Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Cost-effectiveness of adenotonsillectomy in reducingobstructive sleep apnea, cerebrovascular ischemia,vaso-occlusive pain, and ACS episodes in pediatricsickle cell disease
Avnish Tripathi & Jeanette M. Jerrell &James R. Stallworth
Received: 23 November 2009 /Accepted: 4 August 2010 /Published online: 17 August 2010# Springer-Verlag 2010
Abstract In children with sickle cell disease (SCD),adenotonsillar hypertrophy or recurrent tonsillitis arefrequently linked with an increased risk of obstructivesleep apnea, cerebrovascular ischemia, or frequent painepisodes and often require an adenoidectomy and/ortonsillectomy. Interventions designed to prevent thesecomplications, control vaso-occlusive pain episodes, andavoid hospitalizations may reduce the significant personaland economic burden of SCD. This study compares episoderecurrence and treatment costs for cerebrovascular ische-mia, vaso-occlusive pain, acute chest syndrome (ACS), andobstructive sleep apnea in children who had an adenoton-sillectomy (A/T surgery, N=256; 11.7%) and a matchedcohort of those who did not (N=512; 23.3%) from a cohortof 2,194 children and adolescents with SCD from SouthCarolina’s Medicaid system. A/T surgery was associatedwith a significantly reduced rate of visits over time forobstructive sleep apnea and cerebrovascular ischemia (e.g.,stroke, transient ischemic attacks), but not with any change
in the rate of visits for vaso-occlusive pain or ACS/pneumonia visits. The rate of mean acute (emergency andinpatient) service costs was significantly decreasing overtime after an increase about the time the A/T surgery wasperformed. The cost-effectiveness of adenoidectomy and/ortonsillectomy for treating obstructive sleep apnea andpreventing cerebrovascular ischemia without increasingvaso-occlusive pain episodes or long-term acute servicecosts in routine clinical practice settings was demonstrated.The matched control group of SCD patients without A/Tsurgery contained more patients with severe vaso-occlusivepain episodes, ACS visits, and higher mean total costs overtime and appears to represent a different phenotype ofchildren with SCD.
Keywords Sickle cell disease . Adenotonsillectomy .
Vaso-occlusive pain episodes . Cost reductions
Introduction
The cardinal clinical feature of sickle cell disease (SCD) ispain from vaso-occlusive episodes. The pathogenesis of thispain is disruption of blood flow in the microvasculature bysickle-shaped red blood cells, resulting in tissue ischemia [1].Precipitating causes of painful episodes include physicalstress, infection, dehydration, hypoxia, local or systemicacidosis, and exposure to cold for prolonged periods. Theaverage hospital stay for children admitted for vaso-occlusive pain is 3–5 days [1, 2]. Interventions designed toprevent SCD complications, control vaso-occlusive painepisodes, and avoid hospitalizations may reduce the signif-icant individual and economic burden of the disease [3].
A. TripathiDepartment of Epidemiology and Biostatistics,University of South Carolina Arnold School of Public Health,Columbia, SC, USA
J. M. Jerrell (*)Department of Neuropsychiatry and Behavioral Science,University of South Carolina School of Medicine,3555 Harden Street Extension, 15 Medical Park Suite 301,Columbia, SC 29203, USAe-mail: [email protected]
J. R. StallworthDepartment of Pediatrics,University of South Carolina School of Medicine,Columbia, SC, USA
Ann Hematol (2011) 90:145–150DOI 10.1007/s00277-010-1048-4

Children are at risk of developing adenotonsillarhypertrophy and recurrent tonsillitis, which increases therisk of obstructive sleep apnea [4] and vaso-occlusive painepisodes in SCD. Furthermore, obstructive sleep apnea isassociated with an increased risk of serious cerebrovascu-lar complications such as transient ischemic attack (TIA)and stroke [5, 6]. Pertinent literature suggests that amongchildren with SCD, approximately 11% may have overtstrokes while 20% may have silent strokes by 1 year ofage [7]. Adenoidectomy and/or tonsillectomy (A/T sur-gery) is an important clinical intervention for recurrenttonsillitis and the reduction of obstructive sleep apnea [8].Moreover, this intervention may consequently reduce therecurrence and severity of cerebrovascular ischemic eventsand vaso-occlusive pain episodes. Early studies of theeffect of tonsillectomy on the frequency of sickle cell paincrises typically have employed small case studies orclinical samples and brief follow-up periods (i.e., 1–2 years), but the results were generally promising withthe mean number of pain crises decreasing by over 50%during the 12–24 months after surgery without resultingcomplications [9–12].
However, SCD patients undergoing tonsillectomy withor without adenoidectomy are recognized as having arelatively higher risk for postoperative complications,including fever, atelectasis, pneumonia or additional vaso-occlusion, and pain [13], with age and the presence ofobstructive sleep apnea increasing the potential risk forthese postoperative complications. Even with meticulouscare (with simple or aggressive transfusions and hydrationpreoperatively, and extensive perioperative managementwith hospital stays averaging 3 to 5 days), approximately25% to 30% of SCD patients will have a postoperativecomplication [5]. More recent results demonstrate that themajority of these pediatric SCD patients can be managedwith <24-h hospitalization stays with no increase incomplication rates [2].
There is limited literature, especially on large-scaleobservational data, which has demonstrated the cost-effectiveness of A/T surgery in mitigating SCD-relatedcomplications. In this investigation, we assess changeover time in the episodes of obstructive sleep apnea,cerebrovascular ischemia, acute chest syndrome (ACS),and vaso-occlusive pain in a cohort of children with SCDwho had A/T surgery. We then evaluate the cost-effectiveness of A/T surgery by comparing care costs interms of acute (emergency + inpatient), outpatient, andtotal service provision between SCD children whoreceived A/T surgery and a matched group of SCDchildren who did not have A/T surgery, after controllingfor other interventions received, including prophylacticpenicillin, hydroxyurea, and blood transfusions to preventstroke.
Methods and materials
Medical and pharmacy claims for the calendar yearsJanuary 1, 1996 through December 31, 2006 were used toidentify a cohort of child and adolescent patients (ages 17and under) enrolled in and eligible for Medicaid for aminimum of 9 months in each calendar year included in thisanalysis, who had a service encounter with a diagnosis of282.6x (thalassemia and SC trait were not included). Theselection encounter date was the date of the first visit inwhich the SCD diagnosis was made. The Medicaid data-bases are frequently updated prior to being made availablefor analysis. This study was approved by the University ofSouth Carolina Institutional Review Board as exempt fromhuman subject research guidelines under 45 Code ofFederal Regulations part 46.
Primary or secondary diagnosis codes for sickle cellvaso-occlusive pain crises, ACS or pneumonia, obstructivesleep apnea, and cerebrovascular ischemia (i.e., stroke andtransient ischemic attacks) and the outpatient, acute(emergency visits + hospital days), and combined totalcosts of SCD-related health services were aggregated fromthe visits file into two 12-month periods before the A/Tsurgery was performed (baseline) and three 12-monthperiods after it was performed. Five 12-month time periodswere also aggregated for the control cases. Prescriptions forhydroxyurea (HU) (DROXIA, HYDRIA) and penicillinwere coded from the pharmacy file. CPT procedure codesfor A/T surgery and transfusions were obtained from thevisits file. An incidence density matching method was usedto select the comparison group which did not have A/Tsurgery. Cases were matched (one case to two controls) onage, gender, ethnicity, time in the Medicaid data set, andseverity (mean number of vaso-occlusive pain visits duringthe baseline period).
To examine the impact of the A/T surgery over time onthe frequency of vaso-occlusive pain, ACS/pneumonia,obstructive sleep apnea, cerebrovascular visits, and thechange in outpatient, acute, and total costs, a series ofnegative binomial regression models (for non-normallydistributed count data; PROC GENMOD facility in SASversion 9.1; SAS Institute Inc., Cary, North Carolina) wasemployed to calculate a ratio of the log rate of each type ofvisit or cost per time period that the patient was covered inthe Medicaid data set [14, 15]. Receipt of transfusions,prophylactic penicillin, or HU (dichotomously coded as yes/no), and the percentage of SCD services received from aspecialty clinic for SCD were used as covariates to representinterventions or type of care that might also explain differ-ences in effectiveness or costs. The resulting model estimateswere converted into rate ratios and 95% confidence intervaland p values are used to report statistical significance, usingtwo-tailed tests and α≤0.05 for statistical significance.
146 Ann Hematol (2011) 90:145–150

Results
Clinical characteristics of patients
The cohorts of SCD patients who received A/T surgery andthe controls who did not are described in Table 1. Both the A/T surgery and no-surgery cohorts were predominantly male(60%), about 5 years old when their first SCD diagnosis wasdocumented under Medicaid coverage, 41% were AfricanAmerican, and 59% were of mixed African–other race,Hispanic, Middle Eastern, or Asian Indian ancestry. Forty-four percent of each cohort had three to six vaso-occlusivepain episodes per year during the baseline period (severityindicator) and were enrolled in Medicaid, a mean of 8 years.Ten percent of those receiving A/T surgery were cared for byspecialty clinics in South Carolina; whereas, only 7% ofthose in the no-surgery cohort received this care. The A/Tsurgery cohort had significantly more mean visits forobstructive sleep apnea, recurrent tonsillitis, and stroke, butthere were no significant differences between the cohorts forunadjusted vaso-occlusive pain or ACS/pneumonia visits orbeing prescribed penicillin, HU, or blood transfusions. Thecardiovascular, hepatic, renal, spleen, and pulmonary com-
plications associated with SCD were significantly moreprevalent in the A/T surgery cohort.
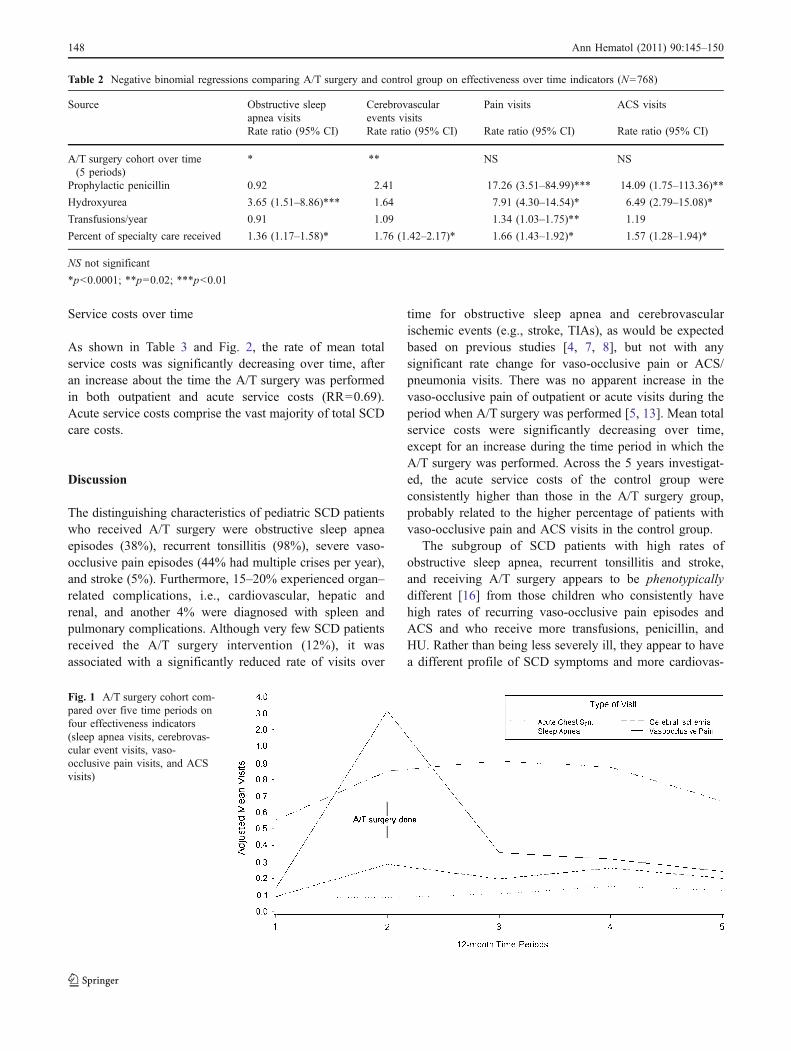
A/T surgery was associated with a significantly reducedrate of visits over time in which obstructive sleep apneaand cerebrovascular ischemia events (e.g., stroke, TIAs)were diagnosed/treated (Table 2; Fig. 1), but not with anystatistically significant change in the rate of visits in whichvaso-occlusive pain or ACS/pneumonia was diagnosed/treated, controlling for receipt of specialty care. As seen inFig. 1, the mean number of obstructive sleep apnea visitsincreased about the same time that the A/T surgery wasperformed, decreased immediately thereafter, andremained lower over time than the rate of obstructivesleep apnea visits for those not having A/T surgery. Alsoportrayed in Fig. 1 is the minimal change in visit rates forvaso-occlusive pain, ACS, or cerebrovascular ischemiaover the 5-year period. Patients who were significantlymore likely to experience pain crises [rate ratio (RR)=17.26; RR=14.09, respectively] and ACS/pneumoniaepisodes (RR=7.91; RR=6.49, respectively) were morelikely to be prescribed prophylactic penicillin and HU(Table 2). HU was also likely to be given to thoseexperiencing more obstructive sleep apnea (RR=3.65).
Table 1 Descriptive comparison of the A/T surgery and the control cohorts
Independent variable A/T surgery cohort Control cohort p value(N=256) (N=512)
Ethnicity African American (%) 104 (40.6) 208 (40.6) 1.00Non-African Americana (%) 152 (59.4) 304 (59.4)
Gender Female (%) 102 (39.8) 204 (39.8%) 1.00Male (%) 154 (60.2) 308 (60.2)
Mean age at SCD diagnosis as documented in Medicaid (SD) 4.8 (4.4) 5.5 (5.1) 0.24
Hydroxyurea: Yes (%) 23 (8.9) 63 (12.3) 0.17
Years in Medicaid (SD) 8.1 (2.6) 8.2 (2.6) 0.58
Baseline vaso-occlusive pain severity: yes (%) 114 (44.5) 228 (44.4) 1.00
Percent receiving care at specialty clinic (SD) 10.2% (12.8) 7.3% (12.3) <0.0001
Penicillin days received (SD) 423.9 (622.4) 563.6 (712.8) 0.21
Mean transfusions/year (SD) 0.9 (5.6) 1.7 (6.4) 0.28
Mean total vaso-occlusive pain visits (SD) 20.1 (45.8) 55.6 (166.0) 0.43
Mean total ACS visits (SD) 3.2 (9.7) 6.1 (15.8) 0.0003
Mean total pneumonia visits (SD) 0.2 (1.5) 0.1 (0.4) 0.08
Mean total obstructive sleep apnea visits (SD) 1.6 (4.4) 0.2 (1.4) <0.0001
Mean total recurrent tonsillitis visits (SD) 5.9 (3.2) 0.6 (1.5) <0.0001
Mean total stroke visits complications (SD) 0.6 (2.1) 0.2 (1.7) 0.04
Cardiovascular (any) yes (%) 48 (18.8) 45 (8.8) <0.0001
Hepatic (any) yes (%) 38 (14.8) 41 (8.1) 0.003
Renal (any) yes (%) 50 (19.5) 34 (6.7) <0.0001
Spleen (any) yes (%) 11 (4.3) 8 (1.6) 0.02
Pulmonary (any) yes (%) 10 (3.9) 6 (1.2) 0.01
a Hispanic, Middle Eastern, Asian Indian, or mixed
Ann Hematol (2011) 90:145–150 147
Service costs over time
As shown in Table 3 and Fig. 2, the rate of mean totalservice costs was significantly decreasing over time, afteran increase about the time the A/T surgery was performedin both outpatient and acute service costs (RR=0.69).Acute service costs comprise the vast majority of total SCDcare costs.
Discussion
The distinguishing characteristics of pediatric SCD patientswho received A/T surgery were obstructive sleep apneaepisodes (38%), recurrent tonsillitis (98%), severe vaso-occlusive pain episodes (44% had multiple crises per year),and stroke (5%). Furthermore, 15–20% experienced organ–related complications, i.e., cardiovascular, hepatic andrenal, and another 4% were diagnosed with spleen andpulmonary complications. Although very few SCD patientsreceived the A/T surgery intervention (12%), it wasassociated with a significantly reduced rate of visits over
time for obstructive sleep apnea and cerebrovascularischemic events (e.g., stroke, TIAs), as would be expectedbased on previous studies [4, 7, 8], but not with anysignificant rate change for vaso-occlusive pain or ACS/pneumonia visits. There was no apparent increase in thevaso-occlusive pain of outpatient or acute visits during theperiod when A/T surgery was performed [5, 13]. Mean totalservice costs were significantly decreasing over time,except for an increase during the time period in which theA/T surgery was performed. Across the 5 years investigat-ed, the acute service costs of the control group wereconsistently higher than those in the A/T surgery group,probably related to the higher percentage of patients withvaso-occlusive pain and ACS visits in the control group.
The subgroup of SCD patients with high rates ofobstructive sleep apnea, recurrent tonsillitis and stroke,and receiving A/T surgery appears to be phenotypicallydifferent [16] from those children who consistently havehigh rates of recurring vaso-occlusive pain episodes andACS and who receive more transfusions, penicillin, andHU. Rather than being less severely ill, they appear to havea different profile of SCD symptoms and more cardiovas-
Table 2 Negative binomial regressions comparing A/T surgery and control group on effectiveness over time indicators (N=768)
Source Obstructive sleepapnea visits
Cerebrovascularevents visits
Pain visits ACS visits
Rate ratio (95% CI) Rate ratio (95% CI) Rate ratio (95% CI) Rate ratio (95% CI)
A/T surgery cohort over time(5 periods)
* ** NS NS
Prophylactic penicillin 0.92 2.41 17.26 (3.51–84.99)*** 14.09 (1.75–113.36)**
Hydroxyurea 3.65 (1.51–8.86)*** 1.64 7.91 (4.30–14.54)* 6.49 (2.79–15.08)*
Transfusions/year 0.91 1.09 1.34 (1.03–1.75)** 1.19
Percent of specialty care received 1.36 (1.17–1.58)* 1.76 (1.42–2.17)* 1.66 (1.43–1.92)* 1.57 (1.28–1.94)*
NS not significant
*p<0.0001; **p=0.02; ***p<0.01
Fig. 1 A/T surgery cohort com-pared over five time periods onfour effectiveness indicators(sleep apnea visits, cerebrovas-cular event visits, vaso-occlusive pain visits, and ACSvisits)
148 Ann Hematol (2011) 90:145–150

cular, hepatic, renal, spleen, and pulmonary complications.The clinical interventions used with these different sub-groups of SCD patients are consistent with the currentstandards of practice.
More of the children receiving A/T surgery (10%) wereserved in a specialty care clinic, although the control groupwith more vaso-occlusive pain and ACS may have moreimminently life-threatening symptoms. Reasons for theoverall low percentages of SCD patients being served inspecialty clinics cannot be determined from this data set,but both practitioner attitudes or knowledge and family orcultural predispositions regarding the use of health careservices play an important role in determining the level andtype of service used [17–19]. The potential for suboptimalcare in the treatment of SCD in the Medicaid system, wherethe largest percentage of African Americans are covered,has been noted previously as a critical issue in SCD carenationally [20].
The major strengths of this study are that: (1) the SCDcohort represents a large, heterogeneous group of childrenand adolescents; (2) the long-term observational studyprovides additional information regarding important clinicalcorrelates and their impact on pediatric SCD; (3) there issufficient power in the SCD cohort to detect somewhat low-incidence medical conditions; and (4) previous studies havefound that although Medicaid databases provide much less
detailed information on individuals than a structuredresearch interview, the physician diagnoses and utilizationdata are more reliable than client or family self-reports andthe administrative data correspond to clinical medicalrecords reviews in 75–95% of the cases examined [21–24]. However, these results also need to be interpreted withseveral limitations in mind: (1) the data were not gatheredusing a prospective, controlled design; (2) structuredclinical research interviews were not employed to confirmany of the assigned medical disorders; (3) these resultsprimarily report associations and, as a result, directions ofcausality cannot be inferred; (4) there is no way to estimatehow representative this Medicaid cohort is in relation tothose in other states and service systems; (5) children andadolescents with SCD who dropped out of treatment orwere periodically ineligible for Medicaid coverage are notrepresented in this data set and their outcomes may differfrom those patients who remained in Medicaid over time;and (6) no clinical data were available on these childrenprior to their Medicaid coverage.
In conclusion, the cost-effectiveness of adenoidectomyand/or tonsillectomy for treating obstructive sleep apneaand preventing cerebrovascular ischemia without increasingvaso-occlusive pain episodes or long-term acute servicecosts in routine clinical practice settings has been demon-strated. Furthermore, these results suggest that there are
Table 3 Negative binomial regressions predicting service costs (N=768)
Source Outpatient service costs Acute service costs Total service costsRate ratio (95% CI) Rate ratio (95% CI) Rate ratio (95% CI)
A/T surgery change over time * NS **
Prophylactic penicillin 1.56 (1.14–2.11)** 0.86 (0.41–1.83) 1.28 (0.75–2.19)
Hydroxyurea 2.58 (1.84–3.61)*** 4.43 (2.75–7.12)*** 4.18 (2.63–6.62)***
Transfusions/year 1.06 (0.98–1.15) 1.01 (0.92–1.11) 1.17 (1.06–1.29)*
Percent of specialty care received 1.01 (0.94–1.08) 1.10 (1.00–1.23) 1.09 (1.00–1.19)
*p<.0001; **p<.001; ***p=.05
Fig. 2 Mean total cost of SCDcare over time for patientsreceiving A/T surgery or not
Ann Hematol (2011) 90:145–150 149

different phenotypic subgroups of SCD patients whosesymptom and complication profiles need to be taken intoaccount for optimal care of the disease. Finally, the findingsshould inspire practitioners to continue to work with SCDchildren and their families to accept referrals and accessspecialty care when it is indicated in order to optimizeoutcomes and decrease the individual and family burden ofthe disease.
Acknowledgement Data acquisition and analysis were supported bythe Departments of Neuropsychiatry and Pediatrics, University ofSouth Carolina School of Medicine. The views expressed are those ofthe authors and do not represent those of the funding sources orofficial findings of the SC Department of Health and Human Services(Medicaid). The authors thank Carla W. Roberts M.D., AssistantProfessor, Department of Pediatrics, University of South CarolinaSchool of Medicine and Wilfried J. Karmaus M.D., MPH, Professor,Department of Epidemiology and Biostatistics, University of SouthCarolina Arnold School of Public Health for helpful suggestionsregarding study design and analyses. Drs. Tripathi, Jerrell, andStallworth have no conflicts of interest to disclose regarding thepublication of these results.
References
1. DeBaun MR, Vichinsky E (2007) Hemoglobinopathies. In Klieg-man RM, Behrman RE, Jenson HB, Stanton B (eds). Nelsontextbook of pediatrics, 18th edition. WB Saunders Elsevier,Philadelphia, PA. Available at http://www.mdconsult.com/das/book/body/143898456-9/853444084/1608/1067.html#4-u1.0-B978-1-4160-2450-7..50464-3–cesec19_8724. Accessed 17 June2009
2. Duke RL, Scott JP, Panepinto JA, Flanary VA (2006) Perioper-ative management of sickle cell disease children undergoingadenotonsillectomy. Otolaryngol Head Neck Surg 134:370–373
3. Kauf TL, Coates TD, Huazhi L, Mody-Patel N, Hartzema AG(2009) The cost of health care for children and adults with sicklecell disease. Am J Hematol 84:323–327
4. Wali YA, al Okbi H, al Abri R (2003) A comparison of twotransfusion regimens in the perioperative management of childrenwith sickle cell disease undergoing adenotonsillectomy. PediatrHematol Oncol 20:7–13
5. Buck J, Davies SC (2005) Surgery in sickle cell disease. HematolOncol Clin North Am 19:897–902
6. Kemp JS (1996) Obstructive sleep apnea and sickle cell disease(comment). J Pediatr Hematol Oncol 18:104–105
7. Heeney MM, Ware RE (2008) Hydroxyurea for children withsickle cell disease. Pediatr Clin N Am 55:483–501
8. Ajulo SO (1994) The significance of recurrent tonsillitis in sicklecell disease. Clin Otolaryngol Allied Sci 19:230–233
9. Ijaduola GT, Akinyanju OO (1987) Chronic tonsillitis, tonsillec-tomy and sickle cell crises. J Laryngol Otol 101:467–470
10. Sidman JD, Fry TL (1988) Exacerbation of sickle cell disease byobstructive sleep apnea. Arch Otolaryngol Head Neck Surg114:916–917
11. Maddern BR, Reed HT, Ohene-Frempong K, Beckerman RC(1989) Obstructive sleep apnea syndrome in sickle cell disease.Ann Otol Rhinol Laryngol 98:174–178
12. Derkay CS, Bray G, Milmoe GJ, Grundfast KM (1991)Adenotonsillectomy in children with sickle cell disease. SouthMed J 84:205–208
13. Halvorson DJ, McKie V, McKie K, Ashmore PE, Porubsky ES(1997) Sickle cell disease and tonsillectomy. Preoperative man-agement and postoperative complications. Arch Otolaryngol HeadNeck Surg 123:689–692
14. Dodd S, Bassi A, Bodger K, Williamson P (2006) A comparisonof multivariable regression models to analyze cost data. J EvalClin Pract 12:76–86
15. Lipscomb HJ, Dement JM, Silverstein B, Cameron W, Glazner JE(2009) Who is paying the bills? Health care costs for musculo-skeletal back disorders, Washington State union carpenters, 1989–2003. J Occup Environ Med 51:1185–1192
16. Steinberg MH (2005) Predicting clinical severity in sickle cellanaemia. Br J Haematol 129:465–481
17. Mvundura M, Amendah D, Kavanagh PL, Sprinz PG, Grosse SD(2009) Health care utilization and expenditures for privately andpublicly insured children with sickle cell disease in the UnitedStates. Pediatr Blood Cancer 53:642–646
18. Haywood C Jr, Beach MC, Lanzkron S, Strouse JJ, Wilson R,Park H, Witkop C, Bass EB, Segal JB (2009) A systematic reviewof barriers and interventions to improve appropriate use oftherapies for sickle cell disease. J Natl Med Assoc 101:1022–1033
19. Stevens GD, Shi L (2003) Racial and ethnic disparities in theprimary care experiences of children: a review of the literature.Med Care Res Rev 60:3–30
20. Brawley OW, Cornelius LJ, Edwards LR, Gamble VN, Green BL,Inturrisi C, James AH, Laraque D, Medez M, Montoya CJ,Poolock BH, Robinson L, Scholnik AP, Schori M (2008) NationalInstitutes of Health Consensus Development Conference state-ment: hydroxyurea treatment for sickle cell disease. Ann InternMed 148:932–938
21. Shankar SM, Arbogast PG, Mitchel E, Cooper WO, Wang WC,Griffin MR (2005) Medical care utilization and mortality in sicklecell disease: a population-based study. Am J Hematol 80:262–270
22. Grosse SD, Boulet SL, Amendah DD et al (2010) Administrativedata sets and health services research on hemoglobinopathies: areview of the literature. Am J Prev Med 38(4 Suppl):S557–S567
23. Hennessy S, Leonard CE, Freeman CP, Deo R, Newcomb C,Kimmel SE, Strom BL, Bilker WB (2010) Validation ofdiagnostic codes for outpatient-originating sudden cardiac deathand ventricular arrhythmia in Medicaid and Medicare claims data.Pharmacoepidemiol Drug Saf 19(6):555–562
24. Chibnik LB, Massarotti EM, Costenbader KH (2010) Identifica-tion and validation of lupus nephritis cases using administrativedata. Lupus 19(6):741–743
150 Ann Hematol (2011) 90:145–150