Embed Size (px)
Citation preview

DEPARTMENT OF ORAL AND MAXILLOFACIAL
PATHOLOGY

PRESENTED BY: SOUNDARYA V III BDS
CHRONIC LEUKEMIAS

REFERENCESTextbook of Oral Pathology - Shafers
Textbook of Oral and Maxillofacial Pathology - Neville
Robbins Textbook of Pathology
Textbook of Clinical Medicine - Chugh

Textbook of Pathology-Harsh mohan
www.wikipedia.com
Google Images
Practical Haematology – Ramnik sood

INTRODUCTION Leukemias are tumors of the white blood cells(leucocytes)
Haematologic malignancies


They are classified into:
1. Chronic myeloid leukemia
2. Chronic lymphocytic leukemia

CHRONIC MYELOID LEUKEMIASynonyms: Chronic granulocytic
leukemia Chronic myelocytic leukemia
• CML is cancer of WBCs

Characterized by increased growth of predominantly myeloid cells in bone marrow
Proliferation of mature granulocytes
Myeloproliferative disease associated with
chromosomal translocation [Philadelphia chromosome]

GENETIC ABNORMALITY: Chromosomal translocation know as
philadelphia chromosome. - parts of 2 chromosomes(9th & 22nd)switch
places - As a result,part of BCRgene from
chromosome 22 is fused with ABLgene on chromosome9
RECENTLY: Abnormally ↑ tyrosinekinase activity
PATHOPHYSIOLOGY


CLINICAL FEATURES
Peak incidence - 3rd and 4th decades
Male = Female
Variant seen in children Juvenile CML
Onset is insidious

SYMPTOMS COMMON : - Anaemia - Splenomegaly - Fatigue - Weight loss - Weakness - Dyspnea - purplish spots - Rashes



MODERATELY COMMON : - Hypermetabolism - Bleeding tendencies - Malaise - Retinal haemorrhage OCCASIONAL : - Joint pain - Bone pain - Amenorrhea - Priapism - Fever



ORAL MANIFESTATION Gingival hyperplasia : most commonest feature - Primary clinical manifestation : Gingivitis
Haemorrhage Petechia Ulceration - Severe : Generalized & teeth completely
hidden - Oedematous & deep red - Bleed easily - Purpuric lesion


Gingival haemorrhage Ulceration
Noma like condition Necrosis
Rapid loosening of teeth
Osseous changes in the jaws like destruction of lamina dura & displacement of teeth
Oral melanosis

LAB DIAGNOSIS
BLOOD PICTURE
BONE MARROW EXAMINATION
CYTOCHEMISTRY
Other investigations



BLOOD PICTUREAnaemia Normocytic and Normochromic type
is seenWhite blood cells Marked leucocytosis
CML consists of 3 phases: 1. chronic 2. Accelerate 3. Blastic

CHRONIC : - Excessive proliferation of myeliod cells
ACCELERATED : - Leucocytosis associated with
thrombocytopenia and splenomegaly
BLASTIC : - Lymphoid blast crisis seen - Development of Chloroma
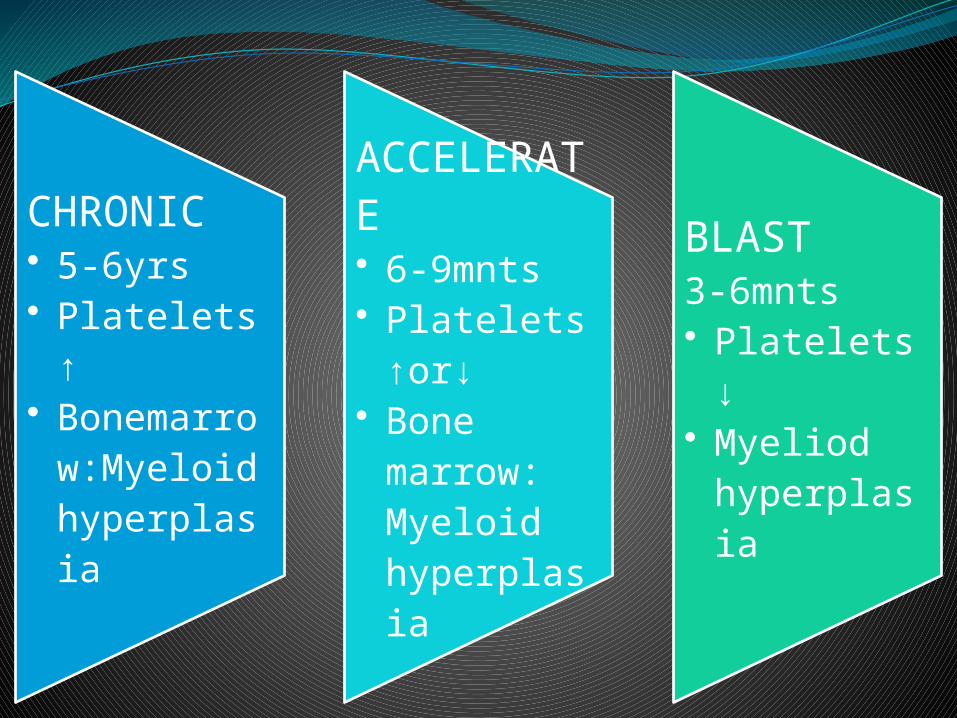
CHRONIC• 5-6yrs• Platelets ↑• Bonemarro
w:Myeloid hyperplasia
ACCELERATE• 6-9mnts• Platelets↑or
↓• Bone
marrow: Myeloid hyperplasia
BLAST3-6mnts• Platelets↓• Myeliod
hyperplasia

BONEMARROW EXAMINATION1. Hypercellularity
2. Myeloid cells Increased myeloid – erythroid ratio
3. Erythropoiesis
4. Megakaryocytes
5. Cytogenetics – philadelphia chromosome


OTHER INVESTIGATIONS Elevated serum B12
Elevated VitB12 binding capacity
Elevated serum uric acid
DIFFERENTIAL DIAGNOSIS Benign neutrophilia
Splenomegaly
Polycythaemia vera
Idiopathic myelofibrosis

TREATMENTIn past : - Antimetabolites -Alkylating agents -Steroids Treated with inhibitors of Tyrosine kinase - first – Imatinib mesylate -Nilotinib & Dasatanib
Bone marrow transplantation rarely used.

SIDE EFFECTS OF TKIs
• Nausea ,Diarrhoea• Skin rash, EdemaImatinib
• Edema, Pleural effusion
• ThrombocytopeniaDasatinib
• Myelosuppression• Hepatic impairementNilotinib

PROGNOSIS
Overall survival rate - 95.2%
Only 1% patients died of leukemia progression.

THANK YOU