Embed Size (px)
Citation preview

DHFPresentations 2004 to 2008
+44(0)1423 506 848+44(0)789 907 4881
www.directhealthfirst.comKent House42 Duchy Rd HarrogateHG1 2ER

Non ApprovedColleges RCs
Specialist Specialist RegistrationRegistration
UKGraduates
EUGraduates
ApprovedColleges
NewProvider Bid
NCSC
TCTC
GM
C FullFull RegistrationRegistration
SurgeryTraining with Supervision
GMC

Performance Management & KPIs
KPIs
SUIs
Outcome measures
DHF

CSS v CPS
The CSS contains everything that should help us specify our procurement safely for the NHS
The CPS only contains that which we consider essential to the ITT and which will deliver a VFM bid

Input and process specifications
So the sponsor can integrate ISTC care with the rest of the health economy.· e.g. what is expected from the provider may differ between one
cholecystectomy package (with a very limited follow up) and another.

When things go wrong
Difficult to justify protocols which are contrary to UK best practice (without evidence base) which leads to unnecessary conflict with national standards organisations· when (not if) there are unacceptable fatalities · legal consistency across England (Clapham Omnibus)

Input and process specifications
Some procedures require specific data for national registers and these have to be specified · e.g. NCEPOD· Cataract National Dataset· e.g. National Joint Registry

Outcomes
The difficulty with outcome(s) is that the results should be attributable to the treatment

Measures
KPIs· 25 ISTCs· NHS TCs
Outcome Measures· NHS TCs· ISTCs

Fear of clinical incompatibility
Personal habit
Agreed team practice
/S Agreed local customs
P/S Nationwide custom
P/S Nationwide best practice
P/S International best practice
P/S Robust evidence practice
/S Legal requirement

KPIs, Clinical Outcomes and JSR process
Commercial KPIs devised by commercial and clinical team working with commercial lawyers
Hence strong clinical element
Consultation with, support of (not approval)• PCLs• RCLs• SHAs• JCC
Cleared in house & sent to be incorporated in contract July 2004

Clinical Outcome measures
• Indicators invited from – RCs– Other professional bodies– Providers– SHAs
• Indicators trawled from literature• Collated set discussed with stakeholders• Final set to stakeholders including JCC• Agreed by board of ISTC programme

Quality
Surgeons and accreditation
Moving on to post-operative care
Pathways, continuity and CPS

Credentialing
•People
•Facilities
•Organisation
•GMC•Specialist Register
•Training
•Buildings, equipment, consumables
•systems, information, registration•HCC

Governance
OCT’s & ISTC’s
Local ad hoc schemes

Note to Table 1 – the presence of an asterisk in the first column denotes that the relevant Performance Indicator is a Starred Performance Indicator
Ref Performance Indicator (measured over preceding Quarterly Period) in respect of [the] [each] Facility
Quarterly Threshold for Joint Service Investigation in respect of [the][each] Facility
1 Incidence of inpatient and/or daycase Activities not commenced because of DNAs as percentage of all Activities
>2% or performance of highest decile for all IS-TCs (for which data is available) if higher
2 Procedures cancelled by the Provider for non-clinical reasons on or after day of Admission; for the purposes of the Performance Threshold measured as a percentage of all Patients Admitted in the Facility
>0.5% or performance of highest decile for all IS-TCs (for which data is available) if lower
3 Procedures cancelled by Provider for clinical reasons on or after day of Admission. For the purposes of the Performance Threshold measured as a percentage of all Patients Admitted in the Facility
>0.65% or performance of highest decile for all IS-TCs (for which data is available) if lower
4 Patient returning to operating theatre for Procedure which was unforeseen at the time the Patient's previous Procedure was Completed as a percentage of all Patients Admitted in the Facility
>0%
5 In relation to each Activity Group, the conversion rate i.e. the percentage of Patients who go on to be given a Patient Appointment for a Procedure following an outpatient assessment
Greater or less than the rate in the Sponsor’s whole population of Referrals by non-consultants by a factor greater than one standard deviation around a proportion (binomial distribution)
6 In respect of [the] [each] Facility the rate of Rejection by the Provider in respect of Patients referred within the Referral Protocol (Schedule 3) as a percentage of all Patients who are Referred
Above level to be agreed with Sponsor

7 For day cases, inpatient Admission to the Facility or other provider's facilities (including NHS providers) which was unforeseen at the time of Admission; for the purposes of the Performance Threshold as a percentage of all day cases in the Facility
>2.0%
8 Transfers of Patients to another provider for inpatient Treatment which was not in the management plan[1] for that Patient upon Admission to the Facility; for the purposes of the Performance Threshold as a percentage of all inpatients in the Facility for:i) ophthalmology and minor surgery;ii) orthopaedics;iii) other Procedures
i) >0% for ophthalmology and minor surgery ii) >1.8% for orthopaedics iii) >0.8% for other Procedures
9 Emergency Admissions/ Readmissions of Patients who have received inpatient Treatment and have been Discharged within 29 days of such Discharge where such Admission or Readmission is related to or arising from the relevant inpatient Treatment. For the purposes of the Performance Threshold measures by HRG as a percentage of all Patients Discharged
Highest decile for performance of all IS-TCs (for which data is available)
[1] Management plan requirements to be set out in Schedule 3

10 Average length of stay in hours for day cases by HRG measured from the time of Admission to the time of Discharge
Lowest and highest decile of performance for all IS-TCs (for which data is available)
11 Average length of stay by HRG measured in inpatient days measured from the time of Admission to the time of Discharge
Lowest and highest decile of performance for all IS-TCs; lowest and highest decile of performance on previous year’s NHS performance if higher or lower (respectively) (all in so far as data is available)
12 Average Procedure time by HRG broken down by:i) induction;ii) time on operating table;iii) recovery measured from [] to [][1]
Lowest and highest decile of performance for all IS-TCs (for which data is available) in respect of (i), (ii) and (iii)
13 Patient receives or is listed or recommended for a further Procedure to put right any aspect of the original Activity less than 5 years from date of Discharge. For the purposes of the Performance Threshold measured as a percentage of all Procedures carried out at the Facility
Highest decile for all IS-TCs (for which data is available)
[1] e.g. Anaesthesia Start – Time when a member of the anaesthesia team begins preparing the patient for an aesthetic.Procedure/Surgery Start Time – Time the procedure is begun (e.g., incision for a surgical procedure, insertion of scope for a diagnostic procedure, beginning of examination for an EUA, taking x-ray for radiologica procedure).Procedure/Surgery Finish – Time when all instrument and sponge counts are completed and verified as correct; all post-op radiological studies to be done in the operating theatre are completed; all dressings and drains are secured; and the surgical team have completed all procedure-related activities on the patient.Discharge from Post Anaesthesia Care Unit – Time patient is transported out of PACU (for inpatients).ORDischarge from Same Day Surgery Recovery Unit – Time patient leaves SDSR, either to home or other facility (for day cases).

14 Percentage of Procedures carried out under local or regional anaesthetic (i.e. other than general) anaesthetic by HRG as a percentage of all Procedures
Lowest and highest deciles of performance for all IS-TCs (for which data is available)
15 Clinical outcomes specified, by Procedure by reference to the PCPs[1]
Lowest (undesirable) or highest (desirable) decile of performance for all IS-TCs (for which data is available)
16* Timeliness, completeness and accuracy of Provider Performance Data provided to the Joint Service Review and/or to Sponsors
Any material
17 Timeliness, completeness and accuracy of Provider clinician reporting to Referring Health Service Body's clinician
Any material
18 Patient/Customer Satisfaction (by survey) based on a survey of 10% of all Patients at each Facility in each [Contract Month]
>20% of Patients surveyed are dissatisfied with any aspect.
19 Rate of Patient Complaints ie number of complaints received as a percentage of all Patients Referred for:i) outpatient Treatment; orii) inpatient/daycase Treatment
Lowest and highest decile of performance for all IS–TCs (for which data is available)
[1] These need to be specified when PCPs completed eg for cataracts, visual acuity is likely to be a relevant clinical outcome.

20 Patient complaints handling – complaints not handled within relevant timescales set out in this Agreement
One incident
21* Incidents which are reportable to the NPSA or other statutory body
One incident
22 Additionality – NHS staff recruited in breach of Clause 9 of this Agreement
One incident
23 Condition of Facility measured by inspection by a Sponsor and/or the Provider and assessed against the requirements of the Facility Manual and Operational Procedures
Any material incident of failure to meet statutory requirements in relation to the condition of the Facilities and/or the requirements of the Facility Manual and/or Operational Procedures in respect of cleanliness, catering, environment, accessibility, maintenance, pest control, housekeeping and waste management.
24 Breach of security related to the Services where there is an identifiable risk of harm, loss or damage to people or property
More than one incident
25 Breach by the Provider of confidentiality and/or data protection requirements in the Agreement
One incident
26 Failure to meet Treat by Date One incident

Prostate: International Prostate Symptom Score [IPSS]
pre- and
post-op, · timings to be confirmed
[patient administration as good as physician administration (Plante M et al. Urology, 1996;26:326-328)]

Cataract: VF-14 Visual acuity
Cataract surgery· pre-op and · 6 weeks post-op
Note that ISTC providers are also required to collect and report the Cataract National Dataset

Cholecystectomy: Leeds Dyspepsia Questionnaire
@ pre-op
@ OP assessment), and
@ 3 months post-operative Questionnaire[1]
· Moayyedi S et al. The Leeds Dyspepsia Questionnaire: a valid tool for measuring the presence and severity of dyspepsia. Aliment Pharmacol Ther, 1998;12:1257-1262

Carpal Tunnel: CTS Questionnaire
CTSQ: · @ Pre op· @ Post op assessment· @ 1 year post-op
Pre-op scores provide information about thresholds at which listing decisions are made, (which may be relevant to PIs #5 and #6 conversion and rejection)· Carpel Tunnel Assessment Questionnaire[1]
[1] Bessette L et al. Comparative responsiveness of generic versus disease-specific and weighted versus unweighted health status measures in carpal tunnel syndrome. Medical Car,e 1998;36(4):491-502
Hip replacement: Oxford Hip Score
Clinical outcome to be before/after comparison
OHS: · @ Pre op· @ Post op assessment· @ 1 year post-op Pre-op scores provide information
about thresholds at which listing decisions are made, (which may be relevant to PIs #5 and #6 conversion and rejection)
ISTCs also to collect and report data on hip replacements as required by the National Joint Registry

National Joint Registry data: (8 February 2004)
Total number of individual patient episodes, submitted electronically: 45,214 records
Contributors since 1 April 2003:• NHS Trusts (England only): 126 • NHS Hospitals (England only): 162

TKR: Oxford Knee Score
Clinical outcome to be before/after comparison
OKS: · @ Pre op· @ Post op assessment· @ 1 year post-op
Pre-op scores provide information about thresholds at which listing decisions are made, (which may be relevant to PIs #5 and #6 conversion and rejection)
ISTCs also to collect and report data on hip replacements as required by the National Joint Registry

Diagnostic procedures
endoscopy, colonoscopy, arthroscopy etc. Questions:· whether a diagnosis was made· whether the diagnosis made was correct
10% sample of referring clinicians to be asked for views (post-discharge) as to: whether the diagnosis was made; whether, in the event, it was (or appears to have been) correct;
Note that: PI#17 captures timeliness, completeness and accuracy of provider clinician reporting to referring clinician

Excision biopsy
All procedures involving excision biopsy
Complete removal of tumour or % incomplete removal of tumour on histology report

All surgery: blood loss during surgery
blood loss during surgery
thresholds set by reference to average blood loss in restricted number of procedures

Overall achievement of objectives
To what extent did your treatment achieve what you expected from it?
Measured on all patients, at 6 weeks post-surgery
at the same time as EQ5D
incorporated into patient satisfaction survey instrument when eventually agreed
providers be required to record the objectives of treatment agreed with the patient at the time informed consent

Problems
To what extent did your treatment cause problems you did not expect?
Measured on all patients, at 6 weeks post-surgery (at the same time as EQ5D and incorporated into patient satisfaction survey instrument when eventually agreed) Providers be required to record the advice on likely side effects and problems of treatment with the patient at the time informed consent

Unexpected need for medical attention
Did you need to contact the ISTC, your GP surgery, or other health facility/professional other than by prior arrangement?
Measured at 6 weeks (as above)
Compared to what you expected, did you have more:· discomfort?· pain?· leakage of fluid from the wound?· bleeding?· limitation of normal activities?

EQ5D
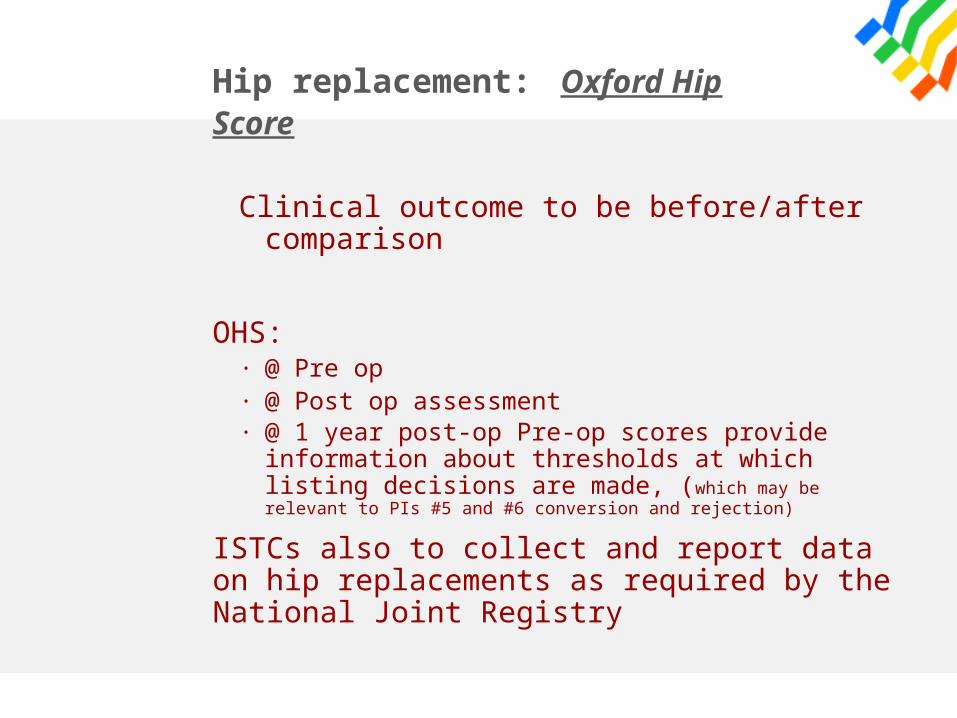
Diagnostics (direct access)
Discharge to NHS - GP - Intermediate
Care - Subsequent
necessary care
Essential OP follow- up as required
Acute Inpatient
Follow-up ?
Surgery & Recovery
Pre-op Assessment
OP Follow-up OP Consultation
NHS OP Consultation (and waiting
list)
A CB D
diagnostics+-
E
New Provider Assessments (Outpatients)
New Provider Surgery (FCEs)
(£A)
(£S)
ISTC ProgrammeTCs Patient Flow Diagram
diagnostics+ -
GP Consultation with Patient

anomalyidentified or
random records
sponsor andprovider jointlyreview case(s)
agree onproblem?
arbitrationN
Y

arbitrationremedial action
agreed?
care asagreed?
Y
N
no penaltyapplied
penaltiesagreed?
arbitration
remedial actiontaken?
N
N
Y
N
Y
f

Joint Service Reviews
actions agreed at previous meetings
routine data, identification of any problem areas, and agreed actions
ad hoc reports and the results of any investigations, identification of problem areas, and agreed actions
figures for the ISTCs concerned, compared with other ISTCs;
all findings from reviews of random case records
presentation by the provider to the sponsor of the results of their clinical audit

Source of data
Anomaly Example
Routine reports
Absolute statistical
Patients waiting longer than contracted maximum
Routine reports
Relative statistical
Procedure time in the highest decile of all comparable providers; visual acuity following cataract surgery in lowest decile of all comparable providers
Ad hoc reports
Significant event
Unplanned transfer of patient to NHS provider
Ad hoc reports
Complaints Patient had not understood proposed treatment when giving consent to surgical treatment
Review randomly from case records
----- -----
Triggers for review

Consequences of review
No problem detected
No penalty, but may be other consequence as per contract
A Provider to take remedial action within specified timescale; possibly increased level of monitoring
B Failure points, proportionate to issue(s)
C Financial penalties
D Contract termination

Perceptions of quality risk
National govt.
Local Govt.
Providers (new territories)
Investors (due diligence)
Professions (mixed interests)
Media
Public

What Procedures can be ‘safely’ performed in the
setting?
not associated w/ excessive blood loss &/or fluid shifts do not require higher specialized operating equipment or intensive post-op care; post-op pain manageabletake a “reasonable period of predictable time”the‘ultimate’ determinant: clinician comfort level

What Patients?
few standardized guidelinesno multi-centre studies; paucity of large prospective studiesMayo Clinic Study 1984: ASA III no higher risk in a Surgery CentreFASA 1987: survey of 87,000 patients, questioned relationship between pre-existing disease and peri-operative complicationsThere is some empiric evidence of certain “patients at risk”

Patients at Risk
“complex morbid obesity/complex sleep apnoea”potential for airway problems, dysmorphic facial features, severe rheumatoid arthritis, extreme age (?)poor physiologic condition: ASA III+/IVhistory of problems with anaesthesia (MH history)Acute substance abuse
The goal of any pre-op system
“Reduce the morbidity of surgery & return patient to normal functioning as
quickly as possible.”

Risk Classification
Surgical Category
1
Surgical Category
2
Surgical Category
3
Surgical Category
4
Surgical Category
5
Anaesthesia Class
1
Anaesthesia Class
2
Anaesthesia Class
3
Anaesthesia Class
4
The Johns Hopkins Risk Classification System

Group of 606 patients, 386 chest x-rays ordered without indication…Among these patients, one with abnormality that ‘may’ have resulted in improved care….the existence of three patients with lung shadows led to three sets of invasive tests, including one thoracotomy, but no discovery of disease
After careful medical history, patients undergoing minimally invasive surgery have little benefit from testing…..30 day morbidity after surgery no different than living 30 days without surgery.
Schein OD, et al. The Value of Routine Preoperative Medical Testing Between Cataract Surgery. NEJM 2000; 342: 168-175
Roizen MF, et al. The relative roles of the history and physical examination, and laboratory testing in preoperative evaluation: the “Starling” curve in preoperative testing. Anesthesiol Clin North Am 5:15, 1987.
Narr BJ, et al. Outcomes of patients with no laboratory assessment before anesthesia and a surgical procedure. Mayo Clin Proc 72:505-509, 1997
18,189 elective cataract patients: no significance differences betweenthe no-testing & testing groups in the rates of Intraoperative events.

Pre-Op Testing: a sample matrix for minimally invasive surgery
NO T E S T ING
YE S
E K G w ith in 1 m on th :h /o C ard iac , D iab e tes
Na+ ,K + ,Bun/C r, G lucose(E lec tro lyte P an e l):
h /o D iab e tes , R en a l D isease ,D iu rec tic u se
C BC w / p la te le ts :h /o an em ia , recen t b lood loss ,(p o ten tia l fo r s ig n b lood loss )
L iver F unction T es ts :ra re ly req u ired
Blood T ype :m isc arriag es
C X R :ra re ly req u ired
se lec ltive tes ting
NO T hea lthy
E K G w ith in 6 m onths
NO , hea lthy but > 75
Is pa tient hea lthy & < 75(n o h osp ita liza tion o r m a jo r c h an g es in las t 6 m on th s )

Surgery Centre Pre-Op Testing: On-Site
ElectrocardiogramHaemoglobinGlucometerUrine Pregnancy Test

The process of the screening process is a crucial first step that allows for the provision of safe, effective, and efficient medical care……The development of preoperative evaluation systems in response to outpatient and same day admission surgery provides the challenge of organizing services into formal systems with guidelines formulated on the basis of mutual agreement and
established clinical practice……
it is imperative that the anesthesia staff reach a consensus on significant preoperative evaluation issues and adhere to them in dealing with patients and surgeons and
associated organizations. Conspicuous or consistent deviation from these practices will only serve to undermine the confidence of all the parties………
Anesthesiologists, in setting up their systems, are well advised to allow for a measure of flexibility.
While adhering to a strong standard of care, reasonable judgement in providing that care is preferable to unyielding policies.
Ambulatory Anesthesiology: A problem oriented approachL. Reuven Pasternak, M.D., Chapter 1, Screening Patients: Strategies and Studies.

On-Time Performance
Updated preference cards
On-site Sterile Processing
Standardize Case packs- supplies pulled day before
Patients walked to OR – short distance, no porters
Quick Prep & Anaesthesia Starts – minimize M.A.S.T.
Rapid turn around time (less than 10 minutes)
Simple Charting – report by exception, utilize checklists
OR flow closely monitored by the OR charge nurse & the charge anaesthetist: “vigilance”

Example Anaesthesia Service Quality Indicators:
Patient and surgeon satisfaction
Accuracy rate on clinical records
Same day cancellation and surgical cases delayed
Cost per case benchmarking
Prolonged post-op nausea/vomiting
Taking longer than 30 minutes in phase I
‘Reportable incident’ rates
















![Finale 2004 - [Showtime I - Fullscore Harmonie.MUS]£ ã ã bb bb bb # # # # b b bb bb bb bb bb bb 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 44 4 4 4 4 4 4 4 4](https://img.pdfslide.us/doc/110x75/5b08e3307f8b9a520e8d5803/finale-2004-showtime-i-fullscore-bb-bb-bb-b-b-bb-bb-bb-bb-bb-bb-44.jpg)





![Geological Map of Mongolia [L-47-X] · bQ3 D1-2er D2-3ts D2-3ts D1-2er D2-3ts D1-2er D1-2er bQ3 dpQ3-4 D2-3ts D1-2er gQ2-3 bN1 D1-2er 4h ... Geological Map of Mongolia [L-47-X] Author:](https://img.pdfslide.us/doc/110x75/5af29b997f8b9ac24690e4d7/geological-map-of-mongolia-l-47-x-d1-2er-d2-3ts-d2-3ts-d1-2er-d2-3ts-d1-2er-d1-2er.jpg)