Embed Size (px)
Citation preview

Disaster Chronicles Number 3: Earthquake in Mexico, September 19and 20, 1985


Table of ContentsDisaster Chronicles Number 3: Earthquake in Mexico, September 19 and 20, 1985..................................1
Prologue.................................................................................................................................................1List of authors who presented papers for this publication.......................................................................11. Introduction.........................................................................................................................................22. Magnitude of the disaster...................................................................................................................6
Damage to buildings........................................................................................................................8Mortality and morbidity.....................................................................................................................9Rescue of victims...........................................................................................................................12Damages to the health infrastructure.............................................................................................14Organization and immediate response..........................................................................................15Mobilization and evacuation of patients.........................................................................................18Evacuation of the national medical center of the IMSS..................................................................18Management of bodies...................................................................................................................19Damages to the hydraulic system..................................................................................................20
3. Public health and preventive medicine.............................................................................................23Shelters and campsites..................................................................................................................24Epidemiologic surveillance.............................................................................................................24Use of chlorine tablets and oral rehydration salts..........................................................................25Psychological consequences and crisis intervention.....................................................................25
4. International cooperation..................................................................................................................305. Perspectives.....................................................................................................................................32Annex : The survival of people in collapsed buildings..........................................................................32Acknowledgements...............................................................................................................................40References...........................................................................................................................................40
i

ii

Disaster Chronicles Number 3: Earthquake in Mexico, September 19and 20, 1985
Earthquake in MexicoSeptember 19 and 20, 1985
Pan American Health Organization
Program of Emergency Preparedness and Disaster Relief Coordination
NOTE: This is a preliminary version of the Disaster Chronicle, which does not contain photographs. The finalversion will be published at a later date.
This publication has been made possible thanks to the financial support of the Canadian InternationalDevelopment Agency (CIDA) and the Office of U.S. Foreign Disaster Assistance of the U.S. Agency forInternational Development (OFDA/AID).
Disaster Chronicles #3, Earthquake in Mexico, is a publication of the Emergency Preparedness and DisasterRelief Coordination Program of the Pan American Health Organization, Regional Office of the World HealthOrganization. The reporting of facts, activities and programs does not imply approbation by PAHO/WHO nordoes it necessarily represent the politics of the Organization.
Prologue
This publication is a synthesis of various studies presented to the Emergency Preparedness and DisasterRelief Coordination Program of the Pan American Health Organization, Regional Office of the World HealthOrganization (PAHO/WHO). Most of the authors participated in the sanitary activities that took place in MexicoCity after it was devastated by the September 19, 1985 earthquake. It represents an attempt to organize theabundant technical and scientific material that was produced as a response from the health sector. It is thehope of PAHO/WHO that this publication is of use not only to those persons who worked in the health sector,but also to other institutions that participate in disaster relief activities. The technical information for thispublication was compiled by Dr. Ney Guzmán. Dr. José Luis Zeballos and Dr. Jean−Luc Poncelet alsocontributed to the initial preparation of this report
Photographs:
Julio Vizcarra/PAHOJosé Luis Zeballos/PAHO (Page 41)
List of authors who presented papers for this publication
Carrillo Silva, Raúl; Cruz Vega, Felipe y del Toro Gallardo, J. Lecciones que deben aprenderse del terremotode México. Secretaría de Salud, Subsecretaría de Servicios de Salud, Direcci6n general de medicinepreventiva, Direcci6n de prevención contra accidentes y atención de la salud en caves de desastre, México,D.F., 1987.
Castañón Romo, Roberto. Organización de la atención médica a cargo del Departamento del Distrito Federal.Dirección general de servicios médicos. México, D.F., mayo de 1987.
Castañón Romo, Roberto. Procedimientos médicos regales para la identificación de cadáveres.Departamento del Distrito Federal. Dirección general de servicios médicos. México, D.F., mayo de 1987.
López Cervantes, Malaquías; López Carrillo, Lizbeth y Escamilla Cejudo, José Antonio. "Algunasconsecuencias de los sismos de septiembre de 1985 en la Ciudad de México." Salud Publica Mexicana28:527−536, 1986.
1
Chávez Villaseñor, Luis Arturo. Los recién nacidos sobrevivientes del terremoto. Informe de la búsqueda ysalvamento de los cuatro últimos sobrevivientes de la unidad de ginecobstetricia del Hospital General deMéxico en septiembre de 1985. Hospital General de México, D.F., 1987.
Cruz Vega, Felipe. Evacuación del Centro Médico Nacional del IMSS. IMSS. Subdirección general medica,México, D.F., mayo de 1987.
Díaz de la Garza, Juan Antonio; Rubio Loyola, Juan Eduardo; Jerezano de la Rosa, Olga E.; EscobarRodríguez, Martha Rebeca y Hernández Juárez, Rebeca. El terremoto y la infraestructura hospitalaria.Secretaria de Salud. Subsecretaría de Servicios de Salud. Direcci6n general de medicine preventivaDirecci6n de prevención contra accidentes y atención de la salud en caves de desastre. México, D.F., 1987.
Estrada Vásquez, Mario y Bribiesca Yáñez, Rodolfo. Experiencias del Dispositivo operativo implementado porel Instituto de Salud, Estado de México en el terremoto de 1985. Instituto de Salud del Estado de MéxicoToluca, Estado de México.
Frausto Pérez, Guadalupe et al. Conducta de la familia en relación a la utilización de sobres de rehidrataciónoral y pastillas de cloro de UNICEF en una zona de desastre en el D.F. Escuela de Salud Publica de México.Programa de Especialización de Enfermería en Salud Publica. México, D.F., 1985.
Jerezano de la Rosa, Olga E.; Díaz de la Garza, Juan Antonio; Ortiz Salgado, Carmen; Morales Valentino,Elena Patricia. Repercusiones del sismo en el campo de la salud. Secretaría de Salud. Subsecretaría deServicios de Salud. Direcci6n general de medicine preventiva Dirección de prevención contra accidentes yatención de la salud en caves de desastre. México, D.F., 1987.
Medina González, Alfredo; Ortiz Salgado, María del Carmen y Luna Sánchez, Lucía G. Consideracionesgeológicas de la República Mexicana y el terremoto del 19 de septiembre de 1985. Secretaría de Salud,Subsecretaría de Servicios de Salud. Dirección de prevención contra accidentes y atención de la salud encaves de desastre. México, D.F. 1987.
Pacheco Regis, Carlos; Padilla Galindo, Paula; López Gibson, Eduardo; Sánchez Baez, José Juan y GómezEspinosa, María. Desastre sísmico y crisis psicológica, modelo de intervención preventiva, desarrollado por elIMSS. IMSS Subdirección general médica. Coordinación de Psiquiatría y Salud Mental México, D.F., mayo de1987.
Rojas Enríquez, Carlos A. El terremoto de 1985 en el Hospital Juárez de la Ciudad de México. Secretaría deSalud. Subsecretaría de servicios de Salud. Hospital Juárez II. México, D.F., mayo de 1987.
Sabido, Raúl Cicero; Padua Gabriell, Antonio; Rodríguez Martínez, Héctor; Toledo, Bibiana y Yáñez Villar,Alvaro. "Efectos del terremoto del 19 de septiembre de 1985 en el Hospital General de la Ciudad de México,algunas consideraciones." Salud Pública Mexicana 28: 521−526, 1986.
Vina Sánchez, Ramón. Daños producidos por los sismos del mes de septiembre de 1985, en el sistemahidráulico del Distrito Federal. Departamento del Distrito Federal. Dirección general de construcción yoperación hidráulica. Secretaría general de obras. Dirección de operación. México, D.F., mayo de 1987.
Zeballos, José Luis. Aspectos de salud en el terremoto de México (19 de septiembre de 1985).Informe−crónica. Programa de la OPS de preparativos pare situaciones de emergencia y coordinación delsocorro en caves de desastre, OPS/OMS, Washington, D.C., octubre 1985.
Zeballos, José Luis. Emergency medical response during the Mexico earthquake. 2nd InternationalEarthquake Conference, Los Angeles, California, 1987. Programa de la OPS de preparativos pare situacionesde emergencia y coordinación del socorro en caves de desastre, OPS/OMS, Washington, D.C.
1. Introduction
Historical Review
According to historical documents dated 1325 AD., the ancient Aztec city of Tenochtitlan was founded on anislet of Lake Texcoco (1). This lake had an extension of about 1,575 square kilometers (of which 13 square
2

kilometers are still in the Federal District) and was filled with numerous floating islands made up of roots andstems called chinanpas (2). The Mexica used the chinanpas to expand; by filling up channels, making bridgesbetween them, and using drainage and evaporation techniques, they managed to increase their living spaceand construct the city.
The Aztec empire was destroyed by the conquistadores and among its ruins Hernán Cortés founded the cityof Mexico in 1522. Work on the water and drainage system in the valley of Mexico was reinitiated during thecolonial period, due to the great floods that occurred in 1606. In January of 1637 an earthquake of greatmagnitude destroyed the drainage waterworks of the lake. That is the first historical reference to the pastseismic activity of the city (3).
Earthquake Origins
Mexico is a country with major seismic activity. More than 90 earthquakes per year are registered with amagnitude superior to grade 4 on the Richter scale (4). The regions with major seismic risk are the states ofJalisco, Colima, Michoacán, Guerrero, Puebla, Oaxaca and the Federal District. The seismic energy liberatedis principally tectonic, produced by the subduction of the Cocos plate on the continental platform of NorthAmerica (5).
The majority of earthquakes that have occurred in this century, with a magnitude equal to or greater than a 7on the Richter scale have had their origin on a thin meridional zone between the Sierra Madre on the southand the Pacific coast of the states of Jalisco, Michoacán, Guerrero and Oaxaca (Figure 1).
On September 19, 1985, at 7:19 local time, an intense earthquake with a magnitude of 8.1 on the Richterscale struck the country. The epicenter was located near the coast of the state of Guerrero, about 400kilometers southeast of Mexico City, at 17.8 degrees north latitude and 102.3 degrees west longitude. Theglobal area affected by the seismic shock waves was estimated at 800,000 square kilometers making thisearthquake one of the most powerful of the present century (6). The states most affected were Colima,Guerrero, Oaxaca, Jalisco, Michoacán, Morelos, Veracruz, and the Federal District (Figure 2).
3

Figure 1: Regional Tectonic Map of Mexico
Source: Adapted from Ismael Herrera R., Instituto de Geofísica de la Univesidad Nacional Autónoma deMéxico
The following day, at 19:40 p.m. local time, a second seismic movement measuring 7.5 on the Richter scale,with an epicenter at the same place, caused panic in the population despite the fact that the damages wereminor when compared to the devastating magnitude of the first 0. During the following 45 days after theearthquakes of September 19 and 20, more than 150 secondary earthquakes were registered, with varyingmagnitudes between 3.5 and 5 on the Richter scale (8).
The abrupt liberation of seismic energy produced tsunamis of up to 3 meters in height and an advance of 200meters inland of the ocean coast; numerous cave−ins of roads and rivers; cracks with horizontal and verticaldisplacements of up to 50 cms; total or partial collapse of many buildings and important damages to thenetwork of public services. The populations most affected were in Ciudad Guzm n, Colima, Tecom n, PlayaAzul−Zihuatanejo, Playa Arteaga, Uruspán, Lázaro Cárdenas, Ixtapa Zihuatanejo and Gómez Farias. Withouta doubt, the most serious devastation, based on the magnitude and characteristics of damages, took place inthe Federal District, particularly in the delegations of Cuauhtemoc and Venustiano Carranza, two of the mostdensely populated areas of Mexico City (9,10).
4

Figure 2. Epicenter and Area Affected by the Seismic Waves
In the central areas of the city the seismic shock waves presented an acceleration four times superior to thoseregistered in peripheral areas (8). The structure of the subsoil in this part of the city, located in an ancientswampland area and made up of deposits of white clay with high compressibility, and the topographic andgeological perimeter composition determined a compaction differential of the sediments and liquefactionproducing countless waves that were activated by the resonance of the seismic waves trapped in the valley ofMexico. The greatest damage occurred in the northern part of the Federal District, which is located preciselyover the ancient swampland zone where the old Aztec city of Tenochitlán was located (11 and 12 and Figure3).
5

Figure 3.
Map of the Federal District Indicates Zone 1, Which is Primarily Mountainous; Zone II, Which Corresponds tothe Ancient Swampland and Zone m, Which Corresponds to the Ancient Lake Where the Effects of theEarthquake Were Most Damaging.
Efforts to rescue trapped victims are hampered when buildings are severely damaged. Part of disasterpreparedness includes evaluating the vulnerability of construction areas.
2. Magnitude of the disaster
In 1985 the estimated population projection for the metropolitan area of Mexico City was approximately18,400,000 inhabitants in an area of 1,246 square kilometers (23). This constitutes the city with the most rapiddemographic growth in the western hemisphere. Between 1960 and 1980 the number of inhabitants tripledfrom 5,186,000 to 15,100,000 (Figures 4 and 5).
6

Figures 4 and 5. Demographic Growth in the Federal District, 1960 and 1980
Source: Impacto No. 1857, September, 1985.
The Federal District is divided into 16 political−administrative delegations (Figure 6). The most affecteddelegations from the September 19 and 20 earthquakes were Cuauhtemoc, Benito Juárez, VenustianoCarranza, Coyoacán, and parts of Gustavo Madero and Miguel Hidalgo. The greatest devastation wasconcentrated in an approximate area of 40 square kilometers which corresponds to about 3.2% of the totalarea of the Federal District.
7

Figure 6. Political Delegations of the Federal District
The most affected zone was the Cuauhtemoc delegation. The largest proportion of destroyed buildings werelocated in an area of about 32 square kilometers belonging to this delegation, where there is majorcommercial activity, hotels, tourism zones and other public services of the city (19).
Damage to buildings
As indicated previously the major damage in the architectural structure of the city occurred in the ancientswampland zone and was due principally to the intensity and complexity of the seismic shock waves that werepropagated throughout the valley of Mexico. Apparently there were no buildings in the region of the lake thatremained exactly in the same position. Some were deviated up to 15 degrees from their vertical axis.According to some observers, the obstetrics−gynecology tower and the medical residence of General Hospital
8

rotated 20 to 25 degrees in a southeastern direction. The oscillatory movements of displacement andtrepidation provoked the collapse of buildings, especially those that had between 5 and 21 stories. Many ofthe buildings had resisted the earthquake of 1957 and others were new structures, built to antiseismicconstruction standards.
In a provisional report dated October 2, that is two weeks after the earthquake, the Metropolitan EmergencyCommission of the Federal District, pointed out that 2,831 buildings had suffered structural damage of somekind; 880 (31%) had collapsed in ruins; 370 (13%) were potentially habitable, with major repairs; and 1,581(56 %) were habitable with minor repairs (13).
The proportion of buildings totally or partially collapsed in the Federal District was about 2 per 1,000 buildings(total number of constructions 1,404,000). The proportion of totally collapsed constructions was 8.46 per1,000 and the Cuauhtemoc delegation was the most affected because about 80% of all destroyed buildingswere located in this sector. Table 1 shows the percentage distribution and class of buildings affected by theearthquakes. From a total of 2,831 damaged buildings, the most compromised physical structures wereschools (46% of the total of damaged buildings); privately owned buildings (40%); public offices (4.3%);markets (4%), and movie houses and theaters (3.7%). The damages to educational establishments andoffices (public and private) left about 33% of the school population and 7.3% of the work force idle (14).
Table 1. Number and Type of Buildings Damaged, Mexico, D.F., 1985
Type of Building Number PercentPublic buildings 123 4.3Schools 1,294 46.0Hospitals and health centers 49 1.7Cinemas and theaters 105 3.7Private buildings 1,133 40.0Sports centers 11 .3Pedestrian walkways 1 −Markets 112 3.9Road construction sites 3 .1TOTAL 2,831 100.0Source: Informe de la Comisión Metropolitana de Emergencia al 4 de octubre de 1985.
Three of the largest health centers: the National Medical Center of the IMSS, General Hospital and JuárezHospital of the Ministry of Health (SSA), were seriously affected. In these three institutions the health sectorlost 5,829 hospital beds between those destroyed and evacuated. The National Medical Center lost about40% of its installations; at General Hospital, the six−story obstetrics−gynecology complex collapsed as well asthe eight−story physicians' residence, and at Juárez Hospital the 12−story central tower, which providedvarious medical specializations, collapsed.
Mortality and morbidity
Conflicting information from several sources was published regarding lost human lives (14). The MetropolitanEmergency Commission reported on October 19, 1985 a total of 4,287 deaths based on the number of bodiesmade available to the coroner's office. Combining the data from various sources, an estimate of 7,000 deathswas made (15) and the General Division of Epidemiology of the Ministry of Health estimated the number ofdeaths at approximately 5,000 (16,17). Table 2 shows the number of bodies recovered from collapsedbuildings and those that died later in health institutions.
The mortality rate by age and sex are analyzed taking into consideration the preliminary data presented by theGeneral Division of Epidemiology on October 29, l985 (18). Deaths were more frequent in the intermediateage groups. Half of all registered deaths occurred between the ages of 25 and 64 years of age. In general78% of total deaths were in persons older than 15 years of age (Table 3). The distribution by sex showed aslight predominance in men (52% as opposed to 48% in women). Table 4 shows the fate of people who foundthemselves in General Hospital and Benito Juárez Hospital.
9

It is estimated that in the obstetrics−gynecology unit of General Hospital there were approximately 385 adults(including 10 physicians) and 157 newborns at the time of collapse. Of the adults, 155 died (including the 10physicians), 129 were rescued and 47 were missing. Of the newborns, 94 died and 63 were rescued. In theblock of physicians' residences of the same hospital there were 86 medical residents; 46 perished and 40were rescued alive.
Table 2. Number of Bodies Recovered by Location and Type of Collapsed Building, Mexico, D.F., 1985
DeathsLocation and Type Number PercentEdificio Nuevo León 321 7.7General Hospital 295 7.1Juárez Hospital 561 13.5Multifamiliar Juárez 205 4.9Conalep en Humboldt and Juárez 119 2.9Hotel Principiado 118 2.8Hotel Regis Centro 74 1.9Paraguay 36 50 1.2Av. Universidad 13 47 1.2Ahorro Postal 14 44 1.1Lázaro Cárdenas 44 1.1Calle de Querétaro 179 37 0.9Orizaba 174 35 0.8Liverpool 24 34 0.8Chilpancingo 116 35 0.8Eligio Ancona No. 19 and No. 85 33 0.7Hotel Romana 30 0.7Heroes 214 29 0.7Insurgentes Sur 189 29 0.7Mitla 27 0.6Centro Médico Nacional 10 0.2Persons who perished in various health institutes 241 5.8Persons who perished in other places 1,742 41.9TOTAL 4,160 100.0Source: Adapted from Informes de la Procuraduría General de Justicia y Dirección General EpidemiologíaS.S.A. The preliminary reports were updated with the references (23 and 24).
Table 3. Mortality Distribution by Real and Apparent Age, Mexico, D.F., 1985, (Corpses Recoveredfrom Collapsed Buildings).a
a Preliminary data (until the 29 of October, 1985).
Age Groups Deceased Percent1 173 4.81−4 143 4.05−14 287 8.05−24 770 21.525−44 1,293 36.145−64 519 14.565+ 226 6.3Ignored 168 4.7TOTAL 3,579 100.000Source: Dirección General de Averiguaciones Previas/Procuraduría General de Justicia del Distrito Federal.
10

The proportion of global mortality for this institution was 63%. It was not possible to obtain the exact numberof persons who were in the hospitalization tower of Benito Juárez Hospital when the collapse occurred.
One hundred and seventy−nine (179) persons were rescued alive. Among the 561 fatalities, 266 belonged tothe hospital ranks, including 44 physicians.
Taking into consideration the 536 available beds, with an estimated occupation of 80%, the number ofoperating rooms, the usual personnel for surgeries and the students that frequented the tower, it is reasonableto assume that the total number of trapped persons would surpass those rescued alive and dead
It was difficult to process information on the morbidity caused by the earthquake, especially as it related tomoderate and life−threatening wounds, due to the dispersion of and the quality of information regardingdiagnosis. It is estimated that 10,000 persons suffered life−threatening injuries and 30,000 moderate wounds.The health sector institutions informed the Interinstitutional Commission of the Ministry of Health that of the3,285 patients admitted to hospitals immediately after the earthquake, 83% were released in the first fewdays, and that by October 1, only 141 patients remained hospitalized (19). The distribution of hospitalizedpatients in different institutions is shown in Table 5.
Table 4. Persons Who Perished and Those Who Were Rescued Alive After the Collapse of GeneralHospital and Juárez Hospital, Mexico City, D.F., 1985
Collapsed HospitalsCharacteristics of the Victims General Juárez
Number Percent Number PercentDeceased 295 62.6 561 76.0Patients 85 18.0Newborns 94 20.0 295 40.0Doctors 56 11.9 44 6.0Nurses 37 7.9Administrative personnel 4 0.8 222 30.0Intendant personnel 16 3.4Visitors 3 0.6Rescued alive 129 27.4 179 24.0Adults 26 5.5 171 23.5Newborns 63 13.4 4 0.5Doctors 40 8.5 4 0.5Missing 47 10.0TOTAL 471 100.0 740 100.0Source: References (23 and 24).
Table 5. Hospital Care, Admissions and Releases
Institution Admissions Releases Patients Hospitalized DeceasedDDF 316 289 27 57IMSS 1,935 1,566 50a 106ISSSTE 913 773 56a 23Red Cross 121 113 8 25TOTAL 3,285 2,741 141 221
a Approximate numbers
Source: Ministerio de Salud. Informe de una Comisión Intersectorial, October 1, 1985.
Table 6. Lesions by Type and Topography of the Population Treated in the Medical Services of theFederal District Throughout the First Five Days Following the September 19 Earthquake
Trunk Other Unspecified Total(%)
11

LesionTopography
Headand
Neck
SpinalColumn
SuperiorMember
InferiorMember
TotalPersons
Registered(%)
Contusion 21 4 24 37 20 − 106 (25) 50 156 (18)Injury 39 2 28 16 5 − 90 (21) 5 95 (11)Fracture 13 1 34 41 15 − 104 (24) 116 220 (25)Burn − 1 − 1 1 − 3 (1) 1 4 ( )Intoxication − − − − − 15 15 (4) − 15 (2)PsychologicTrauma
− − − − − 109 109 (25) − 109 (13)
TotalRegistered (%)
73 (17) 8 (2) 86 (20) 95 (22) 41(10)
124(29)
427 (100) − −
Unspecified 16 − 1 4 13 − 237 271 (13)TOTAL 89 (10) 8 (1) 87 (10) 99 (12) 54 (6) 124
(14)− 409
(47)870 (100)
X2 = 38.62 significant p .0005(applicable for information regarding physical lesions)
Source: Dirección General de Servicios Médicos del Departamento del Distrito Federal, Informe de lapoblación atendida en los servicios médicos del Departamento del D.F. dentro de 105 5 primeros díasposteriores d sismo del 19 de septiembre de 1985. November, 1985.
Table 7. Trauma Related to Morbidity by Anatomical Segment, Red Cross Hospital, Mexico, D.F.,September 19, 1985
Head andface
Neck andtrunk
SuperiorExtremities
InferiorExtremities
Other Total
Trauma withfracture
2 5 7 15 − 29 (20.1)
Injury 4 2 5 4 − 15 (10.4)Contusions 1 12 7 12 −Policontusions − − − − 38Simple − − − − 4 74 (51.4)IntracranealTrauma
14 − − − − 14 ( 9.7)
Complications by traumaPolitrauma − − − − 4Others − − − − 1 7 (4.9)Sprain − 1 − 3 − 4 (2.8)Crush syndrome − − − − 1 1 (0.7)TOTAL 21 21 20 34 48 114
(100.0)In this earthquake, as in others registered in the region, it was demonstrated that emergency medical attentiondeclined rapidly after the first 48 hours, and that the majority of the wounded received ambulatory medicalattention. An appreciation of lesions, by anatomical segment, can be observed in Tables 6 and 7. Thesetables are based on partial information registered in the medical Division of the Department of the FederalDistrict and in the Mexican Red Cross Hospital during the first days after the earthquake (20, 21).
Rescue of victims
Although the disaster area was located principally in the Federal District, the collapsed buildings weredispersed in a geographical area of approximately 40 square kilometers. The dispersion of disaster pointsobligated the mobilization of hundreds of search−and−rescue brigades to different sites.
12

When preparing for a disaster, every effort should be made to train local teams to direct and participate insearch−and−rescue operations. Prompt action by the Mexican Red Cross was fundamental in carrying out thefirst rescue activities in the places than had been affected by the earthquake.
It is estimated that approximately 50,000 persons (mainly teenagers, men and women, between the ages of14 and 20 years old) participated in removing debris, rescuing victims, administering first aid, transporting andmanaging the critically wounded and identifying and disposing of bodies. Removing debris and rescuingtrapped victims was a tiring and difficult task. The lack of specialized equipment and heavy machinery toremove fallen structures, combined with inexperienced rescue personnel, especially volunteers with the will tohelp but without unity of command, prolonged these activities a great deal. The arrival from other countries ofspecialized rescue groups, with equipment and trained dogs, contributed significantly to this task.
Fortunately, within hours of the impact both official and informal rescue networks were established and reliefgroups dispatched to diverse disaster sites. At the hospital, triage teams and emergency medical personnelmanaged the situation. The majority of survivors at the obstetrics−gynecology unit and at the physicians'residences of General Hospital, were rescued within the first 48 hours. Among the adults, two physicians wererescued on the fifth and seventh days after the disaster, among the newborns, one was rescued on theseventh day, and although the infant later died from a pulmonary hemorrhage, another infant, rescued on theninth day, survived (22).
After the collapse of the patient hospitalization tower at Juárez Hospital, nine emergency teams wereorganized, each with two nurses, two medical students and one medical specialist. Two physicians tookgeneral control of operations. After the first 72 hours, the most useful and safe procedures were the use oftow trucks and cranes to remove heavy structures, and the construction of mine tunnels, shored up to preventcave−ins. Victims rescued during the first three days were the ones on the surface. The last survivors wererescued eight days later. On the seventh day four newborns were rescued alive (23).
The recovery of bodies trapped in the ruins of the obstetrics−gynecology unit and physicians' residenceslasted until the twentieth day (Figure 7), due to the great difficulties in removing debris. The maintraumatologies identified in 236 bodies can be seen in Table 8. Although no autopsies were performed onthese bodies, it is presumed that all had inhaled dirt and dust (24).
The removal of trapped bodies in the collapsed tower of Juárez Hospital continued until 38 days after thedisaster. The majority of bodies were recovered on the twenty−fourth day after the disaster whendebris−removal equipment arrived at the elevators and stairways (Figure 8).
Figure 7. Number of Bodies Recovered from Juárez Hospital from September 19 (Date of the Earthquake)Through October 8
Source: Reference (23).
Table 8. Traumatology in 236 Individuals Who Perished in General Hospital on September 19, 1985
13

Trauma Area of LesionDeceased No. No Yes Head Thorax Abdomen Members
Patients 85 5 80 51 60 40 80Newborns 94 32 62 42 40 25 53Doctors 56 − 56 23 18 32 56Nurses 37 11 26 12 15 18 24Administrative 4 − 4 1 1 3 4Intendant 16 8 6 2 4 3 7Visitors 3 3 − (?) (?) (?) (?)Total 295 59 236 Dirt and dust inhalation: 236
Note: (?) The 59 unstudied cases were fumed over to the Ministerio Público. The 236 studiedcases were registered m the Pathology Unit of General Hospital of Mexico. Of these, 22perished as a result of crushing or physical dismemberment.
Source: Departamento de Trabajo Social, Unidad de Anatomía Patológica, UNAM Hospital General.Secretaría de Salud, Mexico.
Figure 8. Recovery of Bodies, General Hospital
Source: Reference (24).
Damages to the health infrastructure
In all likelihood, the public health sector was the most affected by the September 19 earthquake. The cost ofdirect material damages was estimated at more than 300 million dollars.
The majority of losses affected secondary and tertiary hospital infrastructures. Three of the most complextechnical−scientific institutions of the Federal District suffered severe structural damages. General Hospitallost the entire obstetrics−gynecology hospital unit, with 244 beds and the residential tower of physicians intraining; Benito Juárez Hospital lost the hospitalization unit with 501 beds; and the National Medical Centersuffered partial damages in seven of its nine hospital units, including pediatrics, obstetrics−gynecology,thaumatology and cardiology services.
A total of 13 hospital installations were either partially or totally destroyed. It should be noted that the buildingswere 6 or more stories high. The majority belonged to the IMSS and ISSSTE. The public sector lost a total of4,397 beds, about one in four of those available in the metropolitan area (25).
14
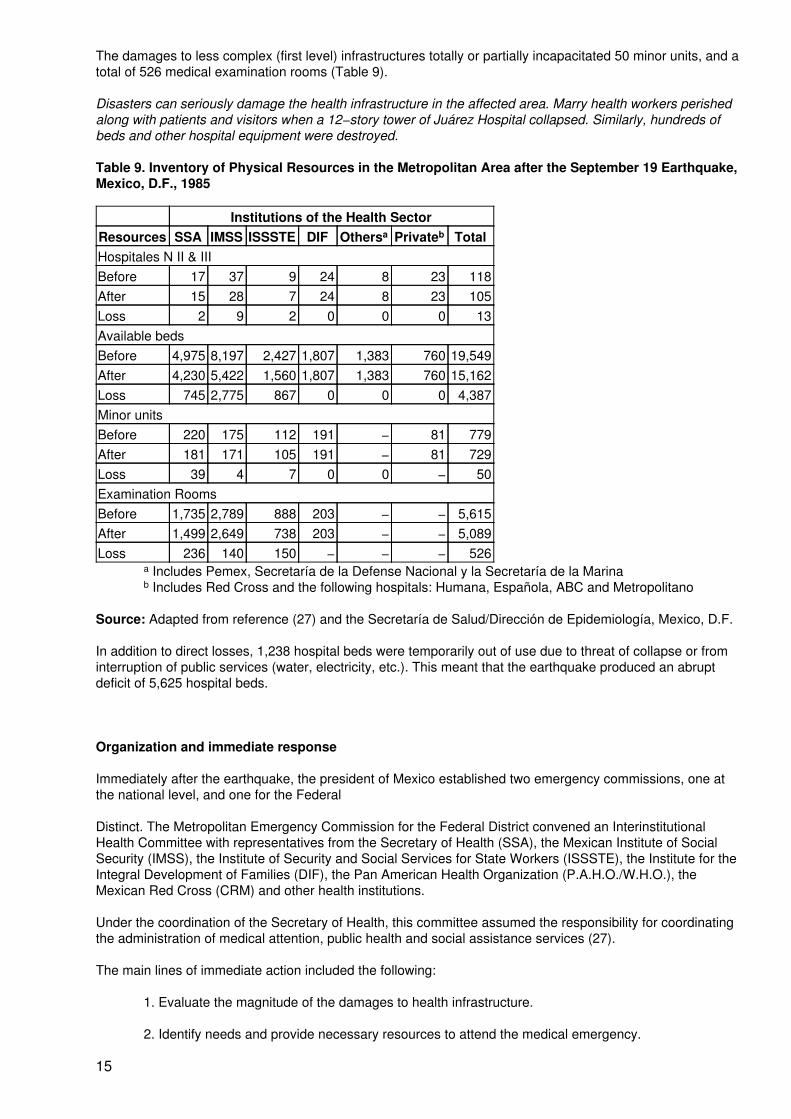
The damages to less complex (first level) infrastructures totally or partially incapacitated 50 minor units, and atotal of 526 medical examination rooms (Table 9).
Disasters can seriously damage the health infrastructure in the affected area. Marry health workers perishedalong with patients and visitors when a 12−story tower of Juárez Hospital collapsed. Similarly, hundreds ofbeds and other hospital equipment were destroyed.
Table 9. Inventory of Physical Resources in the Metropolitan Area after the September 19 Earthquake,Mexico, D.F., 1985
Institutions of the Health SectorResources SSA IMSS ISSSTE DIF Othersa Privateb TotalHospitales N II & IIIBefore 17 37 9 24 8 23 118After 15 28 7 24 8 23 105Loss 2 9 2 0 0 0 13Available bedsBefore 4,975 8,197 2,427 1,807 1,383 760 19,549After 4,230 5,422 1,560 1,807 1,383 760 15,162Loss 745 2,775 867 0 0 0 4,387Minor unitsBefore 220 175 112 191 − 81 779After 181 171 105 191 − 81 729Loss 39 4 7 0 0 − 50Examination RoomsBefore 1,735 2,789 888 203 − − 5,615After 1,499 2,649 738 203 − − 5,089Loss 236 140 150 − − − 526
a Includes Pemex, Secretaría de la Defense Nacional y la Secretaría de la Marinab Includes Red Cross and the following hospitals: Humana, Española, ABC and Metropolitano
Source: Adapted from reference (27) and the Secretaría de Salud/Dirección de Epidemiología, Mexico, D.F.
In addition to direct losses, 1,238 hospital beds were temporarily out of use due to threat of collapse or frominterruption of public services (water, electricity, etc.). This meant that the earthquake produced an abruptdeficit of 5,625 hospital beds.
Organization and immediate response
Immediately after the earthquake, the president of Mexico established two emergency commissions, one atthe national level, and one for the Federal
Distinct. The Metropolitan Emergency Commission for the Federal District convened an InterinstitutionalHealth Committee with representatives from the Secretary of Health (SSA), the Mexican Institute of SocialSecurity (IMSS), the Institute of Security and Social Services for State Workers (ISSSTE), the Institute for theIntegral Development of Families (DIF), the Pan American Health Organization (P.A.H.O./W.H.O.), theMexican Red Cross (CRM) and other health institutions.
Under the coordination of the Secretary of Health, this committee assumed the responsibility for coordinatingthe administration of medical attention, public health and social assistance services (27).
The main lines of immediate action included the following:
1. Evaluate the magnitude of the damages to health infrastructure.
2. Identify needs and provide necessary resources to attend the medical emergency.
15

3. Assure the maximum utilization of the hospital network, public or private, in themetropolitan area.
4. Achieve a permanent information system that would permit followup of the situation.
5. Establish a system of water quality surveillance and control of communicable diseases.
6. Coordinate and integrate forces with the Department of the Federal
District and other governmental organisms to better handle the situation.
The situation was quickly evaluated in the Federal Distinct with the intention of putting these actions intopractice. The physical damages to the health infrastructure were identified, the number of beds lost wasdetermined and the decision was made to evacuate some hospitals and/or temporarily suspend healthservices in other installations due to damage. That evaluation was applied to General Hospital, the NationalMedical Center, some lesser institutions and examination rooms of the primary health network, that weretemporarily incapacitated due to structural damage or interruption of public services (Table 9).
The available resources of the sector to attend the emergency are presented in the summary of Table 10. Theprovision of medical services was undertaken at two levels: prehospital and hospital. At the prehospital level,health personnel participated in removing debris and rescuing victims, and in administering first aid. At someof the disaster zones non−official triage and stabilization were organized in situ in cooperation with Red Crosspersonnel and volunteer groups.
Table 10. Summary of Available Health Resources After the Earthquake, Mexico, D.F., 1985
Resources TotalHospitals II and III 105Minor units 729Hospital beds 15,162Ambulances 600Doctors 20,403Nurses 32,805Source: Informe del Comit‚ Interinstitutional de la Secretaría de Salud, October, 1985.
On the other hand, hospital response was based on the following emergency guidelines:
1. Amplification and extension of emergency and hospitalization services.
2. Integration and coordination of medical attention with the different institutions that providehealth services in the metropolitan area and surrounding states.
To comply with the first criteria, it was agreed to:
1. Release all hospitalized patients with subacute and chronic diseases who were in nodanger of becoming worse or developing complications. This produced an immediateavailability of 2,609 beds. (28)
2. Replace hospital medical attention teams every eight hours, especially for surgical, traumaand emergency services.
3. Habilitate those hospital areas that may require sufficient third level installations to provideservices, for example, care for gyneco−obstetrics patients. A postpartum stay was for 24hours.
4. Utilize available space to the maximum capacity for installing new beds or include others inreduced spaces, such as hallways.
5. Cancel all scheduled surgeries.
16

Regarding the second criteria, it was decided to:
1. Assess demand through triage and reorient patients to first level institutions, homes, orshelters.
2. Remit patients to surrounding states, especially Hidalgo, Mexico, Puebla and Querétaro,since the maximum estimated travelling time was determined to be from one to two hours.
With the previous measures, the "single health system" attended 12,605 victims, 11,770 (93.4%) byinstitutions of the public health sector and 835 (6.6%) by the private health sector.
Fourteen percent of the total (1,879 victims) required hospitalization. The lethality rates for these victims was12.8%, and 1.9% for all those attended at institutions, with or without hospitalizations, see Table 11. (29)
Observe the distribution of hospitalized victims according to age and sex in Table 12. Note the highpercentage of persons with no available data. Unfortunately, the high numbers of patients with incompleteinformation and imprecise diagnosis, frequent in these cases, prevented a better analysis of the attendedmorbidity.
In general, the Federal District showed self−sufficiency in handling the health aspects of these kinds ofemergencies. According to a report by the chief medical officer of the Federal District, close to 90% of theearthquake victims were treated during the first day of the tragedy. After this, hospital demand descendedabruptly. Three days later 1,6(19 beds were available.
Table 11. Number and Percent of Persons Treateda, Hospitalizedb, and Deceased, According to Originof the Institution, Mexico, D.F., 1985
a Proportion treatedb Proportion hospitalized
Treated Hospitalized DeceasedOrigin Number % Number % Number %Public 11,770 93.4 1,510 12.8 212 14.0Private 835 6,6 369 44.2 29 7.8TOTAL 12,605 100.0 1,879 14.9 241 12.8Source: Adapted from the Informe de las acciones e impacto en las instituciones de salud. Dirección Generalde Epidemiología S.S.A.
Table 12. Distribution of Persons Hospitalized by Age and Sex, Mexico, D.F., 1985
MASCULINE FEMININE TOTALGroup Number Percent Number Percent Number Percent> 1 13 0.7 17 0.9 30 1.61−4 24 1.3 11 0.5 35 1.85−14 77 4.1 47 2.5 124 6.615−24 154 8.2 203 10.8 357 19.025−44 210 11.2 242 12.9 452 24.145−64 88 4.7 96 5.1 184 9.865 + 35 1.9 46 2.4 81 4.3Ignored 293 15.6 323 17.2 616 32.8TOTAL 894 47 .6 985 52.4 1.879 100Source: Informe de las acciones e impacto en las instituciones de salud. Dirección General de EpidemiologíaS.S.A.
17

Mobilization and evacuation of patients
Some health institutions had to be evacuated, especially second and third level ones that were in danger ofcaving in or that were unable to function due to lack of public or support services. Those health institutionsthat suffered partial or total collapse were evacuated as well. Patients that required continued hospitalization,including many rescued from the ruins, were sent to other hospitals and all those whose condition was stableand satisfactory were released. At total of 4,363 patients were evacuated; some were sent to differentinstitutions and others were sent directly to their homes or shelters (Table 13).
Evacuation of the national medical center of the IMSS
The National Medical Center is a complex of buildings that includes the hospitals of cardiology andpneumology, cancer, pediatrics, obstetrics−gynecology, general, specializations, ophthalmology,thaumatology and orthopedics, and convalescence. Including the buildings where administrative offices andsupport services were located, the center had 2.400 hospital beds.
Table 13. Number of Persons Rescued, Evacuated, and/or Transferred, by Health institution, Mexico, D.F.,1985
Rescued EvacuatedInstitution Trapped Alive Dead Transferred
General Hospital 471 129 342a 292Juárez Hospital 740 179 561 167Medical Center 10 2.900ISSSTE 640DIF 364TOTAL 1.211 308 913 4 4.363
a Includes 47 missing
Source: Adapted d Ban the Informe de las acciones e impacto en las instituciones de salud. DirecciónGeneral de Epidemiología S.S.A.
At the moment of the impact there were about 1,830 hospitalized patients, and it is estimated that in theexternal consultation areas, laboratories and radiodiagnostic areas, there were approximately 900 ambulatorypatients. (30) The most serious material damages were produced in the buildings where equipment wasstored and in the radiodiagnostic area of the Cardiology and Pneumology Hospitals, where 10 employees ofthe institute perished.
Evacuation activities were developed and undertaken in four stages:
1. Identify security and patient transport areas2. Revise the physical areas and analyze patients' status3. Redistribute employees to other IMSS medical institutions; and4. Recuperate instruments, equipment and furniture
The first two stages were undertaken on the initiative of personnel of the respective health units, after rapidevaluation of structural damages. The first to be evacuated were those patients that did not need help formobilization; second were those that required partial help, and finally those that were invalid or dependent onmedical support equipment.
The Pediatrics and Obstetrics−Gynecology Hospitals concentrated their patients at the Congress Unit;General Hospital and the Convalescence Unit sent their patients to open areas of General Hospital; Traumaand Cancer to the Central Garden, and Cardiology to the exterior circulation. The Specializations andOphthalmology Hospitals suffered no damage, nevertheless, they later had to evacuate their patients due tothe interruption of basic public services.
The third stage was dedicated to the redistribution of patients from the security areas. First, patients wereidentified according to medical criteria, as to whether they could be transported to their homes at no risk to
18

their general health status (many of them were scheduled for elective surgeries the morning of theearthquake); second, decisions were rendered on patients who needed continued hospitalization but could betransported to other IMSS installations without danger, and third, decisions were rendered on the transport ofcritical care patients (intensive care, coronary care, transplant units, etc.) to secure areas that had beenadapted and equipped by engineers. Later on, these patients were transferred to other institutional hospitals,taking all necessary precautions to avoid the inherent risks associated with intensive care.
Of the 1,830 hospitalized patients, 766 or about 42%, remained at the same institution, due to the fact thatthey were being attended in the intensive care, coronary, renal transplant units, etc. The rest were sent totheir homes. In a lapse of about four hours, the whole complex had been evacuated without incident.
Special attention was given to the referral of each patent; the reference institution, date and time werecarefully documented. Patient listings were released to the media that same night, and a daily publication ofthe listings in newspapers continued for a week.
Management of bodies
The task of identifying bodies was made easier, in large measure, due to the presence of representatives fromthe coroner's office in each of the delegations of the Federal District. Each of these institutions has assignedforensic physicians from the General Division of Medical Services whose responsibility it is to participate in alllegal medical procedures of the political−administrative jurisdictions. (31)
After the earthquake the forensic physicians were transported to the disaster sites to initiate recollection,transport and handing over of bodies to relatives with previous elaboration of death certificates or bodyremoval forms according to each case. In these documents the address of where the bodies were picked upwas consigned, including the site in the interior of the fallen building, if it was possible to identify.
All bodies were identified a card that had the address where death had occurred, date, time, name of thevictim, apparent age, sex, name of person who identified or recognized the body, etc. If the body was amplyidentified by family members, a death certificate was issued immediately and the body was handed over, withthe approval of the competent authorities.
Unidentified bodies at the disaster sites and those identified but unclaimed were taken to the morgue of thecorresponding institution. At the morgue, unidentified bodies were regrouped by apparent age and sex, and,during the initial hours, their clothes were left on to facilitate possible identification. Identifying marks, as wellas characteristics of personal belongings (watches, rings, bracelets, medallions, earrings, etc.) were writtendown on each body's identification card. The bodies were maintained at cold temperatures with blocks of ice.After five days formaldehyde was applied to slowly decomposing bodies. The rapidly decomposing bodieswere sent for burial, with the approval of the judicial authorities. Bodies that had to be conserved for more timewere placed in body bags, with the head and identification card visible.
Social and cultural customs are factors to be considered after a disaster. The persons gathered here areprotesting the use of common burials and cremations. Furthermore, they are anxious to recover the bodies oftheir loved ones.
Quick entrance was granted to persons visiting body deposits for identification by friends and/or familymembers. If the bodies were identified, death certificates were expedited and the bodies released. Theunidentified bodies were photographed face front and side view and burial was ordered after a short time.
From September 19 to October 30, 1985, a total of 4,524 death certificates or body release forms wereissued, of which 586 corresponded to unidentified bodies. In a few cases autopsies were undertaken andthese reports were annexed to the personal files of the deceased. Finally a brief report was filed on eachunidentified victim, and together with photographs were exhibited in public places to promote identification.
The General Division of Medical Services, which has direct supervision over forensic physicians with clearlydefined guidelines, completed its task without duplicity of functions or divergence on the collected information.An updated bulletin on victim identification activities of the coroner's office was issued every six hours.
19

Damages to the hydraulic system
Mexico City has at present the largest and most complex hydraulic system in the world. To provide drinkingwater to more than 10,000,000 persons the supply system has the following sources: water from the westernzone, provided by the Lerma and Cutazmala rivers; underground waters via wells located mainly in the south,north, and center of the city and some important springs located in the southeast. The eastern region issupplied from sources out of the Federal District which makes this area extremely vulnerable.
The city has a hydraulic infrastructure (Table 14) which permits it to have an average of 35.4 cubic meters persecond of drinking water. That is enough to satisfy about 97% of the needs of the population with homeconnections. The remaining 3% is supplied by water tank trucks. (Figure 9) The combined drainage systemfor the removal of sewage and rain waters is made up of 12,300 kilometers of secondary networks withdiameters of less than 0.60 meters; 1,200 kilometers of collectors with diameters ranging from 0.60 to 4.00meters, and 64 pumping plants with a total installed capacity of 500 cubic meters per second as well as 400kilometers of main drains for the waterworks of the City. (32) A deep drainage system formed by interceptorsthat converge on a single system for the removal of sewage and rain waters also exists.
Table 14. Hydraulic Infrastructure of Mexico, D.F., 1985
Amount Description202 Storage tanks with a capacity of 1.5 million cubic meter209 km of acueducts with diameters that vary between 1.83 and 2.50
meters467 km of conduction lines of different diameters555 km of primary network from 0.50 to 1.20 meters12,060 km of secondary network with diameters smaller than 0.5 meters102 water pumping plants to provide water to elevated parts of the citySource: Reference (32).
20

Figure 9. Network of Treated Water
21

Figure 10. Zones with Water Problems in the Federal District from September 19, 1985 (Date of Earthquake)Through September 23.
At present, the drainage system serves about 74% of the population. Irregular housing, located on theoutskirts of the city, does not have this service. The supply system of water was the most affected by theearthquake. Thirty−eight cracks occurred in the southeastern aqueducts, secondary drains of San Luis,Tulyehualco, La Noria, Chalco and Tecomitl thereby interrupting the delivery of 7,600 liters per second, whichrepresented about 22% of the total city supply. As a result of these damages approximately 2,000,000inhabitants of the eastern and central parts of the city were left without water (Figure 10).
The most common failure in the aqueducts occurred at the joints of the pipes which did not permit longitudinaldisplacements. One hundred and sixty−eight (168) leaks occurred in pipes made of asbestos, cement andreinforced concrete of the primary network, and mainly in the Cuauhtemoc, Venustiano Carranza, Ixtacalco,Ixtapalapa and Gustavo Madero delegations. Leaks occurred in many ways such as incrustation between twopipes, uncoupling, etc.
In the secondary networks, a total of 7,220 leaks were repaired. These were caused mainly by the rupture ofspecial pieces made of cast iron in the valve boxes; by the changes in direction near the joints or byincrustation of two or more tubes. The reestablishment of normal services was achieved after 40 days ofaround−the−clock work.
Drainage System
22

Irregularities were identified in important structures of La Piedad and Churubusco rivers, Central Supply andthe Central−Western Interceptor.
The collector of the southern towns, a pressurized conduct of the primary network located in the Xochimilcodelegation, suffered cracks all along its extension. The same situation was to be found in various collectorsthat discharge by pump to the main drainage canal. This canal was deformed near the pumping plants due tothe differential sinking produced by the earthquakes.
The oxidation lagoon of San Luis Tlaxialtemalco, located in the south of the city, was practically unable tofunction.
Fissures occurred at some of the sewage pumping plants as well as in other installations such as stormdrains, subcollectors, etc. In general, the damages to the drainage system were less than those to theconduction and distribution systems of potable water. This was probably due to the fact that the conducts areless flexible in their joints, have more freedom to twist and move and are buried deeper.
Repairs to the aqueducts were started immediately thanks to the availability of a large selection of specialmaterials and spare parts. In spite of this, it was necessary to begin intensive production of additional spareparts for the reestablishment of the primary networks and aqueducts.
Water Quality
During the emergency period, the General Division of Hydraulic Operation and Construction (DGCOH)analyzed a total of 59,400 samples to control water quality of the city (for comparison, a total of 40,000samples are taken throughout the whole year).
In order to compensate the lack of water service to shelters, hospitals, nurseries, etc. a total of 15,000 plasticwater bags, provided by a plant in the Benito Juárez delegation, were distributed daily.
Water distribution was carried out by 480 water tank trucks from nearby states, the army, other institutionsand the Federal District. In some affected zones, 90 portable water tanks were installed, each with an 11,000liter capacity and with multiple faucets for public use. All these measures permitted the strict control of waterquality. Nevertheless, bacterial contamination was detected and treated by hyperchlorinization until residualchlorine registered 2 parts per million in network tanks and water tank trucks.
In spite of apparent water contamination, no diarrhea! outbreaks were detected. The increase in the frequencyof diarrheal episodes in some shelters was probably due to alimentary contamination (33).
Environmental health services, as well as water storage, delivery and sewage systems, are vulnerable todisasters. The installations may be damaged, the channels broken or the operations disrupted for lack ofelectricity. Disaster preparedness plans should include provisions to store enough water for the affectedpopulation.
3. Public health and preventive medicine
The initial information on the magnitude and devastation of the earthquake was communicated by all themedia. Some health institutions of the country made decisions based on information from those sources,which at times proved to be unreliable, contradictory and exaggerated. Guided by radio information, oneinstitution established an operations base, one hour later, at different disaster sites, with vaccination postsagainst typhoid fever and tetanus (34).
On September 27, the vaccination order was revoked, but it was not stopped at these posts units the 30th,and during this period 1,117 doses were given due to public demand.
The Interinstitutional Health Committee decided to vaccinate against tetanus, selectively and voluntarily; thiswas particularly important for search and rescue groups. Fumigations with sodium hypochlorite were orderedin certain zones where rescue activities had concluded and only rubble remained to be cleared away. Thehealth sector did not approve of this measure but consented in order to alleviate public concern about theharmful effects of decomposing bodies.
23
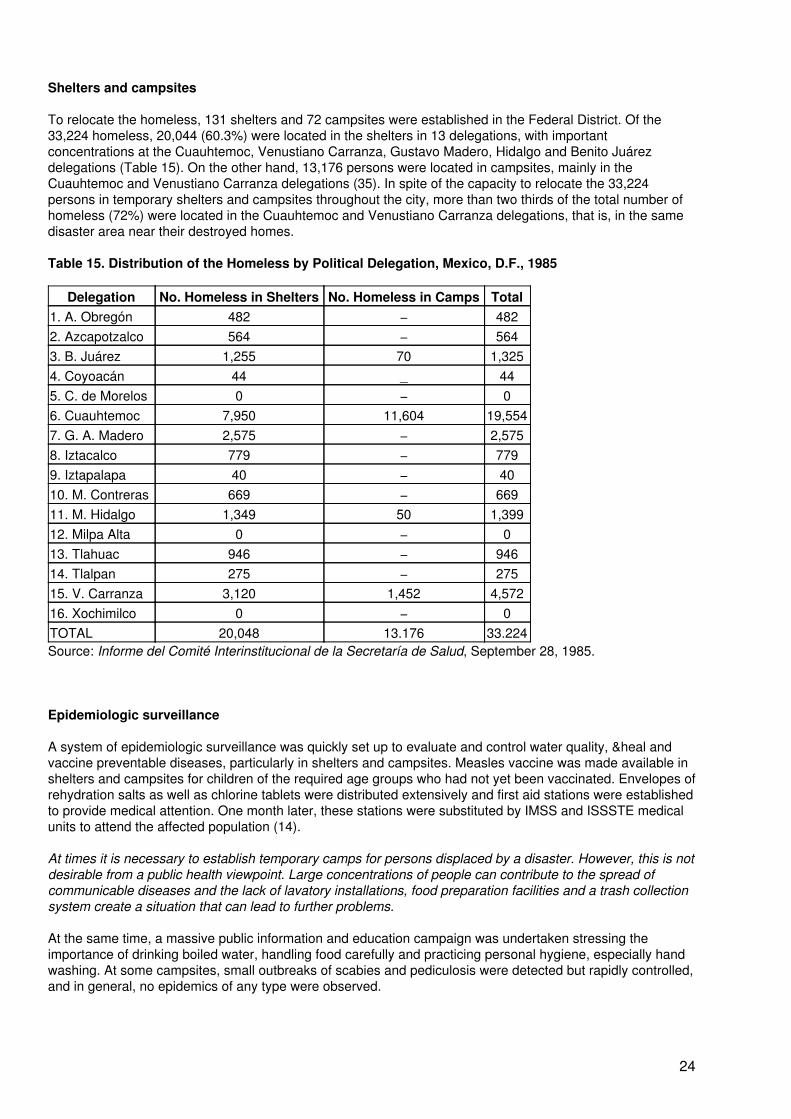
Shelters and campsites
To relocate the homeless, 131 shelters and 72 campsites were established in the Federal District. Of the33,224 homeless, 20,044 (60.3%) were located in the shelters in 13 delegations, with importantconcentrations at the Cuauhtemoc, Venustiano Carranza, Gustavo Madero, Hidalgo and Benito Juárezdelegations (Table 15). On the other hand, 13,176 persons were located in campsites, mainly in theCuauhtemoc and Venustiano Carranza delegations (35). In spite of the capacity to relocate the 33,224persons in temporary shelters and campsites throughout the city, more than two thirds of the total number ofhomeless (72%) were located in the Cuauhtemoc and Venustiano Carranza delegations, that is, in the samedisaster area near their destroyed homes.
Table 15. Distribution of the Homeless by Political Delegation, Mexico, D.F., 1985
Delegation No. Homeless in Shelters No. Homeless in Camps Total1. A. Obregón 482 − 4822. Azcapotzalco 564 − 5643. B. Juárez 1,255 70 1,3254. Coyoacán 44 _ 445. C. de Morelos 0 − 06. Cuauhtemoc 7,950 11,604 19,5547. G. A. Madero 2,575 − 2,5758. Iztacalco 779 − 7799. Iztapalapa 40 − 4010. M. Contreras 669 − 66911. M. Hidalgo 1,349 50 1,39912. Milpa Alta 0 − 013. Tlahuac 946 − 94614. Tlalpan 275 − 27515. V. Carranza 3,120 1,452 4,57216. Xochimilco 0 − 0TOTAL 20,048 13.176 33.224Source: Informe del Comité Interinstitucional de la Secretaría de Salud, September 28, 1985.
Epidemiologic surveillance
A system of epidemiologic surveillance was quickly set up to evaluate and control water quality, &heal andvaccine preventable diseases, particularly in shelters and campsites. Measles vaccine was made available inshelters and campsites for children of the required age groups who had not yet been vaccinated. Envelopes ofrehydration salts as well as chlorine tablets were distributed extensively and first aid stations were establishedto provide medical attention. One month later, these stations were substituted by IMSS and ISSSTE medicalunits to attend the affected population (14).
At times it is necessary to establish temporary camps for persons displaced by a disaster. However, this is notdesirable from a public health viewpoint. Large concentrations of people can contribute to the spread ofcommunicable diseases and the lack of lavatory installations, food preparation facilities and a trash collectionsystem create a situation that can lead to further problems.
At the same time, a massive public information and education campaign was undertaken stressing theimportance of drinking boiled water, handling food carefully and practicing personal hygiene, especially handwashing. At some campsites, small outbreaks of scabies and pediculosis were detected but rapidly controlled,and in general, no epidemics of any type were observed.
24
Use of chlorine tablets and oral rehydration salts
Guadalupe Frausto Pérez (36) and a group of students from the school of Public Health of Mexico conducteda survey among families regarding their use of chlorine tablets and oral rehydration salts. In the interest ofmanaging similar public health situations, pertinent aspects of the study are presented.
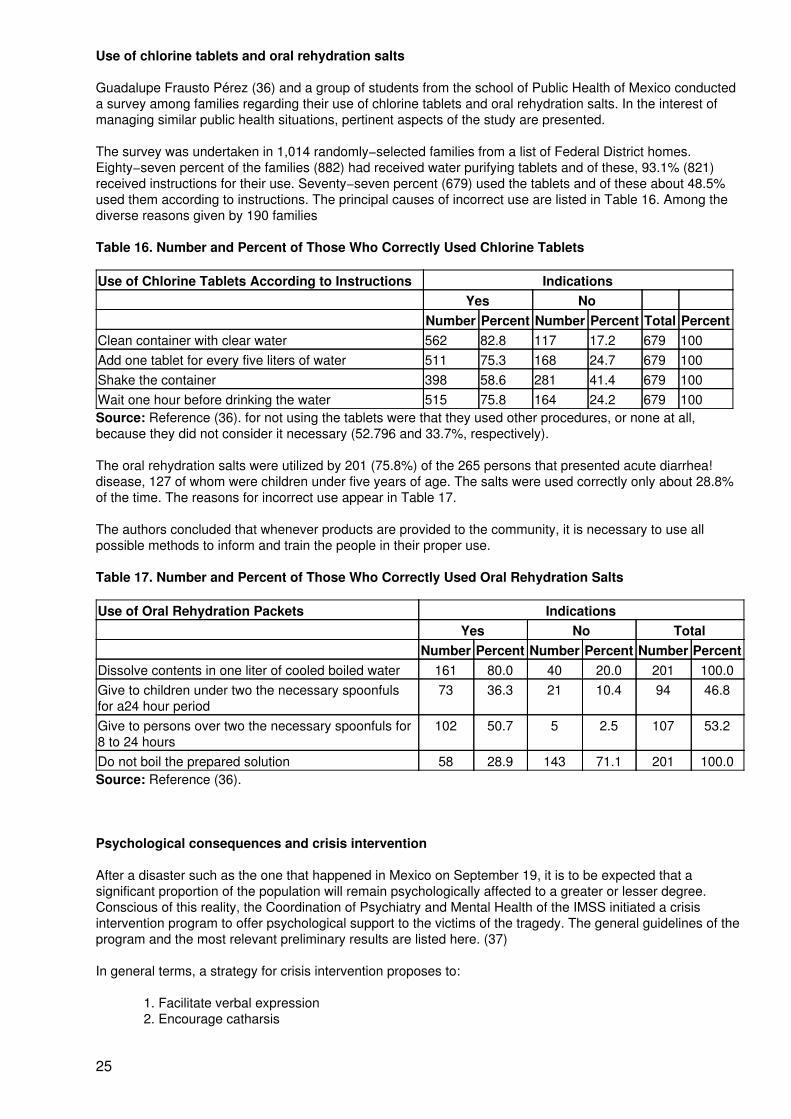
The survey was undertaken in 1,014 randomly−selected families from a list of Federal District homes.Eighty−seven percent of the families (882) had received water purifying tablets and of these, 93.1% (821)received instructions for their use. Seventy−seven percent (679) used the tablets and of these about 48.5%used them according to instructions. The principal causes of incorrect use are listed in Table 16. Among thediverse reasons given by 190 families
Table 16. Number and Percent of Those Who Correctly Used Chlorine Tablets
Use of Chlorine Tablets According to Instructions IndicationsYes No
Number Percent Number Percent Total PercentClean container with clear water 562 82.8 117 17.2 679 100Add one tablet for every five liters of water 511 75.3 168 24.7 679 100Shake the container 398 58.6 281 41.4 679 100Wait one hour before drinking the water 515 75.8 164 24.2 679 100Source: Reference (36). for not using the tablets were that they used other procedures, or none at all,because they did not consider it necessary (52.796 and 33.7%, respectively).
The oral rehydration salts were utilized by 201 (75.8%) of the 265 persons that presented acute diarrhea!disease, 127 of whom were children under five years of age. The salts were used correctly only about 28.8%of the time. The reasons for incorrect use appear in Table 17.
The authors concluded that whenever products are provided to the community, it is necessary to use allpossible methods to inform and train the people in their proper use.
Table 17. Number and Percent of Those Who Correctly Used Oral Rehydration Salts
Use of Oral Rehydration Packets IndicationsYes No Total
Number Percent Number Percent Number PercentDissolve contents in one liter of cooled boiled water 161 80.0 40 20.0 201 100.0Give to children under two the necessary spoonfulsfor a24 hour period
73 36.3 21 10.4 94 46.8
Give to persons over two the necessary spoonfuls for8 to 24 hours
102 50.7 5 2.5 107 53.2
Do not boil the prepared solution 58 28.9 143 71.1 201 100.0Source: Reference (36).
Psychological consequences and crisis intervention
After a disaster such as the one that happened in Mexico on September 19, it is to be expected that asignificant proportion of the population will remain psychologically affected to a greater or lesser degree.Conscious of this reality, the Coordination of Psychiatry and Mental Health of the IMSS initiated a crisisintervention program to offer psychological support to the victims of the tragedy. The general guidelines of theprogram and the most relevant preliminary results are listed here. (37)
In general terms, a strategy for crisis intervention proposes to:
1. Facilitate verbal expression2. Encourage catharsis
25

3. Overcome negation4. Combat negativism5. Tolerate angry behavior6. Avoid inactivity (high risk for individuals or groups experiencing grief)7. Imagine future situations
Considering these guidelines, a strategy was designed to treat people by means of individual and grouptherapy sessions, depending on their need for intervention. Light and moderate cases were attendedopportunely by nonprofessional personnel and severe cases were referred to professionals. Individual andgroup therapy sessions were conducted with a community participation program that promotedself−responsibility and self−sufficiency.
To start this program it was necessary to train professionals and nonprofessionals how to identify emotionalproblems and how to use simple psychological intervention techniques. Staff members were highly motivatedto avoid crisis within themselves and to stimulate good working habits.
The development of the program was preceded by a massive community information and orientationcampaign regarding the locations for receiving treatment and emphasizing the importance of adequate stressmanagement as a personal, family and community goal.
The following risk groups were identified:
1. Persons with lost family members2. Children and old persons lost in shelters3. Homeless persons and families4. Hospitalized survivors and their families and5. Persons and families who had lost family members because as a result of the earthquake
Among the places chosen as treatment sites were community spaces, social security centers of the IMSSserving as shelters, homes, factories (using work security brigades), family medicine units, regional generalhospitals, and centers that provide specialized psychiatry services.
During the first three weeks after the disaster, close to 1,000 mental health promoters (professional andnon−professional) and more than 100 supervisors were trained. The instrument to detect emotional problemshad three sections: Section A explored general physical and emotional health; Section B reviewed Beck'sdepression inventory (38), and Section C included Brown's scale for life's events (39) which explored lossessuffered in three basic areas: personal, family, and social.
The effects of a disaster can cause psychic as well as physical harm. Many persons who live trough thetragedy of an eartquake report symptoms of depression, anxiety and insomnia. Trough group and individualtherapy, the survivors learn techniques of verbal expression so that they can combat accumulated negativityand reestablish their lives.
In Figure 11, the study population is classified into 3 groups to facilitate the identification and management ofcases: healthy persons or those with compensated lesser crisis (grades 0 − 12); persons with moderatelyuncompensated crisis (grades 13 − 25), and persons with uncompensated severe crisis (grades of 26 ormore). Finally a proportional sample of 3,964 persons from risk groups was selected. (Table 18)
Table 18. Study of Psychological Consequences and Intervention. Sample of Population by Location,Mexico, D.F., 1985
Location Number PercentShelters 436 11.0Medical units 396 10.0Administrative units 912 23.0Factories 1,864 47.0Services and commercial locations 277 7.0Other 79 2.0TOTAL 3,964 100.0Source: Reference (37).
26

Results
In Table 19 some socio−demographic characteristics of the study population can be observed, and in Table20, the percentage distribution of the types of crisis are identified according to sex. Note that women hadmoderate and severe crisis D frequency than men (twice as many). Uncompensated severe crisis wascharacterized by insomnia (1796), somatic reactions (13%), anxiety/depression (6%), and social inadequacyproblems (396). In general, the population studied developed anxiety/depression (41%); insomnia (40%);somatic reactions (39%); social inadequacy (26%) and autodestructive ideas (13%) as a consequence of theearthquakes and their devastating effects. (Table 21)
27

Figure 11. Crisis Intervention, Classification and Management of Patients, Mexico, D.F., 1985
28

Table 19. Sociodemographic Characteristics of the Population Studied, Mexico, D.F., 1985
Variable Class Percent(N=3.964)
Sex Feminine 44Masculine 56
Age groups 0 − 20 10.020 − 24 19.025 − 29 21.00 34 16.035 − 39 13.040 − 44 9.045 − 49 6.050 − 54 5.055 and over 1.0
Marital status Married 58.0Single 31.0Widow/Widower 2.0Divorced or separated 4.0Cohabitant 5.0
Education No official education 8.0Grade school incomplete 1.0Grade school complete 25.0High school or equivalent 31.0Preparatory or equivalent 17.0Professional 18.0
Occupation Professionals and educators 9.0Domestic workers 47.0Skilled laborer 19.0Unskilled laborer 13.0Housewife 5.0Student 4.0Others 3.0
Source: Reference (37).
Table 20. Distribution of Crisis by Type and Sex
PercentType of Crisis Women Men TotalLight and with compensation 26.0 47.0 73.0Moderate and without compensation 10.0 6.0 16.0Severe and without compensation 8.0 3.0 11.0Source: Reference (37).
Table 21. Percentagea of Symptomatologic Categories, Using Section A of the InvestigativeInstrument, Mexico, D.F., 1985
a N=3.964
Symptomatology
CrisisSomaticReaction
SocialInadequacy
Insomnia Depression/Anxiety
AutoDestructive
(%) (%) (%) (%) (%)
29

Withoutsymptoms
61.0 74.0 60.0 59.0 87.0
Light 19.0 17.0 16.0 26.0 7.0Moderate 7.0 6.0 7.0 9.0 5.0Severe 13.0 3.0 17.0 6.0 1.0Source: Reference (37).
Depression was more frequent in women than in men, especially in light and moderate degrees. A markedabsence of depression in men is illustrated in Table 22.
In Table 23, the number of losses suffered with respect to four specific areas is shown. The social area wasthe most affected (35%); followed by the economic (26%); family (23%) and personal (20%).
Table 22. Percenta of Depression Intensity by Sex, Using Section B of the Investigative Instrument,Mexico, D.F., 1985
a N=3.964
Intensity Women Percent Men Percent Total PercentNot depressed 25.0 45.0 70.0DepressedLight 12.0 8.0 20.0Moderate 6.0 3.0 9.0Severe 0.5 0.5 1.0Source: Reference (37).
Table 23. Frequency and Percenta of Loss in the Areas Investigated (Section A), Mexico, D.F., 1985
a N=3.964
No. of Losses or Events Personal Area Economic Area Familial Area Social Area(%) (%) (%) (%)
Without loss 80.0 74.0 77.0 65.01 16.0 15.0 10.0 19.02 3.0 7.0 6.0 10.03 − 4 1.0 3.0 5.0 5.05 or more − 1.0 2.0 1.0Source: Reference (37).
Disasters affect women and children to a disproportionately greater extent. The statistics indicate that in thisdisaster, women were more vulnerable than men to suffer deep depression and anxiety.
4. International cooperation
International solidarity was demonstrated from the first hours of the disaster. Upon reestablishment ofcommunications systems with the international community, specific aid was solicited according to priorities toattend the following needs:
1. Specialized search−and−rescue equipment to extract persons trapped in destroyed buildings. Heavymachinery such as cranes to remove rubble.
2. Equipment for second and third level hospitals, and particularly rehabilitation equipment as well as suppliesfor operating and recovery rooms, intensive care units, maternity wards and clinical laboratories.
3. Equipment and supplies for suturing, intravenous perfusion, x−ray films and refrigeration units.
30

During the first 10 days after the earthquakes, the General Comptroller's Ministry of the Federal Districtregistered 177 international flights from 31 countries with 1,088 tons of aid, Table 24. (40) (41) These diversedonations went directly to various institutions, (Table 25). Of these, 748 tons (69%) were not solicited bynational authorities and consisted of non−priority items such as medicines, food, clothes, blankets andsupplies. The comparison of supplies and other items received and utilized appears in Table 26. Note thedeficit that occurred with respect to some of the solicited articles such as x−ray film, anesthetics andimmobilization materials.
There was ample availability of blood and derivatives thanks to voluntary donors throughout the city. UNDROinformed that as of October 1, 1985, contributions from United Nations organisms, government organizations,voluntary agencies and the International Red Cross had reached a sum of 10,750,000 dollars, and that moreaid was expected.
Table 24. Mexico Earthquake, International Aid (from September 20−30, 1985)
Category of Aid Tons PercentMedicines 335 31.0Clothes and blankets 259 24.0Food 154 14.0Rescue equipment 150 13.6Tools 73 6.7Machines and vehicles 69 6.3Medical instruments 48 4.4TOTAL 1,088 100.0Source: Secretaría de la Contraloría General de la Federación, 1985.
Table 25. International Aid and Receiving Institutions, Mexico, D.F., 1985
Receiving Institution Tons PercentFederal Government 335 30.7Mexican Red Cross 210 19.3Embassies 251 23.0Private institutions 292 27.0TOTAL 1,088 100.0Source: Secretaría de la Contraloría General de la Federatión, September, 1985
Table 26. International Aid Received and Used in the Emergency Phase, Mexico, D.F., 1985
Item ReceivedBoxes/Packets
Pieces UsedPieces
Medicines (analgesics, sedatives, antibiotics) 5,493 28,614 27,595Disposable syringes 1,014 67,800 10,080Needles 710 12,950 12,600Antiseptics 128 2,007 368 Lt.Supplies for immobilization 159 0 6,426Medical supplies (bandages, gauze, adhesive tape, absorbentpads, cotton, etc.)
2,428 8,923 10,332
I. V. solutions 3,808 4,650 6,778 LtAnesthetics 42 608 2,500Surgical material 2,166 5,393 789X−ray equipment (and film) 133 0 1,879Biologicals 10 200 50,000
DosBlood and derivatives 231 0 1,732
Units
31

Non−classified medical material 20,469 26,574 0Others (blankets, tents, food, clothes, etc.) 13,969 2,789 0Search−and−rescue equipment, cranes and towing vehicles forremoving rubble
540 6,421 0
TOTAL 51,293 166,929 −Source: Información de la Secretaría de Salud, Departamento del Distrito Federal y Cruz Roja Mexicana.
International aid after a disaster can be invaluable when it meets a specific need. The French governmentprovided specialized equipment and trained personnel to help in the search−and−rescue operations.
5. Perspectives
Valuable lessons were learned and certain preoccupations awakened in the aftermath of this disaster, whichaffected one of the largest cities in the world. In this city of disperse and complex character, immense lossesof material goods and human lives were sustained, and serious damage, some irreparable, was done to thecultural heritage of this country and of the world.
This unfortunate event revealed the need to:
1. Strengthen the health sector plans for managing disaster situations.
2. Elaborate vulnerability and contingency plans, especially for geographic or geopoliticalareas at high risk.
3. Elaborate hospital plans to manage internal and external disasters, and to continually trainhealth personnel in the management of these types of emergencies.
4. Develop techniques and methodologies for the rescue of trapped persons in collapsedbuildings.
5. Promote information and education programs for the public on first aid, communityparticipation and what to do in the event of a disaster.
6. Promote information and training programs for the communications media on healthaspects after disasters.
7. Develop information and motivation activities for donor countries and institutions so thatthey avoid sending non−solicited aid; provide instructions how to send international aid in anefficient and positive manner.
Annex : The survival of people in collapsed buildings
Michael E. Durkin (1), Anne H. Coulson (2), Martha Hijar (3), Jess Kraus (4), and Hitomi Ohashi Murakami (5)
Introduction
Complete collapse is the most serious outcome of earthquakes for buildings and occupants. However, despiteits obvious implications for life safety, collapse does not result in death for all building occupants. The survivalof some occupants raises important research questions. Why did some occupants survive while othersperished? Did such factors as location of occupants, actions of occupants, injury type and severity,nonstructural cements and building contents, nature and time of entrapment, and method of rescue play a rolein survival − factors which we can learn from and train people about? Or were the survivors mere luckybeneficiaries of fortuitous circumstances? These questions have an obvious bearing on how we prepare forfuture earthquakes.
Following the 1985 Mexico earthquakes, we surveyed eighteen medical residents who survived the collapse
32

of the Medical Residents Dormitory at General Hospital in Mexico City; in addition we surveyed six otherresidents who lived in the dormitory, but were in other structures at the time of the tremor: At the earthquake'sonset, four residents were in the neighboring Obstetrics and Gynecology Hospital building (that alsocollapsed) and two were in a basement corridor connecting the dormitory with a cafeteria (Table 27). Thedormitory and hospital buildings became a major focus of search and rescue efforts lasting for several weeks.
The following paper presents results of these two case studies. Subsequently, other collapsed buildings inMexico City and San Salvador were studied and these findings are presented in the discussion section. Whilethese buildings cannot help us generalize about collapse patterns, they can help us explore a situation thathas received little systematic attention to date. So far we have derived preliminary results on the role oflocation and occupant actions, the severity of injury, nonstructural elements and building contents, andmethod and timing of rescue. In order to derive these results, we used a cohort approach.
Table 27. Location of Interviewed Survivors (N=24)
Location Number of SurvivorsDormitory Building 18Obgyn Hospital Building 4Underground Corridor 2TOTAL 24Background
The Buildings
The Medical Residents Dormitory was an eight−story, reinforced concrete structure. The building had arectangular configuration. Seven of the eight floors were allocated to domiciliary space. Each floor in therepeated floor plan had eight bedrooms, four on either side of a double loaded corridor. An elevator, fire stair,and multi−purpose room were located in the center of each floor.
Four of the residents we interviewed were, at the time of the tremor, located in the Obstetrics andGynecological Hospital building, a six−story reinforced concrete structure that also collapsed. Two otherswere in a basement corridor connecting the dormitory to a cafeteria.
The Occupants
On the morning of September 19th, 1985, this dormitory was home to seventy−six medical residents. Of thisnumber, forty residents ultimately survived, and thirty−six perished from earthquake−related injuries (44)(45).The residents were in different years of the four years' residency training. They ranged in age from 27 to 32.Also, at least ten other students were living in the dormitory illegally when the temblor struck.
Research Approach and Methods
Cohort Approach
In this application, the cohort approach considers a population group that experienced an earthquake. Itattempts to document injury occurrence as related to different types and levels of exposure. A promisingvariation of this approach focuses on the performance of a specific building and the fate of its occupants (42).A useful approach for exploratory studies, the building−specific case study is especially appropriate forinvestigations of the survival of occupants of collapsed buildings − an area receiving little systematicinvestigation. In cases where most building occupants are available for interview and where detailed damageinformation is available, this strategy permits a precise measurement of the exposure with respect to specificpeople to be studied, and enables the calculation of injury rates and severity attributed to specific elementsand situations.
The disadvantage of this approach is that generalization is limited. For one, the results may be influenced byunique features of the situation not found elsewhere; for another, it is difficult to combine or generalize fromother case studies that use different methods and/or data gathering instruments (43).
Specific Methods
33

We used a semi−structured, self−administered questionnaire to document the residents' experience duringand following the September 19 earthquake. The questionnaire covered a number of topics, includingpersonal characteristics, location at the beginning of the earthquake, actions and movements (from thebeginning of the shaking until exiting from the building; or where applicable, actions from time of entrapmentuntil rescue), the cause, type, and severity of injury, the search−and−rescue process, the receipt of medicalcare, and the longer term impacts of the injury.
We subsequently made contact with twenty−eight of the surviving residents, interviewing twenty−four. Of the40 surviving residents, 12 had graduated and could not be located, twenty−four agreed to be interviewed forthis study (including six who were not actually in the building at the time of the collapse), and four declined,finding the remembrance of their experience too traumatic. Of the twenty−four people interviewed, twenty−twowere male and two female. The surviving residents ranged in age from 27 to 32. Since we had no knowledgeof the exact number of "illegal" residents, or the whereabouts of survivors from this group, we excluded themfrom this investigation.
Results
General Factors Timing and Location
Timing as a Factor
Other earthquake injury investigations show that the time of earthquake occurrence is a key factor indetermining occupant exposure to specific hazards (42). For example, when the September 19 earthquakeoccurred, at least thirty−two of the seventy−six residents were in the dormitory (which collapsed): Eleven werein the Obstetrics and Gynecology Hospital building (that also collapsed), and two were in a basement corridor(that sustained no damage) connecting the dormitory with a cafeteria. If the earthquake had occurred later inthe day, fewer residents would likely have been in the two collapsed buildings and more would have beendistributed in other buildings on the General Hospital grounds.
Location of Survivors Within the Building
The eighteen surviving residents interviewed, located in the dormitory at the time of the quake, were residingon the fourth to the eighth floors. One person was on the fourth floor, four on the fifth, three on the sixth, six onthe seventh, and four on the eight. The four interviewed residents in the Obstetrics and Gynecology Hospitalwere making rounds on the fifth and sixth floor(s).
We asked the survivors to indicate others in the same physical setting at the beginning of the earthquake. Wefound that at least eight of the deceased residents were in the dormitory, and three were in the Obstetrics andGynecology Hospital building.
The earthquake occurred at 7:17 a m., a time when most medical residents were preparing for the day.Consequently, seventeen residents were in their rooms, one was on the same floor as his room, two were in acorridor connected to the cafeteria on their way to breakfast, and four were already at work, making rounds atthe nearby six−story Obstetrics and Gynecology Hospital that also collapsed.
Actions of Survivors
We know from our previous injury investigations that occupants of buildings that don't collapse frequently areable to engage in several actions prior to their injury. However, occupant capability in a collapsing structure(rather than a collapsed structure) has not previously been documented. We assume that if people are able toact, then training can possibly reduce their chance of injury. On the other hand, if building occupants cannotact, then training is useless.
We asked respondents to list their actions from the start of the shaking until they were safely outside thebuilding. We asked them to show us when, in this activity sequence, the building collapsed, what actions theyengaged in, and what was the sequence of actions. We found that numerous occupants had both the timeand ability to take several actions before the building collapsed. The actions of occupants in each physicalsetting are summarized below.
The fact that most respondents indicated that their arms or legs were trapped in the collapse reinforces theconclusion that their indicated activities did actually occur prior to collapse.
34

Sequence of Actions of Survivors in the Dormitory
All eighteen residents in the dormitory at the start of the shaking reported being trapped at some point afterthe temblor began. Eight of these residents said that their first action before being trapped was to "stay wherethey were" because they thought it was the right thing to do. Five of these eight were subsequently trappedwithout engaging in any other further action; the remaining three later engaged in several actions before beingtrapped; one getting to a doorway, and two others leaving their dormitory rooms and going into the corridor.
Three others of the eighteen trapped residents said that their first action was to "stay where they were"because they were unable to move (probably because of the shaking intensity in those seconds). Two ofthese residents were then trapped immediately. The third was able seconds later to leave the space he wasin, go into the corridor, and start up a fire stair before being trapped.
The other seven trapped residents were able to leave their rooms and either move to the corridor or stand in adoorway.
Sequence of Actions of Survivors in the Underground Corridor
The two residents in the underground corridor were able to leave the building prior to its collapse. One ofthese residents subsequently administered medical services to his comrades.
Sequence of Actions of Survivors in the Obstetrics and Gynecology Hospital
Two of the four residents, in the Obstetrics and Gynecology Hospital building when the shaking started,stayed where they were because they thought it was the right thing to do. One of these eventually moved intoa doorway. The remaining two immediately moved into a doorway where they were trapped.
Injuries
Of the twenty−four surviving medical residents surveyed, twenty−two suffered an earthquake related injury ormedical problem. Only two respondents had neither, and these had been located in a corridor outside of thebuilding. Eighteen residents suffered multiple injuries. Table 28 contains a line list of the specific injuriessuffered by each respondent. Sixteen of the twenty−two required further treatment, with thirteen requiringhospitalization. In addition, eleven respondents indicated that particular earthquake injuries resulted in acontinuing disability.
The Role of Structural and Nonstructural Elements and Building Contents in Life Preservation
When reinforced concrete buildings collapse, structural elements, nonstructural elements, and buildingcontents often interact to form space pockets within which occupants might be able to survive (46). With thispossibility in mind, we asked our twenty−four survivors if building elements, furniture, or equipment preventeda total collapse in the area that they were in.
The results showed that building elements and building contents clearly played a role in life safety. Ten of thetwenty−two residents (excluding the two who were out of danger) reported such an effect. Eight of theeighteen responding residents located in the dormitory building and two of the four in the Obstetrics andGynecology Hospital building reported that elements or contents performed a role in survival. Table 29presents a further breakdown of responses.
Entrapment
Duration of Entrapment
All of the residents interviewed but the two in basement corridors (22 of the 24 respondents) were trapped.The survivors were mostly rescued quickly. The duration of entrapment ranged from twenty minutes toseventy−two hours, with eighteen of the twenty−two trapped for under five hours, and twenty−one of thetwenty−two trapped for under twenty−four hours. A breakdown of entrapment time is presented in Figure 12.
35

Figure 12. Duration of Entrapment (first 24 hours)
Occupant Actions After Entrapment
If trapped occupants are capable of taking action following a collapse, they can presumably assistthemselves. We therefore asked respondents if 1) they attempted to free themselves, and 2) if their attemptswere successful.
Table 28. Specific Injuries and Severity by Case
Case Age Sex Injury Locus Severity1 28 M a) lacerations back and shoulders light
b) contusions entire body light2 29 M a) contusion lumber region of back mod/severe3 28 M a) multiple abrasions entire body moderate4 29 M a) laceration forehead moderate
b) fracture left femur severec) open contusions arm and forearm moderated) compression thorax moderate
5 32 M a) fracture right tibia severe6 32 M a) crush left ankle moderate
b) hemorrhage left elbow region severec) contusion right hip severe
7 30 M a) fracture severeb) fracture left femur severe
8 28 M a) fracture left femur severe9 27 M a) scratched cornea left eye light
b) rupture left calf moderatec) ruptured tendons right foot light
10 27 M a) fracture right rib moderateb) superficial crush moderatec) cuts and scratches light
11 29 M a) laceration scalp lightb) laceration hand and forearm severec) fracture hand and forearm severe
12 31 M a) fracture both ankles severe13 29 M a) fracture pelvis severe
b) laceration right side light
36

14 28 M a) fracture right femur severeb) fracture hip severec) fracture right leg severe
15 28 M a) sprain right ankle moderateb) cuts and bruises entire body light/mod.
16 27 M a) fracture moderateb) contusion spine moderatec) fracture lower back severe
17 26 F a) fracture right knee moderateb) wound and compression anterior tibia nerve severec) bruise right knee severe
18 26 F a) compound, exposed fracture left foot or leg severeb) dislocation left foot or leg severe
19 28 M a) sprain torso moderate20 28 M a) lacerations front and back light21 30 M a) compression pelvis moderate22 27 M a) fracture left femur severe
b) fracture left humerus severec) scratches and bruises entire body light
Table 29. Performance of Building Elements and Contents
Dormitory N = 18 Obstetrics HospitalN = 4
Yes No Don't know Yes No Don't knowa) structural 4 14 0 0 4 0b) nonstructural 1 17 0 1 3 0c) contents 2 16 0 1 3 0d) don't know 1 0 1 0 0 0Only seven of the residents trapped in the dormitory attempted to free themselves, and only one wassuccessful. The resident who was successful had his right foot bent and trapped. He was able to free the foot,move debris out of the way, and get to the exit.
At least three of the remaining six who tried unsuccessfully to free themselves had a trapped appendage. Oneresident couldn't free his legs. Another couldn't get completely free, although he was ultimately able to free hisright hand. A third resident had almost escaped from the building but the cot/apse caught his foot, leaving hisbody hanging outside the collapsed structure. Three others reported that they were unable to move bythemselves. These data suggest that in certain types of collapses, injuries or building obstacles makeself−help nearly impossible.
Nature of Entrapment
We asked a series of open−ended questions about entrapment. One question helped characterize thephysical setting surrounding the trapped person. We obtained the following results. In eight cases,respondents indicated that part of their body was trapped by falling debris, leaving them with little room inwhich to maneuver. This manner of entrapment (a function of collapse pattern) determined whether or notthey attempted to free themselves, and how successful they were. A second important factor in entrapmentwas the type and severity of injury.
Who Were the Rescuers?
Knowing who actually is likely to rescue trapped earthquake victims is important to effective training andpreparedness planning. Twenty−two of our twenty−four respondents were trapped. Of these, only one wasable to free himself. Table 30 provides a breakdown of who actually performed the rescues. Thirteen residentswere freed by fellow residents. Three residents reported being freed by a combination of fellow residents andother hospital workers. Only two trapped residents were freed by search−and−rescue teams.
37

Table 30. Rescuers by Building Type (N = 21)
Rescuers Dormitory OB\GYN TotalFellow residents 12 1 13Fellow residents and other hospital personnel 2 1 3Fellow residents and search and rescue personnelFellow residents and taxi driver 0 1 1Search and Rescue Personnel 0 1 1Police 1 0 1Rescue Techniques
We also asked people what methods were used in finding them, including how they knew that rescuers werenear. In seventeen of twenty−one cases, the method used was human voices − calling out by both therescuers and by those trapped. Other methods mentioned were knocking and making noise with objects suchas an iron bar. No one mentioned sophisticated technology as a method of contact. Voices were likely thepredominant method because colleagues performed most of the rescues prior to organized search and rescueand use of sophisticated equipment at these collapse sites.
Key Fears Of Those Trapped
We also asked victims if, while they were trapped, any of a list of factors constituted a serious threat to theirsurvival. The results appear in Table 31. Most of the trapped residents indicated that the major threat was theremoval of rubble. Those trapped heard the rescue operations occurring and were afraid that they would becrushed as rubble was shifted and removed.
Table 31. Fears of Those Trapped
Fears Trapped personsRemoval of debris(afraid of being crushed) 15Severity of injury 7Lack of oxygen 6Lack of liquids 3Other (pressure on abdomen) 1Gas 0Fire 0Discussion of Subsequent Results, Conclusions, and Implications
The following discussion integrates the previous results with our subsequent research on survival in buildingscollapse both in Mexico City (case series of 120 survivors) and San Salvador (cohort study; five−storyreinforced concrete office building) (49) (50), completed since publication of the Spanish version of this paperin 1988.
These cumulative research results have important implications for future earthquake casualty estimations andtheir application to preparedness, response, and recovery planning. The results suggest mitigationapproaches for reducing the demand for health services and for increasing the supply of these resources.
First, complete building collapse does not result in death for all building occupants. Even collapsed structurescan have substantial numbers of survivors. For example, three reinforced concrete buildings investigated sofar had gross survival rates of 24%, 45% and 73% respectively suggesting that collapse patterns affectsurvival rates (53).
Second, we found that severe injury in structural collapse is not the exclusive misfortune of the trapped.Thirty−eight percent (38%) of the nontrapped occupants surveyed suffered a severe injury. Conversely, asubstantial proportion (37%) of those trapped suffered relatively minor injuries (52). Although General Hospitalenabled the victims to be rescued by medical personnel, we found that the majority of trapped, injured in othersettings, were either rescued by lay persons (co−workers, family, and neighbors with no rescue or medicalskills) or managed to free themselves. In addition, even trained rescue personnel did not have medicalexpertise (47).
38

Third, our analysis of the proportion of major to minor injuries rescued by each type of rescuer revealed thatover one−third of those rescued by each group, for example by lay persons, had serious injuries. Untrainedrescuers encountered serious injuries that were immediately life threatening or could lead to permanentdisability if mishandled. They encountered those injuries immediately or very soon after the collapse (42) (47).
Fourth, because co−workers in the 50 building General Hospital medical complex performed most of therescues (only two respondents were rescued exclusively by search−and−rescue teams), training should focuson co−workers for essential rescue activities. This training seems essential to the survival of coworkers, asmost residents in the collapsed building were trapped if not killed. The ways that people are entrapped areimportant to the possible training needs of co−workers.
In addition, our overall data on entrapment and rescue support the view that search−and−rescue teams (aspresently constituted) provide relatively little help in saving lives. Most of those trapped were freed beforeorganized search−and−rescue efforts could be launched. By the time the teams arrive, especially foreignteams, and have decided on methods, most survivors have been rescued. Both the relatively short duration ofentrapment and the frequency of rescue by fellow residents or other hospital personnel underscore theimportance of local resources and training. The injury list (Table 28) provides an inventory of types of injuriesthat first responders might anticipate and be trained to cope with. It also suggests the need for carefulevaluation of rescue techniques.
Fifth, the results showed that building elements and building contents clearly played a role in life safety. Thedata have clear implications for training. Building occupants can be taught to identify possible shelters as wellas hazards in the buildings they occupy. The findings also support our contention that occupants can act.These results have important implications for training (51). However, they do not clarify what specific actionshelped. We need further investigation to achieve results from which such information can be derived.
Sixth, the length of time entrapment is crucial to survivability, especially to those who are severely injured. It iscommonly accepted that twenty−four hours is the cut−off time for the survival of large numbers of trappedvictims. Because most medical residents were rescued quickly, and because 36% of our overall group oftrapped respondents were freed within two hours, and 72% within eight hours (53), our data do not helpanswer, at present, a key question: When did the people who perished begin to die? We therefore cannotconfirm or refute the twenty−four hour cut−off time for survival.
Seventh, the rapid rescues also call into question the potential role of foreign rescue teams. We know thatforeign search−and−rescue specialists do in fact rescue people. Since eighteen of our twenty−fourrespondents were trapped under five hours, and all but one under twenty−four hours, a rescue team thatarrives twenty−four hours after a collapse is not going to be effective. Consequently, foreign teams(depending on the country) may be more important as purveyors of equipment and technology rather than ofmanpower.
These findings underscore the importance of the immediate availability of stabilizing care at the collapse siteand the close proximity of definitive care. They also underscore the need to integrate medical assistance intothe search−and−rescue process, and to more effectively combine "external" and "internal" expertise andresources. The external component includes the deployment of medical personnel and technology for themost efficient and effective coverage of collapse sites. The internal component rests on improving thecapabilities of lay persons for providing detection, screening, stabilizing care and to a certain extenttransportation.
Our findings also imply increased attention on managing rescue operations, training rescuers, including laypersons, in appropriate medical care, and integrating emergency medical response and local health caresystem capabilities in light of expected injury patterns. Specific actions include developing localizedsearch−and−rescue procedures that are sensitive to the physical setting circumstances of victims, improvedlight and heavy search−and−rescue training for corporations and individuals, and improved contingencyplanning for local hospitals.
Durkin Associates is further investigating these and other heavily damaged structures to shed more light onthe previous questions. We are locating, contacting, and interviewing additional collapse survivors to developa more complete basis for survival and injury rates and their attribution. We are examining the influence ofsuch factors as occupant location, action, evacuation, damage patterns, and available resources on injury,survival, and search and rescue. Our ultimate goal is to develop a comprehensive earthquake casualtyestimation process for integration in loss estimation methods.
39

To obtain copies of this and other Durkin Associates reports write or call Michael Durkin, Michael E. Durkinand Associates, 22955 Leonora Drive, Woodland Hills, CA, 91367, (818) 704−1493.
(Copyright 1987, Michael E. Durkin, not for publication, quotation, or citation without written permission).
Acknowledgements
We are very grateful to the Director and staff of Hospital General de Mexico, especially Dr. Raúl CiceroSabido, and to Dr. Roberto Castañón of DDF for assisting this continuing research.
Our current research in Mexico City and the preparation of version 1 of this report were made possible by agrant to Michael E. Durkin and Associates from the U.S. National Science Foundation (ECE−8610890): Dr.William A. Anderson, NSF Project Manager. Subsequent data analysis and report revision were supported bythe U.S. Geological Survey (Grant Number 14−08−0001G1785): Dr. Elaine R. Padovani, USGS ProjectManager. At the time of this research, Murakami was a Visiting Scholar at the University of SouthernCalifornia and a Research Associate at Durkin Associates.
1. Principal, Michael E. Durkin and Associates Research Associate Professor, School of Architecture,University of Southern California
2. Research Epidemiologist, School of Public Health, University of California at Los Angeles
3. Jefe Del Departmento de Investigación Aplicadas, Dirección General De Servicio Médicos del DD.F.
4. Professor of Epidemiology, School of Public Health, University of California at Los Angeles
5. Research Associate, Department of Architectural Engineering, Hokkaido Hokkaido University, Sopporo,Japan
References
1. Riva, V. México a través de los siglos. México, Editorial Cumbre, 1981 Tomos II y IV Capítulos I y XI.
2. León, M. Historia de México. México, Ed. Salvat, 1978 Tomo IV pp 759−780.
3. Enciclopedia Monitor. México, Editorial Salvat, 1978 Tomo IX, pp 41764188.
4. Herrera, I. Catálogo de sismos de rnagnitud mayor o igual a 7.0 ocurridos en México en el período1974−1984. Instituto Geofísico, Universidad Nacional Autónoma de México, 1986.
5. Maraboto L. Regionalización sísmica de la República Mexicana. Rev. Sociedad Mexicana Ing. Sísmica,México, junio de 1963.
6. Comunicación del Servicio Geológico de los EEUU, Boulder, Colorado, 19 de septiembre de 1985.
7. México Earthquake, UNDRO Situation Reports Nos. 1−3, 20−22, September, 1985.
8. Comisión Metropolitana de Emergencia, Departamento del Distrito Federal, México. Informe del 19 deseptiembre al 19 de octubre de 1985: 1−6.
9. Instituto Nacional de Estadística, Geografía e Informática. Secretaría de Desarrollo Urbano y Ecología:Información estadística, sector asentamientos humanos. México, Cuaderno No. 1, 1−8.
10. Secretaría de Programación y Presupuesto: X Censo General de Población y Vivienda. México, 1980.
11. Gelman, O. Los sismos de septiembre de 1985 en la Ciudad de México. Un estudio de cave. Instituto deIngeniería UNAM. México, 1985.
40

12. Guerrero, J. y Ortega F. Consideraciones geológicas en la Ciudad de México. UNAM, Gaceta Informativa,7 octubre, 1985.
13. Comisión Metropolitana de Emergencia. Información Pública. México, D.F., 2 de octubre de 1985.
14. López Cervantes, M., López Carillo L. y Escamilla Cejudo, J.A. "Algunas consecuencias de los sismos deseptiembre de 1985 en la Ciudad de México." Salud Pública Mexicana. 28:527−536, 1986.
15. Almada, B. I. De riesgos, cicatrices y secuelas. Excelsior, México, 29 de octubre de 1985.
16. Sepulveda A., J. "Vigilancia epidemiológica posterior a los sismos de septiembre de 1985." BoletínMensual de Epidemiología. Sector salud. México, 1986: 1: 1.
17. Boraido, A.A. ''Earthquake in México." National Geographic 169: 654674, 1986.
18. Dirección General de Averiguaciones Previas. Procuraduría General de Justicia del Distrito Federal.Datos procesados pare el Departamento de Estudios Epidemiológicos de Mortalidad. Dirección deEpidemiología S.S.A. (Datos preliminares, 29 de octubre de 1985.)
19. Zeballos, J.L. Health aspects of the Mexico earthquake. Disasters 10/2/86.
20. Malilay, J. A preliminary analysis of health operations following the earthquake in Mexico City. PAHOcontract APO−MEX 018−85. January 1986.
21. Malilay, J. Comparison of morbidity patterns in two hospitals following the September 19, 1985 earthquakefield report. May 9, 1986.
22. Editorial: Las prospectivas de salud después del sismo. Jornada No. 3878, octubre 1985.
23. Rojas Enríquez, C.A. El terremoto de 1985 en el Hospital Juárez de la Ciudad de México. Secretaría deSalud, Hospital Juárez II, México D.F. mayo de 1987.
24. Cicero Sabido R., Padua Gabriell, A., Rodríguez Martínez, H. y Yáñez Villar, A. "Efectos del terremoto del19 de septiembre de 1985 en el Hospital General de la Ciudad de México, algunas consideraciones." SaludPública Mexicana 28: 521−526.
25. Comisión Interinstitucional del sector salud. Secretaría de Salud, Minuta, 1 de octubre de 1985.
26. UNFPA, Population Projection, New York, 1985.
27. Soberón, G., Carrillo, R., y Valdez, C. "La emergencia médica y las jornadas médicas asistenciales."Aspectos médicos. El Sistema Nacional de Salud y la Reconstrucción. México D.F. Editorial Porrua, 1980 pp9−22.
28. Dirección del Departamento del Distrito Federal. Informe del 22 de septiembre de 1985.
29. Secretaría de Salud, Subsecretaría de Servicios de Salud. Dirección General de Medicina Preventiva,Dirección de planeación contra accidentes y atención a la salud en caves de desastre. La experiencia deMéxico en asistencia médica y rescate a raíz de los terremotos de septiembre, 1985. México D.F. mayo de1987.
30. Cruz Vega, F. Evaluación del Centro Médico Nacional del Instituto Mexicano del Seguro Social.IMSS/Subdirección General Medica, Ciudad de México, mayo de 1987.
31. Castañón Romo, R. Procedimientos medio regales para la identificación de cadáveres. Dirección generalde servicios médicos. Departamento del Distrito Federal. México, D F., mayo, 1987.
32. Vila Sánchez, R. Daños producidos por los sismos del mes de septiembre de 1985, en el sistemahidráulico del Distrito Federal. D.D.F. Dirección general de construcción y operación hidráulica SecretaríaGeneral de Obras/Direcci6n de Operación, México, D.F. mayo de 1987.
41

33. OPS/OMS, México. Informe diario sobre la situación de vigilancia epidemiológica, 30 de septiembre de1985.
34. Estrada Vásquez, M. y Bribiesca Yáñez, R. Experiencias del dispositivo operativo implementado por elInstituto de Salud en cl Estado de México en el terremoto de 1985. ISEM, Subdirección de urgencias delEstado de México. Toluca, Estado de México, abril, 1987.
35. Comisión Interinstitucional del sector salud, Secretaría de Salud. Minuta, 28 de septiembre de 1985.
36. Frausto Pérez, G. et al. Conducta de la familia en relación a la utilización de sobres de rehidratación oraly pastillas de cloro de UNICEF en una zona de desastre en el D.F. Escuda de Salud Publica de México.Programa de especialización de enfermería en salud publica. México D.F., 1985.
37. Pacheco Regis, C; Padilla Galina, P.; López Gibson, E.; Sánchez Baez, J.J. y Gómez Espinosa, M.Desastre sísmico y crisis psicológicas. Modelo de intervención preventiva. IMSS, Subdirección GeneralMédica. Coordinación de psiquiatría y salud mental. México, D.F., mayo, 1987.
38. Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J. and Erbaugh, J.: "An Inventory Measuring Depression."Arch Gen Psychiatry 4: 561−571.
39. Brown, G.W.: Meaning, measurement and stress of life events. In Stressful Life Events: Their Nature andEffects. Ed. B.S. Dohrenwend and B.P. Dohrenwend. New York, 1974 pp 87−97.
40. Carrillo Silva, R. Ayuda internacional. Dirección de prevención contra accidentes y atención a la salud encaves de desastres, Secretaría de Salud y Asistencia. Dirección general de medicine preventiva. México,D.F., 1987.
41. Secretaría de la Contraloría General de la Federación. Informe Público, 30 de septiembre de 1985.
42. Durkin, M. E., "Injuries Resulting from Earthquake Damage," paper delivered at the 2nd InternationalEarthquake Conference − Los Angeles, CA, April 1987. (Woodland Hills: Michael E. Durkin and Associates)1987.
43. Durkin, M. E., "A Review of Architectural Methods and Their Effectiveness in Communicating HumanRequirements," Technical Report A−DA−012733 (Springfield, VA: National Technical Information Service)1975.
44. Cicero Sabido R., Padua Gabriell A., Rodríguez Martínez H., Toledo B., and Y ñez Villar A., "Efectos delterremoto del 19 de septiembre de 1985 en el Hospital General de la Ciudad de México. Algunasconsideraciones." Salud Pública Mexicana 1986; 28: 521−526.
45. Zeballos, J. L., "Emergency Medical Response During the Mexico Earthquake," in Proceedings of theSecond International Earthquake Conference (Los Angeles, CA: City of Los Angeles) 1988.
46. Durkin, Michael, "Casualities, Search and Rescue, and Response of the Health Care System," in The SanSalvador Earthquake of October 10, 1986. Earthquake Spectra, Vol. 3, No. 3, 621−639 (1987).
47. Durkin, Michael, "Earthquake Related Injuries: A Case Study." Paper presented at the Business andIndustry Council for Emergency Preparedness Planning (BICEPP) Conference on Search and Rescue forBusiness and Industry, Los Angeles, California, March 1989.
48. Durkin, Michael, "The Role of Building Evaluation in Earthquake Hazard Reduction." In W.F.E. Preiser(ed.) Building Evaluation: Advances in Methods and Applications (New York: Plenum Publishing Company)1989.
49. Durkin, Michael E., "The Role of the Physical Setting in Earthquake Damage: The México Experience −Final Progress Report," (El Cerrito, California; Earthquake Engineering Research Institute) (In press).
50. Durkin, Michael and Hitomi Ohashi, "Casualties, Survival, and Entrapment in Heavily Damaged Buildings."in Proceedings of the Ninth World Conference on Earthquake Engineering (Kyoto, Japan) 1989.
42

51. Murakami, Hitomi Ohashi, and Michael E. Durkin, "Studies of Occupant Behavior in Earthquakes −Review and Perspectives," in Proceedings of the Ninth World Conference on Earthquake Engineering (Kyoto,Japan) 1989.
52. Durkin, Michael E., "The Role of the Physical Setting in Earthquake Damage: The Mexico Experience −Third Progress Report," (El Cerrito, California: Earthquake Engineering Research Institute) May 1988.
53. Durkin, Michael E., "The Role of the Physical Setting in Earthquake Injuries: The Mexico Experience −Second Progress Report," (El Cerrito, California: Earthquake Engineering Research Institute) November1987.
43

44