Embed Size (px)
Citation preview
Br Heart J 1987;57:446-57
Coronary disease, cardioneuropathy, and conductionsystem abnormalities in the cardiomyopathy ofFriedreich's ataxia*THOMAS N JAMES,t B WOODFIN COBBS4 H CECIL COGHLAN,tWALTER C McCOY,t CHARLES FISCH§
From the t University of Alabama School of Medicine, Birmingham, Alabama, the tEmory UniversitySchool of Medicine, Atlanta, Georgia, and the §University of Indiana School of Medicine, Indianapolis,Indiana, USA
SUMMARY Abnormalities of the heart are a frequent and possibly ubiquitous problem in patientswith Friedreich's ataxia, but their pathogenesis is unclear. Postmortem findings are reported fromthe hearts of three patients with Friedreich's ataxia who died of congestive heart failure and atrialarrhythmias. Particular attention was paid to the following: the large and small coronary arteries,the nerves and ganglia, the conduction system, and the histological and cellular features of thecardiomyopathy. There were pleomorphic nuclei and focal fibrosis and degeneration throughouteach heart including the conduction system. There were distinctive abnormalities of both largeand small coronary arteries, and focal degeneration of nerves and ganglia. These observationssuggest a mosaic concept for the pathogenesis for the cardiomyopathy of Friedreich's ataxia thatinvolves the interplay of molecular faults, cardiomyopathy, cardioneuropathy, and coronarydisease.
In Friedreich's original description of the heritableataxia that now bears his name he reported that fiveof his six cases showed clinical evidence of heartdisease.1 Although the existence of such heart dis-ease has been recognised for many years-anddespite Friedreich's own experience-it has onlyrecently come to be widely appreciated how often theheart is abnormal in these ataxic individuals. Cur-rent estimates in two large series of carefully studiedcases suggest that between 90% and 100% of pa-tients with definite Friedreich's ataxia will havesome demonstrable abnormality of the heart,whether or not any clinical cardiac manifestationshave yet appeared.2"
Despite the continuing investigations of heart dis-ease of Friedreich's ataxia,4- 31 uncertainty about itspathogenesis remains. It is known that affected indi-viduals may develop cardiac hypertrophy of either
Requests for reprints to Dr Thomas N James, Callaway Laboratoryof the Department of Medicine, University of Alabama MedicalCenter, Birmingham, Alabama 35294, USA.
*Presented in part at the annual meeting of the Association ofUniversity Cardiologists on 17 January 1986 in New Orleans.
Accepted for publication 11 December 1986
the symmetrical or asymmetrical type and with orwithout dilatation, that they eventually haveprogressively increasing congestive heart failurewhich is often the cause of death, and that theirclinical course is characterised by the occurrence ofarrhythmias and various other forms of electricalinstability of the heart. But these clinical descriptivefeatures are of little help in determining the funda-mental basis of the heart disease; and without thatknowledge it will continue to be difficult to deter-mine prognosis or to develop optimal forms oftreatment.
Previous studies have unequivocally shown thatthe small coronary arteries are abnormal in patientswho have cardiac disease and Friedreich'sataxiaS 6 8-12; but the functional significance of thisfinding has been challenged, particularly by Hewer"1whose findings have been widely quoted in virtuallyall subsequent reviews. In the present report we de-scribe our own findings in three patients, which sup-port the importance of small coronary artery disease,and show why we believe that Hewer's personal ob-servations do in fact accord our findings.A second cardiac abnormality originally described
by Dorothy Russell,5 who may also have been the
446
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
Heart disease in Friedreich's ataxia
first to call attention to the coronary disease in hercase 3, is a form of myocarditis which we believe isbetter regarded as a form of cardiomyopathy. Whilethe cardiomyopathy is undoubtedly influenced bydisease of the small coronary vessels, cardio-myopathy seems unlikely to be explained entirely bysuch disease.The third abnormality that is abundantly present
is cardioneuropathy, which we believe is describedfor the first time in this report. A fourth componentof our study deals with the conduction system of theheart, abnormalities of which help to explain thefrequent manifestations of cardiac electrical in-stability in these patients. We believe that inter-dependent relations of all these factors form the basisfor a mosaic concept of the pathogenesis of heartdisease in patients with Friedreich's ataxia.
Clinical observations
CASE 1This twenty year old white man was first found tohave Friedreich's ataxia at about the age of eight, andwithin two years intermittent heart failure that wasresponsive to treatment with conservative measuresdeveloped. Over the next decade his cardiac failureprogressed only gradually, although several boutswere transiently severe. These were often associatedwith episodes of pulmonary infection. He was usu-ally in sinus rhythm with multiple atrial extra-systoles, but several bouts of atrial fibrillation weredocumented, especially in his last year of life. Theterminal illness was characterised by an abrupt onsetof severe hypotension accompanied by cyanosis anddyspnoea. It was briefly and incompletely responsiveto treatment with digitalis, diuretics, and similarmeasures. He died eight days after the onset ofhypotension.
CASE 2A twenty two year old white man was first diagnosedas having Friedreich's ataxia at the age of six. In thelast five years of his life he had recurring bouts ofatrial flutter and fibrillation that were eventually as-sociated with steadily worsening congestive heartfailure. Several episodes of pulmonary infectioncomplicated cardiac disease. During this time hecomplained of a dull substernal non-radiating pain,which lasted 10 to 15 minutes. It was often producedby emotional stress. He was too disabled to under-take any activity that was physically taxing. His finaladmission was for severe pulmonary congestionwhich became intractable and led to cyanosis andcoma. He died the next day.
CASE 3This twenty year old white man had Friedreich's
447
ataxia with progressive cardiac failure for five years.There were intermittent bouts of atrial fibrillation.Recurring episodes of pulmonary infection aggra-vated the cardiac insufficiency. During his last ad-mission the congestive failure was more severe andthere was atrial flutter with partial heart block. Hedied quietly on the fifth hospital day. Other details ofthis case have been reported before.8 It is includedhere after further assessment of the coronary diseaseand a special study of the nerves and ganglia of theheart, which were not a subject of the previous study.
Morphological observations
In all three cases the heart was generally enlarged butnot much dilated. Gross heart weights for cases 1, 2,and 3 were 470 g, 495 g, and 550 g respectively. Allthree cases had extensive pulmonary and other vis-ceral congestion, varying amounts of bron-chopneumonia, and histological evidence ofspinocerebellar degeneration. Within the heartsthere was no valve disease, the interatrial and inter-ventricular septa were intact, and there were no gross
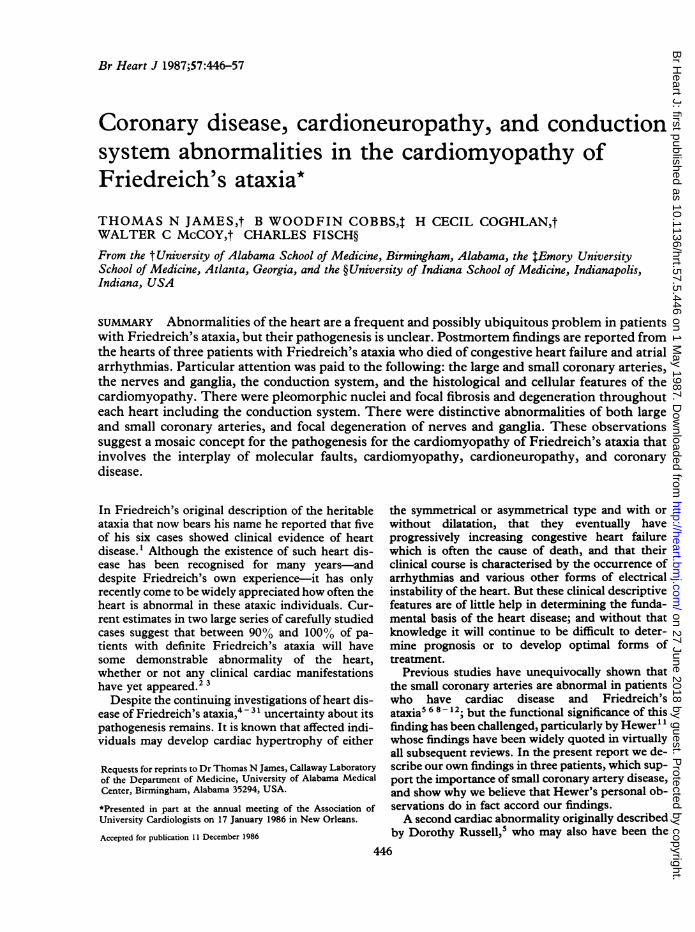
Fig 1 Photomicrographs showing focal fibromusculardysplasia of the main right coronary artery shown at twomagnifications (a and b). Verhoeff-van Gieson elasticstain. All magnifications are indicated by reference bars.
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
James, Cobbs, Coghlan, McCoy, Fisch
-W.
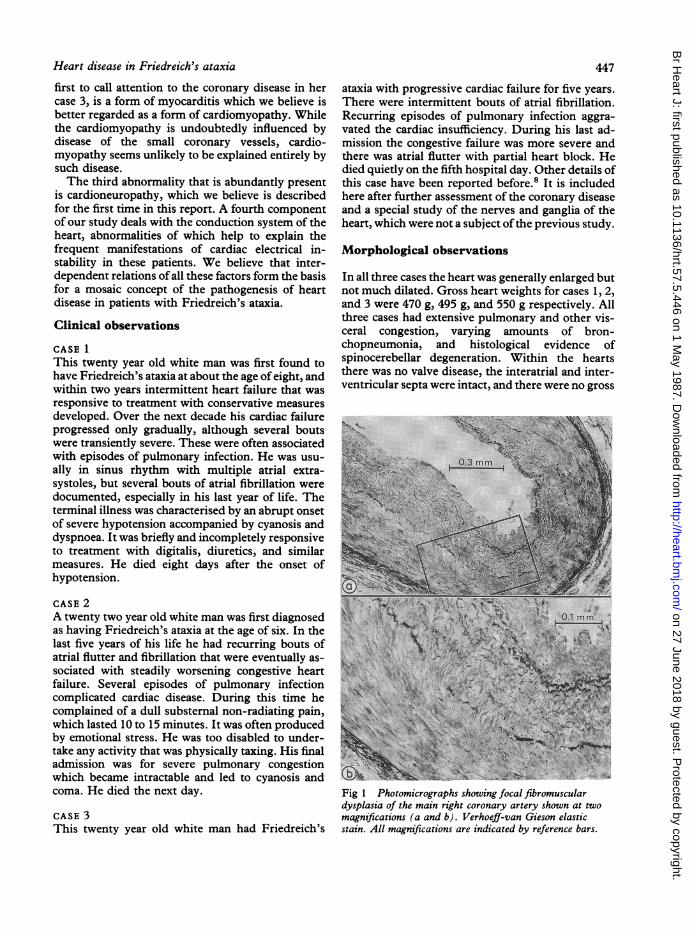
Fig 2 Photomicrographs showing focal fibromusculardysplasia of the sinus node artery at two magnifications (aand b). This section and all subsequent sections are stainedwith Goldner trichrome unless stated otherwise.
anomalies or malformations. In each case the peri-cardium was slightly fibrotic, especially in cases 1and 3, but there was no active pericarditis and therewere no important adhesions.
Because there was atrial arrhythmias in all threecases the sinus node, atrioventricular node, and Hisbundle were examined.32 33 In addition to tissue re-moved for examination of the conduction system, wealso examined four slices of left ventricle (minimalsize 15 by 40 mm), four of right ventricle (at least 10by 40 mm), and two of left atrium (at least 5 by 25mm). The sinus node sections included considerableamounts of right atrium. At least 10 serial 2 mmslices of sinus node were available from each case.The sections of atrioventricular node and His bundleincluded at least 2 cm of both atrial and ventricularseptal tissue, and for each case there were at leasteight 2 mm slices cut serially from this region. Fromeach of these tissue slices at least 10 serial sections of8 gm thickness were prepared with the Goldner tri-chrome stain; additional sections were stained withthe periodic acid Schiff, Verhoeff-van Gieson elastic,and congo red methods.
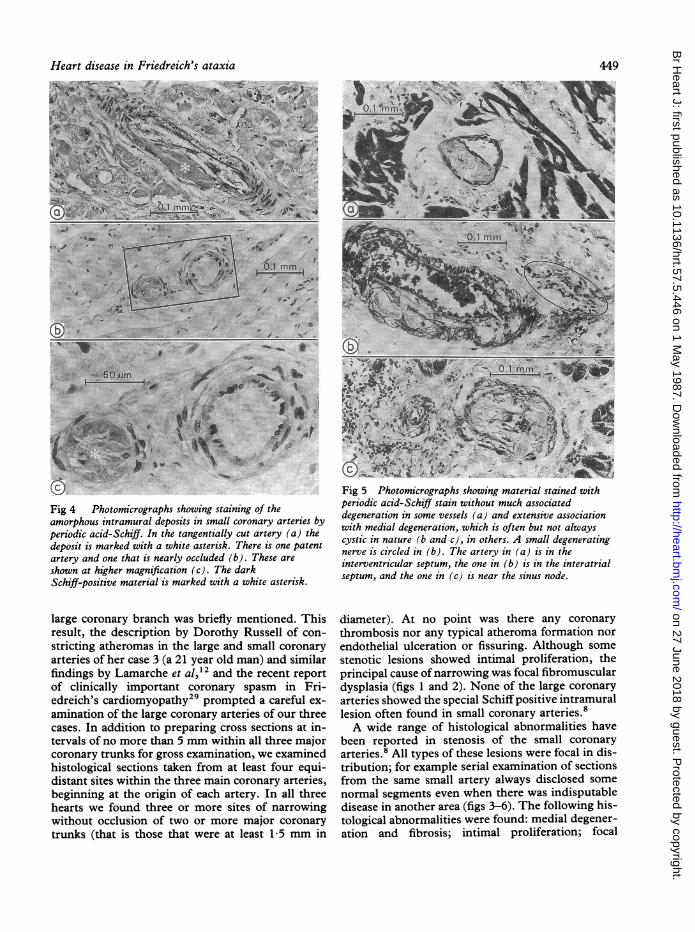
Fig 3 Photomicrographs showing abnormalities of thesmall coronary arteries in branches of the atrioventricularnode artery. The lumen (asterisk) in (a) is narrowed by anintramural amorphous deposit and there is degeneration ofthe tunica media. (b) Only thin tunica media remains, withan even larger amorphous intramural deposit in the artery.This is shown at higher magnification in (c). The tinylumen remaining is indicated by an asterisk.
As part of the light microscopic examinations atleast 400 colour photomicrographs were prepared ofeach of the three cases. Study of both these and thehistological slides showed that the myocardial, neu-ral, and arterial lesions were similar in nature anddistribution in each case. Black and white photo-micrographs from case 1 were then prepared; theyare representative of all three cases. The importantcategories of abnormalities are the coronary disease,the cardioneuropathy, and the conduction system aswell as a probably separate myocytopathy of theheart.
CORONARY DISEASEIn the previous report of case 3 an abnormality ofone
448
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
Heart disease in Friedreich's ataxia
Fig 4 Photomicrographs showing staining of theamorphous intramural deposits in small coronary arteries byperiodic acid-Schiff. In the tangentially cut artery (a) thedeposit is marked with a white asterisk. There is one patentartery and one that is nearly occluded (b). These are
shown at higher magnification (c). The darkSchiff-positive material is marked with a white asterisk.
large coronary branch was briefly mentioned. Thisresult, the description by Dorothy Russell of con-
stricting atheromas in the large and small coronary
arteries of her case 3 (a 21 year old man) and similarfindings by Lamarche et al,2 and the recent report
of clinically important coronary spasm in Fri-edreich's cardiomyopathy29 prompted a careful ex-
amination of the large coronary arteries of our threecases. In addition to preparing cross sections at in-tervals of no more than 5 mm within all three majorcoronary trunks for gross examination, we examinedhistological sections taken from at least four equi-distant sites within the three main coronary arteries,beginning at the origin of each artery. In all threehearts we found three or more sites of narrowingwithout occlusion of two or more major coronary
trunks (that is those that were at least 1-5 mm in
Fig 5 Photomicrographs showing material stained withperiodic acid-Schiff stain without much associateddegeneration in some vessels (a) and extensive associationwith medial degeneration, which is often but not alwayscystic in nature (b and c), in others. A small degeneratingnerve is circled in (b). The artery in (a) is in theinterventricular septum, the one in (b) is in the interatrialseptum, and the one in (c) is near the sinus node.
diameter). At no point was there any coronarythrombosis nor any typical atheroma formation norendothelial ulceration or fissuring. Although somestenotic lesions showed intimal proliferation, theprincipal cause of narrowing was focal fibromusculardysplasia (figs 1 and 2). None of the large coronaryarteries showed the special Schiff positive intramurallesion often found in small coronary arteries.8A wide range of histological abnormalities have
been reported in stenosis of the small coronaryarteries.8 All types of these lesions were focal in dis-tribution; for example serial examination of sectionsfrom the same small artery always disclosed somenormal segments even when there was indisputabledisease in another area (figs 3-6). The following his-tological abnormalities were found: medial degener-ation and fibrosis; intimal proliferation; focal
449
01
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
James, Cobbs, Coghlan, McCoy, Fisch
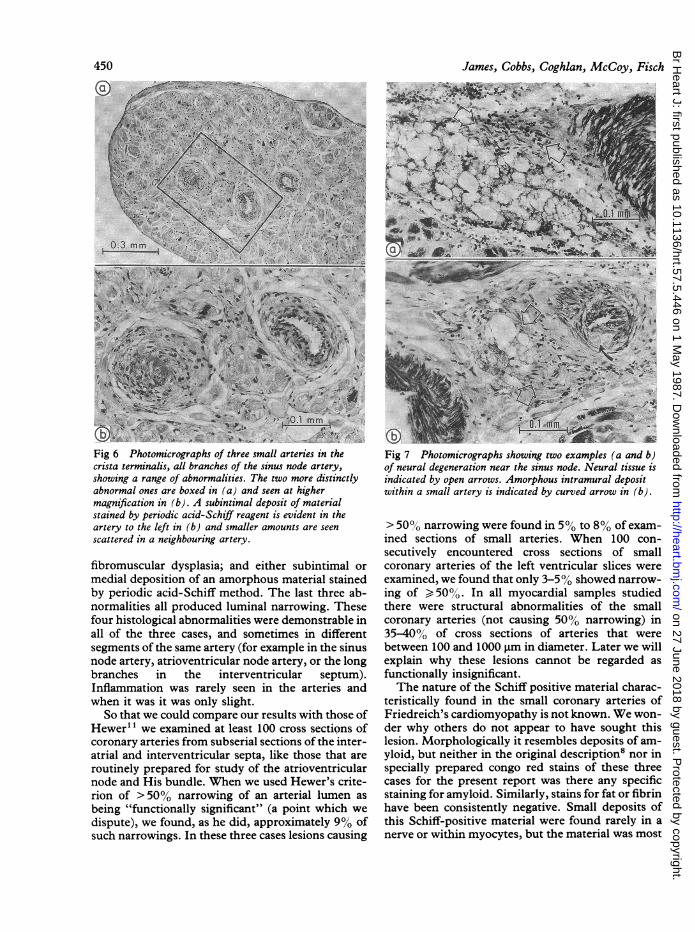
Fig 6 Photomicrographs of three small arteries in the Fig 7 Photomicrographs showing two examples (a and b)crista terminalis, all branches of the sinus node artery, of neural degeneration near the sinus node. Neural tissue isshowing a range of abnormalities. The two more distinctly indicated by open arrows. Amorphous intramural depositabnormal ones are boxed in (a) and seen at higher within a small artery is indicated by curved arrow in (b).magnification in (b). A subintimal deposit of materialstained by periodic acid-Schiff reagent is evident in theartery to the left in (b) and smaller amounts are seenscattered in a neighbouring artery.
fibromuscular dysplasia; and either subintimal or
medial deposition of an amorphous material stainedby periodic acid-Schiff method. The last three ab-normalities all produced luminal narrowing. Thesefour histological abnormalities were demonstrable inall of the three cases, and sometimes in differentsegments of the same artery (for example in the sinusnode artery, atrioventricular node artery, or the longbranches in the interventricular septum).Inflammation was rarely seen in the arteries andwhen it was it was only slight.
So that we could compare our results with those ofHewer" we examined at least 100 cross sections ofcoronary arteries from subserial sections of the inter-atrial and interventricular septa, like those that are
routinely prepared for study of the atrioventricularnode and His bundle. When we used Hewer's crite-rion of > 50% narrowing of an arterial lumen as
being "functionally significant" (a point which we
dispute), we found, as he did, approximately 9% ofsuch narrowings. In these three cases lesions causing
> 50%0 narrowing were found in 5% to 8% of exam-ined sections of small arteries. When 100 con-secutively encountered cross sections of smallcoronary arteries of the left ventricular slices wereexamined, we found that only 3-50% showed narrow-ing of 50%. In all myocardial samples studiedthere were structural abnormalities of the smallcoronary arteries (not causing 50% narrowing) in35-40% of cross sections of arteries that werebetween 100 and 1000 gm in diameter. Later we willexplain why these lesions cannot be regarded asfunctionally insignificant.The nature of the Schiff positive material charac-
teristically found in the small coronary arteries ofFriedreich's cardiomyopathy is not known. We won-der why others do not appear to have sought thislesion. Morphologically it resembles deposits of am-yloid, but neither in the original description8 nor inspecially prepared congo red stains of these threecases for the present report was there any specificstaining for amyloid. Similarly, stains for fat or fibrinhave been consistently negative. Small deposits ofthis Schiff-positive material were found rarely in anerve or within myocytes, but the material was most
450ION
ji
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
Heart disease in Friedreich's ataxia
A..
451
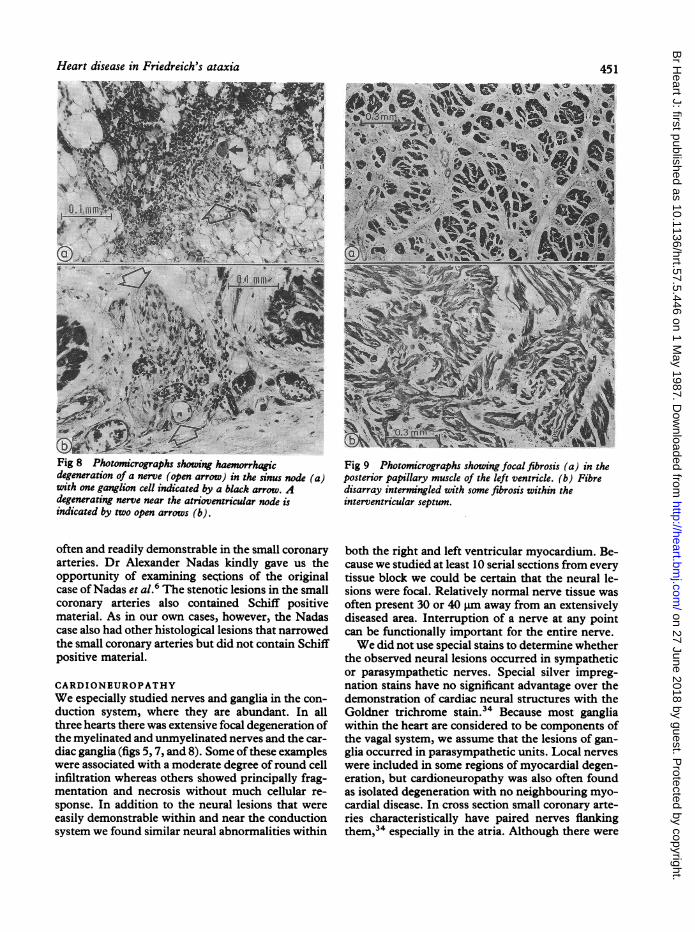
Fig 8 Photomicrographs showing haemorrhaic Fig 9 Photomicrographs showing focal fibrosis (a) in thedegeneration of a nerve (open arrow) in the sinus node (a) posterior papillary muscle of the left ventricle. (b) Fibrewith one ganglion cell indicated by a black arrow. A disarray intermingled with some fibrosis within thedegenerating nerve near the atrioventricular node is interventricular septum.indicated by two open arrows (b).
often and readily demonstrable in the small coronaryarteries. Dr Alexander Nadas kindly gave us theopportunity of examining sections of the originalcase ofNadas et al.6 The stenotic lesions in the smallcoronary arteries also contained Schiff positivematerial. As in our own cases, however, the Nadascase also had other histological lesions that narrowedthe small coronary arteries but did not contain Schiffpositive material.
CARDIONEUROPATHYWe especially studied nerves and ganglia in the con-duction system, where they are abundant. In allthree hearts there was extensive focal degeneration ofthe myelinated and unmyelinated nerves and the car-diac ganglia (figs 5, 7, and 8). Some ofthese exampleswere associated with a moderate degree of round cellinfiltration whereas others showed principally frag-mentation and necrosis without much cellular re-sponse. In addition to the neural lesions that wereeasily demonstrable within and near the conductionsystem we found similar neural abnormalities within
both the right and left ventricular myocardium. Be-cause we studied at least 10 serial sections from everytissue block we could be certain that the neural le-sions were focal. Relatively normal nerve tissue wasoften present 30 or 40 pm away from an extensivelydiseased area. Interruption of a nerve at any pointcan be functionally important for the entire nerve.We did not use special stains to determine whether
the observed neural lesions occurred in sympatheticor parasympathetic nerves. Special silver impreg-nation stains have no significant advantage over thedemonstration of cardiac neural structures with theGoldner trichrome stain.34 Because most gangliawithin the heart are considered to be components ofthe vagal system, we assume that the lesions of gan-glia occurred in parasympathetic units. Local nerveswere included in some regions of myocardial degen-eration, but cardioneuropathy was also often foundas isolated degeneration with no neighbouring myo-cardial disease. In cross section small coronary arte-ries characteristically have paired nerves flankingthem,34 especially in the atria. Although there were
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
452
juxta-arterial lesions of nerves accompanying somearterial lesions, the two abnormalities were oftenfound separately, that is neural lesions were foundaway from arteries and abnormal arteries had localnerves of normal appearance.
CONDUCTION SYSTEMThere were distinct and consistent abnormalities ofthe conduction system in all three hearts. In each thesinus node (figs 2, 5, 6, and 8) was more affected thanthe atrioventricular node or the His bundle. Therewere focal narrowings of local arteries both in thesinus node and the atrioventricular junctional re-gion, and cardioneuropathy was also found at bothsites. Within the three sinus nodes there was focaldegeneration and fibrosis, attributable in part to thecoronary disease but also separate from it. For exam-ple, the bizarre pleomorphic nuclei seen in myocytesoutside the conduction system were also presentwithin it, particularly in the sinus node. The Hisbundle was generally intact in all three cases and wasthe least affected component of conduction system.
James, Cobbs, Coghlan, McCoy, Fisch
In case 2 focal degeneration in the atrioventricularnode almost equalled that seen in the sinus node, butin cases 1 and 3 the atrioventricular node was onlyslightly affected. Since all three cases had clinicallysignificant atrial arrhythmias, the presence and ex-tent of disease in the sinus node and adjacent atrialmyocardium must be interpreted as being func-tionally important.
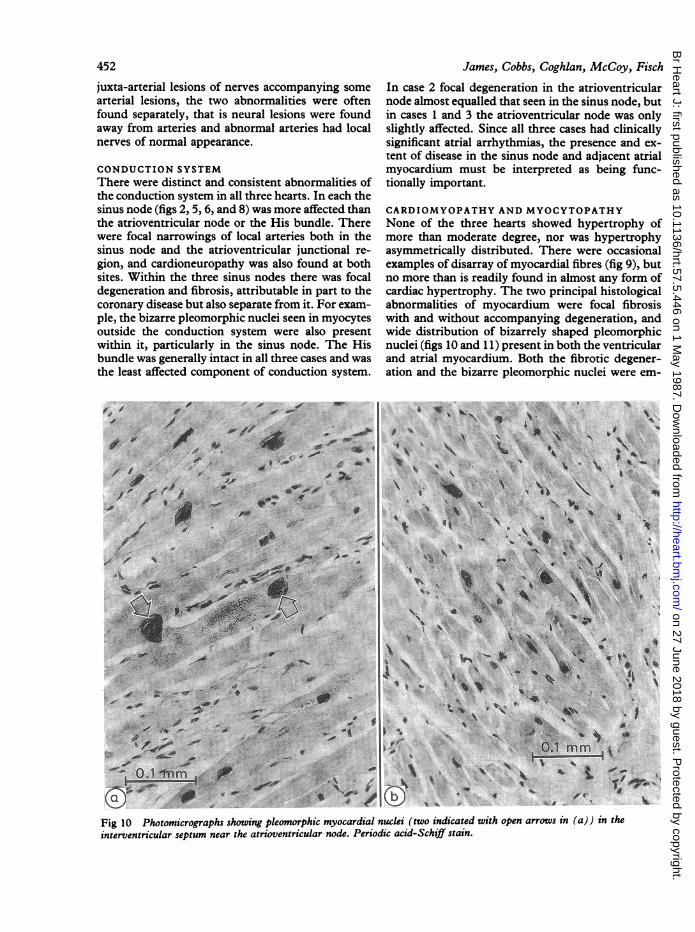
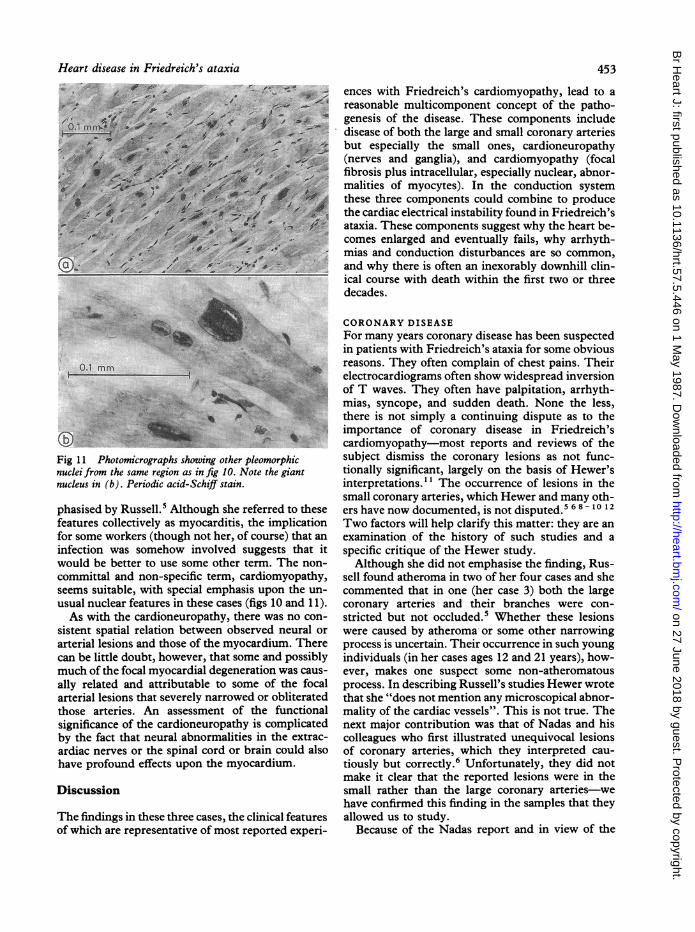
CARDIOMYOPATHY AND MYOCYTOPATHYNone of the three hearts showed hypertrophy ofmore than moderate degree, nor was hypertrophyasymmetrically distributed. There were occasionalexamples of disarray of myocardial fibres (fig 9), butno more than is readily found in almost any form ofcardiac hypertrophy. The two principal histologicalabnormalities of myocardium were focal fibrosiswith and without accompanying degeneration, andwide distribution of bizarrely shaped pleomorphicnuclei (figs 10 and 11) present in both the ventricularand atrial myocardium. Both the fibrotic degener-ation and the bizarre pleomorphic nuclei were em-
Fig 10 Photomicrographs showing pleomorphic myocardial nuclei (two indicated with open arrows in (a)) in theinterventricular septum near the atrioventricular node. Periodic acid-Schiff stain.
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
Heart disease in Friedreich's ataxia
.:..A B.
Fig 11 Photomicrographs showing other pleomorphicnuclei from the same region as in fig 10. Note the giantnucleus in (b). Periodic acid-Schiff stain.
phasised by Russell.' Although she referred to thesefeatures collectively as myocarditis, the implicationfor some workers (though not her, of course) that aninfection was somehow involved suggests that itwould be better to use some other term. The non-
committal and non-specific term, cardiomyopathy,seems suitable, with special emphasis upon the un-
usual nuclear features in these cases (figs 10 and 11).As with the cardioneuropathy, there was no con-
sistent spatial relation between observed neural or
arterial lesions and those of the myocardium. Therecan be little doubt, however, that some and possiblymuch of the focal myocardial degeneration was caus-
ally related and attributable to some of the focalarterial lesions that severely narrowed or obliteratedthose arteries. An assessment of the functionalsignificance of the cardioneuropathy is complicatedby the fact that neural abnormalities in the extrac-ardiac nerves or the spinal cord or brain could alsohave profound effects upon the myocardium.
Discussion
The findings in these three cases, the clinical featuresof which are representative of most reported experi-
453
ences with Friedreich's cardiomyopathy, lead to areasonable multicomponent concept of the patho-genesis of the disease. These components includedisease of both the large and small coronary arteriesbut especially the small ones, cardioneuropathy(nerves and ganglia), and cardiomyopathy (focalfibrosis plus intracellular, especially nuclear, abnor-malities of myocytes). In the conduction systemthese three components could combine to producethe cardiac electrical instability found in Friedreich'sataxia. These components suggest why the heart be-comes enlarged and eventually fails, why arrhyth-mias and conduction disturbances are so common,and why there is often an inexorably downhill clin-ical course with death within the first two or threedecades.
CORONARY DISEASEFor many years coronary disease has been suspectedin patients with Friedreich's ataxia for some obviousreasons. They often complain of chest pains. Theirelectrocardiograms often show widespread inversionof T waves. They often have palpitation, arrhyth-mias, syncope, and sudden death. None the less,there is not simply a continuing dispute as to theimportance of coronary disease in Friedreich'scardiomyopathy-most reports and reviews of thesubject dismiss the coronary lesions as not func-tionally significant, largely on the basis of Hewer'sinterpretations." The occurrence of lesions in thesmall coronary arteries, which Hewer and many oth-ers have now documented, is not disputed.5 68-10 12Two factors will help clarify this matter: they are anexamination of the history of such studies and aspecific critique of the Hewer study.Although she did not emphasise the finding, Rus-
sell found atheroma in two of her four cases and shecommented that in one (her case 3) both the largecoronary arteries and their branches were con-stricted but not occluded.5 Whether these lesionswere caused by atheroma or some other narrowingprocess is uncertain. Their occurrence in such youngindividuals (in her cases ages 12 and 21 years), how-ever, makes one suspect some non-atheromatousprocess. In describing Russell's studies Hewer wrotethat she "does not mention any microscopical abnor-mality of the cardiac vessels". This is not true. Thenext major contribution was that of Nadas and hiscolleagues who first illustrated unequivocal lesionsof coronary arteries, which they interpreted cau-tiously but correctly.6 Unfortunately, they did notmake it clear that the reported lesions were in thesmall rather than the large coronary arteries-wehave confirmed this finding in the samples that theyallowed us to study.
Because of the Nadas report and in view of the
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
454
widely recognised electrocardiographic abnormal-ities, interpreted by some as representing myocardialischaemia and even infarction, Boyer et al studied 33cases of Friedreich's cardiomyopathy for whichthere was necropsy information on two of the eightthat died.7 It was clear from their report that theywere seeking large coronary lesions of the type oftenassociated with conventional myocardial infarction,and they found coronary atherosclerosis "withoutlumen occlusion" in one of the two necropsy cases,
a 25 year old woman. Based upon clinical evidence,mainly electrocardiograms (there were no coronary
arteriograms), they concluded that coronary diseasewas not the basis of Friedreich's cardiomyopathy.But they did not examine the small coronary arteriesin the two necropsy cases, or at least they did notreport that they had. Since then the clinical im-portance of coronary spasm has come to be widelyaccepted, including its occurrence in Friedreich'scardiomyopathy.29 Thus it is possible that some ofthe "insignificant" lesions in the large coronaryarteries may have been erroneously dismissed.The study reported by Hewer in 1969 is often
cited as providing the definitive answer."1 From areview of 27 cases he concluded that lesions causingnarrowing of the small coronary arteries were indeedpresent but "that the vast majority of cardiac arteriesare not obviously narrowed"; this is a misin-terpretation of his own findings to which we willreturn. He further concluded that the coronary nar-
rowing that he did find was secondary to involutionof cardiac muscle, although little evidence ispresented to support this interpretation. If he exam-ined any of his sections with the periodic acid-Schiffstain, for example, he does not report it. He does notexplain how this unusual and perhaps unique lesionin Friedreich's cardiomyopathy could be secondaryto involution of cardiac muscle or how such a processcould lead to focal fibromuscular dysplasia or otherstructural lesions. It is at least as plausible to inter-pret involution of muscle as being due to coronarydisease as the reverse.
But the conduct of the Hewer study itself is morefundamentally flawed. Most subsequent reviewersdescribing the cardiomyopathy of Friedreich's ataxiarefer to his 27 cases, but Hewer was able to examinetissue from only 16 of these cases. Neither theamount or nature of the tissue or its source in theheart is described for these 16 cases and it is uncer-tain whether he had one slide or more, whether wettissue was included for special staining, whether thesample came from representative areas of any givencardiac chamber, or how well preserved and suitablefor any sort of study some of these archival sampleswere. He had three (not the often quoted 27) wholehearts to examine, and he made bread loaf slices of
James, Cobbs, Coghlan, McCoy, Fisch
them to obtain a large segment of myocardium fromwhich to do his 100 count examinations. Con-ventional ventricular sections prepared with cutsperpendicular to the epicardium are suitable for ex-aminations of right ventricular or atrial coronary ar-teries, where most of the small branches run parallelto the epicardium, but not for the left ventricle orinterventricular septum where such cuts would lieparallel to the major course of most small coronaryarteries.35 Though this limited Hewer's samplingopportunity, his subsequent count of 100 con-secutively encountered cross sections of arteries doesprovide the data he sought although it may not berepresentative of all regions of the heart.His use of the 100 count approach was then en-
cumbered by the arbitrary criterion that a narrowingwas regarded as functionally significant only if> 50% of the lumen was affected. This makes noallowance for postmortem shrinkage of hearts inwhich the vessels were not fixed in distension (whichwould have led to an overestimate of lesions) nor forthe possible importance of spasm in diseased arterieswith < 50% narrowing (which would underestimatesignificance). Most of the coronary branches thatregulate flow are of the size being considered (100 to1000 gm in diameter) and observed abnormalities oftheir walls cannot be dismissed simply becausethey do not cause 50% narrowing of the lumen atnecropsy.
Small arteries of the heart are not simply passiveconduits. To regulate coronary flow they must notonly have an adequate lumen but they must also becapable of responding appropriately to neu-rohormonal signals for dilatation or constriction asmetabolic and functional needs require. Structuraldisease of such vessels may be expected to distortsignificantly their responses to either neural or hor-monal influences, so that they would be unable todilate or to constrict when they should. Some of theexamples we report here (figs 3-6) as well as figs 7 to9 in Hewer's own study could hardly be expected tobehave in a physiological manner, whatever thedegree of luminal narrowing may have been.The most serious error in the Hewer study is his
interpretation that 910% of arteries were normal, orconversely that only 9% had significantly narrowedlumens. His data do not represent arteries per se, butonly cross sections of arteries. What he observed wasthat 9% of such cross sections were significantlynarrowed, which tells us about only a thin section ofa comparatively long artery. In the human left ven-tricle such arteries are regularly 20 to 30 mm long,and in the interventricular septum they are oftenlonger.36 The sinus node artery is frequently 50 to100 mm long in the normal adult human heart.37 Astudy with 8 gim sections to assess the patency of
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
Heart disease in Friedreich's ataxia
such arteries would require several thousand sec-
tions per artery. Even with Hewer's 30 gm slices onewould need over one thousand sections to assess thepatency of such arteries.An obstructing lesion (50% or even 100% oc-
clusion) need not be very long, but it would eliminateall distal flow in that vessel. If such a lesion were 100jm long (some of the pronounced narrowings we
observed in serial sections were shorter than that), anobserver would have only one chance in several hun-dred sections of a 30 or 40 mm (30 000 to 40 000 gm)artery of finding such a lesion; Hewer reported thathe found lesions in 9% of the arteries that he exam-ined. This is at least several times more than wouldbe expected by chance alone. We do not dispute theaccuracy of his observations which we were able toconfirm, but his interpretation is wrong. Hewer inessence made a two dimensional analysis of a threedimensional problem.
In addition to the significant lesions in small coro-nary arteries we should probably reconsider thefindings in the large coronary arteries. Several pre-vious observers have found "atheroma" of majorcoronary arteries but have regarded them as not clin-ically significant because the lumen was not obstruc-ted (sic).' 7 8 We can no longer think of largercoronary arteries as simply passive conduits either.Not only is spasm of the large coronary arteries an
accepted clinical entity but it has been found in a
patient with Friedreich's cardiomyopathy.29 Thusthe entire coronary tree must be suspect in thepathogenesis of heart disease in patients withFriedreich's cardiomyopathy.
CARDIONEUROPATHYTo our knowledge this is the first study of abnormal-ities of the nerves and ganglia of the heart in Fri-edreich's ataxia. Extracardiac neural abnormalities(not studied here) may also contribute to dis-turbances of cardiac rhythm or conduction or re-
polarisation, as well as contractility and coronarytone. They apparently are responsible for labile hy-pertension in some patients with Friedreich's
26
ataxia.One of the most familiar clinical features of Fri-
edreich's cardiomyopathy is widespread inversion ofT waves in the electrocardiogram. Possible expla-nations must include the known focal degenerationand fibrosis in the myocardium, some but certainlynot all ofwhich may be related to disease of the smallcoronary arteries. Another explanation, however,may be neural disease both within and outside theheart. Neural control of the heart profoundlyinfluences almost every component of its function,but it is especially effective upon the processes gov-erning repolarisation and thus the appearance of the
455
ST segment and T wave.38
Cardioneuropathy may also affect myocardial con-
tractility. The inevitable regional variations in theneural inotropic influence may be the basis of someof the unusual changes in segmental wall motion or
other ventricular contractile abnormalities describedin Friedreich's cardiomyopathy.13- 16 20 27-29
CARDIOMYOPATHYThere is not much dispute about the general nature
of the myocardial lesions: hypertrophy of fibres,widely scattered focal degeneration and varying de-grees of fibrosis, and the unusual nuclear abnormal-ities first described by Russell. Hypertrophy ofthe heart is generalised, as are each of the myo-
cardial lesions. Hypertrophy is sometimes asym-
metrical"3-5; but this is the exception rather thanthe rule. As discussed previously,8 it seems reason-
able to attribute some of the focal degeneration andfibrosis in the myocardium to narrowing lesions ofthe small coronary arteries. The association with fo-cal lesions in the sinus node that we saw in all threeof the present cases coupled with focal pronouncednarrowing of branches of the sinus node artery isparticularly persuasive since all three patients haddocumented atrial arrhythmias. Neither the patho-genesis nor the functional significance of the bizarrepleomorphic nuclei is apparent.
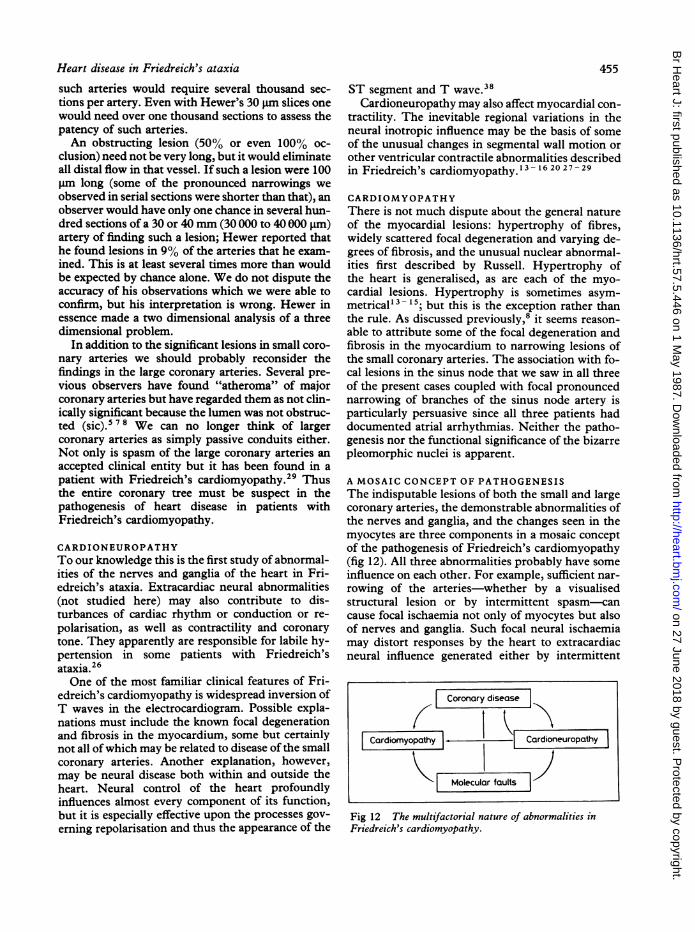
A MOSAIC CONCEPT OF PATHOGENESISThe indisputable lesions of both the small and largecoronary arteries, the demonstrable abnormalities ofthe nerves and ganglia, and the changes seen in themyocytes are three components in a mosaic conceptof the pathogenesis of Friedreich's cardiomyopathy(fig 12). All three abnormalities probably have someinfluence on each other. For example, sufficient nar-
rowing of the arteries-whether by a visualisedstructural lesion or by intermittent spasm-cancause focal ischaemia not only of myocytes but alsoof nerves and ganglia. Such focal neural ischaemiamay distort responses by the heart to extracardiacneural influence generated either by intermittent
Fig 12 The multifactorial nature of abnormalities inFriedreich's cardiomyopathy.
I Coronary disease
Cardiomyopathy |, Cardioneuropathy I1
L a I1I Molecular faults I
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
456 James, Cobbs, Coghlan, McCoy, Fischreflexes or by more sustained disease of the typeintrinsic to Friedreich's ataxia. Neural injury mayalso be the source of either excitatory39 ordepressive40 cardiogenic reflexes. For example, la-bile hypertension observed in Friendreich's ataxia27could have its origin within the heart.39 From a gen-eral assessment of the areas of focal degeneration andfibrosis of myocardium it seems unlikely that thesecan be entirely attributed to the arterial lesions, butsome must be. Further studies in vivo, such as thal-lium scans and assessment of coronary reserve, areneeded to determine how much of the myocardialabnormality is the result of ischaemia, which islargely attributable to the functional behaviour of thesmall coronary arteries.41 4
In one study of 14 patients with Friedreich's car-diomyopathy thallium scans showed abnormalmyocardial perfusion in every case.27 Although theworkers did not interpret their findings as beingcaused by abnormal coronary flow, claiming that intheir own experience the large and small coronaryarteries did not show "significant atherosclerotic in-volvement", their previous morphological studyactually demonstrated mild to moderate disease ofthe small coronary arteries in each of their threecases. 1 Therriault et al offer no convincingalternative explanation,27 but we agree withothers42 43 47 - 49 that the most logical cause of func-tional abnormalities in such thallium scans isabnormal small coronary arteries.Hypertrophy and myocytopathy of the heart in
Friedreich's ataxia can also partially be attributed toa compensatory response to recurring focal is-chaemia, but the prevalence of bizarre nuclei withinthe myocytes suggests some more fundamental fault,perhaps in intracellular metabolism. Whether thecardioneuropathy contributes to myocardial hyper-trophy depends upon several factors. If the nervesaffected are of sympathetic origin then during anyexcitatory phase of the disease they may releasesufficient local noradrenaline to produce hyper-trophy.50 5 Later, when the nerves may be de-stroyed or inactive, the focal loss of a positiveinotropic influence may lead to abnormal local stresswhich could end in compensatory hypertrophy.Overactivity of local nerve endings could even leadto fibromuscular dysplasia of the small or large coro-nary arteries, as was suggested for the myocardium.If such focal fibromuscular dysplasia has its origin insome non-neural process it may nevertheless makethe local area supplied by the affected artery overresponsive to either normal or increased neuralinfluence.
All three of these pathogenetic components con-verge in the cardiac conduction system and particu-larly the sinus node. There one finds abnormally
narrowed arteries, degenerated nerves and ganglia,and pleomorphic nuclei in abundance. Since atrialarrhythmias are common in patients with Fri-edreich's cardiomyopathy (all three of our cases),this added physiological stress brought about by dis-ease within the conduction system could even beconsidered a fourth component in the pathogenesisof Friedreich's cardiomyopathy.Only by concomitantly considering all of the arte-
rial, neural, and myocardial facets of this complexdisease can any reasonable synthesis be made of thepathogenesis of Friedreich's cardiomyopathy. Indifferent cases the individual contributions of thesecomponents will undoubtedly vary both in size andtiming. Ultimately, of course, we must seek furtherfor the various postulated molecular faults whichmay be responsible,' 7 21 - 24 but it is perplexing howa single or closely related group of such molecularfaults could account for such diverse components inthis pathogenesis. If there is a common thread, asindeed there may be, it is not yet apparent.
This work was supported in part by the NationalHeart, Lung and Blood Institute (H-7108 and HL11,310) and by the State of Alabama Program forResearch on Sudden Death.
References
1 Friedreich N. Ueber degenerative atrophie der spinalenhinterstrange. Arch Path Anat Physiol Klin Med1863;27:1-26.
2 Pentland B, Fox KAA. The heart in Friedreich's ataxia.I Neurol Neurosurg Psychiatry 1983;46:1138-42.
3 Child JS, Perloff JK, Bach PM, et al. Cardiac in-volvement in Friedreich's ataxia: a clinical study of 75patients. J Am Coll Cardiol 1986;7:1370-8.
4 Laubry C, Heim de Balsac R. A propos des troublescardiaques de la maladie de Freidreich. Bull Soc MedHop Paris 1936;52:756-9.
5 Russell DS. Myocarditis in Friedreich's ataxia. J PatholBacteriol 1946;58:739-48.
6 Nadas AS, Alimurung MM, Sieracki LA. Cardiacmanifestations of Friedreich's ataxia. N Engl J Med1951;244:239-44.
7 Boyer SH, Chisholm AW, McKusick VA. Cardiacaspects of Friedreich's ataxia. Circulation 1962;25:493-505.
8 James TN, Fisch C. Observations on the cardiovascularinvolvement in Friedreich's ataxia. Am Heart J1963;66:164-75.
9 Ivemark B, Thoren C. The pathology of the heart inFriedreich's ataxia. Changes in coronary arteries andmyocardium. Acta Med Scand 1964;175:227-37.
10 Varnauskas E, Ivemark B, Paulin S, Ryden B. Obscurecardiomyopathies with coronary artery changes. AmJ Cardiol 1967;19:531-41.
11 Hewer RL. The heart in Friedreich's ataxia. Br HeartJ 1969;31:5-14.
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from
Heart disease in Friedreich's ataxia 457
12 Lamarche JB, Cote M, Lemieux B. The cardio-myopathy of Friedreich's ataxia: morphological ob-servations in 3 cases. Can JNeurol Sci 1980;7:389-96.
13 Gach JV, Andriange M, Franck G. Hypertrophic ob-structive cardiomyopathy and Friedreich's ataxia.Am J Cardiol 1971;27:436-41.
14 Boehm TM, Dickerson RB,-Glasser SP. Hypertrophicsubaortic stenosis occurring in a patient with Fri-edreich's ataxia. Am J Med Sci 1971;260:279-84.
15 Ruschhaupt DG, Thilenius OG, Cassels DE. Fri-edreich's ataxia associated with idiopathic hyper-trophic subaortic stenosis. Am Heart J 1972;84:95-102.
16 Van der Hauwaert LG, Dumoulin M. Hypertrophiccardiomyopathy in Friedreich's ataxia. Br Heart J1976;38:1291-8.
17 Blass JP, Kark RAP, Menon NK. Low activities of thepyruvate and oxoglutarate dehydrogenase complexesin five patients with Friedreich's ataxia. N EngilJMed1976;295:62-7.
18 O'Brien ET, Dajee H, Ward OC. Friedreich's disease-a family study. Eur J Cardiol 1977;6:15-24.
19 Cote M, Bureau M, Leger C, et al. Evolution of cardio-pulmonary involvement in Friedreich's ataxia. Can JNeurol Sci 1979;6:151-7.
20 Berg RA, Kaplan AM, Jarrett PB, Molthan ME. Fri-edreich's ataxia with acute cardiomyopathy. Am J DisChild 1980;134:390-3.
21 Barbeau A. Friedreich's ataxia 1980. An overview of thephysiopathology. Can J Neurol Sci 1980;7:455-68.
22 Gottdiener JS, Hawley RJ, Maron BJ, Bertorini TF,Engle WK. Characteristics of the cardiac hyper-trophy in Friedreich's ataxia. Am Heart J1982;103:525-31.
23 Stumpf DA. Friedreich's disease: a metabolic cardio-myopathy. Am Heart J 1982;104:887-8.
24 Pasternac A, Wagniart P, Olivenstein R, et al. Increasedplasma catecholamines in patients with Friedreich'sataxia. Can J Neurol Sci 1982;9:195-203.
25 Harding AE, Hewer RL. The heart disease of Fri-edreich's ataxia: a clinical and electrocardiographicstudy of 115 patients, with an analysis of serial elec-trocardiographic changes in 30 cases. Q J Med1983;52:489-502.
26 Margalith D, Dunn HG, Carter JE, Wright JM. Fri-edreich's ataxia with dysautonomia and labile hyper-tension. Can J Neurol Sci 1984;11:73-7.
27 Therriault L, Lamoureux G, Cote M, Plourde G, Lem-ieux B. Cardiomyopathy in Friedreich's ataxia: ven-triculography and myocardial imaging withthallium-201. Can J Neurol Sci 1984;11:588-91.
28 Steinsapir K, Lewis W. Dilated cardiomyopathy asso-ciated with Friedreich's ataxia. Arch Pathol Lab Med1985;109:454-6.
29 Sohi GS, Drake C, Flowers NC. Friedreich's ataxiaassociated with hypertrophic cardiomyopathy andcoronary vasospasm. Clin Cardiol 1985;8:537-41.
30 Hawley RJ, Gottdiener JS. Five-year follow-up of Fri-edreich's ataxia cardiomyopathy. Arch Intern Med1986;146:483-8.
31 Casazza F, Ferrari F, Finocchiaro G, et al. Echo-cardiographic evaluation of verapamil in Friedreich'sataxia. Br Heart J 1986;55:400-4.
32 James TN. The sinus node. Am J Cardiol
1977;40:965-86.33 James TN. Structure and function of the AV junction.
The Mikamo Lecture for 1982. Jpn Circ J1983;47:1-47.
34 James TN. Primary and secondary cardioneuropathiesand their functional significance. J Am Coll Cardiol1983;2:983-1002.
35 James TN. Small arteries of the heart. The 36th GeorgeE Brown Memorial Lecture. Circulation1977;56:2-14.
36 James TN, Burch GE. Blood supply of the human in-terventricular septum. Circulation 1958;17:391-6.
37 James TN. Anatomy of the coronary arteries. Hag-erstown, Maryland: Harper and Row, 1961.
38 Abildskov JA. Adrenergic effects on the QT interval ofthe electrocardiogram. Am Heart J 1976;92:210-6.
39 James TN, Isobe JH, Urthaler F. Analysis of com-ponents in a hypertensive cardiogenic chemoreflex.Circulation 1975;52:179-92.
40 Frink RJ, James TH. The intracardiac route of the vonBezold-Jarisch reflex. Am J Physiol 1971;221: 1464-9.
41 Strauer BE. Die quantitative bestimmung der ko-ronarreserve zur diagnostik koronarer durch-blutungsstorungen. Der Internist 1977;18:579-87.
42 Factor SM, Minase T, Cho S, Dominitz R,Sonnenblick EH. Microvascular spasm in the cardio-myopathic Syrian hamster; a preventable cause offocal myocardial necrosis. Circulation 1982;66:342-54.
43 Cannon RO III, Watson RM, Rosing DR, Epstein SE.Angina caused by reduced vasodilator reserve of thesmall coronary arteries. J Am Coll Cardiol1983;1:1359-73.
44 Opherk D, Mall G, Zebe H, et al. Reduction of coro-nary reserve: a mechanism for angina pectoris in pa-tients with arterial hypertension and normal coronaryarteries. Circulation 1984;69:1-7.
45 Strauer BE. The coronary circulation in hypertensiveheart disease. Hypertension 1984;6 (suppl III):74-80.
46 Cannon RO III, Watson RM, Rosing DR, Epstein SE.Efficacy of calcium channel blocker therapy for an-gina pectoris resulting from small-vessel coronary ar-tery disease and abnormal vasodilator reserve. Am JCardiol 1985;56:242-6.
47 Kahan A, Nitenberg A, Foult J-M, et al. Decreasedcoronary reserve in primary scleroderma myocardialdisease. Arthritis Rheum 1985;28:637-46.
48 Legrand V, Mancini GBJ, Bates ER, Vogel RA. Evi-dence of abnormal vasodilator reserve in coronaryspasm. Am J Cardiol 1986;57:481-2.
49 Kimball BP, Shurvell BL, Mildenberger RR, Houle S,McLaughlin PR. Abnormal thallium kinetics in post-operative coarctation of the aorta: evidence for diffusehypertension-induced vascular pathology. J Am CollCardiol 1986;7:538-45.
50 Laks MM, Morady F, Swan HJC. Myocardial hyper-trophy produced by chronic infusion of sub-hypertensive doses of norepinephrine in the dog.Chest 1973;64:75-8.
51 Simpson P. Stimulation of hypertrophy of culturedneonatal rat heart cells through an oc,-adrenergic re-ceptor and induction of beating through an oz1-and, 1-adrenergic receptor interaction. Circ Res1985;56:884-94.
on 27 June 2018 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.57.5.446 on 1 M
ay 1987. Dow
nloaded from