Embed Size (px)
DESCRIPTION
Covering the latest articles, dental congresses, and the innovation in dental products.
Citation preview

www.dentalnews.com Volume XXII, Number I, 2015
SDA8th Sudanese Dental AssociationConference
KDA18th Kuwait Dental AssociationInternational Scienti�c Conference
STAYCONNECTED
SDS26th Saudi Dental Society
International Dental Conference
AEEDC 201519th UAE International Dental Conference, Dubai

Dental News, Volume XXII, Number I, 2015


Dental News, Volume XXII, Number I, 2015
A strong bond provides confidence and support
• Powerful luting materials
• Tried-and-tested product combinations
• A wide collection for different demands:
ESTHETICS | UNIVERSALITY | SIMPLICITY
Variolink® N | Multilink® N | Multilink® Speed
www.ivoclarvivadent.comIvoclar Vivadent AGBendererstr. 2 | 9494 Schaan | Principality of Liechtenstein | Tel.: +423 / 235 35 35 | Fax: +423 / 235 33 60
Luting materials from Ivoclar Vivadent
N-Cement Collection
N-Cement Collection_INS_e_A4.indd 1 29.05.13 15:28
KaVo Dental GmbH · Arjaan Tower 9th Floor · Dubai Media City, UAE · PO Box 71569 Phone +971 4 433 21 86 · Fax +971 4 457 93 73 · Email: [email protected] · www.kavo.com/mea
KaVo DIAGNOcam – a whole new perspective on caries
• Significantly improved diagnosis quality – in unsurpassed image quality
• Ideal for patient information and outstanding monitoring
• X-ray-free imaging method for caries identification
KaVo DIAGNOcam – simply illuminating
Images that change your world.
Find out more about KaVo DIAGNOcam:
www.kavo.com/diagnocam
KaVo DIAGNOcam

A strong bond provides confidence and support
• Powerful luting materials
• Tried-and-tested product combinations
• A wide collection for different demands:
ESTHETICS | UNIVERSALITY | SIMPLICITY
Variolink® N | Multilink® N | Multilink® Speed
www.ivoclarvivadent.comIvoclar Vivadent AGBendererstr. 2 | 9494 Schaan | Principality of Liechtenstein | Tel.: +423 / 235 35 35 | Fax: +423 / 235 33 60
Luting materials from Ivoclar Vivadent
N-Cement Collection
N-Cement Collection_INS_e_A4.indd 1 29.05.13 15:28

Dental News, Volume XXII, Number I, 2015
hydrorise

hydrorise3
ADVERTISING INDEX
ARTICLES CONGRESSES
64.
68.
60.
56.
How to Prevent Failure of Veneered Zirconia Ceramic
Variations of Periotest Values at Different Prosthetic Implant Stages: A Pilot Study
SDS 2015 - 26th Saudi DentalSociety Int’l Dental Conference
AEEDC 2015 - 19th UAEInternational Dental Conference& Arab Dental Exhibition
SDA 2014 - 8th SudaneseDental Association Conference
KDA 2014 - 18th Kuwait DentalAssociation InternationalScientific Conference
3SHAPE 7ACE Surgical 19ACTEON 35A-DEC 57 BA International 19BIEN AIR 65 BISCO 23CARESTREAM 44 CAVEX 6 COLTENE 17DENTAURUM 15DENTSPLY 13DEPURDENT 4DURR 61EMOPHORM 5 FKG 22
GC 9 GSK C3, 8, 29, 39 GENDEX 67HENRY SCHEIN 43HU FRIEDY 47ITENA 33IVOCLAR 1, C4KAVO C2 KERR 63MECTRON 55 MEDESY 21MICRO MEGA 31 MORITA 53NSK C1ORMCO 37ORTHO ORGANIZERS 42
18.
12.
30.
46.
38.
Dental News, Volume XXII, Number I, 2015
Polyamide Resins in Removable Dentures
Direct Replacement of Anterior Tooth with Fiber-Reinforced Composite and Natural Tooth Pontic: A Case Report
Coronectomy
January 13 - 15Riyadh, KSA
February 17 - 19, 2015Dubai, UAE
December 2 - 4, 2014Khortoum, SUDAN
November 19 - 22, 2014Jumeirah Messilah Beach, KUWAIT
Dr. Elias Smaira, Dr. Mireille Rahi,Dr. Najib Abou Hamra, Dr. Danielle El Hakim
Dr. Danielle El Hakim, Dr. Mireille Rahi,Dr. Najib Abou Hamra, Dr. Elias Smaira
Pr. Mayada Jemâa, Pr. Bassem Khattech,Pr. Nouha Mghirbi, Pr. Hayet Hajjami,Pr. Sonia Zouiten, Pr. Abdellatif Boughzala
Dr. P. Dhanrajani, Dr. R. Weld-Moore
Dr. Ghassan Moustapha, Dr. Habib Abi Aad,Dr. Elias Smaira
PLANMECA 27RITTER 51SCHEU 71SIRONA 25SOREDEX 49VOCO 45 W&H 59 ZHERMACK 2ZIRLUX 51ZOOM PHILIPS 10

Dental News, Volume XXII, Number I, 2015
DEPURDENT For dazzling white teeth
• Free from chemical bleaching substances, preservatives and enzymes
• Eliminates easily plaque and stains of tea, nicotine, coffee and fruits
• Contains the natural active ingredient pumice
• For professional and home use
DEPURDENT® cleaning and polishing paste for a brilliant smile
DEPURDENT® Mouthrinse - The perfect supplement to DEPURDENT® cleaning and polishing paste!
• Its special formula prevents the formation of plaque and stains and helps to retain the natural white color of the teeth.
• Fluoride protects against caries.• Refreshing taste for long-lasting fresh breath.
®
Dr. Wild’s Mideast Regional Office: Actco, P.O. Box 40746, Larnaca 6306, Cyprus, Tel.: (24) 623515 / 654252, Fax: (24) 623844. E-Mail: [email protected]: Awal Pharmacy, East Riffa, Bahrain. Egypt: Sesic, Alexandria. Jordan: Areel for Cosmetics Trading, Amman. Kuwait: Al-Maseela Pharmaceutical Co., Safat. Lebanon: A.M.G. Medical.Jdeideh-Azur Center. Libya: Al Osra, Benghazi. Oman: Ibn Sina Pharmacy L.L.C., Muscat. Qatar: Masar Medical, Doha. Saudi Arabia: Depot Pharmaceutique du Moyen Orient, Jeddah. United Arab Emirates: Al Hayat Pharmaceuticals, Sharjah. Yemen: Al Rawdha Trading Group, Sana’a.
Dr. Wild & Co. AG www.wild-pharma.com Swiss professional oral care
Dental_News-DEPURDENT.indd 1 04.02.15 14:38
Special toothpaste and mouthbath with Ems salts for sensitive teeth and denuded toothnecks, irritations ofthe gums, plaque
• desensitizes teeth and denuded toothnecks
• firms up the gums and combats dental plaque
• neutralizes acids harmful to the teeth
Special toothpaste and mouthbathfor sensitive teeth and denuded toothnecks, caries prophylaxis andgum care
• desensitizes teeth and denuded toothnecks
• caries prophylaxis
• stimulates salivation
Alcoholfree
Alcoholfree
Bahrain: Awal Pharmacy, East Riffa, Bahrain. Egypt: Sesic, Alexandria. Jordan: Areel for Cosmetics Trading, Amman. Kuwait: Al-Maseela Pharmaceutical Co., Safat. Lebanon: A.M.G. Medical.Jdeideh-Azur Center. Libya: Al Osra, Benghazi. Oman: Ibn Sina Pharmacy L.L.C., Muscat. Qatar: Masar Medical, Doha. Saudi Arabia: Depot Pharmaceutique du Moyen Orient, Jeddah. United Arab Emirates: Al Hayat Pharmaceuticals, Sharjah. Yemen: Al Rawdha Trading Group, Sana’a.
Dr. Wild & Co. AG www.wild-pharma.com Swiss professional oral care

Special toothpaste and mouthbath with Ems salts for sensitive teeth and denuded toothnecks, irritations ofthe gums, plaque
• desensitizes teeth and denuded toothnecks
• firms up the gums and combats dental plaque
• neutralizes acids harmful to the teeth
Special toothpaste and mouthbathfor sensitive teeth and denuded toothnecks, caries prophylaxis andgum care
• desensitizes teeth and denuded toothnecks
• caries prophylaxis
• stimulates salivation
Alcoholfree
Alcoholfree
Bahrain: Awal Pharmacy, East Riffa, Bahrain. Egypt: Sesic, Alexandria. Jordan: Areel for Cosmetics Trading, Amman. Kuwait: Al-Maseela Pharmaceutical Co., Safat. Lebanon: A.M.G. Medical.Jdeideh-Azur Center. Libya: Al Osra, Benghazi. Oman: Ibn Sina Pharmacy L.L.C., Muscat. Qatar: Masar Medical, Doha. Saudi Arabia: Depot Pharmaceutique du Moyen Orient, Jeddah. United Arab Emirates: Al Hayat Pharmaceuticals, Sharjah. Yemen: Al Rawdha Trading Group, Sana’a.
Dr. Wild & Co. AG www.wild-pharma.com Swiss professional oral care

Dental News, Volume XXII, Number I, 2015
CAVEXYOUR IMPRESSION IS OUR CONCERN Cavex Holland BV, P.O. Box 852, 2003 RW Haarlem, The Netherlands. Tel +31 23 530 77 00 Fax +31 23 535 64 82 [email protected] www.cavex.nl
Cavex AlginatesSuperior in strength, control and balance
Cavex ColorChange• 9 days dimensional stable• Fast set• Functional colour change
Cavex Impressional• Extremely elastic• Normal and fast set
Cavex Orthotrace• Firm consistency• Firm consistency• Developed for the orthodontic practice• Developed for the orthodontic practice• Extra fast setting• Extra fast setting
5 years shelf life
snap-setsuperior tearresistance
Cavex ImpreSafe• Kills bacteria, viruses an fungi in just 3 minutes• 1litre of concentrate for over 30 weeks disinfected impressions• Safe for alginate, polyether and silicone impressions
2011
Top Infection Control Product
Cavex GreenClean• The effi cient alginate and gypsum remover• The effi cient alginate and gypsum remover• Fresh lemon aroma• Fresh lemon aroma• 1 jar = 500 clean trays!• 1 jar = 500 clean trays!
ad algsystem WB dentalnews 205x275.indd 1 28-10-13 08:27

TRIOS® - MORE THAN AN IMPRESSION
DIGITAL IMPRESSIONS IN LIFELIKE COLORS
MEASURE TEETH SHADES AS YOU SCAN
HD PHOTOS FOR SUPREME MARGIN DETECTION
Choose the optimal TRIOS® solution for your clinic – Cart, Pod, Chair Integrationwww.3Shapedental.com/TRIOS
Shade Measurement
A1 A2 A3 A3.5 A4
HD PhotosColor Digital Impressions

Dental News, Volume XXII, Number I, 2015
Clinically proven relief from the pain of sensitivity*1-4
Gently lifts stains and help prevent new stains from forming5-7
Ultra-low abrasive formulation appropriate for your patients with exposed dentine8
*With twice-daily brushing References.. 1. Jeandot J et al. Clinc (French) 2007; 28: 379–384. 2. Nagata T et al. J Clin Periodontol 1994; 21(3): 217–221. 3. GSK data on file. DOF Z2860473. 4. Leight RS et al. J Clin Dent 2008 19(4) 147-153. 5. Schemehorn BR et al. J Clin Dent 2011 22(1) 11-18. 6. Shellis RP et al. J Dent 2005 33(4) 313-324. 7. GSK data on file. DOF Z2860415. 8. GSK data on file. DOF Z2860435.
Recommend Sensodyne – specialist expertise for patients with dentine hypersensitivity
Arenco Tower, Media City, Dubai, U.A.E.Tel: +971 4 3769555, Fax: +971 3928549 P.O.Box 23816.For full information about the product, please refer to the product pack.For reporting any adverse event/side effect related to GSK product, please contact us on [email protected] Prepared: December 2014, CHSAU/CHSENO/0034/14f.
Ultra-low abrasion for your patients who need sensitivity relief and seek gentle whitening
We value your feedbackSaudi Arabia: 8008447012All Gulf and Near East countries: +973 16500404

GC EUROPE N.V. Head Office Tel. +32.16.74.10.00 [email protected] http://www.gceurope.com
The of creating
smiles.
Welcome to the
GC G-ællery –
aesthetic solutions
for every case …
with exactly the handling
you prefer
G-ænial from GC
www.gceurope.com
165249-GC-GAENIAL FAMILY-POST-850x1050-E.indd 1 20/01/14 08:45

Dental News, Volume XXII, Number I, 2015
* #The 1 patient-requested
professional whitening systemis now better than ever.
*In the United States.Philips is a registered trademark of Koninklijke Philips Electronics N.V. ©2011 Discus Dental, LLC. All rights reserved. To be dispensed by or on the order of a dental professional only. ADV-3529 111011
The new Philips Zoom WhiteSpeed Light-Activated Whitening System is now better than ever with an advanced LED light technology and variable settings that help you maximize patients comfort and minimize operating costs. You’ll have the answer to the con�dent and beautiful smile your patients are asking for!

* #The 1 patient-requested
professional whitening systemis now better than ever.
*In the United States.Philips is a registered trademark of Koninklijke Philips Electronics N.V. ©2011 Discus Dental, LLC. All rights reserved. To be dispensed by or on the order of a dental professional only. ADV-3529 111011
The new Philips Zoom WhiteSpeed Light-Activated Whitening System is now better than ever with an advanced LED light technology and variable settings that help you maximize patients comfort and minimize operating costs. You’ll have the answer to the con�dent and beautiful smile your patients are asking for!
INTERNATIONAL CALENDAR11
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg.
POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: [email protected]
Website: www.dentalnews.com
www.facebook.com/dentalnews1
www.facebook.com/dentalnews1
twitter.com/dentalnews
Dental News App on both
Appstore & Google play
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY
IN THE MIDDLE EAST & NORTH AFRICA IN
COLLABORATION WITH THE COUNCIL OF DENTAL
SOCIETIES FOR THE GCC.
Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
Alfred Naaman, Nada Naaman,Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-JammazSuha NaderElie HajjMicheline Assaf, Nariman NehmehJosiane YounesAlbert SaykaliGisèle Wakim, Marielle KhouryTony Dib1026-261X
EDITORIAL TEAM
COORDINATORART DEPARTMENT
SUBSCRIPTIONADVERTISING
PHOTOGRAPHYTRANSLATION
DIRECTORISSN
Volume XXII, Number I, 2015w w w.d e n ta ln ew s .co m
This magazine is printed on FSC – certified paper.
18th APEC and 4th Jordanian Endodontic Conference 2015
April 8 - 10, 2015at Le Royal Hotel, Amman, JORDANEmail: [email protected] Website: www.apec2015.jo
Dental News, Volume XXII, Number I, 2015
The International Team for Implantology Congress Middle East
October 15 - 16, 2015Dead Sea, JORDANEmail: [email protected]: www.iti.org
The Egyptian Dental Association Meeting
November 11 - 13, 2015Cairo, EGYPTEmail: [email protected]
10th CAD/CAM &Computerized Dentistry International Conference
May 8 - 9, 2015at the Jumeirah Beach Hotel,Dubai, UAEEmail: [email protected]: www.capp-asia.com
The Lebanese University International Convention
May 13 - 16, 2015 Beirut, LEBANON Website: www.ul.edu.lb
ICOI International Implant Symposium
April 16 - 18, 2015at the Saint Joseph University, Dental School, Damascus road, Beirut, LEBANONEmail: [email protected]: 00961 1 421268
October 8 - 10, 2015at the BIEL, Beirut, LEBANONWebsite: www.bidm-lda.com
BIDM 2015 - The 25th Lebanese Dental Association Congress
ASIA PACIFIC DENTAL CONGRESS 2015
April 9 - 10, 2015at the Suntec, SINGAPOREEmail: [email protected]: www.apdc2015.sg
7th Dental-Facial Cosmetic International Conference
November 13 - 14, 2015at the Jumeirah Beach Hotel,Dubai, UAEEmail: [email protected] Website: www.capp-asia.com
AIO 2015 The Italian Dental Association Congress
June 11 - 13, 2015at the Chia Laguna Resort in Sardinia, ITALY Website: www.congress2015.aio.it
FDI 2015 Annual World Dental Congress
September 22 - 25, 2015Bangkok, THAILANDEmail: [email protected] Website: www.fdi2015bangkok.org

Dental News, Volume XXII, Number I, 2015
Variations of Periotest Values at Different Prosthetic Implant Stages: A Pilot Study
12
Implant Dentistry
AbstractPeriotest values seem to differ between the gingiva former, abutment placement and after single crown cementation on implants.
Material and Methods28 patients were selected and measurements were taken on 42 implants at the gingiva former level, abutment level and after single crown cementation. Mean values of all stages were then calculated and compared.
ResultsAn increased mean value of 2.7 was noted between the gingiva former and single crown final stages.
ConclusionPositif Periotest values on implant single crown might be considered normal when the healing abutment measurements range between -3 and 0.
IntroductionTo evaluate the degree of osseointegration, various methods have been proposed: histology and histophotometry,1 removable torque analysis,2 pull and push through tests3 and x-ray examination.4 However, due to problems of invasiveness and inaccuracy new devices were needed. The Periotest device (Siemens AG, Bensheim, Germany) Fig.1 is an instrument specially developped for the diagnosis of periodontal diseases.5 It can also be used to assess the bone anchorage of implants6,7,8 and monitor their stability.9 The range in Preiotest®
values (PTV), shown by clinically immobile dental implants, depends on the damping characteristics of the surrounding tissues (bone in successful implants and fibrous tissues in failed implants).10
Periotest measurements give better results when measurements are made bucally during intra and interobserver tests. It is a reliable technique for the quantification of the implant stability.11 When comparing the Periotest to other systems, the Periotest is reliable on implants with a good stability and is more reliable when implants are less stable.12
A successful implant value should be inferior to zero as directed by the fabricant, but some positif measurements were collected on well anchored implants when taken at different steps of the prosthetic treatment. That is why further investigation was needed.The purpose of this study was to determine the periotest mean values of measurements for implants at 3 different restoration stages: gingiva former in place, abutment screwed on implant and single crown after cementation, in order to determine the variations of these mean values.
Dr. Elias Smaira
Dr. Mireille Rahi
Dr. Najib Abou Hamra
Dr. Danielle El Hakim
Fig 1: Periotest Device
Fig 1

DENTSPLY Ltd | Building 3 | The Heights | Weybridge | KT13 0NY | United KingdomPhone: +44 (0) 1932 853422 | www.dentsplymea.com
UKX
L935
. Dat
e O
f Pre
para
tion
Febr
uary
201
5
293 One Brand Advert 205 x 275 FINAL:Layout 1 3/2/15 18:37 Page 1

Dental News, Volume XXII, Number I, 2015
14
4
0
-4
2
-2
-6
-8
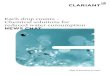
Gingival Former Crown Abutment Single Crown
Material and Methods42 implants (36 Deukega, 6 Zimmer suiss plus)on 28 patients were selected for the periotest measurements: 15 in the mandibule and 27 in the maxilla. The mean age of the patients was 52.2, the youngest was 38 and the eldest 74 years old. 16 weeks after implant placement the measurements at each implant were taken, first with the gingiva former in place, then with the crown abutment (Deukega solid abutment) Fig. 2, and finally after delivery of the final single crown. The prostethis was delivered in an average of 18 weeks after implant placement. The crown abutment was fastened with a torque ratchet at 30N. The crown measurement was performed after cementation with glass ionomer luting cement (Ketac Cem 3M Espe). The periotest measurement was performed as directed by the fabricant and: 2mm above the cervical gingiva. At least two measurements were made for each implant, if measured values were divergent, the measurement was continued until two subsequent values were identical.13 This value was then noted on the data sheet. Mean values on each three groups were calculated and compared, using descriptive
ResultsTable 1 and fig. 3 show the average differences and changes in the periotest measurements between the values of the placed gingiva formers, crown abutments, and recently placed single crowns. These changes amounting to -1.47 or -1.23 significantly differed from 0. The periotest value increased by 2.7 from gingiva former stage until the single crown placement.
DiscussionThe Periotest device has the advantage of measuring the implant stability at any stages from implant placement to crown elaboration and even many years after the crown cementation. Most of the studies determined the reliability of Periotest on implant stability with all measurements taken at the gingiva former stage only.11 German et al. conducted a study comparing the measurements of the Periotest at the 3 stages of the crown elaboration (gingiva former, abutment placement, crown cementation) using 2 different types of abutments. They found a main value increase of 3.5 between measurements taken at the gingiva former stage and at the final single crown cementation.13
To check these findings using one type of abutments instead of two was of great interest. It was obvious that Periotest measurements at the three stages were not identical and were increasing. (fig 2)The Periotest measurements on implants were made 2 mm above the cervical gingiva in order
Fig 2: Deukega Solid Abutments
Fig 2
Fig 3
statistical tests (mean and averages), in order to determine the difference between the three groups.
Fig 3: Difference between the three stages values
Implant Dentistry
High
Low
Close

Visit us!10. – 14. March 2015
Hall 10.1 Stand E10/F11
2015YearsImplantology.
Turnstraße 31 I 75228 Ispringen I Germany I Phone + 49 72 31 / 803 - 0 I Fax + 49 72 31 / 803 - 295www.dentaurum-implants.de I [email protected]
A Dentaurum Group company
YESI WANTTHE COMPLETECAD/CAM SOLUTION.
Innovation has a name: tioLogic® digital. Your step towards digital implantology. Say yes!
EN_2901_YES_CADCAM_205x275_mStörer.indd 1 02.02.15 08:27

Dental News, Volume XXII, Number I, 2015
16
Average Change
Maximum Change
Minimum Change
Total Average Change = -2.7
Gingiva Former
-1.47
-3.8
+0.1
-1.23
-3.8
-0.3
Crown Abutment Single Crown
Table 1 : individual differences in Periotest values
1. Ericsson i, Johansson cB, BystEdt h, norton Mr. a histoMor-phoMEtric Evaluation of BonE to iMplant contact on MachinE-prEparEd and roughEnEd titaniuM dEntal iMplants. apilot study in thE dog.oral iMplant rEs.1994;5:202-206.2. WEnnErBErg a, alBErktson t, andErson B, krol JJ. a histoMor-phoMEtric and rEMoval torquE study of scrEW shapEd titaniuM iM-plants With thrEE diffErEnt surfacE topographiEs. clin.oral iMplants rEs.1995;6:24-30.3. dhErt WJ, vErhEyEn cc, Braak lh, dE WiJn Jr, klEin cp, dE groot k, rozing pM. a finitE ElEMEnt analysis of thE push-out tEst: influEncE of tEst conditions. J.BioMEd.MatEr.rEs.1992;26:119-130.4. MErEdith n. assEssMEnt of iMplant staBility as a prognostic dEtEr-Minant.int.J.prosthodont.1998;11:491-501.5. shultE W, lukas d, ErMst E. pEriotEst valuEs and tooth Mo-Bility in pEriodontal disEasE: a coMparativE study. quintEssEncE int 1990;21:289-293.6. huang h.M., chiu c.l., yEh c.y., lin c.t., lin l.h., lEE s.y. Early dEtEction of iMplant hEaling procEss using rEsonancE frEquEncy analysis. clin. oral iMplants rEs. 2003;14:437–443. 7. chavEz h,ortMan lf , dE franco rl, MEdig J.assEssMEnt of oral iMplant MoBility. J,prosthEt.dEnt.1993;70:421-426.8. stEflik dE, WhitE sl, parr gr Et al. clinical Evaluation data froM a coMparativE dEntal iMplant invEstigation in dogs. J.oral.iMpl.1993;19:199-208.9. tEErlink J,quirynEn M, darius p, van stEEnBErghE d. pEriotEst:an oBJEctivE clinical diagnosis of BonE apposition toWard iMplants. int. J. oral Maxillofac. iMplants.1991;6:55-61.10. alBrEktsson t., JacoBsson M. BonE–MEtal intErfacE in ossEointE-gration. J. prosthEt. dEnt. 1987;57:597–607.11. Bilhan h, cilingir a,Bural c,BilMEnoglu c, sakaro o, gEckilio.thE Evaluation of thE rEliaBility of pEriotEst for iMplant staBility MEasurMEnts: an in vitro study. J.oral. iMplantology.2014 Mar 4(EpuB a hEad of print).12. saMEr al JEtaily,aBdullah al farraJ al dosari.assEssMEnt of osstEl and pEriotEst systEM in MEasuring dEntal iMplant staBility(in vitro study).saudi dEntal J. Jan 2011;23(1):17-21.13. gErMan goMEz-roMan, diEtEr lukas. influEncE of thE iMplant aButMEnt on thE pEriotEst valuE: an in vivo study.quintEssEncE int.2001;32(10):797-799.14. cranin an, dEgrado J, kaufMan M,Et al. Evaluation of thE pEriotEst as a diagnostic tool for dEntal iMplants. J oral iMplantol. 1998;24:139-146.15. truhlar rs, lauciEllo f, Morris hf, ochi s. thE influEncE of BonE quality on pEriotEst valuEs of EndossEous dEntal iMplants at stagE tWo surgEry. J oral Maxillofac surg 1997; 55:55-61.
References
Table 1
Implant Dentistry
to eliminate the moment effect. In tissue level implants, this hitpoint will be almost at the same distance from the implant neck for all the implants included in this study.On average, the increased mean value of 2.7 indicates that a positive measurement does not necessarly show a failure. For example, an implant measurement on the healing abutment of -1.5 can lead on average to a +1 to +2 measurment on the single crown. If the fabricant considers zero to be the reference for success of osseointegration this number should be reconsidered when the measurements are performed on the crown itself.The increased mean value may be due to the cement layer interface and to the modulus of elasticity of the abutment screw.Periotest measurments might represent a reliable method for the assessment of the implant-bone interface. If measurements are taken after crown cementation one should take into consideration the increased mean value of 2.712-14-15
ConclusionPeriotest values measured at gingiva formers increased on average by 2.7 after crown cementation.While measurements on the abutment revealed a mean increase of 1.23.Finally, positif Periotest measurements on single crown should be considered as normal when values on healing abutment are between -3 and 0.

0018
55
www.coltene.com/contact
Route to successful endodontics

Dental News, Volume XXII, Number I, 2015
18
How to Prevent Failure of Veneered Zirconia Ceramic
18
Prosthetic Dentistry
AbstractIn spite of high zirconia mechanical strength, chipping and fracture of layering porcelains applied to zirconia frameworks continue to be a problem. The mechanical integrity and the bonding of the layering porcelain to the framework material are key factors in the successful performance of veneer/framework restorations. Another clinical problem with the use of zirconia is the difficulty in achieving suitable adhesion to resin cement. Traditional adhesive techniques used with silica based ceramics do not work effectively with zirconia. This article reviews the literature to find the favored protocol to prevent delamination between veneering materials and zirconia framework from one part; and to focus on currently available techniques for internal surface roughness and preferred approaches for zirconia cementation.
IntroductionSince zirconium dioxide was introduced in dentistry as a framework material for all ceramic restorations, a particular attraction resulted to its use in prosthodontics, due to its excellent mechanical properties (flexural strength 900-1200Mpa, fracture toughness 9,10 Mpa m½) and improved appearance, having a high degree of crack resistance. Due to suitable additives, e.g. yttrium oxide, the crystal lattice is stabilized in its tetragonal high temperature phase, which avoids further transformation into the monoclinic phase, occurring during the cooling process. When a fault takes place; at the beginning of a crack, zirconia grains are transformed locally from tetragonal to monoclinic form, and accompanied by an increase in volume. This procedure is described as transformation toughening.1,2
When properly veneered, it could turn out
to be clinically acceptable regarding its color match and having the capability to mask dark backgrounds such as dark tooth or cast post and core.3
It has promising clinical results and high survival rate. However the mechanical complications reported were chipping of veneering ceramic, framework fracture and loss of retention. Chipping has several causes: inappropriate framework support for the layering porcelain, coefficient of thermal expansion mismatch, firing shrinkage of the ceramic and insufficient bond strength. Finally the structural characteristics of zirconia resist conventional conditioning methods usually employed for bonding traditional ceramic restorations to teeth.1,4
Tooth preparationPreviously, all-ceramic restorations should be placed on a heavy-chamfer or on a shoulder preparation to ensure that it will withstand the stresses that occur in the oral environment.For zirconia, a smaller finish line can be used.5 Its classical preparation should provide 0.5mm (in case of a collar) to 1mm at the margin, 1.2 to 1.5mm at the circumferential wall, and 1.5 to 2mm at the occlusal surface for ceramic and framework thicknesses.2,6 But with the monolithic zirconia restorations, gentle preparation of only 0.5 to 1 mm are indicated.7
The finish line design does not influence the fatigue or the fracture resistance of veneered zirconia crowns. Selection of any of the finish line designs should be based on the clinical condition of the restored tooth.8
Framework designFor optimal success, it is critical that the design of the substructure provides proper support and a uniform thickness of overlay porcelain.
Dr. Ghassan Moustapha
Dr. Mireille Rahi
Dr. Habib Abi Aad
Dr. Elias Smaira

A COMPLETE DENTAL SOLUTION
Infinity Implants from ACE Surgical deliver a truly compatible dental implant
solution at a price that makes sense for your practice. Discover the savings and
outstanding quality across all of our implant lines. To learn more, visit our website
www.acesurgical.com.
ACE Surgical Supply Co., Inc.
Dental Implant Systems
For more information contact your local dealerwebsite: www.acesurgical.com • email: [email protected]
cancel lous and cor t ical granules
resorbable col lagen membrane
resorbable col lagen membrane

Dental News, Volume XXII, Number I, 2015
20
The non-uniform porcelain thickness would heat at different rates which could lead to thicker porcelain areas not being fully processed.9 Therefore a uniform layer thickness between 0.7 and 1.2mm of the veneering ceramic is recommended.2
Using a CAD/CAM, porcelain support begins by applying a full anatomical contour of the crown (Fig. 1). A thickness of 1mm is removed to make space for the layered porcelain (Fig. 2). As presented in (Fig. 3) the final design of the coping leaving proper support for the porcelain. Regarding the connectors dimension, the minimum cross section requirement are 7 mm² for anterior 3 unit bridges, 9 mm² for posterior 3 units bridges or anterior 4 unit bridges and 12 mm² for posteriors 4 units bridges or cantilever bridges. The height of the connector surfaces should be as large as possible.2,6,10
Coefficient of thermal expansionThe ideal coefficient of thermal expansion (CTE) between the zirconia framework and layering porcelain has not been established. The use of layering porcelain with a higher (CTE) than that of the zirconia framework results in veneer delamination and extensive micro crack formation.11 A general trend is to use a slightly lower (CTE) to generate compressive stresses in the weaker veneering ceramic; this technique is used with porcelain fused to metal. In the same manner, to prevent chipping and cracking of the layering porcelain, it is recommended to have CTEs slightly lower than or identical to those of zirconia ceramics.4,12,13
Firing of the ceramicZirconia has the lowest thermal conductivity (2 W/ (mk) base metal 40 W/ (mk)). Consequently, zirconia requires longer duration for heat to be transferred within the material in order to insure even heat distribution in the interfacial area between the framework and the veneer, as well as the outer surfaces of the restoration even with different framework thicknesses. It also requires slowing cooling rate to prevent stresses within the porcelain, to reduce the risk of chipping or delamination, and to obtain the desired compression of the overlay porcelain.6,9
Bond strength between zirconia and layering porcelain To achieve best bond strength between zirconia and layering porcelain, the manufacturer’s instructions should be taken into consideration and applied as per recommended. E.max ZirCAD and VITA In-Ceram YZ don’t allow sandblasting or grinding the framework, since this can damage the surface leading to undesired phase transformation and jeopardize the bond with the layering ceramic. In case of minor correction after sintering, a thermal treatment (regeneration firing) can reverse any phase transformation.2,6 For E.max ZirCAD Zirliner must always be applied prior to the
Fig 1
Fig 2
Fig 3
Prosthetic Dentistry

21
Dental News, Volume XXII, Number I, 2015
layering procedure in order to achieve a sound bond as well as an in depth shade effect and fluorescence. Zirliner has four shades for non shaded zirconia framework or clear for shaded framework.6
With the Lava Zirconia coping, sandblasting the outer surface is not necessary as the milling process results in an adequately rough surface to accept the overlay porcelain. Remarkably, very light sandblasting does not appear to have affected the bonding strength and appears to increase wetting of the porcelain.9
Whereas for the Cercon Degudent, it is advised to sandblast the inside and outside of the framework with alumina (110–125 μm, max 0.3 to 0.4Mpa, 45° angle).10 Applying a liner is indicated for the Cercon framework with the layered porcelain,14 but not required with the pressed porcelain.15
Aboushelib et al. evaluated in 6 papers the microtensile bond strength (MTBS) between the zirconia and the veneering ceramic.11,16,17,18,19,20 (MTBS) was chosen because shear bond strength (SBS) test may lead to undesirable stress distribution, causing cohesive failure and wrong interpretation of the data.When comparing polishing to sandblasting Cercon disc or roughening Vitablocks Mark II, no effect on the core-veneer bond strength was noted. The (MTBS) of the Cercon core-veneer would be weaker if the liner was not applied which is basically used to mask the white color of the zirconia and enhance the bond strength between the core and the veneering porcelain.11
The liner should be used with some layering veneers but not in combination with pressable veneers. The two materials have different structural composition and pressing the veneer ceramic over smooth fired liner material results in poor contact between the two materials. The pressable veneers failed mainly cohesively (within the porcelain) with no liner and interfacially (between the core and veneer) when liner is applied, whereas the layered veneers failed cohesively with liner and interfacially with no liner.16
Using the pressing technique will improve the bond strength while the esthetic outcomes are more difficult to achieve because it depends on the precolored ceramic ingots. Aboushelib et al. introduced a double-veneer technique combining layering porcelain over a previously pressed-on ceramic.17
Hence, the (MTBS) of zirconia and press on ceramic wasn’t affected by the addition of a second layer of veneering esthetic porcelain.When colored zirconia frameworks were introduced to enhance the final esthetics of the layered all-ceramic restoration, Aboushelib et al.18 found that the bond strength of colored zirconia was significantly weaker than the white
Prosthetic Dentistry
MEDESY srl33085 Maniago, PN - ITALY
Viale dell’Industria, 1 - Industrial Areawww.medesy.it - [email protected]

Dental News, Volume XXII, Number I, 2015
22
zirconia frameworks. It was observed that the concentration of the coloring pigments (ferric oxide) was higher at the grain boundaries, which was at the expense of the concentration of the yttrium stabilizing elements.18 Furthermore, sandblasting these yellow samples decreased the bond strength in comparison to the white samples.In the other two papers, Aboushelib et al.19,20 used a new CAD/CAM veneering method to fabricate a resin replica of the esthetic ceramic seated on the zirconia framework and then processed using press on technologies. In comparison to conventional layering the CAD veneered specimens failed cohesively, while conventional layered specimens failed interfacially. Whereas Nakamura et al.21 postulated that sandblasting at a pressure 0.4 Mpa developed a strong bond to veneering porcelain compared to no sandblasting or sandblasting at a pressure of 0.2 Mpa, while using a tensile bond strength test. Yet the study didn’t include any fatigue
testing.One study 22 evaluated the influence of cyclic loading and flexural strength on zirconia after being subjected to particle abrasion with either 50 or 110μm, grinding or polished as control. It was interesting to note that the polished specimens demonstrated the least reduction in flexural strength after cyclic loading. Different surface treatment increased the amount of surface damage and the number of already available surface cracks ready to propagate.The (SBS) between zirconia and veneering ceramics wasn’t affected by thermocycling,23
however, the metal ceramic group in this study exhibited higher (SBS) than zirconia and e max group. In a recent study by means of fracture mechanics test, the toughness of zirconia veneer interface with no treatment is significantly higher than that of interfaces subjected to airborne particle abrasion.24
FKG Dentaire SAwww.fkg.ch
iRace sequence,Quick, effective and safe
SafetyMemoDisc
Easy management of number of uses and metal fatigue
Optimal cutting efficiency
No screwing-in effect
Improved resistance to torsion and fatigue
Precision guiding
For most cases, iRace sequence includes 3 instruments for finishes of ISO 30/.04*
For more information or to book your next endo training in FKG Dubaï CenterPlease contact: [email protected]
*for larger preparation sizes and lengths, please visit www.fkg.ch
Prosthetic Dentistry

1mm layer TheraCal LC
Regenerative layer stimulates hydroxyapatite
TheraCal LC® is the FIRST light-curable restorativethat aids in the regenerative process!
� Doesn�t run, stays where it is placed
� Perfect replacement forcalcium hydroxide and RMGI
� Direct/indirect liner
� Easy placement and technique
Infected dentin removed.TheraCal LC is applied to thepreparation. Light cure eachincrement.TheraCal LC is an internal flow-able pulpal protectant materialknown as Resin ModifiedCalcium Silicates (RMCS).
Surrounding enamel is etchedwith Select HV® Etch and applyAll-Bond Universal® and lightcure.
All-Bond Universal single-bottlelight-cured adhesive can be usedfor any dental procedure.
Seated crown using Bisco�seCEMENT®.
eCEMENT is a resin cementationsystem designed to strengthenand simplify the placement oflithium disilicate.
To learn more e-mail [email protected] visit www.bisco.com
TheraCal LC
NEW Products from BISCO
All-Bond Universal eCEMENT
Dental News.qxp 2/18/2015 2:34 PM Page 1

Dental News, Volume XXII, Number I, 2015
Bonding resin cement to zirconia
A major weakness of dental zirconia is its inferior ability to adhere to resin cement. As zirconia has a polycrystalline structure and limited vitreous phase, neither hydrofluoric acid etching nor silanization can achieve durable zirconia-resin bonding.25 To promote micromechanical retention, sandblasting method can be used instead of acid etching, and for chemical bonding, instead of silane coupling agents, adhesive monomer could be applied.26 The surface treatment with primers or resin cement containing phosphate ester monomer such as MDP is recommended to improve the bonding to zirconia.MDP containing resin cement and airborne particle abrasion resulted in the most initial and durable bond strength after water storage and thermocycling.27,28,29 Still, it wasn’t sufficient to use MDP alone without sandblasting when subjected to thermocycling.26 Airborne particle abrasion with 50-110μm alumina particle at 0.25 Mpa is effective in roughening zirconia surface but it can create sharp crack tips and structural defects. Therefore it is recommended to reduce the pressure and use particles up to 50μm. After airborne particle abrasion (with 50 μm Al2O3 ), water storage for 150 days, and thermocycling, (37500 cycles 5˚/55˚) the MDP containing resin cement (Panavia) showed the highest tensile bond strength30 and the highest shear bond strength after sandblasting and thermocycling (10000 times).31
Tribochemical silica coating air abrades the zirconium surface with alumina particles that have been coated with silica embedding the surface with it. This results in preparing the surface for silanization and micromechanical retention, though there can be a loss in bond strength over a long term.27,29 And simple air abrasion can get the same initial bond strength.28,32
A combination between silica coating and primer application increased the bond strength between zirconia and resin cement but it wasn’t sufficient after artificial aging like water storage and thermocycling (12000 cycles 5˚/55˚) even with the MDP containing system.When testing the retentive strength (removal force along the path of insertion) of zirconia crowns cemented over extracted molars after
airborne particle abrasion (with 50 μm Al2O3)33 or
silica coating34 and thermocycling (5000 cycles 5˚/55˚), minor difference was detected between various resin cement self adhesive cement and resin modified glass ionomer cement.In comparison to other resin cements, MDP monomer resulted in the highest (MTBS) values with zirconia and produced higher bond strength than two phosphate monomers (RelyX UniCem, and Multilink) while microshear test failed to detect such difference.35 (MTBS) is recommended to test the adhesive bonding effectiveness and the interfacial material property as its result is comparable to the micro tensile fatigue resistance which is more labor-intensive and time consuming to do.36 The (MTBS) of the MDP containing resin cement is higher than self adhesive or conventional resinous cement, independently of the surface treatment (sandblasting or silica coating).37,38
Rely X unicem had lower bond strength value but like Panavia wasn’t affected by the water aging38 or thermocycling (10000 times)31 and both cement demonstrated satisfactory performance in media with different pH.39
With RelyX Unicem, air abrasion at 0.25Mpa is recommended to contribute to a durable bond yet it can initiate surface defect. The combination of low pressure air abrasion (0.05 Mpa) and MDP containing primer is useful to achieve durable bond after 37500 thermocycling.40 On a shear bond strength test, the better bond were obtained by dual-polymerizing (Panavia, Variolink II) cements than auto polymerizing (Rely X and Multilink) resins. The better bond is associated with sand¬blasting or silica coating and an adhesive containing MDP.41
Some primers mix MDP with another molecule like Monobond plus (phosphate monomer with silane (MPS) 42 or Z-prime plus (organophosphate and carboxylic acid monomers)43 they also showed high bond strength same as the use of a phosphonic acid monomer (6-MHPA).44
Different alternative methods to treat zirconia surfaces have been evaluated to produce reliable long term adhesion. The most innovative was introduced by Aboushelib et al.45,46 and tested to (MTBS). This method was named selective infiltration etching (SIE). They applied a low temperature molting glass on selected zirconia
24
Prosthetic Dentistry

B-75
3-01
-760
0-V0
sirona.com
By choosing an orTHoPHos XG you are investing in a secure future. This is because the units in the orTHoPHos XG family offer you high quality, durability and the best image quality with the lowest dose and a perfect workflow. so it‘s no surprise that more than 100,000 dentists all over the world have decided on an orTHoPHos XG. Enjoy every day. With Sirona.
ORTHOPHOS XG
simPLY rELiaBLE.EVERY DAY.
B-753-01-76-V0_205x275.indd 1 06.08.13 15:06

Dental News, Volume XXII, Number I, 2015
26
surfaces which is submitted to a heat-induced maturation by 2 short thermal cycles 650-750˚C which resulted in stressing the grain boundary region and infiltration of the glass materials. Then the glass is removed by hydrofluoric acid solution, leaving porosities for the resin cement. The (SIE) specimens bounded with Panavia had the highest bond strength (49.8 Mpa) in comparison with airborne particle abrasion that bonded with the same cement (33.4 Mpa) or with Rely X (23.3Mpa). Contrarily to other cement with selective infiltration etching the MDP containing cement conserved their bond strength after one month of water storage. MPS also produced greater bond strength, but the use of silanes with SIE didn’t aid in producing a hydrolytically stable bond.47
A large range of mechanical, chemical or both approaches have tried to modify the zirconia surface and improve resin bonding. Nano structured alumina coating48 consists of precipitating aluminum hydroxide originating from alumina nitride powder with subsequent thermal treatment. It can improve the bond strength compared to air abrasion pretreatment. Another technique is the Chloro silane combined with vapor phase allows pretreatment that deposits a silica like layer used to increase adhesion with traditional silane and bonding technique.49 In addition, Hot etching acidic solution (HCl and FeCl3 (100˚C))also increases the surface roughness, enabling optimal bond to resin cement.50 Likewise the application of a glass-ceramic/glaze containing a major lithium disilicate phase subsequently treated with hydrofluoric acid and silane might also be useful in improving the bond strength of zirconia to resin cements.51 Furthermore, laser application that removes particles through ablation process by micro explosions and vaporization, inducing phase transformation. Yet its durable bond strength is contradictory.52,53,54,55 One more is the treatment of zirconia with plasma, which reduces the contact angle, and increases the surface wettability which may also improve its bond strength.56
Finally, a subject that’s worth studying is the aging of zirconia or low temperature degradation. It consists of a spontaneous slow
transformation from the tetragonal phase to the more stable monoclinic phase in the absence of any mechanical stresses. This phenomenon decreases the physical properties of the material. Moreover, leaving the zirconia framework without ceramic veneering would expose this framework to salivary environment increasing the potential of plaque retention and reducing resistance to low temperature degradation and service life.1
Conclusion According to the reviewed literature it is possible to prevent failure of veneered zirconia ceramics, and to conclude that:
- Smaller finish line can be used with zirconia.
- The framework design should provide a uniform layer thickness of the veneering ceramic.
- It is better to have identical CTE or slightly lower between veneering ceramics and zirconia.
- Veneering ceramics need longer firing time and slower cooling rate.
- Further treatment or sandblasting of the external surface before veneering, doesn’t seem to increase the bond strength, yet it can damage the surface and jeopardize the bond with layering ceramic.
- The liner is beneficial for colored zirconia using the layered technique, but not necessary for the pressed on technique.
- The use of MDP containing resin cement on air-abraded zirconia crown with 50 microns alumina particles at low pressure can be recommended as most retentive luting method. Likewise, the selective infiltration etching (SIE) method with MDP is a reliable and promising method for establishing a strong and durable bond. Many sophisticated techniques are developed to increase this bonding, but simple methods are also applicable like glass-ceramic glaze.
Prosthetic Dentistry

Planmeca Romexis® 4.0.ROne software – all solutionsImaging and CAD/CAM in one system
Planmeca IDS 2015 novelties
The completely redefinedPlanmeca Romexis® 4.0Discover Planmeca Romexis® 4.0 – the brains behind Planmeca’s products. Built around an improved user-friendly interface, the new version of the unequaled all-in-one software combines 2D and 3D imaging with the complete CAD/CAM workflow, while also providing innovative connectivity with Planmeca equipment.
Welcome the new era of digital dentistry!
Find more info and your local dealer www.planmeca.com
Planmeca Oy Asentajankatu 6, 00880 Helsinki, Finland. Tel. +358 20 7795 500, fax +358 20 7795 555, [email protected]

Dental News, Volume XXII, Number I, 2015
28
1. zaronE f, russo s, sorrEntino r. froM porcElain-fusEd-to-MEtal to zir-conia: clinical and ExpEriMEntal considErations. dEnt MatEr. 2011 Jan; 27(1):83-96. 2. vita in-cEraM® yz Working instructions .2011 nov.3. aBoushEliB Mn, dozic a, liEM Jk. influEncE of fraMEWork color and layEr-ing tEchniquE on thE final color of zirconia vEnEErEd rEstorations. quintEssEncE int. 2010 May; 41(5):E84-9.4. koMinE f,struBJ, MatsuMura h. Bonding BEtWEEn layEring MatErials and zirconia fraMEWorks. JapanEsE dEntal sciEncE rEviEW (2012) 48, 153—161.5. akEsson J, sundh a, sJögrEn g.fracturE rEsistancE of all-cEraMic croWns placEd on a prEparation With a slicE-forMEd finishing linE. J oral rEhaBil. 2009 Jul; 36(7):516-23.6. ips E.Max®zircad instructions for usE .ivoclar vivadEnt tEchnical 2010 fEB. 7. zEnostar dEntal rEstorations froM WiEland. thE clEar Monolithic linE in dEntal tEchnology.2013 apr.8. aBoushEliB M. fatiguE and fracturE rEsistancE of zirconia croWns prE-parEd With diffErEnt finish linE dEsigns. J prosthodont. 2012 Jan; 21(1):22-7.9. EspErtisEtM sciEntific facts. zirconia-supportEd cEraMic rEstorations: un-covEring thE MystEriEs. 3M EspE 200910. cad/caM cErcon®. product dEscription and instructions for usE, cEr-con® BasE/cErcon® ht. dEgudEnt 2011 dEc.11. aBoushEliB M, JagEr n, klEvErlaan c, fEilzEr a. MicrotEnsilE Bond strEngth of diffErEnt coMponEnts of corE vEnEErEd all-cEraMic rEstorations. dEnt MatEr. 2005 oct; 21(10):984-91.12. aBoushEliB M, fEilzEr a, JagErn,klEvErlaan c. prEstrEssEs in BilayErEd all-cEraMic rEstorations. J BioMEd MatEr rEs part B: appl BioMatEr 87B: 139–145, 2008.13. saito a, koMinE f, Blatz M, MatsuMura h. a coMparison of Bond strEngth of layErEd vEnEEring porcElains to zirconia and MEtal. J prosthEt dEnt 2010; 104:247-257.14. cErcon cEraM kiss. product dEscription and procEssing Manual for cEr-con cEraM kiss vEnEEring cEraMics. dEgudEnt 2009 nov.15. cErcon cEraM prEss. product dEscription and instructions for cErcon cEraM prEss. prEss-on porcElain- dEgudEnt 2006 sEp.16. aBoushEliB M, klEvErlaan c, fEilzEr a. MicrotEnsilE Bond strEngth of dif-fErEnt coMponEnts of corE vEnEErEd all-cEraMic rEstorations part ii: zirconia vEnEEring cEraMics. dEnt 2006 sEp; 22(9):857-63.17. aBoushEliB Mn, klEvErlaan cJ, fEilzEr aJ. MicrotEnsilE Bond strEngth of diffErEnt coMponEnts of corE vEnEErEd all-cEraMic rEstorations. part 3: douBlE vEnEEr tEchniquE. J prosthodont. 2008 Jan; 17(1):9-13.18. aBoushEliB M, klEvErlaan c, fEilzEr a. EffEct of zirconia typE on its Bond strEngth With diffErEnt vEnEEr cEraMics. J prosthodont. 2008 Jul; 17(5):401-8.19. aBoushEliB Mn, dE klEr M, van dEr zEl JM, fEilzEr aJ. MicrotEnsilE Bond strEngth and iMpact EnErgy of fracturE of cad-vEnEErEd zirconia rEsto-rations. J prosthodont. 2009 apr; 18(3):211-6.20. aBoushEliB Mn, dE klEr M, van dEr zEl JM, fEilzEr aJ. EffEct of vEnEEring MEthod on thE fracturE and Bond strEngth of BilayErEd zirconia rEstorations. int J prosthodont 2008; 21:237-240.21. nakaMura t, WakaBayashi k, zaiMa c, nishida h, kinuta s, yatani h. tEnsilE Bond strEngth BEtWEEn tooth-colorEd porcElain and sandBlastEd zirco-nia fraMEWork. J prosthodont rEs 2009; 53:116-119.22. aBoushEliB M. long tErM fatiguE BEhavior of zirconia BasEd dEntal cE-raMics. MatErials 2010, 3, 2975-2985.23. guEss p, kuli s a, WitkoWski s, WolkEWitz M, zhang y, struB J. shEar Bond strEngths BEtWEEn diffErEnt zirconia corEs and vEnEEring cEraMics and thEir suscEptiBility to thErMocycling. dEnt MatEr. 2008 nov; 24(11):1556-67.24. Wang g, zhang s, Bian c, kong h.EffEct of zirconia surfacE trEat-MEnt on zirconia/vEnEEr intErfacial toughnEss EvaluatEd By fracturE MEchanics MEthod. J dEnt. 2014 Jul; 42(7):808-15.25. lEE t, ahn J, shiM J, han c, kiM s. influEncE of cEMEnt thicknEss on rEsin-zirconia MicrotEnsilE Bond strEngth. J adv prosthodont 2011; 3:119-25.26. yun J, ha s, lEE J, kiM s. EffEct of sandBlasting and various MEtal priMErs on thE shEar Bond strEngth of rEsin cEMEnt to y-tzp cEraMic. dEnt MatEr. 2010 Jul; 26(7):650-8.27. qEBlaWi d, Muñoz c, BrEWEr J, Monaco E. thE EffEct of zirconia surfacE trEatMEnt on flExural strEngth and shEar Bond strEngth to a rEsin cEMEnt. J prosthEt dEnt 2010; 103:210-220).28. MattiEllo r, coElho t, insaurraldE E, coElho a, tErra g, kasuya a,
References
Prosthetic Dentistry
favarão i, gonçalvEs l, and fonsEca r. a rEviEW of surfacE trEatMEnt MEthods to iMprovE thE adhEsivE cEMEntation of zirconia-BasEd cEraMics. isrn BioMatErials, vol. 2013, articlE id 185376, 10 pagEs, 2013.29. thoMpson J, stonEr B, piascik J, sMith r. adhEsion/cEMEntation to zirco-nia and othEr non-silicatE cEraMics: WhErE arE WE noW? dEnt MatEr. 2011 Jan; 27(1):71-82.30. Wolfart M, lEhMann f, Wolfart s, kErn M. duraBility of thE rEsin Bond strEngth to zirconia cEraMic aftEr using diffErEnt surfacE conditioning MEth-ods. dEnt MatEr. 2007 Jan; 23(1):45-50.31. lüthy h, loEffEl o, haMMErlE c. EffEct of thErMocycling on Bond strEngth of luting cEMEnts to zirconia cEraMic. dEnt MatEr. 2006 fEB; 22(2):195-200.32. chEn l and suh B. Bonding of rEsin MatErials to all-cEraMics: a rE-viEW. curr. rEs. dEnt 2012, 3: 7-17.33. palacios r, Johnson g, phillips k, raigrodski. rEtEntion of zirconiuM oxidE cEraMic croWns With thrEE typEs of cEMEnt. J prosthEt dEnt 2006; 96:104-14.34. Ernst cp, cohnEn u, stEndEr E, WillErshausEn B. in vitro rEtEntivE strEngth of zirconiuM oxidE cEraMic croWns using diffErEnt luting agEnts. J prosthEt dEnt. 2005 Jun; 93(6):551-8.35. MirMohaMMadi h, aBoushEliB M, salaMEh z, fEilzEr a, klEvErlaan c. innovations in Bonding to zirconia BasEd cEraMics: part iii. phosphatE MonoMEr rEsin cEMEnts. dEnt MatEr. 2010 aug; 26(8):786-9236. poitEvin a, Munck J, cardoso M, MinE a, pEuMans M, laMBrEchts p, MEErBEEk B. dynaMic vErsus static Bond-strEngth tEsting of adhEsivEintErfacEs.dEnt MatEr. 2010 nov; 26(11):1068-76.37. oyagüE r, MonticElliB f, tolEdano M, osorio E, fErrari M, osorio r. in-fluEncE of surfacE trEatMEnts and rEsin cEMEnt sElEction on Bonding to dEnsEly-sintErEd zirconiuM-oxidE cEraMic. dEnt MatEr. 2009 fEB; 25(2):172-9.38. oyagüE r, MonticElli f, tolEdano M, osorio E, fErrari M, osorio r. EffEct of WatEr aging on MicrotEnsilE Bond strEngth of dual-curEd rEsin cE-MEnts to prE-trEatEd sintErEd zirconiuM-oxidE cEraMics. dEnt MatEr. 2009 Mar; 25(3):392-9.39. gEraMipanah f, MaJidpour M, sadighpour l, fard MJ. EffEct of artificial saliva and ph on shEar Bond
strEngth of rEsin cEMEnts to zirconia-BasEd cEraMic. Eur J prosthodont rEstor dEnt. 2013 Mar; 21(1):5-8.40. yang B, Barloi a, kErn M. influEncE of air-aBrasion on zirconia cEraMic Bonding using an adhEsivE coMpositE rEsin. dEnt MatEr. 2010 Jan; 26(1):44-50.41. roMán-rodríguEz J, fons-font a, aMigó-Borrás v, granEll-ruiz M, BusquEts-Mataix d, panadEro r, solá-ruiz M. Bond strEngth of sElEctEd coMpositE rEsin-cEMEnts to zirconiuM-oxidE cEraMic. MEd oral patol oral cir Bucal. 2013 Jan 1; 18 (1):E115-23.42. oBradovic-dJuricic k, MEdic v, dodic s, gavrilov d, antoniJEvic d, zrilic M. dilEMMas in zirconia Bonding: a rEviEW. srparhcEloklEk. 2013 May-Jun; 141(5-6):395-401.43. MagnE p, paranhos M, BurnEtt Jr. l. nEW zirconia priMEr iMprovEs Bond strEngth of rEsin-BasEd cEMEnts. dEnt MatEr. 2010 apr; 26(4):345-52.44. kitayaMa s, nikaidot, takahashi r, zhu l, ikEda M,foxton r, sadr a, tagaMi J. EffEct of priMEr trEatMEnt on Bonding of rEsin cEMEnts to zirconia cEraMic. dEnt MatEr. 2010 May; 26(5):426-32.45. aBoushEliB M, klEvErlaan c, fEilzEr a. sElEctivE infiltration-Etching tEch-niquE for a strong and duraBlE Bond of rEsin cEMEnts to zirconia-BasEd MatEri-als. J prosthEt dEnt 2007; 98:379-388.46. aBoushEliB M, Matinlinna J, salaMEh z, ounsi h. innovations in Bonding to zirconia-BasEd MatErials: part i. dEnt MatEr. 2008 sEp; 24(9):1268-72. 47. aBoushEliB M, MirMohaMadi h, Matinlinna J, kukk E, ounsi h, salaMEh z. innovations in Bonding to zirconia-BasEd MatErials. part ii: focusing on chEMical intEractions. dEnt MatEr. 2009 aug; 25(8):989-93.48. JEvnikar p, krnEl k, kocJan a, funduk n, kosMačt. thE EffEct of nano-structurEd aluMina coating on rEsin-Bond strEngth to zirconia cEraMics. dEnt MatEr. 2010 Jul; 26(7):688-96.49. piascik Jr ,sWift EJ, thoMpson Jy, grEgo s, stonEr Br .surfacE Modi-fication for EnhancEd silanation of zirconia cEraMics. dEntMatEr.2009 sEp;25(9)1116–1121. 50. casucci a, MazzitElli c, MonticElli f, tolEdano M, osorio r, osorio E, papacchini f, fErrari M. Morphological analysis of thrEE zirconiuM oxidE cEraMics: EffEct of surfacE trEatMEnts. dEnt MatEr. 2010 aug; 26(8):751-60.51. ntala p, chEn x, niggli J, cattEll M. dEvElopMEnt and tEsting of Multi-phasE glazEs for adhEsivE Bonding to zirconia suBstratEs. J dEnt. 2010 oct; 38(10):773-81.52. foxton rM, cavalcanti an, nakaJiMa M, pilEcki p, shErriff M, MElo l, Watson tf. duraBility of rEsin cEMEnt Bond to aluMiniuM oxidE and zirconia cEraMics aftEr air aBrasion and lasEr trEatMEnt. J prosthodont. 2011 fEB; 20(2):84-92.

Maintain your patients’ confidence and satisfaction with their dentures by helping them overcome daily social, emotional and physical challenges.
Help your patients eat, speak and smile with confidence with the Corega® denture care regime.
For full information about the product, please refer to the product pack.For reporting any Adverse Event/Side Effect related to GSK product please contact us on [email protected] of preparation: June 2014, CHSAU/CHPLD/0008/14b
We value your feedbackSaudi Arabia: 8008447012All Gulf and Near East countries: +973 16500404
Arenco Tower, Media City, Dubai, U.A.E.Tel: +971 4 3769555, Fax: +971 3928549 P.O.Box 23816.

Dental News, Volume XXII, Number I, 2015
18
Polyamide Resins in Removable Dentures
30
Prosthetic Dentistry
AbstractThermoplastic resins have been used in dentistry for over 50 years. In the meantime, their use has spread due to their superior characteristics, and the interest in polyamide based materials (nylon) have increased. Their ongoing development has yielded new classes of more and more advanced materials and technologies, which make possible new applications for thermoplastic resins in the future. The dentists have to meet growing demands for prosthetic rehabilitation due to population aging and higher requirements on the quality of life. In this article we will talk about physical, mechanical and thermal properties of polyamide materials, surface roughness, flexibility and absence of monomer in comparison with PPMA, and the various applications of polyamide resins in removable dentures.
IntroductionPolymethylmethacrylate (PMMA) resin has been a commonly used denture base biomaterial since 1937. The properties of favorable working characteristics, ease of manipulation, ability to repair, aesthetic appearance, low cost, acceptability by most of the patients, stability in the oral environment, and accurate fit have contributed to the success of this material.1-4
They are synthetically obtained materials that can be modeled, packed or injected into molds during an initial plastic phase, which solidify through a chemical reaction-polymerisation.5
Its mechanical feature, however, is far from the ideal because it has weak flexural and impact strength and low fatigue resistance. These often lead to denture failure during chewing or when it is dropped.3 Denture fractures is one of the most common clinical problems.6 Other disadvantages of PMMA resin are increased
porosity, high water retention, volume variations and irritating effect of the residual monomer. Researches have attempted to improve the mechanical properties of PMMA denture bases by reinforcement with fiber glass or carbon, (Fig.1,2) and also by chemical modification.7
Development of alternative materials such as thermoplastic resins has also been reported in the literature.2,8
Dr. Danielle El Hakim
Dr. Mireille Rahi,
Dr. Najib Abou Hamra,
Dr. Elias Smaira
Fig 1: Glass fiber reinforcement
Fig 2: Carbon fiber reinforcement
Fig 1
Fig 2

MICRO-MEGA 5-12 rue du Tunnel - 25006 Besançon Cedex - France - www.micro-mega.com®
Your single rotary file for glide path development
Simplicity
Efficiency
Safety
110 WithYouYears

Dental News, Volume XXII, Number I, 2015
32
Thermoplastic resins may be repeatedly softened by heating and hardened by cooling without undergoing a chemical change. They may be considered as being composed of bundles of chainlike molecules (called polymers) of many different lengths and molecular weights. They can be classified as thermoplastic acetal, thermoplastic polycarbonates, thermoplastic acrylic and thermoplastic nylon (polyamides).9
However, the desired denture base material has not been developed yet.3
Thermoplastic polyamide (nylon), synthesized by the condensation reaction between a diamine and a dibasic acid,1,10 was first studied as a denture base biomaterial in the 1950s. The early form of polyamides displayed several problems, such as high water absorption, discoloration tendency, surface roughness, bacterial contamination, and difficulty in polishing.1,11 It was especially used in exceptional cases like repeated denture fracture and for patients with tissue allergies against acrylic denture base or denture fractures.3 In recent years, polyamide has been attracting attention as a denture base biomaterial due to the advantages of: favorable aesthetic outcome, reflect the color of gingival tissue beneath due to highlight transparency, they have high quality esthetic properties; toxicological safety to patients allergic to conventional metals and resin monomers; higher elasticity than conventional heat-polymerizing resins; high physical strength, flexible and strong structure; heat resistance and chemical resistance, low water absorption and solubility, low porosity.1,9,10,12,13,14 The polyamide resins could be injection-molded, the advantages of using this system lay in the fact that the resin is delivered in a cartridge, thus excluding mixture errors with long-term shape stability, reduces contraction, and gives mechanical resistance to aging.14,15
Some disadvantages of polyamide are also described, mainly the lack of chemical bonding between the base and the acrylic teeth, thus the need for mechanical retention (Fig. 3), and the difficulty in repairing and relining the denture.2,10,14,16
Physical, Mechanical and Thermal Properties of Polyamide Resins in Comparison with PPMANylon is a crystalline polymer whereas polymethylmethacrylate is amorphous.1 This results in lack of solubility in solvents, high heat resistance, and high strength coupled with more ductility.9 Polyamide molecules contain hydrogen bonding, which increases the melting point of the polyamide.1 The outstanding features of the nylons are their toughness, low density, abrasion resistance, higher melting point and resistance to chemical attack. The flexibility coupled with its strength, enables it to resist all normal attempts to fracture.9
The main advantage of nylon lies in exceptional mechanical properties of resistance to shock and repeated stressing, it has higher fatigue resistance compared to PMMA. Polyamide denture bases are strong and light. Nylon has higher abrasion resistance, elastic memory, creep resistance and is conductive to cyclic stress.9 The polyamide denture base resins have lower flexural strength at the proportional limit
Fig 3: Mechanical retention between polyamide denture base and acrylic teeth.
Fig 3
Prosthetic Dentistry

DesinfectionTHE POWER
OF EFFICIENCY
CONCEPT PATENTED
Tip oscillationto allow perfect
desinfection.
Here is the absolute desinfection in Endodonties !
OF EFFICIENCYOF EFFICIENCYOF EFFICIENCYOF EFFICIENCYOF EFFICIENCYOF EFFICIENCYIrrigation
YOUR ROOT CANALCLEANING EVEN MORE EFFECTIVE
IRRIGATYS : the new two-in-one handpiece with dual fonctions
A removable tank allows the irrigation of the root canal with Hypochlorite and EDTA. The irrigation line leads the solu-tion through the Irriga-Tip®. These patented technology, developed after 6 years of research, optimize the result of the complex procedure of root canal irrigation.
Class IIa medical device. CE0120. For dental healthcare professional use only. Certifying body SGS United Kingdom
Two-in-one system that can provide the solution and strongly activate the liquid for a perfect cleaning.
IDS 2015
Co
me to our booth
Hall 11.2 , R
58
AnnonceIRRIGATYS_162x227-ALG.indd 1 09/02/2015 17:54

Dental News, Volume XXII, Number I, 2015
34
and low elastic modulus12 along with good fracture resistance.9
Though nylon has superior mechanical properties than any other non-metallic base yet there are some serious limitations such as processing difficulties and dimensional changes. Nylon is hygroscopic; its moisture content varies slowly with the surrounding conditions. On immersion in water the material swells, i.e. there is linear expansion. Processing the denture base materials produced unequal deformation in different dimensions (anterior-posterior and cross-arch). The magnitude of this dimensional change depends on the conditions of molding, shape of the mould, and direction in which it is measured.9
Nylon has low coefficient of linear expansion and galvanic conductance.9 Less sorption and solubility of thermoplastic polyamide nylon resin would extremely decrease porosity of the denture base and thus promote hygiene maintenance.13
Surface Roughness of Polyamide Resins in Comparison with PPMASurface roughness is an important factor, which affects the clinical life of materials and resistance to plaque formation. Surface roughness is related to the abrasion of materials. Rough denture surface makes accumulation of microorganisms easier and a higher level of biofilm formation occurs compared to smooth surfaces. Rough surfaces also affect staining resistance, health of oral tissue, comfort of the patient, aesthetics and retention of the dentures directly or indirectly.14
Polyamide denture base material when polished with conventional laboratory technique became more than 7 times smoother whereas processed PMMA when polished became more than 20 times smoother using the same polishing technique. However the surface roughness of polyamide is well within the accepted norm of 0.2 μm Ra. Polyamide produces a clinically acceptable smoothness after conventional polishing.2
FlexibilityUnilateral or bilateral undercuts are frequently encountered and may complicate successful fabrication of denture prosthesis. Management of these situations conventionally includes
alteration of the denture prosthesis bearing area, adaptation of the denture base, careful planning of the path of insertion and the use of resilient lining material. An alternative denture prosthesis design in which optimal flange height and thickness can be achieved is by using flexible denture basematerial. Polyamide denture base materials are more flexible than the commonly used PMMA.2,13 The flexibility of nylon varies greatly depending on the type of molding powder used, temperature of injection, pressure of injection.9
With thermoplastic materials, the clasps are made of the same material as the denture base (Fig. 4), when using superflexible polyamide, we used ready-made clasps, in the case of using medium-low flexibility polyamide. When manufacturing polyamidic dentures, the support elements blend in with the rest of the denture, as they are made of the same material.17
Fig 4: The clasps are made of the same material as the denture polyamide base.
Fig 4
Prosthetic Dentistry

I AM
demanding
Pantone : 130 CC : 0 M : 30 J : 100 N : 0
SOPRO S.A. • A company of ACTEON Group • ZAC Athélia IV • Avenue des Genévriers13705 LA CIOTAT cedex • FRANCE
Tel + 33 (0) 442 980 101 • Fax + 33 (0) 442 717 690 E-mail: [email protected] • www.acteongroup.com
Dental news ad renewal3.indd 1 06/03/2015 10:09:38

Dental News, Volume XXII, Number I, 2015
36
Material Free of MonomerComplete biocompatibility is a major advantage of polyamide resins, because the material is free of monomer and metal, these being the principle causes of allergic reactions in conventional denture materials.14
Applications of Polyamide Resins in Removable DenturesFlexible denture bases may be indicated in patients requiring replacement of teeth in esthetic zone, patients with restricted mouth opening,13 severe soft and hard tissue undercuts,2,13,14 sensitivity to PMMA monomer or metal,2,13,14,18 bruxism cases, thin mucosa and excessive bone resorption, cases where the patient cannot tolerate the force applied by the denture, very old patients with low motor capacity,14 temporary prosthesis after implants,13,14 precision attachment, combination with metal framework, single cast partial dentures, preformed partial denture clasp, immediate dentures,9 space maintainers,13 occlusal appliances,18 flexible tooth born partial denture framework,9,18 denture bases of RPDs without metal clasps, the flexibility of polyamide allows retentive elements that match the color of the gums or teeth.11,12,18
ConclusionsThermoplastic resins have been used in dentistry for many years. During that time the applications have continued to grow and the interest in these materials by both the profession and the public have increased. The materials have superior properties and characteristics and provide excellent esthetic and biocompatible treatment options.Polyamide denture base materials proved to be a useful alternative to conventional denture base resins in clinical situations, including patients who demonstrate a certain degree of tissue undercuts or repeated fracture of dentures and also persons who have sensitivity or allergy to methyl methacrylate monomer.In spite of the various advantages and indications of thermoplastic polyamide resin, further long-term studies are recommended to assess the overall usefulness of the material.
1. kürkçüočlui, köročlua, özkirsE, özdEMirt. a coMparativE study of polyaMidE and pMMa dEnturE BasE BioMatErials: i. thErMal, ME-chanical, and dynaMic MEchanical propErtiEs. intErnational Journal of polyMEric MatErials 2012; 61: 768-777.2. aBuzar Ma, BEllur s, duong n, kiM BB, lu p, palfrEyMan n, surEndran d, tran vt. Evaluating surfacE roughnEss of a polyaMidE dEnturE BasE MatErial in coMparison With poly (MEthyl MEthacrylatE). Journal of oral sciEncE 2010; 52: 577-581.3. soygun k, Bolayir g, Boztug a. MEchanical and thErMal propEr-tiEs of polyaMidE vErsus rEinforcEd pMMa dEnturE BasE MatErials. Journal of advancEd prosthodontics2013;5:153-160.4. yu sh, lEE y, oh s, cho hW, oda y, BaE JM. rEinforcing Ef-fEcts of diffErEnt fiBErs on dEnturE BasE rEsin BasEd on thE fiBEr typE, concEntration, and coMBination. dEntal MatErials Journal 2012; 31: 1039-1046.5. phoEnix rd, MansuEto Ma, ackErMan na, JonEs rE. Evalua-tion of MEchanical and thErMal propErtiEs of coMMonly usEd dEnturE BasE rEsins.Journal of prosthodontics 2004; 13:17-24.6. yu sh, ahn dh, park Js, chung ys, han is, liM Js, oh s, oda y, BaE JM. coMparison of dEnturE BasE rEsin rEinforcEd With polyaroMatic polyaMidE fiBErs of diffErEnt oriEntations. dEntal MatE-rials Journal 2013; 32: 332-340.7. John J, gangadhar sa, shah i. flExural strEngth of hEat-polyM-ErizEd polyMEthylMEthacrylatE dEnturE rEsin rEinforcEd With glass, araMid, or nylon fiBErs. Journal of prosthEtic dEntistry 2001; 86: 424-427.8. nEgrutiu M, Bratu d, roMinu M. polyMErs usEd in tEchnology of rEMovaBlE dEnturEs.roManian Journal of stoMatology 2001; 4:30-41.9. kohli s, Bhatia s. polyaMidEs in dEntistry. intErnational Journal of sciEntific study 2013; 1: 20-25.10. ucar y, akova t, aysan i. MEchanical propErtiEs of polyaMidE vErsus diffErEnt pMMa dEnturE BasE MatErials. Journal of prosth-odontics 2012; 21: 173-176.11. WiEckiEWicz M, opitz v, richtEr g, BoEning kW. physical prop-ErtiEs of polyaMidE-12 vErsus pMMa dEnturE BasE MatErial. BioMEd rEsEarch intErnational 2014.12. haManaka i, takahashi y, shiMizu h.MEchanical propErtiEs of inJEction-MoldEd thErMoplastic dEnturE BasE rEsins. actaodonto-logicascandinavica 2011; 69: 75-79.13. shah J, BulBulE n, kulkarni s, shah r, kakadE d. coMparativE Evaluation of sorption, soluBility and MicrohardnEss of hEat curE polyMEthylMEthacrylatE dEnturE BasE rEsin & flExiBlE dEnturE BasE rEsin. Journal of clinical and diagnostic rEsEarch 2014; 8: 1-4.14. durkan r, ayaz Ea, Bagis B, gurBuz a, ozturk n, korkMaz fM. coMparativE EffEcts of dEnturE clEansErs on physical propEr-tiEs of polyaMidE and polyMEthylMEthacrylatE BasE polyMErs. dEntal MatErials Journal 2013; 32: 367-375.15. parvizi a, lindquist t, schnEidEr r, WilliaMsond, BoyEr d, daWson dv. coMparison of thE diMEnsional accurancy of inJEction-MoldEd dEnturE BasE MatErials to that of convEntional prEssurE-pack acrylic rEsin.Journal of prosthodontics 2004; 13: 83-89.16. korkMaz fM,BagisB,özcan M, durkan r, turgut s, atEsM.pEEl strEngth of dEnturE linEr to pMMa and polyaMidE: lasEr vEr-sus air aBrasion. Journal of advancEd prosthodontics 2013; 5: 287-295.17. szalina la. tEhnologiaExEcutariiprotEzElortErMoplasticEflExitE.dEntis 2005; 4:36.18. Mustafa MJ, aMir hM. Evaluation of candida alBicans attach-MEnt to flExiBlE dEnturE BasE MatErial (valplast) and hEat curE acrylic rEsin using diffErEnt finishing and polishing tEchniquEs. Journal of-Bagh collEgE dEntistry 2011; 23: 36-41.
References
Prosthetic Dentistry

Twins Digital Auxiliaries Practice Development Education
Self Ligation Aligners Tubes/Bands Archwires Lab Products Dig into the Numbers! ormco.com/insignia
© 2014 Ormco Corporation
* Weber II, Dennis J., Koroluk, Lorne D., Phillips, Ceib, Nguyen, Tung, Proffit, William R., “Clinical Effectiveness and Efficiency of Customized vs. Conventional Preadjusted Bracket Systems”, Journal of Clinical Orthodontics, Volume XLVII, No. 4 (2013): 261-266.
Your All-inclusive Solution with customized brackets, wires and placement trays.
The Proof is in the Numbers
Reduced Treatment Time* Fewer Patient Visits*
For more information please contact:Tarek Haneya – Area Sales [email protected]: + 971 56 1746 575
Or contact your local distributor, list is available at ormcoeurope.com
Optimize your practice with the award-winning Insignia™ Advanced Smile Design™, providing the largest array of customized appliances including brackets, wires and even clear aligners.
• Delivers Precise and Predictable Outcomes
• No Inventory Costs
• Combine with Lythos Digital Impression system for Greater Savings and More Streamlined Workflow
• Grow your Practice with Digital Technology
Insignia-Ad-2014-A4Size.indd 1 3/6/14 12:45 PM

Dental News, Volume XXII, Number I, 2015
18
Coronectomy: A Review
38
Oral Surgery
IntroductionThe problem of inferior alveolar nerve involvement during surgical procedure of the removal of lower third molars is often a source of litigations.1,2,3 At the same time the impact of this on a person’s quality of life should not be overlooked.Coronectomy or partial odontectomy reduces the likelihood of nerve injury by insuring retention of the vital roots when they are close or associated with the inferior alveolar nerve as evaluated by plain radiography or CBCT. 4,5
The method aims to remove only the crown part of an impacted mandibular third molar while leaving the root and pulp undisturbed, thereby avoiding direct or indirect damage to the inferior alveolar nerve. 6,7,8
Literature so far has hailed its merits and many practitioners regularly use the approach of coronectomy in order to minimise Inferior alveolar nerve injuries. This technique got in lime light in last decade although results are encouraging but long term outcome needs to be followed. 9,10
This paper presents a comprehensive review on coronectomies and discusses indications, procedure and its complications. We are encouraged by the initial patients satisfaction and requires further long term assessment.
CoronectomyCoronectomy or partial odontectomy is the elective decoronation of a tooth and removal of tooth structure below the level of crest of the alveolar ridge with the intention of allowing the tissue to heal over the remaining vital roots maintaining their vitality and desirably with formation of bone over the roots. This is performed on lower third molars that have an intimate relationship with the inferior dental nerve (IDN) as an alternative to complete
extraction of the tooth, thus reducing risk to the nerve. Reports of permanent nerve damage as a result of wisdom tooth removal have been reported in 1% to 4% of cases which is quite significant considering lower third molar removal is one of the most commonly performed oral surgery procedures. Review of the literature shows coronectomy procedure is becoming more commonly reported and recent studies show quite favourable outcomes when compared to extraction. Due to increasing amount of favourable evidence it will likely become a more common practice, and therefore it is important that general dental practitioners are familiar with the procedure, as patients may present with post op complications such as infection, dry socket in the short term following coronectomy and re-eruption of the roots which tends to present some time later, and thus clinicians will need to consider this in their differential diagnosis.There are many factors to consider when treatment planning for coronectomy on a third molar tooth. History of the patient’s presenting complaint and a full medical history need to be taken. A patient who is medically compromised is not an ideal candidate for coronectomy due to risk of poor healing. Patients should not be immunocompromised (uncontrolled diabetes, long term steroid therapy, HIV) or due to have radiotherapy to the jaw. 5,11,12,13
Patients are assessed clinically and radiographically. If a plain film x-ray is suggestive of an intimate relationship with the ID nerve then cone beam computerized tomography (CBCT) should be utilised to determine the relationship with the nerve as well as the lingual and buccal plate. If it is found that there is not an intimate relationship then complete removal of the tooth rather than coronectomy is indicated. 14,15,16
Dr. P. Dhanrajani, BDS, MDS, MSc, MSC, FRACDS,
FDSRCS, FFDRCSIOral Surgeon
Dr R. Weld-Moore, BDSDentist, Australia
Sensodyne Repair & ProtectPresenting a new layer of protection
Think beyond pain relief and recommend Sensodyne Repair & Protect
Sensodyne Repair & Protect harnesses advanced NovaMin® technology to help build
a robust hydroxyapatite-like layer over exposed dentine and within dentine tubules.1–5
With Sensodyne Repair & Protect, you can do more than treat the pain of dentine
hypersensitivity – you can repair and protect your patients’ exposed dentine.
For full information about the product, please refer to the product pack.For further information please contact your doctor/healthcare professional.For reporting any Adverse Event/Side Effect related to GSK product please contact us on [email protected] of Preparation: June 2014, CHSAU/CHSENO/0063/14
Arenco Tower, Media City, Dubai, U.A.E.Tel: +971 4 3769555, Fax: +971 3928549 P.O.Box 23816.
We value your feedbackSaudi Arabia: 8008447012All Gulf and Near East countries: +973 16500404
References: 1. Burwell A et al. J Clin Dent 2010; 21(Spec Iss): 66–71. 2. LaTorre G, Greenspan DC. J Clin Dent 2010; 21(3): 72-76. 3. West NX et al. J Clin Dent 2011; 22(Spec Iss): 82-89. 4. Earl J et al. J Clin Dent 2011; 22(Spec Iss): 62-67. 5. Efflandt SE et al. J Mater Sci Mater Med 2002; 26(6): 557-565. Prepared December 2011, Z-11-516.

Sensodyne Repair & ProtectPresenting a new layer of protection
Think beyond pain relief and recommend Sensodyne Repair & Protect
Sensodyne Repair & Protect harnesses advanced NovaMin® technology to help build
a robust hydroxyapatite-like layer over exposed dentine and within dentine tubules.1–5
With Sensodyne Repair & Protect, you can do more than treat the pain of dentine
hypersensitivity – you can repair and protect your patients’ exposed dentine.
For full information about the product, please refer to the product pack.For further information please contact your doctor/healthcare professional.For reporting any Adverse Event/Side Effect related to GSK product please contact us on [email protected] of Preparation: June 2014, CHSAU/CHSENO/0063/14
Arenco Tower, Media City, Dubai, U.A.E.Tel: +971 4 3769555, Fax: +971 3928549 P.O.Box 23816.
We value your feedbackSaudi Arabia: 8008447012All Gulf and Near East countries: +973 16500404
References: 1. Burwell A et al. J Clin Dent 2010; 21(Spec Iss): 66–71. 2. LaTorre G, Greenspan DC. J Clin Dent 2010; 21(3): 72-76. 3. West NX et al. J Clin Dent 2011; 22(Spec Iss): 82-89. 4. Earl J et al. J Clin Dent 2011; 22(Spec Iss): 62-67. 5. Efflandt SE et al. J Mater Sci Mater Med 2002; 26(6): 557-565. Prepared December 2011, Z-11-516.

Dental News, Volume XXII, Number I, 2015
40
Fig 1: Signs of an intimate relationship with the nerve on a plain film x-ray include:- Darkening of the root as the ID canal crosses
- Interruption of the lamina dura of the canal
- Sudden diversion of the course of the canal
- Narrowing of the canal as it passes over the
root
- Narrowing of the third molar roots
The tooth itself ideally should be non carious or
in the very least not have any pulpal involvement
or periapical infection. A non-vital tooth with a
necrotic pulp is a source of infection and this is a
contraindication for coronectomy. While most
clinicians would find the idea of decoronating
a tooth and leaving the pulp tissue in the roots
somewhat counter-instinctive, evidence has
shown that the tooth maintains its vitality.
Histological examination of roots that erupted
into the oral cavity following coronectomy
shows vital pulp tissue in the canal, and also
there are reports of roots being sensitive when
they re-erupt which suggests vitality. In fact a
control study by Sencimen et al 201012 showed
that roots that were endodontically treated
actually had quite a high infection rate resulting in these roots requiring removal whereas in the control group there was no reports of infection. Also coronectomy is contraindicated in a horizontal tooth that is lying directly over the nerve as the process of decoronating the tooth may in fact result in damaging the nerve. Other contraindications include pre–existing tooth mobility, patients due to have orthognathic surgery on the mandible, and cystic tissue that
Fig 1
is unlikely to resolve if left in situ. 8,9,17
Following assessment if it is determined that the third molar is suitable for coronectomy the implications of both procedures need to be explained to the patient and then fully informed consent is obtained for both coronectomy and full removal of the tooth. This is because if the root becomes mobilized during the procedure it will require removal. This is not uncommon and in one study 38% of teeth planned for coronectomy required removal due to mobilisation of the roots.
The most commonly described technique is as followsAdequate local anaesthetic is administered. A triangular full thickness buccal mucoperiosteal flap is raised; a lingual flap is not used. A gutter of bone is made around the buccal aspect of the tooth to expose the cemento-enamel junction (CEJ).A fissure bur is then used to drill into the tooth at the CEJ and at a depth of 2/3 to 3/4 through the crown making sure not to cut completely through to the lingual plate as the lingual plate needs to be preserved and also to avoid any damage to the lingual nerve. A small elevator is used carefully to decoronate the tooth taking as much care as possible to apply as little torque as possible so as not to mobilise the roots. If the roots are mobilised then they will require removal.A bur is then used to remove any pieces of enamel which may be present as enamel is non vascular and will be recognised by the body as
Fig 1: orthopantomogram showing
a: darkening of root as the ID canal crosses
b: interruption of the lamina dura of the canal
c: narrowing of the canal as it passes over the root
d: sudden diversion of the course of the canal.
Oral Surgery

41
Dental News, Volume XXII, Number I, 2015
a foreign body. Also the bur is used to reduce the root to at least 3mm below the level of the buccal and lingual alveolar crest. The socket is then copiously irrigated to remove any debris.The flap is then sutured with resorbable sutures. The aim of suturing is to completely close the surgical site, as the desire is to have healing by primary intention. This may require scoring of the periosteum to advance the flap over the surgical site. 3,5,7,9 The patient is given the necessary post op instructions and is seen for post op review. Any post op complications are treated, as they would if it was an extraction. Patients are then seen for appropriate follow up. Patients have a panoramic X-Ray immediately post op (fig.2). Further radiographs are then taken at the discretion of the clinician (fig 3). Any post-
operative complications are dealt with, as they would be with an extraction: irrigation and alvogyl in the case of dry socket, antibiotics, irrigation with chlorhexidine and drainage in the case of infection. Should infection persist then extraction of the root is indicated.There are variations in technique described in the literature. Pogrel 20076 describes a technique of raising both a buccal and a lingual flap. The intention of the lingual flap is to protect the lingual nerve and the lingual plate. The crown is sectioned completely using a bur at an angle of 45o. The aim is to completely transect the crown so it can be easily removed with a mosquito forceps, so as no to apply any torqueing forces to the roots thus reducing the chance of mobilisation.8,10,13
A less commonly described technique is to use a rose head bur to remove crown tissue.
Fig 2
Fig 3
Fig 2: immediate post op-erative orthopantomogram showing sectioning of crown at cementoenamel junction-above the furcation of roots.
Fig 3: one year postoperative orthopantomogram showing roots covered with bone.
Oral Surgery

Dental News, Volume XXII, Number I, 2015
The disadvantages to this are that it takes longer to perform the procedure and produces more debris, and as such is not commonly used. Some authors advocate prophylactic administration of antibiotics however this does not appear to be universal.
Discussion In recent years there have been a number of studies showing quite favourable outcomes for coronectomy. To date there have been two randomised control trials of coronectomies: Leung 20093 and Renton 2005.9 The Leung et al. 20093 study consisted of a control group of extractions n=178 against a trial group of planned coronectomies n=171. Out of the trial group 16 coronectomies (9.4%) failed due to mobilisation of the roots and had to be extracted. Pain and dry socket were reported to be lower in the coronectomy group and there was no difference in infection rates in either group. 1 coronectomy patient required re-operation due to exposure of the root. In terms of IDN damage out of the extraction group, 9 (5.1%) presented with sensory deficit compared to 1 (0.65%) in the coronectomy group. While this does show quite favourable results the mean follow
up time was quite short being less than 12 months. Renton 20059 published a randomised study consisting of 128 patients being treated for 196 third molars. The coronectomy group n=94 had quite a high failure rate in terms of mobilisation of roots (38%). No sensory deficit was reported in the coronectomy group whereas 19 nerves were damaged after extraction. There was no difference in the incidence of dry socket in either group, 5%. The mean follow up was 25 months. Hatano et al. 200913 published a case control study. 220 wisdom teeth were divided into an extraction control group n=118 and a coronectomy group n=102. The mean follow up was 13 months in the control group and 13.5 months in the coronectomy group. 6 cases of IDN damage were reported in the extraction group compared to 1 in the coronectomy group. 4 of the coronectomy roots had to be subsequently removed due to post-operative infection, and out of these 4 there was no nerve damage. Pogrel et al. 20047 performed 50 coronectomies on 41 patients. A lingual flap was raised for each coronectomy. There were no cases of IDN damage and one case of lingual nerve deficient, which subsequently resolved. 1 patient required removal
42
Oral Surgery

of both roots because of failure to heal and another patient required removal of a root due to migration to the surface. X-rays were taken immediately post op and after 6 months and root migration was evident in 30% of patients.Root migration has been reported in long-term follow up. Leung 20123 reported on a 3 year follow up of their original study. Of the original 108 patients 98 returned for 3 year follow up. Out of the 98 patients there were 135 coronectomies. These were reviewed at 3, 6, 12, 24 and 36 months follow up. Root migration was reported in most cases in the first 12 months and stopped at 24 months. The mean root migration was 2.8 mm at 36 months and root eruption occurred in 4 (3%) of cases. These 4 roots were extracted without any report of IDN damage. Dolanmaz14 in a study of 47 coronectomies reported a mean eruption of 4mm at 24 months. Knutsson16 1989 reported the most migration of up to 7mm after 1 year. It can be argued that with re-eruption patients may require two procedures rather than one, thus questioning the efficacy of coronectomy. Most authors report in cases where roots re-erupt they migrate away from the IDN and therefore a counter argument could be made that taking the nerve into account,
43
Oral Surgery
Dental News, Volume XXII, Number I, 2015
this is safer, the outcome is ultimately the same as a planned extraction and considering the effect that permanent nerve damage could have on a patient’s quality of life then this is a much more favourable outcome. However there has been a case reported of the IDN migrating with the tooth as it re-erupted following coronectomy, but this is quite a rare finding.
ConclusionAs an alternative to extraction of lower third molars with an established high risk to the inferior dental nerve, coronectomy offers a safe alternative. The evidence that is emerging is quite positive and in general shows good outcomes when compared to extraction. As there is less radiation associated with cone beam CT than standard CT it has become more justifiable to assess third molars using this technology. This has allowed more accurate assessment of third molars and therefore it is likely in time coronectomy will become a much more routine procedure. Further research is required as there is little evidence in terms of long-term studies.

Dental News, Volume XXII, Number I, 2015
1. rEnton t. notEs on coronEctoMy. Br dEnt J 2012; 212; 323-3262. patEl v, kWok J, sproat c, Mcgurk M. to rEtriEvE or not to rEtriEvE thE coronEc-toMy root thE clinical dilEMMa. dEntal updatE 2013; 40; 370-3763. lEung yy, chEung lk. coronEctoMy of thE loWEr third Molar is safE Within thE first 3 yEars. Journal of oral and Maxillofacial surgEry 2012; 70; 1515- 15224. McardlE l, Mcdonald f, JonEs J. distal cErvical cariEs in thE MandiBular sEcond Molar: an indication for thE prophylactic rEMoval of third Molar tEEth? updatE. British Journal of oral and Maxillofacial surgEry 2014; 52; 185-1895. glEEson c, patEl v, kWok J, sproat c. coronEctoMy practicE. papEr 1. tEchniquE and trouBlE-shooting British Journal of oral and Maxillofacial surgEry 2012; 50; 739 -7446. pogrEl Ma. partial odontEctoMy. oral and Maxillofacial surgEry clinics of north aMErica 19 2007; 19; 85-917. pogrEl Ma, lEE JJ, Muff df. coronEctoMy: a tEchniquE to protEct thE infErior alvEolar nErvE. Journal of oral and Maxillofacial surgEry 2004 62 (12) 1447-14528. lEung yy, chEung lk. safEty of coronEctoMy vErsus Excision of WisdoM tEEth: a randoMizEd controllEd trial. oral surg oral MEd oral pathol oral radiol Endod 2009; 108; 821-8279. rEnton t, hankins M, sproatE c, Mcgurk M. a randoMisEd controllEd clinical trial to coMparE thE incidEncE of inJury to thE infErior alvEolar nErvE as a rEsult of coronEctoMy and rEMoval of MandiBular third Molars. British Journal of oral and Maxillofacial surgEry 2005; 43; 7-1210. patEl v, sproat c, kWok J, BEnEng k, thavaraJ s, Mcgurk M histological Evalu-ation of MandiBular third Molars rEtriEvEd aftEr coronEctoMy British Journal of oral and Maxillofacial surgEry 2014; 52; (5) 415-41911. cilasun u, yildiriM t, guzEldEMir E, pEktas zo. coronEctoMy in patiEnts With high risk of infErior alvEolar nErvE inJury diagnosEd By coMputErisEd toMography. Journal of oral and Maxillofacial surgEry 2011; 69;(6): 1557-6112. sEnciMEn M, ortakoglu k, ayclin c, aydintug ys, ozyigit a, ozEn t, gunaydin y. is Endodontic trEatMEnt nEcEssary during coronEctoMy procEdurE? Journal of oral and Maxillofacial surgEry 2010; 68;(10) 2385-9013. hatano y, kurita k, kuroiWa y, yuasa h, ariJi E. clinical Evaluations of coro-nEctoMy (intEntional partial odontEctoMy) for MandiBular third Molars using dEntal coMputErisEd toMography: a casE-control study. Journal of oral and Maxillofacial surgEry 2009; 67;(9) 1806-14 14. dolanMaz d, yildiriM g, isik k, kucik k, ozturk a. a prEfEraBlE tEchniquE for pro-tEcting thE infErior alvEolar nErvE: coronEctoMy. Journal of oral and Maxillofacial surgEry 2009; 67;(6): 1234-8 15. o’riordan Bc. coronEctoMy (intEntional partial odontEctoMy of loWEr third Mo-lars). oral surg oral MEd oral pathol oral radiol Endo 2004; 98;(3): 274-8016. knutsson k, lysEll lEif, rohlin M. postopErativE status aftEr partial rEMoval of thE MandiBular third Molar. sWEdish dEntal Journal 1989;13;15-2217. dragE na, rEnton t. infErior alvEolar nErvE inJury rElatEd to MandiBular third Molar surgEry: an unusual casE prEsEntation. oral surg oral MEd oral pathol oral radiol Endo 2002; 93;(3): 358-361
References
© Carestream Health, Inc. 2015.
Visit www.carestreamdental.com/solutionsor call 800.944.6365.
PATIENTS AREN’T
PATIENT SO DO FIXED RESTORATIONS IN ONE APPOINTMENT
WELCOME TO THE NEW REALITY
Visit our Stand at:
THE CAD/CAM & DIGITAL DENTISTRY INTERNATIONAL CONFERENCE, DUBAION 08-09 MAY 2015
Our new digital restoration solution is designed to complement your work, not complicate it—and let you simply work better.
SCAN MILLDESIGN
646-Dental_News.indd 1 2/3/15 10:44 AM

������������������ ���
��������� �����
øe IQƒ£àŸG ƒfÉædG á«æ≤JVOCOº««≤àd kGójóL kÉ«©Lôe kiƒà°ùe äOqóM
AGOC’G á«dÉY âjRƒÑªμdG ´GƒfCG
:(kÉfRh) % 87 á``ÄdÉŸG OGƒŸG áÑ°ùf• AGÎgÓd á≤FÉa áehÉ≤e
•»©«Ñ£dG ø°ù∏d πKɇ …QGôM Oó“
• äGhOC’ÉH ¥É°üàd’G ΩóY ,π«μ°ûàdG ádƒ¡°S) á≤FÉa πeÉ©J ádƒ¡°S
•(π«μ°ûàdG ó©H ΩGƒ≤dG ≈∏Y á¶aÉÙGh
•ójóe ʃd QGô≤à°SG :óeC’G á∏jƒW á«dÉY á«dɪL
káfQÉ≤e %50-%30 `H πbCG »éæJGôdG ÖdÉ≤dG áÑ°ùf:ájó«∏≤àdG äRƒÑªμdG ´GƒfCÉH
•(kɪéM) %1^57 kGóL ¢†Øîæe »Ñq∏°üJ ¢ü∏≤J
• »`dÉY …ƒ``«M π`` qÑ≤J
• Ò°üb ≥«Ñ£J øeõH á«dɪ÷G á«dÉY äɪ«eÎd AÉHô◊G á«°UÉN
:»ŸÉ©dG »`°SÉ«≤dG ºbôdG 87%á``ÄdÉe OGƒ``e
Voco Grandio 205x275mm 19.03.2013 11:49 Uhr Seite 1

Dental News, Volume XXII, Number I, 2015
4618
Direct Replacement of Anterior Tooth with Fiber-Reinforced Composite and Natural Tooth Pontic: A Case Report
46
AbstractThe fiber-reinforced composite (FRC) bridges can be an excellent alternative to conventional prosthetic techniques since it is a conservative, fast and cost effective treatment method.Properties of FRC, such as strength, desirable esthetic characteristics, ease of use, adaptability of various shapes, and potential for direct bonding to tooth structure make it suitable for various applications (Hyeon Kim et al, 2014)The anterior permanent extracted tooth can be directly bonded to the adjacent teeth with the FRC. 8
This non invasive provisional method leads to exact repositioning of the coronal part of the anterior extracted tooth in its original intraoral three-dimensional position. 8
The purpose of this article was to present a clinical case of a single anterior tooth replacement by means of fiber- reinforced composite and natural tooth pontic.
Key WordsCase report, Fiber-reinforced composite, anterior tooth replacement, esthetic, function
IntroductionEvery day, dentists are exposed to various and complex esthetic, functional and restorative challenges.Following traumatic loss of the anterior tooth, it is important that an immediate replacement is provided in order to avoid esthetic, masticatory and phonetic difficulties, and to maintain the edentulous space (Smriti Bhargava et al. 2011)A wide range of treatment options can be proposed as solutions for the replacement of a traumatically missing anterior permanent incisor.Some authors consider that implants are the treatment of choice in this clinical situation, since they enable a more conservative approach.
Of course, they are indicated when general and local conditions are favorable. 9, 11
However, the need for surgical procedures and its high cost may reduce its accessibility for some patients (Hyeon Kim et al. 2014). In addition, we should not ignore the patient anxiety and fear about this surgical process. 9
The missing incisor can be replaced with conventional porcelain-fused-to-metal or all ceramic bridge or even with resin-bonded fixed partial denture (Maryland Bridge). 10, 11
The disadvantages of these treatment options: invasive reduction of healthy tooth structure (conventional bridge), non esthetic aspect of the metal framework, dental reduction (grooves…) and lack of longevity (partial denture) and sometimes compromised esthetics. 10, 11
Over the last few years, the development of an innovative treatment using fiber-reinforced composite (FRC) has been reported to replace a single anterior tooth. It offers the possibility of fabricating resin-bonded, esthetically good and metal-free tooth restorations. 3, 7, 9
In some studies, even the missing posterior teeth can be replaced by means of prefabricated FRC technique. 5 The development of the FRC materials and technologies may also allow alternatives for directly made molar replacements (Sufyan Garoushi et al. 2012).Using the natural tooth as a pontic offers the benefits of being the right size, shape, and color. Moreover, the positive psychological value to the patient in using his or her natural tooth is an added benefit (Smriti Bhargava et al. 2011).The current article describes a clinical case treated with a FRC bridge, which was fabricated using the natural tooth as a pontic for immediate replacement of a central permanent incisor in a teenage patient.
Mayada Jemâa,Assistant Professor
Nouha Mghirbi,Assistant Professor
Hayet Hajjami,Professor
Sonia Zouiten,Professor
Abdellatif Boughzala,Professor
Hospital Farhat Hached, Sousse, Tunisia
Bassem Khattech,Professor
Military Principal Hospital of Instruction, Tunis, Tunisia
Restorative Dentistry

©2014 Hu-Friedy Mfg. Co., LLC. All rights reserved.
IMPLACARE™ II
The solution to gentle implant scaling
NEW!
POINTS OF PERFORMANCE
• Made of PLASTEEL™: A high grade, unfilled resin that causes the least amount of alteration to implant abutment surfaces
• 20% thinner tip design: Allows for improved access to implant abutment surfaces and allows for more effective maintenance and care of implants
• Two NEW universal curette designs: The Barnhart 5/6 and Langer 1/2 join the Columbia 4R/4L, 204S, and H6/H7 to provide a well-rounded set of options so you can select the instrument best suited for each patient’s needs
Columbia 4R/4L
IMPL4R/4L6Implacare II 4R/4L Kit (Handle + 12 Refi ll Pairs)
H6/7
IMPLH6/76Implacare II H6/H7 Kit (Handle & 12 Refi ll Pairs)
204S
IMPL204S6Implacare II 204S Kit (Handle & 12 Refi ll Pairs)
NEW Barnhart 5/6
IMPLBH5/66Implacare II BH5/6 Kit (Handle & 12 Refi ll Pairs)
NEW Langer 1/2
IMPLLG1/26Implacare™ II LG1/2 Kit (Handle & 12 Pairs)
UNIVERSAL CURETTEBlade designed with two cutting edges and a rounded toe that allows for adaptation on all surfaces.
SICKLE SCALERDual cutting blades that come to a point designed for removal of supragingival debris.
Please ask for other additional kits.
Please visit our website www.hu-friedy.euor contact us by e-mail: [email protected]
CHICAGO MILAN ROTTERDAM SHANGHAI TOKYO TUTTLINGEN
Implacare II_EN_A4_Dental Magazine_Ziad.indd 1 28.04.14 12:38

Dental News, Volume XXII, Number I, 2015
48
Clinical significanceThe use of FRC restoration as a novel concept for immediate replacement of missing anterior tooth can provide minimally invasive and esthetically promising clinical result.
Case reportA 13-year-old patient who lost a maxillary cen-tral incisor due to trauma reported to the Dental Department for replacement of the same. On discussion, for this adolescent patient, non-invasive transitory prosthetic solutions are indi-cated. The replacement was performed using FRC Bridge because of its conservative nature, the favorable occlusal conditions, esthetic result, and preserving tooth substance.This treatment is an ideal and esthetic option for patients who need a provisional fixed prosthesis before a definitive treatment is chosen (between a classical prosthetic and the implant one).The treatment was accomplished in a one-visit appointment.
Fig 1
Fig 3
Fig 4
Fig 5
Fig 6
Fig 2
Fig 1: Intra-oral preoperative labial view, showing the miss-ing central maxillary incisor
Fig 3: Decoronation of the tooth, removal of the pulp tissue and the apical end of the root was formed into an ovate pontic design with finishing diamond burs. The pulp space was restored with light cure composite.
Fig 4: Fitting of the crown
Fig 5: Palatal view
Fig 6: Conservative box preparations are prepared (limited to enamel), Dimensions: 1.5 to 2 mm long, 1.5 to 2 mm wide, and 2 mm deep the proximal as-pects of the abutment two teeth
Fig 2: The tooth was immersed in saline solution, and then scaled from the remaining soft tissue
Restorative Dentistry

www.soredex.com
Imaging with easeCRANEX® 3Dx 3-in-1 imaging system with 5 FOVs extends the application areas from 2D pan and ceph imaging to accurate CBCT imaging from a single tooth to the entire cranio-maxillofacial region.
Read more: http://www.soredex.com/en/product/cranex-3dx/
Expanded Expanded vision.Expanded vision.Expanded
CRANEX® 3Dx
New
Meet the SOREDEX Team at AEEDC, Dubai 17 - 19 February 2015, Booth 6D06
CRANEX _3Dx_ad_Dental_News_200x270mm_2014.indd 1 11/10/2014 2:51:21 PM

Dental News, Volume XXII, Number I, 2015
50
Fig 13: The adhesive was polymerized for 20 seconds
Fig 14: A tunnel was prepared across the pontic from one proximal side to another with round burs at the predetermined level
Fig 15: The Box preparations on the two abutment teeth were etched (37% phosphoric acid gel, 30 sec-onds), rinsed and gently air-dried
Fig 12: The pontic was placed into the predetermined position and the fibers were condensed through the resin composite
Fig 7Fig 7: Premeasured FRC mate-rial was cut with the Ribbond cutter
Fig 8
Fig 9
Fig 10
Fig 11
Fig 8 - 9: The adhesive bond-ing agent was applied to all the prepared tooth structure according to the manufactur-er’s guidelines
Fig 11: Premeasured FRC was immersed into the specified bonding agent and flowable composite for 15 minutes. Then, it was passed through the tunnel with clear cotton pliers
Fig 12
Fig 13
Fig 14
Fig 15
Restorative Dentistry

Henry Schein Dental, Dr. Ghassan Nasser Hussein, Sales and Marketing Director (Henry Schein)Middle East and North Africa, Mobile: +971 50 4813292, Tel: +971 6 5252842, Fax: +971 6 5531291E-mail: [email protected]
Ritter Concept GmbH, Germany, Christian FindeisenSales and Key Account Manager , Middle East/ AfricaRitter Concept GmbH, Mobile: +971 56 9578689 E-mail: [email protected]
Rittermade in germany
l Reliable and flexible electronic Ritter Unit / *** Gold Line
l Synchronized patient chair with seamless upholstery
l Very interesting in price and efficiency, can also be fully equipped with multimedia/ monitor & camera
Ritter Autoclave CleanTec BB with LED Display, 18 and 23 liter
Ritter Ultra Performance E
class B
*** Exclusively distributed by Henry Schein Middle East ***
Ritter_AD_205x130_2014.indd 1 24.11.14 10:54
Help your patients love their smile.
The introduction of colored, highly translucent zirconia like Zirlux
FC2 allows laboratories to deliver extremely aesthetic restorations
to their dentists which is ultimately what gives the patient
something to smile about.JONATHAN L. FERENCZ, D.D.S.
Diplomate American Board of Prosthodontics
For a certified Zirlux® Lab near you: 1-866-248-9657 • www.zirlux.com
ZirluxAd_Full_MiddleEast.indd 1 11/20/14 10:41 AM

Dental News, Volume XXII, Number I, 2015
52
Fig 16Fig 16: Measuring of the sur-face of the pontic from one side to another
Fig 17
Fig 18
Fig 19
Fig 17: Immediate final resto-ration
Fig 18: Palatal view of the final restoration. The Occlusion was carefully adjusted, especially the anterior guidance using articu-lating paper
Fig 19: Frontal view
We recommended to the patient to keep a good hygiene and maintain the FRC restoration free from dental plaque. 1
Fig 20: 3 months following up restoration
Fig 20
DiscussionThe replacement of a traumatically missing permanent anterior maxillary tooth can be performed by different treatment options. 6, 11
The missing tooth can be replaced with conventional 3-unit bridge or even with resin- bonded fixed partial denture (Maryland Bridge) or a single implant. 10, 11
A traditional 3-unit bridge (porcelain-fused-to-metal or all ceramic) is a viable solution (Gerard J et al. 2001). However, this treatment leads to excessive reduction of the structure of the abutment two teeth and high risk of pulp exposure. 1, 10, 11
Referring to the study of Garoushi S et al. 2011, the conventional fixed partial denture was not indicated in our clinical case due to the young age of the patient.The resin-bonded fixed partial denture (Maryland Bridge) has some disadvantages as the non-esthetic aspect of the metal framework and the necessity of preparation of the dental grooves. 11
It is also considered that partial removable dentures can be exposed to fracture and can irritate the palatal mucosa when used for a long period. 8
Dental implant can be a suitable solution for the replacement of the missing central maxillary incisor but it is considered as an expensive, invasive treatment and we should not ignore the anxiety and fear of the patient about the surgical procedure. 1, 9, 10, 11 Systemic problems may also contraindicate surgery (H Kermanshah et al. 2010).In our case report and referring to other studies, the young age of the patient was a clear contraindication for an implant therapy. 4
Over the last few years, the development of fiber reinforced composite (FRC) has given the dental profession the possibility of fabricating adhesive, aesthetic, and metal-free dental replacements (Kaur Inderjeet et al. 2011).The FRC prosthesis are considered as an innovative and conservative alternative treatment to conventional fixed bridges or partial dentures and even to implants. 2
Compared to traditional prosthetic options, a fiber-reinforced composite bridge is generally less costly (Amir Chafaie et al. 2004)The thin filaments that are incorporated to a
Restorative Dentistry


Dental News, Volume XXII, Number I, 2015
base resin offer an excellent fracture resistance, fatigue strength, improved flexural and tensile strength. 2
While clinical performance is the final determinant of success, flexure is still the most widely reported mechanical property (H Kermanshah et al. 2010).The FRC restorations can be performed directly or indirectly with an artificial acrylic tooth, a direct build up by composite resin or with the crown of the expulsed tooth. 11
The primary type of failures identified were either bulk fracture at the connector or the pontic area, debonding of the veneering composite or fiber exposure (H Kermanshah et al. 2010).In the literature, some authors do not recommend the use of composite materials for definitive restoration because of the risk of the increased wear, accumulation of dental plaque and unstable esthetic clinical result. 1
In our clinical case, all these risks are diminished since we used the natural crown as a pontic. Thus, we avoided complicated laboratory procedure. 8
In the study of Hyeon Kim et al. 2014, the extracted tooth presented no esthetic problems, but the pontic was build up with composite because of the difference of the shape of the adjacent teeth and presence of malalignement of the anterior teeth.The biggest advantage of using the natural crown of the patient as a pontic for the FRC Bridge is the better patient acceptance and tolerance of the tooth loss. Added to that the better shape, color, size and alignement of this natural pontic. 8
The preparations (grooves) of the two abutment teeth were minimal and confined to enamel, it was a non-invasive approach.2
In this case report, the immediate restoration of the missing central permanent maxillary incisor by means of FRC using the natural tooth as a pontic offered promising esthetic result and psychological acceptance from the patient.The technique is practical, economically feasible, requires limited laboratory support and materials, and can be accomplished in a single appointment (Smriti Bhargava et al. 2011).In the visit of control (three months after restoration), the clinical evaluation showed successful result, no evidence of problems and
the teenage patient maintained a good oral hygiene as it was recommended before. He was satisfied with the final restoration.It should be emphasized that FRC prosthesis cannot be a long-term treatment; it is a provisional treatment before conventional fixed prostheses or implant therapy.Garoushi S et al. in (2011, 2012) showed that there is a lack of long-term clinical research of FRC prostheses. Moreover, those longitudinal studies reported general failure rates between 5% and 16% over periods up to 4-5 years.
ConclusionThe replacement of the missing anterior maxillary incisor is an esthetic and functional challenge. The growing desire of patients for esthetic and metal free restorations led to an innovative, conservative, simple and cost-effective approach using FRC prostheses. The success of this technique depends on different factors such as the use of high quality materials and the correct clinical indication of this technique.
54
1. iMMEdiatE tooth rEplacEMEnt using fiBEr-rEinforcEd coMpositE and natural tooth pontic, h kErManshah, f MotEvassElian; opErativE dEntistry, 2010, 35-2, 238-2452. rEplacing a Missing antErior tooth With fiBEr rEinforcEd coM-positE BridgE - a casE rEport, kaur indErJEEt, shrEsht khandpur, harnEEt kaur, Jida, vol. 5, no. 4, april 20113. fiBEr-rEinforcEd coMpositE for chairsidE rEplacEMEnt of antErior tEEth: a casE rEport, garoushi s, vallittu pk and lassila lvJ, liByan J MEd, aop: 0810014. rEsin-BondEd fiBEr-rEinforcEd coMpositE for dirEct rEplacEMEnt of Missing antErior tEEth: a clinical rEport, sufyan garoushi, lippo lassila, pEkka k. vallittu, intErnational Journal of dEntistry, voluME 20115. chairsidE rEplacEMEnt of postErior tEEth using a prEfaBricatEd fiBEr-rEinforcEd rEsin coMpositE fraMEWork tEchniquE: a casE rE-port, Jonathan c. MEiErs, rEza B. kazEMi, J EsthEt rEstor dEnt 17:335–342, 20056. antErior fiBEr-rEinforcEd coMpositE rEsin BridgE: a casE rEport
aMir chafaiE, richard portiEr, pEdiatric dEntistry – 26:6, 20047. singlE visit rEplacEMEnt of Maxillary caninE using fiBEr-rEin-forcEd coMpositE rEsin, sufyan garoushi, lippo lassila, pEkka k vallittu, thE Journal of contEMporary dEntal practicE, January-fEBruary 2012;13(1):125-1298. iMMEdiatE fixEd tEMporization With a natural tooth croWn pontic folloWing failurE of rEplantation, sMriti Bhargava, ritu naMdEv, saMir dutta, raJkuMar tiWari, contEMporary clinical dEntistry /Jul-sEpt 2011/vol2/issuE39. EsthEtic rEhaBilitation of singlE antErior EdEntulous spacE using fiBEr-rEinforcEd coMpositE, hyEon kiM, Min-Ju song, su-Jung shin, yoon lEE, JEong-Won park, rEstor dEnt Endod 2014;39(3):220-22510. fiBEr- rEinforcEd BridgE rEplacEMEnt for congEnitally Missing lat-Eral incisors, gErard J. lEMongEllo Jr
contEMporary EsthEtics and rEstorativE practicE, fEBruary 200111. antErior fiBEr- rEinforcEd coMpositE rEsin BridgE: a casE rEport anuraag gurtu, chandrWati guha, kanishka dua, Journal of dEn-tal sciEncEs and oral rEhaBilitation, oct-dEc 2010, vol.1 - issuE 1
References
Restorative Dentistry


Dental News, Volume XXII, Number I, 2015
56
More Pictures Available Onwww.facebook.com/dentalnews1
معالي وزير الصحة الدكتور علي العبيدي راعي المؤتمر،البروفسور ايلي المعلوف أمين عام اتحاد أطباء األسنان العرب،
السادة الوكالء، السادة النقباء ورؤساء جمعيات طب األسنان،
السادة عمداء كليات طب األسنان،الزمالء والزميالت أطباء األسنان األعزاء،
حضورنا الكريم.
أبدأ كلمتي بتوجيه التحية لصاحب السمو أمير البالد الشيخ صباح االحمد الصباح باختيار سموه من قبل األمم المتحدة
قائدا للعمل اإلنساني، ولذلك فإن دولة الكويت وبقيادة صاحب السمو أمير البالد ملتزمة بالتطوير المستمر لمنظومة الصحة في
الكويت وعلى رأسها صحة الفم واألسنان.
ومن هذا المنطلق، كانت دعوتنا لعقد هذا المؤتمر الذي يعد المؤتمر األضخم في الكويت في هذا المجال، حيث يجمع بين مؤتمرين دولي و عربي في الوقت نفسه، والذي يضم نخبة من
كبار األطباء والمتخصصين على مستوى العالم، ووضعنا على رأس أهدافنا إثراء مجال طب األسنان بكل ما هو جديد من
أبحاث علمية وطرق عالجية وتقنيات حديثة مما يساهم في مواكبة وإطالع جميع العاملين في مجال طب األسنان على آخر
المستجدات العلمية.
والجدير بالذكر بأن مؤتمرنا سوف يوفر أكثر من ٣٠ محاضرة علمية وما يقارب العشرون ورشة عمل، تعمل على تطوير
November 19 - 22, 2014Jumeirah Messilah Beach, KUWAIT
Photo from the oPening Ceremony
The 18th Kuwait Dental Association International Scientific Conference
Left to right: Dr Sami aL manih, Dr. youSSef aL Douery,Dr. abDuLwahab aLawaDhi
قدراتهم عبر اإلطالع على التقنيات الحديثة واستخدامها عن طريق نخبة من الخبراء والمتخصصون، وكما يضم المؤتمر معرض به نخبة من المؤسسات والهيئات و شركات القطاع الخاص المتخصصة في
مجال طب األسنان والتي سوف تعرض آخر ما توصل اليه طب األسنان من أجهزة حديثة و تقنيات جديدة.
الدكتور عبد الوهاب العوضي،رئيس جمعية أطباء األسنان الكويتيين

The 18th Kuwait Dental Association International Scientific Conference
Combine the A-dec 200 with our A-dec 300 delivery system today and get more control over the way you work.
Plus, you also have the option to upgrade to our multi- award winning LED dental light.
To learn more visit a-dec.com or contact your local dealer.
The Power of 2.

Dental News, Volume XXII, Number I, 2015
Dr. abDuLwahab aLawaDhi greetingDr. mohameD aLobeiDa from the KSa
Photo of the memberS of the organizing CommitteearounD Dr. abDuLwahab the PreSiDent of the Kuwait DentaL aSSoCiation

Assistina 3x3:Clean inside, clean outside
The new Assistina 3x3 cleans and maintains up to three instruments automatically.Automatic internal and external cleaning, short cycle time,
easy to use: perfect preparation of straight and contra-angle
handpieces and turbines for sterilization.
Bring me to life!Download the »W&H AR« App free of charge from Google Play (for Android) or the Apple App Store. Open the App and hold your device 50 cm from the ad.
20130917_AD_Assistina3x3_205x275 mm_mit AR.indd 1 17.09.2013 09:06:23

Dental News, Volume XXII, Number I, 2015
December 2 - 4, 2014Khortoum, SUDAN
60
More Pictures Available Onwww.facebook.com/dentalnews1
SDA2014
األخوة / أطباء األسنان الكرام،
إن ما شهده السودان من تطور في طب األسنان كما وكيفا في السنوات السابقة يجعل التحديات امامنا كبيرة والتخطيط السليم واجب ال بد منه. إن أعداد أطباء األسنان في السودان قد قاربت الستة الف طبيب وأن كليات األسنان عشر كليات
وإن أعداد الخريجين سنويا يفوق الخمسمائة طبيب. وقد زادت مراكز وعيادات األسنان بصورة بلغت الستت تستدعي اإلهتمام
بالجودة وتكاتف كل األصعدة لتحقيق ذلك، ومحاولة اإلرتقاء بالتدريب والتعليم المستمر كبيرة.
في رحاب هذا المؤتمر الثامن، ظهر جليا قدرة اإلتحاد في تنظيم المؤتمرات الدولية التي تعكس تطور وقدرة وتكاتف الجميع إلبراز الصورة المشرفة لطب األسنان في السودان خاصة وإننا
من أوائل الدول التي قامت بها كليات لطب األسنان في المنطقة العربية واالفريقية.
نشكر كل أطباء األسنان في مختلف بقاع السودان على مشاركتهم ودعمهم الكبير لنشاطات اإلتحاد، ونرجو ان يكون
هذا المؤتمر بداية موفقة لهذه الدورة الجديدة، سائلين الله ان يمهد لنا الطريق لتحقيق كل األهداف المرسومة لإلرتقاء بمهنة
طب األسنان في السودان، إنه سميع مجيب.
الدكتور أحمد عثمان حسن رزقرئيس إتحاد أطباء األسنان السودانيين
The 8th Sudanese Dental Association Conference
Dr. ahmaD othman rizK,PreSiDent of the SuDaneSe DentaL aSSoCiation
ribbon Cutting by the miniSter of heaLth


Dental News, Volume XXII, Number I, 2015
PiCtureS from the exhibition fLoor
Pr. ibrahim ghanDour between gueStS from arounD the worLD

OptiBond™ XTR Unmatched power for all your direct and indirect restorations.
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
• Outstanding bond strengths to dentin and enamel. Extraordinary performance for long-lasting restorations.
• Self-etch. Minimizes post-operative sensitivity, maximizes patient comfort.
• For direct and indirect restorations. A true universal adhesive.
• Universal compatibility. Enables use with all cements, core build-up materials and substrates.
For more information visit: www.kerrdental.eu/optibondxtr
Your practice is our inspiration.™ KerrHawe SA P.O. Box 268 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu
OptiBond XTR well-defined hybrid layer.
Clear, long resin tags with penetration intolateral dentin tubule branches (2,000x).
AD_OptiBond_XTR_bullet 12.11.2010 10:46 Pagina 1
OptiBond™ XTR Unmatched power for all your direct and indirect restorations.
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
• Outstanding bond strengths to dentin and enamel. Extraordinary performance for long-lasting restorations.
• Self-etch. Minimizes post-operative sensitivity, maximizes patient comfort.
• For direct and indirect restorations. A true universal adhesive.
• Universal compatibility. Enables use with all cements, core build-up materials and substrates.
For more information visit: www.kerrdental.eu/optibondxtr
Your practice is our inspiration.™ KerrHawe SA P.O. Box 268 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu
OptiBond XTR well-defined hybrid layer.
Clear, long resin tags with penetration intolateral dentin tubule branches (2,000x).
AD_OptiBond_XTR_bullet 12.11.2010 10:46 Pagina 1
OptiBond™ XTR Unmatched power for all your direct and indirect restorations.
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
• Outstanding bond strengths to dentin and enamel. Extraordinary performance for long-lasting restorations.
• Self-etch. Minimizes post-operative sensitivity, maximizes patient comfort.
• For direct and indirect restorations. A true universal adhesive.
• Universal compatibility. Enables use with all cements, core build-up materials and substrates.
For more information visit: www.kerrdental.eu/optibondxtr
Your practice is our inspiration.™ KerrHawe SA P.O. Box 268 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu
OptiBond XTR well-defined hybrid layer.
Clear, long resin tags with penetration intolateral dentin tubule branches (2,000x).
AD_OptiBond_XTR_bullet 12.11.2010 10:46 Pagina 1OptiBond™ XTR Unmatched power for all your direct and indirect restorations.
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
• Outstanding bond strengths to dentin and enamel. Extraordinary performance for long-lasting restorations.
• Self-etch. Minimizes post-operative sensitivity, maximizes patient comfort.
• For direct and indirect restorations. A true universal adhesive.
• Universal compatibility. Enables use with all cements, core build-up materials and substrates.
For more information visit: www.kerrdental.eu/optibondxtr
Your practice is our inspiration.™ KerrHawe SA P.O. Box 268 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu
OptiBond XTR well-defined hybrid layer.
Clear, long resin tags with penetration intolateral dentin tubule branches (2,000x).
AD_OptiBond_XTR_bullet 12.11.2010 10:46 Pagina 1
OptiBond™ XTR Unmatched power for all your direct and indirect restorations.
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
• Outstanding bond strengths to dentin and enamel. Extraordinary performance for long-lasting restorations.
• Self-etch. Minimizes post-operative sensitivity, maximizes patient comfort.
• For direct and indirect restorations. A true universal adhesive.
• Universal compatibility. Enables use with all cements, core build-up materials and substrates.
For more information visit: www.kerrdental.eu/optibondxtr
Your practice is our inspiration.™ KerrHawe SA P.O. Box 268 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu
OptiBond XTR well-defined hybrid layer.
Clear, long resin tags with penetration intolateral dentin tubule branches (2,000x).
AD_OptiBond_XTR_bullet 12.11.2010 10:46 Pagina 1
OptiBond™ XTR Unmatched power for all your direct and indirect restorations.
OptiBond XTR Self-Etch, Light-Cure Univesal Adhesive.
• Outstanding bond strengths to dentin and enamel. Extraordinary performance for long-lasting restorations.
• Self-etch. Minimizes post-operative sensitivity, maximizes patient comfort.
• For direct and indirect restorations. A true universal adhesive.
• Universal compatibility. Enables use with all cements, core build-up materials and substrates.
For more information visit: www.kerrdental.eu/optibondxtr
Your practice is our inspiration.™ KerrHawe SA P.O. Box 268 6934 Bioggio Switzerland Freephone: 00800 41 05 05 05 Fax: ++41 91 610 05 14 www.kerrdental.eu
OptiBond XTR well-defined hybrid layer.
Clear, long resin tags with penetration intolateral dentin tubule branches (2,000x).
AD_OptiBond_XTR_bullet 12.11.2010 10:46 Pagina 1
OptiBond XTR Self-Etch, Light-Cure Universal Adhesive.

Dental News, Volume XXII, Number I, 2015
64
More Pictures Available Onwww.facebook.com/dentalnews1
On behalf of the Organizing Committee, it is a pleasure for me to welcome you to the 26th Saudi Dental Society International Dental Conference held at Riyadh Interna-tional Convention and Exhibition Center from 13-15 Janu-ary 2015.So far this Conference is Riyadh’s largest annual event de-voted to the dental care in Saudi Arabia, and it will give participants a platform to exchange ideas, discover new trends in dentistry, reacquaint with colleagues, meet new friends, and broaden their knowledge.The Ministry of Health gives its utmost priority to provide the best health care services throughout the Kingdom making use of the latest technology in the sector. The health care policy of the Kingdom has been designed according to the vision of Custodian of the Two Holy Mosques, who once said: “Nothing is more important than the health of the people”.
Aside from the scientific sessions during the Conference, there will be hands-on teaching workshops and of course our popular poster sessions to give the presenter as much exposure as possible to their peers, and research awards for the Graduates, Young Dentists and Dental Interns.We are thankful to the many international speakers who will shed light on the research and clinical issues that shape our field today. We hope that presentations from many different speakers from other countries shared during this Conference will en-rich knowledge to the dental professions in Saudi Arabia and help provide even better treatment, and dental care to the community they served.Your participation will make this conference wonderful, fruitful and successful. DR. MOHAMMAD I. AL-OBAIDAPresident The Saudi Dental Society
January 13 - 15Riyadh, KSA
SDS 2015
Dr. mohammaD aL-obaiDa
PrinCe turKi bin abDaLLah oPenSthe SauDi internationaL ConferenCe
reCognition to Dr hoDa abDuLLatiffrom PrinCeSS noura unverSity
Transforms your existing unit by seamlessly adding the latest technology
iOptima – I am the one and only
uniqueelectric solution
www.bienair-ioptima.comBien-Air Dental SA länggasse 60 case postale cH-2500 Bienne 6, switzerland tel. +41 (0)32 344 64 64 Fax +41 (0)32 344 64 91 [email protected] www.bienair.com

Transforms your existing unit by seamlessly adding the latest technology
iOptima – I am the one and only
uniqueelectric solution
www.bienair-ioptima.comBien-Air Dental SA länggasse 60 case postale cH-2500 Bienne 6, switzerland tel. +41 (0)32 344 64 64 Fax +41 (0)32 344 64 91 [email protected] www.bienair.com

Dental News, Volume XXII, Number I, 2015
PiCtureS from the exhibition fLoor


Dental News, Volume XXII, Number I, 2015
68
His Highness Sheikh Hamdan Bin Rashid Al Maktoum, Deputy Ruler of Dubai, Minister of Finance and President of the Dubai Health Authority inaugurated the 19th edition of the UAE International Dental Conference and Arab Dental Exhibition (AEEDC Dubai) held at the Dubai International Convention and Exhi-bition Center with the participation of a large number of regional and international officials, heads of delegation, representatives from 130 countries, and more than 1400 company
February 17 - 19, 2015Dubai, UAE
More Pictures Available Onwww.facebook.com/dentalnews1
PiCtureS from the exhibition fLoor

PiCtureS from the exhibition fLoor

Dental News, Volume XXII, Number I, 2015
More than1400 company
Representatives from130 countries
PiCtureS from the exhibition fLoor

www.ca-clear-aligner.com
biocompatible material
clinically proven 3-splint-system for effective treatment
individual fabrication solutions in cooperation with CA LAB or CA DIGITAL
treatment corrections are possible at any time
intelligent software CA® SMART, digital measurement technique for set-up, visual data transfer in real time by webcam
The invisible way of teeth correction.
SCHEU-DENTAL GmbHDubai Office www.scheu-dental.comphone +971 50 6255046 [email protected]
For more information please see:
IDS 2015 in CologneHall 10.1Stand: C040 D049

Dental News, Volume XXII, Number I, 2015
troPhy DiStribution to
THE 12th GLOBAL SCIENTIFICDENTAL ALLIANCE
The Global Scientific Dental Alliance GSDA meetingwas held with participation from 40 countries
the oman DentaL SoCiety
the ameriCan DentaL aSSoCiation
the frenCh DentaL aSSoCiation DentaL newS
the turKiSh DentaL aSSoCiation
the umm aL Qura univerSity

DentaL newS
the turKiSh DentaL aSSoCiation
the umm aL Qura univerSity
the LebaneSe DentaL aSSoCiation
the greater new yorK DentaL meeting the emirateS DentaL aSSoCiation
the itaLian DentaL aSSoCiation
the SauDi DentaL SoCietythe bahrain miniStry of heaLth
Dr. hany ounSi the egyPtian DentaL aSSoCiation
the SauDi miniStry of heaLththe Kuwait miniStry of heaLth

Dental News, Volume XXII, Number I, 2015
Visitors of the DENTAL NEWS Booth From Around the Globe

Around the Globe

Dental News, Volume XXII, Number I, 2015
76
The number of dentists and specialists considering a more conservative and biological approach for Endo treatment has grown dramatically these last years. FKG Dentaire, pioneer in this approach has developed the largest range of NiTi files in the world with over 120 different sizes to fit all kinds of canals anatomy and avoiding the use too stiff files that may change the roots anatomy, which could create dangerous micro cracks or weaken the tooth by over treating the case.Here the concept is to give the dentists the best endo tool box with high quality and efficient Swiss endo files so dentists can adapt their sequence to the best treatment inaccordance with the patients root canals and reach higher success rate. FKG has in its range the renown user friendly sequences iRace, BioRace (non-sterile or sterile) and BT-Race (sterile and single-use).In 2014 we have launched Rooter, a new generation of endo wireless motor with LED light and TotalFill, one of the latest development in Bioceramic Sealer and root repair materials.These new products, this trend for a more conservative approach and following a high demand for continuous education has led FKG Dentaire to open microscopes equipped training centers around the globe (Switzerland, United Arab Emirates). Any dentists willing to get trained on FKG Products locally or in our Training Centers can get in touch with their local FKG distributors.
Website: www.fkg.ch/dealer
FKG Dentaire: 2014 has seen great developments in Endo. In 2015 FKG Dentaire propels Endo in the future...
• G-aenial Anterior & PosteriorG-ænial is one of the rare composite materials that can be really qualified as being user-friendly, not only because of the shade concept, but because it is a unique composition that offers effortless manipulation. Consistency and working times are accommodated to all restorative classes.• G-aenial Universal Flo an innovative concept in composite restorative New concept, new composition: the art of injectable compositeG-ænial Universal Flo benefits from a composition that features a unique filler technology. It has a higher filler load and a homogeneous dispersion of fillers. The resulting improved strength and wear resistance are two key features of this product, opening up the potential for a broader use than standard flowables and making it more suitable for class I to V restorations. Essentially, it looks like a flowable but behaves like a restorative. Its indications are for direct restorations, minimum intervention cavities and fissure sealing. • G-aenial BondOne bonding agent, two choicesOffering a selective etching approach, G-ænial bond offers the best of both worlds: the simplicity and reduced post-operative sensitivity of a self-etch adhesive together with the greater bond strength that was traditionally found only with etch & rinse adhesives. It is a reliable bonding that had proven its efficiency and durability via several studies.
GC continuously seeks to offer the most adequate products for your daily use

Under the patronage of the Faculty of dental medicine Saint-Joseph University
Campus of Medical Sciences, Saint Joseph University, Beirut - Lebanon
April 16-18, 2015
In collaboration with:
Faculté demédecine dentaire
INTERNATIONAL CONGRESS OF ORAL IMPLANTOLOGISTS
Lebanon
International Piezosurgery Academy
Jochen Alius (GER)Wael Att (GER)Joseph Choukroun (FRA)Georges Goumenos (GRE) Georges Khoury (FRA)Alvaro Ordonez (USA)Stavros Pelekanos (GRE)
Gerardo Pellegrino (ITA) Pedro Peña (SPA)Alberto Rebaudi (ITA) Marco Ronda (ITA) Gerard Scortecci (FRA)Simone Verardi (ITA)Tomaso Vercellotti (ITA)
Lecturers
Tel. +961-1-421283 www.fmd.usj.edu.lb/icoi
Co-ChairpersonsProf. Nada Naaman Dr. Kenneth Judy
Dr. Christian MakaryScientific chairperson
Dr. Ghassan YaredChairperson organizing [email protected]
Contacts

Dental News, Volume XXII, Number I, 2015
78
• Handle with 4 interchangeable blades, for atraumatic extraction of teeth with minimal damage to the surrounding alveolar bone.• Thanks to the sharp and delicate blades, the marginal gingiva and periodontal ligament can be carefully detached.• Its use is particularly important when considering dental implants.
Upgradings:• Innovative design «DALILA» handle, specially designed to ensure fast cleaning, easier sterilization and a more comfortable and secure grip• New inclined blade allowing full detachment at mesial & distal position. This blade replaces the previous one article 868/3• Improved with a locking air-tight mechanism• A new holding system for the blade ensures maximum stability
website: www.medesy.it
NEW PERIOTOME – 868 Kit
Cavex Bite&White ExSense offers fast and long-lasting relief from sensitive teeth thanks to a revolutionary blend of hydroxyapatite and a ‹hydro-dispersing clay›. The unique properties of the hydro-dispersing clay ensure accelerated dispersion that helps boost the hydroxyapatite penetration. Thanks to the synergetic composition of Cavex Bite&White ExSense, the hydroxyapatite penetrates deep into the tubules and micro-cracks in the enamel. This means that the areas causing sensitivity are sealed off com-pletely, while at the same time, a process of crystallisation helps to restore micro-hardness and accelerates the re-mineralisation process.
Website: www.biteandwhite.com
NEW! Cavex Bite&White ExSense - Tooth Conditioner
10 th
06 - 10 MAY, 2015JUMEIRAH BEACH HOTELDUBAI, UAE
www.cappmea.com/cadcam1014 CME HOURS
CAPP Designates this activity for 14 CE Credits
Centre for Advanced Professional Practices (CAPP) is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not ap-prove or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry.
Supported By:Organized By:06-10 May
2015
MEET THE
TARGET AUDIENCE:These events are designed forDentists, Dental Technicians & Dental Team
SCIENTIFICCONFERENCE
08-09 MAY2015
C
M
Y
CM
MY
CY
CMY
K
dental news a4.pdf 1 3/6/2015 3:48:59 PM

10 th
06 - 10 MAY, 2015JUMEIRAH BEACH HOTELDUBAI, UAE
www.cappmea.com/cadcam1014 CME HOURS
CAPP Designates this activity for 14 CE Credits
Centre for Advanced Professional Practices (CAPP) is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not ap-prove or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry.
Supported By:Organized By:06-10 May
2015
MEET THE
TARGET AUDIENCE:These events are designed forDentists, Dental Technicians & Dental Team
SCIENTIFICCONFERENCE
08-09 MAY2015
C
M
Y
CM
MY
CY
CMY
K
dental news a4.pdf 1 3/6/2015 3:48:59 PM

Dental News, Volume XXII, Number I, 2015www.fdi2015bangkok.orgwww.fdiworldental.org
Annual World Dental Congress22 - 25 September 2015 - Bangkok Thailand
FDI 2015BANGKOK