Embed Size (px)
Citation preview

American Journal of Obstetrics and Gynecology (2005) 193, 1591–8
www.ajog.org
EDITORS’ CHOICE
Dexamethasone treatment does not improve the outcomeof women with HELLP syndrome: A double-blind,placebo-controlled, randomized clinical trial
Javier E. Fonseca, MD, MSc,a,b,c Fabian Mendez, MD, PhD,a Claudia Catano, MD,b,c
Fernando Arias, MD, PhDd
School of Public Healtha and School of Medicine,b Universidad del Valle; Department of Gynecology and Obstetrics,Hospital Universitario del Valle,c Cali, Colombia; Department of Obstetrics and Gynecology, The Toledo Hospital,Medical College of Ohio, Toledo, OHd
Received for publication March 15, 2005; revised April 4, 2005; accepted July 5, 2005
KEY WORDSDexamethasone
HELLP (hemolysis,elevated liverenzymes and low
platelet count)syndrome
Clinical trial
Objective: The purpose of this study was to determine the efficacy of dexamethasone fortreatment of HELLP (hemolysis, elevated liver enzymes and low platelet count) syndrome.Study design: A prospective, double-blind clinical trial was conducted among 132 women with
HELLP syndrome who were assigned randomly to treatment or placebo groups. Pregnant womenin the experimental group received 10-mg doses of dexamethasone intravenously every 12 hoursuntil delivery and 3 additional doses after delivery. Puerperal women received 3 10-mg doses ofdexamethasone after delivery. The same schedule was used in the placebo group. The main
outcome variable was the duration of hospitalization. In addition, we evaluated treatment effectson the time to recovery of laboratory and clinical parameters and on frequency of complications.Results: The mean duration of hospitalization of patients who received dexamethasone therapy
was shorter than in the placebo group (6.5 vs 8.2 days), but this difference was not statisticallysignificant (P = .37). No significant differences were found in the time to recovery of plateletcounts (hazard ratio, 1.2; 95% CI, 0.8-1.8), lactate dehydrogenase (hazard ratio, 0.9; 95% CI, 0.5-
1.5), aspartate aminotransferase (hazard ratio, 0.6; 95% CI, 0.4-1.1) and to the development ofcomplications. The results were found in both pregnant and puerperal women.Conclusion: The results of this investigation do not support the use of dexamethasone for
treatment of HELLP syndrome.� 2005 Mosby, Inc. All rights reserved.
Supported in part by the Valle State Secretariat of Health; the
dexamethasone and placebo were provided by Organon Laboratories,
The Netherlands.
Reprints not available from the authors. Address correspondence to
Javier E. Fonseca, Universidad del Valle, Obstetrics and Gynecology,
Hospital Universitario del Valle, Cali, Valle 57, Colombia.
E-mail: [email protected]
0002-9378/$ - see front matter � 2005 Mosby, Inc. All rights reserved.
doi:10.1016/j.ajog.2005.07.037
Multisystemic abnormalities that are associated withadverse maternal and fetal outcomes have been recog-nized for many years in women with preeclampsia1-3;HELLP (hemolysis, elevated liver enzymes and lowplatelet count) syndrome4 is one of its most dangerouspresentations.5 Women with HELLP syndrome may beclassified by the degree of thrombocytopenia into

1592 Fonseca et al
HELLP 1 (%50,000 platelets/mm3), HELLP 2 (between50,000 and 100,000 platelets/mm3), and HELLP 3 (be-tween 100,000 and 150,000 platelets/mm3).6
Treatment of HELLP syndrome usually is restrictedto measures of support and treatment of complications.However, since a first report in 1993,7 several clinicaltrials have suggested that corticosteroids, mainly dexa-methasone therapy, can ameliorate and stabilize thedisease in the antepartum period and accelerate recoveryafter delivery.8-11 However, these studies were not dou-ble-blind or placebo-controlled trials and had smallsample size, and there is a definite need for additionalrandomized clinical trials.5 For this reason, we con-ducted a study that was aimed to determine the efficacyof dexamethasone for the treatment of HELLPsyndrome classes 1 and 2.
Material and methods
This was a double-blind, placebo-controlled randomizedclinical trial that involved pregnant and puerperalwomen who were admitted to the Hospital Universitariodel Valle in Cali, Colombia, between October 2001 andSeptember 2003. Women who were at O20 weeks ofgestation or during the first 3 days of puerperium wereasked to participate in the study if hypertension devel-oped during the pregnancy or the puerperium and metthe criteria for complete HELLP syndrome as definedby Sibai12: platelet count, %100,000/mm3; aspartateaminotransferase (AST), O70 U/L; lactate dehydrogen-ase (LDH), O600 U/L. Exclusion criteria were oraltemperature O37.5(C and diabetic ketoacidosis. Be-cause of the potential for spontaneous recovery, puer-peral women were excluded if randomization was notaccomplished in the first 24 hours after diagnosis. Thestudy was approved by the Institutional Review Boardsof the Hospital and the Medical School.
Pregnant and puerperal women were assigned ran-domly to treatment or placebo groups, with the use ofstratified and random permuted blocks of 4. Theassignment was kept inside consecutively numberedopaque envelopes that were labeled as pregnant orpuerperal and that were opened after informed consenthad been obtained. Pregnant women in the experimentalgroup received 10-mg doses of dexamethasone sodiumphosphate (Oradexon) intravenously every 12 hoursuntil delivery and 3 additional doses after delivery.Puerperal women received 3 10-mg doses after delivery.The same schedule was used in the control group toadminister sterile water as placebo. Dexamethasone andplacebo were packed in identical vials in sealed boxesthat were labeled with the corresponding treatmentcodes. Codes were not broken until the end of theunivariate analysis. Treatment was to be discontinued iforal temperature rose above 37.5(C.
All patients received 1 to 1.5 g/hr of magnesiumsulfate intravenously. Nifedipine, 10 mg orally every6 hours, was administered to women with diastolicarterial pressure O100 mm Hg. Another antihyperten-sive medication (clonidine and amlodipine) was admin-istered if the diastolic pressure remained elevated. Inaddition, patients received 1000 mL of normal salinesolution during the first 2 hours and 1000 mL of normalsaline solution every 6 hours afterwards. If the urinaryoutput remained !30 mL/hr, an additional 500 mL ofnormal saline solution was given during 1 hour; ifoliguria persisted, 20 mg of furosemide was adminis-tered intravenously. Renal failure was diagnosed if theserum creatinine level was O1.5 mg/dL and if pulmo-nary edema was diagnosed by physical examination andchest radiography. When surgery was indicated, 8 unitsof platelets were transfused to women with plateletcounts !50,000/mm3. Because the standard of care ofthe community is interruption of pregnancy after diag-nosis of HELLP, induction of labor or cesarean deliverywere performed, depending on the maternal and fetalcondition. If the gestational age was between 26 to 34weeks, betamethasone (12 mg intramuscularly) wasgiven every 24 hours for up to 2 doses before delivery.Withholding steroids was considered unacceptable bythe investigators and the Institutional Review Board.
Duration of hospitalization was measured from ran-domization to discharge. The duration of hospitaliza-tion of the 4 maternal deaths was excluded for thecalculation of mean and median but was included andtreated as censored data in survival analysis. Criteria fordischarge included a platelet count O100,000/mm3,regardless of AST or LDH levels. However, if evidenceof organ damage or other clinical complications waspresent, the patients remained in the hospital untilrecovery.
Measurements of blood pressure and urine outputwere carried out every 2 hours. Baseline and follow-uplaboratory studies included platelet count, AST, LDH,and serum creatinine measurements every 12 hours.Platelet counts were performed by automated counting;LDH and AST were processed at 25(C, with a referencepattern of 120 to 240 U/L and 0 to 18 U/L, respectively.
Medical personnel were trained on protocol proce-dures for enrollment and follow-up of patients. Qualitychecks of clinical and laboratory forms were carried outbefore data entry. After entry, programs were run toverify the consistency of responses within each ques-tionnaire. Any detected inconsistencies were resolved bycorrection against original data sheets.
Sample size was calculated by the duration of hospi-talization, as defined earlier.13 We assumed an averagehospital stay of 6 days in the control group andconsidered as significant a 33% decrease in stay forthe experimental group, with a significance level of .01and a power of 90%. The required sample size was

Fonseca et al 1593
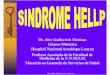
Figure 1 Trial profile.
67 subjects per group. Analysis was carried out on thebasis of intention to treat. A planned subgroup analysiswas performed according to pregnant and puerperalstrata. An additional, unplanned subgroup analysis wasconducted by severity of clinical presentation at diag-nosis. We carried out an interim analysis, at a samplesize of 50 individuals, with no differences with finalresults. Continuous variables were analyzed with un-paired t-test or Mann-Whitney test, according to theirdistribution. If needed, transformations were carried outto allow for normal based statistics. Time to recovery oflaboratory parameters (platelets, LDH, and AST) andduration of hospitalization was analyzed by Kaplan-Meier. Categoric variables were compared by chi-squared test or Fisher’ s exact test. Multivariate analysis
was performed with linear, logistic, or Cox regression,correspondingly. In addition to treatment (ie, the expo-sure of interest), other variables were considered in thefinal model if their probability values were !.2 in theunivariate analysis.14-16 Antepartum use of betametha-sone up to 2 weeks before randomization was alsoconsidered during modeling. Where appropriate, resultsare presented as relative risk with 95% CI, odds ratio,and hazard ratio.
Results
A total of 144 patients were considered eligible and wereinvited to participate in the study. Two patients (1.4%)were excluded because of fever, and 2 patients (1.4%)

1594 Fonseca et al
declined to participate. Eight puerperal women (5.5%)were not allocated to treatment during the first 24 hoursafter diagnosis and were also excluded. After these ex-clusions, 132 women were eligible for randomization: 60women were still pregnant, and 72 women were in thepuerperal state. Two patients received only 2 doses ofsteroid after delivery because of death. Two women (inthe experimental and control groups) received 1 dose ofdexamethasone that was not provided by the study(Figure 1).
The mean age of enrolled women was 25.3 years(range, 14-44 years); the mean gestational age was 33.6weeks (range, 20-41 weeks), and the mean parity was 2.4pregnancies (range, 0-12 pregnancies). Platelet countsranged from 13,000 to 100,000/mm3, with mean and
Table I Baseline characteristics
Therapy
CharacteristicPlacebo(n = 66)
Dexamethasone(n = 66)
Age (y)* 26.2 G 7.20 24.5 G 7.00Gestational age (wk)* 33.5 G 4.20 33.8 G 4.50Parity (n)* 2.0 G 2.06 1.2 G 1.25Platelets (n/mm3)* 58,446 G 21,053 61,171 G 18,912AST (U/L)* 492 G 579 573 G 621Alanine
aminotransferase(U/L)*
229 G 251 281 G 300
LDH (U/L)* 2,242 G 1,671 2,124 G 1,849Total bilirubin
(mg/mL)*3.7 G 4.67 3.3 G 3.20
Creatinine (mg;/mL)* 0.9 G 0.53 0.9 G 0.49Urinary
output (mL/min)*85 G 65.50 92 G 59.70
Systolic pressure(mm Hg)*
141 G 21.01 145 G 21.00
Diastolic pressure(mm Hg)*
93 G 13.40 93 G 12.61
Qualitative protein in urine (n)Positive 57 (87.36%) 55 (83.33%)Negative 4 (6.06%) 4 (6.6%)Unknown/
unavailable5 (7.58%) 7 (10.61%)
Acute renalfailure atenrollment
4 (6.06%) 6 (9.09%)
Pulmonary edema 1 (1.52%) 1 (1.52%)
HELLP class at enrollment (n)HELLP 1 28 (42.42%) 21 (32.31%)HELLP 2 38 (57.58%) 44 (67.69%)
Steroid use up to 2 weeks before delivery (n)No 44 (66.67%) 48 (72.73%)Yes 21 (31.82%) 16 (24.24%)Unknown 1 (1.52%) 2 (3.03%)
* Data are given as mean G SD.
median values of 57,798/mm3 and 59,200/mm3, respec-tively. The mean LDH was 2183 U/L, with a median of1701 (range, 623-12,600); the mean AST was 532 U/L,with a median of 280 (range, 71-2870). Baseline charac-teristics according to study groups were similar (Table I).
Duration of hospitalization
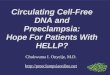
The distribution of duration of hospitalization wastransformed (1/duration of hospitalization) to allowthe use of statistical methods that are based on theGaussian distribution. The mean duration of hospital-ization was shorter among patients who received dexa-methasone therapy; however, this difference was notstatistically significant. Median and interquartile rangesalso were found to be no different (Table II). Theunivariate and multivariate analysis showed that alonger duration of hospitalization was associated witha lower urinary output (!30 mL/h) and higher LDHlevels. Survival analysis of time to discharge showedno differences (Figure 2,A; hazard ratio, 1.3; 95% CI,0.9-1.9).
Time to recovery of laboratory tests
There was no statistically significant difference betweendexamethasone-treated and placebo-treated patientswith respect to the time that was required to achieve aplatelet count of O100,000/mm3 (Figure 2,B; Table III).Recovery of the platelet count was more likely to occuramong patients with urinary output at enrollment ofO30 mL/h and less likely among those with renalfailure, although these findings were not significant atthe multivariate analysis. Platelet counts did not reachlevels of O100,000/mm3 in all 4 maternal deaths.
LDH levels of !600 U/L were not reached beforedischarge by 72 patients (38 experimental patients and34 control patients), which included the 4 deaths and 68patients who were discharged when their platelet countswere O100,000/mm3. There was no statistically signif-icant difference between treated and control patientswho reached an LDH of !600 U/L before dischargeregarding their time to recovery (Figure 2,C; Table III)or other patient characteristics at enrollment.
Table II Duration of hospitalization according to treatment
Duration ofhospitalization (days) Placebo (66) Dexamethasone (66)
Mean (D.S.) 8.2 (12.55) 6.5 (9.66)Median 4 4Range 2-89 2-64Interquartile range 3-8 3-6
Difference of mean: 1.7 (�2.28-5.61), P = .37

Fonseca et al 1595
Figure 2 Cumulative risk of (A) discharge, (B) platelet recovery (count O100,000), (C) LDH recovery (!600 U/L), (D) AST
recovery (!70 U/L) according to treatment received.
AST levels of !70 U/L were not reached by 53patients (32 experimental patients and 21 control pa-tients), which included 2 of the maternal deaths and 51patients who were discharged once their platelet countsreached O100,000/mm3. Among patients with an ASTlevel of !70 U/L before discharge, there was a trend tofaster recovery among those patients who receivedplacebo (log rank test probability value, .07) that wasnot significant after adjustment for renal failure, ethnic-ity, and parity (hazard ratio, 0.7; 95% CI,0.4-1.1; Figure2,D; Table III).
Recovery of clinical parameters
No significant differences in urinary output were foundbetween the 2 treatment groups. Furosemide wasrequired in 23 patients: 13 patients received placebo,and 10 patients received dexamethasone therapy (rela-tive risk, 0.8; 95% CI, 0.4-1.6). All patients werehypertensive, and 124 patients (93.9%) required nifed-ipine therapy; therefore, we were not able to evaluatechanges in blood pressure, because they could havebeen associated with antihypertensive use. The additionof a second antihypertensive drug was necessary in 30patients, 13 of whom received dexamethasone therapy
(P= .32). A third antihypertensive drug was required in8 patients, 4 per treatment group.
Complications and blood transfusion
There were 4 maternal deaths, 3 deaths in the dexa-methasone group and 1 death in the placebo group.Three of the maternal deaths occurred in women withliver failure and severe hemolysis, with AST and LDHlevels of O2600 U/L and O6450 U/L, respectively. Theother death was due to a cerebrovascular accident. Thetreatment groups were not different regarding develop-ment of complications or transfusion need (Table IV).Interestingly, there were a higher number of infectionsamong those patients who received placebo, and mater-nal death and pulmonary edema were more frequentamong those women who received dexamethasone ther-apy, even after adjustment. Infections were found to beassociated independently with admission to the intensivecare unit (odds ratio, 10.4; 95% CI, 2.2-48.2), renalfailure (odds ratio, 8.8; 95% CI, 1.9-38.8), and vaginaldelivery (odds ratio, 6.7; 95% CI, 1.3-33.3). The higherodds of infection with vaginal delivery remained afteradjustment for the occurrence of premature rupture ofmembranes and the use of antibiotics and steroids

1596 Fonseca et al
Table III Determinants of duration of hospitalization, platelet count, LDH and AST recovery by univariate Cox regression
Duration of hospitalization Platelets* LDHy ASTz
Hazard ratiox 95% CI Hazard ratiox 95% CI Hazard ratiox 95% CI Hazard ratiox 95% CI
TreatmentPlacebok 1 1 1 1Dexamethasone 1.3 0.87-1.94 1.2 0.80-1.77 0.9 0.53-1.52 0.6 0.39-1.05
Steroid use up to 2 weeks before deliveryNok 1 1 1 1Yes 0.9 0.60-1.46 0.9 0.59-1.43 1.0 0.58-1.88 1.2 0.73-2.12
DeliveryVaginalk 1 1 1 1Cesarean 0.8 0.51-1.27 0.7 0.47-1.09 1.2 0.68-2.17 1.4 0.8-2.33
Class HELLP at admisionHELLP 1k 1 1 1 1HELLP 2 0.8 0.54-1.28 1.2 0.79-1.81 1.3 0.76-2.32 0.9 0.56-1.5
Acute renal failure at admissionNok 1 1 1 1Yes 0.3 0.15-0.44 0.5 0.22-0.99 0.3 0.07-1.17 0.5 0.17-1.36
Urinary output at admision!30 cc/hourk 1 1 1 131-100 cc/hour 4.7 1.94-11.52 2.4 1.07-5.17 1.2 0.47-3.26 1.3 0.50-3.46O100 cc/hour 5.8 2.13-15.80 2.6 1.07-6.22 0.8 0.23-2.45 1.9 0.64-5.46
* Platelets above 100,000/mm3.y LDH below 600 U/L.z AST below 70 U/L.x Non-adjusted Hazard ratio.k Reference category.
before randomization. Platelet transfusion was found tobe associated with the development of renal failure(odds ratio, 4.0; 95% CI, 1.1-14.3) and AST levels atenrollment.
Subgroup analysis by pregnantand puerperal patients
Stratified analysis of pregnant and puerperal groupsshowed no differences in the occurrence of complica-
Table IV Complications associated with HELLP syndromeaccording to steroids use
ComplicationPlacebon (%)
Dexamethasonen (%)
R.R. crude(95% CI)
Acute renalfailure*
8 (12.9) 6 (10.0) 0.8 (0.29-2.10)
Oliguria 4 (6.06) 5 (7.58) 1.3 (0.35-4.45)Pulmonary
edema*1 (1.54) 3 (4.62) 3.1 (0.32-28.09)
Eclampsia 10 (15.15) 8 (13.79) 0.8 (0.34-1.90)Infections 10 (15.15) 5 (7.58) 0.5 (0.18-1.38)Dead 1 (1.52) 3 (4.62) 3.0 (0.32-28.1)Platelets
transfusion10 (15.15) 12 (18.18) 1.2 (0.56-2.58)
Plasmatransfusion
6 (9.09) 5 (7.58) 0.8 (0.27-2.60)
* Only included patients without the event before randomization.
tions, recovery of laboratory parameters, transfusionneed, or duration of hospitalization. Among puerperalwomen, the mean duration of hospitalization tended tobe lower in those women who received placebo than inthose women who received dexamethasone therapy (6.8vs 8.2 days), but this difference was not significant.Median duration was 4 days in both groups; theinterquartile ranges were 3 to 9 days and 3 to 6 days,respectively. Among pregnant women, the duration ofhospitalization was lower in the women who receiveddexamethasone therapy (4.5 vs 9.9 days), but thisdifference did not reach statistical significance. TheFigure 3 Interval between randomization and recovery of theplatelet count to O100,000/mm3 by study group amongpatients with HELLP 1.

Fonseca et al 1597
Table V Randomized clinical trials of corticosteroids in HELLP syndrome
Author Year Number of subjects Antepartum Postpartum Placebo controlled Double blind Benefical effect Ref
Magann 1994 25 Yes No No No Yes 8Magann 1994 25 No Yes No No Yes 9Vigil-De Gracia 1997 34 No Yes No No Yes 10Yalcin 1998 30 No Yes No No Yes 11Isler 2003 32 No Yes No No Yes 19Present work 2005 132 Yes Yes Yes Yes No
median duration was 4 days in both groups, and theinterquartile ranges were 3 to 4.5 days and 3 to 7 daysfor dexamethasone therapy and placebo, respectively.
Subgroup analysis by severity
The time to recovery of the platelet count was found tobe heterogeneous when the cases were stratified byHELLP class at the time of enrollment (Mantel-Coxtest: chi-squared test, 4.76; P = .03). Therefore, weperformed a subgroup analysis according to severity atenrollment. No differences were found among patientswho were classified as HELLP class 2 and controlsubjects; however, among 49 patients with HELLP1 (28 patients with placebo and 21 patients with dexa-methasone therapy), the conditional probability ofplatelet recovery was higher in those patients whoreceived dexamethasone therapy (Figure 3), even afteradjustment for potential confounders (hazard ratio, 3.4;95% CI, 1.3-8.5). Also, the duration of hospitalizationwas shorter among women who received dexamethasonetherapy when means (4.6 and 10.4 days), medians (3.5and 5.0 days), and interquartile ranges were compared.This trend persisted after adjustment (P = .03).
Comment
Several randomized clinical trials have been published toevaluate the effect of dexamethasone therapy in womenwith HELLP syndrome.9-11 Although they indicate thatdexamethasone therapy is beneficial, the strength of thisconclusion is limited because of small number of patientsin each trial, the lack of blinding and placebo controls,the inclusion of women with mild forms of the disease,and the lack of an strict definition of the syndrome (TableV). Observational studies have also found better out-comes in patients with HELLP syndrome who receiveddexamethasone therapy. However, 2 of the studies wereretrospective, with historic control groups,17,18 and theother 2 studies compared different steroids.19,20
To the best of our knowledge, this is the largestreported clinical trial to evaluate the use of dexameth-asone therapy in HELLP syndrome and the first that isdouble blind and placebo controlled. This is also the first
study among patients with HELLP syndrome thatreport sample size estimation. The estimate was basedon the duration of hospitalization because it has beenwidely accepted that this outcome variable reflects thedevelopment of complications and the rate of recoveryof clinical and laboratory variables and because it is auseful indicator for patients and clinicians. Other valu-able features in this study that support its internalvalidity are the study design (stratified randomizationin blocks and double blind) and the small number ofprotocol violations that result in compliance with theassigned treatment of O95%. The external validity ofthis study is also high probably because of the largenumber of eligible patients who accepted randomiza-tion, the adoption of a widely accepted dose of dexa-methasone for the treatment group, the use ofbetamethasone in preterm deliveries, and the clinicalrelevance of the outcome measures.
A weakness of this study is that 28.03% of ourpatients received betamethasone during the 2 weeksbefore delivery for the purpose of accelerating fetal lungmaturity and preventing neonatal intracranial bleeding.However, analyses were carried out to adjust by previ-ous steroid administration (Table III). Furthermore,analyses were carried out that included only women whodid not received other steroids before delivery (45women in the placebo group and 50 women in thedexamethasone group; power, O90%; a, .05) withsimilar results; therefore, previous administration ofbetamethasone did not affect final results.
The results of this study indicate that the adminis-tration of dexamethasone in patients with complete class1 and 2 HELLP syndrome, when compared with similarpatients who received placebo, does not reduce thenumber of complications or the need for blood productsadministration or shorten platelets and LDH recovery.These results were consistent in global and plannedsubgroup analysis. Contrasted with previous studies,AST recovery was slower in patients who were assignedto dexamethasone therapy than to placebo, and thisfinding remained in the subgroup analysis. Unfortu-nately, we cannot speculate about the clinical implica-tions of the last finding, given that patient follow-upevaluations finished at the time of platelets recovery,regardless of AST levels.

1598 Fonseca et al
Although no statistically significant differences werefound in the planned analysis of the duration of hospi-talization, those pregnant women who received placebostayed, on average, twice as long as those women whoreceived dexamethasone therapy (9.9 vs 4.5 days). Thisdifference was due to 2 patients of the control groupwho stayed long periods (49 and 89 days), one of whomhad rupture of the uterus and subsequent complications,and the other who refused blood transfusion, regardlessof clinical indication (hemoglobin levels of 6.2 and 2.8 g/dL before and after cesarean delivery), and experiencedrespiratory distress syndrome and renal failure thatprolonged the hospitalization. These 2 outliers affectedthe mean duration of hospitalization, but comparisonsof median and interquartile range did not show differ-ences between groups.
Subgroup analysis according to the severity of diseaseshowed that, among patients with HELLP 1, there werea shorter average time to platelet recovery and lessduration of hospitalization in women who receiveddexamethasone therapy. The importance of this findingis diminished because this was an unplanned analysisand the severity of the disease was not taken intoaccount at randomization. It is accepted that the resultsof an unplanned subgroup analysis should be consideredexploratory.21
In summary, the results of this investigation do notsupport the use of dexamethasone for treatment ofHELLP syndrome. In women with class 1 HELLP,further studies would be required to evaluate thepotential benefit of this intervention.
Acknowledgments
We thank the residents in Obstetrics and Gynecology atthe University Hospital, Universidad del Valle, Cali,Colombia, for their help in this project.
References
1. Pritchard JA, Weisman R, Ratoff OD, Vosburg GJ. Intravascular
hemolysis, thrombocytopenia, and other hematologic abnormali-
ties associated with severe toxemia of pregnancy. N Engl J Med
1954;250:89-98.
2. Romero R, Vizoso J, Emamian M, Duffy T, Riely C, Halford T,
et al. Clinical significance of liver dysfunction in pregnancy-in-
duced hypertension. Am J Perinatol 1988;5:146-51.
3. Romero R, Mazor M, Lockwood CJ, Emamian M, Belanger KP,
Hobbins JC, et al. Clinical significance, prevalence, and natural
history of thrombocytopenia in pregnancy-induced hypertension.
Am J Perinatol 1989;6:32-8.
4. Weinstein L. Syndrome of hemolysis, elevated liver enzymes, and
low platelet count: a severe consequence of hypertension in
pregnancy. Am J Obstet Gynecol 1982;142:159-67.
5. Sibai BM. Diagnosis, controversies, and management of the
syndrome of hemolysis, elevated liver enzymes, and low platelet
count. Obstet Gynecol 2004;103:981-91.
6. Martin JN, Blake PG, Perry KG, McCaul JF, Hess LW, Martin
RW. The natural history of HELLP syndrome: patterns of disease
progression and regression.Am JObstetGynecol 1991;164:1500-13.
7. Magann EF, Martin RW, Isaacs JD, Blake PG, Morrison JC,
Martin JN. Corticosteroids for the enhancement of fetal lung
maturity: impact on the gravida with preeclampsia and the HELLP
syndrome. Aust N Z J Obstet Gynaecol 1993;2:127-31.
8. Magann EF, Bass D, Chauhan SP, Sullivan DL, Martin RW,
Martin JN. Antepartum corticosteroids: disease stabilization in
patients with the syndrome of hemolysis, elevated liver enzymes,
and low platelets (HELLP). Am J Obstet Gynecol 1994;171:
1148-53.
9. Magann EF, Perry KG, Meydrech EF, Harris RL, Chauchan SP,
Martin JN. Postpartum corticosteroids: accelerated recovery from
the syndrome of hemolysis, elevated liver enzymes and low
platelets (HELLP). Am J Obstet Gynecol 1994;171:1154-8.
10. Vigil-De Gracia P, Garcia-Caceres E. Dexamethasone in the
post-partum treatment of HELLP syndrome. Int J Gynecol Obstet
1997;59:217-21.
11. Yalcin OT, Sener T, Hassa H, Ozalp S, Okur A. Effects of
postpartum corticosteroids in patients with HELLP syndrome. Int
J Gynecol Obstet 1998;61:141-8.
12. Sibai BM. The HELLP syndrome (hemolysis, elevated liver
enzymes and low platelets): Much ado about nothing? Am J
Obstet Gynecol 1990;162:311-6.
13. Piantadosi S. Clinical trials: a methodologic perspective. New
York: Wiley-Interscience; 1997.
14. Hosmer D, Lemeshow S. Applied logistic regression. New York:
Wiley-Interscience; 1989. p. 307.
15. Stata Reference Manual: release 6. vol. 3. College Station (TX):
Stata Press; 1999. p. 392-4.
16. Hosmer D, Lemeshow S. Applied survival analysis: regression
modeling of time to event data. New York: Wiley-Interscience;
1999.
17. Martin JN, Perry KG, Blake PG, May WA, Moore A, Robinette
L. Better maternal outcomes are achieved with dexamethasone
therapy for postpartum HELLP (hemolysis, elevated liver en-
zymes, and thrombocytopenia) syndrome. Am J Obstet Gynecol
1997;177:1011-7.
18. Varol F, Aydin T, Gucer F. HELLP syndrome and postpartum
corticosteroids. Int J Gynecol Obstet 2001;73:157-9.
19. Isler CM, Magann EF, Rinehart BK, Terrone DA, Bass JD,
Martin JN. Dexamethasone compared with betamethasone for
glucocorticoid treatment of postpartum HELLP syndrome. Int J
Gynecol Obstet 2003;80:291-7.
20. Tompkins JM, Thiagarajah S. HELLP (hemolysis, elevated liver
enzymes, and low platelet count) syndrome: the benefit of corti-
costeroids. Am J Obstet Gynecol 1999;181:304-9.
21. Assmann SF, Pocock SJ, Enos LE, Kasten LE. Subgroup analysis
and other (mis)uses of baseline data in clinical trials. Lancet 2000;
355:1064-9.