Embed Size (px)
Citation preview

fain, 52 (19931 179-185 0 1993 Elsevier Science Publishers B.V. All rights reserved 03~-3959/93/$06.00
179
PAIN 02199
CSF and plasma concentrations of morphine and morphine glucuronides in cancer patients receiving epidural morphine
Hgkan Samuelsson ‘, Thomas Hedner b, Richard Venn ‘*’ and Andrew ~icha~kiewicz ’ Departments of ’ Anaesthesia, Central Hospital, Bor& fdwedeni, ’ Clinical Pharrnachology, Sahlgrenska University Hospital, Giiteborg (Sweden)
and L Pain Research Institute, Licerpool (UK)
(Received 3 July 1992, revison received 24 August 1992, accepted 28 August 1992)
Summary Thirty-five cancer patients, treated with chronic epidural morphine, were assayed for plasma and cerebrospinal fluid (CSF) minimum steady-state concentrations (Css min) of morphine (Ml, morphine-3-glucuronide (M3Gl and morphine-6glucuronide (M6Gl by high performance liquid chromatography (HPLC). A linear dose-con- centration relationship was found for the 3 substances in plasma and for morphine and M3G in CSF. The mean + S.E.M. CSF/plasma morphine ratio was 158 + 43. In CSF, the concentrations of morphine exceeded those of the metabolites substantially and, normahzed to morphine, the mean CSF M/M3G/M6G ratio was 1: 0.05 : 0.02. In plasma, the metabolite concentrations were higher than the parent drug and the plasma M/M3G/M6G ratio was 1: 12 : 3. The mean M3G and M6G concentrations in CSF were 40-60% of those found in plasma. Indication of cerebral formation of M3G was found in 1 patient. Pain relief, evaluated by a visual analogue scale (VAS), did not correlate with the CSF M3G concentrations or with the M3G/M ratio. CSF M6G concentrations were low and did not contribute to any detectable analgesia. We conclude that after epidural administration of morphine, the M3G and M6G metabolites in CSF are low compared to unchanged morphine and seem to have little influence on analgesia. Howewer, the fact that a significant passage of the glucuronide metabolites occurs to the CSF may indicate a role in morphine analgesia after other routes of administration.
Key words: Pain; Cancer; Morphine; Morphine metabolites; M3G; M6G
Introdudtion
During oral or intravenous administration of mor- phine (M) in man, glucuronidation at the phenolic and alcoholic hydroxyi groups at positions 3 and 6, respec- tively, occurs to a large extent in the liver (McQuay and Moore 1984; Joel et al. 1985). This metabolic processing results in the formation of morphine3- glucuronide (M3G) and morphine-6-glucuronide (M6G) which may be found in large concentrations in plasma. In fact, during chronic therapy, circulating concentra- tions of M3’G and M6G markedly exceed those of morphine itself, since hepatic metabolism converts ap-
’ Present address: Department of Drug Metabolism, Pfizer Central Research, Sandwich, Kent CT13 9NJ, UK.
Correspondence to: Dr. Hdkan Samuelsson, Pain Section, Depart- ment of Anaesthesia, Central Hospital, S-501 82 Boris, Sweden.
proximately 70% of morphine into M3G (55%) and M6G (15%) (Boerner et al. 1975; Osborne et al. 1990). Among opioids, morphine is relative water soluble, which also would be expected for the glucuronide metabolites. However, an unexpected high Iipophilicity has recently been reported for M3G and M6G (Car- rupt et al. 1991) which implies that significant dura passage may occur.
Electrophysiological studies on spinal dorsal horn neurones have shown that spinally applied M6G pro- duces a profound suppression of C fibre-evoked re- sponses whereas no such inhibition could be observed for M3G (Sullivan et al. 1989). Interestingly, animal experiments have shown that M6G is a potent I*-opioid agonist, which may significantly contribute to the anal- getic response after morphine administration (Shimo- mura et al. 1971; Yoshimura et al. 1973; Pasternak et al. 1987; Abbot and Palmour 1988; Paul et al. 1989; Gong et al. 1991). M3G, on the other hand, exhibits no

analgesic effects (Shimomura et al. 1971; Yoshimura et al. 1973; Gong et al. 1991) or may even induce a slight hyperalgesia or behavioural excitation (Labella et al. 1979; Woolf 1981; Yaksh 1986; Gong et al. 1992). Recent animal studies also show that M3G antagonises the analgesic effects of morphine and of M6G (Smith et al. 1990; Gong et al. 1992). In man, the potential contribution of the morphine glucuronides to the anal-
gesic response of epidurally or spinally administered morphine is not yet fully known, since M3G and M6G concentrations in the vicinity of the receptor, i.e.. in
the cerebropinal fluid (CSF), have not been thoroughly investigated.
In the present study, taking experimental data into account, our aim was to investigate if concentrations of M3G and/or M6G reached in lumbar CSF could be of relevance for the analgesic response of epidurally ad- ministered morphine in patients with cancer pain. Moreover, considering in vitro post-mortem studies showing that glucuronidation may occur within brain
tissue (Wahlstrom ct al. 19881, we also wanted to see if we could provide clinical support for a brain formation of M3G and M6G by measuring CSF to plasma con- centration gradients.
Patients and methods
Thirty-five patients with advanced cancer pain were included in
the study. All patients gave informed consent prior to inclusion. The
study was approved by the Ethics Committee of the Medical Faculty.
University of Goteborg, Sweden. The patients were on oral or
systemic opioid medication with insufficient pain relief when in-
cluded. Once an optimal intermittent epidural morphine dose on a
fixed time schedule was established, a blood and a CSF sample were
drawn after at least 3 days of stable dosage conditions in order to
ensure pharmacokinetic steady state for morphine as well as the
metabolites studied (Osborne et al. 1990). Lumbar puncture was
carried out at the L?-L, or L?-L, interspaces to obtain CSF and
blood was collected from an antecubital vein for plasma concentra-
tion measurements. All sampling was performed immediately before
a scheduled dose was to be given. The plasma was separated by
centrifugation and the samples were frozen at -20°C and later
analysed for morphine, M3G and M6G by high performance liquid
chromatography (HPLC) with fluorescence detection (Venn et al.
199Oa). The lowest determinable concentrations were 0.003, 0.001
and 0.003 nmol/ml for morphine, M3G and M6G. respectively.
While CSF morphine and M3G values were above detection limit in
all patients, CSF concentrations of M6G were available in 14 of 35 cases. In plasma, all M3G concentrations exceeded the lowest deter-
minable concentrations while values for morphine and M6G were
obtained in 25 and 27 patients, respectively. The calculations have
heen based on the determinable values only. In order to evaluate the
impact of the M6G concentrations below detection limit on the
results obtained. we also performed calculations where values below
detection limit were given a numerical MhG value which was one-half
that of the lower limit of detection, i.e., 0.002 nmol/ml.
Pain relief was evaluated in 27 patients, using a 100 mm visual
analogue scale (VAS) before the epidural treatment was instituted
and immediately before the blood and CSF samples were obtained.
The reduction in the VAS score after introduction of epidural
TABLE I
MEANS + S.E.M.. MEDIANS AND RANGES OF METABOLITE
TO MORPHINE RATIOS AND CSF OF PLASMA RATIOS
M3G = morphine-3Lglucuronide. M6G = morphine-6glucuronide.
Ratio Mean i S.E. Median Range
M3G : morphine.
plasma tn = 25) I? i 1.5 x.4 0.25 -116
M6G : morphine.
plasma tn = 21) 2.7 f 0.5 2.0 I).05 x.0
M3G: morphine.
CSF (n = 35) 0.05 f 0.01 0.03 0.003~ 0.26
MhG: morphine,
CSF tn = 14) 0.02 + 0.007 0.01 0.002- 0.11)
CSF: plasma. mor-
phine (n = 24) IS8 +43 66 2.5 -X06
CSF: plasma,
M3G (n = 35) 0.59 + 0.27 0.27 O.IO - 9.x
CSF: plasma,
M6G (n = 14) It.41 +- 0.07 0.33 0. I I - 0.97
morphine was expressed as percent (“r VAS) improvement com-
pared to the initial VAS score.
Results are presented as meaniS.E.M. as well as medians and
ranges. Linear regression was tested by the Spearman’s rank-order
correlation test. A P value of 0.05 or lower was considered as
significant.
Results
The daily epidural dose of morphine during steady- state conditions ranged from 8 to 120 mg. In general, the dose was titrated to the best possible pain relief or to a level where unacceptable side effects occurred.
Relationships between plasma and CSF concentrations of morphine and its metabolites
The ratios between the metabolites and parent drug as well as the CSF/plasma ratios for each substance are given in Table I. The epidural administration of morphine resulted in high CSF concentrations of un- changed morphine compared to plasma. The mean CSF/plasma morphine ratio was 158 with a range of 2.5-806. In the CSF compartment, the concentration of unchanged morphine considerably exceeded that of the M3G and M6G metabolites. The CSF M/ M3G/M6G ratio normalized relative to morphine was 1 : 0.05 : 0.02. In contrast the plasma metabolites were higher than the parent drug and plasma M/M3G/ M6G ratio was 1: 12: 3. The CSF/plasma ratios for M3G and M6G were 0.59 (range: 0.1-9.8) and 0.41 (range: 0.1 l-0.97), respectively, indicative of a substan- tial passage of the metabolites across the blood-brain barrier. These ratios were independent of the dose of epidural morphine given. Calculations performed in- cluding the below-detection limit M6G values gave

181
y =,0006x +.0294 60
y = .32nx -2.7914
50 1
0
-,02 1 -10 J 0 20 40 60 80 100 120 140 0 20 40 60 60 100 120 140
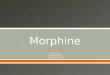
Dose in 24 hr(mg) Dose in 24 hr(mg) Fig. 1. Relationship between daily dose of epidural morphine and steady-state concentrations of morphine in plasma (n = 25, rs = 0.43, P < 0.05)
and CSF (n = 35, rc = 0.56, P < 0.01). Equations to the lines are given in the figure.
almost identical results. Thus the mean CSF M/ M3G/ M6G ratio was then 1: 0.05 : 0.01 and the plasma M/ M3G/ M6G ratio was 1: 12 : 2. The calculated M6G CSF/plasma ratio was 0.45 when these data were included.
Dose-concentration relationships The plasma and CSF concentrations of morphine
and the M3G and M6G metabolites are shown in relation to the dose in Figs. l-3. For morphine, as well as M3G and M6G, there appeared to be linear in- creases in steady-state minimum plasma and CSF con- centrations in relation to the administered epidural dose of morphine. Regression analysis using the Spear- man rank-order correlation test showed the following rs values in plasma: M (0.43, P < 0.051, M3G (0.51, P < 0.01) and M6G (0.48, P < 0.05). The corresponding values in CSF were: M (0.56, P < 0.011, M3G (0.52, P < 0.01) and M6G (0.50 P = 0.07). The rs values were
2.251 y=,o141x-,0169
2. 0
.75.
13. 25.
-.25 1 -.I 1 0 20 40 60 00 100 120 140 0 20 40 60 80 100 120 140
Dose in 24 hr (mg) Dose in 24 hr (mg)
found to be significant, except for CSF M6G regardless of whether substitution was made for the below limit of detection M6G values.
Indication of morphine degradation in the CNS The distributions of the CSF/plasma ratios for M6G
and M3G are shown in Figs. 4 and 5. All M6G values were below 1.0 while the CSF level of M3G exceeded that in plasma in 1 patient, indicating the possibility of cerebral formation of M3G (Fig. 5). Repeated sam- pling was performed in this patient, whose data are presented separately in Table II. With increasing doses of epidural morphine, as well as duration of the mor- phine therapy in that patient, the CSF/plasma ratio for M3G increased from 2.3 to 9.8. There were no indications of a corresponding increase in M6G since measured concentrations remained or decreased below the detection level.
,6-
Fig. 2. Relationship between daily dose of epidural morphine and steady-state concentrations of M3G in plasma (n = 35, rs = 0.51, P i 0.01) and
CSF (n = 35, rs = 0.52, P < 0.01). Equations to the lines are given in the figure.

-,I 1 0 20 40 60 a0 100 120 140
Dose tn 24 hr (mg)
20 40 60 60 100 120 140
Doss in 24 hr (mg)
Fig. 3. relationship between daily dose of epidural morphism and steady-state c~)nc~ntrations of MhG in plasma (n = 27. I’, = 0.38. P < 0.05) and
CSF (n = 14. r, = 0.50. P = 0.07). Equation to the line is given for plasma. Linear regression was not proven to he significant for CSF.
0.3 OS 0.7
M6G CSFl plaMla ratio
Fig. 4. Distribution of CT/plasma ratios of M6G in patients recek
<O.l 0.1 0.3 0.5 0.7 0.9 9.7
M3G CSFI plasma ratii
ing chronic rpidural morphine therapy. All ratios are < 1 .O, Fig. 5. Distribution of CSF/plasma ratios of M3G in patients receiv-
ing chronic epidural morphine therapy. One patient with a ratio of
0.7 indicates the possibility of CNS ~[~rmation of M3G.
Possible influence of M3G and M6G or1 pairs w&j
The CSF M3G/M ratio (ranging from 0.003 to 0.26) relief. As seen in Fig. 6, no such relationship was in relation to pain relief is shown in Fig. 6. Since M3G found, neither was there any correlation between the may have potentiai hyperalgetic properties, it might he M3G concentrations and pain relief. In the patients in expected that there could be a negative correlation whom pain analysis were performed, the M6G concen- between the M3G/M ratio and the degree of pain trations in CSF were close to or below the detection
TABLE II
DATA FROM REPEATED SAMPLING IN ONE PATIENT WITH POTENTIAL BRAIN M3G ~ORMA.~It~~~
M = morphine: M3G = morphine-3-glucilronide, M6G = Inorphine-h-ylucuronide, VAS = visual aoalogue scale and n.d. = non-detectable.
- Sampling
on day
Prior to
6
21
EpiduraG
dose (my/d)
-_-_
2-t
48
- Pain intensity MCSSmin MhG Css min ~ M3G Css rnin
VAS (mm) (nmol/ml) (nmol/mU (nmol/ml) __-
plasma CSF plasma CSF plasma CSF ~-____- ____-
80 _ _
30 n.d. 5.6 n.d. 0.(113 0.02H O.OhS
15 n.d. s.3 n.d. n.d. 0.032 0.313 ~________l__l~ --~

too
1 0
p o n
00 - 0
0 .n 00
H 60-I n z 0
._ ii 0. 40- z;p 0
‘U
:i’, 0.0 0.1 0.2 0.3
CSF M3GfM ratio Fig. 6. Pain relief related to CSF M3G/M ratios in cancer patients receiving chronic epidural morphine therapy. The ratios are low and
no correlation could be detected.
limit and, therefore, no corresponding analysis was performed for M6G.
Discussion
The principai findings in this study were the extent to which the glucuronides passed to the CSF and that epidural administration of morphine resulted in a high CSF ratio of morphine relative to the M3G and M6G metabolites. The fact that epidural administration re- sults in on average 20 and 50 times higher concentra- tions of unchanged morphine compared to M3G and M6G, respectively, in the CSF has not been previously reported. Certainly CSF concentrations of morphine metabolites after any form of administration has yet only been investigated to a limited extent (Bigler et al. 1990; Hanna et al. 1990; Poulain et aI. 1990; Venn et al. 1990b). After epidural administration of morphine, approximately 98% of the administered dose is dis- tributed to the peripheral compartment while the re- mainder, i.e., only 2% enters the CSF compartment (Nordberg 1984). Thus, the plasma morphine concen- trations seen after epidura1 morphine administration are fully comparable to those reached after an identi- cal intravenous dose. Due to this fact, the hepatic formation of the M3G and M6G metabolites after epidural administration should result in similar plasma concentrations of these metabotites as achieved after intravenous injection. In fact the piasma concentration ratio observed in our study at steady state agrees well with previous reports @awe 1986; Osborne et al. 1990) studying acute or steady-state intravenous administra-
183
tion of morphine. The plasma steady-state M3G and M6G concentrations are also linearly related to the daily dose of oral morphine @awe 1986; McQuay et al. 1990). Interestingly, the equations to the lines describ- ing the relationships for plasma morphine versus daily dose as well as plasma M6G versus daily dose were remarkably similar to those previously described (Mc- Quay et al. 19901. Thus the plasma concentration-dose linearity could be shown for epidural administration as well in this study.
The CSF/plasma ratios for M3G and M6G were on average 0.59 and 0.41, respectively, which indicates a substantiai passage of the metabolites across the blood-brain barrier. The metabolite concentrations in CSF after epidural morphine administration should be comparable to those expected after conventional intra- venous therapy. The concentrations of unchanged mor- phine achieved in CSF after epidural therapy are ap- proximateIy 100 times those reached after intravenous injection (Nordberg 1984). This is the main reason behind the high ratio of morphine relative to M3G and M6G found in the CSF after epidural administraion in the present investigation. The dose-CSF concentration relationship for morphine after epidura1 administration has previously been shown to be linear (Nordberg 1984; Samuelsson et al. 19871. This relationship was further confirmed in the present investigation. The dose-CSF concentration relationship for the main metabohtes M3G and M6G have not previousIy been studied. In our investigation there was evidence of a dose linearity which, however, was not significant for CSF M6G. The lower number of individuals with de- tectable CSF concentrations of M6G and the low con- centrations achieved are probable explanations for the lack of significant linearity in our investigation.
Morphine gIucuronides can be formed in the micro- somes isolated from human liver, kidney and gut speci- mens (Pacifici et al. 1982). Moreover, recent evidence indicates that M3G, and to some extent M6G, may be formed in the microsoma~ fraction of human brain tissue (Wahlstriim et al. 1988). The present study pre- sents in vivo data supporting this notion, since 1 of 35 patients had a M3G CSF/plasma ratio clearly exceed- ing 1.0 on two separate occasions. Futhermore, the distribution of the CSF/plasma ratios tended to be skewed towards higher ratios. It is unlikely that this finding is due to an accumulation of the M3G metabo- lite in the CSF since there was no such high ratio for M6G which should be cleared by similar mechanisms from the CSF.
We have previously demonstrated that there is no clear relationship between relief of cancer pain and steady-state CSF concentrations of unchanged mor- phine following epidural administration (Samuelsson et al. 1987; Samuelsson and Hedner 19911. Since M3G may oppose the analgetic actions of morphine (Smith

184
et al. 1990) as well as M6G (Gong et al. 1992), one might expect a negative relationship between the de- gree of pain relief and the CSF M3G/morphine ratio. However, in the present investigation, we found no evidence for such a relationship. There may be several plausible explanations for this. Firstly, CSF morphine concentrations after epidural administration are sub- stantially higher than the M3G concentrations, and therefore the possible M3G antagonism of morphine- induced analgesia may not be apparent. However, if other routes of adminstration are used which result in lower CSF concentrations of unchanged morphine, the antagonistic actions of M3G may be of clinical impor- tance. Secondly, cancer pain comprises several pain types, originating from different structures and may thus vary in responsiveness to spinal morphine analge- sia (Samuelsson and Hedner 1991). This may result in inter-individual variations in response to morphine as well as M3G which could cloud any potential clinical dose-effect relationship further. Finally, it is possible that M3G is not a functional opioid antagonist in man since animal studies may be compromised by be- havioural non-specific effects. Considering the present results and a potency ratio of 13 for M6G compared to morphine (Sullivan et al. 1989), or higher (Pasternak et al. 1987), it is likely that M6G would contribute sub- stantially to morphine analgesia, given orally or i.v. but following spinal morphine administration the M6G CSF concentrations were low and we could not detect any role in analgesia.
In conclusion, in the present study we have demon- strated the passage of the main metabolites M3G and M6G over the blood-brain barrier and that epidural administration of morphine results in lumbar CSF con- centrations of unchanged morphine which are high compared to the metabolites. Furthermore, there was evidence indicating possible cerebral formation of M3G. There was, however, no clinical evidence that M3G concentrations impaired the morphine-induced analgesia in cancer pain after epidural administration. The situation for other routes of administration such as i.v. and oral may, however, be different since such administration will result in higher concentrations of the metabolites relative to morphine.
Acknowledgements
This research was in part supported by ASTRA Lakemedel AB by the ASTRA award 1991, given to HAkan Samuelsson by the Scandinavian Association for the Study of Pain. We gratefully acknowledge the sec- retarial assistance of Miss Pia Hjert.
References
Abbott, F.V. and Palmour, R.M., Morphine-6-glucuronide: analgesic
effects and receptor binding profile in rats, Life Sci., 43 (1988)
1685-3695.
Bigler, D., Broen Christensen, C.. Eriksen, J. and Jensen, N.H.,
Morphine, morphine-h-glucuronide and morphine-3-glucuronide
concentrations in plasma and cerebrospinal fluid during long-term
high-dose intrathecal morphine administration, Pain, 41 (1990)
15-18.
Boerner, U., Abbott, S. and Roel, R.L., The metabolism of morphine
and heroin in man, Drug Metab. Rev., 4 (1975) 39-73.
Carrupt, P.A., Testa, B., Bechalany, A.. Tayar, E.N., Descas, P. and
Perrissoud, D., Morphine h-glucuronide and morphine 3-
glucuronide as molecular chameleons with unexpected lipophilic-
ity, J. Med. Chem., 34 (1991) 1272-1275.
Gong, Q.L., Hedner, T., Hedner, J.. Bjiirkman, R. and Nordberg. G.,
Antinociceptive and ventilatory effects of morphine metabolites:
morphine-6-glucuronide and morphine-3-glucuronide, Eur. J.
Pharmacol.. 193 (1991) 47-56.
Gong, Q.L., Hedner, J., Bjdrkman, R. and Hedner, T., Morphine-3-
glucuronide may functionally antagonize morphine&glucuronide
induced antinociception and ventilatory depression, Pain, 48
(1992) 249-255.
Hanna, M.H., Peat, S.J., Woodham, A.. Knibb, A. and Fung. C.,
Analgesic efficacy and CSF pharmacokinetics of intrathecal mor-
phine-6-glucuronide: comparison with morphine, Br. J. Anaesth.,
64 (1990) 547-550.
Joel, S.P., Osborne, R.J., Nixon, N.S. and Slevin, M.L., Morphine&
glucuronide, an important metabolite, Lancet, i (1985) 1099-1100.
Labella, F.S., Pinsky, C. and Havilicek, V., Morphine derivatives with
diminished opiate receptor potency show enhanced central exici-
tatory activity. Brain Res.. 174 (1979) 263-271.
McQuay, H. and Moore, A., Metabolism of narcotics. Br. Med. J.. 288 (1984) 237.
McQuay, H.J., Carroll, D.. Faura, CC., Cavaghan, D.J., Hand, C.W.
and Moore, R.A., Oral morphine in cancer pain: influences on
morphine and metabolite concentration, Clin. Pharmacol. Ther., 48 (1990) 236-244.
Nordberg, G., Pharmacokinetic aspects of spinal morphine analgesia,
Acta Anaesthesiol. Stand.. 28, Suppl. 79 (1984) 1-38.
Osborne. R.. Joel, S., Trew. D. and Slevin, M., Morphine and
metabolite behavior after different routes of morphine adminis-
tration: demonstration of the importance of the active metabolite
morphine-6-glucuronide, Clin. Pharmacol. Ther., 47 (1990) 12-19.
Pacifici, G.M., S&we, J., Kager, L. and Rane. A. Morphine glu-
curonidation in the human fetal and adult liver. Eur. J. Clin. Pharmacol., 22 (1982) 553-558.
Pasternak, G.W., Bodnar, R.J., Clark, J.A. and Inturrisi. C.E., Mor-
phine-6-glucuronide. a potent mu agonist, Life Sci., 41 (1987) 2845-2849.
Paul, D., Standifer, K.M., Inturrisi, C.E. and Pasternak, G.W., Phar-
macological characterization of morphine-h-glucuronide, a very
potent morphine metabolite, J. Pharmacol. Exp. Ther., 251 (1989) 471-483.
Poulain, P., Moran Ribon, A.. Hanks, G.W., Hoskin, P.J., Aherne,
G.W. and Chapman, D.J., CSF concentrations of morphine-6- gluouronide after oral administration of morphine, Pain, 41 (1990) 115-116.
Samuelsson, H. and Hedner, T., Pain characterization in cancer
patients and the analgetic response to epidural morphine, Pain, 46 (1991) 3-8.
Samuelsson, H.. Nordberg, G., Jledner, T. and Lindqvist, J.. CSF
and plasma morphine concentrations in cancer patients during
chronic epidural morphine therapy and its relation to pain relief, Pain, 30 (1987) 303-310.

185
Sawe, J., High-dose morphine and methadone in cancer patients, Chn. Pharmacokinet., 11 (1986) 87-106.
Shimomura, K., Kamata, O., Ueki, S., Oguri, K., Yoshimura, H. and Tsukamoto, H., Analgesic effect of morphine glucuronides, J. Exp. Med., 105 (1971) 45-52.
Smith, M.T., Watt, J.A. and Cramond, T., Morphine-3-glucuronide, a potent antagonist of morphine analgesia, Life Sci., 47 (1990) 579-585.
Sullivan, A.F., McQuay, H.J., Bailey, D. and Dickenson, A.H., The spinal antinociceptive actions of morphine metabolites morphine- 6-glucuronide and normorphine in the rat, Brain Res., 482 (1989) 219-224.
Venn, R.F. and Michalkiewicz, A., Fast reliable assay for morphine and its metabolites using high-performance liquid chromatogra- phy and native fluorescence detection, J. Chromatogr., 525 (1990a) 379-388.
Venn, R.F., Michalkiewicz, A., Hardy, P. and Wells, C., Concentra- tions of morphine, morphine metabolites and peptides in human CSF and plasma, Pain, Suppl. 5 (199Ob) S188.
Wahlstrom, A., Winblad, B., Bixo, M. and Rane, A., Human brain metabolism of morphine and naloxone, Pain, 35 (1988) 121-127.
Woolf, C.J., Intrathecal high dose morphine produce hyperalgesia in the rat, Brain Res., 209 (1981) 491-495.
Yaksh, T.L., Harty, L.G. and Onofrio, B.M., High doses of spinal morphine produce a nonopiate receptor-mediated hyperesthesia: clinical and theoretic implications, Anesthesiology, 64 (1986) 590-597.
Yoshimura, H., Ida, S., Oguri, K. and Tsukamoto, H., Biochemical basis for analgesic activity of morphine-6-glucuronide-1: penetra- tion of morphine-6-glucuronide in the brain of rats, Biochem. Pharmacol., 22 (1973) 1423-1430.






















![Donald H. Lambert Boston, Massachusetts Spinal - Epidural - [Combined Spinal Epidural]](https://img.pdfslide.us/doc/110x75/5517e537550346d5568b46b6/donald-h-lambert-boston-massachusetts-httpwwwdebunk-itorg-spinal-epidural-combined-spinal-epidural.jpg)



