Embed Size (px)
Citation preview

BritishJournal ofOphthalmology, 1991,75,633-635
Diffuse unilateral subacute neuroretinitis
Marcia D Carney, James L Combs
AbstractThe clinical syndrome of diffuse unilateralsubacute neuroretinopathy (DUSN) has beencharacterised in its early and late stages.Different types of migrating worms in thesubretinal and intraretinal space have beendescribed as the cause of the clinical syn-drome. We observed a patient with a longhistory of visual loss, vitritis, and a fundus ofabnormal appearance where the worm wasnoted to migrate to different areas over thecourse of hours.
Department ofOphthalmology, MedicalCollege of Virginia,Richmond, Virginia, USAM D CarneyJ L CombsCorrespondence to:Marcia D Carney, MD,Medical College of Virginia,Box 209, MCV Station,Richmond, Virgina 23298,USA.Accepted for publication15 March 1991
Between 1963 and 1973 thirteen patients weredescribed at Bascom Palmer with a clinicalsyndrome consisting of decreased vision, inflam-matory cells in the vitreous, optic atrophy,vascular attenuation, diffuse and focal retinalpigment epithelial atrophy, and abnormalities ofthe electroretinographic responses. This wasreferred to as the 'unilateral wipe-out' syndrome.In 1975 the earlier stages ofthe clinical syndromewere recognised as including mild optic discoedema, vitritis, extensive pigment epithelialchanges, and yellow-white lesions affecting thedeep retina. In 1978 Gass and Scelfo' describedlater stages of the disease characterised by optic
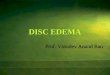
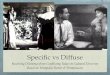
Figure I Left optic disc with nematode in the deep retina (arrow) on 25 November 1987, one
disc diameterfrom the disc, in a dumbbell configuration, along a branch ofthe inferonasalartery.
atrophy, vascular attenuation, arterial sheath-ing, and diffuse retinal pigment epithelialchanges with focal and course mottling of thepigment epithelium and atrophy. With markedinflammatory disease of the retina and opticnerve, the syndrome was named 'diffuse uni-lateral subacute neuroretinitis.'
Gass et all in 1978 reported 37 more cases. Itwas suggested from the newer observations thatthe syndrome may be related to toxic damage tothe optic nerve and retina caused by a wormmigrating in the subretinal space. Gass et alemphasised the early or subacute stage and theappearance of 'successive crops of evanescentlesions', either grey-white or yellow-white,involving the deep layers of the retina. Theselesions would fade in several days, leaving colourchanges in underlying pigment epithelium. Intwo of these patients a motile subretinal wormwas noted close to active retinal lesions.2 Thechanges in the pigment epithelium produced adull-reflex which was similar to changes noted ina diffuse tapetoretinal degeneration.The electroretinogram (ERG) was normal in
two patients in the early stages of the disease.2 Inthe late stages there was more B-wave reductionthan A-wave reduction. The ERG was notextinguished in any of the patients.2 Electro-oculograms were abnormal in 16 of 29 per-formed.2 It has been suggested that thisuniocular syndrome may be caused by severalnematodes, with Baylisascaris procyonis, theraccoon roundworm, being one possible cause.35
Case reportA 22-year-old Liberian woman presented to theOphthalmology Office of the Medical College ofVirginia on 13 August 1987 complaining chieflyof decreased vision in the left eye. Before leavingLiberia in 1979 she was seen by an ophthalmolo-gist. At that time she complained of nyctalopiaand decreased vision in the left eye. The condi-tion was essentially stable until two months priorto her visit to the Medical College of Virginia, atwhich time she noted a further decrease in thevisual acuity of the left eye and intermittentmicropsia. Her past eye history was otherwisenormal. Her seven siblings had no history ofnyctalopia or known tapetoretinal degeneration.On examination she was found to have a visual
acuity of 20/20 in the right eye and 20/50 in theaffected left eye. There was an afferent pupillarydefect in the left eye. The intraocular pressureswere normal. There was pallor of the left opticdisc, with marked arteriolar attenuation anddiffuse patchy retinal pigment epithelial changeswithout overt bony spicule changes; a decreasedmacular reflex was present.The patient was examined by the Neuro-
ophthalmology Service on 9 September 1987.Her visual acuity had decreased to 15/200 in the
633
on January 27, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.10.633 on 1 October 1991. D
ownloaded from

634
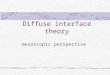
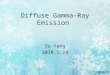
Figure 2 At 1130 the worm (small arrow) has moved nasally, located in the inner retinasuperonasal to the fovea (large arrow). Note the tail ofthe worm overlies the vessel.
left eye. Colour discrimination was absent in theleft eye and normal in the right eye. The funduswas decribed 'as that of a unilateral retinitispigmentosa'. The right eye yielded visual evokedpotential (VEP) and ERG. An absent pattern
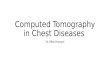
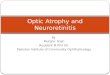
Figure 3 At 1400 the worm (small arrow) was located inferotemporal to the optic disc margin.
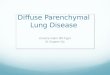
VEP response was present on the left; the flashVEP response was present. On the left the ERGwas absent to photopic stimuli with reducedscotopic A and B waves. On 25 November 1987while she was being examined, a motile wormwas seen inferonasal to the optic disc (Fig 1).It was approximately 800 [tm in length andapproximately 33 [m in width. The patientreturned on 1 December 1987 for follow-up, andthe location of the worm was followed for severalhours. At 1000 h the worm was seen coiled in thesuperotemporal macula. At 1130 it had movednasally in the superior macula (Fig 2). At 1400the worm was noted to be inferotemporal to theoptic disc margin (Fig 3). At 1600 it had movedback into the superior macular area (Fig 4).Light stimulation was used at 1630 to move theworm further into the superior macula area,where photocoagulation was applied.The patient returned on 2 January 1988. Her
visual acuity remained 20/400. No other para-sites were noted. The area of laser photocoagula-tion involving the worm showed evidence ofchorioretinal scarring.
DiscussionFurther observations"'4 have supported those ofGass et a12 that the clinical syndrome of diffuseunilateral subacute neuroretinitis (DUSN) iscaused by a nematode. It was initially suggestedthat this syndrome was caused by Toxocaracanis.2 However, evidence has been presentedwhich supports that there are nematodes of twodifferent sizes or nematodes at two differentstages of development. Gass and Braunstein3 onexamining 18 patients noted that in 12 thenematode measured 400 to 1000 iim in length; inthe other six patients they measured 1500 to 2000lim. The majority of patients with the smallernematodes were residing in the south-easternUnited States, whereas most of those with thelarger nematodes resided in the northern mid-western United States.Our patient was born in Liberia and moved to
the south-eastern United States in 1979. It is note-worthy that her diagnosis of DUSN is suggestedprior to her moving from Liberia when, in 1979,at about the age of 14, she was given the diagnosisby an ophthalmologist of a 'circulation problem'ofunknown aetiology. There are no other knownreports from Africa characterising the size andpossible types of nematodes that may cause thissyndrome. The worm's size in our patient,approximately 800 tim in length, is within thesize category (400-1000 [tm) of the nematodefound mainly in the south-eastern United States.Like several of the reported patients of Gass etall who had reductions in the A or B wave ofthe electroretinogram, or both, our patient'sscotopic electroretinogram had reduced A and Bwaves and an extinguished photopic ERG.
Kazacos et all have made further experimentalobservations in animals giving support to thepossible cause of diffuse unilateral subacuteneuroretinitis. Infection by Baylisascarisprocyonis, the raccoon roundworm, parallels thehuman infection by Toxocara canis in that it isacquired by ingestion of soil containing raccoonova. The larvae of this parasite are larger than
Carney, Combs
on January 27, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.10.633 on 1 October 1991. D
ownloaded from

635Diffuse unilateral subacute neuroretinitis
Figure 4 At 1600 the worm (small arrow) has moved back superotemporal to the fovea (largearrow) beneath the superotemporal artery.
those of Toxocara canis, which average about400Om.7 8 Although infection by nematodes of at
least two different sizes has been suggested byGass et al,2 Kazacos et all suggest that DUSN is
probably caused by a variety of nematode speciesincluding Toxocara species,2 3 6 Baylisascarisprocyonis, and other larvae not yet identified.With the report of exposure to a pet raccoon
prior to the onset of visual symptoms in the
patient reported by Raymond et al9 and with the
more recent reports' " of its zoonotic potential,B. procyonis has been suggested as one of the
possible causes of the ocular larva migranssyndrome and DUSN.412 Kazacos et al5 have
suggested that indeed the two sizes of worms
reported by Gass and Braunstein3 are not incon-sistent with the growth range of baylisascaris ininfected animals and humans,'"I 15 16 which maycause many cases of DUSN.
John et all3 have studied the choroidal andretinal response to ascarid-infected eyes in
guinea pigs. A closer antigenic relationship existsbetween baylisascaris and ascaris than betweeneither parasite and toxocara.'3 With intravitrealinjection ofAscarid suum into guinea pig eyes theresulting response was a diffuse eosinophilicchoroiditis, neuroretinal degeneration, andretinal pigment epithelial changes.'3 IntraocularIgE antibody production and mass cell degenera-tion may lead to the release of a number ofeosinophil chemotaxins (eosinophil chemotacticfactor of anaphylaxis, histamine). After antigen-
antibody complement activation, the focalrelease of other diffusible eosinophilotacticfactors may lead to alterations in the chorioca-pillaris which contribute to a more generalisedand progressive retinal degeneration distantfrom sites of DUSN. This is probably caused bya number of intraocular nematodes producing a
clinical syndrome of decreased visual acuity,anterior uveitis, vitritis, optic disc oedema, andlater optic disc atrophy. Diffuse retinal pigmentepithelial changes and probable outer and innerretinal damage are suggested by changes in theelectro-oculogram and the A and B waves of theelectroretinogram.The worm may cause destructive changes and,
as in our patient, lie dormant for years, only to
cause further decrease in visual acuity later. Liketoxocara, an enzyme-linked immunosorbentassay may soon be available for the diagnosis ofBaylisascaris procyonis larva migrans or DUSN.'4Regardless of the type of nematode causing thesyndrome, this diagnosis must be considered bythe ophthalmologist when patients present withunilateral visual loss of unknown aetiology,particularly when they are young, healthy adultsin whom the diagnosis of a 'unilateral retinitispigmentosa' is considered.
This work was supported in part by a grant from Research toPrevent Blindness, Inc.
1 Gass JDM, Scelfo R. Diffuse unilateral subacute neuroretini-tis.J'RSocMed 1978; 71: 95-111.
2 Gass JDM, Gilbert WR, Guerry RK, Scelfo R. Diffuseunilateral subacute neuroretinitis. Ophthalmology 1978; 85:521-45.
3 Gass JDM, Braunstein RA. Further observations concerningthe diffuse unilateral subacute neuroretinitis syndrome.Arch Ophthalmol 1983; 101: 1689-97.
4 Kazacos KR, Vestre WA, Kazacos EA, Raymond LA. Diffuseunilateral subacute neuroretinitis syndrome: probablecause. Arch Ophthalmol 1984; 102: 967-8.
5 Kazacos KR, Raymond LA, Kazacos EA, Vestre WA. Theraccoon ascarid: a probable cause of human ocular migrans.Ophthalmology 1985; 92: 1735-44.
6 Oppenheim S, Rogell G, Peyser R. Diffuse unilateral subacuteneuroretinitis. Ann Ophthalmol 1985; 17: 336-8.
7 Nichols RL. The etiology of visceral larva migrans. Diagnosticmorphology of infective second-stage toxocara larvae.J7Parasitol 1956; 42: 349-62.
8 Arean VM, Crandall CA. Toxocariasis. In: Marcial-Rojas RA,ed. Pathology ofprotozoal and helminthic diseases, with clinicalcorrelation. Baltimore: Williams and Wilkins, 1971: 808-42.
9 Raymond LA, Gutierrez Y, Strong LE, Wander AH, Buten R,Cordan D. Living retinal nematodes (filarial-like) destroyedwith photocoagulation. Ophthalmology 1978; 85: 944-9.
10 Huff DS, Neafie RC, Binder MJ, DeLeon GA, Brown LW,Kazacos KR. The first fatal baylisascaris infection inhumans: an infant with eosinophilic meningoencephalitis.PediatrPathol 1984; 2: 345-52.
11 Fox AS, Kazacos KR, Gould NS, Heydemann PT, Thomas C,Boyer KM. Fatal eosinophilic meningoencephalitis andvisceral larva migrans caused by the raccoon ascarid,Baylisascaris procyonis. NEnglJMed 1985; 312: 1619-23.
12 Kazacos KR, Vestre WA, Kazacos EA. Raccoon ascarid larvae(Baylisascaris procyonis) as a cause of ocular larva migrans.Invest Ophthalmol VisSci 1984; 25: 1177-83.
13 John J, Barsky HJ, Donnelly JJ, Rockey JH. Retinal pigmentepitheliopathy and neuroretinal degeneration in ascarid-infected eyes. Invest Ophthalmol Vis Sci 1987; 28: 1583-98.
14 Little AS, Kazacos KR. Enzyme-linked immunosorbent assayfor diagnosis of baylisascaris larva migrans. Proc Am AssocVet Parasitol 1984; 29: 16-7.
15 Reed WM, Kazacos KR, Dhillon AS, Winterfield RW,Thacker HL. Cerebrospinal Nematodiasis in Bobwhitequail. Avian Dis 1981; 25: 1039-46.
16 Kazacos KR, Wirtz WL, Burger DP, Christmas CS. Raccoonascarid larvae as a cause of fatal central nervous systemdisease in subhuman primates. J Am Vet Med Assoc 1981;179: 1089-94.
on January 27, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.10.633 on 1 October 1991. D
ownloaded from