Embed Size (px)
DESCRIPTION
Coronary Heart March / April 2007 Edition
Citation preview

coronaryheart.com
FREE SUBSCRIPTION!! REGISTER ONLINE
coronaryheart.com
FREE SUBSCRIPTION!! REGISTER ONLINE
March / April 2007Issue 5
MassachusettsGeneral Hospital
Coffs Harbour Health Campus, Australia
LATEST NEWS,EDUCATION
+ more...
EMP
LO
YMENT
MMPP
LLOOMM
PPLLO
Arrhythmias in the Himalayas
Cath Lab Visit
“The World’s Fastest
Growing Cath Lab
Magazine!!”
Special feature
Designedfor yourCath/EP
Lab
International

“Great quality of the articles. This magazine has everything to be between the top magazines in the Cardiology world.”
- Barnet Hospital, UK
“The education presentations on the website are particularly excellent.”
- Southampton General Hospital, UK
“I had an opportunity to read the Dec 2006/Jan 2007 issue and enjoyed the articles and layout.”
- Hotel-Dieu Grace Hospital, Canada
“....found it very educational, as well as entertaining. It let’s me compare how my organization is in relation to others around the nation and the world.”
- Miami VA Medical Center, USA
“Great magazine with interesting topics that are quick and easy to read. Images are excellent and a great tool as visual resources.”
- Bankstown Hospital, Australia
“It’s very educational and informative. As a student, I found it very useful.”
- Nursing Student, UK
“Extremely informative with the latest in technology and procedures.”
- Sarasota Memorial Hospital, USA
“Fantastic, very worthwhile and interesting.”
- Greenslopes Private Hospital, Australia
“Saw an issue at work. Love the magazine.”
- Mononhahela Valley Hospital, USA
“Very Impressive.”
- Florida Hospital, USA
“Excellent blend of educational and entertaining articles.”
- Dorset County Hospital, UK
“Your articles are very relevant to practice.”
- Southlake Regional Health Center, Canada
“January 2007 issue was very interesting.”
- UCSD Medical Center, USA
“I was particulary impressed by the quality and visual appeal of your magazine. I believe it will appeal to cardiac nurses working across all spectrums of the cardiac health care sector - both nationally and internationally.”
- Austin Health, Australia
“The First time I saw this in our Cath Lab breakroom I thought it was a great publication, and read it entirely.”
- Tomball Regional Hospital, USA
“Excellent for learning. Good articles to read.”
- Sinai-Grace Hospital, USA
“So, what did you think of our last edition?”

CONTENTSMarch / April 2007
ContentsCORONARYHEART
CORONARY HEART ™ 3
04 Welcome Editorial
06 Latest News
12 Future
14 Product Focus‘BIOTRONIK CRT’
16 Product Focus‘3D Cardiology’
18 Special Feature‘Revealing Arrhythmias in the Himalayas’
24 Site Visit (USA)‘Massachusetts General Hospital’
29 Site Visit (AUS)‘Coff s Harbour Health Campus’
33 EP Education‘Adenosine in Electrophysiology’
37 Competition
38 Medical Imaging‘RCA, Interesting Case, + Hot Tip’
40 Conferences
42 Conference Preview
44 Cardiac Societies‘SICP Overview’
04 Welcome
THIS EDITION
47 Languages‘Cardiac Tagalog”
48 Employment + General Info
51 Next Edition Preview
Managers Nurses Radiologic Technologists Cardiovascular Technologists RCIS Echo
Page: 24
Page: 18

Welcome EditorialEDITORIAL
What an amazing last three months it has been for our publication. Some of you are
already aware that we performed a printing date realignment during this period, which meant we had to skip February. So now we are back in line with other bimonthly publication printing dates which makes it easier for us to manage and more consistent for companies within the industry for budgeting and marketing.
Another important change that has occurred is that the distribution of Coronary Heart has tripled since the last edition, reaching 8691 readers, 90% of which are based in the USA. Th is is the world’s largest cardiac market. It now gives us a pool of resources to provide readers from around the globe with the latest information, strategies, and techniques to assist others in the industry. It is hoped that this ultimately will improve working conditions around the world and provide better care for patients.
We have also been lucky to achieve the support of two major cardiac groups in the USA, being the Alliance of Cardiovascular Professionals (ACVP) and the Society of Invasive Cardiovascular Professionals (SICP). All members from these two groups have been included on our mailing list for this and future issues.
Finally we would also like to thank everybody who fi lled in the “Comments” section when subscribing online. Some of your remarks have been included on page 2. We are sure you will enjoy this edition just as much as the last.
Disclaimer:Coronary Heart should never be regarded as an authoritative peer reviewed medical journal. Coronary Heart has been designed as a guide only, to inform readers who work in the cardiology environment about latest news stories and the diff erent techniques used by others around the world. Whilst all care is taken in reviewing articles obtained from various companies and contributors, it is not possible to confi rm the accuracy of all statements. Th erefore it is the reader’s responsibility that any advice provided in this publication should be carefully checked themselves, by either contacting the companies involved or speaking to those with skills in the specifi c area. Readers should always re check claims made in this publication before employing them in their own work environment. Opinions expressed by contributors are their own and not necessarily those of their institution, Coronary Heart Publishing Ltd or the editorial staff .
Coronary Heart Publishing Ltd145 - 157 St John Street
London, EC1V 4PYUnited Kingdom
Phone: +44 (0) 207 788 7967Fax: +44 (0) 207 160 9334
Visit us online at www.coronaryheart.com
Director / Chief EditorTim Larner
Clinical EditorDr Rodney Foale
Consulting EditorsDr Richard Edwards
Ms Voncile Hilson-MorrowMr Ian WrightMr Stuart Allen
ADVERTISING
Request Media Kits online
CIRCULATION
8691 Cardiac Professionals in six countries.
Copyright 2007 by Coronary Heart Publishing Ltd. All rights reserved.
Material may only be reproduced by prior arrangement and with due acknowledgment of
Coronary Heart Publishing.Th e publication of an advertisement or product
review does not imply that a product is recommended by Coronary Heart Publishing Ltd.
Subscribe Online to get your own
free copy
Tim LarnerDirector
Tim �
Clinical Editor
Dr Rodney Foale, FRCP. FACC. FESC. FCSANZ.Clinical Director, Surgery, Cardiovascular Sciences and Critical Care. SMHT.
COVER PHOTO (from left): Sharon McKenna, RN BSN Nurse Manager and Dr MichaelFifer, Medical Director, standing at the entrance to the Massachusetts General Hospital Cath Lab.
4 CORONARY HEART ™

A New MemberEDITORIAL
Th e ARDMS requires that to maintain eligible status, registrants must accrue 30 continuing medical education (CME) credits per three year period.
Th e Cardiovascular Credentialing International (CCI) administers examinations and awards credentials in many areas including:
RCIS: Registered Cardiovascular Invasive Specialist (similar to Generic Worker course in UK)RCS: Registered Cardiac Sonographer RVS: Registered Vascular Specialist CCT: Certifi ed Cardiographic Technician (similar to Cardiac Physiologists)
Th e CCI requires that to maintain eligible status, registrants must accrue 36 continuing education units (CEU), 30 of which must be cardiovascular related.
•
•••
It is our great pleasure to welcome to the Coronary Heart Editorial Board, Ms
Voncile Hilson-Morrow. Th is inspiring lady is known by many people within the industry through her various speaking engagements on topics of department management. Her experience comes from over ten years as the Director of Invasive Cardiology at Washington Heart at Washington Hospital Center, which is one of the busiest Cath Labs in the USA.
She was responsible for implementing operational initiatives and managing a staff of over 100 full time employees and 20,000 procedures annually. She has coordinated implementation and replacement for over 15 cath and EP laboratories this included facility and staff planning, design and capital equipment acquisition also many other multi-million dollar expansion projects.
Prior to Washington Hospital Center, Hilson-Morrow held cardiology management positions at Western Pennsylvania Hospital in Pittsburgh,
PA and Th e Methodist Hospitals, Gary, Indiana. She earned her bachelor’s degree from St. Francis University, Joliet, IL, and her AS in Allied Health from Indiana University. Ms. Hilson-Morrow, a Registered Technologist, also completed her radiography training at Th e Methodist Hospitals’ School of Radiologic Technology.
After 25 years of Cardiology Management exprerience, Voncile is
now the Chief Executive Offi cer of Healthworks, Inc. new Baltimore/Washington division branch offi ce. Using her vast previous experience she identifi es opportunities and establishes collaborative client relationships to provide qualifi ed technical staff , clinical education and consulting services to health care provider organizations such as hospitals and group practices.
Apart from reviewing management related articles from readers, Voncile will also be conducting various interviews with leading cardiac department directors. Th ese interviews will be designed
to give directors and managers around the world an insight into the experience of running a large department, from the most enjoyable bits to those that cause nightmares. We believe that readers will be able to implement some of the advice given to improve their own departments.
GLOSSARY
Ms Voncile Hilson-Morrow
Coronary Heart’s New Management Consulting Editor
AMENDMENTSt Th omas’ Hospital in London for our
Edition 4 Site Visit has eleven F/T radiographers, instead of one.
CORONARY HEART ™ 5
UK, AUS, NZ, IRE USA
Registered Nurse (RN) sameRadiographers Radiologic or X-ray Technologists,
which can include Radiation Therapists, but also others (Mammographers, CT Technologists, etc). Most Radiologic Technologists are Registered Technologists (RTs). To be a Registered Technologist, one must pass an exam and to maintain this credential, registrants must accrue 24 continuing education (CE) credits per two-year period.Canada: Medical Radiation Technologists
Cardiac Physiologists Cardiovascular Technologists, also known as CVTs
Cardiac Registrars Cardiology Residents

Latest NewsLATEST NEWS
Stereotaxis and Philips Combined in the USA
Philips recently announced the installation of two new cardiac electrophysiology (EP) labs at the
University of California San Francisco Medical Center, San Francisco, and St. Elizabeth’s Hospital, Boston. Th e system combines a ceiling-mounted Philips Allura Xper FD10 X-ray system with the Stereotaxis Niobe system.
Th e Stereotaxis Niobe Magnetic Navigation System was previously featured in Edition 1, and with more than 6000 procedures already performed and over 100 of these systems on order you may see one in a city near you soon.
So what makes it so special?
Basically the system
allows physicians to more eff ectively navigate guidewires, catheters, and other magnetic interventional devices to areas of the heart that require treatment such as ablation.
To achieve this it uses two computer-controlled devices that produce magnetic fi elds. which are activated to steer the devices. In EP it is easiest to imagine a compass needle pointing to magnetic north. Th e magnetic fi eld is then adjusted to robotically move the catheter tip in three dimensions, to a pre-defi ned target obtained from 3D images of the patients heart.
Th e Niobe system can achieve angulations up 45 degrees LAO/RAO to allow the navigation to produce a 3D environment.
Dr. Charles Haff ajee,
director of the cardiac electrophysiology program, at St. Elizabeth’s Hospital stated, “We use the Niobe system in 40 percent of cases in the lab, and in that time the combination Allura Xper and Niobe system has proven to be highly reliable and has helped our staff to better manage the lab.”
Dr. Jeff rey Olgin, associate professor of Medicine and chief of Cardiac Electrophysiology, University of California San Francisco (UCSF) Medical Center discussed the advantage of using the Philips system. He stated, ““Th e ceiling-mounted system reduces
the footprint in the lab and allows the possibility of using both interventional cardiology and electrophysiology procedures.
Another important benefi t of this system is increased patient
accessibility during the procedures, which improves the work
environment of patient and staff .”
Visit www.stereotaxis.com for more information on this
system.
INTERNATIONAL
St. Elizabeth’s Hospital, Boston. Th e system combines a ceiling-mounted Philips Allura Xper FD10 X-ray system with the Stereotaxis Niobe system.
Th e Stereotaxis Niobe Magnetic Navigation System was previously featured in Edition 1, and with more than 6000 procedures already performed and over 100 of these systems on order you may see one in a city near you soon.
So what makes it so special?
Basically the system
catheter tip in three dimensions, to a pre-defi ned target obtained from 3D images of the patients heart.
Th e Niobe system can achieve angulations up 45 degrees LAO/RAO to allow the navigation to produce a 3D environment.
Dr. Charles Haff ajee,
Medical Center discussed the advantage of using the Philips system. He stated, ““Th e ceiling-mounted system reduces
the footprint in the lab and allows the possibility of using both interventional cardiology and electrophysiology procedures.
Another important benefi t of this system is increased patient
accessibility during the procedures, which improves the work
environment of patient and staff .”
Visit www.stereotaxis.com for more information on this
system.
Philips Allura Xper FD10 with the Stereotaxis Niobe System Image courtesy of Philips
CAUTION: Some products within this magazine may be restricted to specific regional usage, and may not
be available in your region. Always check with the manufacturer to determine availability.
6 CORONARY HEART ™

Latest NewsLATEST NEWS
FDA and CE Approval for New St Jude EP Products
In early January 2007, St Jude announced they had received US FDA and European CE
approval to market their Refl exion Spiral™ Variable Radius Mapping Catheter and the EnSite® System workstation computer.
Th e Refl exion Spiral Variable Radius catheter features a circular loop at the tip that expands from 15 mm to 25 mm to fi t a variety of patient anatomies. St Jude say
that it is the only variable radius circular mapping catheter available with bi-directional defl ection, which provides enhanced versatility for complex left atrial procedures. Another important feature is the ComfortGrip™ handle which allows more improved comfort during long cases.
Th e Ensite system now includes a new computer with twin dual-core processors for extremely fast processing speeds. Th is has allowed for the most complex processing and image rendering times to be reduced by up 80%.
Visit www.sjm.com for more information.
New research presented at the Canadian Cardiovascular Congress 2006 in Vancouver
shows that depression in people who have had a heart attack is under-diagnosed and under-treated. And new evidence is suggesting that, especially among males, depression could indicate a signifi cant risk for a second heart
attack.
“About 50 percent of patients experience blue moods after a heart attack, especially in the fi rst six weeks after treatment. In many people this is a passing thing and not unnatural. Others will require treatment for major depression,” says Dr. Beth Abramson, Heart and Stroke Foundation of Canada spokesperson and one of the presenters.
“What is surprising is the very limited data we have concerning the safety and tolerability of antidepressant medication in patients with coronary artery disease who have major depression.”
In a study of 17,000 patients in Alberta, Dr. Padma Kaul found that anti-depressant medication (ADM) use is less frequent among
males. But those males who do take antidepressants have a higher risk of mortality than females who take anti-depressants.
Dr. Kaul discovered ADM use among males was 10 percent compared to 18.1 percent among females. After one year, her study showed that mortality among males who took an ADM was 8.4%, while among females it was 4.5%.
“It is hard to imagine why treatment of depression should be hazardous to males, but it may be that men fi nd it more diffi cult to admit that they might need an antidepressant,” says Dr. Kaul, assistant professor of cardiology at the University of Alberta and Capital Health in Edmonton. “So those men who ultimately do take an ADM could be sicker and more likely to die.”
Dr. Kaul’s is the fi rst population-based study to quantify the role of depression in mortality among patients presenting to emergency departments with heart disease symptoms.
INTERNATIONAL
Depression Undertreated in Heart Attack Survivors
CORONARY HEART ™ 7

Latest NewsLATEST NEWS
8 CORONARY HEART ™
New HIFU Trial in Pennsylvania for AF
Clinical researchers at the University of Pennsylvania Health System are starting a
trial utilizing a new technology for treating atrial fi brillation.
Made by ProRhythm Inc, the high intensity focused ultrasound (HIFU) ablation system is the fi rst to treat atrial fi brillation using ultrasound energy refl ected forward in a complete circle to isolate pulmonary veins.. Th is invasive procedure is done in the lab with balloon catheters while the patientis awake but sedated or under general anaesthesia.
Up until now, physicians have had to deliver radio frequency energy bursts to the tissue in a dot-by-dot fashion around the veins. “Th at can cause swelling, and when that swelling goes down, you may still have viable tissue left behind, gaps, where the electricity can still conduct itself or get through,” explains David Callans, MD,
director of the electrophysiology laboratory at the Hospital of theUniversity of Pennsylvania and principal investigator of this study.
Electrophysiologists use ablation procedures (using intense heat to kill small areas of tissue) to electrically isolate pulmonary veins from the atria. Th e pulmonary veins produce rapid impulses which initiate and help to sustain AF and isolating them treats this arrythmia in some patients.. “Since this new system sits outside of the vein, and delivers energy forward rather than immediately around it, there is no damage to the inside of the vein. Th is maintains a normal blood fl ow.
Plus, this new system could shorten the ablation procedure time which
currently takes about four hours,” adds Callans. Here at Coronary Heart we have actually seen this system in use in a trial at St Mary’s Hospital in London, UK.
Th e potential to isolate pulmonary veins in one energy application should allow for faster and perhaps more eff ective procedures than using the traditional “spot-welding” method.
Innerspace Release New Storage Solutions
Innerspace Corporation has been a market leader in medical storage
and inventory solutions for over twenty years, and have recently announced the launch of a new range of carts to their collection. Called Harmony, the carts come in
four sizes and are available in a variety of specifi cations.
Heavy-duty plate casters, central key-lock and a pull-out writing surface are standard on every Harmony. An optional electronic keyless entry is also available that incorporates an auto re-lock feature, low battery indicator and manual key override. Anesthesia and Crash carts also come standard with a tracking caster, making the carts easy to maneuver when pushing over long distances.
Visit www.innerspacecorp.com for more information
INTERNATIONAL
CAUTION: Some products within this magazine may be restricted to specific regional usage, and may not
be available in your region. Always check with the manufacturer to determine availability.
The HIFU Ablation System Image courtesy ProRhythm, Inc.

Latest NewsLATEST NEWS
Valecor™ Stent Receives CE Mark
On December 19, 2006, CorNova, Inc., announced it
had received CE Mark marketing approval for its Valecor™ Coronary
Stent System. Th e company aims for the Valecor™ to become the premier bare metal stent on the market due to the advanced cobalt-chromium alloy, which gives excellent strength and fl exibility.
Th e system also has minimal strut thickness which is believed to signifi cantly reduce restenosis. And with its open cell architecture providing uniform expansion and
conformity, it should prove useful during complex procedures.
Th e CE Mark approval allows for the Valecor™ Coronary Stent System to be sold in all European Union countries, and many other countries worldwide, excluding the United States and Japan.
Visit www.cornova.com for more information
CORONARY HEART ™ 9
Siemens’ Generation NeXt
Siemens Medical Systems demonstrated at the EuroEcho 10 conference held in Prague,
Czech Republic, and for the fi rst time at a cardiology congress, their new generation ultrasound units. Th e ultrasound systems Acuson X300 and Acuson Antares are claimed to provide outstanding performance through advanced offl ine and online applications such as the syngo Arterial Health Package and syngo Mitral Valve Assessment.
Th e Acuson X300 is an ultra-compact unit that is designed for busy settings such as emergency departments where staff can easily manoeuvre the unit alongside the patient, perform the exam, and leave without disrupting the workfl ow of the area.
Th e system’s TGO (tissue grayscale optimization) technology delivers consistent image quality, while advanced Hanafy (acoustic) lens transducers enable improved image uniformity when scanning technically diffi cult-to-image patients.
Th e Acuson Antares, premium edition, 5.0 release is equipped with a high-
resolution 19-inch fl at panel display mounted on an articulating arm for optimal viewing position.
Other ergonomic design features include the natural and extended reach zone concept that makes controls and peripheral devices easily accessible; allowing for greater patient comfort, easier examination and departmental workfl ow.
Th e syngo Arterial Health Package helps physicians evaluate cardiac
risk factors and quantifi cation of cardiovascular age with automated intima-media thickness measurements. While the syngo Mitral Valve Assessment application provides for a rapid 3D/4D evaluation of mitral valve morphology and physiology to aid diagnosis and planning of surgical procedures.
Visit www.medical.siemens.com for more information
INTERNATIONALINTERNATIONAL
Siemens Generation NeXt: Acuson Antares Image courtesy Siemens Medical Systems

Latest NewsLATEST NEWS
GE Displays New Innova Bi-Plane at RSNA
The world renowned Radiological Society of North America in Chicago (RSNA)
92nd annual meeting is the site where imaging companies and consumers came together to see the latest advances in their industry.
Naturally any trade show of this type wouldn’t be complete without GE displaying something impressive from their vast array of imaging equipment, and RSNA was no exception. On display was the Innova® 3131IQ digital fl at panel Biplane Imaging System. At the time it was claimed to be the fi rst system available that would cover the full size of the patient’s lateral and frontal anatomy simultaneously for a variety of diagnostic and interventional procedures.
Th e system is indicated for use in cardiovascular imaging, diagnostic
and interventional procedures, and with over 1200 Innova’s installed internationally it is backed by great service support.
One of the advantages of the GE panel is that it is able to perform high quality
3-D Flat Panel Rotational Imaging to produce three-dimensional images of the vascular system, bone and soft tissue in the body.
Visit www.gehealthcare.com for more information
Medtronic Tests New MRI Safe Pacemaker
MRI scanners, like the one pictured, have proved
very popular with physicians for the diagnosis of many ailments, however a major disadvantage for many patients is its inability to be used with pacemakers due to their metallic componentry and construction.
A few weeks ago though Medtronic announced they have started an international clinical study to confi rm the safety and effi cacy of the Medtronic EnRhythm® MRI SureScan™ pacing system. Th is system is the fi rst of its type and if successful will have a major advantage over other manufacturers.
Medtronic have completely redesigned the leads and pacemaker to make it compliant with MRI’s, with the fi rst trials held in Europe. Th ere will be 350 patients
involved in the trial which is expected to last 24 months.
Visit www.medtronic.com for more information
The new GE Innova 3131IQ Biplane Imaging System Image courtesy GE Healthcare
INTERNATIONAL
CAUTION: Some products within this magazine may be restricted to specific regional usage, and may not
be available in your region. Always check with the manufacturer to determine availability.
10 CORONARY HEART ™
the Medtronic EnRhythm® MRI SureScan™ pacing system. Th is system is the fi rst of its type and if successful will have a major advantage over other manufacturers.
Medtronic have completely redesigned the leads and pacemaker to make it compliant with
in Europe. Th ere will be 350 patients
SureScan™ pacing system. Th is system is the fi rst of its type and if successful will have a major advantage over other manufacturers.
Medtronic have completely redesigned the leads and pacemaker to make it compliant with
will be 350 patients Image Courtesy GE Healthcare

Latest NewsLATEST NEWS
Accuracy of Cardiac CT to Determine Blood Flow?
New research that appeared in the Dec. 19 edition of the Journal of the American
College of Cardiology showed that coronary artery disease (CAD) seen using mulit-slice CT (MSCT) does not necessarily correlate to fl ow limitation.
Th e study which involved 114 patients who had chest pain and/or risk factors for CAD, but no prior history of CAD, was led by Jeroen J. Bax, MD, PhD, Department of Cardiology at the Leiden University Medical Center in
the Netherlands.
Th e researchers sought to determine whether MSCT, a non-invasive imaging technique that detects narrowing of the coronary arteries due to plaque build-up (atherosclerosis), can also accurately identify reduced blood fl ow in the arteries due to the blockage (ischemia).
Th e study compared MSCT to another non-invasive imaging technique, myocardial perfusion imaging (MPI) with single-photon emission computed tomography (SPECT), among patients with a moderate risk of CAD to fi nd the answer.
Results of the study show that only 45 percent of patients who were shown to have atherosclerosis through the use of MCST were also found to have
ischemia through the use of MPI. In other words although CT showed a stenosis, this does not necessarily correlate with exercise induced ischaemia.
“Th is study has major implications in the management of patients in clinical practice,” said Dr. Bax. “One possibility is to use MCST to identify the presence and extent of plaques in the arteries and if (considerable) atherosclerosis is shown to be present, then clinicians may proceed to use SPECT imaging to evaluate if the patient has ischemia.”
It is important to remember that the main of advantage of MSCT is it is low risk and could prevent unnecessary invasive coronary angiography in patients.
INTERNATIONALINTERNATIONAL
ECG Problem Solving by Mr Stuart Allen, Cardiac Rhythm Group Manager - Southampton University Hospitals NHS Trust, UK
Visit our website www.coronaryheart.com
for the answerCASE HISTORY
Patient had insertion of a dual chamber pacemaker. At one-month follow-up this is his 12-lead ECG. What’s the problem?
CORONARY HEART ™ 11

Cardiology AdvancesFUTURE
12 CORONARY HEART ™
Growing Replacement Heart Muscle in Just 4 Days
Imagine a day when damaged heart muscle from an MI can simply be replaced with a quick
surgical patch, or when an entirely new heart can be grown easily, putting an end to heart transplant waiting lists. Well thanks to researchers from the University of Michigan (U-M) we are now a vital step closer to achieving this goal.
In a recent article published online in the Journal of Biomedical Materials Research Part A, the team led by Ravi K. Birla, Ph.D., of the Artifi cial Heart Laboratory in U-M’s Section of Cardiac Surgery and the U-M Cardiovascular Center, reported signifi cant progress in growing bioengineered heart muscle, or BEHM, with organized cells, capable of generating pulsating forces and reacting to stimulation more like real muscle than ever before. Th e research is still in the animal testing phase.
Th e three-dimensional tissue was grown using an innovative technique that is faster than others that have been tried in recent years, but still yields tissue with signifi cantly better properties. Th e approach uses a fi brin gel to support rat cardiac cells temporarily, before the fi brin breaks down as the cells
organize into tissue. Th is may be a key achievement for future use of BEHM as a treatment option, because the tissue could be grown and implanted relatively quickly.
Th e researchers used a transducer to measure the tensile strength of the new cells and found that the BEHM that had formed in just four days after a million cells were layered on fi brin gel could contract with an active force of half that generated with a live human heart. However when bathed in specifi c solutions this contraction increased further.
BEHM is still a few years away from use as a human heart treatment,
however the U-M researchers say their results should help accelerate progress toward this goal. U-M is applying for patent protection on the development and is actively looking for a corporate partner to help bring the technology to market.
Breakthrough for BP Monitoring
SunTech Medical and Empirical Technologies Corporation have announced they are collaborating
to introduce a clinical blood pressure monitor that measures, with every heart beat, aortic pressure at the
wrist. Th e companies are already preparing for commercial deployment of a device called BPGuadian™, which monitors blood pressure beat-by-beat and non-invasively without discomfort, attached to the wrist. Information from the sensor is then sent via a Bluetooth connection to a nearby computer or handheld device, such as a PDA.
Visit www.empiricaltechnologies.com for more information
A schematic of how the BEHM can be used to repair damaged heart muscle
Images and Press Release “Copyright University of Michigan - Used with permission”
A patch of bioengineered heart muscle
12 CORONARY HEART ™

Cardiology Advances (cont...)
FUTURE
CORONARY HEART ™ 13
European Space Agency Heart Study
Following on from our Edition Th ree look at the cardiology projects underway above our heads in the International Space Station, we have tracked down a
study underway by the European Space Agency.
Th e experiment, called ‘A Model For Investigating Mechanisms Of Heart Disease & Mechanisms Of Activation
Of Sympathoadrenal Activity In Humans During Spacefl ight’ (CARD), is helping scientists
examine the relationship between salt intake and the cardiovascular system when exposed
to the microgravity environment.
Crew members typically experience reduced blood pressure in microgravity. To help them
readjust to gravity on Earth, they take salt tablets just before returning, which temporarily increases
the blood volume. CARD is looking at the eff ects of ingesting occasional salt supplements throughout the long duration mission. Th is experiment’s results could give insight into helping improve treatment of patients with heart failure.
Battery Free Pacemaker Under Development
A project currently underway in the UK may herald a major
breakthrough in cardiac technology. Th e project is to design an in-body microgenerator that will convert energy from human body movement into power for implanted medical devices, such as
pacemakers and ICD’s.
On average batteries need replacing every seven to ten years, at a cost of up £10,000. And with increased functionality such as wireless monitoring, and the relentless push for smaller devices, the demand on battery life is being stretched to the limit.
Th e two-year SIMM (self-energizing implantable medical micro system)
project will prototype a device capable of harvesting energy
from movement in or on the body, including joint movement and heartbeats. Body energy will be harvested by means of a microgenerator
manufactured as a MEMS
(micro-electrical-mechanical system). Th is prototype design is expected to achieve 10-100 times more power than previous attempts to harvest human energy.
“Th e ability to fi t and forget implantable devices in terms of their power supply is groundbreaking with signifi cant clinical and quality of life advances,” said David Hatherall, external project leader at Zarlink’s Caldicot facility and SIMM project coordinator.
Th e project is being led by Zarlink Semiconductor which recently announced it had received £500,000 in funding from the UK Department of Trade and Industry, which would be match-funded by a consortium of UK-based companies.
Heart Studyollowing on from our Edition Th ree look at the cardiology projects underway above our heads in the International Space Station, we have tracked down a
study underway by the European Space Agency.
Th e experiment, called ‘A Model For Investigating Mechanisms Of Heart Disease & Mechanisms Of Activation
Of Sympathoadrenal Activity In Humans During Spacefl ight’ (CARD), is helping scientists
examine the relationship between salt intake and the cardiovascular system when exposed
to the microgravity environment.
Crew members typically experience reduced blood pressure in microgravity. To help them
readjust to gravity on Earth, they take salt tablets just before returning, which temporarily increases
the blood volume. CARD is looking at the eff ects of ingesting occasional salt supplements throughout the long duration mission. Th is experiment’s results could give insight into helping improve treatment of patients with heart failure.
Heart Study
Following on from our Edition Th ree look at the cardiology projects underway above our heads in the International Space Station, we have tracked down a
study underway by the European Space Agency.
Th e experiment, called ‘A Model For Investigating Mechanisms Of Heart Disease & Mechanisms Of Activation
Of Sympathoadrenal Activity In Humans During
readjust to gravity on Earth, they take salt tablets just before returning, which temporarily increases
the blood volume. CARD is looking at the eff ects of ingesting occasional salt supplements throughout the long duration mission. Th is experiment’s results could give insight into helping improve treatment of patients with heart failure.
convert energy from human body movement into power for
implantable medical micro system) project will prototype a device
capable of harvesting energy from movement in or
on the body, including joint movement and heartbeats. Body energy will be harvested by means of a microgenerator
manufactured as a MEMS
convert energy from human body movement into power for
project will prototype a device capable of harvesting energy
from movement in or
CORONARY HEART ™ 13

BIOTRONIK Update PRODUCT FOCUS
14 CORONARY HEART ™
A New Landmark in Heart Failure Therapy
A new Cardiac Resynchronisation Device has been launched to market that will set the bench
mark for all future CRT-D devices. Th e Lumax HF-T system from BIOTRONIK is revolutionary in that it is the fi rst and only fully automated system that enables patient monitoring through telecardiology.Th e new Lumax CRT-D, in conjunction with the innovative ‘Twin Flex’ co-radial Bipolar Corox OTW left heart lead and the Vision Guidewire, off ers the most comprehensive therapy package for Heart Failure patients. Coupled with the Biotronik Home Monitoring® and the new IEGM Online HD® it is truly an unrivalled system.
CRT has been proven to be a very successful therapy in numerous clinical studies, however some challenges remain. One such challenge with CRT pacing is the propensity for elevated LV thresholds and the possibility of diaphragmatic stimulation. Th is issue can often exclude patients from benefi ting from eff ective resynchronisation therapy. Th e Lumax HF-T device has the ability to manage this by electrically repositioning the LV lead. Dr. Barr, Consultant Cardiologist at Russell’s Hall Hospital, Dudley commented “Th e Lumax system off ers unrivalled programmability for diffi cult patients. Th e ability to programme alternative LV pacing confi gurations enables those patients with high LV thresholds and extra cardiac stimulation to be managed eff ectively.”
In addition to the extensive options for CRT, the device is equipped with
algorithms that ensure the patient receives optimum therapy. ATP One Shot® can provide pain free therapy for fast ventricular tachycardias that fall within the programmed ventricular fi brillation zone. Th e PainFree II Rx Trial showed that by adopting pain free programming 3 out of 4 high energy shocks can be avoided. Th e ability to deliver an ATP attempt in the ventricular fi brillation zone is a great advantage. ICD shocks can have a signifi cant psychological impact on patients and if this can be reduced to only those that are absolutely necessary it is of great benefi t.
Th e Lumax HF-T family includes a high energy version. Th e 40J option ensures eff ective therapy in patients that
ADVERTISEMENT
IEGM Online HD®
>>

PRODUCT FOCUS
BIOTRONIK Update (cont...)
CORONARY HEART ™ 15
have elevated defi brillation thresholds. Th is revolutionary device has the ability to not only provide high energy therapy, but to automatically confi rm via Biotronik Home Monitoring ® and IEGM Online HD® that it was eff ective, ensuring maximum safety for patients.
BIOTRONIK has always been the pioneer of telecardiology and has further enhanced its Home Monitoring technology. Th e information transmitted by the Lumax device will include an advanced Heart Failure Monitor and three channel IEGMs, thus supplying the clinical team with highly signifi cant data in outstanding quality. “Th is appears to be another step forward in the optimal management of patients with heart failure and implantable defi brillators.Th is latest development not only allows the daily monitoring of device performance and arrhythmia burden but can also help in the early detection of deteriorating cardiac function. Ultimately this may prevent a hospital admission.” commented Dr. Stuart Harris at St.Bartholomew’s Hospital, London.
Every year more and more patients suff er from severe heart failure. Th e development of the Lumax HF-T device combines the best cardiac resynchronisation therapy with the most advanced remote monitoring technology available and represents a landmark in modern heart failure therapy. Th is underlines again the commitment BIOTRONIK has towards technological innovation, providing best solutions for effi cient therapy management and improving patients’ quality of life.
For more information please contact [email protected] or visit www.biotronik.com

3DcardiologyPRODUCT FOCUS
16 CORONARY HEART ™
Here at Coronary Heart, we just love supporting new companies trying to gain a
foot hold in the cardiac industry. Th is issue we take a look at 3Dcardiology, a new cath lab computer simulation program designed by a radiographer from the UK. Th e program is still in developmental stages, however they would like our readers to have their say to help with the fi nal development before market. So have a read of what they say, trial the product free online, and tell them (nicely) how they need to improve their product.
Introduction
Fluoroscopic procedures may involve high radiation doses to both patients and staff . Quick and accurate positioning of the patient and image intensifi er combined with good radiological/surface anatomical awareness generally comes with experience, and is learned by performing procedures in real life.
By combining a realistic environment for fl uoroscopy with a radiological/cross-sectional anatomical reference tool, 3dcardiology may help to increase the effi ciency and safety of diagnostic and interventional procedures, whilst at the same time reducing the radiation dose to both staff and patients.
‘Virtual cath lab’ – fl uoroscopy and MRI
3dcardiology is a computer-based fl uoroscopy simulator and anatomical viewer. It uses a real-time interactive 3D games rendering engine (similar to the Playstation and X-box) to deliver a fl uoroscopy simulation environment. Th is ‘virtual cath lab’ environment enables visualisation and interaction between computer generated anatomical models and
fl uoroscopic equipment models to realistically replicate the movement and visualisation physics of a real image intensifi er with a patient on the table.
Within the ‘virtual cath lab’, the table movements, bi plane c-arm angulations and corresponding display of radiological anatomy on frontal and lateral monitors are a completely accurate representation of what you would expect to see if you were to practise screening in a real catheterisation laboratory using a set of phantom anatomical models.
To aid correlation between fl uoroscopic and cross-sectional anatomy, ‘MRI mode’ has been incorporated into the ‘virtual cath lab’. Th is enables instant switching between fl uoroscopic anatomical visualisation and cross-sectional anatomical visualisation, using the c-arms as ‘mini-MRI scanners’. Th e cross-section thickness can be user-defi ned, and both frontal and lateral scan-planes can be adjusted whilst simultaneously allowing free range of movement of the c-arms and table.
Dedicated centrally hosted 3D servers
Most ’virtual environments’ using 3d games technology require the very latest and fastest computer hardware, combined with a variety of specialist software plug-ins to deliver real-time simulation performance to the end user. 3dcardiology diff ers from this in that the only requirement to run 3dcardiology is a computer with an internet connection. All the complicated processing required to deliver the ‘virtual environment’ to your computer is done on our 3d servers in a remote centrally hosted data centre.
When you log on to 3dcardiology over the internet, we will set up a unique personal dedicated link between your computer and the processing power of our 3d servers. Furthermore, you don’t need a windows-based PC, you can use an Apple Mac, a Linux based PC or even a wi-fi enabled PDA. All of this is done using thin-client technology.
Screenshot 1: Screening Disabled
Coronary Heart™ BETA TestingCoronary Heart™ BETA TestingCoronary Heart™ BETA Testing

3Dcardiology (cont...)
PRODUCT FOCUS
CORONARY HEART ™ 17
3dcardiology’s three interactive modes:
‘Screening Disabled’
Th is is how 3dcardiology looks when fi rst started. Th e arrow buttons on your keyboard allow you to rotate around the ‘virtual cath lab’ and the left and right mouse buttons can be used to zoom in and out, allowing you to take a closer look at objects.
Th e mouse cursor can be used to ‘select’ various objects, and a corresponding text panel will give you more information about the selected object.
Th ere is a ‘menu bar’ along the right hand side of the screen which can be moved up and down. Th e menu bar displays various icons allowing the user to access the help system, show/hide anatomical features and equipment, load additional anatomical models, etc.
‘Screening Enabled’
Pressing the ‘spacebar’ on your keyboard will allow you to switch to
‘screening enabled’ mode. Now the arrow buttons on your keyboard will move the frontal and lateral c-arms (they are initially synchronised but can also be moved independently).
In addition the visibility of the lateral c-arm can be toggled by pressing the ‘F6’ function key. Th e left and right mouse buttons will control table height, and your mouse movements now directly translate to fl oating top table movements.
‘MRI Mode’
With a couple of keystrokes, you can turn the ‘virtual cath lab’ into an MRI scanner, enabling instant correlation of fl uoroscopic anatomy with cross-sectional MRI anatomy.
Th e future- we need your help
We are developing 3dcardiology to help cardiologists, radiographers and anyone else responsible for controlling fl uoroscopic equipment during
radiological procedures to work as effi ciently as possible.
However we also believe that the best way to carry our products forward is to ask the users of our products what they think about them- what they like, dislike, want to see added or taken away, etc.
To this end, we hope to encourage an active user community to help us further develop 3dcardiology, so that our users take a lead in its development.
Please visit their websites for more details:
3dcardiology.com
Coronary Heart BETA Testing Review
Th e free version gives only single plane fl uoro. Once at their website, click on Products to read the benefi ts before clicking the link at the bottom to get the free software. As this is free software a licence isn’t required so you will go through a couple of warning messages before the download actually begins. Th e download time will vary for users, but ours took only two minutes using broadband.
Don’t forget to use the function keys to magnify and show specifi c structures.
We believe that there is defi nitely a market for this product particularly for those new to the cath labs, including doctors. Being able to practice on a simulator fi rst to see what the angles show without irradiating the patient and staff is a huge step forward. We particularly liked Th e Bones function that shows when the spine overlaps the anatomy. Users then can rotate the tube to remove the obstruction.Give it a go today.Screenshot 2: Screening Enabled

By Mr Stuart Allen
Revealing Arrhythmias
in the HimalayasCardiac Rhythm Group Manager - Southampton University Hospitals NHS Trust, UKCardiac Rhythm Management Consulting Editor for Coronary Heart.
•
•
18 CORONARY HEART ™

SPECIAL FEATURE
Revealing Arrhythmias
CORONARY HEART ™ 19
The evaluation of patients with unexplained palpitations or syncope, as we know, can be
diffi cult. Traditionally external Holter monitoring is often used to diagnose these events. 24hr holter monitoring is most commonly used and yet provides a very small diagnostic yield. Th is can be improved with the use of prolonged monitoring but is still prone to the problem of electrodes detaching from their skin placement. Prolonged monitoring or the use of external patient activated recorders, even if the electrodes are changed regularly, may still produce diffi culties if the event occurs during dressing or showing etc.
My colleagues and I had an opportunity to study the eff ects of high altitude on arrhythmias when Dr David Woods participated in a British Army expedition to the Himalayas.
To date there has been little study of the eff ects of altitude on the electrophysiological properties of the heart; empirical evidence suggests that at altitude humans are more prone to arrhythmias. A number of cases of sudden cardiac death (SCD) have been documented during high altitude expeditions and in the majority of cases this is attributed to high altitude pulmonary oedema (HAPE), but it is unknown whether the initial or fi nal event was an arrhythmia.
Holter monitoring in extreme temperatures is fraught with technical diffi culties and constraints. Th ese include failure of the surface electrodes to maintain adequate contact, mechanical failure of the holter monitor tape-driving mechanism, and restraints of layers of clothing and temperature. An alternative way of recording arrhythmias at altitude is thus needed.
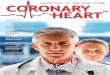
Th e Reveal™ Implantable Loop Recorder (ILR) (shown above) is a
subcutaneous ECG monitor developed by Medtronic Ltd to aid in the diagnosis of patients with unexplained infrequent syncope. Th e device stores segments obtained during symptomatic events in its memory, and storage of these events occur through a manually triggered external patient activator. Th ese events occur with an automatic storage facility in the later model.
Th e quality of the ECG recorded by the Reveal is demonstrated by the two examples on the following page. Two patients, whilst under the care of Southampton General Hospital and not part of the expedition, experienced several events of unexplained syncope for over 12 months, and serial external monitoring failed to uncover the cause. Th is is further highlighted by the examples on the following page.
On the following pages, Fig. 1 demonstrates a 25 second pause, which occurred 5 months post Reveal
implant; the patient subsequently received a pacemaker.
Fig. 2 demonstrates an episode of Torsades de Pointes whereby the patient experienced an attack of syncope 9 months post Reveal implant; this patient received an ICD.
Fig. 2 demonstrates an episode of Torsades de Pointes whereby the patient experienced an attack of syncope 9 months post Reveal implant; this patient received an ICD.
Medtronic Reveal Implantable Loop Recorder - ILR
>>
CORONARY HEART ™ 19

Revealing Arrhythmias (cont...)
SPECIAL FEATURE
20 CORONARY HEART ™
Studies concerned with the eff ects of altitude on cardiac arrhythmias is limited, these have concentrated on either repeated 12 lead surface electrocardiograms or intermittent holter monitoring. It is apparent that altitude is associated with an increased incidence of arrhythmia; however, the majority of these arrhythmias have been relatively benign in nature. It is apparent that the baseline heart rate, (both) when asleep and awake, is increased with altitude, and this is proportional to the degree of elevation. Both atrial and ventricular ectopic rhythms may be observed in healthy subjects at high altitude, and again the degree of elevation plays a role. Ectopy occurs almost always during exertion and tends to diminish with acclimatization ⁽².⁷⁾.
In one study at altitude it was noted that a profound sinus arrhythmia occurred during sleep, and it was felt that this represented a mechanism similar to that found in patients with sleep apnoea. It is important to note that the majority of these studies have monitored the ECG during rest rather than exercise or strenuous activity. It would seem logical that most arrhythmias might occur during the latter as a result of the increased circulating catecholamines and relative hypoxia. It is clear to see why the data is scarce during strenuous activity as palpitations at high altitude have been experienced, but seldom recorded. Th e explorer
D’Orbigny, on the crest of the Peruvian Cordilleras 1826-1834, is quoted as saying “At the least movement, I felt violent palpitations”[1]. Two other studies using single Holter monitoring up to altitudes of up to 5,895 meters showed sinus arrhythmia, occasional ectopy, and ventricular ectopics. A simulated accent to 8,448m by 8 individuals, who spent 40 days in a hypobaric chamber, showed an increase in heart rate and ventricular ectopics, but no signifi cant arrhythmias.
Our study was to use an ILR Reveal recorder implanted in the subcutaneous tissue of 9 healthy volunteers to examine the eff ect of altitude on the heart during an expedition to 6325m in the Himalayas. At altitudes above 5000m all subjects reported palpitations during exercise, abnormal heart rhythms were identifi ed in all, and signifi cant ischaemia in one.
Th e partial pressure of oxygen at Everest base camp (5300m) is half that at sea level, a fact manipulated by the Levy test of the 1940s, which simulated the hypoxic environment of 5500m as a diagnostic tool for coronary artery disease [2]. Hypoxia, sympathetic activation, and alkalosis of altitude predispose to cardiac ischaemia and arrhythmia.
Figure 1: Refer to previous page
Figure 2: Refer to previous page

SPECIAL FEATURE
Revealing Arrhythmias (cont...)
CORONARY HEART ™ 21
Indeed, sudden cardiac death (SCD) accounts for 30% of all deaths during mountain sports at altitude; 642 SCDs over 8 years in Austria alone[3].
Despite these factors a paucity of data exist due to the logistical diffi culties of monitoring the ECG at altitude. Early pioneers recorded interference from the static electricity generated by fl apping nylon tents in the high winds on Makalu.
Current conviction that maximal exercise at high altitude is not accompanied by signifi cant ischaemia or arrhythmia is primarily based on data from a simulated ascent of Everest i.e. resting ECGs on 8 subjects at 5
altitudes and exercise ECGs at two altitudes[2]. Th is accepted wisdom seems incongruous with the 10% of fatalities while trekking in Nepal that are due to heart attacks [4], or the 642 SCDs over an 8 year period in the Austrian Alps[3].
We therefore sought to establish the previously undetermined nature of palpitations at high altitude and the incidence of ischaemia and arrhythmia using an implanted ECG recorder during ascent to high altitude. Nine healthy male volunteers, aged 29.9 ± 5.2 years, had a normal cardiovascular examination, a normal 12-lead ECG, a normal 2-D cardiac echo, and achieved at least stage 5 of the Bruce
protocol without any abnormality pre-expedition.
Implantable loop recorders (ILR, Reveal, Model 9525 Medtronic, USA) were inserted subcutaneously in the left pectoral region under local anaesthesia 6 weeks prior to departure. Subjects fl ew to Kathmandu (1250m) and then Lukla (2800m) before immediately commencing an identical ascent and descent profi le. All subjects reached intermediate camp at 5600m (day 15), six members attained 5700m, four members attained 6070m and two members attained 6325m. No subjects used prophylactic medication against acute mountain sickness. Th e ILR was activated remotely using an
Dr David Woods interrogating a reveal with Mount Everest in the background

SPECIAL FEATURE
Revealing Arrhythmias (cont...) electromagnetic induction unit that ‘freezes’ the loop of ECG recording, which is then stored in the memory ‘bins’ of the unit. Data was downloaded to diskette daily from the ILR using a pacemaker programmer (Model 9790, Medtronic) driven by an altitude modifi ed petroleum generator.
Th e ILR was programmed alternately to record 3 activations (6 minutes pre, 1 minute post) or 1 single activation (40 minutes pre, 2 minutes post).
Devices were activated during episodes of palpitations, and during exercise, rest and sleep. Arterial oxygen saturation was also assessed concurrently during device activations. 263 ECG recordings were made during the expedition, 29.2 ± 2.6 per subject. Analysis of R-R intervals at increasing altitudes demonstrated a progressive increase in mean heart rate both during exercise, at rest, and also mean maximum achieved heart rate during exercise (98.6 ± 24.2, 106.7 ± 27.8, 144.1 ± 13.7, and 152 ± 23.8, mean±sd, at 2-2999m, 3-3999m, 4- 4999m, 5-5999m respectively).
All subjects experienced palpitations during exercise above 5000m with 2 symptomatic episodes at rest (5,600m and 6300m).
Analyses of all symptomatic recordings were found to correlate with sinus tachycardia. In one subject an episode of asymptomatic atrial fl utter with 2:1 conduction was observed for 8.5 minutes immediately after a period of severe exertion at 4500m (SaO2 76%).
Sleep recordings revealed sinus arrhythmia in all individuals with non-conducted ectopic p waves in one subject. Another subject demonstrated sinus arrhythmia during exercise (not previously reported at altitude). In one individual, during exercise at 6300m, there was clear evidence of a change in repolarisation associated with dramatic
ST segment depression (SaO2 59%). It is possible that these repolarisation changes represent cardiac ischaemia.
In two tracings derived from asymptomatic individuals during exercise, it was not possible to clearly identify the underlying cardiac rhythm. In both cases analysis of the apparent R-R intervals identifi ed a frequency of 300 beats per minute consistent
with a diagnosis of atrial fl utter with 1:1 conduction. It is possible that these tracings represent artifact but extensive provocation during both rest and exercise post-expedition failed to reproduce such a pattern.
Th is expedition demonstrated that the implantable loop recorder is eff ective for recording ECGs even under extreme conditions and is more
Atrial Flutter post exercise at 4500m, oxygen saturation 76%
Atrial flutter 1:1 conduction on exercise at 4,600m, oxygen saturation 87%
22 CORONARY HEART ™

SPECIAL FEATURE
Revealing Arrhythmias (cont...)
favourable than conventional holter monitoring for recording the possible arrhythmic eff ects of high altitude. Th e ILR demonstrated abnormal heart rhythms in all subjects and signifi cant repolarisation changes in one. Above 5,000m all subjects reported palpitations during exercise that were associated with sinus tachycardia.
Current evidence regarding the risk of ischaemia and arrhythmia at high altitude is based on a paucity of data and is incongruous with the rate of SCD. Further evaluation is required, particularly in the elderly who account for 15% of the 100 million visitors to high altitude annually. Th ese fi gures are of real concern due to the fact that up to 60% of elderly individuals in Western societies have signifi cant coronary lesions at autopsy [5].
Acknowledgements:
Dr Paul Roberts ,Consultant Cardiologist and Electrophysiologist, Southampton General HospitalDr David Woods, Consultant in Endocrinology and Diabetes, Northumbria and Newcastle.Th e members of the expedition from the Army Training Regiment, Lichfi eld, UK.
References:
Bert P. La Pression Barométrique, recherches de physiologie expérimental. Masson, Paris (1878). English translation (1943) by Hitchcock MA and
1.
Hitchcock FA, College Book Co., Columbus, Ohio, p37.
Malconian M, Rock P, Hultgren H, et al. Th e electrocardiogram at rest and exercise during a simulated ascent of Mt. Everest (Operation Everest II). Am J Cardiol. 1990; 65: 1475-1480.
Burtscher M, Mittleman MA. Time-dependent SCD risk
during mountain sports changes with age.
2.
3.
Circulation. 1995; 92: 3151-3152.
Shlim DR, Gallie J. Th e causes of death among trekkers in Nepal. Int J Sports Med. 1992; 13: S74-6.
Levine BD, Zuckerman, JH, deFilippi CR. Eff ect of High-Altitude Exposure in the Elderly. Circulation. 1997; 96: 1224-1232.
4.
5.
Sinus arrhythmia/non conducted p -wave during sleep at 4,300m, oxygen saturation 84%
Repolarisation Abnormality. Significant ST segment depression seen at 6300m (59% oxygen saturation).
(1878). English translation Everest II). Am J Cardiol. 1990; deFilippi CR. Eff ect of High-(1878). English translation (1943) by Hitchcock MA and
Everest II). Am J Cardiol. 1990; 65: 1475-1480.
Burtscher M, Mittleman MA. Time-dependent SCD risk
during mountain sports changes with age.
3.
deFilippi CR. Eff ect of High-Altitude Exposure in the Elderly. Circulation. 1997; 96: 1224-1232.
CORONARY HEART ™ 23

CARDIAC SITE VISIT
Massachusetts General Hospital
24 CORONARY HEART ™
The Massachusetts General Hospital (MGH), located in Boston is the third oldest
general hospital in the United States, founded in 1811. Today, the 898-bed hospital is also the oldest and largest in New England, and has developed into a world renowned medical center. Th e MGH conducts the United States’ largest hospital based research program, and forms the oldest and largest teaching hospital of the Harvard Medical School.
All of these achievements don’t go unnoticed with the MGH named one of the country’s best hospitals by U.S. News and World Report for the sixteenth year, ranking third nationwide in July 2005. In 2006 the MGH Heart Center was ranked number one in New England and number four in America by the same organisation.
Th e following questions have been answered by Sharon McKenna, the Nurse Manager for the Knight Center for Interventional Cardiovascular Th erapy at MGH.
1) Size of hospital and cath lab facilities?
Massachusetts General Hospital is the oldest and largest hospital in New England with a capacity of 898 beds. Th e cardiac cath lab has six procedure rooms. Two of these rooms are biplane. Th ree of the rooms are hybrid rooms that are capable of both coronary and peripheral procedures.
UNITED STATES OF AMERICA
Christine Joyce, RN with a patient in the post procedure area
ADDRESS
MAP
Heart Center - Cath LabMassachusetts General Hospital 55 Fruit Street Boston, MA 02114 United States of America
FAST FACTS
MGH Heart Center ranked Number 4 in USA by US News.
Teaching hospital for Harvard Medical School
36 Cath Lab Staff
6 Procedure Rooms
Combination of peripheral and coronary procedures
1.
2.
3.
4.
5.
>>

Massachusetts General Hosp.
CARDIAC SITE VISIT
CORONARY HEART ™ 25
2) Staff numbers?
There are currently 20 nurses and 16 techs in this lab. The techs are a combination of RTs and CVTs. Some but not all are RCIS certified.
3) Main staff roles?
Nurses administer medications including conscious sedation. The RTs and CVTs are cross-trained to perform similar duties, including panning and driving the table. They are also responsible for set up of interventional equipment such as rotational atherectomy, rheolytic thrombectomy, laser, and, pressureand flow wires.
4) Procedures?
This lab performs diagnostic coronary and peripheral angiograms (including carotid, renal, and lower extremities), RHC, LHC, heart biopsies, alcohol septal ablations, PFO and ASD closures, valvuloplasties, intracardiac ultrasound, and coronary interventions (such as angioplasties, stents, rotational and direction atherectomy, rheolytic thrombectomy, laser, intravascular ultrasnound, and pressure and flow wires). Peripheral interventions are also performed. There is a separate three room electrophysiology/pacer lab that is not part of this department.
5) Procedures performed in a year?
We do more than 6,000 procedures a year.
6) Some challenges in setting up the department?
This department has existed for ten years in its present location and over ten years in the location prior to this one. The staff continues to evolve as people move along their career paths. Challenges exist in trying to keep the staff motivated to perform as a team in such a high stress department. Keeping staff current in the latest technologies and research is also a challenge.
UNITED STATES OF AMERICA
The new Philips hybrid roomFrom left, Dr Shaffiq Mandami and Dr M. Ashequl Islam both peripheral vascular
interventional fellows. Dr Ken Rosenfield with the red thyroid collar.On the right is Russell Schmitt (CV tech). >>

CARDIAC SITE VISIT
26 CORONARY HEART ™
7) Surgical back-up?
There is cardiac and vascular surgical back up for complications of our procedures in the hospital.
8) Day cases?
There are between ten and twenty cases a day that come from home for their procedures. Some of these patients return home after a one to four hour recovery period after the procedure. Some are admitted after the procedure.
9) New procedures recently implemented into the department?
We have started carotid stenting within the last few years. Alcohol septal ablations are also relatively new. We are expecting to start the Tandem heart procedure and a percutaneous valve program soon.
10) Alliance’s with other hospitals for treating patients?
In 1994 our hospital joined with other major hospitals to form Partners Healthcare System, Inc. This system provides integrated, cost effective health care delivery.
11) Private cases? Any special considerations?
We do allow Private cardiologists to come to our lab and perform catheterizations on their own patients. We try to accomodate special booking requests when the cases are booked in advance. For emergent cases we absorb these into the schedule as we would any emergency.
12) Haemostasis?
The lab staff are responsible for pulling all diagnostic sheaths. We use a combination of closure devices such as Angioseal, Perclose, and Starclose.These are not suitable for all patients, so the remaining sheaths are pulled by the staff. We use both manual compression and clamps depending on the pullers preference. Interventional sheaths are managed on the inpatient units.
13) Measures implemented to cut costs in the lab?
Our new inventory system has reduced costs by streamlining our par levels and reducing the waste of expired equipment. We have recently changed to a premix flush that reduces the amount of set up time for the staff. It also reduces the amount of waste because we only open what we need instead of premixing larger volumes that may get wasted.
Massachusetts General Hosp.UNITED STATES OF AMERICA

CARDIAC SITE VISIT
CORONARY HEART ™ 27
14) Inventory management?
We have an inventory manager who is responsible for maintaining the equipment in this department. We also use a web based inventory scanning system that helps maintain our par levels by notifying us of low stock levels and impending expiration dates.
15) Staff cross-training?
The RN, RT, and CVT staff are all cross trained. All staff are responsible for prep and drape, circulating, inventory control/equipment pass off, monitoring of vital signs, hemodynamic measurements, and documentation. Staff will also scrub in when neccessary but this is a teaching facility so it happens rarely. All staff are BLS and ACLS certified.
16) Continuing education programs for staff?
There are a wide variety of continuing education options for RNs, RTs, and CVTs. Some unit based product inservices provide CEUs. There are also hospital wide options that are free for employees.
17) Training for new employees?
Our new hires receive a minimum of six weeks orientation. The orientation is tailored to fit the past experience of the employee.
18) Staff competency checks once employed?
There is annual recertification training for some equipment and point of care testing machines (ACTs and hemoximetry). BLS, ACLS, and conscious sedation training is every two years. This is all unit based training.
19) Training facility for cardiac registrars / fellows?
We have a very active training program for both diagnostic and interventional cardiac fellows (American version of registrars).
Massachusetts General Hosp.UNITED STATES OF AMERICA
Siemens Hybrid RoomA group photo of the team whom
make up the Knight Center for Interventional Cardiovascular
Therapy at MGH
>>

CARDIAC SITE VISIT
28 CORONARY HEART ™
20) Any cardiac registrars / fellows from other countries?
We have had fellows from all over the world. Canada, Australia, South America, Europe, Africa and the Middle East have all sent doctors for training at our teaching institution.
21) What is the best part of working at your facility?
Th is a dynamic fast paced environment that never ceases to teach us something
new. We have the honor of working with internationally renowned doctors in one of the most renowned teaching and research institutions in the world. Our cath lab team is exceptional in every sense of the word and we are proud of the care that we provide to our patients. Th e best part of this department are the people that work here.
Visit online: www.massgeneral.org/heartcenter for more information on this facility
Boston is the capital city in the state of Massachusetts, and the largest city in New England on the NE coast of the USA. It is one of the oldest cities, being founded in 1630, with a population of approximately 600,000. The city has a fascinating history with the Boston Tea Party of 1773 known globally for what became a catalyst for the American Revolution.
Th ings to see and do:
Freedom Trail:Take a stroll along this 2.5 mile red brick path past 16 nationally signifi cant historic sites, including those related to the American Revolution.
Boston Common:Take a ride on a swan boat, or simply just chill out on the 75 acres of gardens (dating back to 1634), located in the heart of downtown Boston.
Massachusetts General Hosp.UNITED STATES OF AMERICA
From left, Dr Igor Palacios and Vishal Gupta. In the red lead is Patricia Gannon, RRT and in the blue lead is Carolyn Cain, RN.
28 CORONARY HEART ™28 CORONARY HEART ™
WHY BOSTON?
Custom House Clock
Boston Skyline at Night
28 CORONARY HEART ™

CARDIAC SITE VISIT
Coff s Harbour HealthCampus
CORONARY HEART ™ 29
All around the world new cardiac cath labs are springing up, some in the big cities, whilst others
are in regional towns. One thing they have in common is that they each share the same diffi culties; starting everything from scratch.
Here at Coronary Heart, every so often we will bring you reviews like this, showing how some departments
have succeeded, and the challenges they have overcome. We hope that new departments can gain fresh ideas, ultimately improving the workplace for staff and patients.
Goodluck!!
Coff s Harbour is a 202 bed hospital on the Mid North Coast of New South Wales, Australia. It is part of the North
Coast Area Health Service, combining the Northern Rivers and Mid North Coast Areas.
Th e Coronary Angiography Unit was opened on the 28th September, 2006. It currently operates two days per week undertaking mainly day only angiograms. It is a self contained Unit with a four bed recovery area and direct admission and discharges from the
AUSTRALIA
Brand New Cath Lab
Left to Right: Front row: Jon Waites (Cardiologist)2nd Row: Emma Palmer (RN), Lyn Hales (Clinical Nurse Educator),
Caroline Blaxland (RN), Back Row: Julie Smith (Radiographer), Trish Barnes (RN), Heather Purvis
(RN), David Law (Cardiac Tech), Maura Kelly (Nurse Unit Manager),
>>
ADDRESS
FAST FACTS
MAP
Opened September 2006
Currently operates two days per week
1 Cath Lab
10 Staff (variable)
Located in one of Australia’s favourite holiday locations
1.
2.
3.
4.
5.
Coronary Angiography Unit,Coffs Harbour Health Campus,345 Pacific Highway,Coffs Harbour, New South Wales, 2450, Australia
CORONARY HEART ™ 29

Coffs Harbour Health CampusCARDIAC SITE VISIT
30 CORONARY HEART ™
Unit. It is supported in the hospital by an inpatient stress testing department and 10 bed combined ICU/CCU.
The following questions have been answered by Maura Kelly, Nurse Unit Manager of the Cath Lab.
1) Cath lab facilities?
We have one Siemens Axiom Artis Lab with a four bed recovery area. There are three chairs that are used for patient admission/preparation as well as part of the recovery phase.
2) Staff numbers?
We have one full time Nurse Unit Manager, and 6 part time RN’s.We have one part time radiographer based in the Unit as well as one casual relief radiographer. We are completely separate from the radiology department. Haemodynamic monitoring is looked after by the Cardiac Technician/ Scientific Officer who is employed on a consultancy basis.
3) Main staff roles?
The RN is responsible for patient admission and preparation, as well as rotating through scrub, scout and recovery of the patient. The scrub nurse is responsible for the pressure injector (all coronaries are injected by pressure injector), or hand injections if required.
The nurses are responsible for sheath removal once in recovery. The scrub nurse usually follows the patient out to recovery for sheath removal for continuity of care. Radiographers are responsible for imaging. The Cardiologist is responsible for the manoeuvring of the camera and table.The Cardiac technician is responsible for all monitoring, valve studies etc.
4) Procedures?
Having recently opened in September 2006, we currently perform diagnostic angiograms only.
5) Procedures performed in a year?
We are currently averaging 60 cases per month, and are aiming for 700-800 for the year.
6) Emergency cases?
We currently do not do emergency cases, but we do have a balloon pump in the Unit for emergencies.
7) Day cases?
70% of patients are performed as day only cases. The remainder are current inpatients.
8) Surgical back-up?
Coffs Harbour is a rural Cath Lab that has no surgical backup. If needed, patients are transported via Air Ambulance to a tertiary centre in Sydney, 500 kms away.
9) Do patients arrive via air ambulance, helicopter etc, from outlying towns?
Patients from our feeder hospitals arrive via road ambulance or internal transport for day only procedures.
10) Private cases? Any special considerations?
We are a Public Hospital and primarily do public patients; however we do approximately 20% as private cases.
11) New procedures recently implemented?
Being a completely new service to the area, everything is new and has been a big learning curve for the hospital.
The Siemens Axiom Artis Lab Left to right: Caroline Blaxland (RN), Heather
Purvis (RN), Dr Jon Waites (Cardiologist).
AUSTRALIA

CARDIAC SITE VISIT
Coffs Harbour Health Campus
CORONARY HEART ™ 31
12) Inventory management?
Inventory is managed by the Unit Manager or RN delegate on a weekly basis. All stock is ordered online. Prosthetics and some interventional products are managed on a consignment basis.
13) Haemostasis?
RN’s remove the sheaths, and use Femostops and CompressARs depending on patient needs and RN preference. Digital pressure is rarely used. Angioseals are also used depending on patient need.
14) Measures implemented to cut costs?
All interventional balloons and stents are on consignment. Otherwise, careful monitoring of budget.
15) Some of the challenges setting up the department?
Coffs Harbour is the fourth rural Cath Lab Site in New South Wales to be established under a Rural Health Plan. A purpose built extension to the 5 year old hospital was needed to house the new Unit. This provided the challenge of building and commissioning the new Unit under budget within a short time frame.
Finding experienced staff to work in the Unit was also a challenge due to geographical isolation from the major tertiary centres and limited number of staff that had worked in the Cath Labs previously who were currently employed in the hospital. Added to this was the inability to offer full time positions in the Unit at the present time, which was no incentive for prospective staff to relocate to the area.
The other major challenge has been the education process for General Practitioners, Hospital Staff and the community regarding the safety and efficacy of diagnostic angiograms without on site surgical backup. Previously, all patients requiring angiography had been flown out to Sydney, and it has been a steep learning curve in some areas to change to the idea of onsite angiograms.
16) Cross Training?
All nurses and radiographers are being trained in haemodynamic monitoring. We also encourage the Radiographers
and Cardiac Technician to cross train in the scouting role.
17) Training new employees can expect to receive?
Full orientation to the Unit, with an orientation handbook covering all aspects of angiography, and PCI with competencies for staff to achieve. In-service prior to being buddied up with a senior staff member for training in all roles in the Unit.
18) Continuing education programs available to staff?
Staff are encouraged to attend any in house education, as well as accessing NSW College of Nursing and Area Health service courses as they feel the need. They are also encouraged to attend local and international meetings with support.
AUSTRALIA
Left to right: Caroline Blaxland (RN), Lyn Hales (Clinical Nurse Educator), Maura Kelly (Nurse Unit Manager), Dr Jon Waites
(Cardiologist), Julie Smith (Radiographer), David Law (Cardiac Tech), Trish Barnes (RN), Emma Palmer (RN), Heather Purvis (RN)
Dr Jon Waites (Cardiologist) >>

Coff s Harbour Health CampusCARDIAC SITE VISIT
19) Competency checks staff undergo once employed?
Annual competencies include Advanced Life Support, whilst staff must also be assessed for competency in IV cannulation, scrubbing, scouting, recovery and sheath removal.
20) New training initiatives implemented?
Prior to opening the Unit, we sent our RN’s to Nepean Hospital, in Sydney, for training in their Unit. We are very grateful to them; they did a wonderful job and were very accommodating. We also accessed the University of New South Wales School of Rural Health training
21) Growth potential of the Unit?
Currently, we have one Cardiologist
performing diagnostic angiograms. He is currently the only Cardiologist covering an area with over 140 000 people.
Th ere is a signifi cant elderly population in the area, and previously, the hospital had needed to send to Sydney over 800 people per year for diagnostic angiograms. Th is did not include those who needed interventional procedures, and we expect the numbers of people requiring purely diagnostic angiography will increase with the establishment of the Unit.
We are in the process of advertising for and recruiting another cardiologist with interventional skills, and plan to hopefully start interventional cases after that.
22) Training facility for cardiac registrars (fellows)?
No.
23) What is the best part of working at your facility?
Wonderful staff , and a great new Unit in a beautiful part of Australia.
Surrounded by banana plantations, this small city of only 60,000 people, lies midway between Sydney and Brisbane on the east coast of Australia. It is a popular location for families wanting a change from big city life with activities ranging from sailing, golf, and rafting, to simply lying on a beach enjoying the sun.
Th ings to see and do:
Solitary Islands Marine Park:NSW’s largest marine protected area is one of Australia’s top scuba diving sites. 550 fi sh species, 4 turtle species, and 90 species of coral, and of course humpback whales.
Dorrigo National Park:Th ese easily accessible rainforests are located on the edge of the Great Escarpment. Walk through the canopy on boardwalks, or follow the trail past stunning waterfalls surrounding the now extinct Ebor Volcano.
AUSTRALIA
Left to right: Heather Purvis (RN), Jon Waites (Cardiologist), Julie Smith
(Radiographer),
Photo: Robbi Newman.
Photos Courtesy Tourism New South Wales
Photo: Ashley Mackevicius
Coffs Harbour Marina
Rafting near Coffs
WHY COFFS HARBOUR?
32 CORONARY HEART ™

EP EDUCATION
ADENOSINE in ELECTROPHYSIOLOGY
An important drug you will come across in electrophysiology is ADENOSINE
Th is article introduces uses of adenosine in electrophysiology. It does not cover indications/contraindications or dose, for which local/national guidelines should be consulted.
Adenosine is a naturally occuring compound that plays an important role in many biochemical processes. It inhibits calcium channels causing a decrease in the conduction velocity of the atrioventricular (AV) node. At suffi cient dose this causes transient AV nodal block, an action that can be useful to the electrophysiologist.
Adenosine also slows the rate of fi ring of pacemaker cells, resulting in sinus bradycardia. Because it is rapidly metabolised these eff ects last ony seconds.
Because the depolarisation of cardiac muscle cells is less dependent on calcium channels, atrial/ventricular tissue is much less sensitive to adenosisne.
Accessory pathways including those responsible for Wolff Parkinson White syndrome are comprised of normal cardiac muscle cells so are not usually aff ected by adenosine.
Summary of the electrophysiological eff ects of adenosine:
Profound eff ect on “pacemaker” cells
At suffi cient dose blocks the AV node
Will terminate a re-entry circuit which involves the AV node
Doesn’t aff ect most accessory
•
•
•
•
pathways
May terminate some focal atrial and focal ventricular tachycardias
Use of Adenosine in Electrophysiology
Adenosine is used in two ways. Firstly, for non-invasive termination of tachycardias and second, in the EP lab to unmask accessory pathways or confi rm their ablation. Th e eff ect of adenosine given in an attempt to terminate tachycardia can provide useful clues about the nature of the arrrythmia.
Th erapeutic use: To terminate symptomatic tachycardias in an emergency room setting
Adenosine is often chosen to terminate tachycardias in particular narrow complex tachycardia because it blocks the AV node - an essential part of the re-entrant circuit for two very common arrhythmias - AV nodal re-entrant tachycardia (AVNRT) and AV re-entry
•
tachycardia (AVRT). Th e very short half life is also useful.
Diagnostic information provided by adenosine
Termination of tachycardia by adenosine suggests involvement of the AV node in a re-entry circuit. Th e AV node is one limb of the re-entrant circuit in AVNRT and AVRT.
Failure to terminate indicates either that the dose was insuffi cient to cause AV nodal block or that the AV node is not a requisite structure for maintenance of the particular tachycardia.
Th e AV node is not essential for maintenance of atrial or ventricular tachycardia and so these arrythmias may continue in the presence of AV nodal block. I have stressed may continue because, to make things awkward some atrial and indeed some ventricular tachycardias are terminated by adenosine (see next page).
Fig. 1 AV nodal block on administration of adenosine in the absence of an accessory pathway. There are more atrial than
ventricular signals – note the relationship of the high right atrial signal (HRAp) and the QRS complexes on the ECG leads (at the
bottom).
ADENOSINE in
Written By: Ian Wright, St. Mary’s Hospital, London, UK
>>CORONARY HEART ™ 33

EP EDUCATION (cont...)
34 CORONARY HEART ™
When atrial tachycardia is conducted to the ventricles in a 1:1 relationship the frequent QRS complexes and T waves can obscure the p waves and make diagnosis diffi cult or impossible.
By introducing a higher degree of AV block adenosine allows p waves to be seen. Continuation of tachycardia with more p waves than QRS complexes is indicative of atrial tachycardia
and the p waves morphology can be ascertained. Atrial fl utter may present with 1:1 conduction (see fi g 3). Th is is more common when the fl utter rate is somewhat slower than usual or has been slowed by anti-arrhythmic medication.
Administration of adenosine often allows underlying fl utter waves to be seen and a diagnosis to be made. Flutter is not terminated by adenosine but changing AV node conduction from 1:1 to 2:1 reveals the fl utter waves in the inferior leads (see Fig 5).
Use of Adenosine during EP and Ablation Procedures
Electrophysiologists use the ability of adenosine to selectively block the AV node to reveal “hidden” accessory pathways. A pathway may be hard to identify because it has conduction and refractory properties similar to the AV node. Sometimes during an ablation attempt an accessory pathway becomes diffi cult to detect because of damage it has sustained during energy application.
By blocking AV node conduction adenosine can reveal accessory pathway conduction and can help confi rm successful pathway ablation.
Figure 5 shows the surface ECG during administration of adenosine in a patient with Wolff Parkinson White (WPW) following a number of energy applications. Although there is a suspicion of remaining pre-excitation even before adenosine (see V2), slowing/block in AV node conduction caused by adenosine reveals a more overt WPW appearance. Note also the slowing of the sinus rate also due to adenosine.
In the tachycardia above there are more p waves than QRS
complexes. Th e rhythm is atrial tachycardia. AV block caused by adenosine will not terminate this arrhythmia because the tachycardia is confi ned to the atrial tissue – you can already see the rhythm continuing despite alternate atrial beats not being conducted to the ventricles. However, adenosine terminates many focal atrial tachycardias by its eff ect on cAMP, which is involved in the mechanism (cAMP dependent triggered activity) behind many such arrhythmias. Macro-reentrant atrial rhythms such as atrial fl utter are not
terminated by adenosine.
Termination of an atrial tachycardia with adenosine strongly suggests a focal rather than a re-entrant mechanism.
In a similar way adenosine may sometimes terminate focal ventricular tachycardia where the mechanism is cAMP dependent triggered activity. Where the mechanism for VT is re-entry, adenosine is ineff ective. Re-entry is usually the mechanism where myocardial scarring is present (for example post MI).
Adenosine in EP
Fig 2. Atrial and Ventricular Tachycardia
Fig 3. Atrial Flutter with 1:1 Conduction

EP EDUCATION (cont...)
Adenosine in EP
CORONARY HEART ™ 35
Intra-cardiac signals
Figure 6 (bottom) documents the administration of adenosine. Th e fi rst two QRS complexes on the ECG (bottom left) are narrow and appear normal. Th e last two are broad with a right bundle branch block appearance. Look at the middle ECG complex – the QRS morphology is a mixture of the other two – a fusion complex. As is often the case, the His electrogram is key to understand EP. Th e AH interval, which represents conduction through the AV node is normal for the fi rst two beats but starts to lengthen
on the third. On the last two beats the His spike apparently disappears (it has probably fused with the ventricular component labelled V).
Now look at CS 11-12. Th ere are two components for each beat – the fi rst is sharp (the atrial component) and the second smaller and more rounded (the ventricular component). If you run your eye along the trace you notice that the interval between these left atrial and left ventricular components stays constant.
Th is patient has a left-sided accessory pathway yet there is little evidence of this on the surface ECG. Adenosine has caused progressive slowing of the AV node but pathway conduction remains constant. Consequently more and more of the ventricles are activated via than pathway, resulting in fi rst a fused and then a pre-excited complex.
Fig 4. Administration of Adenosine
Fig 5. Administration of Adenosine in a patient with Wolff Parkinson White
Fig 6. Administration of Adenosine

EP EDUCATION (cont...)
36 CORONARY HEART ™
Th e previous examples document the use of adenosine to demonstrate anterograde (atrium to ventricle) accessory pathway function. However some accessory pathways, known as concealed pathways only conduct retrogradely (ventricle to atrium). For adenosine to be useful in determining the presence or absence of such pathways it must be administered during ventricular pacing instead of sinus rhythm. VA block demonstrates the absence of a concealed accessory pathway in the same way that AV block demonstrates absence of an anterograde pathway.
Figure 7 shows adenosine given at the end of an ablation to confi rm procedural success. It is given during continuous ventricular pacing (note the surface ECG). Th e fourth V paced beat is not conducted to the atrium (there are no corresponding atrial signals) due to retrograde block in the AV node. (Note - the third beat is probably conducted via the slow AV nodal pathway).
Figure 8 In this case the retrograde activation sequence was very
similar to that during normal AV node conduction because of the anatomical location of the pathway (right anterior/right antero-septal). Continuation of VA conduction despite anterograde AV block added to the evidence for an accessory pathway.
Adenosine is administered and V pacing initiated immediately anterograde AV block is observed. Th ere is VA conduction at the onset of pacing and if the AV node is blocked this conduction must be taking a
diff erent route- over an accessory pathway.
© Ian Wright, Jan 2007
Adenosine in EP
Fig 7. Administration of Adenosine to confirm procedural success
Fig 8.
Caution: Initiatiation of Atrial FibrillationBy causing a shortening of the atrial refractory period adenosine can promote atrial fi brillation, which may initiate polymorphic VT or VF in some patients with WPW syndrome. Evidence of the pathway may not be present in tachycardia, which may
have a narrow complex (orthodromic AVRT).

CORONARY HEART ™ 37

MEDICAL IMAGING
RAO 30 for RCA
Objectives:
Th is angle is usually the third in the series of projections to demonstrate the right coronary artery. (Refer to Edition 4 for the fi rst two views of the RCA). It is used to show the mid RCA perpendicular to the LAO 40 view. As the RCA is located more posterior compared to the LCA, radiographers who have not adjusted the table height to compensate for the new isocenter will have to pan the table left in order to fi nd the origin of the RCA in RAO 30. Th is occurs after the fi rst two LAO views are performed.
Th is projection should not be used to demonstrate the proximal and distal RCA due to major foreshortening. However depending upon the length of the PDA, it can be a useful projection for possible PCI in the mid / distal PDA.
If there is a blockage in the LAD, collateral-fi lling will occur from the RCA. Th e length of the LAD is seen without foreshortening. Pan further to the left at the distal PDA to see it fi lling.
Catheter Positioning On-Screen:
Th e catheter should be positioned in the middle of the screen close to the top before the start of the acquisition.
Alternatives:
Less RAO (eg. RAO 15):
Th is projection has the potential of improving visualisation of the proximal PDA where it bifurcates with the PLV.
More RAO (eg. RAO 50):
Increasing your angle to this degree begins to open up the proximal and
distal RCA. It also overlaps the RCA on the PDA. Here’s
a secret: if you want to see the RCA origin specifi cally, it is best to use a spider view (LAO 40/CAU 20),
magnify if required and collimate in to
the area of interest.
RAO 30More RAO (eg. RAO 50):
Increasing your angle to this degree begins to open up the proximal and
distal RCA. It also overlaps the RCA on the PDA. Here’s
a secret: if you want to see the RCA origin specifi cally, it is best to use a spider view (LAO 40/CAU 20),
magnify if required and collimate in to
the area of interest.
RAO 30
RCA Right Coronary
AM Acute Marginal
PDA Posterior Descending
PLV Posterior Left Ventricular
MODEL: Rob Edwards
38 CORONARY HEART ™

MEDICAL IMAGING
LAD to Pulmonary Artery Fistula. On image 2 it is possible to see the small jet of contrast into the Pulmonary Artery, which was only seen in a couple of frames and nearly missed. Th e jet is overlapped in Image 1.
Treatment: As it was only small, the Cardiologist decided to leave it, however as the patient was being operated on for a valve replacement, the cardiac surgeons fi xed it.
Hot Tip!!When designing a new lab or getting new
equipment installed, it is a good idea to have a circle placed on the floor outlining the collision zone of the imaging equipment. This is particularly useful for all staff in the lab to know where it is safe to place drip stands and anaesthetic trolleys so they don’t get damaged.
Send us your interesting cases, lab studies, or hot tips to [email protected] or visit our website for more details at:www.coronaryheart.com
Image 1 Image 2
Right: Red circle and different colour vinyl floor to show the collision zone of the GE Innova
2100 at St Thomas’ Hospital, London, UK
Interesting Case
PHOTO: Tim Larner
CORONARY HEART ™ 39

Conferences 2007CONFERENCES
40 CORONARY HEART ™
March 11-1523rd Annual Cardiovascular Conference (CSS)Location: Lake Louise, CanadaWebsite: www.css.ca
March 21-23ACCA 18th Cardiovascular Administrators’ Leadership ConferenceLocation: New Orleans, USAWebsite: www.aameda.org
March 22-232007 ACVP Cardiovascular Leadership ConferenceLocation: New Orleans, USAWebsite: www.acp-online.org
March 24-27American College of Cardiology 56th Annual Scientifi c SessionsLocation: New Orleans, USAWebsite: www.acc.org
April 17-20Trends in Trauma and Cardiovascular NursingLocation: King of Prussia, PA, USAWebsite: www.aacn.org/Chapters/sepa.nsf/TrendsSplashPage
April 18–21Concepts in Contemporary Cardiovascular MedicineLocation: Houston, TXWebsite: www.cv-concepts.org
April 29 - May 28th International Conference of Nuclear Cardiology (ICNC8)Location: Prague, Czech RepublicWebsite: www.escardio.org
May 4-5Challenges in Cardiology VIILocation: Brisbane, QLD, AustraliaWebsite: www.heartfoundation.com.au/qld
May 9-12Heart Rhythm 2007Location: Denver, CO, USAWebsite: www.heartrhythm2007.org
May 9-12SCAI 30th Anniversary Annual Scientifi c Scientifi c SessionsLocation: Orlando, FL, USAWebsite: www.scai.org
May 22-25EuroPCR CongressLocation: Barcelona, SpainWebsite: www. europcr.com

Conferences 2007CONFERENCES
CORONARY HEART ™ 41
June 4-7British Cardiac Society Annual Scientifi c ConferenceLocation: Glasgow, UKWebsite: www.bcs.com
June 7-10The 2007 Port Douglas Heart Meeting & ExpoLocation: Port Douglas, QLD, AustraliaEmail: [email protected]
June 9-12Heart Failure 2007Location: Hamburg, GermanyWebsite: www.escardio.org
June 18-21American Society of Echocardiography - 18th Annual Scientifi c SessionsLocation: Seattle, WA, USAWebsite: www.asecho.org
June 24-27EuroPaceLocation: Lisbon, PortugalWebsite: www.escardio.org
June 28 - July 11st World Congress on Controversies in Cardiovascular DiseasesLocation: Berlin, GermanyWebsite: www.comtecmed.com/ccare
August 9-1255th ASM of the Cardiac Society of Australia and New ZealandLocation: Christchurch, NZWebsite: www.csanz.edu.au
October 20-24Canadian Cardiovascular Congress 2007Location: Quebec City, CanadaWebsite: www.css.ca
October 22-26TCT 2007: Transcatheter Cardiovascular TherapeuticsLocation: Washington DC, USAWebsite: www.tctmd.com
October 29-312007 Heart Rhythm UK CongressLocation: BirminghamWebsite: www.ukheartrhythm.org.uk
November 4-7AHA Scientifi c SessionsLocation: Orlando, FL, USAWebsite: scientifi csessions.americanheart.org
November 25-30RSNALocation: Chicago, USAWebsite: www.rsna.org

Concepts in Contemporary Cardiovascular MedicineApril 18 – 21, 2007
George R. Brown Convention Center, Houston, Texas
www.cv-concepts.org
Please plan to join us in April at Th e Contemporary Cardiovascular Medicine Symposium is an exceptional conference for invasive cardiovascular professionals. Now in its 6th year, the symposium is designed to serve as a comprehensive update on the emerging, as well as the accepted, techniques and methodologies for treating patients in all areas of cardiovascular disease. World renowned faculty will present didactic lectures, workshops, and discussions, and live case presentations from major cardiovascular centers. Topics for this year’s conference are: Congestive Heart Failure, Lower Extremity Revascularization, Venous Interventions, Peripheral Vascular Disease, Valvular Heart Disease, Coronary Artery Disease, Adult Congenital Heart Disease, Cerebrovascular Disease, Cardiovascular and Vascular Surgery, Debates in Cardiovascular Medicine
Saturday afternoon will be devoted to nurses and techs, with presentations addressing
our unique interests. Not only will you receive the latest and greatest information about invasive cardiology, SICP members will be given a 50% discount for the whole conference!
New this year is the Nurse/Tech dinner presentation that is a great bargain for SICP members at only $20.00.
I am very proud for the SICP to be a part of this exciting conference. I
extend a sincere “Th ank You!” to Zvonimir Krajcer, MD, Richard Smalling, MD, PHD, Steven R. Bailey, MD, and Alan Lumsden, MD for their support of the invasive cardiovascular professionals who work in cardiac catheterization laboratories.
Please stop by the SICP booth to say hello.Lynne Jones, RN, RCIS, FSICPPresident, SICP
PREVIEW
42 CORONARY HEART ™
The Society of Invasive Cardiovascular Professionals will present a 2 day Registry Review Course conducted by a few of our premier review course presenters.
This course is designed to review information for the CCI RCIS invasive registry exam. This course will help you identify areas in which you need to concentrate your self study, or will serve as an overview for those who are prepared to take the exam.
Hemodynamics, Calculations, Cardiovascular A&P, Interventions, Pharmacology, Equipment and Instrumentation, Radiation Safety, Patient Care and Assessment
Saturday...................................................................8:00 am - 4:00 pmSunday .....................................................................8:00 am - 4:00 pm
For complete schedule details and instructor information, please visit www.sicp.com
The Review Course fee for members is $70 and $120 for non-members. 2007 SICP Membership is included with the cost of a non-member registration.
The GCNKY is generously hosting this course which allows for a favorable registration fee.
Name _________________________________________________________________ Credentials ______________________________________
Facility _________________________________________________________________________________________________________________
Address ________________________________________________________________________________________________________________
City ____________________________________________________State __________ Zip _____________________________________________
Phone __________________________________________________________________________________________________________________
Fax ____________________________________________________________________________________________________________________
Email (required for confirmation) ____________________________________________________________________________________________
SICP Member...................................................................................$70SICP Non Member ........................................................................$120(2007 SICP Membership is included with the cost of a non-member registration)
Registration deadline is April 1, 2007. Any registrations received after April 1st will be accepted as space is available and will be assessed a $25 late fee.
There are 100 spaces available; you must pre-register. There will be limited on-site registration.
Cancellation notices received prior to April 1, 2007 will receive a full refund. Notices received after April 1st are subject to the cancellation policy at the discretion of SICP staff and will depend on wait-listed attendees.
Check #_________________ (payable to SICP) Visa MasterCard
Card#__________________________________ Exp _____________
Name on Card ___________________________________________
Signature ________________________________________________
Please mail this form with payment to SICP headquarters:Attn: GCNKY Review CourseSociety of Invasive Cardiovascular Professionals1500 Sunday Drive, Suite 102Raleigh, NC 27607-5151
Or fax completed form with credit card information to:(919) 787-4916
For more information, please visit www.sicp.com or contact SICP Headquarters at 919-861-4546 or [email protected]
For schedule details and instructor information, please visit www.sicp.com.
Customer #________ Order #________ Registrant #________
April 14-15, 2007
Hosted by the Greater Cincinnati / Northern Kentucky Chapter
Conference Preview
SICP’s Signature RCIS Review Course
SICP’s SignatureRCIS Review Course
April 14-15, 2007 • Cincinnati, OH
Hosted by the Greater Cincinnati/Northern Kentucky Chapter
The Society of Invasive Cardiovascular Professionals will present a two-day Registry Review Course conducted by a few of our premier review course presenters.
The Greater Cincinnati/Northern Kentucky Chapter is generously hosting this course which allows for a favorable registration fee.
This course is designed to review information for the CCI RCIS invasive registry exam. This course will help you identify areas in which you need to concentrate your self-study, or will serve as an overview for those who are prepared to take the exam.
The Review Course fee for members is $70 and $120 for non-members. Course fee for non-members includes SICP membership for 2007.
This program has been approved by the American Association of Critical Care Nurses (AACN) for 14 Contact Hours, Category A credits. This course is ASRT approved for 12 category A credits. This course is SICP approved for 12 credits.
For schedule details and registration information, please visit www.sicp.com

CORONARY HEART ™ 43
The Society of Invasive Cardiovascular Professionals will present a 2 day Registry Review Course conducted by a few of our premier review course presenters.
This course is designed to review information for the CCI RCIS invasive registry exam. This course will help you identify areas in which you need to concentrate your self study, or will serve as an overview for those who are prepared to take the exam.
Hemodynamics, Calculations, Cardiovascular A&P, Interventions, Pharmacology, Equipment and Instrumentation, Radiation Safety, Patient Care and Assessment
Saturday...................................................................8:00 am - 4:00 pmSunday .....................................................................8:00 am - 4:00 pm
For complete schedule details and instructor information, please visit www.sicp.com
The Review Course fee for members is $70 and $120 for non-members. 2007 SICP Membership is included with the cost of a non-member registration.
The GCNKY is generously hosting this course which allows for a favorable registration fee.
Name _________________________________________________________________ Credentials ______________________________________
Facility _________________________________________________________________________________________________________________
Address ________________________________________________________________________________________________________________
City ____________________________________________________State __________ Zip _____________________________________________
Phone __________________________________________________________________________________________________________________
Fax ____________________________________________________________________________________________________________________
Email (required for confirmation) ____________________________________________________________________________________________
SICP Member...................................................................................$70SICP Non Member ........................................................................$120(2007 SICP Membership is included with the cost of a non-member registration)
Registration deadline is April 1, 2007. Any registrations received after April 1st will be accepted as space is available and will be assessed a $25 late fee.
There are 100 spaces available; you must pre-register. There will be limited on-site registration.
Cancellation notices received prior to April 1, 2007 will receive a full refund. Notices received after April 1st are subject to the cancellation policy at the discretion of SICP staff and will depend on wait-listed attendees.
Check #_________________ (payable to SICP) Visa MasterCard
Card#__________________________________ Exp _____________
Name on Card ___________________________________________
Signature ________________________________________________
Please mail this form with payment to SICP headquarters:Attn: GCNKY Review CourseSociety of Invasive Cardiovascular Professionals1500 Sunday Drive, Suite 102Raleigh, NC 27607-5151
Or fax completed form with credit card information to:(919) 787-4916
For more information, please visit www.sicp.com or contact SICP Headquarters at 919-861-4546 or [email protected]
For schedule details and instructor information, please visit www.sicp.com.
Customer #________ Order #________ Registrant #________
April 14-15, 2007
Hosted by the Greater Cincinnati / Northern Kentucky Chapter

CARDIAC SOCIETIES
SICP Overview
44 CORONARY HEART ™
A Message From The Society Of Invasive Cardiovascular ProfessionalsPresidentLynne Jones, RN, RCIS, [email protected]
I am very pleased to contribute to CoronaryHeart. Congratulations to everyone who worked so hard to put this publication together and thank you for circulating in the United States! You give cardiovascular professionals everywhere the opportunity to learn about and from each other.
I would like to take this opportunity to introduce the SICP to CoronaryHeart subscribers. The SICP is the only professional society that represents invasive cardiovascular professionals exclusively, including nursing, radiologic and cardiovascular technology, as well as other allied health professionals who have become members of the cardiovascular care team. We encourage membership from the international community. Invasive cardiovascular professionals everywhere have unified goals – the highest quality patient care. Participation in your professional society enhances the perception of professionalism and high quality of care delivered to patients undergoing procedures in cardiac catheterization laboratories.
I invite you to learn more about the SICP.
Description Of The Society
Founded in 1993, The Society of Invasive Cardiovascular Professionals (SICP) was formed with encouragement from the SCAI (Society
for Cardiovascular Angiography and Interventions). The SCAI recognized the need for a professional society to create and promote professional standards, provide continuing education, and to act as an advocate for the non-physician members of the cardiovascular care team.
Catheterization and electrophysiology laboratories are staffed by allied health professionals from various disciplines. This diversity of disciplines and highly skilled professionals compliments and strengthens the ability to provide a high standard of patient care. The SICP is an inclusive professional group, representing members of all these various disciplines.
The SICP: Was organized at the request of the SCAI and is recognized by the ACCIs inclusive of all the allied health professionals working in cardiac catheterization laboratoriesProvides education for the non-physician professionals who staff the cardiac catheterization laboratoriesPublishes practice standards and position statementsProvides SICP representation on the Board and recommends curriculum to the Joint Review Committee on Education in Cardiovascular Technology (JRC-CVT)Is a member of The Commission on Accreditation of Allied Health Education Programs (CAAHEP)Provides SICP representation on the Board of Cardiovascular Credentialing International (CCI)Endorses the Registered Cardiovascular Invasive Specialist (RCIS) as the minimum credential for those practicing in invasive cardiologyIs a member of the Alliance for Quality Medical Imaging and
•
•
•
•
•
•
•
•
•
Radiation TherapyDevelops and supports local chapters
Mission And Core Values
The Society of Invasive Cardiovascular Professionals is a non-profit organization that promotes and encourages participation of the invasive cardiovascular professional in his/her professional organization. Participation and support of the SICP will serve to enhance the perception of professionalism and high quality of care delivered to patients undergoing procedures in Cardiac Catheterization Laboratories. The SICP is committed to providing educational and networking opportunities to all members and cardiovascular professionals.
Core values define the fundamental beliefs and principles that guide the Society. The core values guiding The Society of Invasive Cardiovascular Professionals are:
CollegialityIntegrityStewardship
Using these core values to direct the development of the Society, the following statements reflect those beliefs:
The SICP:Promotes the highest quality care to patients undergoing invasive procedures in cardiac catheterization laboratories by providing scope of practice, orientation guidelines, position statements and written standards.Provides premium educational offering to invasive specialists at reasonable costs. Acts as an advocate for the profession.Supports invasive cardiovascular leaders.
•
•••
•
•
•
•

SICP OverviewCARDIAC SOCIETIES
CORONARY HEART ™ 45
Vision And Goals
The vision of Society of Invasive Cardiovascular Professionals Executive Board in two year’s time is:The Society of Invasive Cardiovascular Professionals will be the recognized representative of Invasive Cardiovascular Professionals who support physicians and patients in the Cardiac Catheterization and Electrophysiology Laboratories.
The Society will:
Retain current membership and increase new membership by 20%/yearPublish position statements and standards specific to the cath lab environment and work to have those endorsed by leading physician, hospital organizations, and regulatory agencies. Recruit professionals to join and support an Advocacy Committee that will develop a process to assist with and support recognition of the RCIS credential at the federal and state level. Present RCIS review courses regularly. Update and publish curriculum for accredited CVT programs
Standards Of Care/position Statements
The SICP identifies the need for direction in key areas of practice. The Standards Committee provides the invasive cardiovascular community with up to date position statements and standards that correlate with evidence-based practice and regulatory guidelines.
Advocacy
The SICP is a member of AQMIRT (Alliance for Quality Medical Imaging and Radiation Therapy). This group of over thirty organizations representing
•
•
•
•
•
thousands of imaging professionals is instrumental in the advancement of the CARE Bill (Consistency, Accuracy, Responsibility, and Excellence in medical imaging) in the Senate and the House of Representatives. The Bill is designed to set minimum educational and licensure/credentialing standards for medical imaging technologists (including those working in catheterization and EP laboratories), radiation therapists and medical physicists. Once passed, these standards must be met to receive reimbursement for medical imaging or radiation therapy performed on patients covered by Medicare, Medicaid or any program under the jurisdiction of the U.S. Department of Health and Human Services. The SICP fully supports the intent of the Bill and our focus is to support and gain recognition of the RCIS credential at the Federal level.
Educational Focus Of The Society
The SICP is fortunate to have generous industry supporters to assist us with our education initiatives. This support makes it possible for the SICP to provide many educational offerings at an affordable cost to our members and professional community. SICP’s volunteer faculty provides review courses and gives educational presentations at other conferences.
RCIS Credential
The SICP recognizes that the RCIS (Registered Cardiovasacular Invasive Specialist) examination represents the minimum knowledge base necessary for the allied health professional to effectively function in invasive cardiovascular laboratories. The RCIS credentials cardiovascular technologists, and supplements the RT (radiologic technologist) and RN licensure. The ASRT (American Society of Radiologic Technologists) recommends that RT’s working in the invasive cardiovascular laboratory who are not otherwise
credentialed in invasive cardiovascular through ARRT (American Registry of Radiologic Technologists) be credentialed as and RCIS.
The SICP has established the RCIS review course program. The SICP’s goal is to assist RCIS Registry Exam candidates to successfully prepare for the exam by providing quality fundamental and advanced content at affordable prices.
The SICP courses follow the exam matrix published by CCI (Cardiovascular Credentialing International). All SICP courses are conducted by RCIS instructors following a standardized curriculum.
Annual Conference
The SICP recognizes the need for ongoing education to meet the educational requirements to maintain the RCIS credential. The Society meets these needs by conducting annual conferences that include up to date information as well as RCIS review.
Board Members
Each position requires a two year commitment. The SICP Executive Board is comprised of the Immediate Past-President (advisory role), President, President-Elect, and Secretary/Treasurer. The Board meets twice annually in conjunction with the SCAI Annual Meeting/Conference and the SICP Annual Conference. All SICP board positions are on a volunteer basis and members do not receive compensation for their contribution.
All members of the board are dedicated to the advancement of the invasive cardiovascular profession. The SICP has representation on the boards of CCI, The JRC-CVT (Joint Review Committee on Education in Cardiovascular Technology), is a

CARDIAC SOCIETIES
SICP Overview
46 CORONARY HEART ™
member of the Alliance for Quality Medical Imaging and Radiation Therapy. The Executive Board works closely with the SCAI to ensure consistency between the two societies.
Chapter Activity
The chapter development initiative is successful because SICP members enjoy a close relationship with the Society. It is through local networking that the Society and the profession flourishes. There are currently twelve established chapters and several more in the formation stage. These chapters and their members are instrumental in educating their facilities to the importance of the Invasive Cardiovascular Professional
and the RCIS credential. Chapters offer support from facility to facility for both educational and networking opportunities.
Gulf Coast ChapterConnecticut ChapterIndiana ChapterCentral Texas ChapterNorth Carolina ChapterKeystone ChapterIllinois ChapterEmerald Coast ChapterGreater Cincinnati ChapterOregon ChapterTexas Riviera ChapterWisconsin Chapter
The SICP is very proud to share the mission of our professional society with
you. By the time of this publication we will have participated in the 2007 CARE Bill Alliance meeting in Washington, DC. We have meetings scheduled with several Senators and Congressional Representatives to educate them and gain their support for the CARE Bill. As this most important legislature moves forward we will continue to keep you informed of its progress.
We invite and encourage you to become involved with the SICP as members, instructors, Chapter founders and developers, and to serve on the various committees and board positions. I look forward to hearing from you!
SICP Excellence Award Sponsored by Terumo Interventional Systems
The Society of Invasive Cardiovascular Professionals is excited to announce the inaugural year of the SICP
Excellence Award sponsored by Terumo Interventional Systems (Somerset, NJ). This annual award will recognize excellence in the invasive cardiovascular profession. The SICP focuses on recognizing the importance of the non-physician invasive cardiovascular professionals in the cath lab. This award gives the SICP an opportunity to recognize these special individuals and the facility they work in.
Gary Clifton, Marketing Manager announced, “Terumo is very excited and honored to be part of the SICP and their mission to bring education and training to their membership through their varied programs and initiatives. We feel it is essential to identify and recognize excellence in the allied health professionals who are an integral part of the cardiac catheterization teams. Terumo is looking forward to a lasting and meaningful relationship that will bring value to both of our organizations.”
This year’s award theme will be “Excellence in Promoting Community Involvement and Participation With the SICP”.
Please submit nominees to [email protected].
Award Requirements
Nominee must be a current SICP member of two (2) or more consecutive years credentialed as an RCIS.Nominee should be peer nominated – nomination deadline is April 30, 2007.Nominee should show evidence of their involvement with the SICP, their local community, and promoting the SICP within their work environment. Nominee will be required to submit an essay describing how their involvement has affected them and their practice. Essays due no later than May 31, 2007.Nominee will be selected by committee review and winner announced in June.
Award Winners
Award Recipient will receive the award at the SICP’s annual meeting in 2007 (location to be announced). Recipient’s expenses will be covered by Terumo Interventional Systems.SICP will sponsor the recipient’s registration fee. In addition Terumo Interventional Systems will award the recipient a $5,000 educational credit to be used by the recipient’s cath lab to promote education.
•
•
•
•
•
•
•
••

LANGUAGES
CORONARY HEART ™ 47
Photo: Boracay Beach, Philippines
Translated with the assistance of Mrs Jai Baña, from Manila, Philippines, now training in London, UK, as a Cardiac Physiologist.
English Tagalog Phonetic
Good morning. Magandang umagama-gan-DANE
oo-MA-ga
Yes. Oo O-o
No. Hindi heen-DI
Don’t move. (Keep still)
Huwag kang gumalaw Wug kung goo-ma-LAO
Deep breath Hingang malalim Hee-ngang ma-LA-lim
Don’t breathe. Itigil ang paghingaee-TEE-gil ung parg-hee-NGA
Breathe Hinga hee-NGA
Good Magaling mug-a-LEENG
Slowly, slowly. Dahan - Dahan duh-hun DUH-hun
Any chance of being pregnant?
Sa palagay mo, posible kayang nagdadalang tao ka?
Suh pu-lu-guy moh, po-see-ble kuh-YUNG
nug-DUH-duh-lung TUH-o-kah?
We don’t recommend you eat roast pork for a healthy heart! *
Hindi na pwede ang lechon para sa malusog na puso
heen-DEE nuh pwe-deh ung le-CHOON pa-ra suh muh-loo-sog
nuh poo-so
To assist you in the cardiac environment
with patients whom have limited knowledge of English we have given you a helping hand. With the assistance of either internationally recognised translators or locals fluent in their native tongue, we have converted common cardiac phrases into foreign languages, and also provided their phonetic pronunciation in English.
This issue we look at the island nation of the Philippines, with the widest spoken dialect of Tagalog. The country has a population of 85 million located over 7, 107 islands, therefore it is not surprising that there are many dialects. Also after the almost 50 years of ruling by the USA which ended in 1946, the country luckily has a firm grasp of English.
Many cardiac departments throughout the world are staffed by Filipino’s. They are a proud race, quietly spoken, hard working, and rarely judgmental, with a fascinating history which stretches back 2500 years.
Past Issue Languages available online:
Edition 1 = GermanEdition 2 = FrenchEdition 3 = ArabicEdition 4 = Spanish
PHILIPPINES
Cardiac Tagalog
* Quite funny in the Philippines where they eat a lot of fatty pork.

Telephone 0845 363 1187 Facsimile 020 8249 6561Email [email protected] Internet www.rigradiography.co.uk
Setting newstandards for Cardiac ProfessionalsRIG Radiography Recruit has expanded it’s highlysuccessful Radiography business to now include ateam dedicated to the Cardiac sector.
We have become the largest supplier of Radiographystaff to the UK through our premier level of serviceand the proactive nature of our staff.
The team operates throughout various Cardiac Servicedepartments including Angiography andPacing/Cardiac Units, Cardiac Physiology Clinical Unitsand Cardiothoracic Units amongst others.
Our team has over twenty years specialist recruitmentexperience and we pride ourselves on the level ofservice we offer to both clients and candidates.
We cover the following areas–
Cardiac Cath LabsECGEchocardiographyHolter MonitorsExercise Stress TestsPacing ImplantsLung Function TestingTape AnalysisBP MonitoringTilt Testing
Our comprehensive Benefitsand Support Structure includes–
Highly Competitive RatesWide range of posts acrossthe UKLimited Company Set upDedicated Cardiac Recruitment ConsultantsCPD Contributions*CV Assistance and Preparation
* Subject to qualification criteria.
We are always recruiting for Cardiac Cath LabTechnicians, Cardiac Physiologists, Cardiac Clinical Scientific Officers, Echocardiographers Cardiac Sonographers amongst others.
Check out our website and contact the team today to see what we can do for you!

Medical Recruitment Specialists in Cardiology and Radiography Your Career is our world
LONDON SYDNEY AUCKLAND
Locum and Permanent positions domestically and internationally for Cardiac Physiologists, Cath Lab staff, Cardiology Nurses and Echo/Sonographers. Trainee roles are also available.
AUSTRALIA – OFFICEYour World Recruitment Pty LtdLevel 14 Lumley House309 Kent Street, Sydney 2000, AustraliaFREEPHONE 1300 36 23 37PHONE +612 9994 8074FAX +612 9994 [email protected]
UNITED KINGDOM – OFFICEYour World Recruitment17 Blossom Street,London, E1 6PL, United KingdomPHONE +44 (0) 20 7426 6992FAX +44 (0) 20 7426 [email protected]
NEW ZEALAND – OFFICEYour World RecruitmentLevel 20 ASB Bank Centre135 Albert Street, Auckland, New ZealandFREEPHONE 0800 508 018FREEFAX 0800 543 [email protected]
PLEASE CALL NOW TO REGISTER YOUR INTEREST IF YOU ARE SEEKING WORK OR STAFF.Telephone 0845 363 1187 Facsimile 020 8249 6561
Email [email protected] Internet www.rigradiography.co.uk
Setting newstandards for Cardiac ProfessionalsRIG Radiography Recruit has expanded it’s highlysuccessful Radiography business to now include ateam dedicated to the Cardiac sector.
We have become the largest supplier of Radiographystaff to the UK through our premier level of serviceand the proactive nature of our staff.
The team operates throughout various Cardiac Servicedepartments including Angiography andPacing/Cardiac Units, Cardiac Physiology Clinical Unitsand Cardiothoracic Units amongst others.
Our team has over twenty years specialist recruitmentexperience and we pride ourselves on the level ofservice we offer to both clients and candidates.
We cover the following areas–
Cardiac Cath LabsECGEchocardiographyHolter MonitorsExercise Stress TestsPacing ImplantsLung Function TestingTape AnalysisBP MonitoringTilt Testing
Our comprehensive Benefitsand Support Structure includes–
Highly Competitive RatesWide range of posts acrossthe UKLimited Company Set upDedicated Cardiac Recruitment ConsultantsCPD Contributions*CV Assistance and Preparation
* Subject to qualification criteria.
We are always recruiting for Cardiac Cath LabTechnicians, Cardiac Physiologists, Cardiac Clinical Scientific Officers, Echocardiographers Cardiac Sonographers amongst others.
Check out our website and contact the team today to see what we can do for you!
CORONARY HEART ™ 49
March / April 2007EMPLOYMENT ADVERTISING INTERNATIONAL
CARDIAC MEETINGS UNITED KINGDOM March / April 2007

Coronary Heart3/1/200789850-IN50983EXEHEA3.7008” x 10.3937”Kelly Swenk v.4
YOU have committed yourself to providing the best possible care toyour patients. So has Exempla. With three distinct facilities serving thecommunity, we have been ranked among the Solucient “100 TopHospitals” more than any other hospital system in Colorado for thepast 10 years. You also place a high priority on your life away fromwork. Our Colorado locations will ensure that those priorities are met.Come join us.
CV LAB NURSING OPPORTUNITIES - 12195As a Registered Nurse in the CV lab, you will be directly involved inthe assessment, planning, intervention, and evaluation of the patientduring diagnostic and interventional cardiovascular procedures,including coronary angiography, bilateral heart catheterization, stentimplantation, intra-aortic balloon pump insertion, and intravascularultrasound. Additional peripheral procedures include permanentpacemaker implantation and cardia defibrillator implantation.
Qualified candidates must be graduates of an accredited school ofnursing. CV Lab experience preferred. Will consider RN’s with two -three years of critical care experience. Must obtain a Colorado RNlicense. ACLS and BLS certifications are also necessary. On call hoursare required with a 30 min. response time.
If you’re considering relocating - consider us. We’ll fly you out toDenver so you can experience first-hand the manyamazing facets to our wonderful city. To schedule your trip,contact Cass Ohnstad at 303-689-6501 or [email protected].
Find out more about Exempla Healthcare and available opportunitiesby visiting www.exemplajobs.org.
ELEVATING HEALTHCARE FOR ALL
TOGETHER
EOE
LEADING BY EXAMPLE
You don’t need to have your JOB AD
printed in this publication
Just advertise online and save money!!
Only US$150
30 day run.Hypertext link to your website.
••
Quick Ad placementGlobal audience
Email: [email protected]
EMPLOYMENT ADVERTISING
50 CORONARY HEART ™50 CORONARY HEART ™
March / April 2007USA / New Zealand
You will radiate in this role!
Radiographer (MRT)Auckland City Hospital, New ZealandCardiac Investigation UnitAre you an experienced Radiographer looking to defi ne your skills into a more specialised area? Our Cardiac Investigation Unit is modern and fully digital. Work duties are varied and may include:■ Adult diagnostic coronary studies and interventional procedures ■ Renal, Carotid and Aortic stent implantation■ IVUS■ Trial centre■ Paediatric diagnostic and interventional proceduresThere is also the opportunity to be trained in Coronary Angiogram reporting, ECG and pressure monitoring.Registration with the New Zealand MRT Board is essential.For more information, please contact Andrew Large, Acting Charge MRT on +64 9 307 4949 ext 24364 or email [email protected] apply, please submit an online application at www.aucklandhealthcareers.co.nz
Ref No: 010381
www.aucklandhealthcareers.co.nz

Edition 6 May/JuneNEXT ISSUE PREVIEW
CORONARY HEART ™ 51
Southampton General Hospital, United KingdomOn the south coast of England, this lab serves a population of 2.8 million and is one of the most widely respected departments in the UK.
St Joseph Medical Center, Reading, PA, USAJust what are the Cath Lab logistics when a large city hospital shifts to a brand new location over a weekend?
SITE VISITS
Drug Eluting Stents and Hospital AwarenessAn overview of the current controversy involving Drug Eluting Stents, by Dennis Holloway, Director Diagnostic Cardiovascular Services, Bay Medical Center, Florida
ACC 07 and the Cardiovascular Leadership ConferenceCoronary Heart heads to New Orleans, USA, for three big events on the cardiac calender. We’ll tell you how it all unfolds, as the surrounding city still recovers from the devastation of Hurricane Katrina.
Especially designed for Cardiac Rhythm Management specialists, with great articles, challenging problems, and the latest from this growing
industry. Covering Electrophysiology, ICD’s, Pacemakers etc.In every issue from Edition 6.
As of Edition 6 Coronary Heart will be split into 3 distinct versions. The content will remain exactly the same for each, however the
advertising will become more regional focused. Here is the region breakdown: USA/Canada, UK/Ireland,
and Australia/New Zealand
READER SUBMITTED
CONFERENCESdepartments in the UK.departments in the UK.
Above: Ambulances line up at St Joseph Medical Center,
PA to transfer patients across town to their new site.
New Orleans after the HurricanePLUS A LOT MORE!!

Solutions for cardiovascular and imaging services
515 Old Swede Road, Suite C-1, Douglassville, PA 19518Phone 610-385-1227 n Fax 610-385-1229
www.healthworksonline.cc
Let us help you solve your cardiovascular
and imaging challenges.
“When I callHealthworks,I don’t have
to worry aboutquality.”
Charles Minehart, MD, FACCBerks Cardiologists, Ltd.
Pennsylvania
EDUCATIONBoost employee retention and cut the productivity losses that oftenaccompany new hires or service lines with Healthworks clinical education programs, available both onsite and online.
CONSULTING
Resolve challenging service line issues like staffing shortages, quality assurance, inventory control and cath lab planning and construction with expert advice from Healthworks consultants.
STAFFING
Meet your staffing needs with help from our experienced technologists and nurses. Or achieve financial efficiencies of up to 30% when Healthworks manages and staffs your lab. Staffing services are currently available in the Mid-Atlantic region.
To find out more, just call us at 1-610-385-1227 or e-mail [email protected].