Embed Size (px)
Citation preview

SYMPOSIUM: ENDOCRINOLOGY
Delayed pubertyGary Butler
Normal UK pubertal milestones
Girls
Age (years) Mean 2nde98th centile range
Breast development
(Tanner stage 2)
11.0 8.2e13.8
Menarche 13.0 11.0e15.0
AbstractThe onset of puberty may be late e in the latter part of the predicted
normal range or truly delayed e beyond this range. This is usually
regarded as 13 years in girls and 14 years in boys. A height plot beyond
the prepuberty phase limit on the UK-WHO 0e18 year charts also defines
delayed puberty. The initial approach requires a detailed history and clin-
ical examination to exclude other medical or psychological problems. The
presence or absence or pubertal signs should be documented. Investiga-
tions should be targeted at ruling out any medical causes and deter-
mining whether the delay is due to central gonadotrophin deficiency or
a gonadal disorder. Physiological or constitutional delay is more common
in boys but is a diagnosis of exclusion. Treatment may be given using low
doses of sex steroids, testosterone or oestradiol initially in a short course
of 3e6 months, but continuing in escalating doses mimicking the normal
course of puberty, watching regularly for the spontaneous resumption of
progress and gonadotrophin secretion. Counselling, reassurance and
support are key elements in the management of adolescents with delayed
puberty.
Keywords breast development; gonadotrophin; growth chart; Kallmann
syndrome; menarche; oestradiol; puberty phase; Tanner stage; testicular
enlargement; testosterone
What constitutes late or delayed puberty?
There is a wide range in the timing, start and subsequent mile-
stones of normal puberty so it is important to appreciate the
considerable variability in healthy adolescents (Table 1). Puberty
starts with breast development in girls around age 11 years and is
associated with rapid growth, so no signs of this happening in
a girl over 13 years warrants further investigation. The lack of the
appearance of breasts and an absent growth spurt is usually
pretty obvious to girls and their families. Primary failure of
menstruation by 15 years needs evaluating, but if the rest of
puberty has been slow then late onset of menstruation is prob-
ably just part of slow normal development.
Boys’ first signs of puberty are much more subtle e just early
testicular enlargemente normally around age 12 years. Very little
else occurs in the early stages and so these early signs are often not
recognized by boys who think nothing is happening to their
pubertal development. The peak of the growth spurt and other
changes such as voice breaking, muscle bulking and facial hair
growth usually do not appear for another 2e3 years. Most worried
boys just have late-normal puberty and clinical examination
Gary Butler MD FRCP FRCPCH is Consultant in Paediatric and Adolescent
Medicine and Endocrinology, at University College Hospital, London
and Great Ormond Street Hospital for Children, London and Honorary
Professor at UCL Institute of Child Health, London, UK. Conflicts of
interest: none.
PAEDIATRICS AND CHILD HEALTH 21:7 306
demonstrating growth of the testes is all that is needed for reas-
surance. No evidence of testis growth or other signs over 14 years
constitutes delayed puberty. A reason should always be found.
A more unusual problem is a normal commencement of
puberty but a subsequent halting with failure to progress or
complete sexual development. This is always worrying and
needs a thorough investigation along a similar thought process to
that which delays the onset. The most common presenting
complaint is secondary amenorrhoea. The details of assessment
are outside the scope of this review.
The new UK-WHO 0e18 year growth charts contain two
puberty zones. The starting zone clearly defines the acceptable
range for the onset of puberty in each sex. Failure to begin with
any sign of development at an age beyond this zone defines
puberty as delayed. The second or finishing zone delineates the
normal age range for the completion of sexual development.
Using a similar approach, the lack of completion of puberty e
menstruation is the defining feature in girls, and failure to
develop breaking of the voice and facial hair in boys are the
obvious signs that puberty has not progressed.
When might delayed puberty be expected?
Longstanding chronic childhood conditions may delay growth
and puberty especially where inflammatory processes are present
and corticosteroids have been used in the treatment regimen.
Despite an obvious cause, pubertal assessment is necessary as
active treatment of the delay in growth and puberty can improve
the growth prognosis, reduce the long-term risk of osteoporosis
and can boost self-esteem, so careful evaluation may be benefi-
cial. Delayed puberty may be due to an unrecognized chronic
condition so the initial approach to investigation always starts
from a general footing.
Monitoring pubertal progress is mandatory in all adolescents
with chronic conditions as failure to progress through puberty
may also be a sign of disease reactivation, poor adherance to
medical treatment or the development of complications of the
condition or its treatment. Common chemotherapy and radio-
therapy regimens used in childhood cancer treatment are
a classic example of this.
Boys
Age (years) Mean 2nde98th centile range
Testicular enlargement
(Tanner stage 2)
12.0 9.8e14.2
Peak of growth spurt 14.0 11.8e16.2
Table 1
� 2011 Elsevier Ltd. All rights reserved.
SYMPOSIUM: ENDOCRINOLOGY
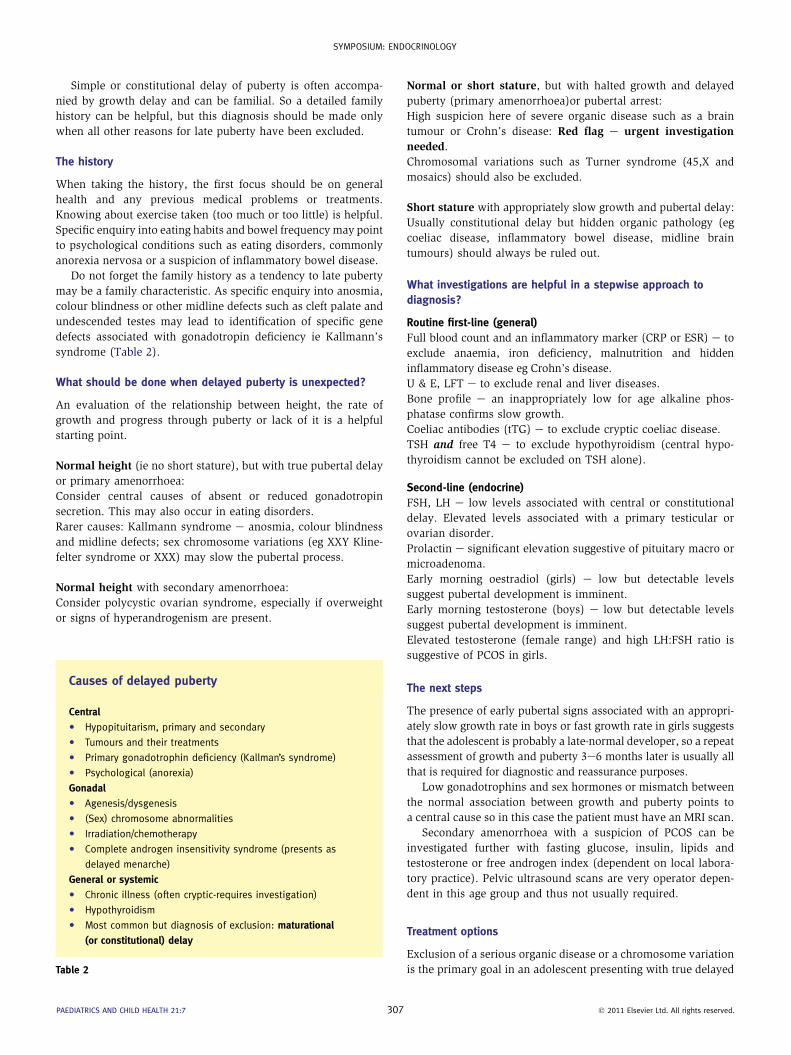
Simple or constitutional delay of puberty is often accompa-
nied by growth delay and can be familial. So a detailed family
history can be helpful, but this diagnosis should be made only
when all other reasons for late puberty have been excluded.
The history
When taking the history, the first focus should be on general
health and any previous medical problems or treatments.
Knowing about exercise taken (too much or too little) is helpful.
Specific enquiry into eating habits and bowel frequency may point
to psychological conditions such as eating disorders, commonly
anorexia nervosa or a suspicion of inflammatory bowel disease.
Do not forget the family history as a tendency to late puberty
may be a family characteristic. As specific enquiry into anosmia,
colour blindness or other midline defects such as cleft palate and
undescended testes may lead to identification of specific gene
defects associated with gonadotropin deficiency ie Kallmann’s
syndrome (Table 2).
What should be done when delayed puberty is unexpected?
An evaluation of the relationship between height, the rate of
growth and progress through puberty or lack of it is a helpful
starting point.
Normal height (ie no short stature), but with true pubertal delay
or primary amenorrhoea:
Consider central causes of absent or reduced gonadotropin
secretion. This may also occur in eating disorders.
Rarer causes: Kallmann syndrome e anosmia, colour blindness
and midline defects; sex chromosome variations (eg XXY Kline-
felter syndrome or XXX) may slow the pubertal process.
Normal height with secondary amenorrhoea:
Consider polycystic ovarian syndrome, especially if overweight
or signs of hyperandrogenism are present.
Causes of delayed puberty
Central
C Hypopituitarism, primary and secondary
C Tumours and their treatments
C Primary gonadotrophin deficiency (Kallman’s syndrome)
C Psychological (anorexia)
GonadalC Agenesis/dysgenesis
C (Sex) chromosome abnormalities
C Irradiation/chemotherapy
C Complete androgen insensitivity syndrome (presents as
delayed menarche)
General or systemic
C Chronic illness (often cryptic-requires investigation)
C Hypothyroidism
C Most common but diagnosis of exclusion: maturational
(or constitutional) delay
Table 2
PAEDIATRICS AND CHILD HEALTH 21:7 307
Normal or short stature, but with halted growth and delayed
puberty (primary amenorrhoea)or pubertal arrest:
High suspicion here of severe organic disease such as a brain
tumour or Crohn’s disease: Red flag e urgent investigation
needed.
Chromosomal variations such as Turner syndrome (45,X and
mosaics) should also be excluded.
Short stature with appropriately slow growth and pubertal delay:
Usually constitutional delay but hidden organic pathology (eg
coeliac disease, inflammatory bowel disease, midline brain
tumours) should always be ruled out.
What investigations are helpful in a stepwise approach to
diagnosis?
Routine first-line (general)
Full blood count and an inflammatory marker (CRP or ESR) e to
exclude anaemia, iron deficiency, malnutrition and hidden
inflammatory disease eg Crohn’s disease.
U & E, LFT e to exclude renal and liver diseases.
Bone profile e an inappropriately low for age alkaline phos-
phatase confirms slow growth.
Coeliac antibodies (tTG) e to exclude cryptic coeliac disease.
TSH and free T4 e to exclude hypothyroidism (central hypo-
thyroidism cannot be excluded on TSH alone).
Second-line (endocrine)
FSH, LH e low levels associated with central or constitutional
delay. Elevated levels associated with a primary testicular or
ovarian disorder.
Prolactin e significant elevation suggestive of pituitary macro or
microadenoma.
Early morning oestradiol (girls) e low but detectable levels
suggest pubertal development is imminent.
Early morning testosterone (boys) e low but detectable levels
suggest pubertal development is imminent.
Elevated testosterone (female range) and high LH:FSH ratio is
suggestive of PCOS in girls.
The next steps
The presence of early pubertal signs associated with an appropri-
ately slow growth rate in boys or fast growth rate in girls suggests
that the adolescent is probably a late-normal developer, so a repeat
assessment of growth and puberty 3e6 months later is usually all
that is required for diagnostic and reassurance purposes.
Low gonadotrophins and sex hormones or mismatch between
the normal association between growth and puberty points to
a central cause so in this case the patient must have an MRI scan.
Secondary amenorrhoea with a suspicion of PCOS can be
investigated further with fasting glucose, insulin, lipids and
testosterone or free androgen index (dependent on local labora-
tory practice). Pelvic ultrasound scans are very operator depen-
dent in this age group and thus not usually required.
Treatment options
Exclusion of a serious organic disease or a chromosome variation
is the primary goal in an adolescent presenting with true delayed
� 2011 Elsevier Ltd. All rights reserved.

Approach to the treatment of prolonged physiologicaldelayed puberty in girls
C Start low-dose ethinyloestradiol as per induction of puberty
C Perform 6 monthly ovarian US to look for follicular activity and
thus evidence of gonadotrophin secretion
C Continuation of treatment is usually only required if there is
a defect in gonadotrophin regulation
Table 4
Approach to the treatment of prolonged physiologicaldelayed puberty in boys
C Continue dosage increments as per induction of puberty
C Use approx 6 monthly dose increases until there is evidence of
testicular growth which represents spontaneous gonadotrophin
secretion
C Total treatment may include several courses of testosterone
C Growth hormone is not necessary unless there is a proven
deficiency
Table 3
SYMPOSIUM: ENDOCRINOLOGY
sexual development. If all is normal, andpuberty is just late, simple
reassurance & support and an understanding of the problem from
patient’s perspective is all that is needed. Delay, especially when
accompanied by short stature can produce anxiety, depression and
low self-esteem, isolation and school refusal. Counselling in life
style skills may be helpful. Repeating the clinical assessment for
progress in puberty may be welcomed for reassurance.
As delayed puberty is almost always an issue for boys due to
the difference in physiological timing of the physical events
between the sexes, a short-term course of low-dose testosterone
treatment for around 3e6 months can boost growth, pubertal
progress and morale. Treatment options include depot testos-
terone esters (Sustanon, Virormone) 50e100 mg given intra-
muscularly on a monthly basis, or oral testosterone undecanoate
capsules (Restandol Testocaps) 40 mg daily. Both are equally
effective. Transdermal testosterone (Testogel, Testim, Tostran) is
under evaluation in this age group but 10e20 mg daily is an
appropriate starting dose.
Testosterone is usually continued until there is clear evidence
of spontaneous puberty (testicular growth). Appropriate active
management of puberty does not adversely affect the long-term
growth prognosis (Table 3). The duration and dosing of therapy
should be monitored by a paediatric endocrinologist however as
overdosage or excessively long courses may reduce the period of
pubertal growth. The best approach requires an active manage-
ment of the growth and lack of secondary sex characteristics
whilst keeping a watchful eye on the resumption of normal
gonadotrophin secretion.
PAEDIATRICS AND CHILD HEALTH 21:7 308
Therapeutic management of physiological delayed puberty is
rarely required in girls, but in such cases very low doses of
ethinyloestradiol starting with 1e2 mg daily are the mainstay of
treatment (Table 4).
Conclusion: cardinal points in the management of delayed
puberty
� Use all previous growth measurements and family information
� Think about the process of puberty as a whole
� Carefully plan your investigations
� Keep an open mind as to causes and consequences of the delay
� Manage the patient as an individual with appropriate
psychological support
� Keep a watchful eye on the resumption of gonadotrophin
secretion from a clinical perspective if using sex hormone
treatment. A
FURTHER READING
Banerjee I, Clayton PE. Puberty. Oxford textbook of medicine. 5th Edn.
OUP, 2010. 13.9.1, 1958e62.
Brook CGD, Clayton PE, Brown RS, eds. Clinical pediatric endocrinology.
Oxford: Blackwell, 2010.
Butler GE. Normal growth and its disorders. Oxford textbook of medicine.
5th Edn. OUP, 2010. 13.9.1, 1948e58.
Butler GE, Kirk JMW. Oxford specialist handbook of paediatric endocri-
nology and diabetes. OUP, 2011.
Kelnar CJH, Butler GE. Endocrine gland disorders and disorders of growth
and development. In: McIntosh N, Helms P, Smyth R, Logan S, eds.
Forfar and Arneil textbook of paediatrics. Elsevier, 2008: 409e512.
� 2011 Elsevier Ltd. All rights reserved.






![Successful Transition from Pediatric to Adult Care in ... · ing, linear growth retardation, and delayed puberty [39]. The etiology of growth failure is multifactorial and includes](https://img.pdfslide.us/doc/110x75/5f14efc67e6c73569018842d/successful-transition-from-pediatric-to-adult-care-in-ing-linear-growth-retardation.jpg)