Embed Size (px)
Citation preview

CRANIUM; IT’S NOT JUST A GAME: MILD & MODERATE TRAUMATIC BRAIN INJURIES IN CHILDREN
Andrew W. Kiragu, MD, FAAPInterim Chief of Pediatrics
Medical Director, PICUHennepin County Medical CenterAssistant Professor of Pediatrics
University of Minnesota

FACES OF TBI
Disclosures
• I have no relevant financial relationships with the manufacturers of any commercial products and/or commercial services discussed in this CME activity
• I do not intend to discuss any unapproved commercial product/device in this presentation

GOALS OF THE PRESENTATION
• Discuss a representative case of pediatric TBI
• Review epidemiology, evaluation and initial management of traumatic brain injury
• Briefly review pathophysiology of TBI
• Review other aspects of TBI management including follow-up, family-centered care and injury prevention

GOALS OF THE PRESENTATION
• Discuss a representative case of pediatric TBI
• Review epidemiology, evaluation and initial management of traumatic brain injury
• Briefly review pathophysiology of TBI
• Review other aspects of TBI management including follow-up, family-centered care and injury prevention

CASE REPORT• Patient FP is an 11 year-old boy who presented to
the ED after being struck by a vehicle while riding his bicycle.
• He was out riding with his friends and they had been going fairly fast downhill when he swerved to avoid an object on the road.
• Swerved into the path of a slow moving truck, was struck and flung off his bike.
• Landed on the pavement and struck his unhelmeted head. He was observed to lose consciousness for about 2-3 minutes.

CASE REPORT
• The driver called 911 and paramedics arrived to find him still lying on the sidewalk somnolent but rousable
• He opened his eyes to voice, was able to talk but was confused and could only localize pain

CASE REPORT
• Initial GCS 12 (E3, V4, M5)
• He was transported to the ED for additional evaluation and treatment

CASE REPORT• Initial Vital signs: T36.7 C, HR124, RR20, BP110/56,
SpO2 98% on RA
• Gen: more awake and somewhat combative. Bruise and swelling noted over forehead and large abrasion noted of right forearm
• HEENT: NC, swelling and bruising of forehead, PERRL, no nasal dc,
• Chest: CTA B
• CV: nl S1S2, RR increased heart rate

CASE REPORT• Abdomen: soft, NT, NABS, no HSM
• Ext: abrasion of R forearm, MAE, WWP
• Neuro: awake but somewhat combative, intermittently following commands, GCS 14(E4, V4, M6)
• Taken for head CT which significant for two small punctate hemorrhage in frontal lobe. Soft tissue swelling of forehead seen. No fracture
• Labs in ED including electrolytes and CBC normal
• Sent to PICU for overnight observation

EPIDEMIOLOGY
• There are approximately 1.7 million traumatic brain injuries sustained in the US annually
• 50,000 die;
• 235,000 are hospitalized; and
• 1.1 million are treated and released from an emergency department.

EPIDEMIOLOGY• Over 85% of the 1.7 million TBI’s occurring
annually in the US are considered mild.
• The average incidence of mild TBI was 503.1 per 100,000 population, with a peak among American Indians/Alaska Natives (1026/100,000 population) and in children younger than 5 years old (1115.2/100,000 population).
• The mechanisms by which children sustain head injury vary by activity, age, helmet use, and geographic location.

EPIDEMIOLOGY
• Among children aged 0 to 14, TBI results in over 400,000 ED visits, 2685 deaths and 37,000 hospitalizations each year. Injury rates are highest among children 0 to 4.
• Approximately 50% of patients hospitalized with TBI are younger than 20

INTRODUCTION• The term concussion has been used
interchangeably with mild traumatic brain injury (TBI)
• Defined as a trauma-induced alteration in mental status that may or may not involve the loss of consciousness (LOC).
• Cerebral concussion is considered a diffuse brain injury and is associated with widespread disruption of brain function.

INTRODUCTION
Wing, R & James, C; Emerg Med Clin N Am 31 (2013) 653–675

INTRODUCTION
• Not usually associated with visible lesions that can be detected by current imaging techniques.
• The primary injury mechanism for a concussion is thought to be from a rotational acceleration force .
• No head injury should be considered minor.

EPIDEMIOLOGY
• Falls
• Motor vehicle crashes
• Sports and recreational injuries
• Violence including child abuse and child on child violence

EPIDEMIOLOGY
• Severity
• Mild 80-85%
• Moderate to Severe 12-15%
• Fatal 4-5%

EPIDEMIOLOGY• Average cost of hospitalization for a child with
mild TBI $10,000 up to $3+ million for severe TBI leading to PVS.
• The annual cost of hospitalization for TBI estimated in the US at $100 billion.
• Immeasurable price to individual and family and to society as a whole.
• Head injury the single greatest cause of lost potential productivity in children.

EVALUATION• History
• Physical Examination
• Laboratory evaluation
• Imaging
• Cognitive evaluation/Neuropsychology
• PT/OT/SLP

EVALUATION• Primary Survey
• Airway
• Breathing
• Circulation
• Disability
• Exposure
• Neurologic Assessment
• Pupillary response
• Responsiveness
• Glasgow Coma Scale
• Modified Glasgow Coma Scale

EVALUATION
Wing, R & James, C; Emerg Med Clin N Am 31 (2013) 653–675

EVALUATION• Head CT imaging an important tool in the
management of TBI.
• Provides valuable information regarding the type, location, and severity of intracranial injuries, skull fractures, and cervical spine injuries.
• Newer improved technology allows faster and more detailed imaging to be obtained.
• Unfortunately, increased CT use leads to increased radiation exposure as well as increased costs

EVALUATION

Advances in Imaging: MRI DTI Tractography
RISK FACTORS FOR DELAYED
COMPLICATIONS
• Age of less than 2 years a moderate risk factor for ICI after head trauma.
• Lower threshold for imaging studies of younger children because historical and clinical factors may not be available or present for assessment
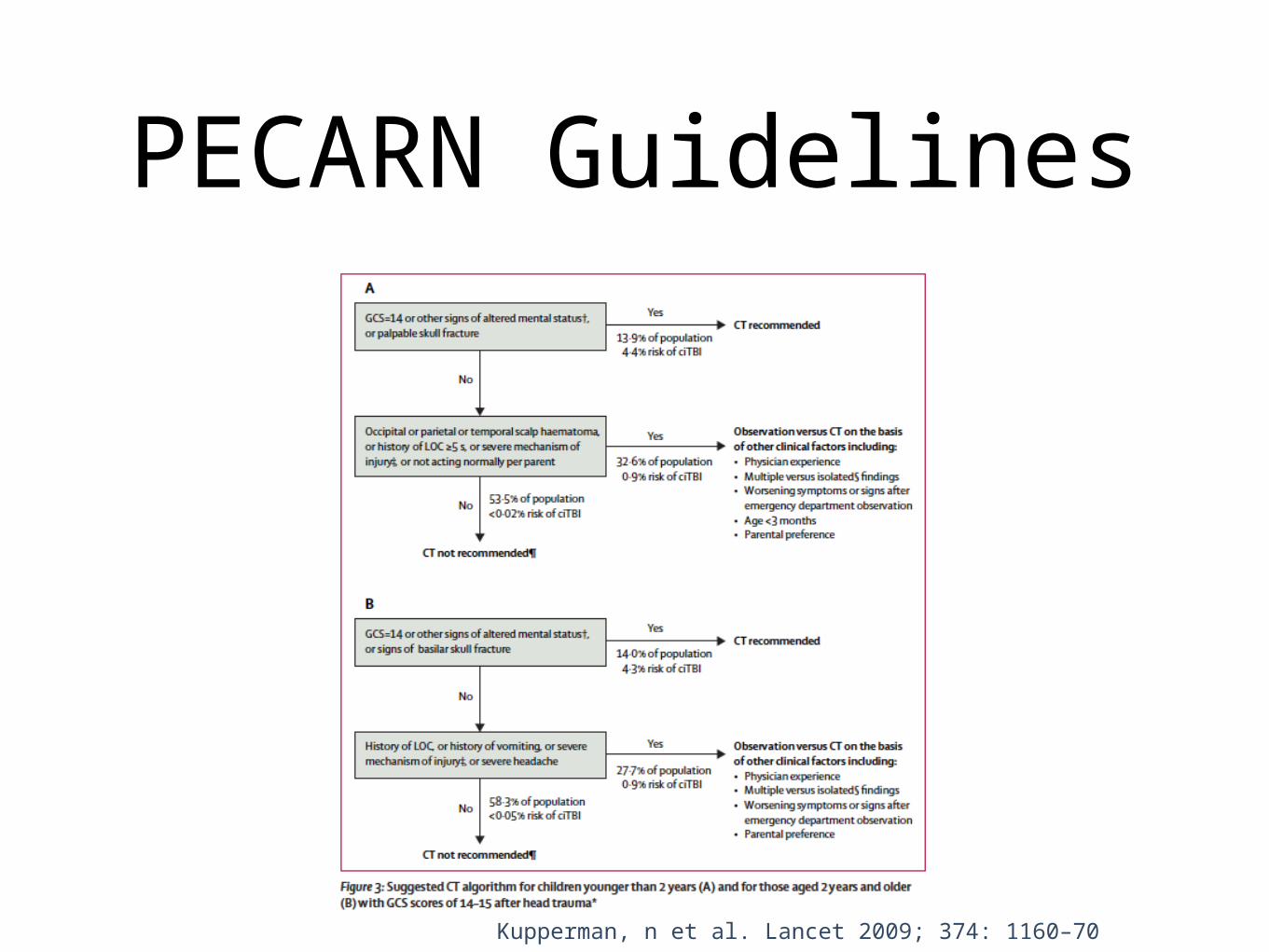
PECARN Guidelines
Kupperman, n et al. Lancet 2009; 374: 1160–70

PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
• Impact -head striking a surface or being struck by object
• Inertial (translational, rotational or both)
• Penetrating
• Anoxic

PATHOPHYSIOLOGY• Are potentially preventable and are caused by:
• Hypoxia/ischemia
• Energy failure
• Brain swelling/edema
• Excitotoxicity
• Necrosis/Apoptosis
• Inflammation

SPORTS CONCUSSIONS

SPORTS CONCUSSIONS
• High concussion risk organized sports such as wrestling and boxing described as early as 776 BC
• Sports related concussions recognized historically but remain a frequent and controversial topic
• Increased concern, awareness and prevention efforts including at the legislative level

SPORTS CONCUSSIONS
• Differences between sports concussions and concussions from other etiologies
• Sports concussions a particular problem in pediatrics
• Children at increased risk

SPORTS CONCUSSIONS• More than 300 000 sport-related concussions
occur annually in the United States
• More than 60 000 cases of concussions occur at the high school level, with football accounting for the majority of these.
• Approximately 4% of high school and collegiate football players sustain concussions during each season.
• 1 250 000 student-athletes participating at the high school level

SPORTS CONCUSSIONS
• Recent concerns over the health of athletes who sustain concussions.
• Practice guidelines and parameters for evaluating and managing the head-injured athlete have been developed.
• The various guidelines released have raised controversy since not enough data on concussion grades and return-to-play criteria

SPORTS CONCUSSIONS
• Baseline and post concussion neuropsychological testing
• ImPACT testing (Immediate Post-Concussion Assessment and Cognitive Testing)
• Return to play guidelines
• Return to school guidelines

SPORTS CONCUSSIONS
• Heads Up Campaign-CDC
• Information for coaches, parents and student athletes regarding concussions
• Guidelines for recognition and treatment

SPORTS CONCUSSIONS

SPORTS CONCUSSIONS
Thiessen, ML & Woolridge, DP; Pediatr Clin N Am 53 (2006) 1 – 26

SPORTS CONCUSSIONS
Thiessen, ML & Woolridge, DP; Pediatr Clin N Am 53 (2006) 1 – 26

OUTCOMES OF MTBI• Related to:
• Severity of injury
• Severity of intracranial hypertension
• Secondary brain injuries
• 20% of mild brain injury have some deficit
• 90-100% of moderate to severe will have deficit

OUTCOMES OF MTBI• Neurologic sequelae
• motor deficits
• sensory deficits
• hearing and vision should be formally tested
• Communication difficulties
• Cognitive deficits
• Behavioral problems

OUTCOMES OF MTBI• The short- and long-term complications of
mild TBI in children are poorly understood.
• Postconcussive syndrome refers to the constellation of acute symptoms after a mild TBI.
• These symptoms can be somatic (headache, dizziness, blurriness), emotional (irritability, anxiety), and cognitive (concentration and memory)

POST-CONCUSSION SYNDROME

POST-CONCUSSION SYNDROME• Studies have assessed physical, behavioral, and
cognitive outcomes across the severity continuum of head injuries.
• Speech and feeding difficulties associated with an increasing severity of head injury, but not walking.
• Headaches are among the most common postconcussive symptoms reported
• Also, temper outbursts, dizziness, mood swings, anxiety, and aggressive behavior have been reported.

POST-CONCUSSION SYNDROME
• Children with mild TBI do well in their recovery, but studies have found that not all mildly injured children recover completely.
• In one study 50% of the study group made a good recovery, but only 18.4% made a full recovery without discernible sequelae.
• Unclear what the threshold of injury severity below which the risk of late morbidity could be discounted.

CTE
• Concerns about effects of repetitive head trauma
• Recent professional athlete cases
• NFL money for research etc.

Rehabilitation• Treatment directed at maximizing functional
independence by reducing impairment, disability and handicap.
• Early intervention.
• Interdisciplinary team effort/organization.
• Short-term rehabilitation- consider intra-facility resources
• Long-term rehabilitation-specialized facility(note age-restrictions)

RETURN TO SCHOOL• When children with head injury return to school,
they may be expected to assimilate immediately with the class.
• The child’s teacher may not understand the head injury or even know the child suffered a MHI, which could affect how the child is treated, observed, or graded.
• In one study, teachers knew of the child’s head injury in only 39.8% of the children, and there was a significant linear trend across injury severity groups.

RETURN TO SCHOOL• Special educational needs were provided for
only 65% of the children identified with such needs.
• At follow-up, 18.7% of the children were currently having difficulties with schoolwork
• Interestingly, 18% of the children had been disciplined by the school for problem behavior after sustaining their head injury

Return to Play
Wing, R & James, C; Emerg Med Clin N Am 31 (2013) 653–675

FOLLOW-UP• Pediatric Traumatic Brain Injury Clinic
• Mild/Moderate TBI Clinic
• Primary care Physicians
• Return to school
• Return to sports
• PT/OT/Neuropsychology/SLP
• Brain Injury Association of Minnesota

PREVENTION• All head trauma is potentially preventable.
• Ensure a safe environment for kids.
• Educate regarding motor safety.
• Emphasize helmet use, age-appropriate MV restraints to prevent or attenuate injury.
• Educate about guns (limit access).
• Educate about prevention of inflicted head injuries.

PREVENTION
• Heads Up Campaign by CDC
• National and regional injury prevention programs
• Role of pediatricians
• State and federal legislation

RESEARCH
• Need for ongoing research into brain injury treatment
• Need for increased federal and foundation funding for traumatic brain injury.

Conclusions• Traumatic brain injuries are a common cause of
morbidity and mortality in children
• Damage to the brain cannot be reversed
• Sports related concussions are a continued problem for the pediatric population
• Advances in management of MTBI offer hope for improved outcomes
• Research into the pathophysiology of MTBI crucial
• PREVENTION IS KEY

QUESTIONS?