Embed Size (px)
Citation preview

1 Confidential not for sharing outside of Evaluation Group|

2 Confidential not for sharing outside of Evaluation Group|
Times Agenda item Areas for discussion Presenter
3:00pm 1. Welcome and purpose Patrick Figgis
3:05pm 2. Minutes of the meeting 31/08/16
Patrick Figgis
3:10pm 3. Declarations of interest
Mark Easton
3:30pm 4. Overview of non financial evaluation scoring
• Confirmation of scoring • Updates to travel analysis • Expert clinician comparison of
GRIFT reports
Patrick Figgis Mark Easton
4:00pm 5. Financial analysis • Update on analysis and submissions
Mark Cheung and Nick Jones
4:45pm 6. Summary and recommendations to the CiC
Patrick Figgis

3 Confidential not for sharing outside of Evaluation Group|

4 Confidential not for sharing outside of Evaluation Group|
• To review the consolidated scorings of the non-financial criteria from the previous session
• To receive updated financial analysis and assess the proposals against the financial criteria
• For the evaluation panel to agree the recommendation to be made to the Committee in Common

5 Confidential not for sharing outside of Evaluation Group|
There are many possible options for configuring the two elective orthopaedic centres in SEL. During 2016 providers have developed submissions to host one of the two centres. By applying agreed evaluation criteria, the evaluation panel will recommend the most appropriate to the committee in common. The process is mapped out below: March 2016 - 1st submission:
initial long list identified
1. Application of hurdle criteria by evaluation panel – shortlist of options identified
2. Application of non financial and financial criteria by evaluation panel. Recommend a preferred option to CiC & business case created
Providers develop expressions of interest to host EOC and identify sites not suitable to host
Providers develop full submissions for sites on the long list
July 2016 - 2nd submission: Long list options for evaluation
Several potential sites
and options
4 potential sites and 6 potential
options
November 2016 CiC agree consultation on shortlisted options (inc. preferred option)
• Hurdle and non-financial criteria have been analysed on 31/8/16
• Financial criteria to be assessed today

6 Confidential not for sharing outside of Evaluation Group|
• Recommended to the Committee in Common that the following sites proposed by providers as not suitable to host an EOC are discounted from the evaluation process and therefore will not be considered for hosting an EOC in SEL:
– St Thomas’ Hospital (GSTT)
– Queen Elizabeth Hosptial (LGT)
– Denmark Hill (KCH)
– Princess Royal University Hospital (KCH)
• Recommended to the Committee in Common that the proposal to host an elective orthopaedic centre at Queen Mary’s Hospital, Sidcup does not pass the hurdle criteria and therefore should not be taken forward in the evaluation of proposals and possible configurations.
• Recommended to the Committee in Common that the following sites (and configurations of these sites) pass all the hurdle criteria and therefore are taken forward in the evaluation of proposals and possible configurations:
– Guy’s Hospital (GSTT)
– Orpington Hospital (KCH)
– Lewisham Hospital (LGT)
• Completed the scoring of all non-financial criteria for the three configuration options.

7 Confidential not for sharing outside of Evaluation Group|

8 Confidential not for sharing outside of Evaluation Group|

9 Confidential not for sharing outside of Evaluation Group|
Name Organisation Declared interests
Dr. Jonty Heaversedge Southwark CCG • Director of Vitality Ltd
• User of health service in Southwark
Dr. Hany Wahba Greenwich CCG • Joint Medical Director of Grabadoc
• Board member of Grabadoc
Moira McGrath Lambeth CCG • None
Dr. Faruk Majid Lewisham CCG • None
Dr. Jhumur Moir Bexley CCG (None received)
Mark Cheung Bromley CCG • User of health service in Lambeth
John King PPV and chair of PPAG • Health user at Kings college Hospital and GSTT
• Member Southwark CCG EPEC
• Patient rep from EPEC to the Dulwich Programme Board
• Member of NHSE Adult screening board (London)
• Member of 111 procurement board
Gaby Charing (on behalf of Ian Fair)
PPV • Health user at Kings college Hospital and Guy’s Hospital
Rikki Garcia Healthwatch Greenwich (None received)

10 Confidential not for sharing outside of Evaluation Group|
Name Organisation Declared interests
Mr. Julian Owen Independent Orthopaedic Clinician Director MSK Clinical Business Unit & Consultant T&O Surgeon Cambridge University Hospitals NHS Trust
(None received)
Tom Brown • London Borough Bexley • None
Aileen Buckton London Borough Lewisham (None received)
Sarah Blow OHSEL Planned Care SRO Chief Officer, Bexley CCG
• None
Malcolm Hines OHSEL Planned Care CFO Chief Financial Officer, Southwark CCG
• None
Mark Easton OHSEL Programme Director Director of octopus Ltd

11 Confidential not for sharing outside of Evaluation Group|

12
Confidential not for sharing outside of Evaluation Group|
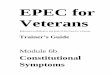
Travel & Access 6
Evaluation
Commentary 0 +5 -5
Criteria
-2 Option 1 Guys + Lewisham
Option 2 Guys + Orpington
Option 3 Orpington + Lewisham
-2
-2
Impact on total transport times
Description Supporting analysis
Travel time analysis (for patients by car and public transport including average travel times by mode of transport)
Weighting
17%
The evaluation panel recommend that given the current level of detail available, it would not be possible to differentiate between the three options and therefore all should be given a common negative score, as all proposals would require some patients to travel further. Further analysis should be explored in relation to the accuracy of the figures, the impact for patients who use the service, consideration of car parking issues and showing a clearer comparison of the impact of changes

13 Confidential not for sharing outside of Evaluation Group|
Following the initial review of the travel analysis by the evaluation panel the following points were highlighted for continued development
Points raised at the evaluation group
Programme response Timeframe
There was some uncertainty about whether modelled car journey times reflect actual journey times. Particular reference was made to trips to Orpington Hospital.
• Undertaking further independent checks of journey time data and reliability of travel models
• Develop presentation of metrics and analysis to clearly show the impact in terms of the increase in peoples journey times in more detail
• Undertake comparison between AM peak travel time and PM peak time
Available to evaluation panel
Analysis is undertaken for the whole population rather than patients who use the service.
• Travel analysis will be updated to understand the impact for actual service users
• A comparison can then be made between a patient’s nearest hospital and hospitals patient’s choose for care
Updated for the consultation period and included for decision making
Time taken / ability to park at provider sites is not included in analysis.
• This is recognised to be an issue at many sites in SEL, further feedback from the public on issues should be sought
Gain public feedback through consultation
Familiarity or complexity of journeys is a challenge for particular sections of the population – this has not been accounted for.
• Familiarity and complexity of journeys will be considered in detail as part of the development of the equalities analysis during consultation
During consultation
Delays to journeys and service cancellations are not taken into account.
• The model takes into account some delays and congestion as the data used is informed by real journey times.
N/A

14 Confidential not for sharing outside of Evaluation Group|
Checks of the car and public transport models have been undertaken against Google Maps online route planner.
• Travel times across the were compared with the times suggested by Google, if a time is within 20% of the time suggested by the model then the journey is deemed accurate. 20% has been used as a majority of the car journey times in the study area are within 30mins so equates to around 6 minutes difference at the most.
• Car travel AM peak. 40 journeys were assessed across all scenarios. 92% of these were within 20% of the time suggested by Google. 3 journeys were outside of the 20% range, 2 of these were journeys of 3 minutes where Google showed a 4 minute journey time.
• Public transport AM peak. 40 journeys were assessed across all scenarios. 70% of these were within 20% of the time suggested by Google. It should be noted that the walking speeds assessed in the model are slower (3.5km/h) than the DfT standard used by Google (4.8km/h)
• Comparisons were also made between the AM peak (7 -10am) and PM peak (4-6pm) travel times for car journeys. Average journey time across the whole study area was comparable in the AM peak and PM peak periods:
– AM peak average: 9.99 minutes
– PM peak average: 9.93 minutes

15 Confidential not for sharing outside of Evaluation Group|
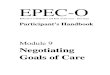
Car Travel time (AM peak, 7-10am)
% of SEL residents with Average increase in travel time
No increase in journey time
<10 min increase
10-20 min increase
>20 min increase
Option 1 (Guys’ and Lewisham) 32% 38% 27% 3% 7 mins Option 2 (Guy’s and Orpington) 14% 37% 40% 9% 10 mins Option 3 (Lewisham and Orpington) 28% 32% 40% 0% 7 mins
• More residents are affected by an increase in journey times in option 2 than options 1 and 3.
• The percentage of residents with an increase of between 10-20 mins is greater (40%) for options 2 and 3 than option 1 (27%)
• The percentage of residents with a less than 10 min increase is more comparable, between 38% and 32%
This suggests:
• Option 1 has the least impact overall on increased car travel time across all SEL residents.
• Option 2 has the most impact overall on increased car travel time across all SEL residents.

16 Confidential not for sharing outside of Evaluation Group|
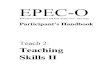
Public Transport Travel time (AM peak, 7-10am)
% of SEL residents with Average increase in travel time
No increase in journey time
<10 min increase
10-20 min increase
20-30 min increase
>30 min increase
Option 1 (Guys’ and Lewisham) 34% 24% 24% 12% 5% 11 mins
Option 2 (Guy’s and Orpington) 20% 30% 35% 13% 2% 12 mins
Option 3 (Lewisham and Orpington) 25% 18% 22% 27% 9% 15 mins
• More residents are affected by an increase in journey times in option 2 than options 1 and 3.
• The percentage of residents with an increase of between 20-30 mins is greater (27%) for options 3 than options 1 and 2 (12% and 13%)
• Increases of 10-20min and below 10 mins affect a higher percentage of people in option 2 (30% and 35%) compared with the other options.
This suggests:
• Option 1 has the least impact overall on increased public transport travel across all SEL residents.
• Option 2 has the most impact overall on increased public transport travel across all SEL residents.

17
Confidential not for sharing outside of Evaluation Group|
Evaluation
Commentary 0 +5 -5
Criteria
2 Option 1 Guys + Lewisham
Option 2 Guys + Orpington
Option 3 Orpington + Lewisham
3
2
Description Supporting analysis Weighting
Deliverability 7
7a. The option is sufficiently flexible, adaptable and resilient to meet the requirements of growth or changes in future demand or change in national policy. i.e. the option demonstrates appropriate flexibility
7b. Ease of implementation: the option can be delivered within a reasonable timescale with minimal risk around transition including impacts and disruption to existing services. Capacity and capability: The option demonstrates the appropriate capacity and capability to deliver the change/transition 7c. Where investment is required, the ease of obtaining required funding or financing is considered.
Points scored resilience to alternative demand scenarios (other than the central one)
Estimate of number of years for implementation Estimate of transition risk
Assessment of financing/funding options (shortlist only)
25%
The evaluation panel recommend the scoring based on: • The relative ease and timescales by when
Guy’s and Orpington can deliver 50% of SEL activity
• Lewisham was felt to score lower based on the level of capital required, longer timescales and larger step up in activity that would need to be delivered

18
Confidential not for sharing outside of Evaluation Group|
Evaluation
Commentary 0 +5 -5
Criteria
3 Option 1 Guys + Lewisham
Option 2 Guys + Orpington
Option 3 Orpington + Lewisham
4
2
Description Supporting analysis Weighting
Quality 8
The operating model provides evidence on how it will optimise both functional and clinical outcomes for all patients receiving elective orthopaedic care in SEL.
Quality impact assessment (e.g. governance and quality systems) Comparison of current clinical quality of sites which are expected to deliver future inpatient activity under each option
17%
The evaluation panel recommend the scoring based on: • Guy’s having developed the most detail
regarding the clinical network and governance required.
• The centralisation of elective orthopaedic services on the Orpington site having already lead to better quality care.
• The Lewisham presentation did not describe the development of the wider clinical network in detail
It was agreed that this assessment was subject to comparison of each trust’s GRIFT report by the independent clinical expert

19 Confidential not for sharing outside of Evaluation Group|
Following the initial review of proposals, providers submitted their individual GRIFT reports to the independent clinical expert on the evaluation panel for review.
Conclusions drawn:
• No unit is consistently outstanding, though good practice exists in areas of all three bidders, suggesting that if the units are combined successfully and best practices adopted then performance should improve
• There is no outstanding differentiator from the available data, though Greenwich and Guy’s & St Thomas’ data was old (2014) and 2016 data should be made available
• Poor #NOF mortality rates at Lewisham and King’s/Orpington suggest investment will be needed for managing elderly joint replacement patients (Ortho-geriatric provision in the bids should be questioned)
• Better LOS for Guy’s & St Thomas’ suggests early adoption of modern pathways
It is therefore suggested that the panel retain the scorings agreed at the meeting on the 31st August as the data serves to corroborate the agreed points allocation.

20
Confidential not for sharing outside of Evaluation Group|
Evaluation
Commentary 0 +5 -5
Criteria
1 Option 1 Guys + Lewisham
Option 2 Guys + Orpington
Option 3 Orpington + Lewisham
2
1
Description Supporting analysis Weighting
Patient Experience
9
• The option promotes equality and minimises disadvantage of protected groups as required by the Equality Act
• The model demonstrates how it will optimise patient experience
• Equality impact assessment • Friends and family and CQC inpatient survey performance
against national benchmark 17%
The evaluation panel recommend that all proposals should receive +1 for the equalities component, however it was acknowledged that the continued development of the equalities analysis during consultation would support a better understanding of any differences by site and impact on travel for these populations. The panel agreed that the Option 2 should receive +2 overall due to the positive patient feedback of the service delivered at both sites

21
Confidential not for sharing outside of Evaluation Group|
Evaluation
Commentary 0 +5 -5
2 Option 1 Guys + Lewisham
Option 2 Guys + Orpington
Option 3 Orpington + Lewisham
3
1
Criteria Description Supporting analysis Weighting
Research & Education
The model provides support the further development of research and education activity
Assessment of impact on research and education
7% 10
The evaluation panel recommend the scoring based on: • Guy’s was felt to have the most potential
as a research centre • Orpington gave detail on the training and
development of anaesthetists and the potential research and education opportunities this could lead to.
• Lewisham’s presentation and Q&A did not provide sufficient additional detail of research and education planning

22
Confidential not for sharing outside of Evaluation Group|
Criteria
Evaluation
Commentary 0 +5 -5
1 Option 1 Guys + Lewisham
Option 2 Guys + Orpington
Option 3 Orpington + Lewisham
3
2
Description Supporting analysis Weighting
Workforce The option is staffable and is attractive to health care professionals working in SEL
• Estimate of future vs actual workforce • Estimate of impact on current job roles 17% 11
The evaluation panel recommend the scoring based on: • All options should be attractive places to
work compared to the current configuration, and hence evaluate positively
• Lewisham was felt to be a higher risk due to the number of appointments that would need to be made
• GSTT is noted as an attractive employer in SEL already
• Orpington can better mitigate transition risks for the workforce, having already had experience of consolidated services

23
Confidential not for sharing outside of Evaluation Group|
Travel & Access
Deliverability
Quality
Patient Experience
6
7
8
9
Research & Education
Workforce
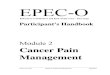
Non-Financial Evaluation Criteria
10
11
Impact on total transport times
Description
7a. The option is sufficiently flexible, adaptable and resilient to meet the requirements of growth or changes in future demand or change in national policy. i.e. the option demonstrates appropriate flexibility
7b. Ease of implementation: the option can be delivered within a reasonable timescale with minimal risk around transition including impacts and disruption to existing services. Capacity and capability: The option demonstrates the appropriate capacity and capability to deliver the change/transition 7c. Where investment is required, the ease of obtaining required funding or financing is considered.
The operating model provides evidence on how it will optimise both functional and clinical outcomes for all patients receiving elective orthopaedic care in SEL.
• The option promotes equality and minimises disadvantage of protected groups as required by the Equality Act
• The model demonstrates how it will optimise patient experience
The model provides support the further development of research and education activity
The option is staffable and is attractive to health care professionals working in SEL
Weighting
17%
25%
17%
17%
7%
17%
1.15 Option 1 Guys + Lewisham
Option 2 Guys + Orpington 2.15
Option 3 Orpington + Lewisham 1.08

24 Confidential not for sharing outside of Evaluation Group|

25 Confidential not for sharing outside of Evaluation Group|
Following the evaluation panel meeting held on the 31st August, all providers have resubmitted finance profromas that describe the costs expected if they were selected to host an EOC, if they weren’t selected to host an EOC and if there was no change in service configuration.
• Following analysis the programme team it has not currently been possible to compare the three submissions in the detail required. This is due to potentially different approaches taken in the development of financial implications and costing, and different approaches to delivering the model of care.
• The agreed evaluation criteria states that the non-financial criteria will be scored separately to the financial assessment of the proposals. It should be noted that the financial analysis does not require scoring by the panel, as it will provide a direct comparable cost between each configuration option.
• Therefore as the panel has completed the scoring of the non-financial requirements it is suggested that the programme team meet individually with each provider to work through their financial assessment in detail and align the three submissions. The assessment will then be shared with the panel and wider stakeholders ahead of being presented to the Committee in Common in November.

26 Confidential not for sharing outside of Evaluation Group|