Embed Size (px)
Citation preview

Slide 1
5,05
4,10
3,50
4,72
11,82 11,82
Diabetes Seminar EASD 2015
Carnegie
Mads Krogsgaard Thomsen
Chief Science Officer
Mexico City – part of Cities Changing Diabetes
Slide 2
5,05
4,10
3,50
4,72
11,82 11,82
Forward-looking statements
Novo Nordisk’s reports filed with or furnished to the US Securities and Exchange Commission (SEC), including this document as well as the company’s Annual Report 2013 and Form 20-F, both filed with the SEC in February 2014, and written information released, or oral statements made, to the public in the future by or on behalf of Novo Nordisk, may contain forward-looking statements. Words such as ‘believe’, ‘expect’, ‘may’, ‘will’, ‘plan’, ‘strategy’, ‘prospect’, ‘foresee’, ‘estimate’, ‘project’, ‘anticipate’, ‘can’, ‘intend’, ‘target’ and other words and terms of similar meaning in connection with any discussion of future operating or financial performance identify forward-looking statements. Examples of such forward-looking statements include, but are not limited to:
• Statements of targets, plans, objectives or goals for future operations, including those related to Novo Nordisk’s products, product research, product development, product introductions and product approvals as well as cooperation in relation thereto
• Statements containing projections of or targets for revenues, costs, income (or loss), earnings per share, capital expenditures, dividends, capital structure, net financials and other financial measures
• Statements regarding future economic performance, future actions and outcome of contingencies such as legal proceedings, and
• Statements regarding the assumptions underlying or relating to such statements.
These statements are based on current plans, estimates and projections. By their very nature, forward-looking statements involve inherent risks and uncertainties, both general and specific. Novo Nordisk cautions that a number of important factors, including those described in this document, could cause actual results to differ materially from those contemplated in any forward-looking statements.
Factors that may affect future results include, but are not limited to, global as well as local political and economic conditions, including interest rate and currency exchange rate fluctuations, delay or failure of projects related to research and/or development, unplanned loss of patents, interruptions of supplies and production, product recall, unexpected contract breaches or terminations, government-mandated or market-driven price decreases for Novo Nordisk’s products, introduction of competing products, reliance on information technology, Novo Nordisk’s ability to successfully market current and new products, exposure to product liability and legal proceedings and investigations, changes in governmental laws and related interpretation thereof, including on reimbursement, intellectual property protection and regulatory controls on testing, approval, manufacturing and marketing, perceived or actual failure to adhere to ethical marketing practices, investments in and divestitures of domestic and foreign companies, unexpected growth in costs and expenses, failure to recruit and retain the right employees, and failure to maintain a culture of compliance.
Please also refer to the overview of risk factors in ‘Risks to be aware of’ on p 42-43 of the Annual Report 2013 on the company’s website novonordisk.com.
Unless required by law, Novo Nordisk is under no duty and undertakes no obligation to update or revise any forward-looking statement after the distribution of this document, whether as a result of new information, future events or otherwise.
Important drug information
• Victoza® (liraglutide 1.2 mg & 1.8 mg) is approved for the management of type 2 diabetes only
• Saxenda® is the intended brand name for liraglutide 3 mg for the treatment of obesity
Investor presentation Carnegie Seminar EASD 2015

5,05
4,10
3,50
4,72
11,82 11,82
Slide 3
Novo Nordisk works with four strategic focus areas based on five core capabilities
Core capabilities
Expand leadership
Expand leadership in DIABETES
Pursue leadership in HAEMOPHILIA
Establish presence in OBESITY
Expand leadership in GROWTH DISORDERS
Strategic focus areas
Investor presentation Carnegie Seminar EASD 2015
Novo Nordisk Way and the Triple Bottom Line business principle
Engineering, formulating, developing and delivering protein- based treatments
Deep disease under- standing
Efficient large-scale production of proteins
Building and maintaining a leading position in emerging markets
Planning and executing global launches of new products

5,05
4,10
3,50
4,72
11,82 11,82
Slide 4
SUBCUTANEOUS DELIVERY
INTRAVENOUS INFUSION
ORAL PROTEIN DELIVERY
Novo Nordisk core capabilities
90 years of innovation based on core capabilities within therapeutic proteins, coupled with disease insight
YEAST
E. COLI
MAMMALIAN CELLS
ACYLATION
AMINO ACID SUBSTITUTION
OTHER MODIFICATION
THERAPY AREA EXPERTISE
MEDICAL INSIGHT
TRIAL DESIGN AND EXECUTION PREFILLED PENS
DURABLE PENS
Investor presentation Carnegie Seminar EASD 2015
5,05
4,10
3,50
4,72
11,82 11,82
Slide 5
OR
Optimisation
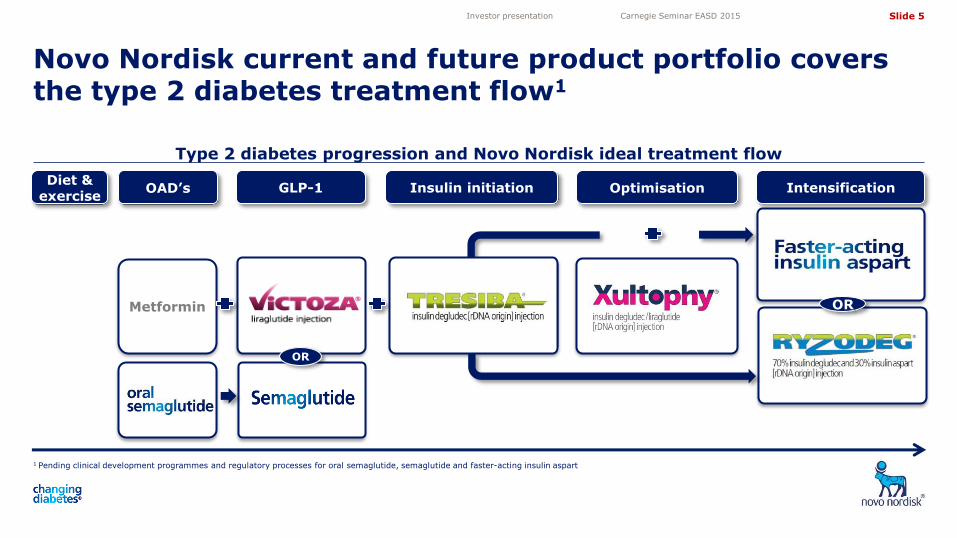
Type 2 diabetes progression and Novo Nordisk ideal treatment flow
1 Pending clinical development programmes and regulatory processes for oral semaglutide, semaglutide and faster-acting insulin aspart
Novo Nordisk current and future product portfolio covers the type 2 diabetes treatment flow1
Investor presentation Carnegie Seminar EASD 2015
Metformin
OAD’s GLP-1 Insulin initiation Intensification
OR
Diet & exercise
5,05
4,10
3,50
4,72
11,82 11,82
Slide 6
OR
Optimisation
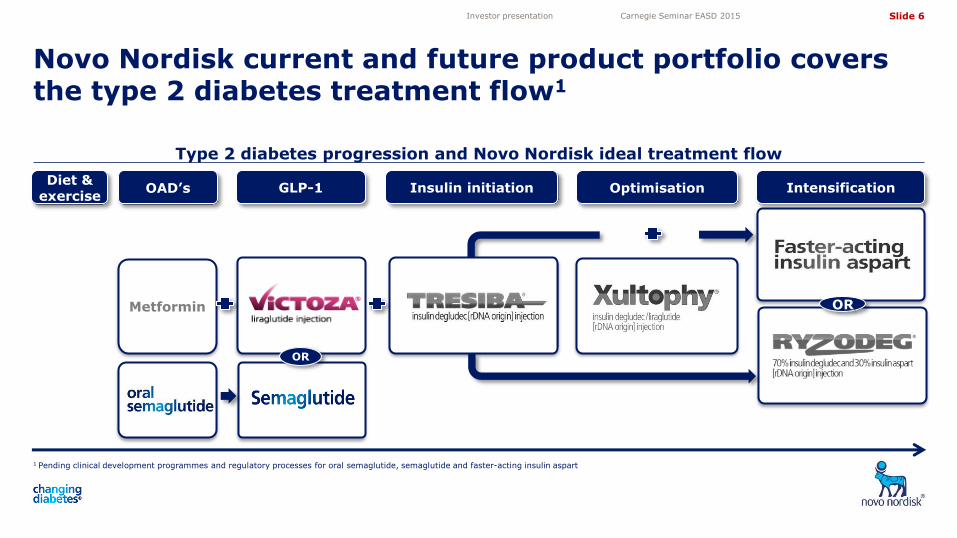
Type 2 diabetes progression and Novo Nordisk ideal treatment flow
1 Pending clinical development programmes and regulatory processes for oral semaglutide, semaglutide and faster-acting insulin aspart
Novo Nordisk current and future product portfolio covers the type 2 diabetes treatment flow1
Investor presentation Carnegie Seminar EASD 2015
Metformin
OAD’s GLP-1 Insulin initiation Intensification
OR
Diet & exercise

5,05
4,10
3,50
4,72
11,82 11,82
Slide 7
Comparison of HbA1c and weight lowering effect of marketed GLP-1 analogues
* p < 0.05; BID: twice daily; QD: once daily; QW: once weekly. Source: Competitive Intelligence, June 2014, from AWARD-6: Dungan et al, Lancet 2014, HARMONY-7: Pratley et al, Lancet Diabetes Endocrinol 2014, DURATION-6: Buse et al, Lancet 2012; LEAD-6: Buse et al, Lancet 2009
Victoza® is the market leader in the GLP-1 segment due to superior efficacy on glycaemic control and weight loss
Investor presentation Carnegie Seminar EASD 2015
-1.1
-1.5
-1.0
-1.4
-0.8
-1.3
-0.8
-1.4
-1.6
-1.4
-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
Change in HbA1c (%)
-3.2
-3.6
-2.2
-3.6
-2.9 -2.7
-0.6
-2.9
-4.0
-3.5
-3.0
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
Liraglutide 1.8 mg QD Dulaglutide QW Exenatide BID Exenatide QW Albiglutide QW
LEAD-6 DURATION-6 AWARD-6 HARMONY-7
Change in weight (kg) LEAD-6 DURATION-6 AWARD-6 HARMONY-7
*
*
*
Non-inferior
non- significant *
*
*
5,05
4,10
3,50
4,72
11,82 11,82
Slide 8
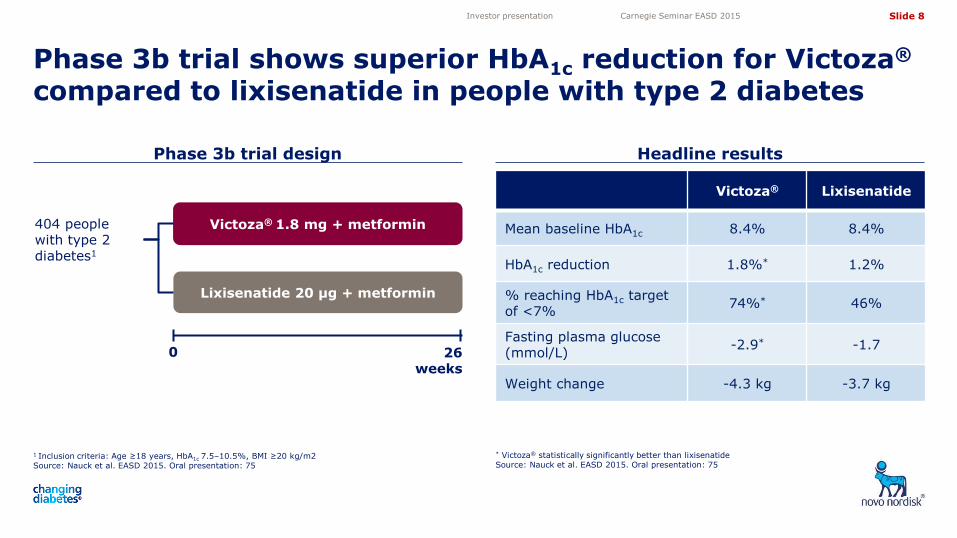
1 Inclusion criteria: Age ≥18 years, HbA1c 7.5–10.5%, BMI ≥20 kg/m2 Source: Nauck et al. EASD 2015. Oral presentation: 75
Headline results
Phase 3b trial shows superior HbA1c reduction for Victoza® compared to lixisenatide in people with type 2 diabetes
* Victoza® statistically significantly better than lixisenatide Source: Nauck et al. EASD 2015. Oral presentation: 75
Phase 3b trial design
Lixisenatide 20 µg + metformin
Victoza® 1.8 mg + metformin
0
404 people with type 2 diabetes1
26 weeks
Victoza® Lixisenatide
Mean baseline HbA1c 8.4% 8.4%
HbA1c reduction 1.8%* 1.2%
% reaching HbA1c target of <7%
74%* 46%
Fasting plasma glucose (mmol/L)
-2.9* -1.7
Weight change -4.3 kg -3.7 kg
Investor presentation Carnegie Seminar EASD 2015

Slide 9
5,05
4,10
3,50
4,72
11,82 11,82
SUSTAIN 1 trial design Headline results
0.5 mg
semaglutide 1.0 mg
semaglutide Placebo
Change in HbA1c (8.1% baseline)
-1.5%* -1.6%* 0.0%
Proportion of patients reaching HbA1c target of <7%
74%* 73%* 25%
Change in body weight (92 kg baseline)
-3.8 kg* -4.6 kg* -1.0 kg
Discontinuation rate due to adverse events
6% 5% 2%
Semaglutide shows superior HbA1c reduction and weight loss compared with placebo in SUSTAIN 1 trial
1 Inclusion criteria: Type 2 diabetes, treated with diet and exercise at least 30 days before screening, HbA1c 7.0-10.0% (53 - 86 mmol/mol) (both inclusive) Source: Novo Nordisk data on file (NN9535-3623)
*Statistically significantly greater compared to placebo Source: Novo Nordisk data on file (NN9535-3623)
Investor presentation Carnegie Seminar EASD 2015
Placebo
Semaglutide 0.5 mg
0 30 weeks
388 drug-naïve people with type 2 diabetes1
Semaglutide 1.0 mg

5,05
4,10
3,50
4,72
11,82 11,82
Slide 10
Source: Novo Nordisk data on file (NN9924-3790)
Phase 2 headline results PIONEER Phase 3a trial design
Phase 3a trials to be initiated with oral semaglutide following positive results for phase 2 trial
QD: once daily
Investor presentation Carnegie Seminar EASD 2015
• From a baseline HbA1c of 7.9% people achieved the following improvements:
• Oral semaglutide: 0.7% to 1.9% (dose dependent) • Sc semaglutide: 1.9% • Oral placebo: 0.3%
• From a baseline of 92 kg people experienced a
comparable weight loss of 6.5 kg with subcutaneous and the highest doses of oral semaglutide versus 1 kg for placebo
• Semaglutide appeared to have a safe and well-tolerated
profile; the most common adverse events were transient nausea and vomiting
• 6 efficacy and safety trials • 1 event-driven cardiovascular outcome trial • ~8,000 patients
• Three doses to be investigated: • 3 mg (QD) • 7 mg (QD) • 14 mg (QD)
• First trial to be initiated in Q1 2016, investigating three doses of once-daily oral semgalutide vs 100 mg sitagliptin
• Remaining trials all to be initiated during 2016
• Investment of 2 billion USD in new production facilities

5,05
4,10
3,50
4,72
11,82 11,82
Slide 11
OR
Optimisation
Type 2 diabetes progression and Novo Nordisk ideal treatment flow
1 Pending clinical development programmes and regulatory processes for oral semaglutide, semaglutide and faster-acting insulin aspart
Novo Nordisk current and future product portfolio covers the type 2 diabetes treatment flow1
Investor presentation Carnegie Seminar EASD 2015
Metformin
OAD’s GLP-1 Insulin initiation Intensification
OR
Diet & exercise

5,05
4,10
3,50
4,72
11,82 11,82
Slide 12
Clinical data demonstrate predictable profile with very low variability
Tresiba® QD vs insulin glargine QD results from BEGIN phase 3a trial
Clinical data demonstrate stable and efficacious profile of Tresiba®
Source: Heise et al. EASD 2010: Poster 971
QD: once daily
1Based on Novo Nordisk data on file (NN1250-3579, NN1250-3586, NN1250-3668, NN1250-3672, NN1250-3770, NN1250-3582 and NN1250-3583)
Investor presentation Carnegie Seminar EASD 2015
Glucose infusion rate (GIR) (mg/kg/min)
Time (hours)
Increasing risk of hypoglycaemia
Optimal glycaemic
control
Increasing risk of hyperglycaemia
0 4 16 20 24 8 12
• Dosing flexibility and superior pen
• Injection volume (U200) – one injection for all Conve- nience
• Lower rate of overall hypoglycaemia
• Lower rate of nocturnal hypoglycaemia Safety
• Improved fasting glucose control
• Less impact of missed dose Efficacy
• Basal insulin with flatter, less variable profile and a doubling in half-life Profile
Degludec Insulin glargine

5,05
4,10
3,50
4,72
11,82 11,82
Slide 13
OR
Optimisation
Type 2 diabetes progression and Novo Nordisk ideal treatment flow
1 Pending clinical development programmes and regulatory processes for oral semaglutide, semaglutide and faster-acting insulin aspart
Novo Nordisk current and future product portfolio covers the type 2 diabetes treatment flow1
Investor presentation Carnegie Seminar EASD 2015
Metformin
OAD’s GLP-1 Insulin initiation Intensification
OR
Diet & exercise

5,05
4,10
3,50
4,72
11,82 11,82
Slide 14
DUALTM V trial design Headline results
People inadequately controlled on insulin glargine benefit from switching to Xultophy® in phase 3b trial
Insulin glargine + metformin
Xultophy® + metformin
0
1:1 randomisation Primary end-point: HbA1c reduction
557 people with type 2 diabetes, currently on insulin glargine + metformin1
* Xultophy® statistically significantly better than insulin glargine Source: Buse et al. EASD 2015. Poster number: 836
1 Inclusion criteria: Type 2 diabetes, 7.0% ≤ HbA1c ≤ 10.0%, BMI ≤ 40 kg/m2, age ≥ 18 years and insulin glargine dose 20-50 units Source: Buse et al. EASD 2015. Poster number: 836
Xultophy® Insulin glargine
Baseline HbA1c 8.4% 8.2%
HbA1c reduction 1.8%* 1.1%
% reaching HbA1c target of 7%
72%* 47%
Weight change -1.4 kg* +1.8 kg
Confirmed and nocturnal hypoglycaemia
-57%*
-83%* n/a 26
weeks
Investor presentation Carnegie Seminar EASD 2015

5,05
4,10
3,50
4,72
11,82 11,82
Slide 15
Xultophy® key clinical results
Note: Typical confirmed hypoglycaemia event rates for treatment with basal insulin are 142-369 episodes per 100 PYE (based on insulin glargine event rates from trials NN1250-3586, 3579 and 3672) where the FPG target and hypoglycaemia definition is similar to the DUAL trials Source: Novo Nordisk Trial IDs: DUAL® I (NN9068-3697), DUAL® II (NN9068-3912), DUAL® III (NN9068-3851), DUAL® IV (NN9068-3951), DUAL® V (NN9068-3952)
Xultophy® has documented strong efficacy across the treatment cascade
Investor presentation Carnegie Seminar EASD 2015
DUAL® I Add-on to
metformin ± Pio n = 833
DUAL® II Add-on to
metformin ± basal insulin
n = 199
DUAL® III Switch from GLP-1
n = 292
DUAL® IV Add-on to SU ±
metformin n = 289
DUAL® V Switch from insulin
glargine n = 557
Mean trial start HbA1c (%) 8.3 8.7 7.8 7.9 8.4
HbA1c change (%) -1.9 -1.9 -1.3 -1.4 -1.8
% to target < 7% (%) 80.6 60.3 75.3 79.2 71.6
% to target < 6.5% (%) 69.7 45.2 63.0 64.0 55.4
Confirmed hypoglycaemia (episodes per 100 PYE)
180.2 153.4 282 351.7 343.3
Weight change (kg) -0.5 -2.7 +2.0 +0.5 -1.4

5,05
4,10
3,50
4,72
11,82 11,82
Slide 16
OR
Optimisation
Type 2 diabetes progression and Novo Nordisk ideal treatment flow
1 Pending clinical development programmes and regulatory processes for oral semaglutide, semaglutide and faster-acting insulin aspart
Novo Nordisk current and future product portfolio covers the type 2 diabetes treatment flow1
Investor presentation Carnegie Seminar EASD 2015
Metformin
OAD’s GLP-1 Insulin initiation Intensification
OR
Diet & exercise

Slide 17
5,05
4,10
3,50
4,72
11,82 11,82
-2
0
2
4
6
8
-60 0 60 120 180 240
Faster-acting insulin aspart shows higher plasma glucose reduction in meal test
Greater glucose-lowering after meal with faster-acting insulin aspart
Faster-acting insulin aspart shows higher prandial glucose reduction in phase 1 trial
Source: Bode et al EASD 2015. Oral presentation: 39
* p<0.05
Source: Bode et al EASD 2015. Oral presentation: 39
Faster-acting insulin aspart vs insulin aspart
Change in plasma glucose following meal test after 14 days
ΔPGav,0–1h, mmol/L –0.50 [–1.07; 0.07]
ΔPGav,0–2h, mmol/L –0.99* [–1.95; –0.03]
Baselin
e a
dju
ste
d p
lasm
a
glu
co
se (
mm
ol/
L)
Nominal time (min)
Insulin aspart Faster-acting insulin aspart
Investor presentation Carnegie Seminar EASD 2015
5,05
4,10
3,50
4,72
11,82 11,82
Slide 18
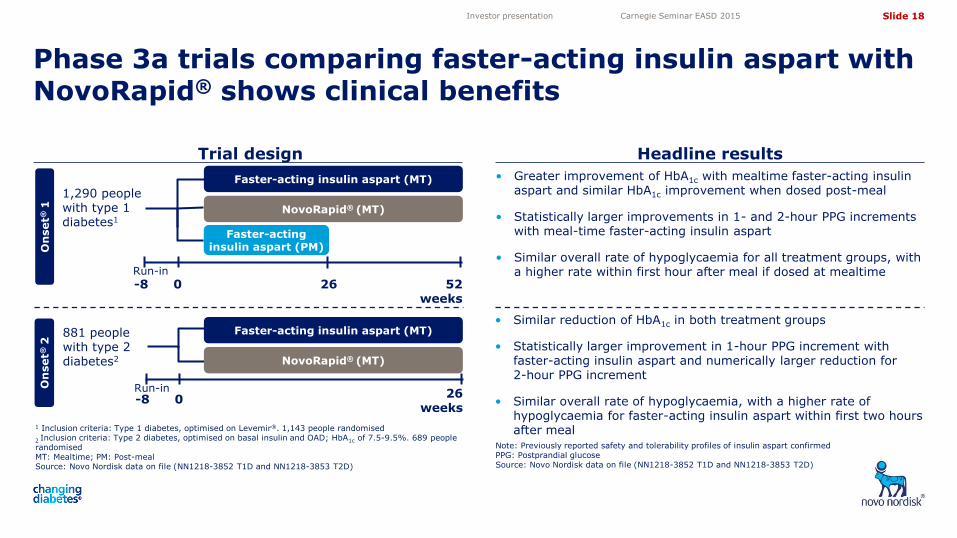
• Greater improvement of HbA1c with mealtime faster-acting insulin aspart and similar HbA1c improvement when dosed post-meal
• Statistically larger improvements in 1- and 2-hour PPG increments with meal-time faster-acting insulin aspart
• Similar overall rate of hypoglycaemia for all treatment groups, with a higher rate within first hour after meal if dosed at mealtime
1 Inclusion criteria: Type 1 diabetes, optimised on Levemir®. 1,143 people randomised
2 Inclusion criteria: Type 2 diabetes, optimised on basal insulin and OAD; HbA1c of 7.5-9.5%. 689 people randomised MT: Mealtime; PM: Post-meal Source: Novo Nordisk data on file (NN1218-3852 T1D and NN1218-3853 T2D)
Trial design Headline results
Phase 3a trials comparing faster-acting insulin aspart with NovoRapid® shows clinical benefits
Note: Previously reported safety and tolerability profiles of insulin aspart confirmed PPG: Postprandial glucose Source: Novo Nordisk data on file (NN1218-3852 T1D and NN1218-3853 T2D)
881 people with type 2 diabetes2
Faster-acting insulin aspart (MT)
NovoRapid® (MT)
-8 0 Run-in 26
weeks
Faster-acting insulin aspart (PM)
Faster-acting insulin aspart (MT)
1,290 people with type 1 diabetes1
52 weeks
NovoRapid® (MT)
26
-8 0 Run-in
• Similar reduction of HbA1c in both treatment groups
• Statistically larger improvement in 1-hour PPG increment with faster-acting insulin aspart and numerically larger reduction for 2-hour PPG increment
• Similar overall rate of hypoglycaemia, with a higher rate of hypoglycaemia for faster-acting insulin aspart within first two hours after meal
On
set®
1
On
set®
2
Investor presentation Carnegie Seminar EASD 2015

Slide 19
5,05
4,10
3,50
4,72
11,82 11,82
NovoEight®
NovoSeven®
NovoThirteen®/TRETTEN®
Norditropin®
Significant growth opportunities fuelled by strong R&D pipeline across all four strategic focus areas
1 Phase 2a proof-of-principle trial initiated in June 2015 2 Phase 3 initiated in adult growth hormone disorder 3 Approved in all triad markets (US, EU and Japan), unless noted 4 Approved in the US on 23 Dec 2014 and EU 23 Mar 2015
Investor presentation Carnegie Seminar EASD 2015
Saxenda® (US/EU4)
Semaglutide – QW GLP-1
Faster-acting insulin aspart OI338GT – Oral insulin1 OG987GT – Oral GLP-1
OG217SC – Oral GLP-1
LATIN – Type 1 diabetes
OG987SC – Oral GLP-1
LAI287 – QW basal insulin
PHASE 1 PHASE 2 PHASE 3 SUBMITTED APPROVED3
NovoRapid®
NovoMix®
Victoza®
Levemir®
NN8640 – Once-weekly GH2
NN7415 – Concizumab
N8-GP – Long-acting rFVIII
N9-GP – Long-acting rFIX
Tresiba® (EU/Japan)
Ryzodeg® (EU/Japan)
Diabetes
Obesity
Haemophilia
Growth disorders
Xultophy® (EU) G530L – Glucagon analogue
LAI338 – QD basal insulin
NN9838 – Amylin analogue
OI320GT – Oral insulin

5,05
4,10
3,50
4,72
11,82 11,82
Slide 20
Significant news flow from late-stage diabetes and obesity pipeline
Investor presentation Carnegie Seminar EASD 2015
Project Past 6 months Past 3 months Within 3 months In ~3-6 months
Oral GLP-1 Phase 2
Faster-acting insulin aspart
LATIN T1D ADJUNCT TWO
Results available
In ~6-9 months
Semaglutide
SUSTAIN® 1
SUSTAIN® 3
SUSTAIN® 2
SUSTAIN® 4
SUSTAIN® 5
Victoza®
SUSTAIN® 6
LEADER®
Saxenda® SCALE® ext. data
ONSET® 1 √
ONSET® 2 √
√
Tresiba® SWITCH 1
SWITCH 2
√
√
√
Note: Indicated timeline as of financial release of first six months of 2015 on 06 August
ADJUNCT ONE √

5,05
4,10
3,50
4,72
11,82 11,82
Slide 21
Share information Investor Relations contacts
Investor contact information
Novo Nordisk’s B shares are listed on the stock exchange in Copenhagen under the symbol ‘NOVO B’. Its ADRs are listed on the New York Stock Exchange under the symbol ‘NVO’. For further company information, visit Novo Nordisk on the internet at: novonordisk.com
Peter Hugreffe Ankersen +45 3075 9085 [email protected]
Daniel Bohsen +45 3079 6376 [email protected]
Melanie Raouzeos +45 3075 3479 [email protected]
Kasper Veje +45 3079 8519 [email protected]
In North America:
Frank Daniel Mersebach
+1 609 235 8567
Novo Nordisk A/S Investor Relations Novo Allé, DK-2880 Bagsværd
29 Oct 2015 Financial statement for the first nine months of 2015
03 Feb 2016 Financial statement for 2015
Upcoming events
Investor presentation Carnegie Seminar EASD 2015






![Programme & Abstract Book · 2019. 5. 20. · 4 7TH MEETING OF EASD STUDY GROUP ON GENETICS OF DIABETES [EASD-SGGD] EASD-SGGD Steering Committee Emma Ahlqvist Lund University Diabetes](https://img.pdfslide.us/doc/110x75/6013bf33b6f6720c7341b1d8/programme-abstract-book-2019-5-20-4-7th-meeting-of-easd-study-group-on.jpg)






















