Embed Size (px)
Citation preview

11
Erythropoiesis stimulating agents

22
Erythropoesis stimulating agents
Erythropoiesis-stimulating agentErythropoiesis-stimulating agent, commonly , commonly abbreviated abbreviated ESAESA, an agent similar to the cytokine , an agent similar to the cytokine (erythropoetin) that stimulates red blood cell production (erythropoetin) that stimulates red blood cell production (erythropoeisis). ESAs, structurally and biologically, are (erythropoeisis). ESAs, structurally and biologically, are similar to naturally occurring protein erythropoietin.similar to naturally occurring protein erythropoietin.Erythropoietin (Epo) Erythropoietin (Epo) Epoetin alfa (Procrit/Epogen) Epoetin alfa (Procrit/Epogen) Epoetin beta (NeoRecormon) Epoetin beta (NeoRecormon) Darbepoetin alfa (Aranesp) Darbepoetin alfa (Aranesp) Methoxy polyethylene glycol-epoetin beta (Mircera) Methoxy polyethylene glycol-epoetin beta (Mircera)

33
Background of Erythropoiesis Background of Erythropoiesis Stimulating Agents (ESAs):Stimulating Agents (ESAs):
The recombinant human erythropoetin, epoetin alfa, was The recombinant human erythropoetin, epoetin alfa, was approved by the FDA in 1993 for the treatment of anemia approved by the FDA in 1993 for the treatment of anemia associated with chemotherapy. It is a 165-amino acid associated with chemotherapy. It is a 165-amino acid hormonehormoneEpoetin alfa - manufactured by Amgen, Inc., - marketed as Epoetin alfa - manufactured by Amgen, Inc., - marketed as Procrit by Ortho Biotech, L.P., a subsidiary of J & JProcrit by Ortho Biotech, L.P., a subsidiary of J & JDarbepoetin, was created by site-directed mutagenesis and Darbepoetin, was created by site-directed mutagenesis and differs from epoetin at five amino acid positions (A30N, H32T, differs from epoetin at five amino acid positions (A30N, H32T, P87V, Y88N and P90T). This results in two additional N-P87V, Y88N and P90T). This results in two additional N-linked oligosaccharide attachments at N30 and N88.linked oligosaccharide attachments at N30 and N88.Darbepoetin - manufactured and marketed by Amgen, Inc. - Darbepoetin - manufactured and marketed by Amgen, Inc. - approved by the FDA for the treatment of anemia associated approved by the FDA for the treatment of anemia associated with chemotherapy in July of 2002.with chemotherapy in July of 2002.

44
AnemiaAnemia
An abnormally low hemoglobin or An abnormally low hemoglobin or hematocrit value -hematocrit value - multiple conditions may multiple conditions may cause anemia, including the loss of erythropoietin cause anemia, including the loss of erythropoietin due to the destruction of kidney function by chronic due to the destruction of kidney function by chronic kidney diseasekidney disease
Other conditions that may cause anemia are Other conditions that may cause anemia are generally unrelated to a deficiency of erythropoietin generally unrelated to a deficiency of erythropoietin and are exemplified by anemias due to iron and are exemplified by anemias due to iron deficiency, certain vitamin deficiencies, deficiency, certain vitamin deficiencies, hemorrhage, and various intrinsic bone marrow hemorrhage, and various intrinsic bone marrow disordersdisorders

55
Use of ESAsUse of ESAs
Generally, regardless of the cause of anemia, Generally, regardless of the cause of anemia, blood transfusions may be necessary to blood transfusions may be necessary to relieve patient symptoms and maintain life relieve patient symptoms and maintain life when the anemic condition becomes severewhen the anemic condition becomes severe
The main goal of treatment with ESAs is to The main goal of treatment with ESAs is to increase the number of red blood cells in increase the number of red blood cells in patients with the specific types of anemia that patients with the specific types of anemia that are responsive to the ESAs so that blood are responsive to the ESAs so that blood transfusions are not needed.transfusions are not needed.

66
Overview of ESA Efficacy and Overview of ESA Efficacy and Safety:Safety:
Treatment with an ESA significantly reduced the RR of blood Treatment with an ESA significantly reduced the RR of blood transfusion by 0.64; 95% CI 0.60 to 0.68, n=6,510. On transfusion by 0.64; 95% CI 0.60 to 0.68, n=6,510. On average, patients treated with ESA received one less unit of average, patients treated with ESA received one less unit of blood than the control group.blood than the control group.
Relative risk for thromboembolic complications was 1.67; 95% Relative risk for thromboembolic complications was 1.67; 95% CI 1.35 to 2.06, n=6,769.CI 1.35 to 2.06, n=6,769.
Overall survival HR was 1.08; 95% CI 0.99 to 1.18, n=8,167.Overall survival HR was 1.08; 95% CI 0.99 to 1.18, n=8,167.
““Suggestive evidence” that treatment with ESAs improves Suggestive evidence” that treatment with ESAs improves quality of life.quality of life.
All data from Bohlius et al. from the Cochrane Database of All data from Bohlius et al. from the Cochrane Database of Systematic Reviews 2006, Issue 3 which is a review of 57 Systematic Reviews 2006, Issue 3 which is a review of 57 trials with 9,353 (cancer) patients.trials with 9,353 (cancer) patients.

77
What is the Correct Hemoglobin What is the Correct Hemoglobin Target (or Range) for ESAs in Target (or Range) for ESAs in
Anemia of Chronic Renal Failure?Anemia of Chronic Renal Failure?

88
Randomized Controlled Clinical Trials Randomized Controlled Clinical Trials of Discrete Hemoglobin Targets:of Discrete Hemoglobin Targets:
““Normal Hematocrit”Normal Hematocrit”
CHOIRCHOIR
CREATECREATE

99
Normal Hematocrit StudyNormal Hematocrit Study
Goal:Goal:
Assess risks and benefits of achieving a Assess risks and benefits of achieving a “normal” hematocrit in hemodialysis patients “normal” hematocrit in hemodialysis patients with clinically evident CHF or ischemic heart with clinically evident CHF or ischemic heart diseasedisease
Conducted:Conducted:
1993 to 1996, with follow-up through 7/19971993 to 1996, with follow-up through 7/1997

1010
Normal Hematocrit Study: DesignNormal Hematocrit Study: Design– Open labelOpen label
– All subjects received Epoetin alfaAll subjects received Epoetin alfa
– 1:1 randomization to:1:1 randomization to:
low hematocrit = 30±3% (Hgb ~10±1 g/dL); orlow hematocrit = 30±3% (Hgb ~10±1 g/dL); or
“ “normal” hematocrit = 42±3% (Hgb ~14±1 normal” hematocrit = 42±3% (Hgb ~14±1 g/dL)g/dL)
– At entry, patients:At entry, patients:
clinically evident ischemic heart disease or clinically evident ischemic heart disease or CHFCHF
on hemodialysison hemodialysis
clinically stable on Epoetin alfaclinically stable on Epoetin alfa
1°1° endpoint: Time to death or non-fatal MIendpoint: Time to death or non-fatal MI

1111
Normal Hematocrit Study Results:Normal Hematocrit Study Results:– Randomization:Randomization:
n = 634 to “normal” hematocrit (42 ± 3%)n = 634 to “normal” hematocrit (42 ± 3%)
n = 631 to low hematocrit (30 ± 3%)n = 631 to low hematocrit (30 ± 3%)
– Terminated earlyTerminated early
““Our study was halted when differences in Our study was halted when differences in mortality between the groups were recognized as mortality between the groups were recognized as sufficient to make it very unlikely that sufficient to make it very unlikely that continuation of the study would reveal a benefit continuation of the study would reveal a benefit for the normal-hematocrit group and the results for the normal-hematocrit group and the results were nearing the statistical boundary of a higher were nearing the statistical boundary of a higher mortality rate in the normal hematocrit group.” mortality rate in the normal hematocrit group.”
NEJM, 1998NEJM, 1998

1212
Normal Hematocrit Study Results:Normal Hematocrit Study Results:
Mean (95% CI) Hematocrit by Study Month (NEJM, 1998)
Hem
ato
crit
(%
)
Time (months)

1313
Normal Hematocrit Study Results:Normal Hematocrit Study Results:
Death or Non-Fatal MI by Study Month (NEJM, 1998)
Probability of death or non-fatal MI
(%)
Time (months)
final log rank p = 0.01
Normal hematocrit group
Low hematocrit group

1414
Normal Hematocrit Study Results:Normal Hematocrit Study Results:Components of Primary EndpointComponents of Primary Endpoint
TargetTarget RRRR 95% CI95% CI
42% 42% (Normal Hct) (Normal Hct)
N = 634N = 634
30% 30% (Low Hct)(Low Hct)
N = 631N = 631
DeathDeath 221 (35%)221 (35%) 185 (29%)185 (29%) 1.191.19 1.01 to 1.40
Non-Non-fatal MIfatal MI 20 (3.2%)20 (3.2%) 16 (2.5%)16 (2.5%) 1.241.24 0.65 to 2.38
EitherEither 241 (38%)241 (38%) 201 (32%)201 (32%) 1.191.19 1.03 to 1.39

1515
<10
.2
10.2
to
10.
6
10.6
to
11.
6
11.6
to
12.
8
>12
.8 .
<10
.2
10.2
to
10.
6
10.6
to
11.
6
11.6
to
12.
8
>12
.8
Hgb quintile (g/dL)
0
10
20
30
40
50
60
70
80
mort
ality
(%
)
206 218 172 29 3 48 33 79 222 249
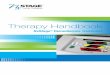
Normal Hematocrit Study:Normal Hematocrit Study:Negative Association Between Mean Hemoglobin Negative Association Between Mean Hemoglobin (throughout study) and Mortality:(throughout study) and Mortality:
Lower target Higher target
FDA analysis of data collected through 7/5/97
n=

1616
Normal Hematocrit Study Summary:Normal Hematocrit Study Summary:
Hemodialysis patients with clinically evident Hemodialysis patients with clinically evident CHF or ischemic HDCHF or ischemic HD
Targeting a hematocrit of 42 ± 3% versus Targeting a hematocrit of 42 ± 3% versus 30 ± 3% (Hgb ~14 ± 1 versus ~10 ± 1 g/dL) 30 ± 3% (Hgb ~14 ± 1 versus ~10 ± 1 g/dL) associated with increased mortality and associated with increased mortality and cardiovascular morbidity.cardiovascular morbidity.
Somewhat paradoxically, higher mean Somewhat paradoxically, higher mean hemoglobin concentrations were hemoglobin concentrations were associatedassociated withwith survival in both treatment arms. survival in both treatment arms.

1717
CHOIR Study DesignCHOIR Study Design– Open label, Epoetin alfaOpen label, Epoetin alfa
– Patients Patients
no Epoetin alfa in past 3 monthsno Epoetin alfa in past 3 months
not on dialysisnot on dialysis
hemoglobin < 11 g/dLhemoglobin < 11 g/dL
– 1:1 randomization to hemoglobin 1:1 randomization to hemoglobin 11.3 or 13.5 g/dL11.3 or 13.5 g/dL
– Primary endpoint: composite of Primary endpoint: composite of mortality, CHF hospitalization, non-fatal mortality, CHF hospitalization, non-fatal stroke, non-fatal MIstroke, non-fatal MI

1818
CHOIR Study ResultsCHOIR Study Results
– Randomization:Randomization:
715 to hemoglobin of 13.5 g/dL715 to hemoglobin of 13.5 g/dL
717 to hemoglobin of 11.3 g/dL717 to hemoglobin of 11.3 g/dL
– Terminated earlyTerminated early
““The DSMB recommended that the study be The DSMB recommended that the study be terminated in May 2005 at the time of the terminated in May 2005 at the time of the second interim analysis…because the second interim analysis…because the conditional power for demonstrating a benefit conditional power for demonstrating a benefit for the high-hemoglobin group was less than for the high-hemoglobin group was less than 5% for all plausible values of the true effect for 5% for all plausible values of the true effect for the remaining data.” NEJM, 2006the remaining data.” NEJM, 2006
DSMB = Data and Safety Monitoring Board

1919
CHOIR Study ResultsCHOIR Study Results
Mean (95% CI) Hemoglobin by Study Month (NEJM, 2006)
mea
n h
emo
glo
bin
(g
/dL
)
time (months)

2020
CHOIR Study ResultsCHOIR Study Results
Primary Composite Endpoint
Probability of
composite event
Time (months)
High hemoglobin group
Low hemoglobin group

2121
CHOIR Study Results: CHOIR Study Results: 1° Endpoint Components1° Endpoint Components
13.5 Hgb13.5 Hgb
N = 715N = 715
11.3 Hgb11.3 Hgb
N = 717N = 717
RR RR (95% CI)(95% CI)
Any Any componentcomponent
125 (17.5%)125 (17.5%) 97 (13.5%)97 (13.5%) 1.29 (1.01, 1.29 (1.01, 1.65)1.65)
DeathDeath 39 (5.5%)39 (5.5%) 26 (3.6%)26 (3.6%) 1.50 (0.93, 1.50 (0.93, 2.44)2.44)
CHF CHF hospitalizationhospitalization
59 (8.3%)59 (8.3%) 42 (5.9%)42 (5.9%) 1.41 (0.96, 1.41 (0.96, 2.06)2.06)
Non-fatal MINon-fatal MI 12 (1.7%)12 (1.7%) 13 (1.8%)13 (1.8%) 0.93 (0.43, 0.93 (0.43, 2.01)2.01)
Non-fatal Non-fatal strokestroke
12 (1.7%)12 (1.7%) 11 (1.5%)11 (1.5%) 1.09 (0.49, 1.09 (0.49, 2.46)2.46)

2222
<11
.1
11.1
to
11.
5
11.5
to
12.
1
12.1
to
13.
0
>13
.0 .
<11
.1
11.1
to
11.
5
11.5
to
12.
1
12.1
to
13.
0
>13
.0
Hgb quintile (g/dL)
0
5
10
15
mort
ality
(%
)
184 247 209 48 14 97 34 72 233 267
CHOIR Study ResultsCHOIR Study Results
Lower target Higher target
n=
FDA exploratory analysis
Negative Association Between Mean Negative Association Between Mean Hemoglobin (throughout study) and Mortality:Hemoglobin (throughout study) and Mortality:

2323
CHOIR SummaryCHOIR Summary
For pre-dialysis patients, administration of For pre-dialysis patients, administration of Epoetin alfa to target a Hgb of ~13.5 versus Epoetin alfa to target a Hgb of ~13.5 versus 11.3 g/dL is associated with increased 11.3 g/dL is associated with increased mortality and CHF hospitalization.mortality and CHF hospitalization.
Paradoxically, higher mean hemoglobin Paradoxically, higher mean hemoglobin concentrations were concentrations were associatedassociated withwith survival in both treatment arms.survival in both treatment arms.

2424
CREATE Study DesignCREATE Study Design– Open label, Epoetin betaOpen label, Epoetin beta
– PatientsPatients
mild anemia (hemoglobin 11 to 12.5 g/dL)mild anemia (hemoglobin 11 to 12.5 g/dL)
not on dialysisnot on dialysis
no prior ESAsno prior ESAs
– 1:1 randomization to normal 1:1 randomization to normal hemoglobin (13 – 15 g/dL) or hemoglobin (13 – 15 g/dL) or subnormal hemoglobin (11 – 12.5 g/dL)subnormal hemoglobin (11 – 12.5 g/dL)
– Epoetin beta begun in subnormal Epoetin beta begun in subnormal group once hemoglobin < 10.5 g/dLgroup once hemoglobin < 10.5 g/dL

2525
CREATE Study Design & ResultsCREATE Study Design & Results
– Primary composite endpoint:Primary composite endpoint: sudden sudden death, MI, acute heart failure, stroke, death, MI, acute heart failure, stroke, TIA, angina requiring hospitalization, TIA, angina requiring hospitalization, peripheral vascular disease peripheral vascular disease complication or cardiac arrhythmia complication or cardiac arrhythmia requiring hospitalizationrequiring hospitalization
– Randomization:Randomization:
301 to normal hemoglobin (13–15 g/dL)301 to normal hemoglobin (13–15 g/dL)
302 to subnormal hemoglobin (11–12.5 302 to subnormal hemoglobin (11–12.5 g/dL)g/dL)

2626
CREATE Study ResultsCREATE Study Results
Median (SD) Hemoglobin by Study MonthNEJM, 2006

2727
CREATE Study ResultsCREATE Study Results
– Primary endpoint events (NEJM, 2006):Primary endpoint events (NEJM, 2006):
- 58/301 in normal hemoglobin group- 58/301 in normal hemoglobin group
- 47/302 in sub-normal hemoglobin group- 47/302 in sub-normal hemoglobin group HR 0.78 (95% CI 0.53 – 1.12)HR 0.78 (95% CI 0.53 – 1.12)
– Few endpoint events despite broad Few endpoint events despite broad composite endpointcomposite endpoint
– Results directionally support lower Results directionally support lower hemoglobin targethemoglobin target

2828
Observational Data – 58,058 U.S. HD Patients:Observational Data – 58,058 U.S. HD Patients:
Regidor DL, Kopple JD, Kovesdy CP, et al. J Am Soc Nephrol. 2006;17:1181.
Database from DaVita, Inc.

2929
NKF K/DOQI Guidelines (2006)NKF K/DOQI Guidelines (2006)““Cohort-based observational trials and cross-Cohort-based observational trials and cross-
sectional analyses of large medical sectional analyses of large medical databases…consistently show that higher databases…consistently show that higher achieved hemoglobin values (including ≥ 12 achieved hemoglobin values (including ≥ 12 g/dL) are associated with improved patient g/dL) are associated with improved patient outcomes …. outcomes …. The failure of observational The failure of observational associations to be confirmed by associations to be confirmed by interventional trials renders use of interventional trials renders use of observational evidence unsuitable to observational evidence unsuitable to support the development of an intervention support the development of an intervention guideline statementguideline statement.”.”
www.kidney.org/professionals/KDOQI/guidelines_anemia/cpr21.htmwww.kidney.org/professionals/KDOQI/guidelines_anemia/cpr21.htm

3030
Data to Support Ideal Hemoglobin Target (1):Data to Support Ideal Hemoglobin Target (1):
8 9 10 11 12 13 14 15 16
hemoglobin concentration (g/dL)
Normal Normal hematocrithematocrit
(hemodialysis)(hemodialysis)
CHOIRCHOIR
(pre-dialysis)(pre-dialysis)
1010
1414
11.311.3
13.513.5
↓ morbidity/mortality
↑ morbidity/mortality
?
Observational data, by association only
↓ morbidity/mortality
↑ morbidity/mortality

3131
Data to Support Ideal Hemoglobin Target (2):Data to Support Ideal Hemoglobin Target (2):
Observational data from HD patientsObservational data from HD patients
Exploratory analyses of NHCT and CHOIR Exploratory analyses of NHCT and CHOIR
– associations between higher mean associations between higher mean hemoglobin concentration achieved and hemoglobin concentration achieved and survivalsurvival
Association does not prove causalityAssociation does not prove causality
Achieved hemoglobin ≠ hemoglobin target. Achieved hemoglobin ≠ hemoglobin target.
J-shape relation suggests that there is J-shape relation suggests that there is somesome Hgb concentration that is excessive in the CRF Hgb concentration that is excessive in the CRF population.population.

3232
Data to Support Ideal Hemoglobin Target (3)Data to Support Ideal Hemoglobin Target (3)
Perhaps patients who achieve higher Perhaps patients who achieve higher hemoglobin concentrations have less hemoglobin concentrations have less advanced renal disease and lower CV advanced renal disease and lower CV disease burden disease burden better outcomes. better outcomes.
We are not aware of a RCT that We are not aware of a RCT that demonstrates, in a convincing way, demonstrates, in a convincing way, that a that a higher hemoglobin target is associated higher hemoglobin target is associated with less cardiovascular morbidity and with less cardiovascular morbidity and mortality than a lower target.mortality than a lower target.

3333
Dose Optimization Challenges; Dose Optimization Challenges;
ESA ResponsivenessESA Responsiveness

3434
Dose Optimization Challenges; Dose Optimization Challenges;
ESA ResponsivenessESA Responsiveness
1. Could we prospectively identify hypo-1. Could we prospectively identify hypo-responders, at higher risk of cardiovascular responders, at higher risk of cardiovascular events?events?
2. If hypo-responders could be identified, 2. If hypo-responders could be identified, how should they be treated?how should they be treated?

3535
<10
.2
10.2
to
10.
6
10.6
to
11.
6
11.6
to
12.
8
>12
.8 .
<10
.2
10.2
to
10.
6
10.6
to
11.
6
11.6
to
12.
8
>12
.8
Hgb quintile (g/dL)
0
10
20
30
40
50
60
70
80
mort
ality
(%
)
206 218 172 29 3 48 33 79 222 249
Survival by Hemoglobin (Normal HCT Study)Survival by Hemoglobin (Normal HCT Study)
Less responsive to ESAsLess responsive to ESAs
Lower target Higher target
FDA analysis of data collected through 7/5/97
n=

3636
Survival by Mean Weight-Adjusted Epoetin Alfa Dose Survival by Mean Weight-Adjusted Epoetin Alfa Dose (Normal HCT Study)(Normal HCT Study)
time (months)
Fra
ctio
n s
urv
ivin
g
0 3 6 9 12 15 18 21 24 27 30 33 360.0
0.2
0.4
0.6
0.8
1.0
<83.5 U/kg/wk (n=252)
83.5 to 155 U/kg/wk (n=252)
155 to 252 U/kg/wk (n=251)
252 to 423 U/kg/wk (n=252)
> 423 U/kg/wk (n=252)
Dose and responsiveness are inversely rated
Highest dose; less responsive to ESAs
FDA exploratory analysis

3737
Prospective Evaluation of ESA- Prospective Evaluation of ESA- Responsiveness (Normal HCT Study) (1)Responsiveness (Normal HCT Study) (1)
FDA exploratory analysisNHCT study provided unique opportunity to assess ESA-responsiveness.Stable HD patients, maintained on Epoetin alfa; hematocrit 27 to 33% for 4 weeksSubjects randomized to “normal” hemoglobin target group had standard protocol-mandated ESA “challenge” Epoetin alfa dose increased by factor of 1.5 on study entry

3838
Prospective Evaluation of ESA- Prospective Evaluation of ESA- Responsiveness (Normal HCT Study) (2)Responsiveness (Normal HCT Study) (2)
Epoetin alfa-responsiveness calculated for patients who received constant weekly Epoetin alfa dosing for 2 to 6 weeks following study entry.
Responsiveness slope of hemoglobin-time relation throughout the 2- to 6-week period (linear regression).

3939
Prospective Evaluation of ESA- Prospective Evaluation of ESA- Responsiveness (Normal HCT Study) (3)Responsiveness (Normal HCT Study) (3)
618 patients randomized to “normal” hemoglobin target
– EPO-responsiveness could be calculated for 414:
117 patients experienced a decrease in hemoglobin, despite a 50% increase in Epoetin alfa dose
297 patients experienced no change or an increase in hemoglobin: divided in quintiles

4040
Prospective Evaluation of ESA- Prospective Evaluation of ESA- Responsiveness (Normal HCT Study) (4)Responsiveness (Normal HCT Study) (4)
Assessments:
Survival by initial Epoetin alfa-responsiveness
Overall Epoetin alfa responsiveness (mean hemoglobin concentration throughout study) by initial Epoetin alfa response

4141
Initial Epoetin Alfa Responsiveness Does Not Initial Epoetin Alfa Responsiveness Does Not Predict Subsequent Mortality in the NHCT StudyPredict Subsequent Mortality in the NHCT Study
FDA exploratory analysis
0 3 6 9 12 15 18 21 24 27 30 33 36
time (months)
0.0
0.2
0.4
0.6
0.8
1.0
fra
cti
on
su
rviv
ing
Hgb decreased (n=117)
Q1: less responsive (n=60)
Q2 (n=58)
Q3 (n=63)
Q4 (n=56)
Q5: more responsive (n=60)

4242
Initial Epoetin Alfa Responsiveness Does Not Initial Epoetin Alfa Responsiveness Does Not Predict Subsequent Mortality in the NHCT StudyPredict Subsequent Mortality in the NHCT Study
FDA exploratory analysis
0 3 6 9 12 15 18 21 24 27 30 33 36
time (months)
0.0
0.2
0.4
0.6
0.8
1.0
fra
cti
on
su
rviv
ing
Hgb decreased (n=117)
Q1: less responsive (n=60)
Q2 (n=58)
Q3 (n=63)
Q4 (n=56)
Q5: more responsive (n=60)

4343
-0.40 -0.24 -0.08 0.08 0.24
Hgb rate of change with initial 50% increase in Epo dose (g/dL/week)
8
9
10
11
12
13
14
Mea
n H
gb th
roug
hout
stu
dy (g
/dL)
Initial Epoetin Alfa Responsiveness Does Not Initial Epoetin Alfa Responsiveness Does Not Predict Overall Hgb Response in the NHCT StudyPredict Overall Hgb Response in the NHCT Study
less initial response more initial response
FDA exploratory analysis
0
Hgb rate of change with initial 50% increase in EPO dose (g/dL/week)
Mea
n H
gb
th
rou
gh
ou
t st
ud
y (g
/dL
)

4444
Could we prospectively identify hypo-responders, Could we prospectively identify hypo-responders,
at higher risk of cardiovascular events?at higher risk of cardiovascular events?
In the NHCT Study, where patients had protocol-In the NHCT Study, where patients had protocol-mandated 50% increase in EPO dose on study mandated 50% increase in EPO dose on study entry:entry:
Initial Hgb response did not predict subsequent Initial Hgb response did not predict subsequent mortality, and did not predict overall Hgb response.mortality, and did not predict overall Hgb response.
* ESA responsiveness may need to be assessed on * ESA responsiveness may need to be assessed on ongoing basis.ongoing basis.

4545
ESA-Hyporesponsiveness in a Single Patient:ESA-Hyporesponsiveness in a Single Patient:
0 16 32 48 64 80
time (weeks)
0
2
4
6
8
10
12
14
16
18
20
[hem
oglo
bin]
(g/d
L)
0
30
60
90
120
150
(Tho
usan
ds)
epoe
tin a
lfa d
ose
(uni
ts/w
eek)
[hemoglobin] g/dL
epoetin alfa dose

4646
Conclusions: Dose Optimization Challenges; Conclusions: Dose Optimization Challenges; ESA Responsiveness (1)ESA Responsiveness (1)
- Prospective identification of h- Prospective identification of hypo-responders may be difficult (i.e., erythropoietic response to an ESA challenge) - Identification of hof hypo-responders is feasible in practice

4747
Conclusions: Dose Optimization Challenges; Conclusions: Dose Optimization Challenges; ESA Responsiveness (2)ESA Responsiveness (2)
For hypo-responsive patients, the labeling suggests a search for causative factors, but does not explicitly state a maximum ESA dose, or what constitutes an adequate attempt to raise hemoglobin.
Key Unanswered Question: whether less responsive patients or those with specific risk factors would experience fewer cardiovascular events if attempts were not made to raise their hemoglobin to some “ideal” target.

4848
Dose Optimization ChallengesDose Optimization Challenges

4949
Dose Optimization ChallengesDose Optimization Challenges
ESA labeling warns against excessive ESA labeling warns against excessive rate of rise of Hgb (> 1 g/dL per 2 rate of rise of Hgb (> 1 g/dL per 2 weeks)weeks)
Is risk related to hemoglobin response?Is risk related to hemoglobin response?

5050
Dose Optimization Challenges: Dose Optimization Challenges: Cycling in a Subject from the Normal Hematocrit StudyCycling in a Subject from the Normal Hematocrit Study

5151
Dose Optimization Challenges: Dose Optimization Challenges: Cycling in a Subject from the Normal Hematocrit StudyCycling in a Subject from the Normal Hematocrit Study

5252
Dose Optimization Challenges: Dose Optimization Challenges: Cycling in a Subject from the Normal Hematocrit StudyCycling in a Subject from the Normal Hematocrit Study
Week 50, hemoglobin 9.9, rate of change 0.6 g/dL/week
Week 49, hemoglobin
9.3

5353
Normal Hematocrit Study:Normal Hematocrit Study:“Dynamic” Analysis of Relations Between Serious “Dynamic” Analysis of Relations Between Serious
Cardiovascular Events, Prevailing Hemoglobin, and Cardiovascular Events, Prevailing Hemoglobin, and Preceding Hemoglobin Rate of ChangePreceding Hemoglobin Rate of Change
Hemoglobin rate of change
(g/dL/wk) [Hem
oglobin
]
(g/d
L)
serious CV
events/ patient-
yr
FDA Analysis

5454
Dose Optimization ChallengesDose Optimization Challenges
ESA labeling warns against excessive ESA labeling warns against excessive rate of rise of Hgb (> 1 g/dL per 2 rate of rise of Hgb (> 1 g/dL per 2 weeks)weeks)
Hemoglobin oscillations are associated Hemoglobin oscillations are associated with serious cardiovascular eventswith serious cardiovascular events
– Due to underlying patient characteristics?Due to underlying patient characteristics?– Worth trying to prevent?Worth trying to prevent?

5555
Dose Optimization Challenges: Dose Optimization Challenges: Development of ESA Dosing AlgorithmsDevelopment of ESA Dosing Algorithms
most recent Hgb
<9 9.0 - 9.5 9.6 - 10.0 10.1 - 10.5 10.6 - 11.0 11.1 - 11.5 11.6 - 12.0 >12.0-0.3 +50% +50% +50% +25% +25% +25% no change hold-0.2 +50% +50% +50% +25% +25% no change no change hold-0.1 +50% +50% +50% +25% +25% no change no change hold
0 +50% +50% +50% +25% +25% no change no change hold0.1 +50% +50% +25% +25% no change no change no change hold0.2 +50% +25% +25% +25% no change no change no change hold0.3 no change no change no change no change no change -25% hold hold0.4 no change no change no change no change -25% hold hold hold0.5 hold hold hold hold hold hold hold holdR
ate
of
chan
ge/
wee
k
Limit hemoglobin oscillationsLimit hemoglobin oscillations Prevent excessive hemoglobin rates of Prevent excessive hemoglobin rates of
changechange Prevent overshootPrevent overshoot Provide appropriate means to identify and Provide appropriate means to identify and
treat hypo-responderstreat hypo-responders

5656
Review of literature and Review of literature and report of experience with report of experience with erythropoietin in ESRD erythropoietin in ESRD
populationspopulations

5757
Different Disease CategoriesDifferent Disease CategoriesESRD or dialysis patients are different from CKD patients and are ESRD or dialysis patients are different from CKD patients and are particularly different from cancer patientsparticularly different from cancer patients
– Anemia of uremia is Anemia of uremia is related torelated to the disease process ( the disease process (renal failure and insufficient renal failure and insufficient erythropoietin productionerythropoietin production) - not another therapy (i.e. chemotherapy).) - not another therapy (i.e. chemotherapy).
– Anemia of uremia is Anemia of uremia is permanentpermanent and is a and is a major contributor of symptoms and co-major contributor of symptoms and co-morbiditymorbidity..
– ESRD patients have a ESRD patients have a high incidence of cardiovascular diseasehigh incidence of cardiovascular disease (for the most part (for the most part medial atherosclerosis) which is medial atherosclerosis) which is related in large part to anemiarelated in large part to anemia..
– ESRD patients are ESRD patients are not on chemotherapeutic agentsnot on chemotherapeutic agents (less than 1% of ESRD patients (less than 1% of ESRD patients being admitted for treatment of cancer in 2006).being admitted for treatment of cancer in 2006).
– ESRD patients have ESRD patients have thrombocytopenia and abnormal platelet functionthrombocytopenia and abnormal platelet function, not the , not the hypercoaguable state often found in cancer patients.hypercoaguable state often found in cancer patients.
– ESRD patients receive large doses ofESRD patients receive large doses of heparin heparin on a regular basis. on a regular basis.– Unlike CKD patients, Unlike CKD patients, hypertension and volume overload are controlledhypertension and volume overload are controlled in ESRD in ESRD
patients by dialysis.patients by dialysis.– ESRD patients ESRD patients respond differently to ESAsrespond differently to ESAs than CKD and particularly cancer than CKD and particularly cancer
patients- the dosing ranges are significantly differentpatients- the dosing ranges are significantly different
The FDA must develop separate and distinct indications, dosage The FDA must develop separate and distinct indications, dosage recommendations and warnings for erythropoietin for these recommendations and warnings for erythropoietin for these different categories of patients.different categories of patients.

5858
Dialysis Facility Ownership and Epoetin Dosing in HemodialysisPatients: A Dialysis Provider’s Perspective. American Journal of Kidney Diseases, Vol 50, No 3 (September), 2007: pp 366-370
Addendum- Parfrey et al JASN 2005 Goal = 13.5 to 14.0g/dl and achieved=13.3g/dl

5959
There may be evidence of death There may be evidence of death risk in ESRD patients at achieved risk in ESRD patients at achieved
hemoglobin values of 13.0 to hemoglobin values of 13.0 to 13.5g/dl but that information comes 13.5g/dl but that information comes
from only one of three RCTs.from only one of three RCTs.
There is There is nono scientific evidence for a scientific evidence for a safety concern at a hemoglobin safety concern at a hemoglobin
level of 12.0g/dl in ESRD patients.level of 12.0g/dl in ESRD patients.

6060
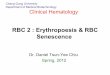
ESRD: Higher Hematocrit is Associated ESRD: Higher Hematocrit is Associated with Lower Risk of Deathwith Lower Risk of Death
1.00
1.55
1.18
0.92 0.86
0.00.2
0.40.60.8
1.01.21.4
1.61.8
<30 30-33 33-36 36-39 >39
Hematocrit (%)
Rela
tive
Risk
of D
eath
50,579 incident HD patients in the US between Jan 98 – Dec 1999Follow-up 2.5 yrs (hospitalization) and 3.0 yrs (mortality)
Li & Collins, Kid Int 2004, 65:626-633

6161
0.0
0.5
1.0
1.5
2.0
2.5
3.0
N=1,607 1,234 4,268 3,466 11,790 9,857 18,758 16,044 6,670 5,515 1,457 1,090
Hgb < 9 9<=Hgb<10 10<=Hgb<11 11<=Hgb<12 12<=Hgb<13 Hgb >13
Baseline Hemoglobin Category (g/dl)
Re
lativ
e R
isk
of
De
ath
Unadjusted
Adjusted
Reference
*
*
*
*
*
**
* *NS
* statistically significant difference from reference; 95% confidence intervals shown
The Effects of Higher Hemoglobin levels on Mortality The Effects of Higher Hemoglobin levels on Mortality and Hospitalization in Hemodialysis Patients*and Hospitalization in Hemodialysis Patients*
July 1998 to July 2000
*Ofsthun et al KI 63:1908-1914, 2003

6262
Role and timing of Transfusions in Role and timing of Transfusions in ESRD PatientsESRD Patients
– Prior to erythropoietin availability the vast majority of dialysis patients Prior to erythropoietin availability the vast majority of dialysis patients received received multiple transfusionsmultiple transfusions at varying levels of hemoglobin to at varying levels of hemoglobin to remain asymptomatic. (Average ~1u RBC/4weeks in my practice and 6-remain asymptomatic. (Average ~1u RBC/4weeks in my practice and 6-8 per year in Amgen data).8 per year in Amgen data).
– The The level level of hemoglobin at which transfusions were administered of hemoglobin at which transfusions were administered differed widely because of differed widely because of
variability of responsevariability of response to ESAs to ESAs Iron overload, risks of hepatitis, and risks of AIDS Iron overload, risks of hepatitis, and risks of AIDS caused caused reluctance to transfuse until the patients were extremely reluctance to transfuse until the patients were extremely symptomatic despite the severe CV consequences of prolonged symptomatic despite the severe CV consequences of prolonged anemia.anemia.Many ESRD patients Many ESRD patients awaiting transplantationawaiting transplantation refused (or their refused (or their physicians advocated against) RBC transfusions because of the physicians advocated against) RBC transfusions because of the problem of sensitization despite profound symptoms and problem of sensitization despite profound symptoms and worsening of heart and CNS diseaseworsening of heart and CNS disease which had severe which had severe consequences consequences afterafter “successful” renal transplantation. “successful” renal transplantation.
– Physicians did not and do not transfuse at some Physicians did not and do not transfuse at some preconceived or pre-identified hemoglobin level.preconceived or pre-identified hemoglobin level.

6363
Summary of ESAs in ESRDSummary of ESAs in ESRDESRD (Dialysis) patients are vastly different.ESRD (Dialysis) patients are vastly different.
Hemoglobin of 12.0g/dl is not scientifically Hemoglobin of 12.0g/dl is not scientifically supported as the level of adverse event concern.supported as the level of adverse event concern.
Variability of response to ESAs in ESRD patients Variability of response to ESAs in ESRD patients mandatesmandates– distinction between distinction between “target”“target” and and “achieved”“achieved”
hemoglobin in the PI.hemoglobin in the PI.– makes the concepts of modifying a dose when makes the concepts of modifying a dose when
“approaching a target” and dosing to “avoid “approaching a target” and dosing to “avoid transfusions” confusing and impracticaltransfusions” confusing and impractical..
Transfusion is a treatment - not an outcome and Transfusion is a treatment - not an outcome and it’s avoidance is poor guidance for clinicians. it’s avoidance is poor guidance for clinicians.

6464
Summary:Summary:Best RCT data available: “Ideal” Best RCT data available: “Ideal” hemoglobin target is 10 g/dL for HD hemoglobin target is 10 g/dL for HD patients; 11.3 g/dL for pre-dialysis patientspatients; 11.3 g/dL for pre-dialysis patients
Data to support a hemoglobin target as high Data to support a hemoglobin target as high as 12 g/dL are observational in nature and as 12 g/dL are observational in nature and of limited utility:of limited utility:– association ≠ causalityassociation ≠ causality– achieved hemoglobin ≠ target hemoglobinachieved hemoglobin ≠ target hemoglobin
Unknown if ESA-hyporesponsive and/or Unknown if ESA-hyporesponsive and/or high-risk patients should be treated high-risk patients should be treated differentlydifferently
Little data to show that current labeling Little data to show that current labeling addresses how best to reduce hemoglobin addresses how best to reduce hemoglobin overshoot and cyclingovershoot and cycling

6565
Potential Path ForwardPotential Path Forward
Hemoglobin target: conduct prospective, Hemoglobin target: conduct prospective, randomized, controlled cardiovascular randomized, controlled cardiovascular outcome study(ies) to determine optimum outcome study(ies) to determine optimum hemoglobin target(s)hemoglobin target(s)– Consider, Consider, a prioria priori, disparate targets , disparate targets
based on risk factor(s)based on risk factor(s)
Develop new dosing paradigm(s):Develop new dosing paradigm(s):– Special dosing strategies might be Special dosing strategies might be
considered for hypo-responsive patients considered for hypo-responsive patients and those at higher risk of CV eventsand those at higher risk of CV events
– Strategy could consider “futility”Strategy could consider “futility”
Test prospectively in RCT(s)Test prospectively in RCT(s)

6666
THANK YOU !THANK YOU !