Embed Size (px)
Citation preview
239
Late Onset Complete Flaccid Quadriplegiaafter Spinal Anaesthesia with Bupivacaine
To,The Editor, IJAMadam,
Neurological complications following spinal ana-esthesia are rare (incidence is less than 0.01%) 1. Vari-ous theories such as direct trauma, chemical irritationand toxicity of anaesthetic agent, ischemia from arterialinjury or severe hypotension and sepsis have been putforth as the etiology 2, 3. We are presenting a case oflate onset complete flaccid quadriplegia after spinalanaesthesia with bupivacaine admitted in our Neuro-ICU.
A 22-year-old female was admitted as referredcase in our institute with the chief complaint of weak-ness in all four limbs following fever for 4 days after acaesarean section. Lower section CS had been per-formed in a private hospital 15 days ago for difficultlabour. As told by patient, CS was done under spinalanaesthesia with bupivacaine, in multiple attempts. Shedeveloped moderate fever without chills and rigors af-ter 10 days of CS. Next day, she could not put herweight on her limbs. There was loss of sensations inlower limbs, felt loss of sensation of bowel and bladderand weakness in upper limbs and gradually developedbreathlessness on talking. There was no history of dif-ficulty in swallowing, backache, root pain, band likesensation on trunk, facial weakness and nasal regurgi-tation.
At the time of admission she had high grade fever(105oC) though fully conscious, dyspneic (RR- 54BPM, Rapid shallow breathing), single breath count 8/breath. Her vitals were PR- 106/m, NIBP- 110/80mmHg, SpO
2 87%. Besides weakness in all four limbs
(Hypotonia in all for limbs, Power was 3/5 in all fourlimbs, sensory level at upper thorax, superficial reflexesabsent, DTR +++, and joint position sense was ab-sent) other systemic examinations were within normal
limit. Her routine investigations and MRI Brain waswithin normal limits. MRI Cervical spine showed intramedullary signal alteration with associated cord swell-ing in the visualized cervico-dorsal cord suggestive ofmyelitis and diagnosed as a case of late onset acutetransverse myelitis. After intubation with 7.5 mm ETT,she was put on ventilator for ventilatory support andmean while 4 sessions of plasma pheresis was alsodone. During her stay in the institute she was kept oninvasive ventilation for 20 days and as her motor powerin upper limbs improved, she was shifted to non- inva-sive BiPAP (7/14). She had tolerated such pressurevery well and gradually she had improved her upperlimb motor power and ventilation power and over next25 days BiPAP was gradually decreased and removedaltogether and she was weaned to oxygen via mask,but she had not gained power in her lower limbs andbladder bowel functions. Ultimately after approximately1 and half month, she was discharged with lower limbweakness.
Acute transverse myelitis is an auto immune dis-ease and studies support that immunosuppressivetherapy is beneficial. Though the etiology of acute trans-verse myelitis is unknown in most of the cases, yet pre-ceding infection with the viral origin account for 27-37% of cases 4. Usubiaga et al have reported seriousneurological complications with an incidence of1:10,000 cases following either spinal or epidural anal-gesia 2.
Various factors have been reported as cause ofthese complications like direct trauma usually associ-ated with multiple attempts with trauma to spinal cordor nerve roots5. Hematoma can occur leading to com-pressive paraplegia. Acidic nature of some local anaes-thetic agents like chloroprocaine may directly irritatenerve roots and may also cause vasospasm. Preserva-tives used for local anaesthetic agents like alcohol, aca-cia, strychnine can further damage the spinal cord. Evensurgical gloves powder; ions of metallic syringes havealso been reported as a cause for such complications.
Correspondence : Letter to Editor
Indian Journal of Anaesthesia 2009; 53 (2):239-257 Correspondence

240
Indian Journal of Anaesthesia, April 2009
Additives like epinephrine may also induce vasospasmleading to ischemic injury or thrombosis of spinal ar-tery. Some drugs as chloroprocaine and bupivacainehave been reported to cause vasoconstriction in graviduterine vessels. Winkleman et al have reported chronicarachnoiditis in 11 patients, which was attributed to thedetergent solutions due to incomplete rinsing of the sy-ringes 6. The coincidental occurrence of paralysis fol-lowing spinal anaesthesia has been reported in case ofpreexisting neurological lesions7. Management relatedfactors-hypotension following regional anaesthesia hasbeen the most common cause of spinal cord damagedue to ischemia. Cases of spinal cord infarction due toprolonged hypotension are well reported following epi-dural anaesthesia.
Though there is no definite cause for late onsetcomplete flaccid quadriplegia in our case, yet either preexisting neurological lesion or spinal anaesthesia withbupivacaine may be the cause.
Mukul Kumar Jain, Assistant ProfessorNeuroanaesthesiology, Institute of Human Behaviour andAllied Sciences, Dilshad Garden, New DelhiEmail:[email protected]
References
1. Seigne T D. Aseptic meningitis following spinal analge-sia. Anaesthesia 1970; 25: 402-407.
2. Usubiaga J. Neurological complications following epi-dural anaesthesia. Int Anesthsiol Clin 1975; 3: 69-75.
3. Tsui BC, Armstrong K. Can direct spinal cord injuryoccur without paresthesias? A report of delayed spinalcord injury after epidural placement in an awake patient.Anesth Analg 2005; 101: 1212-14.
4. Berman M, Feldman S, Alter M, Zilber N, Kahane E.Acute transverse myelitis : incidence and etiology con-siderations. Neurology 1981; 31: 966-971.
5. Murray RR. Maternal obstetric paralysis. Am J ObstetGynaecol 1964; 88:399-403.
6. Winkleman N W. Neurological symptoms following ac-cidental intraspinal detergent injection. Neurology 1952;2: 284-91.
7. Marinacci A A, Courville CB. Electromyogram in evalu-ation of neurological complications of spinal anaesthe-sia. JAMA 1958; 168: 1337-45.
Ondansetron and Acute FulminantPulmonary Edema
To,The Editor, IJAMadam,
Life threatening hypersensitivity (allergic) reactionsto drugs and other foreign substances are observed peri-operatively . Anaesthesiologists are among few physi-cians who administer anaesthetic drugs , antibiotics ,blood products parenterally ; which can cause deathdue to anaphylaxis & associated acute cardiovascular/ pulmonary changes .We wish to share our experiencein a case of ondansetron induced anaphylaxis leadingto acute fulminant pulmonary edema.
A 52- year-old lady weighing 56 kg was postedfor cholelithiasis for open cholecystectomy with no co-existing medical illness, investigation reports within nor-mal limits. She never had any previous surgery or anymajor illness or drug allergy . She was graded as ASAII and underwent open cholecystectomy under generalanaesthesia lasting for approximately one hour . Shewas given 40mg pethidine , 110 mg propofol andvecuronium bromide 6mg .Airway was secured with7.5 mm cuffed E. T. tube & anaesthesia was main-tained with oxygen, nitrous oxide and halothane 0.5% .At the end of operation patient was reversed with 2.5mg neostigmine and 0.6 mg of glycopyrrolate . She wasalso given 75mg of diclofenace sodium for post opera-tive analgesia & as reversal was uneventful , after anhour patient was transferred to recovery ward .In theward pulse was 92/min, B.P. 130 / 80mm Hg , Resp.-16 /min , SpO
2-99% .
After an hour in ward patient felt nausea and wasgiven ondansetron 4mg intravenously ,within 5 min pa-tient felt restlessness , pulse rate , B.P. & respiratoryrate started rising along with fall in SpO
2 level .Oxygen
by face mask failed to raise SpO2 level , level of con-
sciousness deteriorated and was re- intubated and ven-tilated with 100% oxygen , she went into shock (nopalpable pulse , recordable B.P., profuse sweating ).Approximately after 10 min fine froth was noticed in
241
the endotracheal tube, there was no urticaria. Support-ive measures like IV fluid, hydrocortisone, epineph-rine, diuretics, bronchodilators were given .InitiallyIPPV failed to improve SpO
2 . ECG showed this pul-
monary edema to be of non cardiogenic in origin . Frothin E.T.tube changed from froth to continuous drippingof blood tinged fluid .Patient was shifted to ICU andput on ventilatory support with other supportive mea-sures. It took approximately 4 hrs to recover from shockand patient was taken off ventilator only after 24 hrs.
Immune system has a series of complex cellularand humoral elements that interacts with different for-eign molecules as defense against foreign substance.Another aspect of immune response is that it can re-spond inappropriately, causing hypersensitive / anaphy-lactic reactions with drugs used perioperatively, whichmay be life threatening¹.
Anaesthesiologist has to administer many drugsduring peri operative period and under anaesthesia it isvery difficult to distinguish anaphylaxis from other typeof peri- operative catastrophes. Studies suggest ap-proximately one in 2700 hospitalized patient experi-ence drug induced anaphylaxis2.
With ondansetron , following effects have beenreported during controlled clinical trials followingpareneral administration3:
• Cardiovascular: rare cases of angina, ECG alteration ,hypotension, tachycardia.
• Gastrointestinal: Constipation in 11% of cases
• Hepatic: Baseline value of aspartate transaminase(AST) and alanine transaminase (ANT) have been re-ported to exceed twice the upper limit of normal in5% of patients.
• Integumentary: Rash occurs in 1% of cases receivingondansetron.
• Neurological: Extrapyramidal reactions and grand malseizures rarely.
• Biochemical: hypokalemia rarely.
In other controlled trial4 ( n= 547 pts. n=547
placebo) after 4 mg I.V. Ondansetron following werereported : Headache14%, Dizziness 16%, Musculosk-eletal pain 11%, Drowsiness 7% , Fatigue 5%, Injec-tion site reaction 3%, Unspecified chest pain 3%, Anxi-ety/ agitation 3%, Dysuria 2%, Hypotension 2% , Fe-ver 1%, Cold sensation 1%, Pruritus 1%, Paresthesia1% . Common adverse events in Pediatric group 1month to 24 month, Pyrexia 4%, Bronchospasm 2%.Diarrhoea <1% has been reported.
Some adverse events identified and reportedvoluntarily: Arrhythmias( VT, SVT, PVC & AF) ,Bradycardia, 2nd degree heart block, palpitation andsyncope. Anaphylaxis, angioedema , bronchospasm ,cardiopulmonary arrest, hypotension , laryngeal edema, shock , shortness of breath , Hiccups, occulogyriccrisis , blurred vision has also been reported .
Although hypersensitivity / anaphylactic reactionmay occur with any drug / molecule; Ondansetron , isroutinely being used for PONV in different group of pa-tients . Reports of clinical trials and voluntary feedbackare pouring in , it needs to keep in mind that this mol-ecule can also initiate anaphylaxis with disastrous out-come. It was a case of acute fulminant pulmonary edemawhich has not been reported with ondansetron so far.
Ajit Gupta, Additional ProfessorVinod Kr Verma, Asstt. ProfessorDept of Anesthesiology & Critical Care, Indira Gandhi Instituteof Medical sciences, Patna-800014Email:[email protected]
References
1. Levy J. Anaphylactic reactions in Anesthesia and In-tensive care , Boston, Butterworths, 1986 .
2. Watkins J. Hypersensitivity response to drugs andplasma substitute used in anesthesia and surgery, InWatkins J, Salo M.(eds) , Trauma ,Stress and Immunityin anesthesia and surgery, 2p 254, London , Butterworths& co, 1982 .
3. De Witte JL , Shoenmaekers B, Sesslar DL, et al. Adverseevents>2% adults receiving ondensetron at doses 4 mgI/V in clinical trials. Anesth Analg 2001;92: 1319-1321.
4. Arcioni R, Della Rocca M , Romano R, et al. PrincipalAdverse events in comparative trials of antiemetics inadults receiving chemotherapy. Anesth Analg 2002;94:1553-1557.
Correspondence

242
Indian Journal of Anaesthesia, April 2009
Simple CPAP Method - Be Cautious of itsLimitations
To,The Editor, IJAMadam,
We read with interest the technique of CPAP bySinghal et al 1. Though it is good technique for provid-ing CPAP but its limitation must be kept in mind whileusing it and needs to be highlighted. The unmeasuredCPAP with continuous high fresh gas flow can precipi-tate the work of breathing in already compromisedCOPD patients. The partially turning the emergencyoxygen flush valve on , as done by the author also giveunquantified fresh gas flow and may generate very highpressures which may be deleterious in COPD patients.
We reemphasize the need of quantification of ‘par-tially closed APL valve’ and ‘partially turning the emer-gency oxygen flush valve on’ as mentioned by the au-thor in his CPAP method. This quantification can bedone to a certain extent by measuring the airway pres-sures during different phases of respiratory cycle. Ifolder machines are used and the modality of airwaypressure monitoring is not available, then the sphyg-momanometer (aneroid, mercury) can give a rough ideaof airway pressures. Sphygmomanometer tubing canbe connected in the breathing circuit via using three waystopcock and connecting it to the circuit via the portused for connecting capnography tubing (Arndt multiportadaptor may be used as both pressure andcapnography tubing can be connected to this connec-tor, but it is not usually available). This gives continuouspressure monitoring. Although airway pressure moni-toring may be limited via this technique because of largescale of markings but it can be of some role as a usefuladjunct to author’s CPAP technique.
Moreover the oxygen concentration being admin-istered to COPD patient is also a limitation via theauthor’s technique of CPAP. Though the authors men-tions its effective use in COPD patients, but the optionof administering and monitoring oxygen concentrationhas not been highlighted. Hence this CPAP technique
may be used only with anaesthesia machine having anoption of air / oxygen mixture and in-circuit oxygenconcentration to be titrated as per requirement of thepatient especially in COPD patient.
Rakesh Garg, Senior ResidentRavindra Pandey, Assistant ProfessorDepartment of Anaesthesiology and Intensive Care, All IndiaInstitute of Medical Sciences, Ansari Nagar, New Delhi-110029Email: [email protected]
References
1. Singhal SK. Use of simple CPAP method. Indian Journalof Anaesthesia 2008;52:600-602.
An Another Technique for EstablishingZero Reference Point for Central Venous
Pressure Monitoring
To,The Editor, IJAMadam,
Central venous pressure (CVP) is an importantclinical monitoring especially in major abdominal andvascular surgeries. Establishing the zero reference pointis important for accurate measurement. To determinethis, various simple devices such as rulers and bars havebeen described. Snow et al1 has described a transpar-ent plastic tubing (in ‘U’ shape) filled with water. Whenthe water level in one arm of U tube is at the level of theright atrium (mid-axillary line), the water level in theother arm indicates zero level of the monitoring device.We have been using this method to find out the zeroreference point for the CVP monitoring but with fewproblems.
The problem with this technique include that it wasdifficult to look at the upper level of the water columnas the water being colourless (transparent). Whilechanging the height of the table the air might get drawnin. The presence of air bubbles in the water column isdifficult to visualize and it may also change the upperlevel (Fig.1). Sometimes, the surgeons adjust the heightof the operating table frequently; we have to zero itagain. But it was difficult to visualize the upper column
243
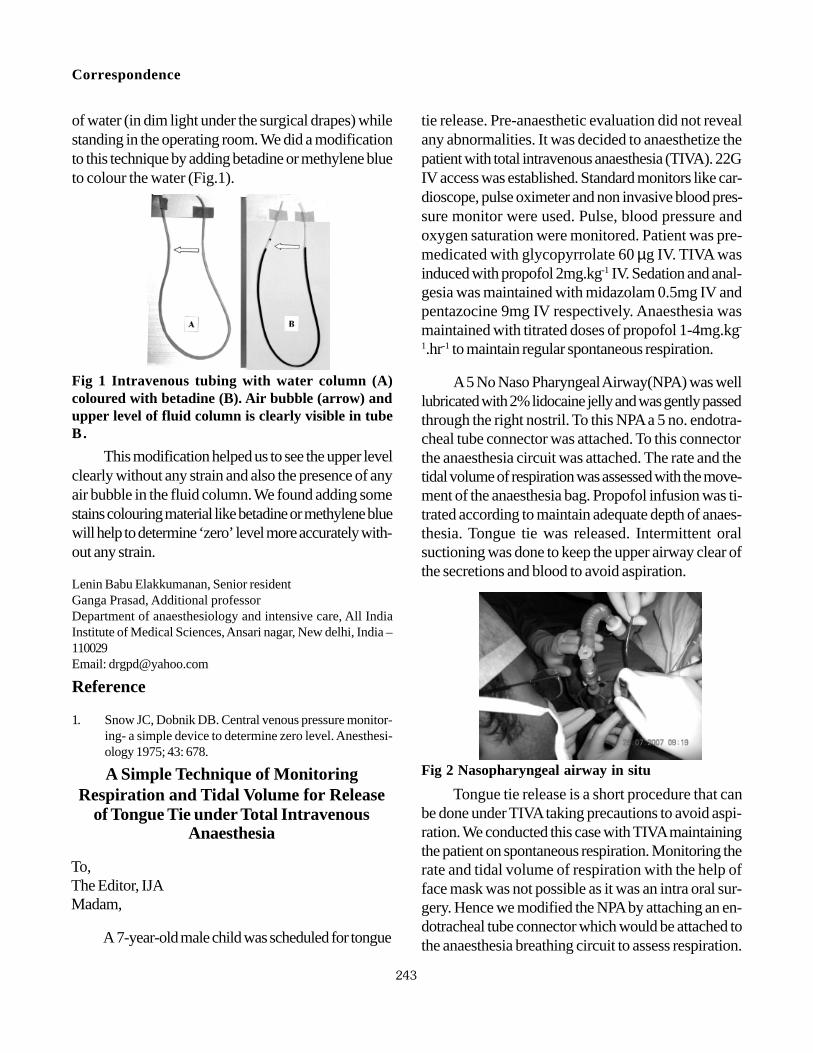
of water (in dim light under the surgical drapes) whilestanding in the operating room. We did a modificationto this technique by adding betadine or methylene blueto colour the water (Fig.1).
This modification helped us to see the upper levelclearly without any strain and also the presence of anyair bubble in the fluid column. We found adding somestains colouring material like betadine or methylene bluewill help to determine ‘zero’ level more accurately with-out any strain.
Lenin Babu Elakkumanan, Senior residentGanga Prasad, Additional professorDepartment of anaesthesiology and intensive care, All IndiaInstitute of Medical Sciences, Ansari nagar, New delhi, India –110029Email: [email protected]
Reference
1. Snow JC, Dobnik DB. Central venous pressure monitor-ing- a simple device to determine zero level. Anesthesi-ology 1975; 43: 678.
Fig 1 Intravenous tubing with water column (A)coloured with betadine (B). Air bubble (arrow) andupper level of fluid column is clearly visible in tubeB.
A Simple Technique of MonitoringRespiration and Tidal Volume for Release
of Tongue Tie under Total IntravenousAnaesthesia
To,The Editor, IJAMadam,
A 7-year-old male child was scheduled for tongue
tie release. Pre-anaesthetic evaluation did not revealany abnormalities. It was decided to anaesthetize thepatient with total intravenous anaesthesia (TIVA). 22GIV access was established. Standard monitors like car-dioscope, pulse oximeter and non invasive blood pres-sure monitor were used. Pulse, blood pressure andoxygen saturation were monitored. Patient was pre-medicated with glycopyrrolate 60 µg IV. TIVA wasinduced with propofol 2mg.kg-1 IV. Sedation and anal-gesia was maintained with midazolam 0.5mg IV andpentazocine 9mg IV respectively. Anaesthesia wasmaintained with titrated doses of propofol 1-4mg.kg-
1.hr-1 to maintain regular spontaneous respiration.
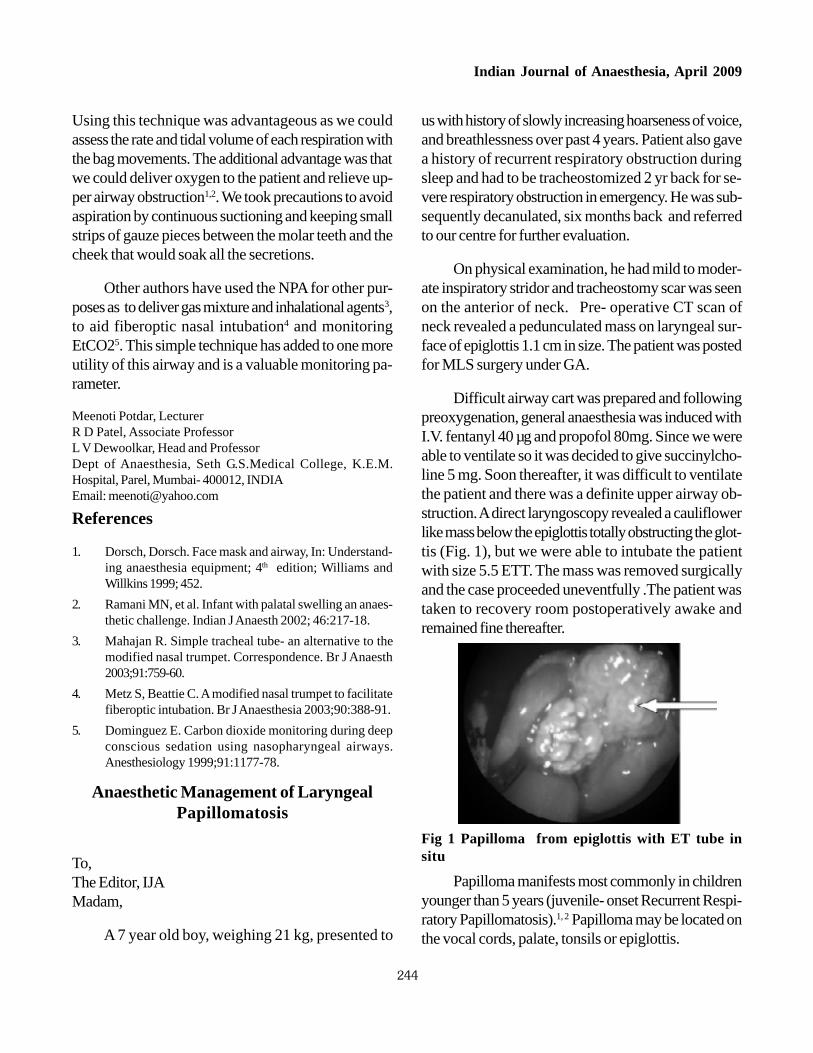
A 5 No Naso Pharyngeal Airway(NPA) was welllubricated with 2% lidocaine jelly and was gently passedthrough the right nostril. To this NPA a 5 no. endotra-cheal tube connector was attached. To this connectorthe anaesthesia circuit was attached. The rate and thetidal volume of respiration was assessed with the move-ment of the anaesthesia bag. Propofol infusion was ti-trated according to maintain adequate depth of anaes-thesia. Tongue tie was released. Intermittent oralsuctioning was done to keep the upper airway clear ofthe secretions and blood to avoid aspiration.
Fig 2 Nasopharyngeal airway in situ
Tongue tie release is a short procedure that canbe done under TIVA taking precautions to avoid aspi-ration. We conducted this case with TIVA maintainingthe patient on spontaneous respiration. Monitoring therate and tidal volume of respiration with the help offace mask was not possible as it was an intra oral sur-gery. Hence we modified the NPA by attaching an en-dotracheal tube connector which would be attached tothe anaesthesia breathing circuit to assess respiration.
Correspondence
244
Indian Journal of Anaesthesia, April 2009
Using this technique was advantageous as we couldassess the rate and tidal volume of each respiration withthe bag movements. The additional advantage was thatwe could deliver oxygen to the patient and relieve up-per airway obstruction1,2. We took precautions to avoidaspiration by continuous suctioning and keeping smallstrips of gauze pieces between the molar teeth and thecheek that would soak all the secretions.
Other authors have used the NPA for other pur-poses as to deliver gas mixture and inhalational agents3,to aid fiberoptic nasal intubation4 and monitoringEtCO25. This simple technique has added to one moreutility of this airway and is a valuable monitoring pa-rameter.
Meenoti Potdar, LecturerR D Patel, Associate ProfessorL V Dewoolkar, Head and ProfessorDept of Anaesthesia, Seth G.S.Medical College, K.E.M.Hospital, Parel, Mumbai- 400012, INDIAEmail: [email protected]
References
1. Dorsch, Dorsch. Face mask and airway, In: Understand-ing anaesthesia equipment; 4th edition; Williams andWillkins 1999; 452.
2. Ramani MN, et al. Infant with palatal swelling an anaes-thetic challenge. Indian J Anaesth 2002; 46:217-18.
3. Mahajan R. Simple tracheal tube- an alternative to themodified nasal trumpet. Correspondence. Br J Anaesth2003;91:759-60.
4. Metz S, Beattie C. A modified nasal trumpet to facilitatefiberoptic intubation. Br J Anaesthesia 2003;90:388-91.
5. Dominguez E. Carbon dioxide monitoring during deepconscious sedation using nasopharyngeal airways.Anesthesiology 1999;91:1177-78.
Anaesthetic Management of LaryngealPapillomatosis
To,The Editor, IJAMadam,
A 7 year old boy, weighing 21 kg, presented to
us with history of slowly increasing hoarseness of voice,and breathlessness over past 4 years. Patient also gavea history of recurrent respiratory obstruction duringsleep and had to be tracheostomized 2 yr back for se-vere respiratory obstruction in emergency. He was sub-sequently decanulated, six months back and referredto our centre for further evaluation.
On physical examination, he had mild to moder-ate inspiratory stridor and tracheostomy scar was seenon the anterior of neck. Pre- operative CT scan ofneck revealed a pedunculated mass on laryngeal sur-face of epiglottis 1.1 cm in size. The patient was postedfor MLS surgery under GA.
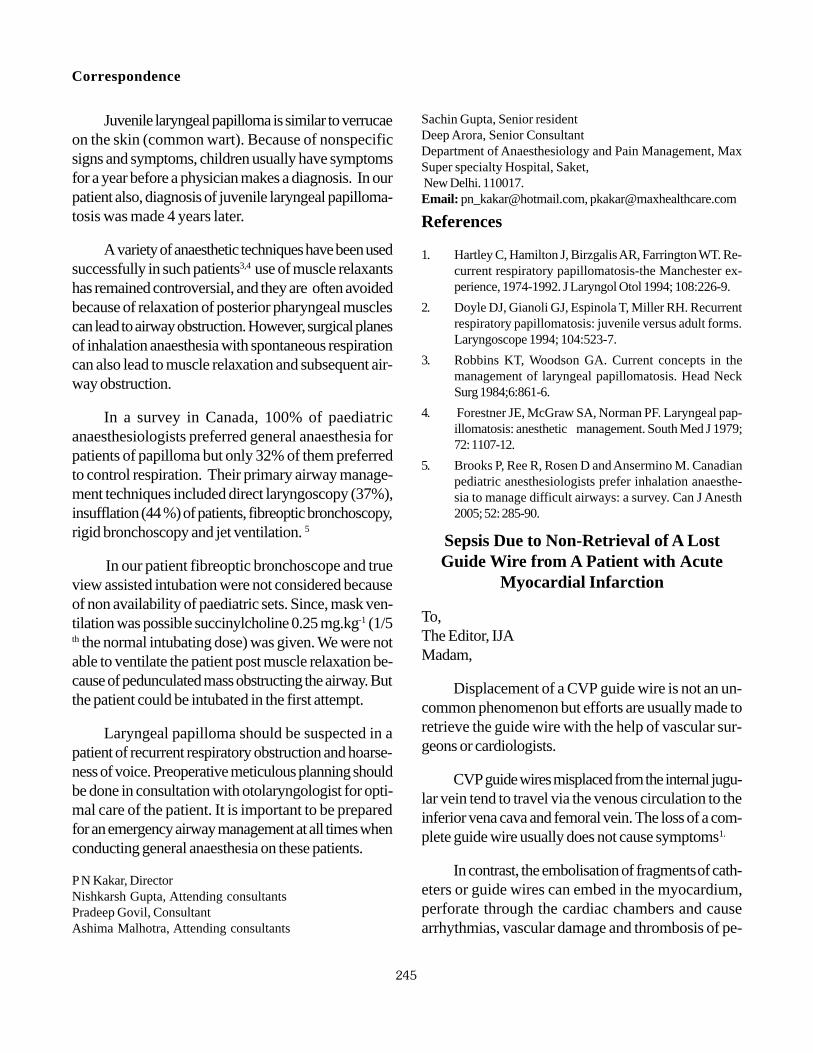
Difficult airway cart was prepared and followingpreoxygenation, general anaesthesia was induced withI.V. fentanyl 40 µg and propofol 80mg. Since we wereable to ventilate so it was decided to give succinylcho-line 5 mg. Soon thereafter, it was difficult to ventilatethe patient and there was a definite upper airway ob-struction. A direct laryngoscopy revealed a cauliflowerlike mass below the epiglottis totally obstructing the glot-tis (Fig. 1), but we were able to intubate the patientwith size 5.5 ETT. The mass was removed surgicallyand the case proceeded uneventfully .The patient wastaken to recovery room postoperatively awake andremained fine thereafter.
Fig 1 Papilloma from epiglottis with ET tube insitu
Papilloma manifests most commonly in childrenyounger than 5 years (juvenile- onset Recurrent Respi-ratory Papillomatosis).1, 2 Papilloma may be located onthe vocal cords, palate, tonsils or epiglottis.
245
Juvenile laryngeal papilloma is similar to verrucaeon the skin (common wart). Because of nonspecificsigns and symptoms, children usually have symptomsfor a year before a physician makes a diagnosis. In ourpatient also, diagnosis of juvenile laryngeal papilloma-tosis was made 4 years later.
A variety of anaesthetic techniques have been usedsuccessfully in such patients3,4 use of muscle relaxantshas remained controversial, and they are often avoidedbecause of relaxation of posterior pharyngeal musclescan lead to airway obstruction. However, surgical planesof inhalation anaesthesia with spontaneous respirationcan also lead to muscle relaxation and subsequent air-way obstruction.
In a survey in Canada, 100% of paediatricanaesthesiologists preferred general anaesthesia forpatients of papilloma but only 32% of them preferredto control respiration. Their primary airway manage-ment techniques included direct laryngoscopy (37%),insufflation (44 %) of patients, fibreoptic bronchoscopy,rigid bronchoscopy and jet ventilation. 5
In our patient fibreoptic bronchoscope and trueview assisted intubation were not considered becauseof non availability of paediatric sets. Since, mask ven-tilation was possible succinylcholine 0.25 mg.kg-1 (1/5th the normal intubating dose) was given. We were notable to ventilate the patient post muscle relaxation be-cause of pedunculated mass obstructing the airway. Butthe patient could be intubated in the first attempt.
Laryngeal papilloma should be suspected in apatient of recurrent respiratory obstruction and hoarse-ness of voice. Preoperative meticulous planning shouldbe done in consultation with otolaryngologist for opti-mal care of the patient. It is important to be preparedfor an emergency airway management at all times whenconducting general anaesthesia on these patients.
P N Kakar, DirectorNishkarsh Gupta, Attending consultantsPradeep Govil, ConsultantAshima Malhotra, Attending consultants
Sachin Gupta, Senior residentDeep Arora, Senior ConsultantDepartment of Anaesthesiology and Pain Management, MaxSuper specialty Hospital, Saket, New Delhi. 110017.Email: [email protected], [email protected]
References
1. Hartley C, Hamilton J, Birzgalis AR, Farrington WT. Re-current respiratory papillomatosis-the Manchester ex-perience, 1974-1992. J Laryngol Otol 1994; 108:226-9.
2. Doyle DJ, Gianoli GJ, Espinola T, Miller RH. Recurrentrespiratory papillomatosis: juvenile versus adult forms.Laryngoscope 1994; 104:523-7.
3. Robbins KT, Woodson GA. Current concepts in themanagement of laryngeal papillomatosis. Head NeckSurg 1984;6:861-6.
4. Forestner JE, McGraw SA, Norman PF. Laryngeal pap-illomatosis: anesthetic management. South Med J 1979;72: 1107-12.
5. Brooks P, Ree R, Rosen D and Ansermino M. Canadianpediatric anesthesiologists prefer inhalation anaesthe-sia to manage difficult airways: a survey. Can J Anesth2005; 52: 285-90.
Sepsis Due to Non-Retrieval of A LostGuide Wire from A Patient with Acute
Myocardial Infarction
To,The Editor, IJAMadam,
Displacement of a CVP guide wire is not an un-common phenomenon but efforts are usually made toretrieve the guide wire with the help of vascular sur-geons or cardiologists.
CVP guide wires misplaced from the internal jugu-lar vein tend to travel via the venous circulation to theinferior vena cava and femoral vein. The loss of a com-plete guide wire usually does not cause symptoms1.
In contrast, the embolisation of fragments of cath-eters or guide wires can embed in the myocardium,perforate through the cardiac chambers and causearrhythmias, vascular damage and thrombosis of pe-
Correspondence
246
Indian Journal of Anaesthesia, April 2009
ripheral vessels.2
We report here a case of misplaced guide wire,presumably after an internal jugular cannulation for strep-tokinase therapy in a state hospital. The guide were leftin situ, without documentation of the adverse event inthe case records. The patient was transferred to ourinstitution ten days after IJV cannulation with fever, car-diogenic shock, left ventricular failure with ecchymoticpatches all over his body.
The 2 D echography showed grade III diastolicdysfunction, severe left ventricular systolic dysfunction,LVEF 20%-25%, global hypokinesia in LAD territoryand trivial mitral regurgitation.
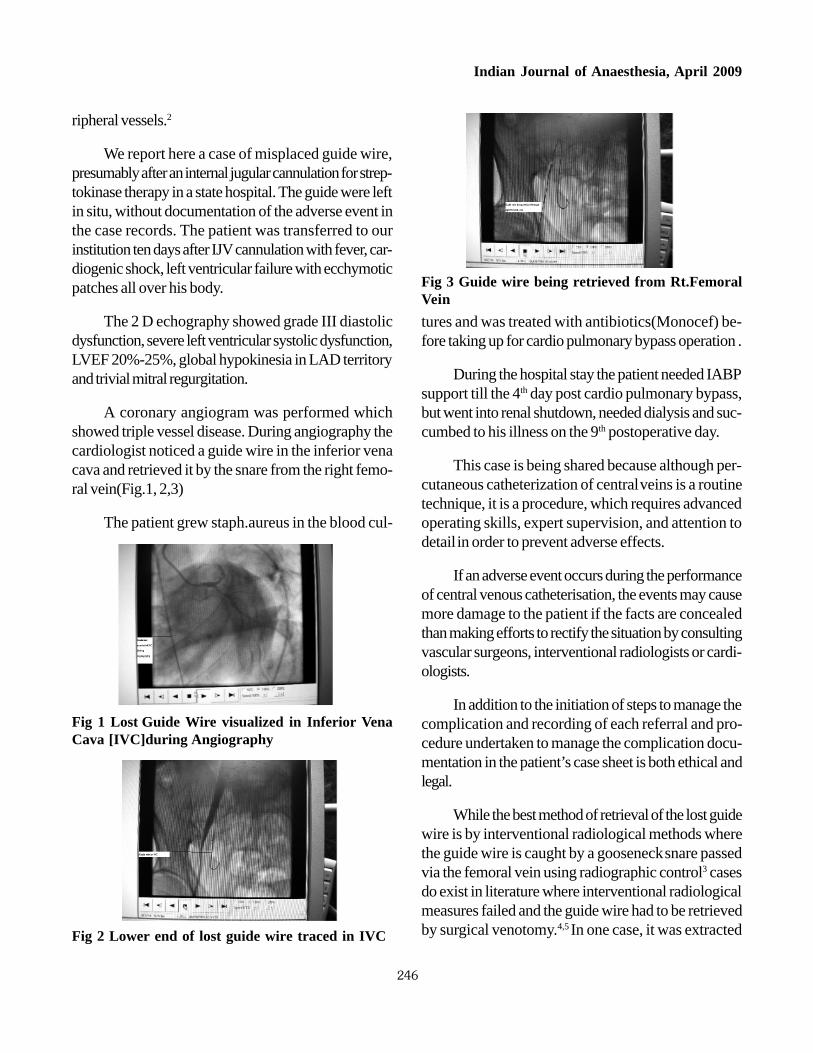
A coronary angiogram was performed whichshowed triple vessel disease. During angiography thecardiologist noticed a guide wire in the inferior venacava and retrieved it by the snare from the right femo-ral vein(Fig.1, 2,3)
The patient grew staph.aureus in the blood cul-
tures and was treated with antibiotics(Monocef) be-fore taking up for cardio pulmonary bypass operation .
During the hospital stay the patient needed IABPsupport till the 4th day post cardio pulmonary bypass,but went into renal shutdown, needed dialysis and suc-cumbed to his illness on the 9th postoperative day.
This case is being shared because although per-cutaneous catheterization of central veins is a routinetechnique, it is a procedure, which requires advancedoperating skills, expert supervision, and attention todetail in order to prevent adverse effects.
If an adverse event occurs during the performanceof central venous catheterisation, the events may causemore damage to the patient if the facts are concealedthan making efforts to rectify the situation by consultingvascular surgeons, interventional radiologists or cardi-ologists.
In addition to the initiation of steps to manage thecomplication and recording of each referral and pro-cedure undertaken to manage the complication docu-mentation in the patient’s case sheet is both ethical andlegal.
While the best method of retrieval of the lost guidewire is by interventional radiological methods wherethe guide wire is caught by a gooseneck snare passedvia the femoral vein using radiographic control3 casesdo exist in literature where interventional radiologicalmeasures failed and the guide wire had to be retrievedby surgical venotomy.4,5 In one case, it was extracted
Fig 1 Lost Guide Wire visualized in Inferior VenaCava [IVC]during Angiography
Fig 3 Guide wire being retrieved from Rt.FemoralVein
Fig 2 Lower end of lost guide wire traced in IVC

247
through the saphanous vein,4 while in the other it wasremoved through the right atrium by performing a me-dian sternotomy and placing the patient on cardiopul-monary bypass.5
During the intervention the patient needs to beheparinized.6 If heparinization is contraindicated, extrac-tion should be attempted by careful surgical explora-tion.
Sunila Sharma, Senior ConsultantJyotirmoy Das, Clinical AssociateFortis Flt.Rajan Dhall Hospital, B-1,Vasant Kunj,New-DelhiEmail:[email protected]
References
1. Santoshi A, Yasishi N, Kunihism H. Unrecognized mi-gration of an entire guide wire on insertion of centralvenous catheter into the cardiovascular system. Anes-thesiology 1996; 84:241-42.
2. Sreedhar R, Srinivas V. Guide wire complication. In:Tempe KD, editor. Selected abstracts of scientific pa-pers presented in the 6th annual conference of the IACTA;2002 Nov 8-10. Lucknow (UP). Annals Cardiac Anes-thesia 2003; 6:68-72.
3. Schummer W, Schummer C, Gaser E, Bartunek R. Lossof the guide wire: Mishap or blunder? Br J Anaesth2002; 88:144-6.
4. Kapadia S. Lost guide wire during central venous can-nulation. Indian J Surg 2006; 68:171.
5. Rai R, Lawton N, Ullah J, Banihani A, Dzumhur S. Lostguide wire during central venous cannulation and itssurgical retrieval. Case Rep Clin Pract Rev 2002; 3:139-40.
6. Kessel D, Robertson I. Interventional Radiology—ASurvival Guide. London: Churchill-Livingstone, 2000;225-9.
Avoiding Duplication of Literature
To,The Editor, IJAMadam,
I read with interest the recent article by Kiran Set al 1 on a technique to avoid backflow of blood intointravenous tubing. Same already established technique2,3 published long (almost 18 years) ago, is routinelypracticed at many centres including ours. The common
technique has also been incorporated in relevant text-books 4. The article1 presents an already described use-ful solution to a common problem; however, it lacksmentioning of original work and relevant authors as ref-erences. Though such mistakes may occur as a resultof relative inexperience or ignorance, these may at timesbe considered as unethical and inappropriate 5 and thusmandate proper care in manuscript preparation.
Madhur Mehta, Assistant ProfessorDepartment of Anaesthesiology, University College of MedicalSciences, & Guru Tegh Bahadur Hospital, Dilshad Garden,New Delhi, India.Email- [email protected]
References
1. Kiran S, Singh T. A technique to avoid backflow of bloodinto intravenous set tubing. Indian J Anaesth 2008; 52:602.
2. Brin EN, Lewis TC, Brin JA. A simple method for reduc-ing backup of blood into intravenous lines caused byinflation of a blood pressure cuff. Anesth Analg 1990;71: 569.
3. Wait CM. Blood pressure measurements and intrave-nous infusions. Anaesthesia 1992; 47: 1012.
4. Dorsch JA, Dorsch SE. Non invasive blood pressuremonitors. In Dorsch JA, Dorsch SE. eds. Understand-ing Anaesthesia Equipment. 5th ed. Philadelphia, UnitedStates of America, Lippincott Williams & Wilkins, 2008:837-844.
5. Loadsman JA, Garner HR, Drummond GB. Towards theelimination of duplication in Anaesthesia and IntensiveCare. Anaesthesia and Intensive Care 2008; 36: 643-645.
Child with Cystic Fibrosis andPyopneumothorax for Thoracotomy for
Emergency Decortication
To,The Editor, IJAMadam,
We read with great interest the Case Report byGarg et al titled “Child with Cystic Fibrosis And Pyop-neumothorax For Emergency Thoracotomy For Deco-rtication”1.
Correspondence

248
Indian Journal of Anaesthesia, April 2009
We appreciate the overall management of a com-plicated case which was done in a very nice manner.However, there are a few points that we would like tobring forth. Firstly, placement of the caudal epiduralcatheter was not followed by a test dose, which isstrongly recommended. A test dose of 0.1 ml/kg of 1%lidocaine with 1:200000 adrenaline may have beengiven2.
Secondly, since the caudal catheter was insertedonly to a distance of 7cm, in all probability the tip of thecatheter was still in the sacral canal or barely reachinglower lumbar segments. Advancing the catheter tip to alevel near or at the midpoint of the dermatomes encom-passing the surgical incision would have been preferable.This position allows a more specific site of administra-tion for both intraoperative anaesthesia and postopera-tive pain management, with the attendant advantage ofbeing able to use a lower dose of medication3.
However, by the caudal route, in patients olderthan 1 year of age, the thoracic epidural space is reachedonly in 17% of children. This may be due to lumbo-sacral curvature appearing beyond 1 year of age dueto standing and walking4. Moreover, since caudal cath-eters are at an increased risk of contamination fromfecal soiling in children, meticulous attention to dress-ing is necessary. If there is any question of contamina-tion, the catheter should be promptly removed3.
Therefore it may be preferable to place epiduralcatheters at a lumbar or thoracic interspace. Advan-tages include exclusion of insertion site from diaper area,less risk of contamination, closer proximity to desiredtip location and a lower volume of drug required for ahigh dermatome level. Lumbar and thoracic epiduralcatheters may be safely placed in anaesthetized chil-dren by experienced anaesthesiologists5.
Anand H Kulkarni, Associate Professor
Basant Bhattarai, Post-Graduate Student
Department of Anaesthesiology, Kasturba Medical College,
Lighthouse Hill Road, Mangalore- 575 001, India.
Email: [email protected]
References
1. Garg R, Kumar A, Nath MP, Shende D, BhattacharyyaR. Child with cystic fibrosis and pyopneumothorax foremergency thoracotomy for decortication. Indian Jour-nal of Anaesthesia 2008; 52: 866-869.
2. Gunter JB, Eng C. Thoracic epidural anesthesia via thecaudal approach in children. Anesthesiology 1992; 76:935-938.
3. Polaner DM, Suresh S, Cote CJ. Pediatric Regional An-esthesia. In: Cote CJ, Todres ID, Ryan JF, GoudsouzianNG, editors. A Practice of Anesthesia for Infants andChildren. 3rd Edition. Philadelphia: WB Saunders Com-pany; 2001. p. 636-674.
4. Blanco D, Llamazares J, Martinez-Mora J, Vidal F. Ana-esthesia epidural toracica por via caudal en anesthesiapediatrica: La edad es un factor limitante. Rev EspAnestesiol Reanim 1994; 41: 214-216.
5. Krane EJ, Dalens BJ, Murat I, et al. The safety ofepidurals placed during general anesthesia. Reg AnesthPain Med 1998; 23: 433-438.
Molar Intubation for Intraoral Swellings;our experience
To,The Editor, IJAMadam,
We read with great interest the case series titled“Molar intubation for intraoral swellings; our experi-ence” by Potdar et al.1 We appreciate their method ofairway management in the patients with anticipated dif-ficult airway where advanced airway equipment is notavailable.
However, we would like to make certain obser-vations. Firstly, all of the patients in the series were in-tubated orally, and had intraoral masses. Operating onthese in presence of an oral endotracheal tube may becumbersome for the surgeons. Therefore, it may bepreferable to use the nasal route for intubation wher-ever possible in such cases.
It would also be ideal to use fiberscopic intuba-tion in such patients as a primary technique since at-tempts at laryngoscopy in presence of intraoral massesmay lead to bleeding, after which fiberscopy may not

249
be possible. There was also no discussion on thebackup plan in the cases described, had there beensignificant bleeding from the masses following laryn-goscopy.
In case # 5, as shown in the photograph, if thenares are smaller than normal, a slightly smaller nasaltube may still be used. In case # 6, where there was areported deviated nasal septum, the roomier nostrilcould have been used for intubation.
Sumesh T Rao, Assistant ProfessorAnand H Kulkarni, Associate ProfessorSaneesh P J, Assistant ProfessorDepartment of Anaesthesiology, Kasturba Medical College,Lighthouse Hill Rd, Mangalore - 1.E-mail: [email protected]
References
1. Potdar M, Patel RD, Dewoolkar LV. Molar intubation forintraoral swellings; our experience. IJA 2008; 52: 861 -865.
Use of Classic Laryngeal Mask AirwayInserted in Prone Position for Controlled
Ventilation: A Feasibility Study
To,The Editor, IJAMadam,
We read with great interest recent article by VinayKumar, Lalitha K and Talib Lone titled “Use of ClassicLaryngeal Mask Airway Inserted in Prone Position forControlled Ventilation: A Feasibility Study.”1 The au-thors have done an exhaustive study but few things needto be addressed simultaneously.
Muscle relaxant (rocuronium) and controlled ven-tilation has been used previously with classic laryngealmask airway (LMA) inserted in prone position.2
There is no mention or view (fig 1) of a sparetrolley in the theatre as a safety measure to return thepatient to supine position in case of airway emergency.2
Chest compliance can decrease in prone posi-
tion3 (more with few frames).4 Therefore, mention ofairway pressures (peak and plateau) and mode of ven-tilation (pressure or volume limited) could relieve thereader’s apprehensions better.
Details of patients’ body mass index might bemore informative than body weight (maximum men-tioned 103 Kg) for ease of control ventilation inprone(less compliant) position and speculative higherairway pressures.4
Inadvertent loss of airway during any stage ofanaesthesia in prone position is life threatening. As apart of anaesthetic care plan, the anaesthesiologist musthave an algorithm to facilitate securing the airway incase of accidental extubation. The rescue options in-clude blind reinsertion, supraglottic devices (LMA, na-sopharyngeal airway and combitube), direct laryngos-copy-tracheal intubation, fiberoptic reintubation andemergency supination of the patient after covering thesurgical site.5
ProSeal LMA allows controlled ventilation withrelatively higher airway pressures, provides a better sealin different neck positions with access to the stomachand is more suitable than classic LMA for securing air-way in prone position by experienced users. 6
Ashish Bangaari, Consultant AnaesthesiologistTrevor Nair, Chief AnaesthesiologistGopika L, Junior ConsultantVikas Chawla, DNB StudentDepartment Of Anaesthesia and Critical Care, MIOT Hospitals,Mount, Poonamallee Road, Chennai, Tamil Nadu – 600089Email : [email protected]
References
1. Kumar V, Lalitha K, Lone T. Use of classic laryngealmask airway inserted in prone position for controlledventilation: A feasibility study. Indian J Anaesthesia2008; 52:813-17.
2. Weksler N, Klein M, Rozentsveig V, Weksler D, SidelnikC, Lottan M, Gurman GM. Laryngeal mask in prone po-sition: pure exhibitionism or a valid technique. MinervaAnestesiol 2007; 73:33-7.
3. Tanskanen P, Kyttä J, Randell T. The effect of patient
Correspondence

250
Indian Journal of Anaesthesia, April 2009
positioning on dynamic lung compliance. ActaAnaesthesiol Scand 1997; 41:602-6.
4. Palmon SC, Kirsch JR, Depper JA, Toung TJK. The ef-fect of the prone position on pulmonary mechanics isframe-dependent. Anesth Analg 1998;87:1175–80.
5. Kramer DC, Lo JC, Gilad R, Jenkins A 3rd. FiberopticScope as a rescue device in an anesthetized patient inthe prone position. Anesth Analg 2007; 105:890.
6. Brimacombe JR, Wenzel V, Keller C. The proseal laryn-geal mask airway in prone patients: a retrospective auditof 245 patients. Anaesth Intensive Care 2007; 35:222-5.
Correspondence
Anaesthetic Management of a Parturientwith HELLP Syndrome
To,The Editor, IJAMadam,
HELLP syndrome(Haemolysis, elevated liver en-zymes and low platelet count) is a serious complicationof severe pregnancy-induced hypertension (PIH) oc-curring in about 0.2 to 0.6 percent of all pregnancies1.A primigravida (36 weeks) with complaints of head-ache, epigastric pain, blurring of vision and difficulty inmicturition with haematuria and oliguria was admittedat Regional Institute of Medical Sciences (RIMS),Imphal. On examination, her B.P was 160/100 mm Hg;peripheral edema+3 (Fig. 1), and crepts and rhonchi
in the presence of HELLP syndrome. Because of fall-ing urinary output magnesium sulphate was suspendedand methyl dopa along with a diuretic was adminis-tered. The anaesthetic procedure was planned undersubarachnoid block after infusion of 3 units of freshfrozen plasma (FFP) along with one unit of fresh blood.A bolus dose of 100 mg hydrocortisone was given in-travenously, to be tapered in the post operative periodalong with infusion of low dose dopamine to facilitaterenal perfusion. After 2 hours of infusion of FFP, clot-ting time was reassessed and the L
3-4 level interverte-
bral space was chosen for the introduction of the Quinkeneedle (27G). A live male baby was delivered and theintraoperative course was uneventful. With proper sup-portive care, the patient was discharged after 2 weeks.
Platelet count is considered as the best indicatorof HELLP syndrome and progressive isolated thromb-ocytopenia is one of the first clues to the diagnosis.Cases with platelet count of less than 70,000/mm3 shouldnot be taken up under spinal or epidural anaesthesia 2.However, in this case, G.A was not without risk as thepatient was having productive cough, rhonchi andcrepts. It is believed that 3-4 units of FFP would raiseall the coagulation factors levels by about 20%3; and itis also considered to be the safest replacement therapyfor a patient with liver disease as it supplies all knowncoagulation factors4. Thus, in an emergency situationwith no other alternative means, compounded with thenon availability of the platelet in our establishment,3(three) units of FFP was administered. Fresh bloodwas transfused as fluid was to be restricted because ofgeneralized oedema and blood had to be replenishedsimultaneously for the loss by hemolysis. The prefer-ence of dopamine in the renal dose over diuretics wasto improve the renal perfusion in presence of oliguria,haematuria and generalized oedema. Glucocort-icosteriod increases the use of regional anesthesia inwomen with antepartum HELLP syndrome who havethrombocytopenia, particularly in those who achieve alatency of 24 hours before delivery5. Many anaesth-esiologists consider a platelet count of <100,000/uL, acontraindication to spinal or epidural placement irre-spective of etiology. Nevertheless, it may be concluded
Fig 1 Showing peripheral oedema
all over the lung fields. Preoperative investigations:-hemoglobin 9gm%, platelet count 70,000/mm3, PTT62.4 seconds, PT 19 seconds. Caesarean section wasplanned because of an alarming fetal heart rate tracing

251
that regional anaesthesia is a reasonable option in pa-tients with platelet counts of <100,000/uL as observedin a condition like the HELLP syndrome, as the mini-mum safe value is yet to be established.
N Ratan Singh, Senior RegistrarL Chaoba Singh, RegistrarS Sarat Singh, Associate ProfessorAnesthesiology Department, Regional Institute of MedicalSciences, Imphal-795004, Manipur,India,Email:[email protected]
References
1. Sibai BM. The HELLP syndrome (hemolysis, elevatedliver enzymes, and low platelets): much ado about noth-ing? Am J Obstet Gynecol 1990; 162:311-6.
2. Sharma RM, Sandhu GS, HELLP Syndrome: Report ofTwo Cases. MJAFI 2006; 62 : 373-374.
3. Doshi H. Blood & blood components therapy, Obstet-ric emergencies: Tips for practicing obstetricians, TheFederation of Obst & Gynec society of India: 17-18.
4. Handin R I. Disorders of hemostasis. In: Braunwald E,Fanei A.S, Kasper DL, Hansen SL, Longo DL andJameson JL, Editors. Harrison’s principles of InternalMedicine.15th Edition. New York: McGraw-Hill; 2001.p.755.
5. O’Brien JM, Shumate SA, Satchwell SL, Milligan DA,Barton JR. Maternal benefit of corticosteroid therapy inpatients with HELLP (hemolysis, elevated liver enzymes,and low platelet count) syndrome: impact on the rate ofregional anesthesia. Am J Obstet Gynecol. 2002 Mar;186:475-9.
Correspondence
6-Hour Positive Pressure Ventilation withSize 5 Laryngeal Mask in 55 kg Patient
To,The Editor, IJAMadam,
Laryngeal mask airway (LMA) is a preferabledevice due to its low haemodynamic responses in in-sertion and extubation.1
We report the case of an uneventful 6-hour posi-tive pressure ventilation (PPV) anaesthesia through LMAin ASA III, 55 kg, 68 year-old man undergoing infected
vascular graft excision. A size 5 classical LMA was useddue to his amputated left foot and right leg (we give aname to him: “half man”). Anaesthesia was induced withmidazolam, etomidate, remifentanil and small dose (0.2mg.kg-1) rocuronium as we experienced it provides easyinsertion. The head was elevated 30 degrees to torso toprevent regurgitation. PPV was done with volume con-trolled mode. Anaesthesia was maintained with 50-50%nitrous oxide-oxygen, sevoflurane and infusion ofremifentanil. At the second hour, nitrous oxide was cutoff and LMA cuff deflated to 30 ml from 40 ml. Theoperation was extended unexpectedly and lasted 6-hour.Ventilation with using LMA was adequate perioperatively.Perioperative cuff pressures were not measured. Patienthad no sore throat, hoarseness and dysphagia and hislaryngoscopic examination was normal at 2, 24 and 48h postoperatively.
Although there have been prolonged anaesthesiaexperiences using LMA in literature we have not met a6-hour case with PPV.2,3 By cutting off the nitrous ox-ide and 25% deflation of the cuff the mucosal traumawas tried to prevent. While we were preparing this ar-ticle my assistants asked me whether I would have usedLMA or not if I have known that the case will becontiniued for 6-hour. I thought a while and said “Iwould not”. My assistants said “We would. Because itwas comfortable”.
Erkalp Kerem, Specialist AnesthetistOzdemir Haluk, Assistant DoctorSaidoglu Leyla, Specialist Anesthetist, Chief of the DepartmentDepartment of Anesthesia and Reanimation, Vakif GurebaTraining Hospital, Istanbul, TurkeyEmail:[email protected]
References
1. Idress A, Khan FA. A comparative study of positivepressure ventilation via larygeal mask airway and en-dotracheal tube. J Pak Med Assoc 2000;50:333-8.
2. Ross B, Vater Y, Dembo G, Hunter RN C, Martay K.Larygeal mask anesthesia in children: a case report.ANAA Journal 2003;71:285-6.
3. Brimacombe J, Shorney N. The laryngeal mask airwayand prolonged balanced regional anesthesia. Can JAnesth 1993; 40: 360-4.

252
Indian Journal of Anaesthesia, April 2009
Spinal Anaesthesia for Caesarean Section inan HIV positive parturient on Anti
Retroviral Therapy
To,The Editor, IJAMadam,
A 30-year-old pregnant patient was diagnosedHIV positive at 24 weeks of gestation following whichantiretroviral therapy with Zidovudine and Ritonavirwas started. At 37 weeks of gestation, she presentedwith labor pains and leaking per vaginum and a caesar-ean section was planned. On examination, patient wasfound to be ASA grade I without any co-morbidityexcept for presence of HIV infection.
Decision to administer spinal anaesthesia for cae-sarean section was taken. Under all aseptic conditionsand with due universal precautions, subarachnoid blockwas given with 2ml of 0.5% bupivacaine (heavy). Sen-sory block up to thoracic 5 level was achieved. Intra-operative period was uneventful and special care wastaken to dispose the sharps. A healthy live baby withApgar score of 9, 9, 9 at 0,1 and 5 min after birth, wasdelivered and was started on Nevirapine syrup.
The incidence of HIV positive parturients is animportant indicator of risk transmission in the commu-nity1. Although the course of pregnancy is not influencedby HIV infection, pregnancy with its immunosuppres-sion can unmask the clinical manifestations of HIV in-fection. The risk of vertical transmission to the babydecreases from 19% in vaginal delivery to 10.4% withelective caesarean section2.
However, considerable controversy exists as towhether general or regional anaesthesia is superior insuch patients.
Despite being anaesthesia of choice in all obstet-ric cases, regional anaesthesia has been avoided in anHIV positive parturient for the fear of transmitting in-fection to CNS. This fear is unfounded and the smallamount of viremeic blood introduced into the CSF dur-
ing regional anesthesia cannot cause infection since thevirus is highly neurotropic, and has usually invaded theCNS at the time of diagnosis itself.
Avidan MS et al, in their study on HIV positiveparturient on ART concluded that caesarean sectionunder spinal anaesthesia was not associated with ahigher complication rate as compared to the controlgroup. There were no perioperative complications,change in immune function or viral load in these pa-tients3. In another retrospective study of 96 HIV posi-tive parturient of which 36 had received regional ana-esthesia, the benefits of regional anaesthesia were con-firmed4. Intra and post operative complications, liketachycardia, fever etc. were seen more with generalthan spinal anaesthesia5.
Regional anaesthesia also circumvents risk oforopharyngeal candidiasis dissemination during intuba-tion and has an advantage of not interfering with im-mune system as with general anaesthesia5. A recentBEAR Analysis for caesarean section in HIV positiveparturient has supported the use of spinal anaesthesia6.The department of Obstetric Anaesthesia Royal FreeHospital, London in its 2006 labour guidelines alsoclaims that HIV is not a contraindication to regionalanaesthesia and can be administered provided stan-dard universal precautions are taken.
In our case, we did not encounter any intra or postoperative complication. The parturient was kept underobservation and followed up after discharge for 3months.No complication of the central nervous system or anyother system was detected during this period.
Spinal anaesthesia provided safe and effectiveanaesthesia in our parturient. In such patients, the ex-tent of underlying HIV disease and the obstetrical con-dition should dictate the choice of anaesthesia ratherthan HIV status per se4,6.
Bharti Taneja, Asstt. Prof.Nitesh Goel, P.G. StudentKirti N Saxena, ProfessorAmit Kohli, Sr. ResidentPrachi Gaba, Jr.Specialist
253
Correspondence
Department of anaesthesiology and intensive care, MAMC,New Delhi.Email: [email protected]
References
1. Shmuel Evron, MD, Marek Glezerman, MD ,Ethan Harow,DO, Oscar Sadan, MD , and Tiberiu Ezri, MD. HumanImmunodeficiency Virus: Anesthetic and Obstetric Con-siderations . Anesth Analg 2004;98:503-511.
2. ACOG Committee Opinion.Scheduled cesarean deliv-ery and the prevention of vertical transmission of HIVinfection.Int J Gynaceol Obstet 1999;341:394-402.
3. Avidan MS, Groves P, Blott M, Welch J, Leung T, PozniakA, Davies E, Ball C, Zuckerman M. Low complicationrate associated with cesarean section under spinal an-esthesia for HIV-1-infected women on antiretroviraltherapy. Anesthesiology 2002;97:320-4.
4. Gershon RY, Manning-Williams D. Anesthesia and theHIV-infected parturient: A retrospective study. Interna-tional Journal of Obstetric Anesthesia 1997: 6; 76-81.
5. Parathasarathy S.,Ravishankar M.HIV and anaesthesia.Indian J Anaesth 2007;51:91-99.
6. Kotur PF. Spinal anaesthesia for LSCS in an AIDS pa-tient. Best evidence anaesthesia reports. Indian JAnaesth 2005; 49:517 – 518.
Endotracheal Tube –A Good Alternative tothe Nasopharyngeal Airway
To,The Editor, IJAMadam,
Nasal intubation is performed in surgical proce-dures involving the nasal cavity, oropharynx and theface where an oral tube would hinder the surgeon’saccess to the operative field1. Other indications includean awake or combative patient, patient with neck inju-ries, and mechanical obstruction to the orotracheal in-tubation, fractured mandible and limitation of move-ment at the temporomandibular joints2. In our hospitalwe routinely do nasal intubation for such patients andsurgeries.
Most of these patients undergoing such kinds ofsurgeries require post operative oxygenation. Oxygenis provided to them by an oxygen and face mask or a
venturi mask. However airway obstruction is a com-mon cause of post operative hypoxemia and can beinduced by a variety of drugs administered during gen-eral anaesthesia, including neuromuscular blockingdrugs3. In all patients developing airways obstruction,a patent airway must be achieved immediately (with ahead tilt chin lift, airways adjuncts, or intubation)4.
With a wired jaw, limited movement at the tem-poromandibular joint the triple manouver of head tilt,chin lift and jaw thrust is either undesirable or impos-sible. This requires introduction of a nasopharyngealairway or in extreme cases, repeat nasal intubation. Thisrepeat instrumentation often results in trauma and bleed-ing from the nasal passages. Bleeding from the nasalcavity in a post operative patient with limited access tothe airway is a highly dangerous situation.
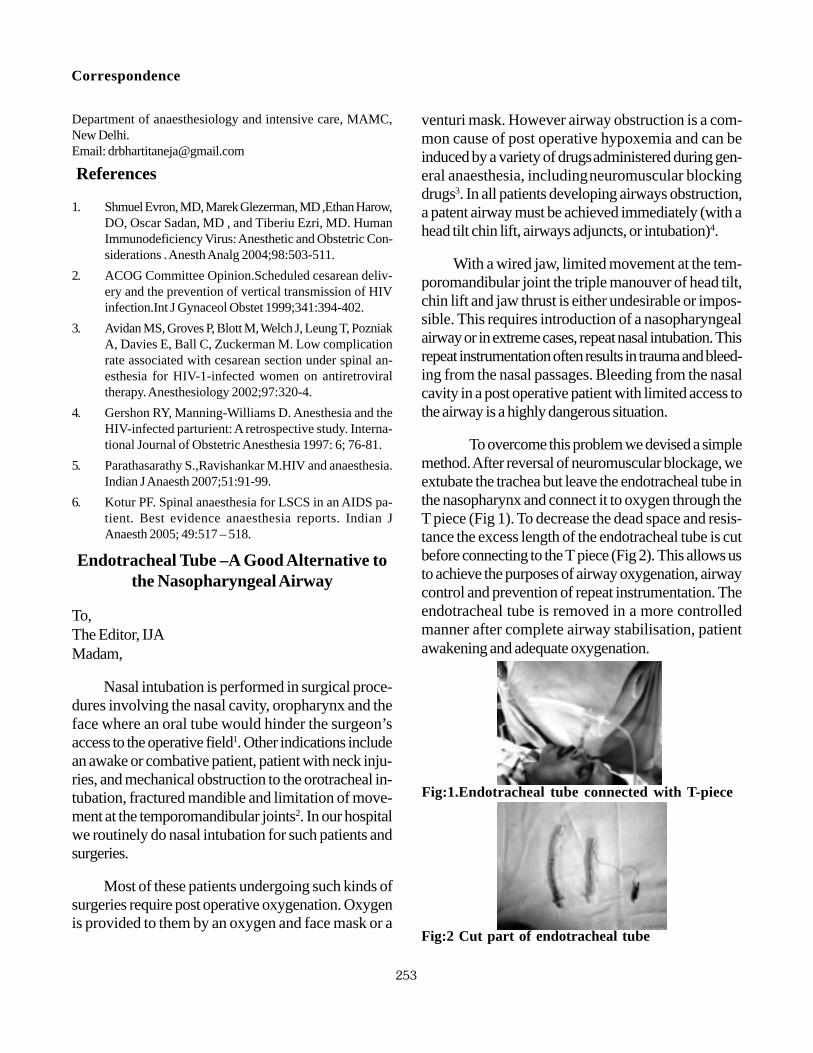
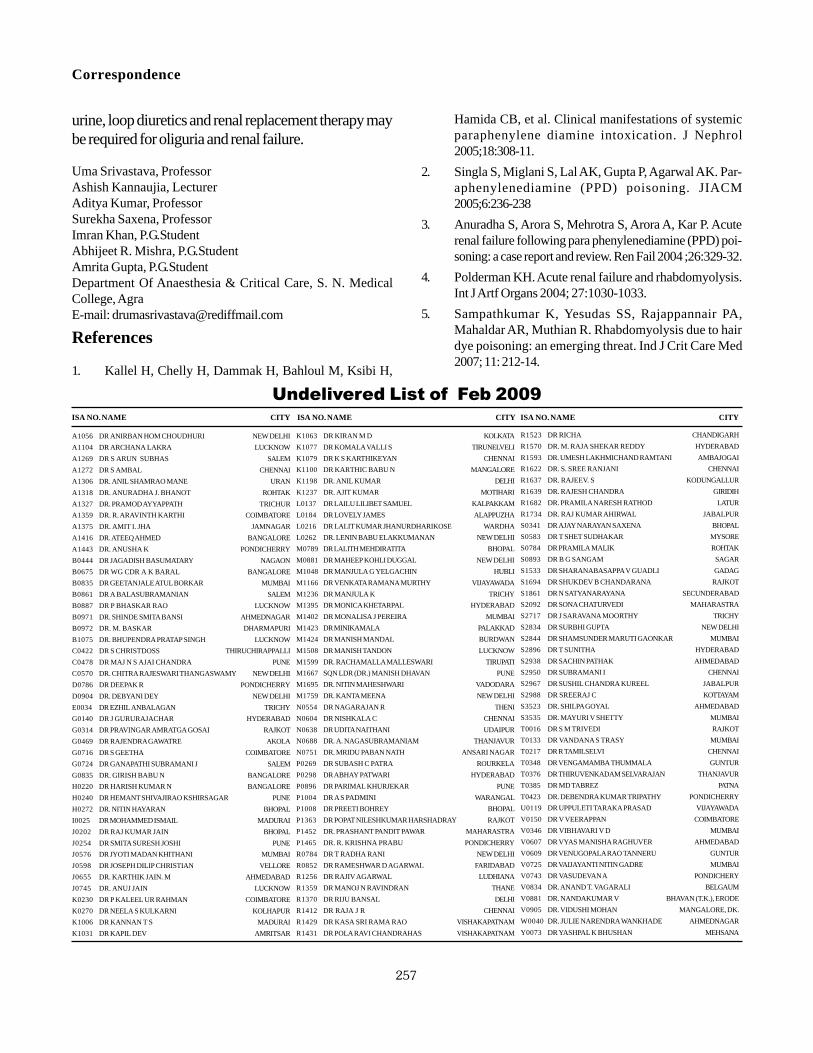
To overcome this problem we devised a simplemethod. After reversal of neuromuscular blockage, weextubate the trachea but leave the endotracheal tube inthe nasopharynx and connect it to oxygen through theT piece (Fig 1). To decrease the dead space and resis-tance the excess length of the endotracheal tube is cutbefore connecting to the T piece (Fig 2). This allows usto achieve the purposes of airway oxygenation, airwaycontrol and prevention of repeat instrumentation. Theendotracheal tube is removed in a more controlledmanner after complete airway stabilisation, patientawakening and adequate oxygenation.
Fig:2 Cut part of endotracheal tube
Fig:1.Endotracheal tube connected with T-piece

254
Indian Journal of Anaesthesia, April 2009
A Novel Use of Slide Clamp of CVPCatheter in MRI Suite
To,The Editor, IJAMadam,
Anaesthesia services in the MRI suite are increasingand require that the anaesthetic equipment is adequate toensure patient safety, is MRI compatible, and has a negli-gible effect on image quality1. Pilot balloon valve of a con-ventional endotracheal tube, pilot balloon springs of oralRAE tubes and laryngeal mask airways have been impli-cated in distortion of MRI images 1-3. A twenty four yearold male had RSA and sustained multiple injuries in-cluding flail chest. Early tracheostomy was done forairway management and initial CT head did not revealany abnormality. Patient was being managed in ICUwhen on day 7 patient had sudden cardiac arrest andwas immediately resuscitated successfully. Since thepatient did not regain consciousness, MRI brain wasplanned in addition to other investigations. The MRIsuite was equipped with an MRI compatible anaesthe-sia machine and monitor, but the portex tracheostomytube with which the patient’s trachea was intubated had
Shahbaz Ahmad, Lecturer,Deepak Malviya, Professor and Head,Department, B.R.D. Medical College, Gorakhpur (U.P.)Mohd Saif Ghaus, Specialist, Department of Anaesthesia, DrAhmad Abanamy Hospital, Riyadh, Saudi ArabiaEmail: [email protected]
References
1. Pearce A. Airway management: In DaviesNJH, CashmanJN. Lee’s Synopsis of Anaesthesia 13th Edition. ElsieverButterworth Heinemann 2005: 212.
2. Dorsch J A, Dorsch S E. Tracheal tubes. Dorsch andDorsch. Understanding anaesthesia equipment. 4th Edi-tion. Williams & Wilkins Philadelphia: USA, 1994: 587
3. Matthias H, Eikermann M, Blobner M, Groeben H, et al.Postoperative upper airway obstruction after recovery ofthe train of four ratio of the adductor pollicis muscle fromneuromuscular blockade. Anesth Analg 2006; 102: 937-942.
4. www.student.bmj.com/issues/07/04/education.studentBMJ 2007;15:133-168 April ISSN 0966-6494.
a metal spring in its one way valve (Fig 1-Arrow 1).Since, we did not have an MRI compatible tracheo-stomy tube so we occluded the inflation tube with aslide clamp of CVP catheter and cut the inflation tubeabove the clamp to remove pilot balloon valve. TheMR head was carried out uneventfully (Fig 1-Arrow2). Earlier, we have used tooth pick and roller clamp ofintravenous infusion set successfully, but we think thatthese objects can slip. Hence, we presume that effi-cacy of slide clamp in occluding the inflation tube andmaintaining the cuff inflation of TT was more reliable.After the procedure this TT was replaced with a cuffedportex TT and patient was shifted to ICU. It is recom-mended that within the 50 Gauss line only non-ferro-magnetic equipment should be used.
Jagdish Dureja, Associate Prof.Anil Thakur, Associate Prof.Nandita Kad, Associate Prof.Deptt. of Anaesthesiology & Critical Care, Pt. BD SharmaPGIMS Rohtak.Email:[email protected]
References
1. Grady RE Jr, Perkins WJ. An unexpected cause of mag-netic resonance image distortion: the endotracheal tubepilot balloon. Anesthesiology 1997; 86:993-4.
2. Crofts S, Campbell A. A source of artifact during generalanesthesia for magnetic resonance imaging. Anaesthe-sia 1993; 48:643.
3. Langston JA, Wilson I, Fell D. Use of the laryngeal maskairway during magnetic resonance imaging. Anaesthe-sia 1992; 47:532.
Fig 1 Arrow 1:Cut pilot balloon showing metalspring in its one way valve, Arrow 2:Slide clamp ofCVP catheter occluding the inflation tube andmaintaining cuff inflation.

255
tients because of high risk of aspiration.1,2 Pan et al3
analysed 19,259 deliveries and observed that only 1.2%patients required general anaesthesia out of 93.5% ofcaesarean deliveries performed under spinal anaesthe-sia. But, regional techniques are associated with 0.35to 46% incidence of inadequate analgesia4 mandatingsupplementary inhalational/intravenous/local anaesthe-sia. Ketamine (0.15-0.25mg/kg) has been successfullyused in parturients.1 In an academic survey, 76% ob-stetric anaesthesiologists suggested IV ketamine tosupplement regional blocks.5 Sen et al observed thatintravenous ketamine (0.15mg/kg) supplementation toLSCS patients provides better analgesia compared tointrathecal bupivacaine with fentanyl 10 µg. In our in-stitute, out of 698 LSCS over six months, 88% previ-ous LSCS patients (28 elective and 89 emergencyLSCS) received regional anaesthesia. Amongst these,6 patients received intraoperative general anaesthesiafor inadequate block and 2 patients were given IVketamine supplementation. While, first patient had anuneventful perioperative course. In our patient, smalldose ketamine supplementation lead to a noncommu-nicable dissociative state. She also had intraoperativenausea vomiting (IONV) inspite of antiemetic prophy-laxis. Though, our patient had also received methergineand oxytocin after the delivery of foetus, which mighthave added to the problem. However, these drugs areroutinely being administered to the parturients intraop-eratively.
Fig 1 Postoperative chest roentgenogram showinghaziness in left upper zone.
Aspiration Pneumonitis in A ParturientFollowing Intraoperative Ketamine
Analgesia
To,The Editor, IJAMadam,
A 28 years, 62 kg, 155 cm, 34+5 weeks, G3P
1,
with previous LSCS for breech, underwent electiveLSCS under spinal anaesthesia (2ml 5% bupivacainewith fentanyl 20 µg) and delivered a 2.2 kg male baby.Soon thereafter, intravenous methergine (0.2mg) andoxytocin infusion (25 units in 500ml normal saline @10units/hour) were given. Patient had fasted for eight hoursand there was no previous history of motion sickness,postoperative nausea/vomiting or any other gastrointes-tinal or respiratory disorder. She had received premedi-cation (Ranitidine 50mg and metoclopramide 10 mgIV) two hours before surgery. Ondansetron 4mg wasalso administered intraoperatively. While rectus sheathwas being closed, patient complained of incisional pain.Vitals at this moment : Pulse 68/min regular, NIBP 104/66 mmHg and level of block reconfirmed upto T4. Shewas reassured, surgical site was infiltrated (10 mlbupivacaine 0.25%) and IV ketamine 15 mg was ad-ministered. Subsequently, she vomited and became non-communicable. Fearing aspiration, rapid sequence in-tubation and thorough endotracheal suction was done.Bilateral air entry was equal and there were no creptsor ronchi. She was put on IPPV using O
2/N
2O mixture
(50:50) with halothane. ABG suggested metabolic aci-dosis {7.20, 386, 46, 18, (-) 10, 99.7% FiO
2
1}→treated with NaHCO3 75 meq IV. Repeat ABG
{7.29, 246, 40, 18.5, (-) 5, 99.8%, FiO2 0.5}. Patient
was extubated after ensuring adequate reversal of neu-romuscular blockade. ABG two hours after extubation[7.37/ 116/ 33/ 18.5/ -6/ 98.2% on FiO
2 0.35]. Post-
operative chest roentgenogram revealed haziness in leftupper zone (Fig.1). She responded to respiratory hy-giene therapy and a course of antibiotics and was dis-charged home after one week in good health.
General anaesthesia is avoided in pregnant pa-
Correspondence

256
Indian Journal of Anaesthesia, April 2009
Therefore, keeping in mind, the high incidenceof IONV during regional anesthesia ie upto 80%.5
ketamine even in lower doses is not a desirable optionduring caesarean section and need to be practiced withextreme caution.
Gyaneshwar M, P.G.StudentDavinder Grewal,Senior ResidentIndu Sen, Associate ProfessorJyotsna Wig, Professor & HeadDepartment of Anesthesia & Intensive care, ChandigarhEmail: [email protected]
References
1. Hughes SC, Levinson G, Rosen M A. Anaesthesia forcaesarean section. In: Shnider & Levinson’s Anaesthe-sia for Obstetrics, Lippincott. William & Wilkins Phila-delphia 2001.
2. Balki M, Carvelho JCA. Intraoperative nausea and vom-iting during cesarean section under regional anaesthe-sia. Int J Obs Anaesth 2004; 12: 230-41.
3. Pan PH, Bogard TD, Owen MD. Incidence and charac-teristics of failures in obstetric neuraxial analgesia andanesthesia: a retrospective analysis of 19,259 deliver-ies. Int J Obstet Anesth 2004 ;13:227-33.
4. Kinsella S M. A prospective audit of regional anaesthe-sia failure in 5080 Caesarean sections. Anaesthesia2008;63:822-832.
5. Beilin Y, Bodian CA, Haddad EM, Leibowitz AB. Prac-tice patterns of anesthesiologists regarding situationsin obstetric anesthesia where clinical management iscontroversial. Anesth Analg 1996; 83:735-41.
Rhabdomyolysis & Acute Renal Failurefollowing Hair Dye (PPD) Poisoning
To,The Editor, IJAMadam,
Paraphenylenediamine (PPD) is an industrial dyebut in some African and Asian countries it is mixed withhenna (Lawasonia alba) to dye the hair dark blackquickly1,2. We are reporting a case of suicidal hair dye(PPD) poisoning which lead to rhabdomyolysis andacute renal failure.
A young female patient aged 25 years was re-
ferred to our ICU from a nursing home following sui-cidal intake of hair dye (PPD). At the time of admissionpatients was unconscious, the pupils were semi-dilatedand sluggishly reacting to light. The pulse rate was 160/min, BP was 95/60 mmHg and respiratory rate was40/min. There was generalized swelling over face andneck with tracheostomy tube in place. The urine wasdark reddish brown in colour.
The laboratory data on admission revealed leu-kocytosis & signs of haemolysis in peripheral bloodsmear. Blood urea, creatinine, electrolytes and SGOT,SGPT were within normal range. The levels of CPKand LDH were >20,000 and 8999 IU/L respectively.Urine had traces of albumin, hemoglobinuria +++ andmyoglobin. IV fluids were started and given accordingto CVP monitoring and the patient was put on ventila-tory support. The condition of patient improved overnext few hours. But her urine output started decliningfrom 3rd day (urine output < 400 ml/24 hrs) with rise inblood urea and serum creatinine (Blood urea 87 mg/dland S. Creatinine 2.8 mg/dl). She was managed byalkalinization of urine and frusemide. The urine outputslightly increased but urea and creatinine remained el-evated. The urine output again started declining from4th day along with progressive rise in blood urea, crea-tinine and serum potassium. She died due to acute re-nal failure.
Rhabdomyolysis is a relatively rare condition, whichcan develop following toxicity due to chemicals or drugs,physical injury or infections3-5. The commonest clinicalmanifestations of PPD poisoning are pain in abdomen,black coloured vomitus, severe angioneurotic cervico-facial and upper respiratory tract oedema causing respi-ratory distress, weakness, pain and swelling of musclestypically of legs, chocolate brown colored urine, oliguriaand acute renal failure3,4. The treatment of PPD poi-soning is mainly supportive as no specific antidote is avail-able. The goal of treatment is to maintain clear airway,manage shock and prevent renal failure. Respiratory dis-tress may need urgent tracheostomy. Generous IV fluids(6-12 L) may be needed in 24 hrs) to correct hypov-olemia and preserve renal functions1,4. Alkalinization of
257
Correspondence
urine, loop diuretics and renal replacement therapy maybe required for oliguria and renal failure.
Uma Srivastava, ProfessorAshish Kannaujia, LecturerAditya Kumar, ProfessorSurekha Saxena, ProfessorImran Khan, P.G.StudentAbhijeet R. Mishra, P.G.StudentAmrita Gupta, P.G.StudentDepartment Of Anaesthesia & Critical Care, S. N. MedicalCollege, AgraE-mail: [email protected]
References
1. Kallel H, Chelly H, Dammak H, Bahloul M, Ksibi H,
Hamida CB, et al. Clinical manifestations of systemicparaphenylene diamine intoxication. J Nephrol2005;18:308-11.
2. Singla S, Miglani S, Lal AK, Gupta P, Agarwal AK. Par-aphenylenediamine (PPD) poisoning. JIACM2005;6:236-238
3. Anuradha S, Arora S, Mehrotra S, Arora A, Kar P. Acuterenal failure following para phenylenediamine (PPD) poi-soning: a case report and review. Ren Fail 2004 ;26:329-32.
4. Polderman KH. Acute renal failure and rhabdomyolysis.Int J Artf Organs 2004; 27:1030-1033.
5. Sampathkumar K, Yesudas SS, Rajappannair PA,Mahaldar AR, Muthian R. Rhabdomyolysis due to hairdye poisoning: an emerging threat. Ind J Crit Care Med2007; 11: 212-14.
Undelivered List of Feb 2009ISA NO.NAME CITY ISA NO.NAME CITY ISA NO. NAME CITY
A1056 DR ANIRBAN HOM CHOUDHURI NEW DELHI
A1104 DR ARCHANA LAKRA LUC KNOW
A1269 DR S ARUN SUBHAS SALEM
A1272 DR S AMBAL CHENNAI
A1306 DR. ANIL SHAMRAO MANE URAN
A1318 DR. ANURADHA J. BHANOT ROHTAK
A1327 DR. PRAMOD AYYAPPATH TRICHUR
A1359 DR. R. ARAVINTH KARTHI COIMBATORE
A1375 DR. AMIT I. JHA JAMNAGAR
A1416 DR. ATEEQ AHMED BANGALORE
A1443 DR. ANUSHA K PONDICHERRY
B0444 DR JAGADISH BASUMATARY NAGAON
B0675 DR WG CDR A K BARAL BANGALORE
B0835 DR GEETANJALE ATUL BORKAR MUMBAI
B0861 DR A BALASUBRAMANIAN SALEM
B0887 DR P BHASKAR RAO LUCKNOW
B0971 DR. SHINDE SMITA BANSI AHMEDNAGAR
B0972 DR. M. BASKAR DHARMAPURI
B1075 DR. BHUPENDRA PRATAP SINGH LUCKNOW
C0422 DR S CHRISTDOSS THIRUCHIRAPPALLI
C0478 DR MAJ N S AJAI CHANDRA PUNE
C0570 DR. CHITRA RAJESWARI THANGASWAMY NEW DELHI
D0786 DR DEEPAK R PONDICHERRY
D0904 DR. DEBYANI DEY NEW DELHI
E0034 DR EZHIL ANBALAGAN TRICHY
G0140 DR J GURURAJACHAR HYDERABAD
G0314 DR PRAVINGAR AMRATGA GOSAI RAJKOT
G0469 DR RAJENDRA GAWATRE AKOLA
G0716 DR S GEETHA COIMBATORE
G0724 DR GANAPATHI SUBRAMANI J SALEM
G0835 DR. GIRISH BABU N BANGALORE
H0220 DR HARISH KUMAR N BANGALORE
H0240 DR HEMANT SHIVAJIRAO KSHIRSAGAR PUNE
H0272 DR. NITIN HAYARAN BHOPAL
I0025 DR MOHAMMED ISMAIL MADURAI
J0202 DR RAJ KUMAR JAIN BHOPAL
J0254 DR SMITA SURESH JOSHI PUNE
J0576 DR JYOTI MADAN KHITHANI MUMBAI
J0598 DR JOSEPH DILIP CHRISTIAN VELLORE
J0655 DR. KARTHIK JAIN. M AHMEDABAD
J0745 DR. ANUJ JAIN LUCKNOW
K0230 DR P KALEEL UR RAHMAN COIMBATORE
K0270 DR NEELA S KULKARNI KOLHAPUR
K1006 DR KANNAN T S MADURAI
K1031 DR KAPIL DEV AMRITSAR
K1063 DR KIRAN M D KOLKATA
K1077 DR KOMALA VALLI S TIRUNELVELI
K1079 DR K S KARTHIKEYAN CHENNAI
K1100 DR KARTHIC BABU N MANGALORE
K1198 DR. ANIL KUMAR DELHI
K1237 DR. AJIT KUMAR MOTIHARI
L0137 DR LAILU LILIBET SAMUEL KALPAKKAM
L0184 DR LOVELY JAMES ALAPPUZHA
L0216 DR LALIT KUMAR JHANURDHARIKOSE WARDHA
L0262 DR. LENIN BABU ELAKKUMANAN NEW DELHI
M0789 DR LALITH MEHDIRATITA BHOPAL
M0881 DR MAHEEP KOHLI DUGGAL NEW DELHI
M1048 DR MANJULA G YELGACHIN HUBLI
M1166 DR VENKATA RAMANA MURTHY VIJAYAWADA
M1236 DR MANJULA K TRICHY
M1395 DR MONICA KHETARPAL HYDERABAD
M1402 DR MONALISA J PEREIRA MUMBAI
M1423 DR MINIKAMALA P ALAKKAD
M1424 DR MANISH MANDAL BURDWAN
M1508 DR MANISH TANDON LUCKNOW
M1599 DR. RACHAMALLA MALLESWARI TIRUPATI
M1667 SQN LDR (DR.) MANISH DHAVAN PUNE
M1695 DR. NITIN MAHESHWARI VADODARA
M1759 DR. KANTA MEENA NEW DELHI
N0554 DR NAGARAJAN R THENI
N0604 DR NISHKALA C CHENNAI
N0638 DR UDITA NAITHANI UDAIPUR
N0688 DR. A. NAGASUBRAMANIAM THANJAVUR
N0751 DR. MRIDU PABAN NATH ANSARI NAGAR
P0269 DR SUBASH C PATRA ROURKELA
P0298 DR ABHAY PATWARI HYDERABAD
P0896 DR PARIMAL KHURJEKAR PUNE
P1004 DR A S PADMINI WARANGAL
P1008 DR PREETI BOHREY BHOPAL
P1363 DR POPAT NILESHKUMAR HARSHADRAY RAJKOT
P1452 DR. PRASHANT PANDIT PAWAR MAHARASTRA
P1465 DR. R. KRISHNA PRABU PONDICHERRY
R0784 DR T RADHA RANI NEW DELHI
R0852 DR RAMESHWAR D AGARWAL FARIDABAD
R1256 DR RAJIV AGARWAL LUDHIANA
R1359 DR MANOJ N RAVINDRAN THANE
R1370 DR RIJU BANSAL DELHI
R1412 DR RAJA J R CHENNAI
R1429 DR KASA SRI RAMA RAO VISHAKAPATNAM
R1431 DR POLA RAVI CHANDRAHAS VISHAKAPATNAM
R1523 DR RICHA CHANDIGARH
R1570 DR. M. RAJA SHEKAR REDDY HYDERABAD
R1593 DR. UMESH LAKHMICHAND RAMTANI AMBAJOGAI
R1622 DR. S. SREE RANJANI CHENNAI
R1637 DR. RAJEEV. S KODUNGALLUR
R1639 DR. RAJESH CHANDRA GIRIDIH
R1682 DR. PRAMILA NARESH RATHOD LATUR
R1734 DR. RAJ KUMAR AHIRWAL JABALPUR
S0341 DR AJAY NARAYAN SAXENA BHOPAL
S0583 DR T SHET SUDHAKAR MYSORE
S0784 DR PRAMILA MALIK ROHTAK
S0893 DR B G SANGAM SAGAR
S1533 DR SHARANABASAPPA V GUADLI GADAG
S1694 DR SHUKDEV B CHANDARANA RAJKOT
S1861 DR N SATYANARAYANA SECUNDERABAD
S2092 DR SONA CHATURVEDI MAHARASTRA
S2717 DR J SARAVANA MOORTHY TRICHY
S2834 DR SURBHI GUPTA NEW DELHI
S2844 DR SHAMSUNDER MARUTI GAONKAR MUMBAI
S2896 DR T SUNITHA HYDERABAD
S2938 DR SACHIN PATHAK AHMEDABAD
S2950 DR SUBRAMANI I CHENNAI
S2967 DR SUSHIL CHANDRA KUREEL JABALPUR
S2988 DR SREERAJ C KOTTAYAM
S3523 DR. SHILPA GOYAL AHMEDABAD
S3535 DR. MAYURI V SHETTY MUMBAI
T0016 DR S M TRIVEDI RAJKOT
T0133 DR VANDANA S TRASY MUMBAI
T0217 DR R TAMILSELVI CHENNAI
T0348 DR VENGAMAMBA THUMMALA GUNTUR
T0376 DR THIRUVENKADAM SELVARAJAN THANJAVUR
T0385 DR MD TABREZ PATNA
T0423 DR. DEBENDRA KUMAR TRIPATHY PONDICHERRY
U0119 DR UPPULETI TARAKA PRASAD VIJAYAWADA
V0150 DR V VEERAPPAN COIMBATORE
V0346 DR VIBHAVARI V D MUMBAI
V0607 DR VYAS MANISHA RAGHUVER AHMEDABAD
V0609 DR VENUGOPALA RAO TANNERU GUNTUR
V0725 DR VAIJAYANTI NITIN GADRE MUMBAI
V0743 DR VASUDEVAN A PONDICHERY
V0834 DR. ANAND T. VAGARALI BELGAUM
V0881 DR. NANDAKUMAR V BHAVAN (T.K.), ERODE
V0905 DR. VIDUSHI MOHAN MANGALORE, DK.
W0040 DR. JULIE NARENDRA WANKHADE AHMEDNAGAR
Y0073 DR YASHPAL K BHUSHAN MEHSANA
258
Indian Journal of Anaesthesia, April 2009
India's First Complete Medical Ozone GeneratorKnown for its precise calibrationEarned reputation as an import substituteUsed by Doctors in twenty five cities across IndiaExported to different countries, Available at Indonesia, PakistanUsed in PAIN MANAGEMENT & TREATMENT OF IBS, RECTAL INSUFFLATIONHospital environment control (ICU, ICCU, NICU, ITU, Burn Ward, Morgues, OT)Burn, Ulcer, Skin & Hair treatment, Bed Sores, Diabetes, Cancer, Aids, Dentistry etc.Used by all major government and corporate hospitals in India and abroad
NEWNEWNEWNEWNEW–Improved Model No.0019 GW P
With Feed Quality Sensing (FQS) & Acclimatizationfor the first time in INDIA
100 Gamma Ozone Production–Highest in the sector,usable for versatile medical applications, including
Autohaemotherapy etc.Exchange previous models with this new one at nominal cost
Offer for Limited Period
CANADIAN Technology in Action
CONTACT:Team Waterhouse75/2B, Purna Das Road,1st Floor, Kolkata – 700 029Phone: 033 – 24651808Fax: 033 – 24653517E-mail: [email protected]: www.teamwaterhouse.netMobile: 0-98311 64364Doctors please enroll for free at:http://groups.google.co.in/group/unconven-tional-medicine?hl=enfor online help on medical application
Disinfecting Hand Wash for Clinics- Pharma Manufacturing facilities