-
Debbie Hebert, OT Reg. Ont.BSc(OT), MSc (Kin)
[email protected]
-
Participants will:
Appreciate the current understanding of apraxia
Be able to discuss current top-down and bottom-up intervention
approaches to treatment
Apply learned knowledge to a case study
-
1. Incidence, Impact and Definitions
2. Selected Model
3. Assessment
4. Intervention approaches and possible strategies to sensory,
conceptual and production issues
5. Occupation based approaches
6. Case study
-
Incidence: 28 – 57% - left hemisphere damage0 – 34% - right
hemisphere damage
(Donkervoort, Dekker, Van den Ende, Stehmann-Saris, &
Deelman, 2000)
- problem persists in 20% diagnosed (Basso, Capitani, Sala,
Liacona, & Spinnler, 1987)
Impact: ◦ direct impact on functional performance (Foundas, 1995
(eating),
Hanna-Pladdy et al., 2003(toiletting and bathing)
◦ increased caregiver burden (Sundet et al., 1988)
-
“a disorder of skilled movement not caused by weakness,
akinesia, deafferentation, abnormal tone or posture, movement
disorders such as tremors or chorea, intellectual deterioration,
poor comprehension, or uncooperativeness.” (Heilman KM, Rothi LJG.
Clinical neuropsychology. Apraxia. 3rd ed. 1993, p141-163)
-
“A deficit of learned skilled purposive movements that
specifically effects the efficiency and accuracy of the production
of a movement and cannot be accounted for by elemental
sensorimotor, cognitive or attentional deficits.” Rothi &
Heilman, 1997, p 294.
gestures are inaccurate (clumsy) due to abnormal spatial
(posture, orientation of hand to objects and direction of movement)
and/or temporal (timing) aspects of movement. (Smania et al.,
2006)
person knows what to do with the object but cannot call upon the
nervous system to execute the command
seen in conditions of verbal command (pantomime) and/or
imitation and/or object use (Staminova et al., 2012)
-
Has been used to describe impairments in actual tool use (De
Renzi, 1985) oran inability to perform a sequence of acts using
tools and objects to achieve an intended goal (Poeck, 1983; Poeck
& Lehmkuhl, 1980).
Ochipa, Rothi and Heilman (1992) suggest ideational apraxia is a
problem in sequencing movements and conceptual apraxia is based on
errors due to loss of object knowledge.
Typical errors involve sequencing or object use errors
Classically, errors are seen, more in Pantomime and Object Use
(Roy, 2001) but not in imitation
-
Ideational Ideomotor
Tool/Object Related ErrorsInappropriate tool
selectionPerformance of a related but incorrect action to the
target object*Performance of an unrelated action to the target
object*Use of hand to perform action rather than imagining
target tool*
Spatial ErrorsSpatial orientation of hands incorrect to imagined
tool (internal configuration)*Finger arm and hand in inappropriate
position with respect to imagined tool and object (external
configuration)*Movement in the wrong plane +use of wrong muscle
groups (movement)*Body part as tool * +Note: Tools are the
instruments performing the action. Objects are the recipients of
the action.
Sequencing ErrorsPerseveration of part of the series of the
action+*Problems in Terminating movements +Sequence of action out
of order +Blending of two actions +Omission of action part
+Repetitions +substitution of movements unrelated to the movement
+
sequencing of individual movements in an action +
Temporal ErrorsTiming of movement irregular*Occurance or
increase in repetitions required for the action*Unsustained
actionClumsiness
Sequencing of pantomime *
OtherNo response
Perplexity +
OtherPerseveration of sub part of the action+No
responseamorphous movementsgestural or verbal augmentation when
performing the movement
*From Rothi, Raymer, Heilman (1997)+From Roy (1998)Unmarked
Other items From Tate and MacDonald (1995)
-
Liepmann’s Model (1905 -1920)
Roy’s Model (1996), Stamenova, Black and Roy (2013)
Cubelli et al. (2000)
Rothi and Heilman (1997)
Buxbaum and Kalenine Model (2010)
Rouinis and Humphreys (2015)
-
System Purpose of System
Sensory-perceptual system
Conceptual
Production System
Analysis of visual-gestural and auditory-verbal information and
visual-tool
Tool function and action storage
Motor execution and motor control
-
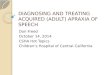
Sensory/Perceptual System
Conceptual System
Production System
Visual/Gestural Information
Auditory/Verbal Information
Visual Tool/Object Information
Knowledge of Action
Knowledge of Tool/Object Function
Image Generation
Response Selection
Working Memory
Response Organization/Control
Delayed Imitation
Concurrent Imitation
Pantomime
Stamenova, V., Black, S. E. and Roy, E. A, An update on the
Conceptual–Production Systems model of apraxia: Evidence from
stroke. Brain and Cognition 80 (2012) 53–63.
-
Pattern Gesture - Tool System ProblemRecognition
P+ / DI- / CI- – Sensory Perceptual Problem
P- / DI+ / CI+ – Conceptual System (Ideational)
P- / DI+ / CI+ + Production System (e.g. Response Selection)
P+ /DI- / CI+ + Production System (working memory)
P- / DI- / CI+ + Production System (preserved analysis)
P+ / DI- / CI- + Production System (Response Organization and
Control)
P- / DI- / CI- + Production System Impairment (Ideomotor)
P- / DI- / CI- – All System Impairment
-
Testing complicated by lack of agreed upon terminology (Tate and
MacDonald, 1995)
Comparability of research tests of apraxia questionable (Butler,
2002)
No Gold Standard
Clinically non-directive
-
Observational
Screening - Identification of the problem and it’s severity
Assessment Batteries - identify the place where the praxis
process breaks down
-
A-One - Arnadottir (1990)
AMPS – Fisher (1990)
Experimental Rating scales: The ADL observations - Van Heugten
et al. (1999, 2000)
-
Comprehensive TULIAItems◦Imitation – non-symbolic◦Imitation –
intransitive◦Imitation – transitive◦Pantomime –
non-symbolic◦Pantomime – intransitive◦Pantomime – transitive
48 items-6 point error based scoring method (0–5)
Also TULIA (AST) 12 item version (Vanbenlingen et al.,
2011)Maximum score =12 with cut off
-
Aphasia Screen, Visual Screen, Perceptual Test Traditional
Apraxia Tests (Transitive
Representational and Non Representational Gestures) Error
scoring is desirable.
Tool and Action Identification Tests Card Sequencing Multiple
Objects Tests Mechanical Problem Solving (new learning)
(See Florida Assessment Battery (Rothi et al. 1997); Florida
Apraxia Battery–Extended and Revised Sydney (FABERS), (Power et al.
2010) and Component Model Assessments )
-
http://www.google.ca/url?sa=i&rct=j&q=&esrc=s&source=images&cd=&cad=rja&uact=8&ved=0ahUKEwjO_-CltbTSAhUJzoMKHYQ7A2kQjRwIBw&url=http://tiny-kylo-ren.tumblr.com/post/148254659481/so-you-want-to-sew-a-button&psig=AFQjCNGv7BNHhdi6J0KOBD2JUuFZKo_O7g&ust=1488427132316634http://www.google.ca/url?sa=i&rct=j&q=&esrc=s&source=images&cd=&cad=rja&uact=8&ved=0ahUKEwjO_-CltbTSAhUJzoMKHYQ7A2kQjRwIBw&url=http://tiny-kylo-ren.tumblr.com/post/148254659481/so-you-want-to-sew-a-button&psig=AFQjCNGv7BNHhdi6J0KOBD2JUuFZKo_O7g&ust=1488427132316634
-
Current Context:
decreased time for intervention and length of stay
lack of research based on models of praxis assessment time
minimal high complexity and variability in presentation of
apraxia and co-morbidities – few people fall into experimental
population eg. Aphasia and apraxia are often co-morbid (Kobayashi
& Ugawa, 2013)
natural environments best for praxis intervention – not often
the setting for clients
-
Limited RCTs
West et al. (2009) Cochrane systematic review found 3 trials and
concluded not enough evidence to support of refute
effectiveness.
Lindsten-McQueen et al. (2014) ◦ Systematic review using FAME
approach (Murphy et al, 2009)
◦ examined 8 studies (4 RCTs) and found Level A, B effectiveness
for Errorless Learning (Goldenberg & Hagmann, 1998) Gesture
Training (Smania et al., 2000, 2006) and Strategy Training (van
Heugten, 1998,2000; Donkervoort et al. 2001, Guesgens et al. 2006,
2007)
-
Apraxic clients have an impaired ability to learn & retain
information (Heilman et al, 1975 (rotary pursuit); Kimura, 1977
(manual sequence box); Poole,1991 (tying shoes)
Learning is specific to targeted interventions and
generalization must be taught? (For exception see Smania et
al.,2000, Geusgens et al. 2007)
Interventions may not improve apraxia dramatically but may
improve occupational performance.
-
Sensory-Perceptual Interventions1. Maximizing sensory reception
(Mary Warren, 1990)
Vision: Use of proper corrective lenses Good lighting Good
contrast between objects and background Allow ample time to study
environmental cues Improve scanning accuracy and speed Augment
features of items important for movement by
using color or arrows Decrease environmental complexity
(decrease patterns on
items and numbers of items) Remove unnecessary items for
task.
-
Audition
Use hearing aids
Ensure reception of command by asking for repetition of
commands
Allow ample processing time
Simplify statements – less information
Decrease steps
-
Tactile:
Ensure ample processing time for exploration of items
Augment sensory awareness through texture
Re-educate re important features of objects
Kinesthetic: Assist client to move slowly enough to ensure
appreciation of movement
-
Assumption: Apraxia key problem is inadequate sensory
integration or an inabiltiy to select the most important sensory
information – could be addressed through sensory input or
enhancement (Ayres, 1985; Croce, 1993; Goodgold-Edwards &
Cermak, 1990)
Sensory Stimulation (Butler, 1997, 2001)
-
Sensory Stimulation (Butler, 1997, 2001)
e.g. 2001 Case Study Male with Ideomotor and Ideational
Apraxia
◦ sensory stim. Protocol + 20 mins Verbal and Visual Mediation
of motor activities (touching targets, imitation, bilateral
imitation, verbalizing hand position) which continued from
baseline
◦ Outcomes – Improvements on motor tests, tests of ideational
apraxia and imitating gestures and less inconsistency of
movements.
-
Which works best as a request for movement?
visual object, visual picture, visual sequence of pictures,
concurrent model imitation, delayed model imitation, tactile object
presentation, combination tactile/visual object presentation,
kinesthetic imitation.
Utilize the strongest method or modality when requesting
movement and correcting movement during a task
When re-teaching a gesture (as in learning gestures for
communication) – use multiple cues and fade out stronger cues first
(Maher et al.,1991; Code and Gaunt, 1986)
Cuing may assist client to remember conceptual representations
that are inaccessible. (Jefferies et al, 2007)
-
Structure and Function Relearning Based on the notion that
persons with
conceptual apraxia have poor mechanical knowledge and problem
solving with respect to objects (Goldenberg 2001).
Re- educate patients on the relationship between the structure
of objects and their function. E.g. What features of objects go
with what functions. (Mechanical Problem Solving)
-
Cubelli et al.1991: Single case study: Client’s acquisition of
communicative gestures improved with Structure/Function training
coupled with modeling gestures that represent the use of the
object.
Goldenberg & Hagmann, 1998, 2001 Studies found that this
“exploratory intervention” was not successful in changing function
in contrast to direct Errorless ADL interventionExploration
training involved: explanation, copying, touching, comparison
between objects, comparison of objects with photographs
-
Limit objects for a task to those needed to decrease confusion
caused by objects that might afford similar actions.
Highlighting objects with a visual symbol of the action may cue
the action associated with the object. (Miller, 1986)
Pictures demonstrating object function for common objects (in
context)
Bypass the conceptual system and request tasks through
imitation
Teach client to self cue by humming/verbalizing rhythmically
through a task – up/down/up/down
Utilize errors such as perseveration to start and complete an
action – e.g. feeding
-
Why address production errors?
Important in relearning communicative gestures
Important in increasing efficiency of movement
Two types of problems:Correction of production errors, spatial
and temporal
Recognition/awareness of making errors
-
Sample Model (Based on Maher et al., 1991)
1. Select gestures for common items used in tasks important to
the client (number could be determined or could select
communicative gestures)
2. Request task using multiple cues (actual tool, picture of
tool, verbal, imitation). Fade cues until you get correct
production of gesture to visual target tool.
3. Provide feedback immediately on correctness of response
4. Correct error using physical manipulation or imitation
5. Set criterion of correct execution 3 times before moving
on.
-
Targeting approach of limb to task, positioning of hand and
activating the correct joint using verbal guidance and repetition,
(Ochipa et al, 1995)
-
2000 RCT: Training was graded for each type of gesture
(transitive, intransitive symbolic and non-symbolic gestures.
E.g. Transitive Gestures: Tool Use – Picture of someone doing a
gesture – Picture of tool
Participants cued manually, verbally, visually
50 mins, 3 Xs per week, 35 sessions produce improved performance
on untrained IA and IMA tasks. No long term follow-up.
2006 RCT: Participants treated for apraxia 50 mins, 3 Xs per
week, 30 sessions improved in praxis
measures for ideational and ideomotor apraxia and ADL (caregiver
burden) – effects sustained 2 months post stroke
-
If client can detect error but does not, slow down the
activity
If client cannot detect error utilize:
Stop action
Videotape
awareness training
-
Most logical focus
Most articles address this method of rehabilitation
-
Theoretical roots in the Conductive Education technique (Cotton
and Sutton, 1986)
Aimed at reorganization of action through using speech to
regulate movement
Utilized in studies and reports by Wilson (1986) and Pilgrim and
Humphreys (1994), Butler
-
break the desired movement/action down into sub-movements.
client executes each sub-movement while the instructor (&
client) verbalize the intent of each sub movement & indicates
timing of movement & perhaps sequencing
assistance to complete each sub movement is given as
required
assistance is faded and then the verbal mediation is faded (in
original form of conductive education, the client is instructed to
internalize this mediated speech or say the instructions to
his/herself)
-
not been investigated in isolation in apraxia intervention
literature but has been used for procedural memory types of
training (Wilson, 1987)
objective is to reestablish the ordered connection of the
subtasks by increasing demands on the client to perform additional
links of the chain together
-
Curran, M. C., Hussain, Z., Park, N. W. (presented at 109th
meeting APA, San Francico [email protected]
Goal: To teach novel naturalistic skills (e.g. wheelchair
transfers, preparing food)
Clients who were given a demonstration with verbal descriptions
accompanying each step (verbal scaffolding) performed in a superior
fashion to those who had a demonstration only.
mailto:[email protected]
-
Picture cards with steps of action
Checklists
Lay out objects in order of action
Use of recorders
-
van Heugten, 1998,200; Donkervoort et al. 2001, Guesgens et al.
2006, 2007
Intervention geared at phases of activity with problems
1. Initiation (selection of action and objects). Instructions
were the focus of intervention
2. Performance (executing the activity)
Assistance
3. Correcting and Controlling Activity
Feedback Strategies
-
van Heugten et al. 1998 ◦ pre/post no control group, ◦ 12 weeks
of (3 – 5 xs/wk, 30 mins) training ◦ 33 subjects improved on motor
function (Motricity
Index), apraxia tests (object use and imitation) and to a
greater extent on ADL observation and Barthel
van Heugten et al. 2000 ◦ used previous treatment cohort and
added control
cohort of non-apraxic participants to compare co-morbidities
◦ demonstrated improvements could occur with cognitive
co-morbidity
◦ most severe apraxic participants (praxis and motor control)
initially improved the most
-
Donkervoort et al. 2001 ◦ strategy training experimental and
usual-treatment control
group – used previous tests◦ tested 8 weeks and 5 months –
treatment time average 25
sessions and 15 hrs (strategy group) and 27 sessions and 19hrs
(control)
◦ strategy training group showed superior performance on ADL
observation test
◦ no difference 5 months follow-up
Geuegens et al. 2006◦ examined trained and untrained ADL
observation tasks in
study above. ◦ change scores in strategy training group were
larger for
non-trained tasks than in usual treatment group
-
van Heugten et al. 1998 ◦ pre/post no control group, ◦ 12 weeks
of (3 – 5 xs/wk, 30 mins) training ◦ 33 subjects improved on motor
function (Motricity
Index), apraxia tests (object use and imitation) and to a
greater extent on ADL observation and Barthel
van Heugten et al. 2000 ◦ used previous treatment cohort and
added control
cohort of non-apraxic participants to compare co-morbidities
◦ demonstrated improvements could occur with cognitive
co-morbidity
◦ most severe apraxic participants (praxis and motor control)
initially improved the most
-
Geusgens et al, 2007
29 participants with apraxia
8 weeks strategy training on 4 out of 6 tasks selected from AMPS
tasks with same level of difficulty. Two were untrained.
Tested pre-treatment, 8 weeks, 8 weeks at home and 5 months
Replicated earlier studies. Strategy training Improved ADL
scores on trained and untrained tasks at hospital, home and 5
months later and was maintained over time.
Apraxia scores also improved
-
Direct Treatment: Focused on errorless completion of ADL;
Support withdrawn when client could do on own; used hand over hand
- “parallel” concurrent imitation – demonstration
◦ 15 subjects
◦ 1of 3 activities trained per week followed by a an ADL test.
Repeated until subjects could perform with 0 or 1 fatal error
◦ no improvement on untrained tasks
◦ 6 months later 7 were retested. Improvements were maintained
in only those who practiced at home.
-
◦ Compared direct treatment and exploratory treatment.
◦ Direct therapy done in intervals of 6 sessions – 1 hour each.
4 activities trained. One pair were trained with exploratory and
then direct. Next pair reversed. 1 week post tested with a variant
of objects used. 3 months tested using original objects
◦ Exploratory not effective. Direct Treatment post ADL
assessment showed reduction in errors (reparable and fatal) &
need for assistance
◦ Treatment effects were maintained on follow-up but error rates
were increased with different tools.
◦ Concluded training should be specific to individual
-
Capitalizing on Mirror Neuron System – Action Observation, Motor
Imagery and Imitation (Garrison et al, 2010)
Wu et al., 2011: Case study combining mental and physical
practice with a 44 yr. old male with hemiparesis and ideomotor
apraxia◦ Tasks practiced: Reach and grasp for cup and turning
pages◦ Person first physically practiced tasks for the day for
30
mins then did 30 mins of audio guided mental practice for the
task. 3xs/week, 6 weeks
◦ Post intervention demonstrated improved function on Arm
Mobility Scale and reported improved performance and satisfaction
untrained tasks (COPM).
-
Alex Milhailidis, Geoff Fernie & colleagues
(http://www.iatsl.org)
-
Client’s hands, the soap and the towel tracked through the video
feed from overhead camera
Using artificial intelligence, the system can play a verbal
audio prompt if (and only if) the client misses or repeats a step
in the activity
Prompt specificity automatically adjusts to suit the client’s
abilities
3rd set of clinical trials are underway, which also investigate
the use of video cues
No images are recorded and the system runs autonomously
-
Mr. P. is a 65 yr. old male with a left hemisphere bleed
affecting his frontal and parietal areas. He has a mild receptive
aphasia. He has difficulty producing movements in all aspects of
apraxia
testing – pantomime, imitation and object use and multiple
object tests. He can recognize objects.
During everyday tasks he misuses objects and often picks up any
object to start a task.
Currently he needs help with dressing and grooming. He can eat
on his own.
He has a 6 week length of stay. He will return to live with his
wife and children but will be alone during the lunch hour. He wants
to prepare lunch for himself at home.
What is your approach?
-
51 yr. old person with stroke affecting left parietal area
On testing, she can pantomime to verbal command and can match
objects and gestures but makes spatial and timing errors during
execution of tasks. This suggests she has preserved conceptual
abilities. Imitation of postures demonstrates the same types of
awkward posturing. In everyday tasks such as brushing her teeth and
putting sugar in her tea, she grasps the correct tool but does so
incorrectly. She keeps on attempting these tasks though she is
failing.
What type of apraxia?
What approach would you choose?
-
Interventions choices are still limited in apraxia intervention.
The team are left to their own creativity to develop or co-develop
strategies with the client to achieve daily living activities
Occupation based interventions seem the most practical in
current climate
Inspired strategies for treating people with apraxia that stem
from the understanding of praxis literature should be shared and
evaluated.
Bring on the clinical case reports and studies!
-
Bienkiewicz, M., Brandi, M., Goldenberg, G., et al. (2014). The
tool in the brain: apraxia in ADL behavioural and neurological
correlates of apraxia in daily living. Frontiers in psychology, 5,
1-13.
Butler,(2000) J. Rehabilitation in severe ideomotor apraxia
using sensory stimulation strategies: a single case design.
BJOT,63, 319 –328.
Butler, J. (1997) Intervention effectiveness: Evidence from a
case study of ideomotor and ideational apraxia. BJOT, 60, 491 –
497.
Butler, JA. (2002) How comparable are tests of apraxia? Clinical
Rehabilitation, 16, 389-398.
Buxbaum, L.J. (2001). Ideomotor Apraxia: a Call to Action.
Neurocase, 7(6), 445-458.
Buxbaum, L.J., Haaland, K.Y., Hallett, M., et al. (2008).
Treatment of Limb Apraxia: Moving Forward to Improved Action.
American Journal of Physical Medicine & Rehabilitation, 87(2),
149-161.
Cantagallo, A., Maini, M. & Rumiati, R. (2012). The
cognitive rehabilitation of limb apraxia in patients with stroke.
Neuropsychological Rehabilitation, 22(3), 473-488.
Code C, Gaunt C. Treating severe speech and limb apraxia in a
case of aphasia. British Journal of Disorders of Communication
1986;21:11-20
Cubelli R, Trentini P, Montagna CG (1991) Re-education of
gestural communication in a case of chronic global aphasia and limb
apraxia. Cognitive Neuropsychology 1991;8:369 –380
Daumuller, M. (2010). Therapy to improve gestural expression in
aphasia: a controlled clinical trial. Clinical rehabilitation, 24,
55-65.
De Renzi, E. Methods of limb apraxia examination and their
bearing on interpretation of the disorder.(1985) In Roy, E.A. ed.
Neruopsychological Studies of Apraxia and Related Disorders.
Amsterdam: Elsevier Science Publishers, 45 – 64.
De Renzi, E. & Luchelli, F. (1988). Ideomotor apraxia.
Brain, 111, 1173 – 1185.
Donkervoort, M., J. Dekker, et al. (2001). "Efficacy of strategy
training in left hemisphere stroke patients with apraxia: A
randomised clinical trial." Neuropsychological Rehabilitation
11(5): 549-566.
Donkervoort M, Dekker J, van den Ende E, Stehmann-Saris JC,
Deelman BG. Prevalence of apraxia among patients with a first left
hemisphere stroke in rehabilitation centres and nursing homes.
Clinical Rehabilitation 2000;14:130 – 136
Foundas A, Macauley BL, Raymer AM, Mayer LM, Heilman KM, Rothi
LJG. Ecological implications of limb apraxia: evidence from
mealtime behaviour. Journal of the International Neuropsychological
Society 1995;1:62 – 66.
Geusgens, C.A., Van Heugten, C.M., Cooijmans, J.P., et al.
(2007). Transfer effects of a cognitive strategy training for
stroke patients with apraxia. Journal of Clinical and Experimental
Neuropsychology, 29(8), 831-841.
Geusgens, C., van Heugten, C., Donkervoort, M., et al. (2006).
Transfer of training effects in stroke patients with apraxia: an
exploratory study. Neuropsychological Rehabilitation, 16(2),
213-229.
-
Goldenberg, G., Daumuller, M. & Hagmann, S. (2010).
Assessment and therapy of complex activities of daily living in
apraxia. Neuropsychological Rehabilitation, 11(2), 147-169.
Goldenberg, G & Hagmann, S. (1998). Therapy of activities of
daily living in patients with apraxia. Neuropsychological
Rehabilitation, 8. 123 – 141.
Goldenberg. G., Daumuller, M. & Hagmann, S. (2001).
Asessment and therapy of complex activities in daily living in
apraxia. Neuropsychological Rehabilitation, 11, 147- 169.
Heilman KM, Rothi, LJG. Limb apraxia: A look back. In: Rothi LJ,
Heilman KM, editors. Apraxia: The neuropsychology of action. Hove,
Psychology Press, 1997: 7-18
Heilman KM, Rothi J, Valenstein E. Two forms of ideomotor
apraxia. Neurology 1982;32: 342 –346
Heugten, C. M. v., J. Dekker, et al. (1998). "Outcome of
strategy training in stroke patients with apraxia: a phase II
study." Clinical Rehabilitation 12: 294-303.
Heugten, C. M. v., J. Dekker, et al. (2000). "Rehabilitation of
stroke patients with apraxia: the role of additional cognitive and
motor impairments." Disability and Rehabilitation 22(12):
547-554.
Kobayashi, S. and Y. Ugawa (2013). "Relationships between
Aphasia and Apraxia." Journal of Neurology and Translational
Neuroscience 2 (1)(1028): 1-5.
Lindsten-Mcqueen, K., Weiner, N.W., Wang, H., Josman, N. &
Connor, L.T. (2014). Systematic review of apraxia treatments to
improve occupational performance outcomes. OTJR: Occupation,
Participation and Heath, 34(4), 183-192.
Maher, L. M. & Ochipa, C. (1997). Management and treatment
of limb apraxia. In. Rothi, L.J.G. & Heilman, K. M. eds.
Apraxia: The Neuropsychology of Action. East Sussex, UK: Psychology
Press, 75 – 91.
Maher, L. M., Reed, E., Schwartz, M. F., Montgomery, M., &
Palmer, C. (1990) Buttering a hot cup of coffee. In. Tupper, D. E
& Cicerone, K. D. eds. The neuropsychology of everyday life.
Boston: Kluwer Academic Publishers. 259 – 285.
Maher L M, Rothi L, JG Greenwald, M L. Treatment of gesture
impairment: a single case. American Speech and Hearing Association
1991;33:195
Pool, J. L.(1998) Effects of apraxia on the ability to learn
one-handed shoe tying. The Occupational Therapy Journal of
Research, 18, 99 – 388.
Rothi, L.J.G & Heilmann, K. M. (1997). Apraxia: The
neuropsychology of action. Hove,UK: Psychology Press
Rothi, L.J.G., Raymer, A. M. & Heilman, K. M. (1997). Limb
Praxis Assessment. In. Rothi, L.J.G. & Heilman, K. M. eds.
Apraxia: The Neuropsychology of Action. East Sussex, UK: Psychology
Press, 61- 73.
Rothi, L.J.G., Ochipa, C. & Heilman, K. M. (1997). A
cognitive neuropsychological model of limb praxis and apraxia. In.
Rothi, L.J.G. & Heilman, K. M. eds. Apraxia: The
Neuropsychology of Action. East Sussex, UK: Psychology Press, 29 -
49.
Roy, E. Hand preference, manual assymentries and limb apraxia.
In Elliott, D., & Roy, E. A. Manual Assymetries in Motor
Performance. London: CRC Press, 215 – 236.
-
Roy, E.A. & Square, P. A. Common considerations in the study
of limb, verbal and oral apraxia. In Roy, E.A. ed.
NeruopsychologicalStudies of Apraxia and Related Disorders.
Amsterdam: Elsevier Science Publishers, 111 – 162.
Smania, N., Aglioti, S.M., Girardi, F., et al. (2006).
Rehabilitation of limb apraxia improves daily life activities in
patients with stroke. Neurology, 67(11), 2050-2052.
Smania N, Girardi F, Domenicali C, Lora E., Aglioti S. The
rehabilitation of limb apraxia: A study in left-brain-damaged
patients. Archives of Physical Medicine Rehabilitation 2000;81:379
– 388
Stamenova, V., Black, S. E., & Roy, E. A. (2012). An update
on the conceptual-production systems
model of apraxia: Evidence from stroke. Brain and Cognition,
80,53–63. doi:10.1016/j.bandc.
2012.03.009
Van Heugten, C. M., Dekker, J., Deelman, B. G., Stehmann-Saris,
J. C., & Kinebanian, A. (2000) Rehabilitation of stroke
patients with apraxia: the role of additonal cognitive and motor
impairments. Disability and Rehabilitation, 22, 547 – 554.
Van Heugten, C. M., Dekker, Deelman, B. G., Stehmann-Saris, J.
C., & Kinebanian, A. (1999) Assessment of disabilities in
stroke patients with apraxia: internal consistency and
inter-observer reliability. The Occupational Therapy Journal of
Research, 19, 55 –73.
Vanbellington, T., Kersten, B., Van Hemelrijk, B., et al.
(2010). European Journal of Neurology, 17(1), 59-66.
West, C., Bowen, A., Hesketh, A. & Vail, A. (2008).
Interventions for motor apraxia following stroke. The Cochrane
database of systematic reviews, 1, CD004132.