Embed Size (px)
Citation preview

Leukemia and Lymphoma, 2000, Vol. 37(1-2), pp. 65-70 Reprints available directly from the publisher Photocopying permitted by license only
0 2000 OPA (Overseas Publishers Association) N.V. Published by license under
the Hanvood Academic Publishers imprint, part of the Gordon and Breach Publishing Group.
Printed in Malaysia
Cost Analyses of Adjunct Colony Stimulating Factors for Acute Leukemia: Can They Improve Clinical Decision
Making CHARLES L. BENNETT MD$'HDab*, TAMMY J. STINSON MSa, JOSEPH H. LAVER MDC, MICHAEL R. BISHOP
MD , JOHN E. GODWIN MDe and MARTIN S. TALLMAN MDb
aChicago VA Healthcare System-Lakeside Division, bDivision of Hematology/Oncology of Northwestern University, Chicago, IL, 'Department of Pediatrics, Division of Hematology/Oncology, Medical University of South Carolina, Charleston, SC, dSection of Oncol-
ogy/Hematology, University of Nebraska Medical Center; Omaha, NE and eL.oyola University, Maywood, IL
(ReceivedJuly 19, 1999; In final form July 29, 1999)
Colony stimulating factors reduce the duration of neutropenia following intensive chemother- apy in a variety of settings, but the advantages in the management of leukemia are inconclu- sive. The variations in clinical results and the high costs of granulocyte colony-stimulating factor (G-CSF) and granulocyte macrophage colony-stimulating factor (GM-CSF) have led to confusion over appropriate use for leukemia patients. In this paper, we reviewed published information on costs and cost-effectiveness of growth factors for childhood and adult leuke- mia patients. Medline and Healthstar databases were searched for original research articles that contain cost or cost-effectiveness analyses of G-CSF (filgrastim) and GM-SCF (sargra- mostiin) in oncology cooperative group trials. Published manuscripts and abstracts presented at national or international oncology conferences were included. The cost of adjunct treat- ment was evaluated in two studies of pediatric ALL, one study of adult AML, and two studies of AML in older adults (>55 years). The use of G-CSF for children with ALL was associated with reductions in days to ANC recovery, fewer documented infections, a shorter duration of hospitalization, and small (but not significant) additional costs. In adult AML patients, bene- fits included a shortening of the duration of neutropenia and hospital stays, a lower incidence of infection and febrile episodes, less use of antibiotics, and cost savings of $2,230 and $2,310 in two studies and an increase if $120 in the third study. This summary suggests that economic analyses can provide useful information to assist clinical decision-making. For pediatric ALL patients, this information indicates that G-CSF use is unlikely to have signifi- cant cost implications, and its use should be based on clinical considerations. In studies of adult and older adult AML patients, both GM-CSF and G-CSF have clinical benefits and can be expected to lead to a decrease in overall costs.
Keywords: leukemia, hematopoietic colony-stimulating factors, cost-effectiveness, economics
* Address correspondence and reprint requests to: Charles Bennett MD PhD, Chicago VA Health Care System-Lakeside Division, 400 E Ontario Street, Chicago, IL. 606 11. Email: [email protected].
65
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
11/
26/1
4Fo
r pe
rson
al u
se o
nly.

66 CHARLES L. BENNETT MD PHD et al.
INTRODUCTION
Prophylactic treatment with colony stimulating fac- tors (CSFs) has been shown to reduce the duration of severe neutropenia in pediatric and adult leukemia patients who receive intensive chemotherapy.[ 1-81 Neutropenia is the most significant factor predispos- ing cancer patients to infection, with the risk of infec- tion increasing with the degree and duration of neutropenia.[9] In acute leukemia treatment, infec- tious complications are common during prolonged periods of neutropenia and are a major cause of mor- bidity, mortality, and high health care costs. [3,10]
Along with reduced duration of neutropenia, some studies have shown that patients receiving adjunct CSFs have a lower incidence of infection.[ 1,4,7,8] and, in one study, increased survival.[7] For example, Rowe et a1 reported that older adult de novo AML patients receiving GM-CSF immediately following induction therapy had fewer grade 4,5 infections (9.6% vs. 36.2%, p=0.002), fewer fatal infections (5.8% vs. 23.4%, p=0.019, fewer fatal pneumonias (14.3% vs. 53.8, p=0.046), fewer deaths due to fungal infections (1.9% vs. 19.1%, p=0.006), and a median survival time of 10.6 months compared to 4.8 months for placebo patients (p=O.O48).[7,8] A decrease in infection rate was also seen in the pediatric setting. Pui et a1 found 12 documented infections in the G-CSF group of pediatric patients with ALL, in com- parison to 27 in the placebo group (p=O.O09).[4]
While clinical advantages of CSFs have been dem- onstrated for patients with AML, particularly for older patients, there remains a lack of consensus regarding the appropriate use of these agents. The substantial cost of treatment adds to this uncertainty. The cost of a 14-day course of treatment with G-CSF (5 pglkglday, NeupogenB, Amgen Inc., Thousand Oaks, CA) ranges from $2,185-$3,480, and for GM-CSF (250 pglm21day, LeukineB, Immunex C o p , Seattle, WA) ranges from $1,649-$3,103, depending on the body size of the patient.[ 111 High costs can be incurred when these agents are used in clinical situations where there is inadequate evidence of clinical efficacy. Alternatively, incremental costs can be small or there can be significant total cost sav-
ings when these agents are used in appropriate and optimized conditions. Cost and cost-effectiveness analyses of well-designed clinical trials can improve clinical decision making by providing information on whether use of a therapy will be prohibitively expen- sive or within the range of generally used treatments.
COST ANALYSES OF CSFS IN LEUKEMIA THERAPY
Methods
The published information on cost analyses of G-CSF and GM-CSF as adjunct therapy for leukemia was summarized. Medline and Healthstar databases (1992-1998) were searched for original research arti- cles that contained cost analyses of cooperative group trials of G-CSF (filgastrim) and GM-SCF (sargra- mostim) as adjunct treatment during induction che- motherapy for adult AML and pediatric ALL. Proceedings from major oncology and hematology conferences (American Society of Clinical Oncology and American Society of Hematology, 1992- present) were also reviewed. Abstracts that did not duplicate peer-reviewed publications were included in this review. The clinical outcomes (including overall duration of neutropenia, rates of infection, and dura- tion of hospitalization) for the published clinical trials corresponding to each of the economic analyses are presented in Table I. Table I1 details the type of cost analysis performed, the incremental cost of using a CSF and the percent increaseldecrease in total costs.
Growth Factors in the Pediatric ALL Setting
In the pediatric setting, the Children’s Cancer Study Group demonstrated a shorter duration of neutrope- nia, a lower incidence of infection, and shorter hospi- tal stays for patients randomized to G-CSF versus placebo following remission-induction therapy.[4] There was no significant difference in total treatment costs. The median total direct medical costs of sup- portive care were $8,768 for the G-CSF arm of the
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
11/
26/1
4Fo
r pe
rson
al u
se o
nly.

COST ANALYSES OF CSFS IN LEUKEMIA THERAPY 67
study and $8,616 for the placebo arm. A similar trial conducted by the Pediatric Oncology Group random- ized patients to receive or not receive G-CSF follow- ing induction and two cycles of maintenance therapy. This study found a decrease in days to an ANC< 500 cells/@ in the G-CSF arm during the maintenance phases of therapy, but not during induction.[l2] An analysis of costs determined total median costs during induction and two cycles of maintenance therapy to be $28,653 for the placebo arm and $34,893 in the G-CSF arm. This difference in costs was not signifi- cant. Both studies were conducted based on similar methodology. The retrospective studies included eval- uating primary data from case report forms for major resource utilization units, and imputing costs using mean and national prices for each resource unit.
Growth Factors in the Adult AML Setting
A large scale, multi-site study by the International AML Study Group (conducted in Europe and Austra- lia) of adults with de novo AML showed significant shortening of the duration of neutropenia, febrile epi- sodes, use of parenteral antibiotics and hospitalization during induction therapy for patients randomized to G-CSF versus those receiving placebo.[5] A retro- spective economic analysis of these data presented at the American Society of Hematology conference reported a cost savings of $2,230 per patient in the G-CSF arm of the study.[14] This study was con- ducted using a decision analytic model incorporating the direct medical costs of resource use for hospital- ization, antibiotics, platelet transfusions, filgastrim administration, and in-hospital physician fees.
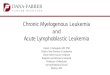
TABLE I Clinical Results of Induction Chemotherapy from Cooperative Group Trial Studies with Cost Analyses, C-SF versus Placebo
Study Growth Patients (n) Median Days #of Documented Median Days Factor of Neutropenia* Infections of Hospitalization
Pui, et al CCG Trial [4] G-CSF Children (148) 5.3 vs 12.7 (p=.007) 12 vs 27 (p=.009) 6 vs 10 ( ~ ~ 0 1 1 )
Laver, et al POG Trial [I21
Heil, et al Intl Group Trial [5]
Godwin, et a1 SWOG Trial [6]
Rowe, et a1 ECOG Trial [7]
G-CSF Children (88) 4.5 vs 4.5 ns na 9 vs 9 ns
G-CSF Adults (521) 20 vs 25 (p=.OOOl) 37% vs 36%+ ns 20 vs 25 (p=.OOOl)
G-CSF Adults >55 (211) 24 vs 27 (p=.014) 163vs141ns 29 vs 29 ns
GM-CSF Adults >55 (99) 13 vs 17 (p=.OOI) 52% vs 70%+ 36 vs 38 ns ns grade 3-5
grade 4-5 10% vs 36% (p=.002)'
*. ANC 4 0 0 cells/pl t. Percent of patients with a documented infection.
Na= not available Ns= not significant
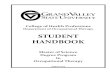
TABLE I1 Cost Analysis Information and Results for Published Cooperative Group Studies
Study Growth Factor Patients (n)
Pui, et a1 CCG G-CSF Trial 141
Trial [13]
Intl Trial [14]
SWOG [15]
ECOG ( 1 61
Pajeau, et a1 POG G-CSF
Lu, et a1 G-CSF
Bennett, et a1 G-CSF
Bennett, et a1 GM-CSF
Analysis Incremental Cost of Percent Increase/ Growth Factor Use Decrease
Retrospective cost minimization of RCT +$152 +1.8%
Retrospective cost minimization of RCT +$2,497 +17%
utilization data
utilization data
Economic model based on RCT -$2,230 na
Economic model based on RCT +$120 +0.2%
Economic model based on RCT -$2,310 -5.7%
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
11/
26/1
4Fo
r pe
rson
al u
se o
nly.

68 CHARLES L. BENNETT MD PHD et al.
Growth Factors in the Older Adult AML Setting
Among older adults (>55 years) with AML, G-CSF use was evaluated in one study and GM-CSF in a sec- ond study. The G-CSF study, conducted by the South- west Oncology Group (SWOG), found a reduction in the days of ANC 4 0 0 cells/pl and days receiving parenteral antibiotics for the G-CSF arm.[6] There were no significant differences in the number of infections or in days of hospitalization. The GM-CSF study, conducted by the Eastern Cooperative Oncol- ogy Group (ECOG), found a 72% reduction in severe infections, four fewer days with an ANC i 500 cells/pl, but no significant difference in the duration of hospitalization. [7-81
Decision analytic modeling was used to analyze the costs of GM-CSF use during induction therapy for older adult AML patients enrolled on the ECOG study.[ 161 Clinical probabilities of acquiring an infec- tion were obtained from the clinical trial data. Eco- nomic data on hospital costs per day for infected and uninfected patients were obtained from billing data from seven of the participating sites. The significant improvements in rates of severe infections were asso- ciated with an estimated $2,310 in cost savings per patient. The reduction in costs was particularly evi- dent among individuals who received two cycles of induction chemotherapy, with median total costs of $37,467 for GM-CSF patients and $59,902 for pla- cebo patients.
The same research team adapted this decision ana- lytic model to estimate the costs of G-CSF use during induction therapy for older adult patients with AML enrolled in the SWOG study.[l5] Estimates of costs per day for patients hospitalized with or without an active infection requiring parenteral antibiotics were derived from two sources: patient billing records at one of the sites and, for comparison, patient billing records from similar patients who received care on the ECOG trial. Of note, the cost estimates from the two sources were very similar, providing additional support for the generalizability of the study methods. Clinical probabilities were obtained from the clinical trial data base. The improvement in the duration of
neutropenia and antibiotic use was accompanied by a slight increase ($120) in total costs in the G-CSF arm.
DISCUSSION
In this study, we found that, in the adult setting, use of G-CSF and GM-CSF was associated with significant clinical benefits and overall cost savings. Net savings of $2,000 per patient were noted in two of three trials. Of the three National Cancer Institute adult coopera- tive cancer groups, ECOG includes CSFs as standard therapy for older adults with AML, with the use for patients less than 55 years of age as optional. SWOG takes a similar intermediate position. While, CALGB does not routinely include CSFs in any acute leuke- mia clinical trials. For pediatric leukemia patients the clinical benefits did not translate to cost savings in these studies. Accordingly, neither pediatric oncology group routinely includes CSFs as adjunctive therapy for pediatric acute leukemia patients.
Economic studies of supportive care agents, such as CSFs, encounter methodologic and statistical chal- lenges that differ from those associated with therapeu- tic modalities. Studies are routinely based on phase I11 clinical trials for various treatments and cancers, mak- ing it difficult to generalize to large numbers of clini- cal situations. Clinical trial results in these settings are often better than those seen in regular practice. One contributing factor is patient selection. Patients on clinical trials must meet specific inclusion criteria, often excluding those with comorbidities or pre-treated disease. Rigorous monitoring of dosage and adverse events that are part of a clinical trial pro- tocol may lead to increased laboratory or pharmacy costs. Conversely, lower costs may result if treatment adherence is better or monitoring results in reduced adverse events. Each of the economic analyses reviewed here was based on multi-site cooperative group clinical trials and is subject to these biases. A reader of these articles will want to carefully review inclusion criteria, patient monitoring protocols, and hospital discharge criteria to determine how well these results will carry over to the clinical setting.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
11/
26/1
4Fo
r pe
rson
al u
se o
nly.

COST ANALYSES OF CSFS IN LEUKEMIA THERAPY 69
A second consideration is that clinical trials of CSFs have short-term endpoints, primarily the dura- tion of neutropenia or incidence of infection during therapy. This may not include all of the endpoints necessary to complete a thorough economic evalua- tion and limits the analyses to comparisons of costs, rather than cost-effectiveness. The short-term out- come may also inappropriately penalize the CSF, when strict economic analyses are carried out. For example, if a CSF were to prevent delays in therapy, short-term health care costs may be greater because patients received more therapy.[ 191 If this produces a survival advantage, it may appear that the CSF arm is more costly in the short-term, while it is more cost-effective in the long-term. The studies described here focus mainly on costs of CSF use during the first cycle of induction therapy, a relatively short time frame considering the total number of cycles of che- motherapy the patients will receive and the cumula- tive nature of neutropenia.
Another methodologic consideration relates to cen- soring data if patients are dropped from study evalua- tion. Excluding patients following randomization may contribute bias to the outcomes of the economic stud- ies if patients who died incurred significantly higher or lower costs or were distributed unequally between treatment groups. When these patients are not evalu- ated, valuable information on “real world” costs can not be estimated. In the pediatric studies, all patients randomized who received study drug were included in the cost analyses. The ECOG and SWOG studies included only patients that survived induction therapy and received blinded study drug. The AML study group included all enrolled patients, the only study based on a true “intent to treat” analysis.
Statistical testing of CSF studies also presents chal- lenges. Economic data collected along side a clinical trial can be considered “stochastic”, i.e. having a mean and variance.[l9] For this type of data it is stan- dard to perform power analyses and/or sample size calculations as part of the study design and tests of significance to determine if true differences exist in the results. However, these data typically have large variances, making it difficult to demonstrate statisti- cal power for cost analyses from a study designed and
powered for clinical efficacy endpoints. Power calcu- lations in the clinical trial design of the POG study included days of hospitalization as a secondary out- come. All other studies were powered only to detect clinical differences in response rates or duration of neutropenia.
While the primary indication for the use of CSFs is clinical efficacy, economic studies provide informa- tion that is likely to be useful to physicians who are concerned with when and where to optimally use them with leukemia therapy. In reviewing these stud- ies, the reader should first consider if there is suffi- cient cause to investigate costs in the setting, then analyze the methodology and thoroughness of the study, and finally interpret the results based on their clinical setting.[20] For older AML patients, CSF use has clinical benefits that are likely to contribute to reductions in the overall costs of care. Use of CSFs in this setting should be considered, a treatment strategy that is consistent with the most recent ASCO guide- lines.[ 17,181 For pediatric ALL patients, clinical results of CSF trials have found shortened periods of neutropenia, without evidence of substantial decreases in costs. While formal ASCO guidelines for CSF use in the pediatric leukemia setting are cur- rently being developed, the available economic evi- dence indicates that cost considerations are unlikely to be an important determinant influencing this clini- cal decision.
Acknowledgements
This work was supported in part by funds from Immunex Corporation.
References Ohno R, Tomonago M, Kobayashi T, et al. Effect of granulo- cyte colony stimulating factor after intensive induction ther- apy in relapsed or refractory acute leukemia. N Engl J Med 323371 ; 1990. Buchner T, Hiddemann W, Koenigsmann M, et al. Recombi- nant human granulocyte-macrophage colony-stimulating fac- tor after chemotherapy in patients with acute myeloid leukemia at higher age or after relapse. Blood 78:1190-97; 1991. Stone RM, Berg DT, George SL, et al. Granulocyte-macroph- age colony-stimulating factor after initial chemotherapy for elderly patients with primary acute myelogenous leukemia. N Engl J Med 332: 1671-83; 1995.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
11/
26/1
4Fo
r pe
rson
al u
se o
nly.

70 CHARLES L. BENNETT MD PHD et al
4. Pui CH, Boyett JM, Hughes WT, et al. Human granulocyte colony-stimulating factor after induction chemotherapy in children with acute lymphoblastic leukemia. N Engl J Med 336:1781-87; 1997.
5. Heil G, Hoelzer D, Sanz MA, et al. A randomized dou- ble-blind, placebo-controlled, phase I11 study of filgrastim in remission induction and consolidation therapy for adults with de novo acute myeloid leukemia. Blood 90:4710-18; 1997.
6. Godwin JE, Kopecky K, Head DR, et al. A double-blind, pla- cebo-controlled trial of granulocyte colony-stimulating factor in elderly patients with previously untreated acute myeloid leukemia. A Southwest Oncology Group Study. Blood 9 1 :3607-1S ; 1998.
7. Rowe JM, Anderson JW, Mazza JJ, et al. A randomized pla- cebo-controlled phase I11 study of granulocyte-macrophage colony-stimulating factor in adult patients with acute myel- ogenous leukemia: A study of the Eastern Cooperative Oncology Group. Blood 86:457-62; 1995.
8. Rowe JM, Rubin A, Mazza JJ, et al. Incidence of infections in adult patients with acute myeloid leukemia treated with yeast-derived GM-CSF: Results of a double blind prospec- tive study by the Eastern Cooperative Oncology Group. In Acute Leukemias V, Hiddemann et al. eds. Heidelberg, Ger- many: Springer-Verlag, 1996.
9. Bodey GP, Buckley M, Sathe YS, et al. Quantitative relation- ships between circulating leukocytes and infection in patients with acute leukemia. Ann Intern Med 64:32840; 1996.
10. Mayer RJ, Davis RB, Schiffer CA, et al. Intensive post-remission chemotherapy in adults with acute myeloid leukemia. N Engl J Med 3312396-03 ; 1994.
11. Desch CE and Ozer H. Neutropenia and neoplasia: An over- view of the pharmacoeconomics of sargramostim in cancer therapy. Clin Ther 19:847-65; 1997.
12. Laver J, Amylon M, Desai S, et al. Effects of r-metHuG-CSF in an intensive treatment for T-cell leukemia and advanced stage lymphoblastic lymphoma of childhood: a Pediatric
Oncology Group pilot study. J Clin Oncol 16(2):522-526; 1998.
13. Bennett CL, Stinson TJ, Lane D, et al. A cost-analysis of filgrastim for the prevention of neutropenia in pediatric T-cell leukemia and advanced lymphoblastic leukemia: A case for prospective economic analysis in a cooperative trial. Med Ped Onc, 1999, in press.
14. Lu ZJ, Luo R, Erder H, et al. Cost impact of filgrastim as an adjunct to chemotherapy for patients with acute myeloid leu- kemia. Proceedings of the American Society of Hematology 1996; 826a.
15. Bennett CL, Hynes DM, Godwin JE, et al. Economic analy- sis of granulocyte colony-stimulating factor as adjunct ther- apy for older patients with AML: Estimates from a SWOG clinical trial. Proceedings of the American Society of Hema- tology, 1998; 2538a.
16. Bennett CL, Stinson TJ, Tallman MS, et al. Economic analy- sis of a randomized placebo-controlled phase 111 study of granulocyte macrophage colony stimulating factro in adult patients with acute myelogenous leukemia. Ann Oncol
17. The American Society of Clinical Oncology. American Soci- ety of Clinical Oncology recommendations for the use of hematopoietic growth factors: evidence based clinical prac- tice guidelines. J Clin Oncol 12: 2471- 2508, 1994.
18. The American Society of Clinical Oncology. Update of rec- ommendations for the use of hematopoietic colony stimulat- ing factors: Evidence-based clinical practice guidelines. J Clin Oncol 14: 1957- 1960; 1996.
19. Drummond MF, Menzin J, Oster G. Problems in undertaking pharmacoenomic assessments in phase I11 clinical trials: The case of colony stimulating factors. In Quality of Life and Pharmacoenomics in Clinical Trials, B Spilker ed. Phila, Pa: Lippincott-Raven Publishers, 1996.
20. Hillner BE, Smith TJ. Does a clinical trial warrant an eco- nomic analysis. J Natl Cancer Inst 90: 724-5: 1998.
10:177-82; 1999.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
itat d
e G
iron
a on
11/
26/1
4Fo
r pe
rson
al u
se o
nly.