, Greece3 Department of Medical Genetics, Medical School,
University of Athens, Greece
Path
olog
y
Case report
Page 2 of 4
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Konstantinidou AE, Souka A, Sofocleous C, Paraskevakou H. Osteogenesis imperfecta type II: postmortem histological diagnosis on curettage material. OA Case Reports 2013 Aug 08;2(7):67.
oedema, ventriculomegaly of the brain and severely hypoplastic upper and lower limbs with mesomelic bowing. The pregnancy was terminated and the abortion material was sent for pathological examination.
On external examination of the received curettage material, only parts of the upper and lower limbs could be retrieved and appeared hypoplastic, while the skull and the thorax were deformed by the curettage proce-dure. The right foot and hand length were 10 mm and 8 mm, respec-tively, corresponding to 12 weeks of gestation. Attempted X-rays of the limbs and remnants of the trunk (not shown) showed hypoplastic humeri and femora, a severely hypoplastic radius and a bent tibia. Only the outer cortex was radiographically depicted in the severely shortened bones, while the metaphyses appeared empty. The vertebral pedicles were apparent, whereas the vertebral bodies were radiolucent, as expected at 14 weeks of gestation. The ribs and pelvis could not be radiologically assessed.
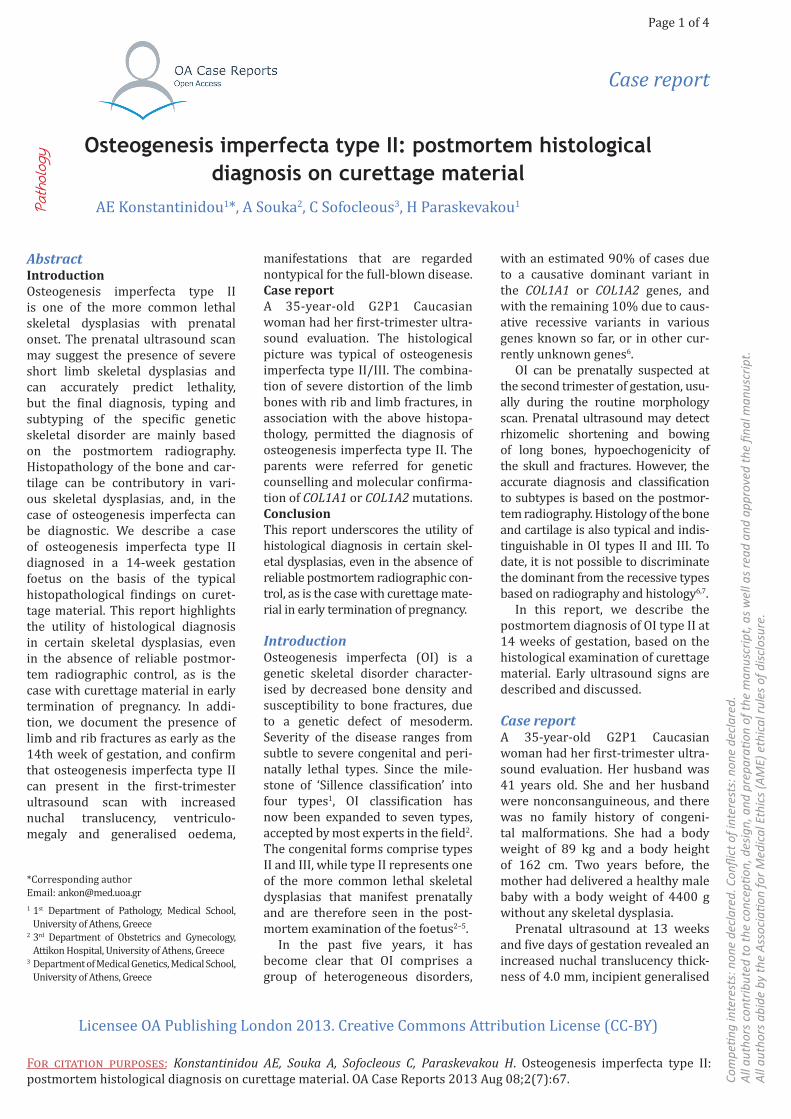
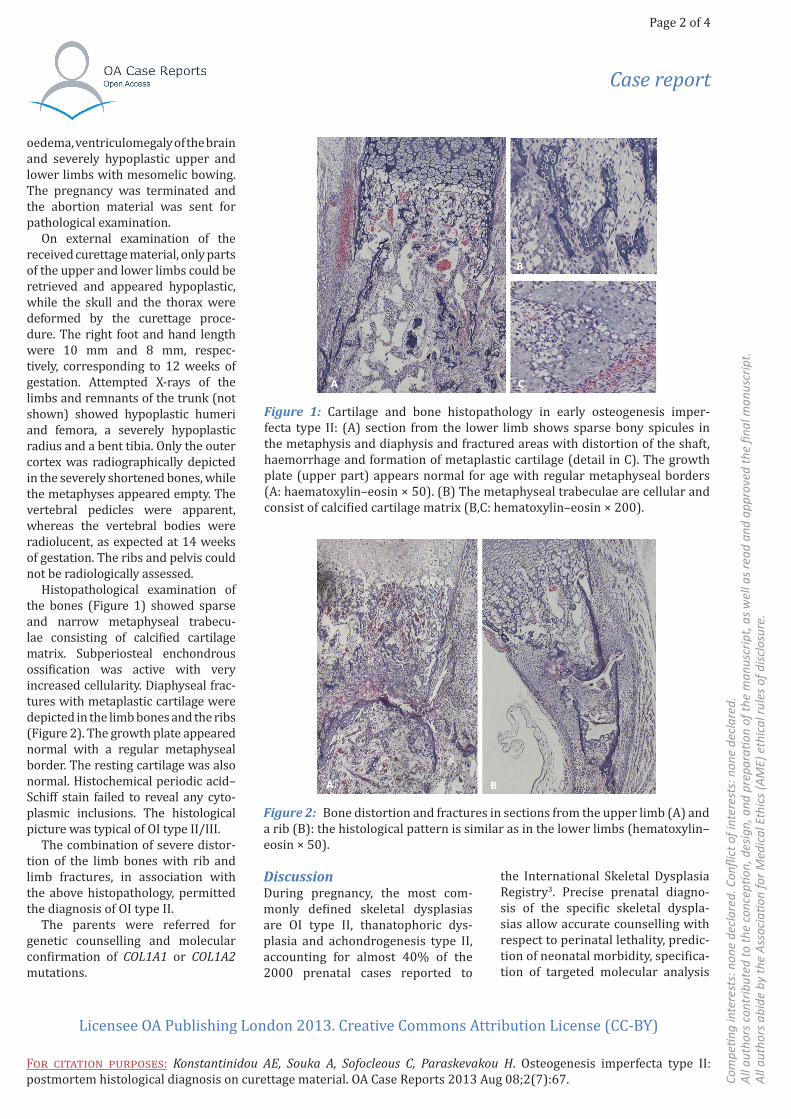
Histopathological examination of the bones (Figure 1) showed sparse and narrow metaphyseal trabecu-lae consisting of calcified cartilage matrix. Subperiosteal enchondrous ossification was active with very increased cellularity. Diaphyseal frac-tures with metaplastic cartilage were depicted in the limb bones and the ribs (Figure 2). The growth plate appeared normal with a regular metaphyseal border. The resting cartilage was also normal. Histochemical periodic acid–Schiff stain failed to reveal any cyto-plasmic inclusions. The histological picture was typical of OI type II/III.
The combination of severe distor-tion of the limb bones with rib and limb fractures, in association with the above histopathology, permitted the diagnosis of OI type II.
The parents were referred for genetic counselling and molecular confirmation of COL1A1 or COL1A2 mutations.
DiscussionDuring pregnancy, the most com-monly defined skeletal dysplasias are OI type II, thanatophoric dys-plasia and achondrogenesis type II, accounting for almost 40% of the 2000 prenatal cases reported to
the International Skeletal Dysplasia Registry3. Precise prenatal diagno-sis of the specific skeletal dyspla-sias allow accurate counselling with respect to perinatal lethality, predic-tion of neonatal morbidity, specifica-tion of targeted molecular analysis
Figure 1: Cartilage and bone histopathology in early osteogenesis imper-fecta type II: (A) section from the lower limb shows sparse bony spicules in the metaphysis and diaphysis and fractured areas with distortion of the shaft, haemorrhage and formation of metaplastic cartilage (detail in C). The growth plate (upper part) appears normal for age with regular metaphyseal borders (A: haematoxylin–eosin × 50). (B) The metaphyseal trabeculae are cellular and consist of calcified cartilage matrix (B,C: hematoxylin–eosin × 200).
Figure 2: Bone distortion and fractures in sections from the upper limb (A) and a rib (B): the histological pattern is similar as in the lower limbs (hematoxylin–eosin × 50).

Case report
Page 3 of 4
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Konstantinidou AE, Souka A, Sofocleous C, Paraskevakou H. Osteogenesis imperfecta type II: postmortem histological diagnosis on curettage material. OA Case Reports 2013 Aug 08;2(7):67.
and estimation of the recurrence risk in subsequent pregnancies.
The foetal skeleton is relatively well-visualised by ultrasound dur-ing the routine morphology scan so that skeletal dysplasias with prenatal onset, especially those severe disor-ders with pronounced shortening of long bones, are often suspected. However, given the large variety and complexity of these anomalies, antenatal diagnosis of the specific disorder is difficult. The prenatal ultrasonographic evaluation can usually predict lethality, but very often fails to identify the particular type of skeletal dysplasia, which is necessary for genetic counselling and future prenatal diagnosis3,5,8,9. Since prenatal ultrasound accuracy in the final diagnosis of genetic skel-etal disorders remains relatively low, the impact of the specific diagnosis is still dependent on the molecu-lar genetic analysis or postmortem examination3–5,7–10. The postmortem radiography is definitely the main diagnostic tool for the correct diag-nosis and typing of foetal skeletal dysplasias. In many instances, in addition to the X-rays, the possible extraskeletal pathological findings at autopsy and the histopathological picture of bones, cartilage, and occa-sionally other organs, are confirming or contributory to the diagnosis4,7. Subsequently, the phenotypic diag-nosis is ideally confirmed by molecu-lar testing, so that the final diagnosis of a skeletal dysplasia is established.
In this report, we describe the diagnostic features of lethal OI type II established on curettage material at 14 weeks of gestation. The value of our report lies on the demonstration of the typical histopathology of this genetic skeletal dysplasia at a very early developmental age, histologi-cally recognisable even on curettage material, where X-rays are not appli-cable or, as in this case, not diagnostic. The prenatal ultrasonographic find-ings of the first-trimester scan were
suggestive of a lethal skeletal dys-plasia, but nonspecific to the final diagnosis. Increased nuchal translu-cency, ventriculomegaly, generalised oedema and hypoplastic long bones, reported in various combinations, have all been previously described as early ultrasound signs in foetuses with OI11–15. These findings, however, could also apply (and even more so) for other lethal skeletal dysplasias, such as achondrogenesis type I/II, thanatophoric dysplasia, hypophos-phatasia, etc.15–18. The histological documentation of limb and rib frac-tures limited the differential diagno-sis between OI II/III, achondrogenesis I/II and hypophosphatasia2. The typi-cal histological lesions of the meta-physes, combined with a normal appearing growth plate and no evi-dence of intracytoplasmic inclusions that characterise achondrogenesis, led to the diagnosis of OI2,7. The severe distortion of the limb bones refined the diagnosis to OI type II2, one of the more commonly occurring lethal skel-etal dysplasias with prenatal onset.
OI type II is a perinatally lethal genetic disorder caused by auto-somal dominant mutations in the COL1A1 or COL1A2 genes. When the parents are phenotypically normal, the disorder is considered sporadic, attributed to de novo mutations, with occasional recurrence due to germ-line mosaicism2. The parents in our case were therefore provided with a precise diagnosis, genetic counsel-ling was feasible and targeted molec-ular confirmation was suggested, sparing the family from superfluous costly genetic testing.
ConclusionThis report underscores the utility of histological diagnosis in certain skel-etal dysplasias, even in the absence of reliable postmortem radiographic con-trol, as is the case with curettage mate-rial in early termination of pregnancy. In addition, we document the presence of limb and rib fractures as early as the
14th week of gestation in an affected foetus with OI type II, and confirm the previously reported observations that OI can present in the first-trimester ultrasound scan with increased nuchal translucency, ventriculomegaly and generalised oedema, manifestations that are regarded nontypical for the full-blown disease.
ConsentWritten informed consent was obtained from the patient for publi-cation of this case report and accom-panying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
References1. Sillence DO, Senn A, Danks DM. Genetic heterogeneity in osteogenesis imperfecta. J Med Genet. 1979 Apr;16(2):101–16.2. Gilbert-Barness E. Osteochondrodys-plasias—constitutional diseases of bone. In: Gilbert-Barness E, editor. Potter’s pathology of the fetus, infant and child 2nd ed. Philadelphia: Mosby-Elsevier; 2007.p1836-97.3. Krakow D, Alanay Y, Rimoin LP, Lin V, Wilcox WR, Lachman RS, et al. Evaluation of prenatal-onset osteochondrodyspla-sias by ultrasonography: a retrospec-tive and prospective analysis. Am J Med Genet A. 2008 Aug;146A(15):1917–24. 4. Konstantinidou AE, Agrogiannis G, Sifakis S, Karantanas A, Harakoglou V, Kaminopetros P, et al. Genetic skeletal disorders of the fetus and infant: patho-logical and molecular findings in a series of 41 cases. Birth Defects Res A Clin Mol Teratol. 2009 Oct;85(10):811–21. 5. Konstantinidou A. Skeletal dyspla-sias of the human fetus: postmortem diagnosis. In: Choy RKW, Leung TY, edi-tors. Prenatal diagnosis—morphology scan and invasive methods 1st ed. Croa-tia: InTech; 2012.p.33-58. 6. van Dijk FS, Cobben JM, Kariminejad A, Maugeri A, Nikkels PG, van Rijn RR, et al. Osteogenesis imperfecta: a review with clinical examples. Mol Syndromol. 2011 Dec;2(1):1–20. 7. Nikkels PGJ. Diagnostic approach to congenital osteochondrodysplasias at autopsy. Diagn Histopathol. 2009 Sep;15(9):413–24.

Case report
Page 4 of 4
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Konstantinidou AE, Souka A, Sofocleous C, Paraskevakou H. Osteogenesis imperfecta type II: postmortem histological diagnosis on curettage material. OA Case Reports 2013 Aug 08;2(7):67.
8. Parilla BV, Leeth EA, Kambich MP, Chilis P, MacGregor SN. Antenatal detec-tion of skeletal dysplasias. J Ultrasound Med. 2003 Mar;22(3):255–8.9. Witters I, Moerman P, Fryns JP. Skeletal dysplasias: 38 prenatal cases. Genet Couns. 2008 Feb;19(3):267–75. 10. Hatzaki A, Sifakis S, Apostolopoulou D, Bouzarelou D, Konstantinidou A, Kappou D, et al. FGFR3 related skeletal dysplasias diagnosed prenatally by ultra-sonography and molecular analysis: pres-entation of 17 cases. Am J Med Genet A. 2011 Oct;155A(10):2426–35.11. Chen CP, Su YN, Chang TY, Huang MC, Pan CH, Chern SR, et al. Osteogenesis imper-fecta type II: prenatal diagnosis and associa-tion with increased nuchal translucency and hypoechogenicity of the cranium. Taiwan J Obstet Gynecol. 2012 Jun;51(2):315–8.
12. Cho FN, Kan YY, Chen SN, Yang T, Hsu PH. Osteogenesis imperfecta associated with first-trimester ventricu-lomegaly as an early ultrasound sign. Prenat Diagn. 2005 Jun;25(6):519–20. 13. Chang LW, Chang CH, Yu CH, Chang FM. Three-dimensional ultrasonography of osteogenesis imperfecta at early preg-nancy. Prenat Diagn. 2002 Jan;22(1):77–8.14. McEwing RL, Alton K, Johnson J, Scioscia AL, Pretorius DH. First-trimester diagnosis of osteogenesis imperfecta type II by three-dimensional sonography. J Ultrasound Med. 2003 Mar;22(3):311–4.15. Makrydimas G, Souka A, Skentou H, Lolis D, Nicolaides K. Osteogenesis im perfecta and other skeletal dysplasias presenting with increased nuchal trans-lucency in the first trimester. Am J Med Genet. 2001 Jan;98(2):117–20.
16. Souka AP, Raymond FL, Mornet E, Geerts L, Nicolaides KH. Hypophosphata-sia associated with increased nuchal translucency: a report of two affected pregnancies. Ultrasound Obstet Gynecol. 2002 Sep;20(3):294–5.17. Souka AP, Snijders RJM, Novakov A, Soares W, Nicolaides KH. Defects and syndromes in chromosomally normal fetuses with increased nuchal translu-cency thickness at 10-14 weeks of ges-tation. Ultrasound Obstet Gynecol. 1998 Jun;11(6):391–400.18. Ngo C, Viot G, Aubry MC, Tsatsaris V, Grange G, Cabrol D, et al. First-trimester ultrasound diagnosis of skeletal dysplasia associated with increased nuchal translucency thick-ness. Ultrasound Obstet Gynecol. 2007 Aug;30(2):221–6.