Modified Pen Grasp: Finger Function DigitsPlacementFunction
Index/ThumbOn instrument handleHold the instrument MiddleRests
lightly on shankGuide the working-end Feels vibrations transmitted
from working- end to shank RingOn oral structure, often a tooth
surface Advances ahead of the other fingers in the grasp Stabilizes
& supports the hand for control and strength LittleNear ring
finger Natural, relaxed No function in grasp Nield p.72
Slide 8
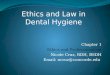
Correct Finger Placement Contact Handle Handle rests Contact
Handle Contacts Shank Rests on Ring Finger Rests on Tooth
Slide 9
Nield p.75
Slide 10
Modified Pen Grasp: LF Nield p.73
Slide 11
Modified Pen Grasp: RT Nield p.73
Slide 12
Slide 13
Modified Pen GraspPalm Grasp
Slide 14
Description Handle of the instrument is held in the palm by
cupped index, middle, ring, and little fingers Thumb is free to
serve as the fulcrum Limitations of use Instruments for calculus
removal, root planing, and maintenance root debridement are not
used with a palm grasp Examples of uses A/W syringe Non-dominant
hand for instruments stabilization while sharpening
Slide 15
Slide 16
Neutral Positions Wrist Straight, and the forearm and the hand
are in the same horizontal plane when in the neutral position Elbow
90 degrees or greater, with the forearm positioned horizontally or
slightly oblique Hand is in straight alignment with the forearm
Shoulder Neutral, both shoulders are level and relaxed to their
lowest position From a lateral position, each is vertically in line
with, and beneath, each ear The upper arms are straight down to the
elbow Nield p.92
Slide 17
Nield p.91
Slide 18
WHICH ONE IS CORRECT?
Slide 19
Nield p.92
Slide 20
Slide 21
Fulcrum Definition: The support, or point of rest, on which a
lever turns in moving a body Finger rest: The support, or point of
finger rest on the tooth surface, on which the hand turns in moving
an instrument Nield p.89
Slide 22
Fulcrum: Finger Rest Objectives 1. Stability: for controlled
action of the instrument 2. Unit control: provides a focal point
from which the whole hand can move as a unit 3. Injury prevention:
to the patients oral tissues can result from irregular pressure and
uncontrolled movement 4. Patient comfort: Confidence in the
clinicians ability, which results from the feeling of securely
applied instruments 5. Control of stroke length: With instrument
grasp, the finger rest limits the instrumentation to where it is
needed Nield p.90
Slide 23
Slide 24
Nield p.89
Slide 25
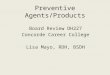
Princess Wave or Wrist-Rock When instrumenting,
wrist/hand/forearm should never break neutral position Instruments
are moved using the Princess Wave or Wrist-rock motion
Slide 26
Slide 27
Slide 28
OBJECTIVE #2 Introduction to Instrument Anatomy
Slide 29
Slide 30
Instrument Anatomy Each instrument is designed for different
purposes Clinicians know the names & numbers Classification by
purpose and use 1. Examination/Assessment Instruments ex: probe,
explorer, mirror 2. Treatment/Working Instruments ex: curets,
scalers, file, hoe, chisel
Slide 31
DENTAL MIRROR
Slide 32
DENTAL EXPLORERS
Slide 33
DENTAL PROBES
Slide 34
DENTAL SCALERS
Slide 35
Instrument Anatomy Wilkins p.580-581 Nield p187-199 1. Handle
2. Shank 3. Working End
Slide 36
Slide 37
Overall design Single-ended instrument 1 working end
Double-ended instrument Paired (mirror image) or complementary
working ends Paired working ends are used for access to proximal
surfaces from the facial or lingual aspects Cone socket handles
Separable from the shank and working end They permit instrument
exchanges / replacements 1. HANDLE
Slide 38
Shape: Round or Hexagonal Solid or Hollow Metal or Silicone
Weight Handles w/lighter weight: enhance tactile sensitivity,
fatigue Diameter 4 available: 3/8, 5/16, 1/4, and 3/16 inch Ideal
instrument: lightweight, serrated (next slide), hollow handle with
a 3/8- or 5/16-inch diameter 1. HANDLE
Slide 39
Surface Texture/Serrations Smooth, Ribbed, Knurled Texturing
increases static friction between fingers & handle Results in
reduced pinch force in the grasp No texturing Decrease control of
instrument in wet environment Increase muscle fatigue Raised
texturing Easier to hold in wet environment Maximize control of
instrument and reduce muscle fatigue 1. HANDLE
Slide 40
Slide 41
Connects working end with handle Shape, length, rigidity govern
the access of the working end to accomplish goals of clinician
Lower / Terminal Shank Section adjacent to the working end (contd
next slide) 2. SHANK Blade ShankLower Shank Handle
Slide 42
Lower Shank contd Provides important visual clues for the
clinician in selecting the correct working-end for the particular
tooth you are working on General rule of thumb: TERMINAL SHANK
PARALLEL TO THE TOOTH for correct adaptation Lengths 1. Standard 2.
Extended: 3mm longer 2. SHANK
Slide 43
Slide 44
Shape 1. Simple/Straight Flat Bent in one plane (front-to-back)
Anterior teeth Ex: Anterior sickle scaler H 6/7, Gracey (your
instruments in clinic) 2. Complex/Angled/Curved Shank bent in 2
planes (front-back and side-to-side) Posterior teeth Ex: Posterior
sickle scaler 204S, Universal scaler 13/14, Gracey 11/12 or 13/14
(your instruments in clinic) 2. SHANK
Slide 45
Slide 46
Nield p.194
Slide 47
Flexibility Varying degrees of thickness and rigidity that
relate to the instruments purpose Rigid/Thick Shank: stronger, able
to withstand greater pressures w/out breaking. Needed for removal
heavy calculus Less Rigid/More Flexible Shank: More tactile
sensitivity. Used for finer scaling, removal smaller deposits,
exploring (feeling) Length Distance from working end/blade/cutting
edge to junction of the shank & handle Most instruments 35-40mm
(1/2in) 2. SHANK
Slide 48
Carries out the purpose/function of the instrument Some
instruments remove deposits, some are used just for assessment or
feeling To determine its use, need to know the parts of the working
end 3. WORKING END
Slide 49
Parts of Working End 1. Cutting Edge Fine line where 2 surfaces
meet Ex: face and lateral surface meet to form the sharp cutting
edge of a curet 2. Lateral Surfaces Meet or are continuous to form
the back of the instrument 3. Face and Back Purple = face Gold =
Back 3. WORKING END Nield p.197
Slide 50
Instrument grasp functions Dominant hand: hold and activate the
treatment instrument Nondominant hand: mirror, suction, syringes
INSTRUMENT USE
Slide 51
Slide 52
OBJECTIVE #3 MOUTH MIRROR
Slide 53
Mouth Mirror Competency
Slide 54
Mouth Mirror Uses 1. Indirect vision: Looking through the
dental mirror to see areas of the mouth 2. Indirect illumination:
reflecting light off dental mirror onto tooth/area 3.
Transillumination: transmission of light through a sample. Ex:
detecting caries or enamel fractures by shining a specific light
through the enamel 4. Direct vision: Looking directly with eyes
into oral cavity
Slide 55
Slide 56
Nield p.93
Slide 57
Nield p.94
Slide 58
Slide 59
Nield p.95
Slide 60
Slide 61
http://www.youtube.com/watch?v=1wykNoiSNMU CRACKED TOOTH &
TRANSILLUMINATION YOU TUBE
Explorers Designed for adaptation around the tooth Used to
detect and assess: 1. Supragingival calculus 2. Subgingival
calculus 3. Cemental irregularities 4. Dental caries 5.
Decalcification 6. Irregularities in margins of restorations 7.
Secondary caries around restorations 8. Morphologic crown and root
anomalies 9. External root absorption
Slide 67
Explorers Made of flexible metal that conducts vibrations from
working-end to clinicians fingers resting on the instrument sank or
handle Circular in cross-section Working-end 1-2mm in length (tip)
Do NOT use actual POINT to detect calculus, use the SIDE Nield
p.281
Slide 68
Explorer Stroke Assessment or Exploratory Stroke Require high
degree of precision Use LIGHT, CONTROLLED STROKES Tactile
Sensitivity Ability to detect tooth irregularities by feeling
vibrations transferred from explorer working end to handle
Slide 69
Insert assessment stroke Nield p.279
Slide 70
WRIST POSITION WHILE EXPLORING More on Neutral Wrist Position
at end of class Nield p.297
Slide 71
Slide 72
Slide 73
Shepherds Hook Competency Point Value: 10 1. Uses Modified Pen
Grasp 2. Uses proper fulcrum 3. Hand is straight with forearm 4.
Keeps 1-2 mm of tip on tooth 5. Tip is angled 75angle on
groove/fissures 6. Repositions correctly as needed 7. Uses wrist to
move instrument 8. Uses light but firm grasp 9. Mirror used
correctly 10. Patient and operator position is correct 11. Light is
positioned correctly *12. Utilizes proper infection control
protocol TOTAL POINTS:
Slide 74
Shepherds Hook Resembles the long stick with a curved end that
was used by ancient shepherds to catch sheep Uses Supragingival
examination of the margins of restorations or to assess for sealant
retention Examine grooves and pits of teeth NOT recommended for
subgingival use
Slide 75
Shepherds Hook Technique Angled 45 onto tooth surface, not 90
Place explorer around grooves and in pits Actual point not used
Keep 1-2mm of tip on tooth surface at all times
Slide 76
ODU 11/12 Competency
Slide 77
WHAT WE ARE DETECTING WITH ODU11/12 Nield p.298
Slide 78
WHAT WE ARE DETECTING WITH EXPLORING Nield p.298
Slide 79
Nield p.299
Slide 80
INTEPRETATION OF SUBGINGIVAL CONDITIONS Nield p.299
Slide 81
Slide 82
Nield p.300
Slide 83
SKILL BUILDING ANTERIOR Nield p.284 Correct Working End For
Anterior Teeth = ODU11/12 Wraps Around the Surface You Are
Exploring NEED TYPODONT & ODU11/12
Slide 84
SKILL BUILDING POSTERIOR Nield p.288 Correct Working End For
Posterior Teeth = ODU11/12 Wraps Around the Mesial Surface
Using Clock Positions for Instrumentation To learn which sides
of the teeth you clean from what clock position RT-Handed Anterior
Surfaces Away/Towards Posterior Surfaces Away/Towards LF-Handed
Anterior Surfaces Away/Towards Posterior Surfaces Away/Towards
Slide 88
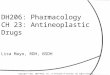
RT-HANDED Anterior Surfaces Away Clock position = 11-1
oclock
Slide 89
RT-HANDED Anterior Surfaces Towards Clock position = 8-10
oclock
Slide 90
RT-HANDED Posterior Surfaces Away Clock position = 10-11 oclock
F F L L
Slide 91
RT-HANDED Posterior Surfaces Towards Clock position = 9 oclock
F F L L
Slide 92
LF-HANDED Anterior Surfaces Away Clock position = 11-1
oclock
Slide 93
LF-HANDED Anterior Surfaces Towards Clock position = 3-4
oclock
Slide 94
LF-HANDED Posterior Surfaces Away Clock position = 1-2 oclock F
F L L
Slide 95
LF-HANDED Posterior Surfaces Towards Clock position = 3 oclock
L F F L
Slide 96
Patient Positioning Be sure to have your patient turn their
heads toward or away from you so you can gain better access and
visibility to different areas of the oral cavity