URINARY DISTURBANCE MANAGEMENT IN ELDERLY
URINARY INCONTINENCE IN ELDERLYDr dr RA Tuty Kuswardhani SpPD
KGer; MARS RS PTN UNUD BALIDivisi Geriatri SMF llmu Penyakit Dalam
FK UNUD
Mrs. L,80 yo; explains that, on the night of the falls and gets
fracture, she woke up to urinate around midnight, and the broke her
shoulder. The conversation reminded Mrs. L that she experienced
frequent nocturnal urination during the hospitalization and on
several occasions was unable to get to the toilet on time and
become incontine she develops urinary urgency as soon as the key
goes into the lock. She has occasionally experienced leakage when
sneezing, standing, or coughing but this most commonly occurs when
she is trying to hold her urine during one of her urgent episodes.
Still, she did not view her urinary pattern as a big problem until
her recent hospitalization.Mrs. L visited her gynecologist 1 year
ago. She has no cystocele, rectocele, or uterine prolapse. She
denies dysuria, fever, or constipation.
QuestionWhat factors contributed to the patients urinary
incontinence?How should her problem be approached? What non
pharmacologic approaches could be of benefit to this patient?
CASE2
3UI - unconsencius not wanted to induce social and problem
hygiene
(International Continence Society, 2002)
Definition of UI
@ Data Geriatry SANGLAH Hospital Denpasar : UI FEMALE IN 60-85
YO (2011) Prevalens 21 % @ USA prevalens: 47% post menopause
(2012)
Prevalence Urinary Incontinence5CLINICAL IMPLICATION UIClinical
significant : health physic and emosional Incontinence Urine
stress, depression ,limitation function sex, risk falls
mortality
Embarrassment Contributes to Rationalization of Condition as not
worth medical attentionEmbarassementDirtySign of old ageSmellNot
worth disturbing the DoctorDisgustChild-likeAstellas Market
Research : Branding Science 20067Type of Urinary Incontinence (Peet
et al ; 2005):Rule out of Transient CausesD eliriumI nfectionA
trophyP harmaceuticalsP sychologicE ndocrine or excess urine
outputR estricted mobilityS tool impaction9
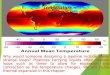
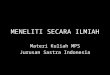
Normal Bladder Over active BladderOverflow BladderStress
Bladder
Neurogenic BladderImages Of Bladder Condition in Normal and Four
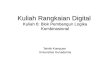
Types of Urinary Incontinence10SKIN: Urinary Incontinence :
iritation, mechanic ,fraillty, infection Dermatitis Perineum/
Incontinence Dermatitis Infection 1 - 2 organisme: Tinea and
Candida Albicans
HealthyUnHealthy
UI AND SKIN INFECTIONIncontinens Urin in MANBPH : Gland prostat
>
> 60 YO: 60% > 90 %: 80 YO, LUTS and BPH
SIGN : Obstruction, < path urinary urgency ; .> urinary at
night; incontinence
Gambar tetep yang lama12UI IN FEMALEMenopause estrogen in
menopause women caused in supportive: tissue, thinning of urethral
and vaginal epitel, vascularisation of urethral submucosa, cellular
Estrogen defisiensi is an important ethiology of lower urinary
tract disease including urge symptoms(frequency, nocturia, urgency,
incontinence urge)
The role of Receptor Estrogen is IMPORTANT in mechanism on
Stress Urinary Incontinence
Assesment : History and Physical :Pertanyaan : Apakah anda
mengompol / BAK atau BAB tanpa disadari ?0tidak
pernah1,0kadang-kadang kehilangan kontrol berkemih/menggunakan alat
bantu untuk berkemih & BAB2,5kehilangan kontrol berkemih
sedikitnya sekali dalam sebulan4,0kehilangan kontrol berkemih
sedikitnya 2 kali sebulan/kadang-kadang kehilangan kontrol
BAB5,0kehilangan kontrol BAB sedikitnya sekali dalam
sebulan5,5kehilangan kontrol berkemih sedikitnya sekali dalam
seminggu6,5kehilangan kontrol BAB sedikitnya 2 kali
sebulan8,0kehilangan kontrol BAB sedikitnya sekali
seminggu/kehilangan kontrol berkemih sedikitnya sekali setiap
hari10kehilangan kontrol BAB sedikitnya sekali sehari10,5tidak bisa
mengontrol fungsi berkemih sama sekali11,5tidak bisa mengontrol BAB
sama sekaliTotal SkorIncontinence Scanning Incontinence classified
: 0 : No Incontinence 1 2,5 : Mild Incontinence 4,0 6,5 : Moderate
Incontinence 8 : Severe Incontinence(Johnston B, UCSF.
2009)DIAGNOSIS 14UI DAILY CARD
Warning TimeThe time between the onset of urgency and or
incontinence
Significant to patients since it represents the time they have
to find a bathroom and avoid possible incontinence
16RD slide
Warning time potential to be one of most useful measures but
difficulty in definition when the start the clock at which
sensation
Affected by external factorsUsing the Urgency Perception Score
(UPS) with a Patient in PracticeThe Urgency Perception Scale
(UPS)Describes the ability of a patient to hold urine and finish
tasks before going to the toilet
Cardozo L et al BJU Int 2005; 95:591-59617PHYSICALABDOMEN :
peritonitis, FLUID, mass
Rectum : impaksion, sphincter tonus, sensasi perineal,
prostat
Man: skin perineum
Female: prolapsus utery
Atrophy organ: pelvis, mass , muscle
Volume urine : test cough
VOLUME PVRURINALYSIS
EVALUATION18THERAPY type functional in man Condom CateterFemale
tampon , pampers Technic Toileting Bladder TrainingKaegel Exercise
1.NON PHARMACOLOGYINTERVENTION Kaegel exerciseMenemukan MUSCLE yang
tepat Menahan otot yang digunakan Jika merasakan perasaan tertarik
maka siap latihan pelvicJangan lakukan pada otot lain pada waktu
bersamaan atau menahan nafas Hanya tekan otot pelvic, tarik otot
pelvic dan tahan selama 3 detik Kemudian rileks selama 3 detik,
Ulangi jangan berlebihan, Latihan sampai 3 X -10 X
THERAPY NON PHARMACOLOGY agonist cholinergic , inhibitor alpha
adrenergic,anti muscarinic
BetaneCol
PrazosinAgonis cholinergicDosis 10 25 mg/oral 6 8 hrs in elderly
SE: UlCus PeptiCum, hYpotensi on OF Postural
Inhibitor alpha adrenergicDosis 1 mg/oral 8 12 hrs hypotenti on
posturalOxybutinin Antimuscarinic effect relaxationMetabolite in
Reseptor M antagonist muscarinic selective receptor M1, M3, M4
Dosis :2,5 5 mg/oral, 24 x perday, patch 3 mg,9 mg/ day syrup 5mg /
15ml, transdermal gel 3%, 9%
SolifenacineSolifenacin Succinate receptor antagonist
cholinergic Dosis : 510 mg/oral /12 x per day CKD & hepar
IMPAIRMENT NO recommendation for dosis > 5mg / day 2. THERAPY
PHARMACOLOGY
Name21Name agonist cholinergic , inhibitor alfa adrenergic, anti
muscarinicTolterodineAntagonis kompetitif anti muscarinik selective
dosis 2 mg/ day Tolterodine : frecuension urine tolerance >,
withdrawl