Embed Size (px)
Citation preview

CH 60 & 63: Patient’s with a Mental/Psychiatric Disorder
Lisa Mayo, RDH, BSDH
“Great opportunities to help others seldom come, but small ones surround us everyday.”
Sally Koch
CH 60 & 63: Patient’s with a Mental/Psychiatric Disorder
Lisa Mayo, RDH, BSDH
“Great opportunities to help others seldom come, but small ones surround us everyday.”
Sally Koch

Topics 1. Down Syndrome (CH60)2. Intellectual Disorder (CH60)3. Schizophrenia4. Depression5. Bipolar6. Post-partum7. Anxiety8. Eating disorders: anorexia nervosa,
bulemia

O Cause: chromosomal abnormality from either mother or father
O Other name: “Trisomy 21 syndrome”O Prenatal screening availableO IQ <70O Like music: can help in dental
environmentO EVERYTHING ABOUT DOWN’S BEEN ON
EVERY BOARD EXAM SINCE COHORT 1!
Down Syndrome

Down SyndromePhysical Characteristics
O Short stalky stature: Waddling gaitO Head: MicrocephalusO Eyes
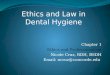
O Obliquely slanted O Epicanthic fold: skin fold from upper eyelid over
inner angle of eyeO Cross eyed, cataracts common
O Nose: short, under-developedO Small earsO Flat facial profile

A: Absence of an epicanthic fold
B: Epicanthic fold in Oriental populations
C: Epicanthic fold of person with Down’s (also FAS)

Down SyndromePhysical Characteristics
O Hypotonia (low muscle tone & strength)
O Dysplasia of pelvisO Poor motor reflexO Joint hyperflexibilityO Hands
O Clinodactyly of 5th fingerO Short stubby fingersO Single, transverse palmar crease
(Simian line/crease)

Also called “floppy baby”

Down SyndromeSocial CharacteristicsOLike attentionORequire affection for feeling of securityOCheerful dispositionORarely irritableOEasily amusedOSociable, observant, take initiativeOTendency to imitateOMischievousOPeriods of stubbornnessODetermined to have their own wayOParental discipline is necessary


Down Syndrome OralO Habits of tongue thrusting, bruxism,
clenching, droolingO Lips: dry, cracked, thick due to drooling O Tongue: Large & fissuredO Higher incidence of cleftsO Increase incidence perio (tend to be severe
types)O Occlusion
O Narrow palate, underdeveloped maxillaO Class III O Posterior crossbite



Down Syndrome OralO Teeth
O Small cone shaped teeth & hypoplastic enamel
O Microdontia O Congenitally missing O Delayed, un-sequential exfoliation and
eruptionO Anomalies: fusion, peg lateralsO NOT INCREASE RISK FOR CARIES, JUST
PERIO! (NBQ)

Down SyndromeO Associated problems
O Mortality rate used to higher due to incidence:1. Respiratory infections2. Leukemia3. Congenital heart lesions (MVP, premed may
be needed)
O Susceptibility to infectionsO SeizuresO Obstructive airway: macroglossia, enlarged
tonsils & adenoids O Alzheimer disease 40+

Down SyndromeO DH Tx Plan Modifications
OSpeak simply and reassuringlyOTell, sow, doOWatch for respiratory issues: Avoid air
polisher and ultrasonicOPositive reinforcementOBuild trustOMD consult regarding premed

Question
What is not a sign of Down’s Syndrome?
A. Simian creaseB. XerostomiaC. Short phalangesD. Short stature

Answer
What is not a sign of Down’s Syndrome?
A. Simian creaseB. XerostomiaC. Short phalangesD. Short stature

Another term for Down syndrome is:A) epicanthusB) disomy 15C) autismD) trisomy 21
Review

Another term for Down syndrome is:A) epicanthusB) disomy 15C) autismD) trisomy 21
Review

Which of the following oral features are frequently associated with Down syndrome?
A) Deeply fissured tongue, mouth breathing, thickened lips
B) Angle’s Class II occlusion, macrodontia, narrow palate
C) Gingivitis, supernumerary teeth, microglossiaD) Atrophic lips, drooling, linear gingival erythema
Review

Which of the following oral features are frequently associated with Down syndrome?
A) Deeply fissured tongue, mouth breathing, thickened lips
B) Angle’s Class II occlusion, macrodontia, narrow palate
C) Gingivitis, supernumerary teeth, microglossiaD) Atrophic lips, drooling, linear gingival erythema
Review

NBQ
Which of the following oral abnormalities are commonly found in patients with Down syndrome?
a. Anterior crossbiteb. Early eruption of teethc. Small tongued. Large nasomaxillary complex

NBQ
Which of the following oral abnormalities are commonly found in patients with Down syndrome?
a. Anterior crossbiteb. Early eruption of teethc. Small tongued. Large nasomaxillary complex

NBQ
Which of the following 2 items are not symptoms of Down’s syndrome?
a. Xerostomiab. Increased cariesc. Flat facial profiled. Decreased resistance to infection

NBQ
Which of the following 2 items are not symptoms of Down’s syndrome?
a. Xerostomiab. Increased cariesc. Flat facial profiled. Decreased resistance to infection

NBQ
Angle’s classification of malocclusion commonly found in clients with Down syndrome is:
a. Class Ib. Class II, division onec. Class II, division twod. Class III

NBQ
Angle’s classification of malocclusion commonly found in clients with Down syndrome is:
a. Class Ib. Class II, division onec. Class II, division twod. Class III

NBQ
Antibiotic premedication is commonly needed in clients with Down syndrome because of the high incidence of:
a. Congenital heart valve defectsb. Obstructive airway problemsc. Impaired leukocyte functiond. Chromosomal abnormalities

NBQ
Antibiotic premedication is commonly needed in clients with Down syndrome because of the high incidence of:
a. Congenital heart valve defectsb. Obstructive airway problemsc. Impaired leukocyte functiond. Chromosomal abnormalities

NBQDelayed and abnormal tooth eruption patterns are common in clients with Down syndrome. The lips are thin, and the tongue is very small, and this contributes to the delayed eruption of teeth.
a. The first statement is TRUE; the second is FALSEb. The first statement is FALSE; the second is TRUEc. Both statements are TRUEd. Both statements are FALSE

NBQDelayed and abnormal tooth eruption patterns are common in clients with Down syndrome. The lips are thin, and the tongue is very small, and this contributes to the delayed eruption of teeth.
a. The first statement is TRUE; the second is FALSEb. The first statement is FALSE; the second is TRUEc. Both statements are TRUEd. Both statements are FALSE

O Formerly called “MR: mental retardation”O Significant limitations in intellectual functioning O Origination prior to 18yrsO 5 Dimensions
1. Intellectual abilities: mental capabilities
2. Adaptive behavior: Collection of conceptual, social, and practical skills
3. Participation, interactions, and social roles4. Health (physical, mental, and etiology)5. Context (environment, culture)
Intellectual Disorder

O TypesO Education & learningO Supported living, health servicesO Employment
O DH CareO Freedom from oral discomfort and painO Teaching daily self-careO Improve quality of life
Intellectual Disorder Support

O Mild: IQ 50-69O Adult mental age 9-12yrsO Education: 3-6th grade
O Moderate: IQ 35-49 O Adult mental age 6-9yrsO Will not learn to read/write, learns personal care and hygiene
w/support
O Severe: IQ 20-34yrsO Adult mental age 3-6yrs O Walks, some speech, limited attention span
O Profound: IQ <20O Adult mental age under 3yrsO Supervision & care necessary: cannot sit up, incontinence,
mobility
Classification of Intellectual Disabilities
*See Wilkins p.925*

A patient with an IQ of 40 has what level of mental disability?
A) MildB) Moderate C) SevereD) Profound
Review

A patient with an IQ of 40 has what level of mental disability?
A) MildB) Moderate C) SevereD) Profound
Review

Intellectual DisorderO Risk Factors/Etiology: Table 60-2, p.924
O Abuse & neglectO Fetal alcohol syndrome, Congenital heart
diseaseO MeningitisO 75% unknownO Etc…. See text

Intellectual DisorderOral Characteristics (note similarities to Down’s)O↑ gingivitis, perio of institutionalizedO↑ cariesO↑ bruxism, mouth breathing, tongue thrustingOGaggingOLips: ↑ thickness, biting OTooth anomalies: imperfect formation, delayed or irregular eruption patterns

Physical features: see text p.926
Intellectual Disorder

NBQ
The high incidence of dental caries in patients with an intellectual impairment is MOST likely caused by:
a. Oral neglectb. Genetic defectsc. Abnormal oral musculatured. Swallowing problems

NBQ
The high incidence of dental caries in patients with an intellectual impairment is MOST likely caused by:
a. Oral neglectb. Genetic defectsc. Abnormal oral musculatured. Swallowing problems

NBQ
Clara is a 75 year old mentally retarded female. She resides in a long-term care facility. Her mother, who has Alzheimer’s, resides in the same facility. Clara’s cousin visits on a regular basis. Oral health care instructions for Clara should be:
a. Provided to her motherb. Provided to the cousinc. Provided to Clara in writingd. Oral care instructions would not be beneficial

NBQ
Clara is a 75 year old mentally retarded female. She resides in a long-term care facility. Her mother, who has Alzheimer’s, resides in the same facility. Clara’s cousin visits on a regular basis. Oral health care instructions for Clara should be:
a. Provided to her motherb. Provided to the cousinc. Provided to Clara in writingd. Oral care instructions would not be beneficial

NBQ
All of the following conditions are commonly found in persons with mental retardation except one. Which one is this exception?
a. Cerebral palsyb. Myasthenia gravisc. Seizure disordersd. Emotional disturbances

NBQ
All of the following conditions are commonly found in persons with mental retardation except one. Which one is this exception?
a. Cerebral palsyb. Myasthenia gravisc. Seizure disordersd. Emotional disturbances

NBQ
In which of the following conditions would delayed eruption of permanent teeth be expected?
a. Graves’ diseaseb. Mental retardationc. Spina bifidad. Muscular dystrophy

NBQ
In which of the following conditions would delayed eruption of permanent teeth be expected?
a. Graves’ diseaseb. Mental retardationc. Spina bifidad. Muscular dystrophy

Psychiatric Disorders
Wilkins CH63

Schizophrenia



Schizophrenia O Complex, chronic mental disorderO Disturbances in feeling, thinking, & behavior
significantly impair function to a level below normal for the individual
O Person “out of touch” with realityO Onset: 15-24 male / 25-35 womenO Etiology: unclear, maybe genetic link?O Symptoms
O Delusions, hallucinations, disorganized thinking

Schizophrenia O Phases: Box 63-2 for all S&S
1. Prodromal: signs for as long as 1yr before active phase
2. Active3. Residual
O ↑ rates alcohol & drug abuse O Poor treatment compliance, ↑
Hospitalization, homelessness, suicide

Treatment of Schizophrenia O Poor prognosis overallO Drugs used to tx symptoms (Antipsychotics)
O Disease assoc w/ excess dopamine in the brain (both class drugs block dopamine)
1.Conventional drugs1) chlorpromazine (Thorazine)2) haloperidol (Haldol)3) thiothixene (Navane)
2.Atypical drugs (fewer side effects)1) clozapine (Clozaril)2) risperidone (Risperdal)3) olanzapine (Zyprexia), 4) Quetiapine (Seroquel)

Treatment of Schizophrenia O Adverse effects of meds
O Need WBC counts often with clozapine therapy due to high risk of agranulocytosis (↓ WBC)
O Table 63-1, p.955: side effects of medsODystonia, dysarthria, tremors, akathisia,
akinesia, tardive dyskinesia, xerostomia, sedation, agranulocytosis**Need to know what above conditions are**

Review
A side effect of antipsychotic medication that causes involuntary mouth and jaw movements is called what?
A) Akathisia B) Dysarthria C) Dystonia D) Tardive dyskinesia

Review
A side effect of antipsychotic medication that causes involuntary mouth and jaw movements is called what?
A) Akathisia B) Dysarthria C) Dystonia D) Tardive dyskinesia

Dental Hygiene CareO Appts when symptoms are reasonably
controlled by medicationsO Analyze meds & know common side effectsO Calm, relaxing environmentO Same routines bestO Mouth prop for tardive dyskinesia

Mood Disorders
1. Major depressive disorder: Unipolar2. Bipolar disorder: marked by severe
mood swings from depression to elation (mania)
3. Postpartum depression4. Anxiety Disorders

Mood Disorders General Characteristics
O Periods of remission and recurrenceO Onset for major depression = mid-20s
O More common in women than men
O Bipolar onset = 20yrs O Equally common in men & women

Major Depressive Disorder
O S&S: Wilkins Box 63-3, p.956O Weight changes, insomnia, depressed, fatigue, etc….
O Tx: Therapy, Electroconvulsive therapy, Psychotherapeutic drugs
fluoxetine (Prozac) sertraline (Zoloft) paroxetine (Paxil) fluvoxamine (Luvox) SNRIs (serotonin and noradrenergic reuptake inhibitors) Tricyclic antidepressants MAOI’s last choice drugs

Dental Hygiene CareO Medication side effects: xerostomiaO Positive reinforcement, reassuranceO May have ↑ sensitivity: use LAO Prevent postural hypotensionO Fluoride

Bipolar DisorderO Major mood disorder in which episodes of varying
degrees of mania (elation) & depression occurO Formerly called “manic-depressive” disorderO Untx’d
O Periods of elation can average 6mo O Periods of depression may last longerO A return to normal behavior between episodes is
usual

Bipolar DisorderO Phases symptoms
O Depressive phase: Box 63-3O Manic phase: Box 63-4O http://www.hlntv.com/video/2011/04/14/
understanding-bipolar-disorder (3:00)O http://www.youtube.com/watch?
v=guqERXhgAo4 (2:00)O Treatment
O Hospitalization may be necessary at 1st O Pharmacotherapy: 3-prong (next slide)O Therapy

Bipolar DisorderPharmacotherapy: 3-prong approach
1. Acute manic phase: stabilize the mood O Sedation with benzodiazepine (ex: Valium)O Anticonvulsants: ex: valproic acid(Depakote)O AntipsychoticsO Lithium carbonate: mood stabilizer
2. Antidepressant therapy3. Maintenance therapy: obtain long-term mood
stabilizationO Lithium & anticonvulsants (Depakote)

Catherine Zeta Jones

Dental Hygiene CareO Manic: not best time to tx ptO High risk for perio & cariesO Over-aggressive brushing – may see trauma
to mucosaO Lithium: may cause dysgeusia (distortion in
sense of taste) & metallic tasteO Stomatitis, glossitis, loss taste acuity from
meds

Review
A patient with bipolar disorder who takes lithium may complain of:
A) bleeding when brushing B) tooth hypersensitivityC) metallic taste in mouthD) sores in the mouth

Review
A patient with bipolar disorder who takes lithium may complain of:
A) bleeding when brushing B) tooth hypersensitivityC) metallic taste in mouthD) sores in the mouth

Postpartum Mood DisturbancesO Postpartum
O Blues: A period of nonpsychotic depression for a few days after giving birth
O Depression: begins in 2nd – 3rd week postpartum O Psychosis: mood disorder, depressive or
manicO Risk factors: pre-existing mental illness, stress,
unwanted pregnancy, anxiety, marital problems

Postpartum Mood DisturbancesO Symptoms: Complaints of insomnia,
restlessness, tearfulness, fatigue, emotional unsteadiness O Progressed: confusion, irrationality,
delirium, obsessive concerns about babyO Treatment: w/out tx= risk of suicide, do not
leave baby alone with mom, observe closely

Anxiety Disorders

Anxiety DisordersO Apprehension or tension that results from the anticipation of
dangerO Anxiety is the result of feeling a threat to the person’s being,
self-esteem, or identityO Types
1. Panic attack: Box 63-5 for symptoms2. Panic disorder: recurrent, unexpected. Agoraphobia (fear
of being in places or situations from which escape might be difficult)
3. Post-traumatic stress disorder: An initiating traumatic event has occurred outside the range of usual human experience
O Kids: Physical, sexual abuseO Adults: war, imprisonment, torture, rape, threat to life
4. Generalized anxiety disorder: persistent, pervasive anxiety and excessive worry but they are not associated with life-threatening fears

Tx Anxiety DisordersO Avoid caffeine, alcohol, other drugs of abuseO ExerciseO TherapyO Pharmacotherapy
1. Benzodiazepines (Valium, Xanax, Ativan) Short term use Potential for addiction Oral side effects: xerostomia
2. Antidepressants

Dental Hygiene CareO Oral implications
O Hypersensitivity of the teethO Xerostomia due to meds - caries
O Appointment interventionsO Review meds closelyO Help the patient to feel in controlO Effective pain control: use LAO Morning apptsO Patient may appear very nervous, jumpy, and
tenseO Stay alert for possible attacks

Eating Disorders

Eating Disorders1. Anorexia nervosa (2 types)
1) RESTRICTING TYPE: Eat couple hundred calories a day. Body gets hungry – AN patients learn to control their hunger and actions in response to it
2) BINGE-EATING/PURGING TYPE: Persons who starve themselves just like the restricting types but then give into their hunger and may binge, eat a normal meal or even just a cookie and make themselves vomit.
2. Bulimia nervosa (2 types)1) PURGING TYPE: Self-induced vomiting2) NONPURGING TYPE: inappropriate compensatory
behaviors such as fasting, excessive exercise, but does not vomit or misuse laxatives

O Self-starvation due to a distorted body image of being overweight
O Behavior ProfileO Female, high rate of occurrence after pubertyO Competitive/obsessive behaviorO Increased risk with upper SESO Family conflict, overbearing parentsO Fear of gaining weight, obsessive weighing, laxative use
O CharacteristicsO Dramatic weight loss (20-40%) below desirable body
weightO Excessive exercise, aversion to foods and altered eating
habitsO Eats 300-600cal/day
O TxO Dietary, psychological, 50% who survive = 6 year
recovery
Anorexia Nervosa


AN DSM-5
1. BMI under 17.55%2. Fear of gaining weight or becoming
fat3. Body image disturbance by feeling
they look extremely fat when at a low body weight
4. Amenorrhea due to low BMI and overall weight

Psychological Physiological
Relentless pursuit of thinness and unwillingness to maintain a normal or healthy weight
Extreme thinness (emaciation)Extremely low BMI and weight (15% below normal)
Intense fear of gaining weight Anemia & muscle wasting/weakness
Distorted body image Dry and yellowish skin, brittle hair & nails
Denial of the seriousness of low body weight
Low blood pressure, slow breathing and pulse, drop in internal body temperature (cold all the time)Heart, brain, organ damage/failure
Self-esteem heavily influenced by perceptions of body weight and shape
Thinning of the bones (osteopenia or osteoporosis)Growth of fine hair all over the body (lanugo) to help keep the body warm
Extremely restricted eating and constantly weighing oneself
Severe constipation, lethargy, sluggish, tired all the time, infertility
Obsessive personality, especially in relation to food and weight
Lack of menstruation among girls and women or a delayed onset of menstruation due to low BMI
Intense fear of being “fat” Dehydration and possible kidney issues
Chronic anxiety, negative moods, perfectionist’s
Fainting

AN TXO Meds generally not needed unless
depression, anxiety co-occuringO Hospitalization in extreme cases
O Vitamins, feeding tubeO Therapy most important
O IndividualO FamilyO Need to discover underlying cause of
disorder to have successful recovery

AN & DH CareO Depression or over-reaction to
situationsO XerostomiaO Anemia common: many oral changesO Denial of a problemO Counsel on diet as patient will permitO Check vitals frequently


Bulimia Nervosa

Bulimia NervosaO Psychiatric compulsive disorder marked by recurrent episodes
of uncontrollable binge eatingO Females more likely to develop than males
O Males = 10% of casesO Restrict food intake then episodes of binge eating
O Binge eating: consumption of excessive amts of food w/in short time (sugary, high calorie, easy to eat foods)O 2,000-15,000 calories in a binge!
O Purge: vomit after bingeO Will also use laxatives, diuretics, enemas (AN also will use)O When binge over – feelings of guilt, depression, anger

Bulimia NervosaO Normal body wt or even slightly overweightO Drug/alcohol abuse by pt or parent
commonO Self-mutilationO Medical Complications
O DehydrationO Electrolyte imbalanceO PRO malnutritionO Cardiac arrhythmiasO Amenorrhea when hx anorexia nervosa

BN TxO Therapy: discover underlying reason
for the disorderO Antidepressants more effective in
people with binge-purge

Dental Hygiene CareO Pt’s socially extroverted and more outgoing in
contrast to the person with anorexiaO Oral findings
O Perimylolysis: chemical erosion of tooth surfacesO Raised restorationsO Caries: cervical, demin, pH saliva more acidicO Xerostomia from diureticsO Palatal trauma from educing vomiting with objects
(fingers)O Taste alteration

ADA: Oral Implications for Pt’s with ED
O Salivary gland enlargement (due to xerostomia)O Purging types: 2-6 days after purge parotid gland will
be enlarged – not know whyO Dry, red or cracked lipsO Lesions on soft tissues which may bleed easilyO Color change (translucency) of teeth O Change in the shape or length of teethO Restorations may be appear elevated with erosion
(usually takes 6 months of constant regurgitation for this effect)
O Teeth that are temperature sensitive (hot or cold)

Pt Care Recommendations
O Diet counseling (be careful w/your words)
O Do NOT brush after vomitingO Alkaline solution sodium-bicarb
(NaHCO3)
O NaF:↓ tooth sensitivity, caries management)
O Xerostomia tx recommendations

NBQ
Perimyolysis of the maxillary anterior lingual teeth is associated with:
a. Epilepsyb. Anorexia nervosac. Cleft palated. Bulimia

NBQ
Perimyolysis of the maxillary anterior lingual teeth is associated with:
a. Epilepsyb. Anorexia nervosac. Cleft palated. Bulimia