Embed Size (px)
Citation preview
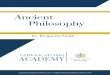
BLOCK TIME MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY
Aug 6 – Aug 10 am
Orientation Lecture‐1 Lecture‐3 Lecture‐5 Clinical Correlation‐1
am Lecture‐2 Lecture‐4 Lecture‐6 Clinical Correlation‐2 Week 1 Overview
pm INTRODUCTION pm
PCM2/Pharm & Ther PCM2‐exam (1pm) PCM2‐MSR Workshop
Aug 13 – Aug 17 am Quiz & its Review Lecture‐8 Lecture‐10 Clinical Correlation‐3 Small Group Exercise‐1
(Clinical Localization) am Lecture‐7 Lecture‐9 Lecture‐11 Clinical Correlation‐4 Week 2
Spinal cord/Brainstem pm
Mass of Holy Spirit
pm Pharm & Therapeutics
Aug 20 – Aug 24 am Quiz & its Review Lecture‐13 Lecture‐15 Clinical Correlation‐5 Quiz & its Review am Lecture‐12 Lecture‐14 Lecture‐16 Clinical Correlation‐6
Week 3 CNs/Brainstem
pm Small Group Exercise‐2 (Clinical Localization)
pm
Pharm & Therapeutics
Aug 27 – Aug 31 am
MID‐TERM EXAM (WEEKS 1‐3)
Week in preview Lecture‐18 Clinical Correlation‐7 Clinical Correlation‐9 am Lecture‐17 Lecture‐19 Clinical Correlation‐8 Clinical Correlation‐10
Week 4 CNs/Thalamus
pm pm
Pharm & Therapeutics
Sep 3 – Sep 7 am
Labor Day
Quiz & its Review Lecture‐21 Clinical Correlation‐11 Small Group Exercise‐3 (Clinical Localization) am Lecture‐20 Lecture‐22 Clinical Correlation‐12
Week 5 Motor systems
pm pm
Pharm & Therapeutics Neuro OSCE (1‐5) Neuro OSCE (1‐5)
Sep 10 – Sep 14 am Quiz & its Review Lecture‐24 Lecture‐26 Clinical Correlation‐13 Clinical Correlation‐15 am Lecture‐23 Lecture‐25 Lecture‐27 Clinical Correlation‐14 Clinical Correlation‐16
Week 6 Cerebral cortex/Motor
pm pm
Pharm & Therapeutics
Sep 17 – Sep 21 am
Rosh Hashanah
Quiz & its Review Lecture‐30 FINAL EXAM
(1/3rd Weeks 1‐3) (2/3rd Weeks 4‐7)
am Lecture‐28 Lecture‐31 Week 7
Neuropathology pm Lecture‐29 pm
Neuropath/P&T
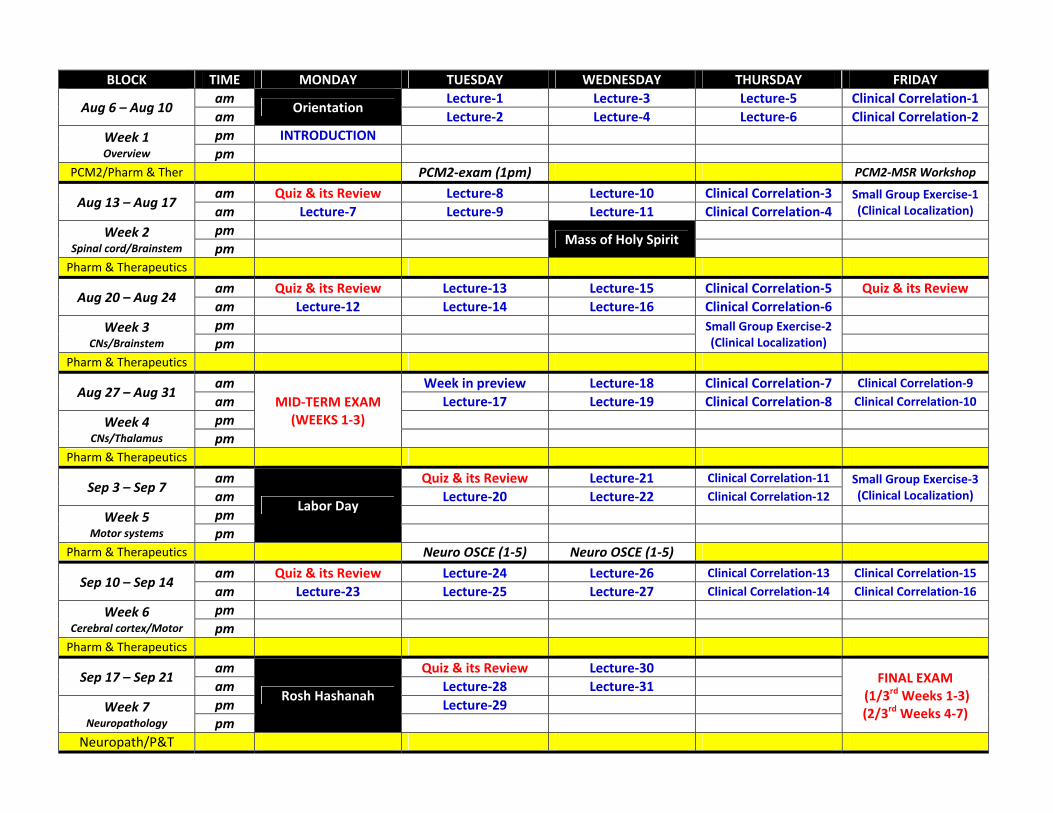
Foundational Neuroscience Course Calendar 2012‐2013
Date Time Session Topic Faculty Aug 6 2:00p Introduction Course Review (grading, expectations, etc) DauzvardisAug 7 9:30a Lecture‐1 Introduction & General Organization (Chap 1, 3) DauzvardisAug 7 10:30a Lecture‐2 Development of the Nervous System (Chap 2) DoncarlosAug 8 9:30a Lecture‐3 Meningeal coverings, Ventricles & CSF (Chap 4, 5) GruenerAug 8 10:30a Lecture‐4 Blood supply of the brain (Chap 6) GruenerAug 9 9:30a Lecture‐5 Sensory system and receptors (Chap 9) DauzvardisAug 9 10:30a Lecture‐6 Spinal cord (Chap 10) DauzvardisAug 10 9:30a Clinical Correlation‐1 Spinal cord disorders MerchutAug 10 10:30a Clinical Correlation‐2 Neuromuscular junction (NMJ) disorders (patient) MerchutAug 13 8:30a Quiz & its Review Quiz on Week 1 Material and Preview of the Week Aug 13 9:30a Lecture‐7 Organization of the brainstem (Chap 11) DauzvardisAug 14 9:30a Lecture‐8 Cranial nerves and nuclei (Chap 12) DauzvardisAug 14 10:30a Lecture‐9 Brainstem summary (Chap 15) DauzvardisAug 15 8:30a Lecture‐10 Chemical senses of taste & smell (Chap 13) DauzvardisAug 15 9:30a Lecture‐11 Hearing and Balance (Chapter 14) GruenerAug 16 9:30a Clinical Correlation‐3 Cranial nerves, Brain stem reflexes and disorders MerchutAug 16 10:30a Clinical Correlation‐4 Multiple sclerosis (patient) Merchut
Aug 17 11:00a ‐ 12:30p Small Group Exercise‐1 Clinical Localization Set #1 FACULTY
Aug 20 8:30a Quiz & its Review Quiz on Week 2 Material and Preview of the Week Aug 20 9:30a Lecture‐12 Hearing and Balance (Chapter 14) – “Once again” GruenerAug 21 9:30a Lecture‐13 Cranial nerves and nuclei (Chap 12) ‐ “Once again” DauzvardisAug 21 10:30a Lecture‐14 Brainstem summary (Chap 15) ‐ “Once again” DauzvardisAug 22 9:30a Lecture‐15 Visual system I (Chap 17) StubbsAug 22 10:30a Lecture‐16 Visual system II (Chap 17) StubbsAug 23 9:30a Clinical Correlation‐5 Coma/Brain death/End‐of‐life MerchutAug 23 10:30a Clinical Correlation‐6 Neuroimaging essentials Merchut
Aug 23 2:00p ‐3:30p Small Group Exercise‐2 Clinical Localization Set #2 FACULTY
Aug 24 10:00a Quiz & its Review Quiz on Week 3 Material
Aug 27 11:00a‐2:00p Mid‐Term Exam Weeks 1‐3 to be covered
Aug 28 9:30a This week in Preview Cranial nerves and thalamus DauzvardisAug 28 10:30a Lecture‐17 Control of eye movements (Chap 21) StubbsAug 29 9:30a Lecture‐18 Cranial nerves and nuclei (Chap 12) ‐ “Once again” DauzvardisAug 29 10:30a Lecture‐19 Thalamus and internal capsule (Chap 16) DauzvardisAug 30 9:30a Clinical Correlation‐7 Visual, Auditory and Vestibular Systems MerchutAug 30 10:30a Clinical Correlation‐8 Headache MerchutAug 31 9:30a Clinical Correlation‐9 Cerebrovascular disease (clinical) MerchutAug 31 10:30a Clinical Correlation‐10 Neuropathy, Myopathy and MND (patient) Merchut
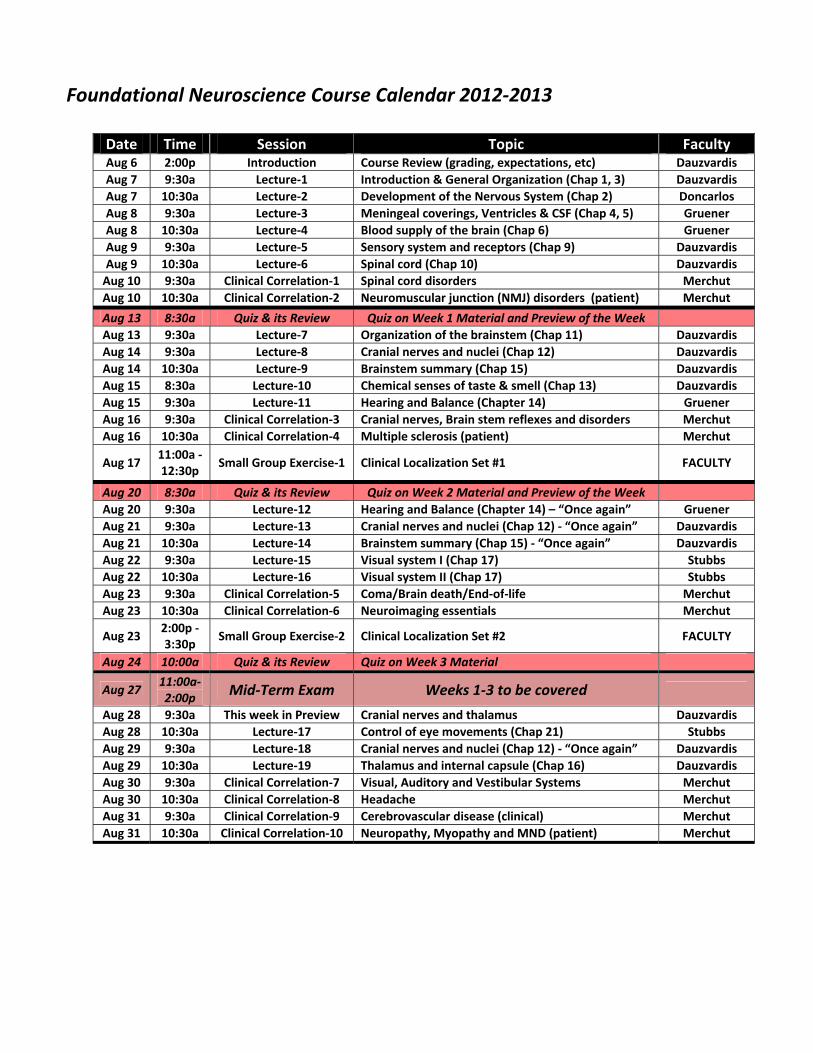
Foundational Neuroscience Course Calendar (cont) 2012‐2013
Date Time Session Topic Faculty Sep 3 Labor DaySep 4 9:30a Quiz & its Review Quiz on Week 4 Material and Preview of the Week Sep 4 10:30a Lecture‐20 Overview of motor systems (Chap 18) GruenerSep 5 9:30a Lecture‐21 Basal ganglia (Chap 19) GruenerSep 5 10:30a Lecture‐22 Cerebellum (Chap 20) GruenerSep 6 9:30a Clinical Correlation‐11 Gait, Cerebellar function, and Movement disorders MerchutSep 6 10:30a Clinical Correlation‐12 Disorders of Basal Ganglia (patient) Merchut
Sep 7 10:30a ‐ 12:00p Small Group Exercise‐3 Clinical Localization Set #3 FACULTY
Sep 10 8:30a Quiz & its Review Quiz on Week 5 Material and Preview of the Week Sep 10 9:30a Lecture‐23 Cerebral cortex (Chap 22) GruenerSep 11 9:30a Lecture‐24 Cerebral cortex (Chap 22) GruenerSep 11 10:30a Lecture‐25 Hypothalamus and limbic system (Chap 23) Don CarlosSep 12 9:30a Lecture‐26 Spinal cord (Chap 10) ‐ “Once again” DauzvardisSep 12 10:30a Lecture‐27 BG & Cerebellum (Chap 19, 20) ‐ “Once again” GruenerSep 13 9:30a Clinical Correlation‐13 Language MerchutSep 13 10:30a Clinical Correlation‐14 Behavior, Cortical function , and Dementia MerchutSep 14 9:30a Clinical Correlation‐15 Intoxications and infections of the Nervous System MerchutSep 14 10:30a Clinical Correlation‐16 Epilepsy AsconapeSep 17 Rosh HashanahSep 18 8:30a Quiz & its Review Quiz on the Week 6 Material
Sep 18 9:30a Lecture‐28 Neuropathology – Trauma, Infections & inflammation Lee
Sep 18 10:30a Lecture‐29 Neuropathology – Neurodegenerative LeeSep 19 9:30a Lecture‐30 Neuropathology – Brain neoplasms LeeSep 19 10:30a Lecture‐31 Neuropathology –Cerebrovascular Disease (CVD) Lee
Sep 21 8:00a ‐ 11:00a
Neuroscience Final Exam
Neuroscience covers Weeks 1‐3 (1/3rd of the exam) Weeks 4‐7 (2/3rds of the exam)
Sep 24 Oct 1 Oct 6 Mid‐Semester Break
Student Grade Assignment: There are 340 total points in the course:
Quizzes: 120 (6 quizzes, 20 points each) Midterm Exam: 100 Final Exam: 120
There will be NO rounding of grades! (e.g. 305 points (89.7%) is a High Pass)
Grade Percentage Points Earned
Honors 90.0% ‐ 100% 306‐340
High Pass 80.0% ‐ 89.9% 272‐305
Pass 70.0% ‐ 79.9% 238‐271
Fail < 70.0% < 238
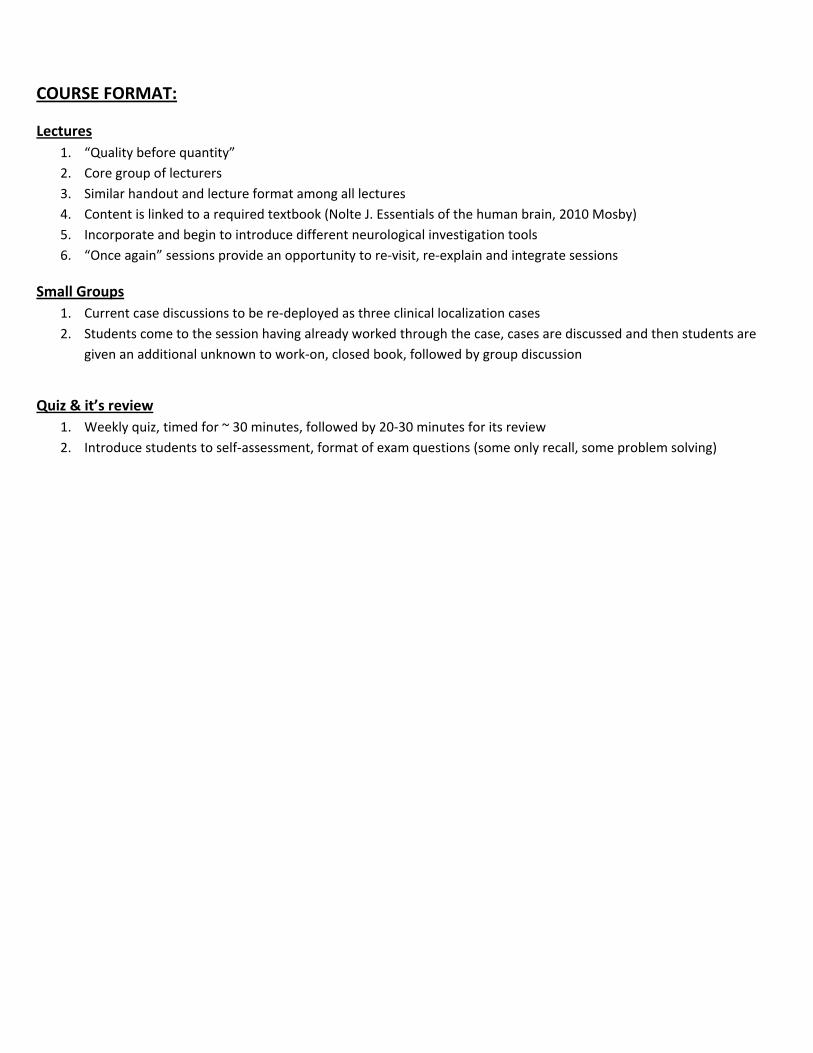
COURSE FORMAT:
Lectures 1. “Quality before quantity” 2. Core group of lecturers 3. Similar handout and lecture format among all lectures 4. Content is linked to a required textbook (Nolte J. Essentials of the human brain, 2010 Mosby) 5. Incorporate and begin to introduce different neurological investigation tools 6. “Once again” sessions provide an opportunity to re‐visit, re‐explain and integrate sessions
Small Groups 1. Current case discussions to be re‐deployed as three clinical localization cases 2. Students come to the session having already worked through the case, cases are discussed and then students are
given an additional unknown to work‐on, closed book, followed by group discussion
Quiz & it’s review 1. Weekly quiz, timed for ~ 30 minutes, followed by 20‐30 minutes for its review 2. Introduce students to self‐assessment, format of exam questions (some only recall, some problem solving)
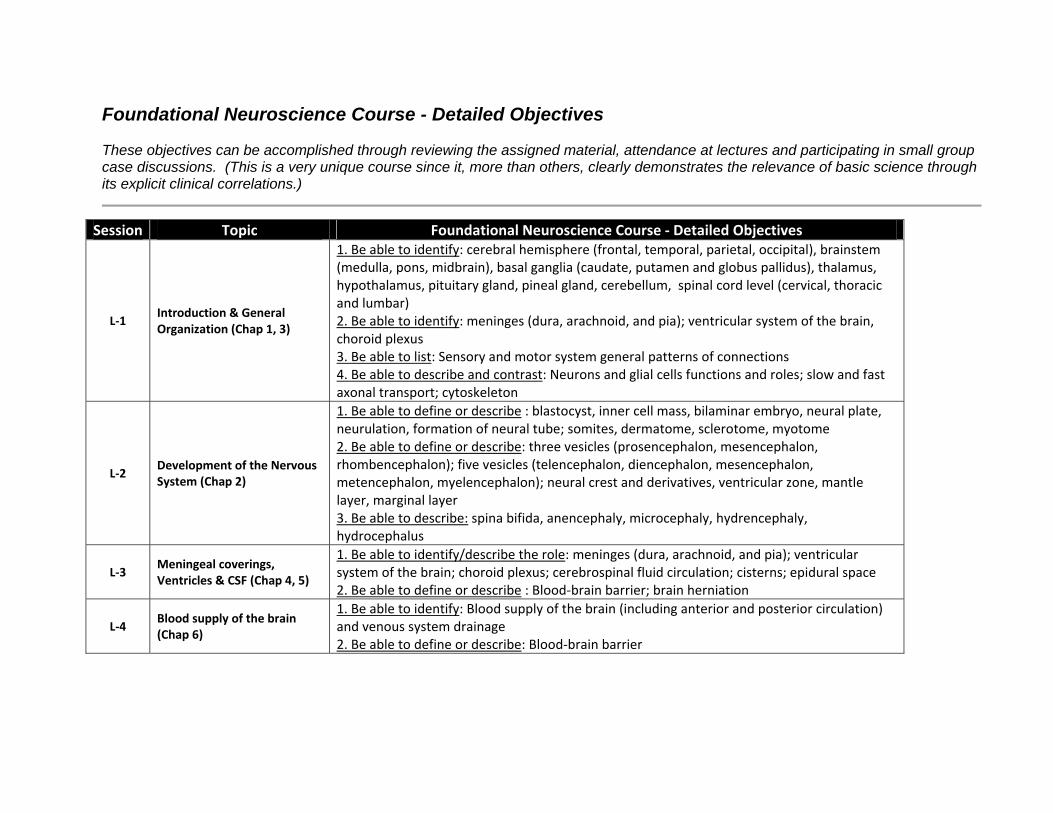
Foundational Neuroscience Course - Detailed Objectives These objectives can be accomplished through reviewing the assigned material, attendance at lectures and participating in small group case discussions. (This is a very unique course since it, more than others, clearly demonstrates the relevance of basic science through its explicit clinical correlations.)
Session Topic Foundational Neuroscience Course ‐ Detailed Objectives
L‐1 Introduction & General Organization (Chap 1, 3)
1. Be able to identify: cerebral hemisphere (frontal, temporal, parietal, occipital), brainstem (medulla, pons, midbrain), basal ganglia (caudate, putamen and globus pallidus), thalamus, hypothalamus, pituitary gland, pineal gland, cerebellum, spinal cord level (cervical, thoracic and lumbar) 2. Be able to identify: meninges (dura, arachnoid, and pia); ventricular system of the brain, choroid plexus 3. Be able to list: Sensory and motor system general patterns of connections 4. Be able to describe and contrast: Neurons and glial cells functions and roles; slow and fast axonal transport; cytoskeleton
L‐2 Development of the Nervous System (Chap 2)
1. Be able to define or describe : blastocyst, inner cell mass, bilaminar embryo, neural plate, neurulation, formation of neural tube; somites, dermatome, sclerotome, myotome 2. Be able to define or describe: three vesicles (prosencephalon, mesencephalon, rhombencephalon); five vesicles (telencephalon, diencephalon, mesencephalon, metencephalon, myelencephalon); neural crest and derivatives, ventricular zone, mantle layer, marginal layer 3. Be able to describe: spina bifida, anencephaly, microcephaly, hydrencephaly, hydrocephalus
L‐3 Meningeal coverings, Ventricles & CSF (Chap 4, 5)
1. Be able to identify/describe the role: meninges (dura, arachnoid, and pia); ventricular system of the brain; choroid plexus; cerebrospinal fluid circulation; cisterns; epidural space 2. Be able to define or describe : Blood‐brain barrier; brain herniation
L‐4 Blood supply of the brain (Chap 6)
1. Be able to identify: Blood supply of the brain (including anterior and posterior circulation) and venous system drainage 2. Be able to define or describe: Blood‐brain barrier
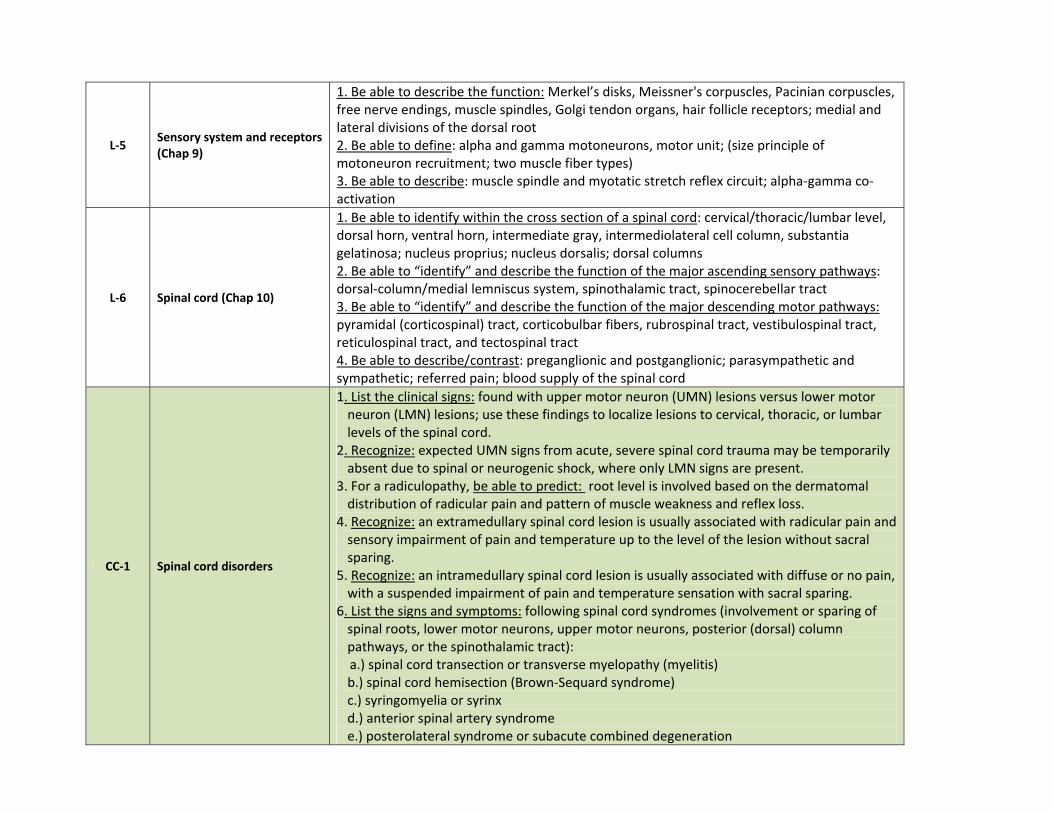
L‐5 Sensory system and receptors (Chap 9)
1. Be able to describe the function: Merkel’s disks, Meissner's corpuscles, Pacinian corpuscles, free nerve endings, muscle spindles, Golgi tendon organs, hair follicle receptors; medial and lateral divisions of the dorsal root 2. Be able to define: alpha and gamma motoneurons, motor unit; (size principle of motoneuron recruitment; two muscle fiber types) 3. Be able to describe: muscle spindle and myotatic stretch reflex circuit; alpha‐gamma co‐activation
L‐6 Spinal cord (Chap 10)
1. Be able to identify within the cross section of a spinal cord: cervical/thoracic/lumbar level, dorsal horn, ventral horn, intermediate gray, intermediolateral cell column, substantia gelatinosa; nucleus proprius; nucleus dorsalis; dorsal columns 2. Be able to “identify” and describe the function of the major ascending sensory pathways: dorsal‐column/medial lemniscus system, spinothalamic tract, spinocerebellar tract 3. Be able to “identify” and describe the function of the major descending motor pathways: pyramidal (corticospinal) tract, corticobulbar fibers, rubrospinal tract, vestibulospinal tract, reticulospinal tract, and tectospinal tract 4. Be able to describe/contrast: preganglionic and postganglionic; parasympathetic and sympathetic; referred pain; blood supply of the spinal cord
CC‐1 Spinal cord disorders
1. List the clinical signs: found with upper motor neuron (UMN) lesions versus lower motor neuron (LMN) lesions; use these findings to localize lesions to cervical, thoracic, or lumbar levels of the spinal cord.
2. Recognize: expected UMN signs from acute, severe spinal cord trauma may be temporarily absent due to spinal or neurogenic shock, where only LMN signs are present.
3. For a radiculopathy, be able to predict: root level is involved based on the dermatomal distribution of radicular pain and pattern of muscle weakness and reflex loss.
4. Recognize: an extramedullary spinal cord lesion is usually associated with radicular pain and sensory impairment of pain and temperature up to the level of the lesion without sacral sparing.
5. Recognize: an intramedullary spinal cord lesion is usually associated with diffuse or no pain, with a suspended impairment of pain and temperature sensation with sacral sparing.
6. List the signs and symptoms: following spinal cord syndromes (involvement or sparing of spinal roots, lower motor neurons, upper motor neurons, posterior (dorsal) column pathways, or the spinothalamic tract):
a.) spinal cord transection or transverse myelopathy (myelitis) b.) spinal cord hemisection (Brown‐Sequard syndrome) c.) syringomyelia or syrinx d.) anterior spinal artery syndrome e.) posterolateral syndrome or subacute combined degeneration
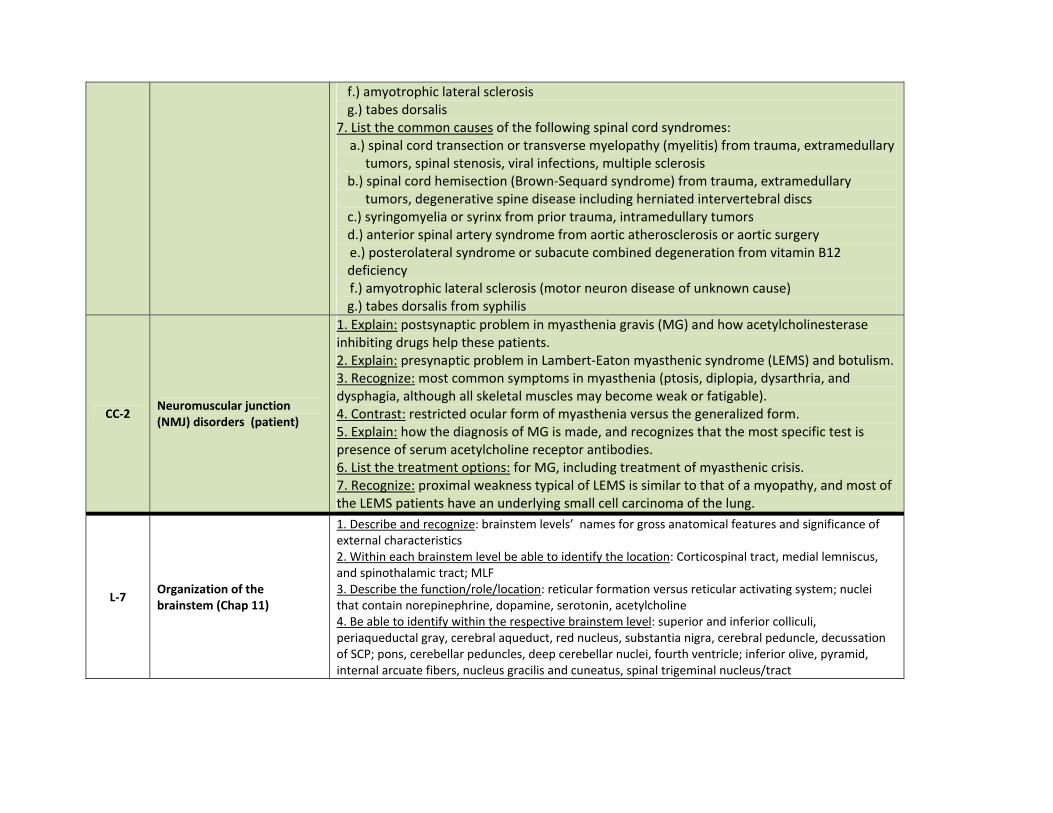
f.) amyotrophic lateral sclerosis g.) tabes dorsalis 7. List the common causes of the following spinal cord syndromes: a.) spinal cord transection or transverse myelopathy (myelitis) from trauma, extramedullary
tumors, spinal stenosis, viral infections, multiple sclerosis b.) spinal cord hemisection (Brown‐Sequard syndrome) from trauma, extramedullary
tumors, degenerative spine disease including herniated intervertebral discs c.) syringomyelia or syrinx from prior trauma, intramedullary tumors d.) anterior spinal artery syndrome from aortic atherosclerosis or aortic surgery
e.) posterolateral syndrome or subacute combined degeneration from vitamin B12 deficiency
f.) amyotrophic lateral sclerosis (motor neuron disease of unknown cause) g.) tabes dorsalis from syphilis
CC‐2 Neuromuscular junction (NMJ) disorders (patient)
1. Explain: postsynaptic problem in myasthenia gravis (MG) and how acetylcholinesterase inhibiting drugs help these patients. 2. Explain: presynaptic problem in Lambert‐Eaton myasthenic syndrome (LEMS) and botulism. 3. Recognize: most common symptoms in myasthenia (ptosis, diplopia, dysarthria, and dysphagia, although all skeletal muscles may become weak or fatigable). 4. Contrast: restricted ocular form of myasthenia versus the generalized form. 5. Explain: how the diagnosis of MG is made, and recognizes that the most specific test is presence of serum acetylcholine receptor antibodies. 6. List the treatment options: for MG, including treatment of myasthenic crisis. 7. Recognize: proximal weakness typical of LEMS is similar to that of a myopathy, and most of the LEMS patients have an underlying small cell carcinoma of the lung.
L‐7 Organization of the brainstem (Chap 11)
1. Describe and recognize: brainstem levels’ names for gross anatomical features and significance of external characteristics 2. Within each brainstem level be able to identify the location: Corticospinal tract, medial lemniscus, and spinothalamic tract; MLF 3. Describe the function/role/location: reticular formation versus reticular activating system; nuclei that contain norepinephrine, dopamine, serotonin, acetylcholine 4. Be able to identify within the respective brainstem level: superior and inferior colliculi, periaqueductal gray, cerebral aqueduct, red nucleus, substantia nigra, cerebral peduncle, decussation of SCP; pons, cerebellar peduncles, deep cerebellar nuclei, fourth ventricle; inferior olive, pyramid, internal arcuate fibers, nucleus gracilis and cuneatus, spinal trigeminal nucleus/tract
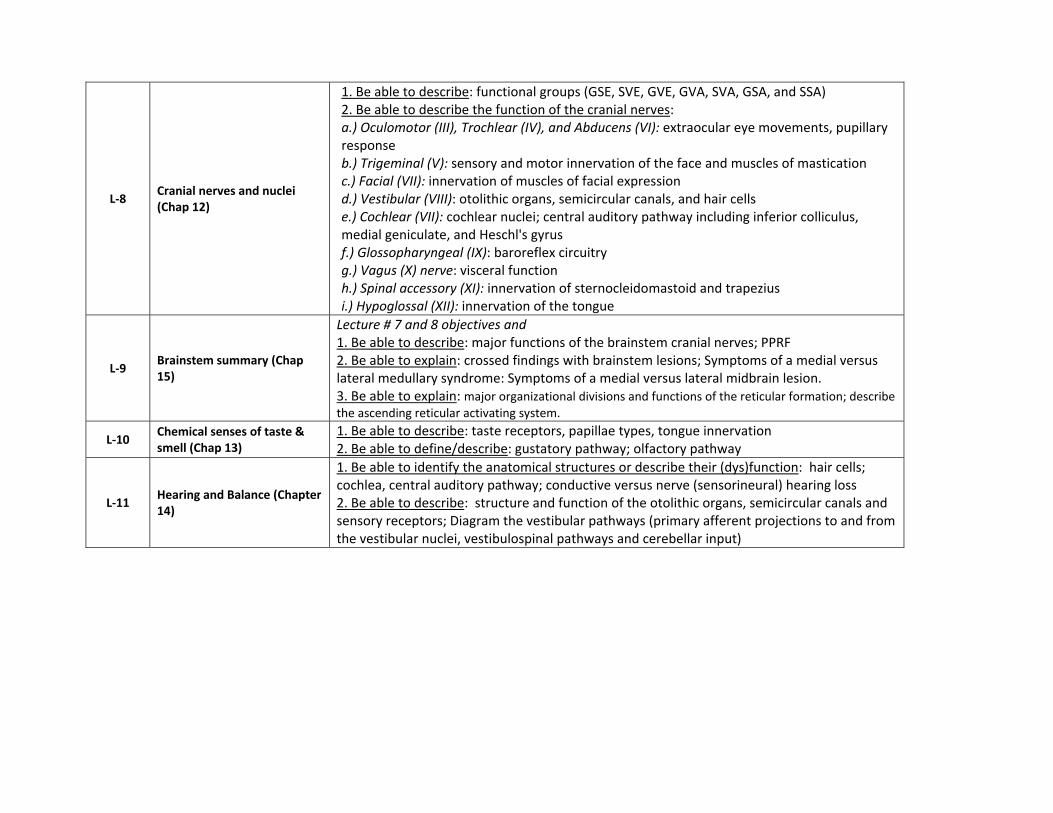
L‐8 Cranial nerves and nuclei (Chap 12)
1. Be able to describe: functional groups (GSE, SVE, GVE, GVA, SVA, GSA, and SSA) 2. Be able to describe the function of the cranial nerves: a.) Oculomotor (III), Trochlear (IV), and Abducens (VI): extraocular eye movements, pupillary response b.) Trigeminal (V): sensory and motor innervation of the face and muscles of mastication c.) Facial (VII): innervation of muscles of facial expression d.) Vestibular (VIII): otolithic organs, semicircular canals, and hair cells e.) Cochlear (VII): cochlear nuclei; central auditory pathway including inferior colliculus, medial geniculate, and Heschl's gyrus f.) Glossopharyngeal (IX): baroreflex circuitry g.) Vagus (X) nerve: visceral function h.) Spinal accessory (XI): innervation of sternocleidomastoid and trapezius i.) Hypoglossal (XII): innervation of the tongue
L‐9 Brainstem summary (Chap 15)
Lecture # 7 and 8 objectives and 1. Be able to describe: major functions of the brainstem cranial nerves; PPRF 2. Be able to explain: crossed findings with brainstem lesions; Symptoms of a medial versus lateral medullary syndrome: Symptoms of a medial versus lateral midbrain lesion. 3. Be able to explain: major organizational divisions and functions of the reticular formation; describe the ascending reticular activating system.
L‐10 Chemical senses of taste & smell (Chap 13)
1. Be able to describe: taste receptors, papillae types, tongue innervation 2. Be able to define/describe: gustatory pathway; olfactory pathway
L‐11 Hearing and Balance (Chapter 14)
1. Be able to identify the anatomical structures or describe their (dys)function: hair cells; cochlea, central auditory pathway; conductive versus nerve (sensorineural) hearing loss 2. Be able to describe: structure and function of the otolithic organs, semicircular canals and sensory receptors; Diagram the vestibular pathways (primary afferent projections to and from the vestibular nuclei, vestibulospinal pathways and cerebellar input)
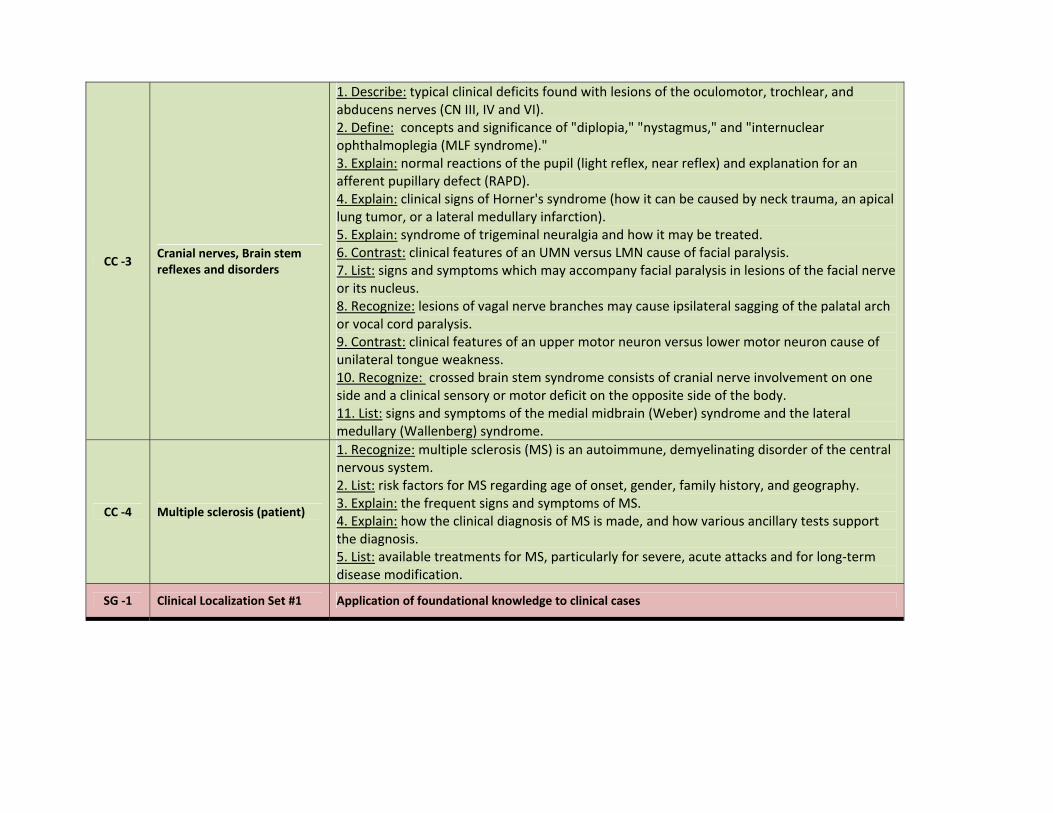
CC ‐3 Cranial nerves, Brain stem reflexes and disorders
1. Describe: typical clinical deficits found with lesions of the oculomotor, trochlear, and abducens nerves (CN III, IV and VI). 2. Define: concepts and significance of "diplopia," "nystagmus," and "internuclear ophthalmoplegia (MLF syndrome)." 3. Explain: normal reactions of the pupil (light reflex, near reflex) and explanation for an afferent pupillary defect (RAPD). 4. Explain: clinical signs of Horner's syndrome (how it can be caused by neck trauma, an apical lung tumor, or a lateral medullary infarction). 5. Explain: syndrome of trigeminal neuralgia and how it may be treated. 6. Contrast: clinical features of an UMN versus LMN cause of facial paralysis. 7. List: signs and symptoms which may accompany facial paralysis in lesions of the facial nerve or its nucleus. 8. Recognize: lesions of vagal nerve branches may cause ipsilateral sagging of the palatal arch or vocal cord paralysis. 9. Contrast: clinical features of an upper motor neuron versus lower motor neuron cause of unilateral tongue weakness. 10. Recognize: crossed brain stem syndrome consists of cranial nerve involvement on one side and a clinical sensory or motor deficit on the opposite side of the body. 11. List: signs and symptoms of the medial midbrain (Weber) syndrome and the lateral medullary (Wallenberg) syndrome.
CC ‐4 Multiple sclerosis (patient)
1. Recognize: multiple sclerosis (MS) is an autoimmune, demyelinating disorder of the central nervous system. 2. List: risk factors for MS regarding age of onset, gender, family history, and geography. 3. Explain: the frequent signs and symptoms of MS. 4. Explain: how the clinical diagnosis of MS is made, and how various ancillary tests support the diagnosis. 5. List: available treatments for MS, particularly for severe, acute attacks and for long‐term disease modification.
SG ‐1 Clinical Localization Set #1 Application of foundational knowledge to clinical cases
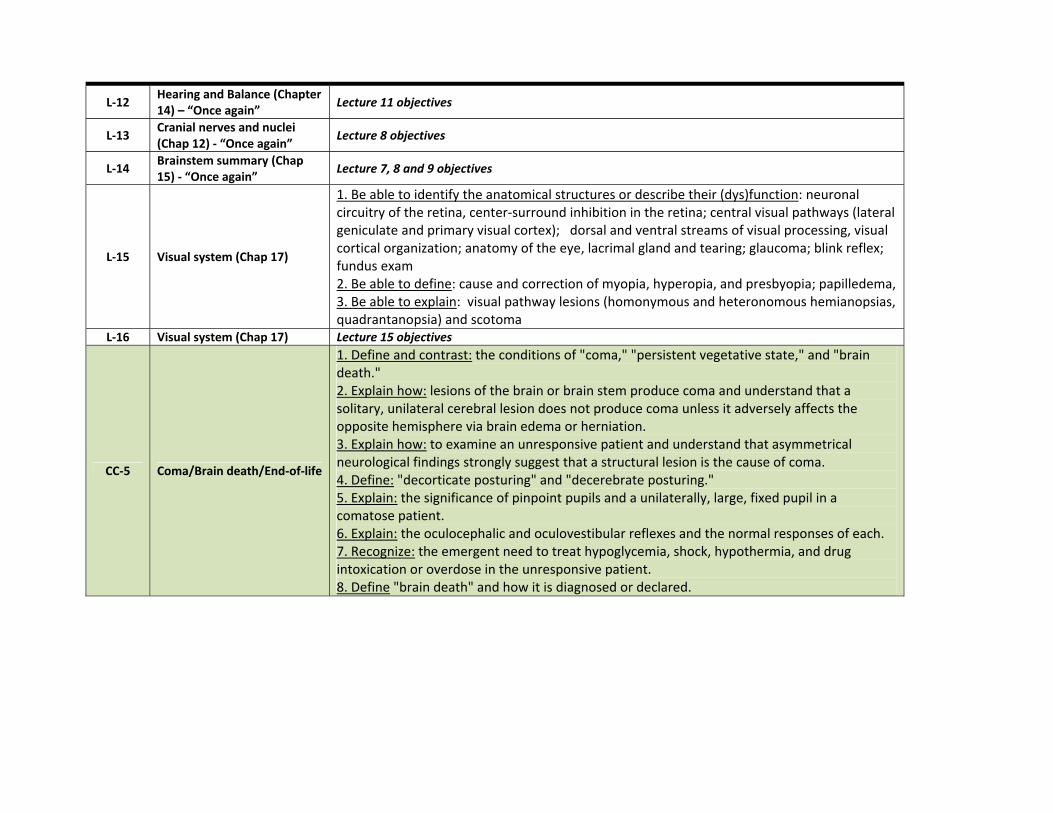
L‐12 Hearing and Balance (Chapter 14) – “Once again” Lecture 11 objectives
L‐13 Cranial nerves and nuclei (Chap 12) ‐ “Once again” Lecture 8 objectives
L‐14 Brainstem summary (Chap 15) ‐ “Once again” Lecture 7, 8 and 9 objectives
L‐15 Visual system (Chap 17)
1. Be able to identify the anatomical structures or describe their (dys)function: neuronal circuitry of the retina, center‐surround inhibition in the retina; central visual pathways (lateral geniculate and primary visual cortex); dorsal and ventral streams of visual processing, visual cortical organization; anatomy of the eye, lacrimal gland and tearing; glaucoma; blink reflex; fundus exam 2. Be able to define: cause and correction of myopia, hyperopia, and presbyopia; papilledema,3. Be able to explain: visual pathway lesions (homonymous and heteronomous hemianopsias, quadrantanopsia) and scotoma
L‐16 Visual system (Chap 17) Lecture 15 objectives
CC‐5 Coma/Brain death/End‐of‐life
1. Define and contrast: the conditions of "coma," "persistent vegetative state," and "brain death." 2. Explain how: lesions of the brain or brain stem produce coma and understand that a solitary, unilateral cerebral lesion does not produce coma unless it adversely affects the opposite hemisphere via brain edema or herniation. 3. Explain how: to examine an unresponsive patient and understand that asymmetrical neurological findings strongly suggest that a structural lesion is the cause of coma. 4. Define: "decorticate posturing" and "decerebrate posturing." 5. Explain: the significance of pinpoint pupils and a unilaterally, large, fixed pupil in a comatose patient. 6. Explain: the oculocephalic and oculovestibular reflexes and the normal responses of each. 7. Recognize: the emergent need to treat hypoglycemia, shock, hypothermia, and drug intoxication or overdose in the unresponsive patient. 8. Define "brain death" and how it is diagnosed or declared.
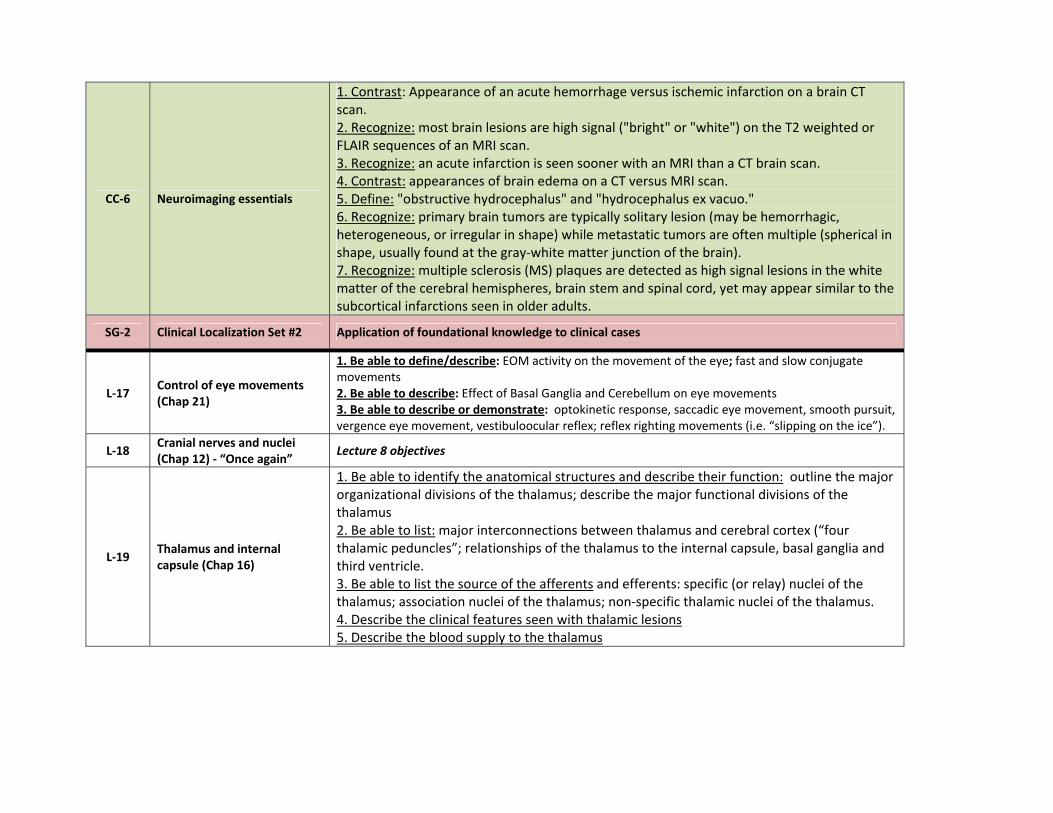
CC‐6 Neuroimaging essentials
1. Contrast: Appearance of an acute hemorrhage versus ischemic infarction on a brain CT scan. 2. Recognize: most brain lesions are high signal ("bright" or "white") on the T2 weighted or FLAIR sequences of an MRI scan. 3. Recognize: an acute infarction is seen sooner with an MRI than a CT brain scan. 4. Contrast: appearances of brain edema on a CT versus MRI scan. 5. Define: "obstructive hydrocephalus" and "hydrocephalus ex vacuo." 6. Recognize: primary brain tumors are typically solitary lesion (may be hemorrhagic, heterogeneous, or irregular in shape) while metastatic tumors are often multiple (spherical in shape, usually found at the gray‐white matter junction of the brain). 7. Recognize: multiple sclerosis (MS) plaques are detected as high signal lesions in the white matter of the cerebral hemispheres, brain stem and spinal cord, yet may appear similar to the subcortical infarctions seen in older adults.
SG‐2 Clinical Localization Set #2 Application of foundational knowledge to clinical cases
L‐17 Control of eye movements (Chap 21)
1. Be able to define/describe: EOM activity on the movement of the eye; fast and slow conjugate movements 2. Be able to describe: Effect of Basal Ganglia and Cerebellum on eye movements 3. Be able to describe or demonstrate: optokinetic response, saccadic eye movement, smooth pursuit, vergence eye movement, vestibuloocular reflex; reflex righting movements (i.e. “slipping on the ice”).
L‐18 Cranial nerves and nuclei (Chap 12) ‐ “Once again” Lecture 8 objectives
L‐19 Thalamus and internal capsule (Chap 16)
1. Be able to identify the anatomical structures and describe their function: outline the major organizational divisions of the thalamus; describe the major functional divisions of the thalamus 2. Be able to list: major interconnections between thalamus and cerebral cortex (“four thalamic peduncles”; relationships of the thalamus to the internal capsule, basal ganglia and third ventricle. 3. Be able to list the source of the afferents and efferents: specific (or relay) nuclei of the thalamus; association nuclei of the thalamus; non‐specific thalamic nuclei of the thalamus. 4. Describe the clinical features seen with thalamic lesions 5. Describe the blood supply to the thalamus
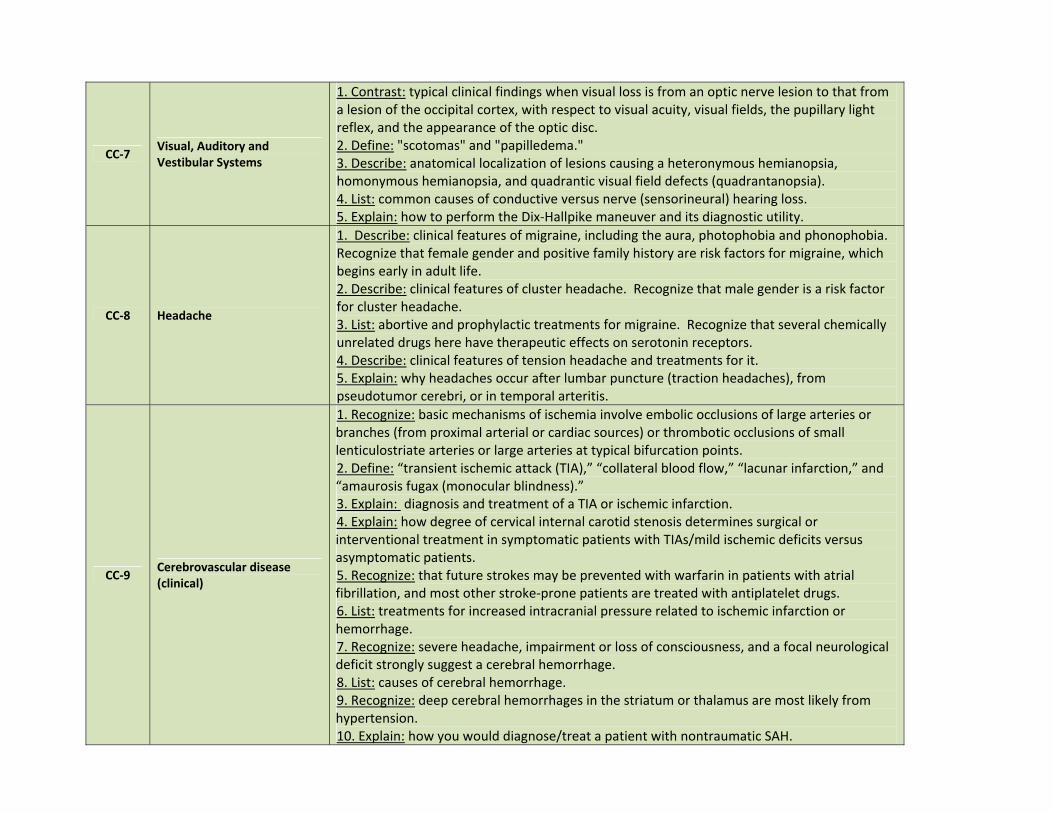
CC‐7 Visual, Auditory and Vestibular Systems
1. Contrast: typical clinical findings when visual loss is from an optic nerve lesion to that from a lesion of the occipital cortex, with respect to visual acuity, visual fields, the pupillary light reflex, and the appearance of the optic disc. 2. Define: "scotomas" and "papilledema." 3. Describe: anatomical localization of lesions causing a heteronymous hemianopsia, homonymous hemianopsia, and quadrantic visual field defects (quadrantanopsia). 4. List: common causes of conductive versus nerve (sensorineural) hearing loss. 5. Explain: how to perform the Dix‐Hallpike maneuver and its diagnostic utility.
CC‐8 Headache
1. Describe: clinical features of migraine, including the aura, photophobia and phonophobia. Recognize that female gender and positive family history are risk factors for migraine, which begins early in adult life. 2. Describe: clinical features of cluster headache. Recognize that male gender is a risk factor for cluster headache. 3. List: abortive and prophylactic treatments for migraine. Recognize that several chemically unrelated drugs here have therapeutic effects on serotonin receptors. 4. Describe: clinical features of tension headache and treatments for it. 5. Explain: why headaches occur after lumbar puncture (traction headaches), from pseudotumor cerebri, or in temporal arteritis.
CC‐9 Cerebrovascular disease (clinical)
1. Recognize: basic mechanisms of ischemia involve embolic occlusions of large arteries or branches (from proximal arterial or cardiac sources) or thrombotic occlusions of small lenticulostriate arteries or large arteries at typical bifurcation points. 2. Define: “transient ischemic attack (TIA),” “collateral blood flow,” “lacunar infarction,” and “amaurosis fugax (monocular blindness).” 3. Explain: diagnosis and treatment of a TIA or ischemic infarction. 4. Explain: how degree of cervical internal carotid stenosis determines surgical or interventional treatment in symptomatic patients with TIAs/mild ischemic deficits versus asymptomatic patients. 5. Recognize: that future strokes may be prevented with warfarin in patients with atrial fibrillation, and most other stroke‐prone patients are treated with antiplatelet drugs. 6. List: treatments for increased intracranial pressure related to ischemic infarction or hemorrhage. 7. Recognize: severe headache, impairment or loss of consciousness, and a focal neurological deficit strongly suggest a cerebral hemorrhage. 8. List: causes of cerebral hemorrhage. 9. Recognize: deep cerebral hemorrhages in the striatum or thalamus are most likely from hypertension. 10. Explain: how you would diagnose/treat a patient with nontraumatic SAH.
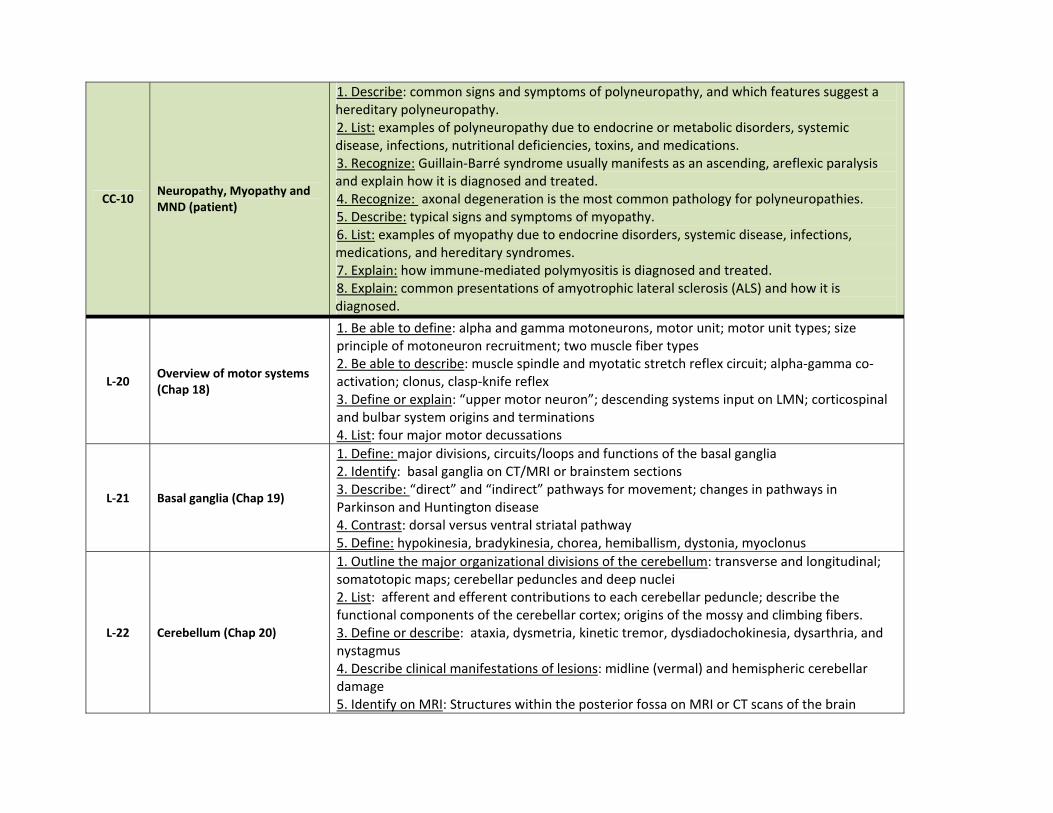
CC‐10 Neuropathy, Myopathy and MND (patient)
1. Describe: common signs and symptoms of polyneuropathy, and which features suggest a hereditary polyneuropathy. 2. List: examples of polyneuropathy due to endocrine or metabolic disorders, systemic disease, infections, nutritional deficiencies, toxins, and medications. 3. Recognize: Guillain‐Barré syndrome usually manifests as an ascending, areflexic paralysis and explain how it is diagnosed and treated. 4. Recognize: axonal degeneration is the most common pathology for polyneuropathies. 5. Describe: typical signs and symptoms of myopathy. 6. List: examples of myopathy due to endocrine disorders, systemic disease, infections, medications, and hereditary syndromes. 7. Explain: how immune‐mediated polymyositis is diagnosed and treated. 8. Explain: common presentations of amyotrophic lateral sclerosis (ALS) and how it is diagnosed.
L‐20 Overview of motor systems (Chap 18)
1. Be able to define: alpha and gamma motoneurons, motor unit; motor unit types; size principle of motoneuron recruitment; two muscle fiber types 2. Be able to describe: muscle spindle and myotatic stretch reflex circuit; alpha‐gamma co‐activation; clonus, clasp‐knife reflex 3. Define or explain: “upper motor neuron”; descending systems input on LMN; corticospinal and bulbar system origins and terminations 4. List: four major motor decussations
L‐21 Basal ganglia (Chap 19)
1. Define: major divisions, circuits/loops and functions of the basal ganglia 2. Identify: basal ganglia on CT/MRI or brainstem sections 3. Describe: “direct” and “indirect” pathways for movement; changes in pathways in Parkinson and Huntington disease 4. Contrast: dorsal versus ventral striatal pathway 5. Define: hypokinesia, bradykinesia, chorea, hemiballism, dystonia, myoclonus
L‐22 Cerebellum (Chap 20)
1. Outline the major organizational divisions of the cerebellum: transverse and longitudinal; somatotopic maps; cerebellar peduncles and deep nuclei 2. List: afferent and efferent contributions to each cerebellar peduncle; describe the functional components of the cerebellar cortex; origins of the mossy and climbing fibers. 3. Define or describe: ataxia, dysmetria, kinetic tremor, dysdiadochokinesia, dysarthria, and nystagmus 4. Describe clinical manifestations of lesions: midline (vermal) and hemispheric cerebellar damage 5. Identify on MRI: Structures within the posterior fossa on MRI or CT scans of the brain
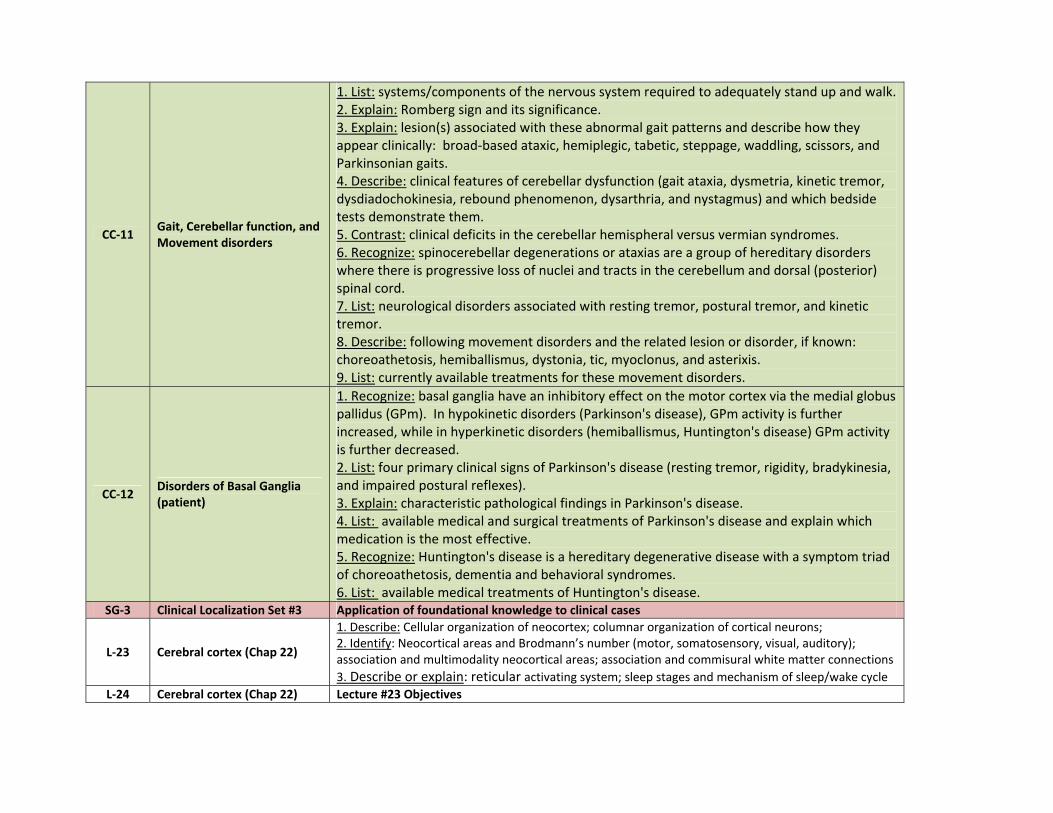
CC‐11 Gait, Cerebellar function, and Movement disorders
1. List: systems/components of the nervous system required to adequately stand up and walk.2. Explain: Romberg sign and its significance. 3. Explain: lesion(s) associated with these abnormal gait patterns and describe how they appear clinically: broad‐based ataxic, hemiplegic, tabetic, steppage, waddling, scissors, and Parkinsonian gaits. 4. Describe: clinical features of cerebellar dysfunction (gait ataxia, dysmetria, kinetic tremor, dysdiadochokinesia, rebound phenomenon, dysarthria, and nystagmus) and which bedside tests demonstrate them. 5. Contrast: clinical deficits in the cerebellar hemispheral versus vermian syndromes. 6. Recognize: spinocerebellar degenerations or ataxias are a group of hereditary disorders where there is progressive loss of nuclei and tracts in the cerebellum and dorsal (posterior) spinal cord. 7. List: neurological disorders associated with resting tremor, postural tremor, and kinetic tremor. 8. Describe: following movement disorders and the related lesion or disorder, if known: choreoathetosis, hemiballismus, dystonia, tic, myoclonus, and asterixis. 9. List: currently available treatments for these movement disorders.
CC‐12 Disorders of Basal Ganglia (patient)
1. Recognize: basal ganglia have an inhibitory effect on the motor cortex via the medial globus pallidus (GPm). In hypokinetic disorders (Parkinson's disease), GPm activity is further increased, while in hyperkinetic disorders (hemiballismus, Huntington's disease) GPm activity is further decreased. 2. List: four primary clinical signs of Parkinson's disease (resting tremor, rigidity, bradykinesia, and impaired postural reflexes). 3. Explain: characteristic pathological findings in Parkinson's disease. 4. List: available medical and surgical treatments of Parkinson's disease and explain which medication is the most effective. 5. Recognize: Huntington's disease is a hereditary degenerative disease with a symptom triad of choreoathetosis, dementia and behavioral syndromes. 6. List: available medical treatments of Huntington's disease.
SG‐3 Clinical Localization Set #3 Application of foundational knowledge to clinical cases
L‐23 Cerebral cortex (Chap 22)
1. Describe: Cellular organization of neocortex; columnar organization of cortical neurons; 2. Identify: Neocortical areas and Brodmann’s number (motor, somatosensory, visual, auditory); association and multimodality neocortical areas; association and commisural white matter connections 3. Describe or explain: reticular activating system; sleep stages and mechanism of sleep/wake cycle
L‐24 Cerebral cortex (Chap 22) Lecture #23 Objectives
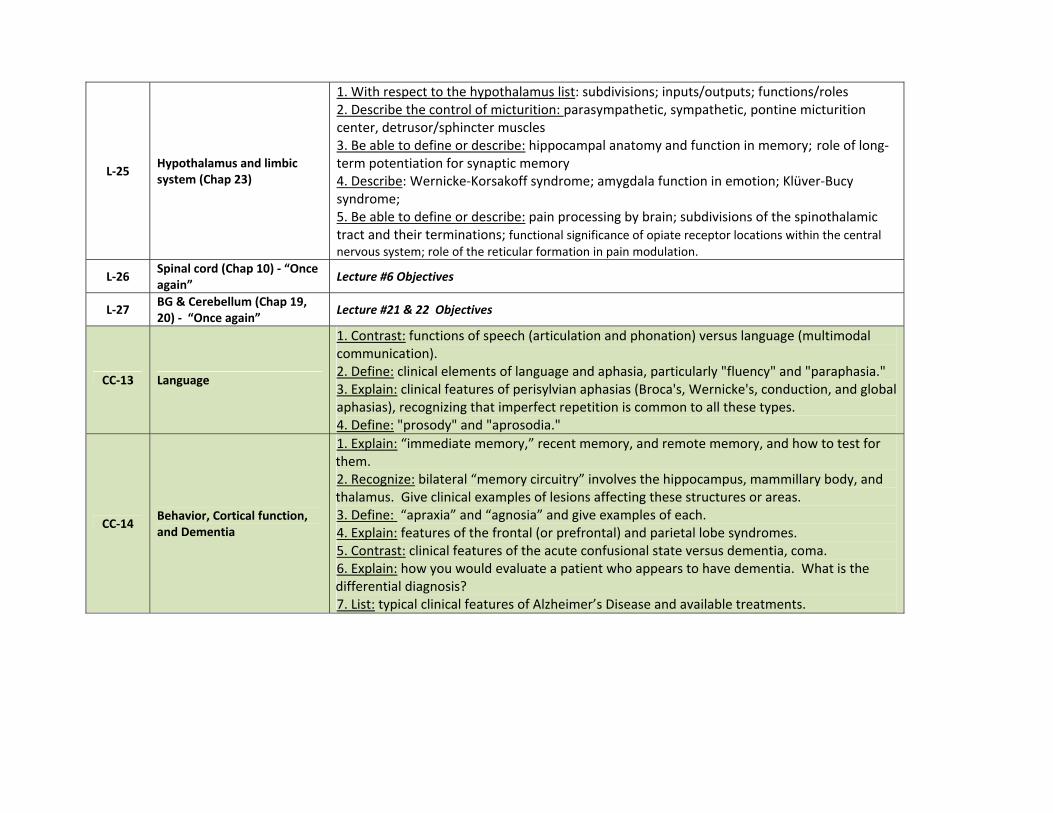
L‐25 Hypothalamus and limbic system (Chap 23)
1. With respect to the hypothalamus list: subdivisions; inputs/outputs; functions/roles 2. Describe the control of micturition: parasympathetic, sympathetic, pontine micturition center, detrusor/sphincter muscles 3. Be able to define or describe: hippocampal anatomy and function in memory; role of long‐term potentiation for synaptic memory 4. Describe: Wernicke‐Korsakoff syndrome; amygdala function in emotion; Klüver‐Bucy syndrome; 5. Be able to define or describe: pain processing by brain; subdivisions of the spinothalamic tract and their terminations; functional significance of opiate receptor locations within the central nervous system; role of the reticular formation in pain modulation.
L‐26 Spinal cord (Chap 10) ‐ “Once again” Lecture #6 Objectives
L‐27 BG & Cerebellum (Chap 19, 20) ‐ “Once again” Lecture #21 & 22 Objectives
CC‐13 Language
1. Contrast: functions of speech (articulation and phonation) versus language (multimodal communication). 2. Define: clinical elements of language and aphasia, particularly "fluency" and "paraphasia." 3. Explain: clinical features of perisylvian aphasias (Broca's, Wernicke's, conduction, and global aphasias), recognizing that imperfect repetition is common to all these types. 4. Define: "prosody" and "aprosodia."
CC‐14 Behavior, Cortical function, and Dementia
1. Explain: “immediate memory,” recent memory, and remote memory, and how to test for them. 2. Recognize: bilateral “memory circuitry” involves the hippocampus, mammillary body, and thalamus. Give clinical examples of lesions affecting these structures or areas. 3. Define: “apraxia” and “agnosia” and give examples of each. 4. Explain: features of the frontal (or prefrontal) and parietal lobe syndromes. 5. Contrast: clinical features of the acute confusional state versus dementia, coma. 6. Explain: how you would evaluate a patient who appears to have dementia. What is the differential diagnosis? 7. List: typical clinical features of Alzheimer’s Disease and available treatments.
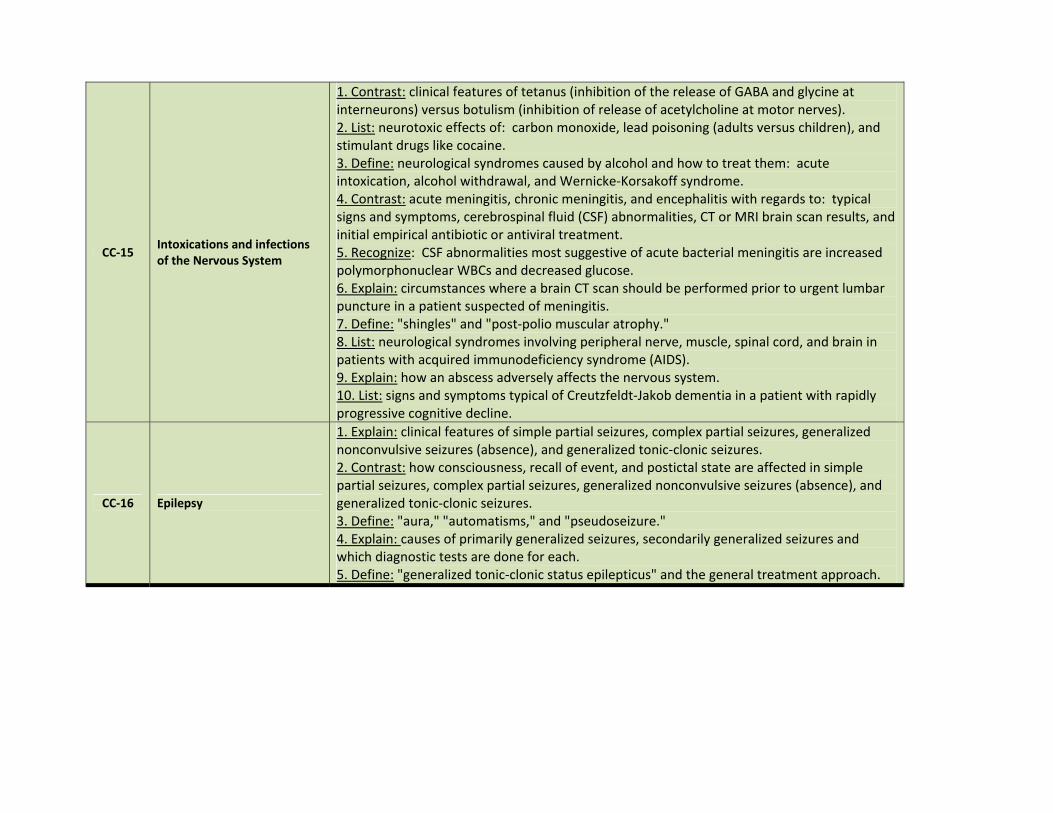
CC‐15 Intoxications and infections of the Nervous System
1. Contrast: clinical features of tetanus (inhibition of the release of GABA and glycine at interneurons) versus botulism (inhibition of release of acetylcholine at motor nerves). 2. List: neurotoxic effects of: carbon monoxide, lead poisoning (adults versus children), and stimulant drugs like cocaine. 3. Define: neurological syndromes caused by alcohol and how to treat them: acute intoxication, alcohol withdrawal, and Wernicke‐Korsakoff syndrome. 4. Contrast: acute meningitis, chronic meningitis, and encephalitis with regards to: typical signs and symptoms, cerebrospinal fluid (CSF) abnormalities, CT or MRI brain scan results, and initial empirical antibiotic or antiviral treatment. 5. Recognize: CSF abnormalities most suggestive of acute bacterial meningitis are increased polymorphonuclear WBCs and decreased glucose. 6. Explain: circumstances where a brain CT scan should be performed prior to urgent lumbar puncture in a patient suspected of meningitis. 7. Define: "shingles" and "post‐polio muscular atrophy." 8. List: neurological syndromes involving peripheral nerve, muscle, spinal cord, and brain in patients with acquired immunodeficiency syndrome (AIDS). 9. Explain: how an abscess adversely affects the nervous system. 10. List: signs and symptoms typical of Creutzfeldt‐Jakob dementia in a patient with rapidly progressive cognitive decline.
CC‐16 Epilepsy
1. Explain: clinical features of simple partial seizures, complex partial seizures, generalized nonconvulsive seizures (absence), and generalized tonic‐clonic seizures. 2. Contrast: how consciousness, recall of event, and postictal state are affected in simple partial seizures, complex partial seizures, generalized nonconvulsive seizures (absence), and generalized tonic‐clonic seizures. 3. Define: "aura," "automatisms," and "pseudoseizure." 4. Explain: causes of primarily generalized seizures, secondarily generalized seizures and which diagnostic tests are done for each. 5. Define: "generalized tonic‐clonic status epilepticus" and the general treatment approach.
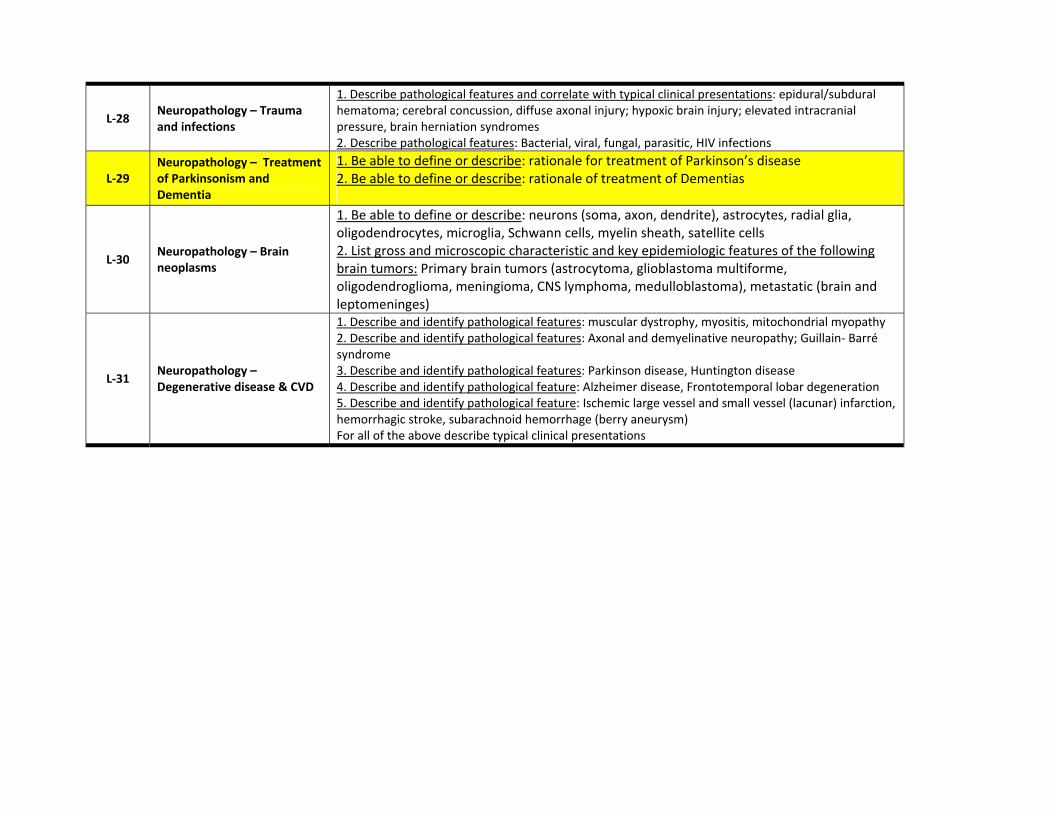
L‐28 Neuropathology – Trauma and infections
1. Describe pathological features and correlate with typical clinical presentations: epidural/subdural hematoma; cerebral concussion, diffuse axonal injury; hypoxic brain injury; elevated intracranial pressure, brain herniation syndromes 2. Describe pathological features: Bacterial, viral, fungal, parasitic, HIV infections
L‐29 Neuropathology – Treatment of Parkinsonism and Dementia
1. Be able to define or describe: rationale for treatment of Parkinson’s disease 2. Be able to define or describe: rationale of treatment of Dementias
L‐30 Neuropathology – Brain neoplasms
1. Be able to define or describe: neurons (soma, axon, dendrite), astrocytes, radial glia, oligodendrocytes, microglia, Schwann cells, myelin sheath, satellite cells 2. List gross and microscopic characteristic and key epidemiologic features of the following brain tumors: Primary brain tumors (astrocytoma, glioblastoma multiforme, oligodendroglioma, meningioma, CNS lymphoma, medulloblastoma), metastatic (brain and leptomeninges)
L‐31 Neuropathology – Degenerative disease & CVD
1. Describe and identify pathological features: muscular dystrophy, myositis, mitochondrial myopathy 2. Describe and identify pathological features: Axonal and demyelinative neuropathy; Guillain‐ Barré syndrome 3. Describe and identify pathological features: Parkinson disease, Huntington disease 4. Describe and identify pathological feature: Alzheimer disease, Frontotemporal lobar degeneration 5. Describe and identify pathological feature: Ischemic large vessel and small vessel (lacunar) infarction, hemorrhagic stroke, subarachnoid hemorrhage (berry aneurysm) For all of the above describe typical clinical presentations
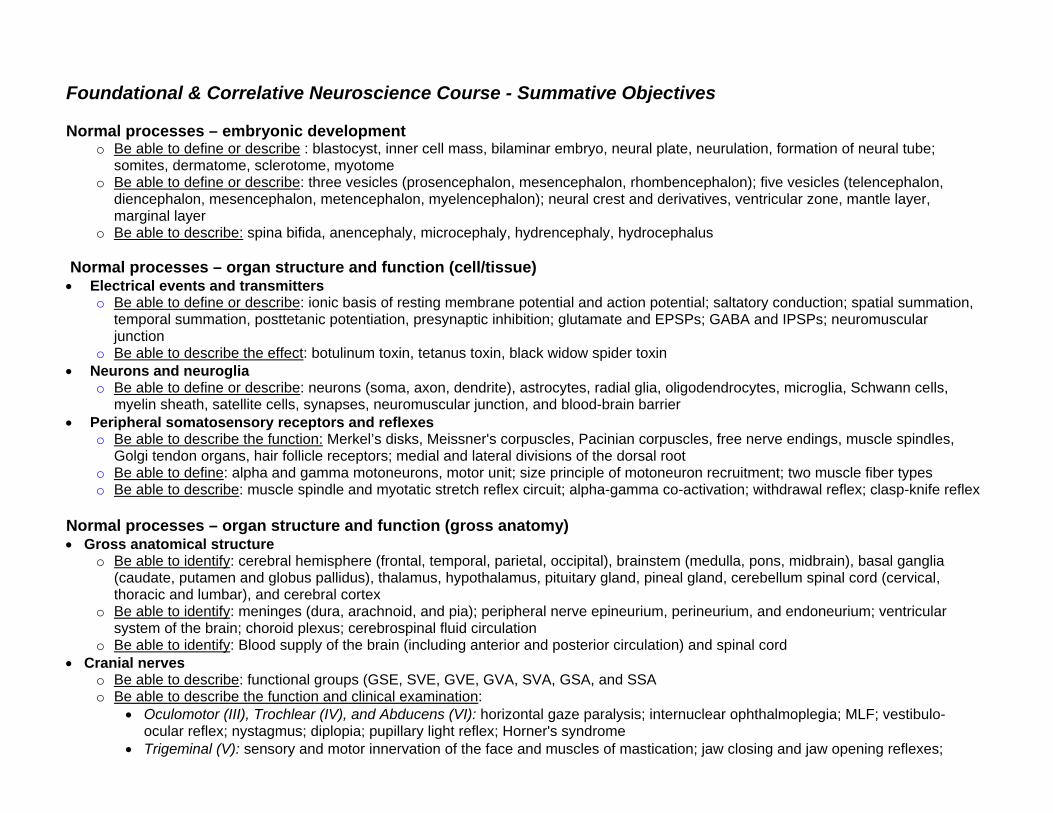
Foundational & Correlative Neuroscience Course - Summative Objectives Normal processes – embryonic development
o Be able to define or describe : blastocyst, inner cell mass, bilaminar embryo, neural plate, neurulation, formation of neural tube; somites, dermatome, sclerotome, myotome
o Be able to define or describe: three vesicles (prosencephalon, mesencephalon, rhombencephalon); five vesicles (telencephalon, diencephalon, mesencephalon, metencephalon, myelencephalon); neural crest and derivatives, ventricular zone, mantle layer, marginal layer
o Be able to describe: spina bifida, anencephaly, microcephaly, hydrencephaly, hydrocephalus
Normal processes – organ structure and function (cell/tissue) Electrical events and transmitters
o Be able to define or describe: ionic basis of resting membrane potential and action potential; saltatory conduction; spatial summation, temporal summation, posttetanic potentiation, presynaptic inhibition; glutamate and EPSPs; GABA and IPSPs; neuromuscular junction
o Be able to describe the effect: botulinum toxin, tetanus toxin, black widow spider toxin Neurons and neuroglia
o Be able to define or describe: neurons (soma, axon, dendrite), astrocytes, radial glia, oligodendrocytes, microglia, Schwann cells, myelin sheath, satellite cells, synapses, neuromuscular junction, and blood-brain barrier
Peripheral somatosensory receptors and reflexes o Be able to describe the function: Merkel’s disks, Meissner's corpuscles, Pacinian corpuscles, free nerve endings, muscle spindles,
Golgi tendon organs, hair follicle receptors; medial and lateral divisions of the dorsal root o Be able to define: alpha and gamma motoneurons, motor unit; size principle of motoneuron recruitment; two muscle fiber types o Be able to describe: muscle spindle and myotatic stretch reflex circuit; alpha-gamma co-activation; withdrawal reflex; clasp-knife reflex
Normal processes – organ structure and function (gross anatomy) Gross anatomical structure
o Be able to identify: cerebral hemisphere (frontal, temporal, parietal, occipital), brainstem (medulla, pons, midbrain), basal ganglia (caudate, putamen and globus pallidus), thalamus, hypothalamus, pituitary gland, pineal gland, cerebellum spinal cord (cervical, thoracic and lumbar), and cerebral cortex
o Be able to identify: meninges (dura, arachnoid, and pia); peripheral nerve epineurium, perineurium, and endoneurium; ventricular system of the brain; choroid plexus; cerebrospinal fluid circulation
o Be able to identify: Blood supply of the brain (including anterior and posterior circulation) and spinal cord Cranial nerves
o Be able to describe: functional groups (GSE, SVE, GVE, GVA, SVA, GSA, and SSA o Be able to describe the function and clinical examination:
Oculomotor (III), Trochlear (IV), and Abducens (VI): horizontal gaze paralysis; internuclear ophthalmoplegia; MLF; vestibulo-ocular reflex; nystagmus; diplopia; pupillary light reflex; Horner's syndrome
Trigeminal (V): sensory and motor innervation of the face and muscles of mastication; jaw closing and jaw opening reflexes;
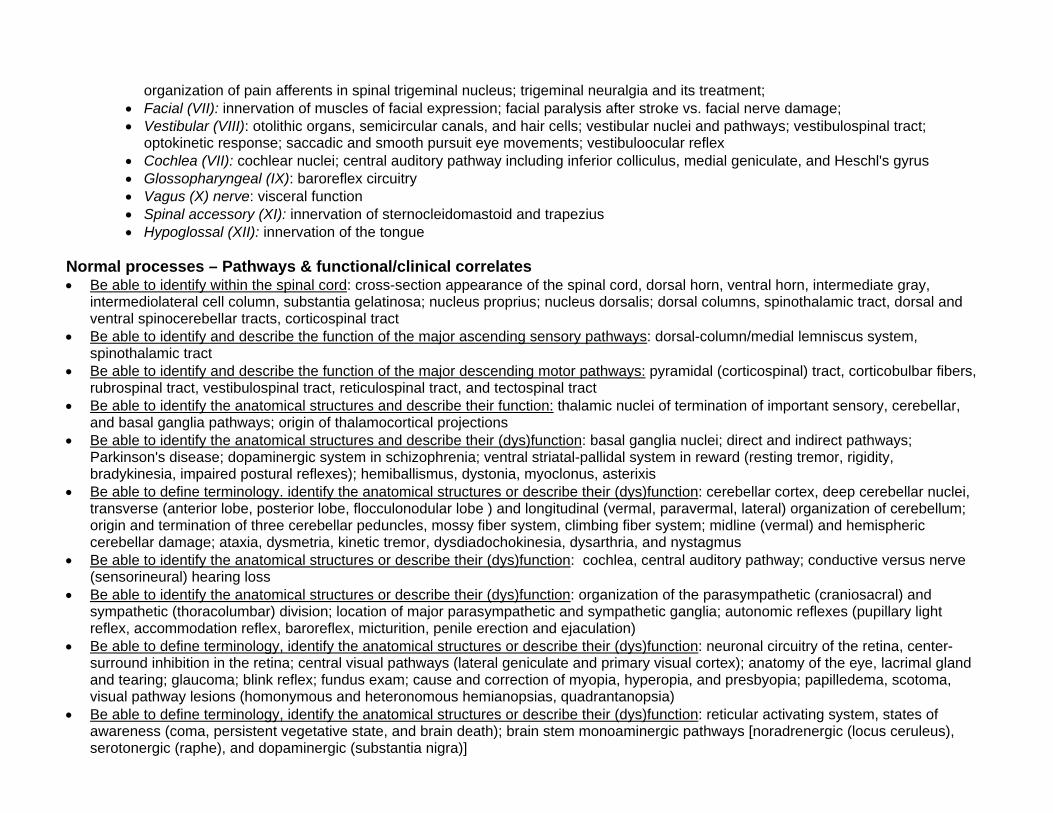
organization of pain afferents in spinal trigeminal nucleus; trigeminal neuralgia and its treatment; Facial (VII): innervation of muscles of facial expression; facial paralysis after stroke vs. facial nerve damage; Vestibular (VIII): otolithic organs, semicircular canals, and hair cells; vestibular nuclei and pathways; vestibulospinal tract;
optokinetic response; saccadic and smooth pursuit eye movements; vestibuloocular reflex Cochlea (VII): cochlear nuclei; central auditory pathway including inferior colliculus, medial geniculate, and Heschl's gyrus Glossopharyngeal (IX): baroreflex circuitry Vagus (X) nerve: visceral function Spinal accessory (XI): innervation of sternocleidomastoid and trapezius Hypoglossal (XII): innervation of the tongue
Normal processes – Pathways & functional/clinical correlates Be able to identify within the spinal cord: cross-section appearance of the spinal cord, dorsal horn, ventral horn, intermediate gray,
intermediolateral cell column, substantia gelatinosa; nucleus proprius; nucleus dorsalis; dorsal columns, spinothalamic tract, dorsal and ventral spinocerebellar tracts, corticospinal tract
Be able to identify and describe the function of the major ascending sensory pathways: dorsal-column/medial lemniscus system, spinothalamic tract
Be able to identify and describe the function of the major descending motor pathways: pyramidal (corticospinal) tract, corticobulbar fibers, rubrospinal tract, vestibulospinal tract, reticulospinal tract, and tectospinal tract
Be able to identify the anatomical structures and describe their function: thalamic nuclei of termination of important sensory, cerebellar, and basal ganglia pathways; origin of thalamocortical projections
Be able to identify the anatomical structures and describe their (dys)function: basal ganglia nuclei; direct and indirect pathways; Parkinson's disease; dopaminergic system in schizophrenia; ventral striatal-pallidal system in reward (resting tremor, rigidity, bradykinesia, impaired postural reflexes); hemiballismus, dystonia, myoclonus, asterixis
Be able to define terminology. identify the anatomical structures or describe their (dys)function: cerebellar cortex, deep cerebellar nuclei, transverse (anterior lobe, posterior lobe, flocculonodular lobe ) and longitudinal (vermal, paravermal, lateral) organization of cerebellum; origin and termination of three cerebellar peduncles, mossy fiber system, climbing fiber system; midline (vermal) and hemispheric cerebellar damage; ataxia, dysmetria, kinetic tremor, dysdiadochokinesia, dysarthria, and nystagmus
Be able to identify the anatomical structures or describe their (dys)function: cochlea, central auditory pathway; conductive versus nerve (sensorineural) hearing loss
Be able to identify the anatomical structures or describe their (dys)function: organization of the parasympathetic (craniosacral) and sympathetic (thoracolumbar) division; location of major parasympathetic and sympathetic ganglia; autonomic reflexes (pupillary light reflex, accommodation reflex, baroreflex, micturition, penile erection and ejaculation)
Be able to define terminology, identify the anatomical structures or describe their (dys)function: neuronal circuitry of the retina, center-surround inhibition in the retina; central visual pathways (lateral geniculate and primary visual cortex); anatomy of the eye, lacrimal gland and tearing; glaucoma; blink reflex; fundus exam; cause and correction of myopia, hyperopia, and presbyopia; papilledema, scotoma, visual pathway lesions (homonymous and heteronomous hemianopsias, quadrantanopsia)
Be able to define terminology, identify the anatomical structures or describe their (dys)function: reticular activating system, states of awareness (coma, persistent vegetative state, and brain death); brain stem monoaminergic pathways [noradrenergic (locus ceruleus), serotonergic (raphe), and dopaminergic (substantia nigra)]
Be able to define terminology, identify the anatomical structures or describe their (dys)function: sleep (different phases of sleep and their EEG pattern, changes in sleep pattern with age); sleep disorders (sleep apnea, restless legs, narcolepsy, insomnia); orexin/hypocretin system and sleep
Normal processes – repair, regeneration and age related changes Be able to define or describe: end of life issues related to brain damage and disease; nutrition or sedation in patients with dementia or
amyotrophic lateral sclerosis; role of physician in palliative care Abnormal processes Brain neoplasms
o Be able to define or describe: histology of different types of brain tumors (astrocytoma, ependymoma, medulloblastoma; meningioma); radiotherapy versus surgical treatment of brain tumors; primary and secondary brain tumors
Hypothalamus and neuroendocrine o Be able to define or describe: releasing factors; energy homeostasis; water balance; reproduction; stress responses;
thermoregulation; circadian rhythms Limbic system
o Be able to define or describe: hippocampal anatomy and function in memory; Wernicke-Korsakoff syndrome; role of long-term potentiation for synaptic memory; amygdala function in emotion; Klüver-Bucy syndrome;
o Be able to define or describe: pain processing by brain; subdivisions of the spinothalamic tract and their terminations; treatment of pain; types of headache (migraine, cluster, tension, post-lumbar puncture, arteritis) and their treatment
Clinical & therapeutic correlation Cerebrovascular disease
o Be able to define or describe: transient ischemic attacks (TIA), collateral blood flow; lacunar infarction; amaurosis fugax, embolic causes of stroke, development of increased intracranial pressure in stroke, headache development in cerebral hemorrhage
o Be able to explain treatment or rationale of care: TIA or ischemic stroke, carotid stenosis, use of warfarin (Coumadin) and antiplatelet drugs, nontraumatic subarachnoid hemorrhage
Cortical disorders o Define or describe the cortical localization: somatosensory, visual, and auditory sensory areas, motor cortex, prefrontal cortical
function o Describe the clinical features: lateral brainstem syndrome (Wallenberg) and medial midbrain (Weber) syndromes o Define or contrast: Broca's, Wernicke's, conduction or global aphasia; articulation, phonation, fluency, paraphasia, prosody and
"aprosodia" o Define or describe: contralateral neglect, catastrophic reaction, hemispheric specialization; dorsal and ventral streams of visual
processing, visual cortical organization o Define and contrast: dementia versus acute confusional state; coma, persistent vegetative state and brain death; decorticate
posturing, decerebrate posturing
Epilepsy and paroxysmal disorders o Explain and contrast the clinical features: simple partial seizures, complex partial seizures, generalized nonconvulsive seizures
(absence), generalized tonic-clonic seizures o Define or describe: automatism, status epilepticus, “pseudoseizure”, primary versus secondarily generalized seizures, EEG
abnormalities in patients with epilepsy o Define: generalized tonic-clonic status epilepticus, general treatment approach to status epilepticus
Peripheral nervous system o Explain or contrast: upper versus lower motor neuron signs and symptoms; radicular versus referred pain; weakness of muscle versus
neuromuscular junction. o Define or describe the clinical features, etiology an treatment: myasthenia gravis, Lambert Eaton myasthenic syndrome; myopathies;
neuropathies (polyneuropathies, Guillain-Barré); amyotrophic lateral sclerosis
Spinal cord o Contrast hemiplegia caused by lesions: cervical spinal cord, brain stem, subcortical areas, or cortical area o Define or describe the clinical features and etiology: intramedullary versus extramedullary spinal lesions; Brown-Sequard hemicord
syndrome, syringomyelia, amyotrophic lateral sclerosis, tabes dorsalis, anterior spinal artery syndrome, subacute combined degeneration, spinal shock
Specific Clinical Disorders o Define and contrast: tetanus versus botulism; viral versus bacterial meningitis o Describe features: carbon monoxide poisoning, lead poisoning, shingles, post-polio muscular atrophy, Creutzfeldt-Jakob dementia o Describe features, diagnosis and treatment: Alzheimer’s disease, headache (migraine, cluster, post-lumbar puncture), multiple
sclerosis, Parkinson disease o Describe or define the etiology or current pathophysiology: Alzheimer's disease, Pick's disease, frontotemporal lobar dementia;
Parkinson's disease, Huntington's disease, progressive supranuclear palsy, multiple system atrophy; multiple sclerosis; spinocerebellar degenerations (Friedreich’s ataxia); amyotrophic lateral sclerosis
o Describe features, diagnosis or treatment: skull fracture, epidural hematoma, cerebral concussion, diffuse axonal injury, hypoxic brain injury, elevated intracranial pressure, brain herniation syndromes
o Describe features, diagnosis or treatment: hypoglycemia, shock, hypothermia, and drug intoxication or overdose in the unresponsive patient
o Describe features, diagnosis: brain death
Neuroimaging (CT and MRI) o Be able to identify: cerebrum, cerebellum, basal ganglia (caudate and lentiform), internal capsule, thalamus, lateral and fourth
ventricles, cerebellopontine angle, sella turcica, cavernous sinus o Be able to distinguish or recognize: "bright" high signal appearance of brain lesions on T2 or FLAIR MRI, acute hemorrhage on CT
versus ischemic infarction, brain edema on CT versus MRI, obstructive hydrocephalus versus hydrocephalus ex vacuo, typical appearance of a primary versus metastatic brain tumor, multiple sclerosis plaques on MRI