Embed Size (px)
Citation preview

since there is no clinical o r laboratory evidence for such. In addition, a short oral course of vitamin E raised the plasma level to well above average values. On the other hand, low plasma levels may reflect an increased demand for vitamin E as an antioxidant. Thus, the low levels may be secondary to primary oxidative damage involving the spinal neurons in WHD. A similar hypothesis was postulated to explain vitamin E deficiency in both thalassemia major [4] and the syndrome of ceroid lipofuscinosis and sea- blue histiocytes [81. In our series, the 3 infants who received pharmacological doses of vitamin E orally reached high plasma levels without any effect on the course of the disease. The same was observed in the other two disorders.
Vitamin E acts as a nonspecific antioxidant that prevents peroxidation of polyunsaturated fatty acids. The products of peroxidation can be highly damaging to the cell. I t is of interest that human infant brain, which is relatively abundant in highly unsaturated fatty acids, contains less tocopherol than any other tissue. It is therefore conceivable that the require- ment for vitamin E is higher in infants than in adults.
Although the role of vitamin E deficiency in W H D is not known, two implications are suggested by our observations: (1) plasma vitamin E levels may be used as a marker for early detection of W H D in hypotonic newborns and ( 2 ) high-dose vitamin E therapy may be indicated in infants with WHD.
Supported by a grant from the Muscular Dystrophy Association of America.
We thank Dr Gerald Fenichel for valuable comments and Mr P. Goldfeder, Ms M. Helfer, and Ms N. Ort for devoted tech- nical assistance.
References 1. Geller A, Gilles F, Schwachman H: Degeneration of the fas-
ciculus gracilis in cystic fibrosis. Neurology (Minneap) 27:185-187, 1977
2. Hashim SA, Schuttringer GR: Rapid determination of to- copherol in macro- and micro quantities of plasma. Am J Clin Nutr 19:137, 1966
3. Pentschew A, Schwartz K: Systemic axonal dystrophy in vita- min E deficient adult rats. Acta Neuropathol (Berl) 1:313-334, 1962
4. Rachmilewitz EA, Shiffer A, Kahane I: Vitamin E deficiency in P-thalassemia major: changes in hematological and bio- chemical parameters after a therapeutic trial with a-tocoph- erol. Am J Clin Nutr 32:1850-1858, 1979
5. Rosenblum JL, Keating JP, Nelson JS, Prensky AL: A progres- sive neurological syndrome in six children with chronic liver disease and alpha-tocopherol deficiency. Pediatr Res 12:555, 1978
6. Sung JH: Neuroaxonal dystrophy in mucoviscidosis. J Neu- ropathol Exp Neurol23:567-583, 1964
7. Sung JH, Stadlan EM: Neuroaxonal dystrophy in congenital biliary atresia. J Neuropathol Exp Neurol 25:341-361, 1966
8. Swaiman KF, Garg BP, Lockman LA: Sea-blue histiocyte and
9.
posterior column dysfunction: a familial disorder. Neurology (Minneap) 2 5 : 1084- 1087, 197 5 Tomasi LG: Reversibility of human myopathy caused by vita- min E deficiency. Neurology (Minneap) 2 9 1 182-1186, 1979
Computerized Tomography in Subacute Necrotizing Encephalomy elopathy (Leigh Disease) William J. Schwartz, MD," Harrol T. Hutchison, MD," and Bruce 0. Berg, MD"t
The computerized tomographic brain scans of two pa- tients with subacute necrotizing encephalomyelopathy contained symmetrical focal lesions that corresponded to the sites of known anatomical abnormalities in this disease.
Schwartz WJ, Hutchison HT, Berg BO: Computerized tomography in subacute necrotizing encephalomyelopathy (Leigh disease). Ann Neurol
10:268-271, 1981
Subacute necrotizing encephalomyelopathy (SNE) is a rare familial disorder, usually affecting infants and children, but with onset at any age [3 ,4] . The disease is characterized by distinctive pathological abnor- malities, with symmetrical and focal lesions in the brainstem tegmentum, lateral walls of the third ven- tricle, spinal cord, and basal ganglia. Microscopi- cally, capillary proliferation and myelin and dendritic destruction are seen with relative preservation of neuronal perikarya and axons [l, 33. Although the clinical diagnosis is difficult to establish, abnormal neurological signs include oculomotor and bulbar dysfunction, weakness, ataxia, dysphagia, and ab- normalities of breathing. Pyruvic and lactic acidemia has been described [6], and evidence suggests that SNE may be a disorder of brain pyruvate metabolism [ I , 51.
From the Departments of *Neurology and +Pediatrics, University of California, San Francisco, School of Medicine, San Francisco, CA 94143.
Received Nov 19, 1980, and in revised form Feb 18, 1981. Ac- cepted for publication Feb 21, 1981.
Address reprint requests to Dr Berg, Departments of Neurology and Pediatrics (Child Neurology), University of California, San Francisco, School of Medicine, San Francisco, CA 94143.
268 0364-5134/Sl/090268-04$01.25 @ 198 1 by the American Neurological Association

We have recent ly cared for t w o pat ients i n w h o m the diagnosis of SNE was suspected on clinical and biochemical grounds . CT brain scans suppor ted t h e diagnosis: symmetr ical focal lesions were observed that cor responded to the sites of known neuropatho- logical changes i n SNE. The diagnosis was confirmed at autopsy in Pat ient 1.
Patient 1 A 6-month-old white girl was transferred to the University of California, San Francisco, Medical Center for neurologi- cal evaluation. She was the 3.75 kg product of an uncom- plicated full-term pregnancy, labor, and delivery, and her early development had been normal until she developed otitis media at the age of 4 months. Thereafter she was lethargic, had a poor cry, and showed decreased spontane- ous movements. The patient’s father had a hemangioma of the right face and trunk but no seizures, mental retardation, or other neurological signs or symptoms.
General physical examination revealed a wasted infant with a cafi-au-lait spot on the left knee. H e r breathing was punctuated by occasional inspiratory gasps. Head circum- ference was 52.5 cm (50th percentile), and the fontanelle was closed. She was alert but did not interact with exam- iners, and she had an infrequent and feeble cry. Cranial nerve examination was notable for inability to maintain lateral gaze and occasional paroxysms of dysconjugate horizontal eye movements. She was restless and showed proximal ballistic and distal choreoathetotic movements,
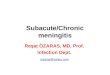
F i g 1 . C T brain scans in Patient 1 show bilaterally sjmmet- vical low-density area in the medial thalamus (arrows in A) and thvozlghout the midbrain (arrows in B).
primarily of the right limbs, as well as adventitial niove- ments of the mouth and tongue. There was less movement of the left limbs, and tone was moderately increased in those limbs. She had an obligate tonic neck reflex to the right. Deep tendon reflexes were brisk and plantar re- sponses were extensor.
The following laboratory studies were unremarkable: complete blood count, serum electrolytes, glucose, liver and renal function tests, chest roentgenogram, electrocar- diogram, erythrocyte protoporphyrin, serum ceruloplas- min, urinalysis, urine amino acids, ketoacids, mucopolysac- charides, reducing sugars, vanillylmandelic acid, mercury, and ferric chloride and nitroprusside tests. Arterial oxygen tension was 122 torr, carbon dioxide tension 22 torr, and p H 7.55. Serum lactate levels were elevated at 25 and 40 mgldl (normal, 5 to 18).
A lumbar puncture was traumatic, and the cerebrospinal fluid (CSF) was grossly bloody with 25,500 red cells and 36 white cells (90% polymorphonuclear leukocytes, 794 lym- phocytes, 2% monocytes, and 1% eosinophils). CSF glu- cose was 58 mg/dl, and protein, 60 mddl . Electromyo- graphic studies and nerve conduction velocities were normal. Brainstem evoked response monaurally on the right was normal, but on the left, components could not be identified. The electroencephalogram showed focal slow- ing in the right temporal leads, and there was no visual evoked response over the right cortex. The CT brain scan is shown in Figure 1.
The patient died one month later. Autopsy was performed and the gross findings were normal. The brain weighed 500 gm; cut sections revealed multiple foci of slightly hem- orrhagic granularity and softening in the thalamus, sub- thalamic nuclei, and substantia nigra. Microscopic sections from the thalamus, subthalamic nuclei, substantia nigra, and wall of the third ventricle revealed edematous areas of
Case Report: Schwartz et al: CT Scan in Leigh Disease 269

neuronal degeneration with microglial and astrocytic pro- liferation and a prominent proliferation of capillaries. Sec- tions taken through the mammillary bodies revealed no pathological abnormalities.
Patient 2 A 12-year-old white boy had been in good health until one month prior to admission, when, after a “flu-like’’ illness, he developed a voracious appetite, hyperpnea, and diplo- pia. His 15-year-old sister was still hospitalized fifteen months after the onset of an illness characterized by ophthalmoparesis, limb weakness, and respiratory embar- rassment requiring ventilatory assistance. She was said to have an elevated CSF protein and abnormal brainstem evoked responses. A clinical diagnosis of SNE had been made by the neurologist who referred the patient.
The general physical examination was normal except for a resting tachycardia of 140 beats per minute and occa- sional inspiratory gasps, although the patient denied dys- pnea. Neurological examination revealed a well-developed boy of normal intellect and mental status. There was no dysarthria. A left paralytic pontine exotropia, left ptosis, and mild facial diplegia were found on cranial nerve exam- ination. There was a mild spastic diplegia with abnormally brisk stretch reflexes, although the ankle jerks were less brisk than the quadriceps reflexes. Plantar responses were extensor bilaterally. Heel-to-shin and tandem gait testing were both mildly ataxic. The sensory examination revealed a subjective loss of temperature sensation to the knees bilaterally.
Fig 2. CT brain scans in Patient 2 show bilateral, symmetri- cal latencies adjacent to the fourth ventricle (arrows in A) as well as lucencies adjacent to the third ventricle in the anterior thalamus (arrows in B) .
The following laboratory studies were unremarkable: complete blood count, erythrocyte sedimentation rate, VDRL, serum electrolytes, glucose, liver and renal func- tion tests, protein electrophoresis, thyroid function tests, serum ceruloplasmin, urinalysis, urine amino acids, keto- acids, mucopolysaccharides, reducing sugars, urine ferric chloride, nitroprusside tests, and toxicology screen. Cre- atine phosphokinase was mildly elevated at 192 IU per liter (normal, 4 to 88); serum aldolase and glutamic oxaloacetic transaminase were normal. Arterial oxygen ten- sion was 124 torr, carbon dioxide tension 18 torr, and pH 7.56. Serum lactate was elevated at 23 mg/dl (normal, 5 to 18).
The CSF was clear and colorless with 7 red cells and 3 white cells (all mononuclear); CSF glucose was 55 mgldl and protein 50 mg/dl, with a normal electrophoresis. Viral and bacterial cultures were negative. Electromyography was normal, but motor nerve conduction velocity in the right common peroneal nerve was slowed to 28 m/sec (normal, 35.6 to 63.5 dsec ) . Brainstem evoked response monaurally on the right was normal, but there was a pro- longed latency of wave V on the left. An electroenceph- alogram was normal. The CT brain scan is shown in Fig- ure 2.
270 Annals of Neurology Vol 10 No 3 September 1981

Discussion The clinical diagnosis in these two patients was SNE, and the CT brain scan appearance was consistent with the described neuropathological features of this dis- ease. Although there is no pathological confirmation of the diagnosis in Patient 2 , the distinctive CT brain scan, when coupled with the constellation of clinical, neurophysiological, and biochemical findings and the positive family history, make the diagnosis of SNE almost certain. A previous report [21 has described the presence of symmetrical putaminal lucencies in the CT scan of four patients with SNE; with im- proved resolution of present CT scans, we now dem- onstrate the expected subtentorial lesions in the dis- ease.
The authors thank Dr Richard Wicklund and Dr Gary Franklin for referring these patients to the University of California, San Fran- cisco, for evaluation.
References 1.
2.
3.
4.
5.
6.
David RB, Mamunes P, Rosenblum W1: Necrotizing en- cephalomyelopathy (Leigh). In Vinken PJ, Bruyn GW (eds): Handbook of Clinical Neurology. Vol 28, Metabolic and Defi- ciency Diseases of the Nervous System, Part 11. New York, American Elsevier, 1976, chap 14, pp 349-363 Hall K, Gardner-Medwin D: CT scan appearances in Leigh's disease (subacute necrotizing encephalomyelopathy). Neu- roradiology 16:48-50, 1978 Montpetit VJA, Andermann F, Carpenter S, et al: Subacute necrotizing encephalomyelopathy: a review and a study of two families. Brain 94:l-30, 197 1 Pincus JH: Subacute necrotizing encephalomyelitis (Leigh's disease): a consideration of clinical features and etiology. Dev Med Child Neurol 14:87-101, 1972 Pincus JH, Solitaire GB, Itokawa Y , et al: Thiamine, thiamine triphosphate and nervous system lesions in subacute necrotiz- ing encephalomyelopathy. Neurology (Minneap) 2 1:444, 197 1 Worsley HE, Brookfield RW, Elwood JS, et al: Lactic acidosis with necrotizing encephalopathy in two sibs. Arch Dis Child 40:492-501, 1965
Mveloma Protein Sinthesis Within the CNS by Plasma Cell Tumors Tali Siegal, MD,"? Joshua Shorr, PhD," Isabelle Lubetzki-Korn, MD," Dov Soffer, MDJ Elizabeth Naparsrek, MD,$ Ron Tur-Kaspa, MD,$ and Oded Abramsky, MD, PhD"
Two patients had central nervous system involvement from plasma cell tumor, one with leptomeningeal infiltration and the other with solitary intracranial plasmacrytoma. In both, cerebrospinal fluid (CSF) elec- trophoresis revealed IgG monoclonal protein and an elevated IgG index consistent with local synthesis of the myeloma protein. The CSF findings were helpful in the diagnosis and evaluation of tumor recurrence.
Siegal T, Shorr J, Lubetzki-Korn I, Soffer D, Naparstek E, Tur-Kaspa R, Abramsky 0:
Myeloma protein synthesis within the CNS by plasma cell tumors. Ann Neurol 10:271-273, 1981
Myeloma protein is the marker for myeloma cells. Evidence of local synthesis of myeloma monoclonal protein within the central nervous system (CNS) would indicate the presence of secreting myeloma cells in the nervous system even if the cerebrospinal fluid (CSF) showed no cells. It would also increase the pathological importance of plasma cells found on cytological examination of the CSF.
We report two patients with CNS involvement by plasma cell tumors in whom analysis of CSF mono- clonal bands and elevated IgG index (CSFlserum IgG and CSFlserum albumin ratio) helped to make the diagnosis of CNS involvement and tumor recur- rence.
Patient 1 Multiple myeloma was diagnosed in August, 1978, in a 72-year-old woman with severe left sided-headaches of eight months' duration. The findings of paraproteinemia (IgG, K type) and a bone marrow examination revealing a predominance of plasma cells established the diagnosis. Her past history was noncontributory.
Neurological examination revealed left twelfth nerve paralysis. A bone survey (including the skull), bone scan, electroencephalogram, and CT scan were all normal. Mel-
From the Departments of 'Neurology, tOncology, $Pathology, and §Hematology, Hadasah-Hebrew University Hospital, PO Box 12000, Jerusalem 91220, Israel. Received Dec 2, 1980, and in revised form Feb 19, 1981. Ac- cepted for publication Feb 21, 1981. Address reprint requests to Dr Siegal.
0364-5134/81/090271-03$01.25 @ 1981 by the American Neurological Association 271