Embed Size (px)
Citation preview


OverviewIntroduction to CPCMission and VisionCore Model ComponentsCurrent Health Initiatives
Respiratory InitiativeImmunization InitiativeHealthy Living Initiative

Colorado Pediatric Collaborative
• Colorado Pediatric Collaborative (CPC), Inc. is a nonprofit partnership between:
– Colorado Pediatric Partners (CPP), an Independent Physician Association of pediatric practices located along the front range of Colorado;
– Physician Health Partners (PHP), a large healthcare management services organization; and
– Children’s Hospital Colorado, the leading provider of inpatient, sub-specialty, and emergent care to children in the Rocky Mountain west

CPC Board Leadership• Joan Bothner, MD - Chairman• Andrew Bauer, MD – Vice Chairman• Jeff Harrington – Secretary/Treasurer• Monica Federico, MD• Robert King, MD• Michael Narkewicz, MD• Stephanie Stevens, MD• Holbrook Stapp, MD• Lisa Wetherbee

CPP PCP Practices
• Advanced Pediatric Associates• Arvada Pediatrics• Aspen Park Pediatrics• Centennial Pediatrics• Child Health Clinic• Children’s Medical Center• Crown Point Pediatrics• Denver Pediatrics• Evergreen Pediatrics• Greenwood Pediatrics• Guardian Angels Health Center• Kids First Pediatrics
• Morarka Pediatric Office• Mountainland Pediatrics, P.C.• Office of Drs. Fleischaker & Khayut• Partners in Pediatrics• Peak Pediatrics, PLLC• Pediatrics 5280• Pediatrics at the Meadows, P.C.• Pediatrics West• Red Rocks Pediatrics, P.C.• Rocky Mountain Pediatrics, P.C.• Stapleton Pediatrics

Colorado Pediatric Collaborative• As of September 2014, the CPC network consists of:
– 23 practices– 120 pediatricians– 200,000 pediatric patients in the Denver Metro area
• CPC is the first organization of its kind in the Denver area combining the expertise of a hospital, primary care physicians, specialists and a medical management company to improve the overall quality of care for the children and families they serve

CPC Vision and Mission• Vision
– Improve the health of children and families through innovative partnerships and clinical models that create an integrated system of care
• Mission– Develop collaborative partnerships across care settings to allow for
effective, efficient, high-quality healthcare– Incorporate a patient-centered philosophy that is focused on value and
efficiency – Demonstrate value and quality outcomes through the implementation of
robust, evidence-based medicine and rigorous analysis of program effectiveness to determine impact and adjust as appropriate
– Serve as a leader in the development and testing of innovative care and reimbursement models that reward quality and value
– Align program and payment strategies with the Triple Aim and demonstrate accountability with respect to quality, cost, and patient experience

CPC Accomplishments• Procured $1.5M Start-up Grant from CO Health Foundation—Expires
2015
• Brought Together Three Independent Parties to Address the Regional Opportunity to Improve Care for Colorado’s Children!
• Developed and implemented innovative health initiatives in the primary care setting
• Procured Two Major Provider Contracts from Anthem and Aetna
Affecting 23 Practices!

Triple Aim

CPC Model Components• Evidence-Based Guidelines & Clinical Education
– Education and training from physician experts• Clinical Quality Improvement
– Assessment– Improvement Team– Training– Implementation– Evaluation and Improvement
• Health Information Technology & Data Analytics– Registries– Electronic Health Records and Health Information
Exchange– Data analysis and reporting

Health Initiatives
Respiratory ImmunizationsHealthy LivingMental HealthSpecial Needs

Respiratory Initiative• Asthma initiative was implemented in 2007 across all
practices– Adherence to evidence based guidelines
– Process measures: Severity assessment, controller meds, influenza
– Outcome measures: ED and urgent care, hospitalizations, missed work and school
– Registry-based tool designed to improve guideline compliance

Background and Research Objective
Study Design and Methods
Principal Findings Conclusions
Authors: Monica J Federico, MD 1, Sara Deakyne, BS, MPH 1, R. Holbrook Stapp, MD 3, Britta Fuglevand, MS 2, and Lalit Bajaj, MD, MPH 1.1Pediatrics, University of Colorado, Aurora, CO, United States; 2Physician Health Partners, Denver, CO, United States and 3Colorado Pediatric Collaborative, Denver, CO, United States.
Improving Asthma Care in a Community Pediatric Independent Practice Association through Academic/Community Collaboration
Relevance to policy, delivery or clinical
practice
• Many children have poorly controlled asthma despite national guidelines for the diagnosis and management of asthma.
• Significant barriers exist in the implementation of evidence-based guidelines into community practice. Strategies addressing these barriers require multi-stakeholder investment and are difficult to coordinate
• Our objective was to assess the long term impact of a community and academic partnership to implement asthma quality improvement in an independent practice association (IPA) of community pediatricians.
In 2006, pulmonologists from the Breathing Institute of Children’s Hospital Colorado worked with Colorado Pediatric Partners, an Independent Physician Association, to create an asthma care quality improvement program. This was an observational study of that program.
Population: The IPA consists of 23 practices/173 providers and serves over 160, 000 children. Inclusion criteria: children over 5 years of age with a provider diagnosis of asthma. Exclusion criteria: Children with lung disease of prematurity, cystic fibrosis, cardiac anomalies, neuromuscular disease.
Intervention:1.Practice redesign and quality improvement curriculum provided by practice coaches assigned to each practice.
2.Case-based asthma education at each practice by a pulmonologist
3.Asthma care tools including intake forms, action plans, electronic health record integration
4.Asthma registry on a separate server with web-based data entry
5.Regular data reporting on demand and scheduled and provided by one of the 3 full time practice coaches at least quarterly
6.Negotiations with payers to support the asthma care program.
7.American Board of Pediatrics approval of the program for MOC.
Analysis: Children with at least two visits in the registry were included in the analysis. Proportions and means were calculated for demographics and process outcomes. Rates were calculated for hospital admissions, ED/UC visits, missed school days and missed work days. Associations with other factors, including age, payer, whether the patient saw a specialist, use of inhaled steroids, asthma teaching and smoke exposure were analyzed using repeated measures Poisson regression.
• Implementing a standardized approach to asthma care leads to sustained improvement in process and health outcomes across a large population of children with asthma
• Medicaid patients’ care and outcomes improved but those patients were still more likely to have ED/UC visits, missed days of work and missed days of school than privately insured
• Continuous process improvement with the appropriate staffing model can lead to sustained improvement in the health outcomes for children with asthma
• A community/academic partnership that combines asthma education, process redesign, and a registry based tracking system, can improve the care delivered to pediatric patients and can improve health outcomes for those patients. The program design also allows for the continuous assessment of gaps in care, and areas that require special attention and more focused intervention.
• Health care policy should encourage government and private payers to help fund the infrastructure that is necessary for providers, practices, and systems to improve health outcomes
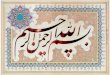
Total patients 1908
Total visits 9,923
2 or more provider surveys 1789
2 or more patient surveys 1615
Mean visits per patient 5
Total patient days 406,149
Mean Age 12.5 years (range: 5-25)
% Male 59%
% Private insurance 72%
Target
2008/2009
(n=1,890)
2011/2012
(n=1,882)
Persistent asthma ̶ 61% 61%
Severity assessment completed
90% 100% 100%
Asthma action plan 60% 69% 90%
Flu shot 90% 91% 95%
Persistent and on controller medication
90% 78% 85%
Demographics Process Outcomes
• Grant support: Colorado Health Foundation• Acknowledgments: Physician Health Partners,
Colorado Pediatric Collaborative, Dan Hyman, MD, Joan Bothner, MD
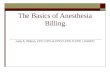
Hospital Admits and ED/UC Visits
Health OutcomeChange in RiskFrom 2008/09 to
2011/12
95% Confidence
Intervalp-value
Hospital Admission* -69% -36%,-85% p=0.0014
ED/UC** -62% -40%,-76% p<0.0001Missed School ŧ -47% -27%,-61% p<0.0001Missed work days ŧŧ -39% -24%,-39% p<0.0001
Adjusted Outcomes Analysis (All patient reported)
* Adjusted for age, asthma education in the office, smoke exposure, specialist involvement, inhaled steroid use
** Adjusted for age, specialist, inhaled steroid use, and payerŧ Adjusted for age, specialist, inhaled steroid use, smoke
exposure and payerŧŧ Adjusted for age, specialist, steroid use and payer
Missed School and Missed Work
Note: Among participating practices, 98.6% of patients in the registry have a
visit in 2011/2012.
Funding and Acknowledgments

Immunizations Initiative• Immunization initiative was implemented in 2009 across
all practices– Adherence to evidence based guidelines– Process measures: HEDIS Childhood Immunization
Measure for 2 yr. olds and 13 yr. olds– CPC practices use the Colorado Immunization
Information System (CIIS) to electronically track immunization status and history for patients
– CPC estimates that 95% of its entire population is affected by this initiative

Healthy Living Initiative• Target Population Patients 2-18 years of age
– Subset population» Patients with BMI 85-94% with risk factors» Patients with BMI ≥ 95%ile
Phase 1 Measures:BMI Percentile,Blood Pressure Screening,Counseling for Nutrition,Counseling for Physical Activity

Healthy Living InitiativeLong Term Goals• Improve adherence to nationally
accepted guidelines and performance measures
• Reduce costs to the health care system associated with preventable co-morbidities and exacerbations due to obesity
• Improve caregiver confidence in managing a healthy lifestyle action plan
Program Goals• Identify children who are at risk of
becoming obese or are obese• Provide counseling on nutrition and
physical activity to children who are not currently at risk as to maintain their health status
• Help children who are obese build healthy lifestyles and improve health outcomes through community wide patient centered intervention
• Provide physicians with the tools to effectively manage obese patients in the primary care setting

Mental Health & Special Needs • Collaborative approach with community organizations to
support primary care providers and patients
– Current areas of focus:• Colorado Psychiatric Access and Consultation for Kids (C-
PACK)• Transition Clinic through the Special Care Clinic at CHCO
• CPC will continue to explore collaborative opportunities to improve quality of care for patients

CPC Strategic Opportunities• Expand the Number of CPC Practices & Pediatricians • Gain Greater Acceptance of the Electronic Medical Record and the Value-
Added Data Submission for Analysis within the Pediatric Community• Introduce a Comprehensive Asthma Registry• Respond to the Need for Enhanced Practice Tools• Acquire and Implement Better Software Tools for Managing & Reporting on
Disparate Patient Data• Identify Emerging Trends and Improvement Opportunities in Children’s
Medicine in CO.• Reduce the Cost of Care!• Expand Our Philanthropic Support Base!• Identify Synergistic Community Collaborators

CPC-The Next Phase• Address the Immediate Need to Secure $1.5-2M in New Funding
Support for 2015-2016• Pursue Grant Scaling on the CHF Commitment• Establish Sophisticated IT Platform and Address CORHIO
Opportunity• Expand Coaching and Direct Support-Outreach to Practices• Continue Building Community Based Support Hybrid Foundation and
Government Grants• Ensure Alignment with Pediatric Needs and Concerns• Continue to Disseminate “Best-Practice Approaches to Prevalent and
Costly Pediatric Conditions

Why Invest in CPC?• CPC is Addressing a Serious, Societal
Healthcare Need in a Responsible Manner• CPC Members Have Voluntarily Committed to
Ensuring CO Children Have the Best Care• CPC Brings Together Three Recognized
Healthcare Entities Working Collaboratively Toward Efficiency and Efficacy in Medicine
• CPC Members Have Invested in Improving Care and Seek Community Funding Partners!