Embed Size (px)
Citation preview

Comparison of Rate Control versus Rhythm Controlfor Management of Atrial Fibrillation in Patients withCoexisting Heart Failure: A Cost-Effectiveness Analysis
Alexandra Perez, Pharm.D., M.S., Daniel R. Touchette, Pharm.D., M.A.,Robert J. DiDomenico, Pharm.D., Thomas D. Stamos, M.D., and Surrey M. Walton, Ph.D.
Study Objective. To compare lifetime costs and health outcomes of ratecontrol versus rhythm control for management of atrial fibrillation inpatients with coexisting heart failure from the third-party payerperspective.
Design. A Markov decision analysis model constructed from costs, utility, andtransition probability inputs obtained from randomized clinical trials andpublically available databases.
Patients. A simulated cohort aged 65 years or older with persistent orparoxysmal atrial fibrillation and heart failure.
Measurements and Main Results. Markov states for rhythm control werecardioversion plus amiodarone and maintenance amiodarone, and those forrate control were �-blocker, digoxin, and calcium channel blocker.Transition states included treatment success, hospitalizations for atrialfibrillation and/or heart failure, and severe adverse effects. Economicinputs included cost for drugs, cost of hospitalizations for atrial fibrillationand/or heart failure, and cost of management of severe adverse effects.Costs were measured in 2009 U.S. dollars, and clinical outcomes in quality-adjusted life-years (QALYs). One-way and multivariable sensitivityanalyses were conducted. Uncertainty intervals (UIs) were obtained fromprobabilistic sensitivity analyses. Rate control was found to be less costlyand more effective than rhythm control. Base case and probabilisticsensitivity analyses cost and effectiveness values for rate control were$7231 (95% UI $5517–9016) and 2.395 QALYs (95% UI 2.366–2.424QALYs); whereas those for rhythm control were $16,291 (95% UI$11,033–21,434) and 2.197 QALYs (95% UI 2.155–2.237 QALYs). Nocritical values were found for any model parameters in the one-waysensitivity analyses. The cost-effectiveness acceptability curves showedthat rate control was considered cost-effective in 100% of cases atwillingness-to-pay ratios between $0 and $200,000/QALY.
Conclusion. Rate control is less costly and more effective than rhythmcontrol and should be the initial treatment for atrial fibrillation amongpatients with coexisting heart failure.
Key Words: atrial fibrillation, heart failure, decision analysis, pharmaco-economics, Markov model, rate control, rhythm control.(Pharmacotherapy 2011;31(6):552–565)

RATE VS RHYTHM CONTROL IN ATRIAL FIBRILLATION AND HEART FAILURE Perez et al
Atrial fibrillation is the most common cardiacdysrhythmia, and its incidence is expected toincrease.1 There are different types of atrialfibrillation. Paroxysmal atrial fibrillation is anepisode of arrhythmia that usually terminatesspontaneously within 24–48 hours. If an atrialfibrillation episode lasts more than 7 days,however, it is called persistent atrial fibrillation.Other types are recurrent and permanent atrialfibrillation. Patients with atrial fibrillation have areduced quality of life, increased morbidity andmortality, and increased health care costs.2, 3
Heart failure is also a highly prevalent conditionand produces significant morbidity, mortality, anda tremendous economic burden.1 Atrial fibril-lation and heart failure have common risk factorsand frequently coexist.4 When occurringsimultaneously, these conditions contribute toeach other’s physiologic development andmaintenance, which leads to a worse prognosisthan with either condition alone.4, 5
For patients with atrial fibrillation, the optimaltreatment strategy—rate control versus rhythmcontrol—remains controversial despite anabundance of clinical trials. Substantially lessevidence comparing these treatment strategies inpatients with both atrial fibrillation and heartfailure is available. Most clinical studies havefound that among those with atrial fibrillation(with or without heart failure), the strategies ofrate and rhythm control are not significantlydifferent in reducing mortality6–9 or stroke.6, 9
Some evidence suggests that rate control mightimprove quality of life more than rhythmcontrol10; however, pharmacoeconomic analyses
have yielded mixed results.11–14
Until recently, studies comparing rate controlwith rhythm control in patients with coexistingatrial fibrillation and heart failure were limited toretrospective studies and post hoc analyses oflarger clinical trials.15, 16 The only large-scaleclinical trial that compared rate and rhythmcontrol in patients with both atrial fibrillationand heart failure mirrored results from earliertrials in the overall atrial fibrillation population,with no significant differences observed incardiovascular and overall mortality, stroke, andother outcomes.17 In addition, one randomizedclinical study found that patients receivingrhythm control had better health-related qualityof life than those receiving rate control treat-ment.18 However, we know of no publishedliterature that describes health care utilizationand costs of the management of atrial fibrillationin patients with heart failure. If the simultaneousexistence of atrial fibrillation and heart failureleads to a worse prognosis, it may not beappropriate to extrapolate the results from theoverall atrial fibrillation population to this subsetof patients.
The objective of this study was to comparelifetime costs and clinical effectiveness of ratecontrol versus rhythm control for atrial fibril-lation management in patients with coexistingheart failure from the third-party payer perspec-tive. The relative cost-effectiveness of these treat-ment methods was assessed by means of aMarkov decision analysis model.
Methods
Markov Model
Decision analytic modeling is growing inpopularity as a method to calculate costs andoutcomes in the health care field.19 Decisionanalytic models have often been used in healtheconomics to provide numeric and/or statisticalrepresentations of acute and chronic diseases.19
Markov models are a specific type of decisionanalysis model typically used to simulate chronicillnesses and calculate average costs and/orhealth consequences beyond the period observedin clinical trials.20 These models are also usefulwhen making complex decisions under uncertainconditions in clinical practice and for resourceallocation and policy.19
For a more detailed introduction to Markovmodeling of health care interventions, the readeris referred to a series of articles and a bookchapter.19–24 In short, when modeling a chronic
553
From the Department of Sociobehavioral andAdministrative Pharmacy, Nova Southeastern University,Fort Lauderdale, Florida (Dr. Perez); the Departments ofPharmacy Practice (Drs. Touchette and DiDomenico) andPharmacy Administration (Dr. Walton), and the Section ofCardiology (Dr. Stamos), University of Illinois at Chicago,Chicago, Illinois.
Dr. DiDomenico has received research support fromJohnson & Johnson Pharmaceutical Research andDevelopment, received speaker honoraria from sanofi-aventis and Bristol-Myers Squibb, and has served onadvisory boards for Arca Biopharma, Inc., and Merck & Co.
Presented at the annual meeting of the American Collegeof Clinical Pharmacy, Anaheim, California, October 18–21,2009.
Manuscript received October 12, 2010. Acceptedpending revisions November 2, 2010. Accepted forpublication in final form December 19, 2010.
For reprints, visit http://www.atypon-link.com/PPI/loi/phco.For questions or comments, contact Alexandra Perez,Pharm.D., M.S., Department of Sociobehavioral andAdministrative Pharmacy, Nova Southeastern University, 3200South University Drive, Fort Lauderdale, FL 33328.

PHARMACOTHERAPY Volume 31, Number 6, 2011
illness, a fundamental step is to define and createthe different stages of an illness represented byMarkov states. In the model, simulated patientspass through the Markov states as the modelcycles, to mimic the passing of time. Thesimulated patients continue to cycle as the illnessprogresses until they reach an absorbing state(usually death).
Another fundamental step is to create criteriathat determine how these patients move throughthe Markov states. These criteria are representedby transition states and transition probabilities.Transition states are temporary states thatdetermine whether patients will stay or move outof the current Markov state. Examples oftransition states are treatment success or failure,hospitalization or no hospitalization, alive ordead. Transition probabilities are defined as thelikelihood, for any given cycle or modeled periodof time, that a patient will move to a transitionstate (i.e., likelihood of either treatment successor failure). As simulated patients move betweenMarkov and transition states, costs and healthoutcomes are counted over time as the modelcontinues to cycle until everyone is in theabsorbing state or until a certain number ofcycles have been run.
Commonly used health outcome units are life-years or quality-adjusted life-years (QALYs),which are the average product of years of life andutility scores specific to the condition of interest.Markov models can calculate average costsand/or QALYs over many years, often for thepatient’s lifetime. Data used to populate thesemodels are usually obtained from observational,epidemiologic, and/or prospective studies (e.g.,clinical trials, databases, and registries). Thesemodels can be used to make comparisons of twoor more interventions in cost-effectivenessanalyses.
To determine how the variation of input valuesaffect the final results, sensitivity analyses mustbe conducted. Input values can be varied one ata time over a specified range (one-way sensitivityanalysis) or randomly all at once within anassigned distribution (probabilities sensitivityanalysis or second-order Monte Carlosimulation).
Data Sources
A literature search was conducted usingMEDLINE and EMBASE to aid in the design ofthis project (initial search January 2008, finalsearch January 2010). Results of the search were
limited to human studies published in theEnglish language, randomized clinical trials, andcontrolled clinical trials; the search was notlimited by year of publication. This literaturereview served two purposes. It guided theMarkov model structure design and was thesource for most input data such as transitionprobabilities, costs, and utilities. The followingsearch terms were used: atrial fibrillation, heartfailure, left ventricular dysfunction, �-blocker,digoxin, calcium channel blocker, andamiodarone. Class I antiarrhythmics were notincluded in the search because they should notbe used in patients with left ventriculardysfunction. Amiodarone was chosen as theantiarrhythmic of choice because it is mostcommonly used in the outpatient setting.
Studies of interest were those evaluatingparoxysmal or persistent atrial fibrillation withcoexisting left ventricular dysfunction, or heartfailure (New York Heart Association [NYHA]functional classes II–IV) in adults. Selection ofstudies as transition probability data sources usedthree criteria (in order of importance): forexternal validity purposes, priority was given tostudies conducted in the United States beforethose conducted in any other countries;randomized clinical trials were given prioritybefore prospective nonrandomized clinical trials,followed by randomized clinical trial subgroupanalyses, and retrospective studies; and thosestudies with at least 1 year follow-up in durationwere prioritized before a shorter time period.Only original research studies were included.
Outcomes of interest were efficacy, hospitali-zations for atrial fibrillation and/or heart failure,and severe adverse effects. Mortality in themodel is addressed below. Data were obtainedfrom literature concerning the atrial fibrillationpopulation if the outcomes of interest were notavailable in the atrial fibrillation–heart failureliterature, and studies were selected according tothe above-listed criteria.
Model Design and Main Outcomes
All model development and reporting of theresults followed the International Society forPharmacoeconomic and Outcomes Research andthe Panel for Cost-effectiveness in Medicineguidelines.19, 24 The model was built andanalyzed in TreeAge Pro 2009 (TreeAge Software,Inc., Williamstown, MA). A Markov decisionanalysis model was developed to comparepharmacologic rate control versus rhythm
554

RATE VS RHYTHM CONTROL IN ATRIAL FIBRILLATION AND HEART FAILURE Perez et al
control to determine which strategy was the leastcostly and most effective for patients with bothatrial fibrillation and heart failure. Because of thelack of publically available data sources withdirect nonmedical and indirect costs andconsequences, this study took the third-partypayer perspective. The Markov model builds onpatients with an established diagnosis of atrialfibrillation (paroxysmal or persistent) and heartfailure (defined as left ventricular ejection fraction≤ 40% and NYHA functional classes II–IVsymptoms). The starting age in the model was 65years, as atrial fibrillation and heart failure aremost prevalent among the elderly population. Tocalculate the lifetime average costs and QALYs, acohort analysis was run. Cycle length was 3months, and all simulations were followed untildeath. A life table for the general population fromthe Centers for Disease Control and PreventionWeb site was used and then adjusted to reflect thesurvival rate observed in the heart failurepopulation.19, 25 This rate has been reported to beless than 15% after 8–12 years.1 This modified lifetable was used to calculate the probability ofdeath in each cycle.
To develop the model, some importantassumptions were made. First, the incidence ofstroke and hemorrhagic events was assumed tooccur at the same rate across rate and rhythmcontrol interventions.6, 9, 17 Because of the higherrisk of stroke in patients with heart failure, weassumed all patients in the simulation receivedanticoagulant therapy with warfarin 5 mg/day forstroke prevention. Second, all patients in bothstrategies were assumed to be receiving standardheart failure management. Third, it was assumedpatients would remain in the rhythm associatedwith the assigned treatment—for rate control,remain in atrial fibrillation; for rhythm control,remain in sinus rhythm—unless the scenariosdescribed below occurred.
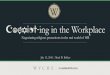
In general, rhythm control as the initial treat-ment strategy was compared with rate control asthe initial treatment strategy (Figure 1A). Bothstrategies shared the same Markov and transitionstates and input data. Transition states weretreatment response, hospitalization for atrialfibrillation and/or heart failure, and severeadverse effects prompting discontinuation of theindex drug (Figures 1B and 1C). Patientsremained in the same Markov state unlesstreatment failure, atrial fibrillation hospitali-zation, and/or a severe adverse effect occurred. Ifany of the latter occurred, patients moved to the
next rhythm control, rate control, or ablationstate, as applicable. A one-time procedure costwas added to patients cycling into the ablationstate; however, life expectancy accrued on eachcycle as long as they remained alive. Death wasthe absorbing state and occurred in any cycle andin any Markov state.
The main differences between treatmentstrategies were the initial treatment modality andthe order in which one cycled through theMarkov states. For example, patients in therhythm control strategy initially entered therhythm control Markov states (described below)and cycled through the rate control Markovstates or ablation state if treatment failures, atrialfibrillation hospitalization, or severe adverseeffects occurred. In contrast, patients in the ratecontrol strategy cycled first through the ratecontrol states (described below), then intorhythm control or ablation states if rate controlwas unsuccessful, an atrial fibrillation hospitali-zation occurred, or severe adverse effects occurred.The assumptions for each of the rate and rhythmcontrol Markov states used in the model aredescribed in more detail below.
Rhythm Control States
Both treatment strategies had two rhythmcontrol Markov states. The initial rhythm controlstate was “cardioversion plus amiodarone” inwhich electrocardioversion enhanced byamiodarone in the inpatient setting was followedby amiodarone for maintenance of sinus rhythm(Figure 1A and 1B). Before and during electro-cardioversion, amiodarone was assumed to begiven at loading doses of 800 mg/day for 14 daysfollowed by 300 mg/day for 4 weeks and 200mg/day for maintenance of sinus rhythm withinthe first 3 months.26, 27 Treatment failure wasdefined as converting back to atrial fibrillation.
The second Markov state was “maintenanceamiodarone,” and patients cycled into it if therapywas successful and no atrial fibrillation hospi-talizations or severe adverse effects occurred inthe previous state. In this state, long-term treat-ment with amiodarone 200 mg/day was given tomaintain sinus rhythm. Patients underwentrepeat cardioversion (maximum of two) if atrialfibrillation recurred after 3 months.26
In either of the rhythm control Markov states,severe adverse effects of amiodarone were assumedto be pulmonary fibrosis and hyperthyroidismprompting the discontinuation of the drug(Figure 1B).
555

PHARMACOTHERAPY Volume 31, Number 6, 2011
Rate Control States
Each treatment strategy had three rate controlMarkov states: “�-blocker” (metoprolol tartrateor carvedilol), “digoxin,” and “calcium channelblocker” (verapamil or diltiazem; Figure 1A and1C). Treatment failure was defined as theinability to maintain a target heart rate range, andthe main adverse effect considered was mild-to-moderate acute decompensation of heart failure
leading to discontinuation of the drug (Figure1C).
Transition Probabilities
Three studies were identified as the mainsources for the transition probabilities in themodel (Appendixes 1 and 2). Two of thesestudies were large, prospective, randomizedclinical trials—the Atrial Fibrillation and
556
AF/HF management
Rhythm control as initial treatment strategy
Rate control as initial treatment strategy
Cardioversion + amiodarone
Cardioversion + amiodarone
Maintenance amiodarone
Maintenance amiodarone
b-Blocker
b-Blocker
Calcium channel blocker
Calcium channel blocker
Digoxin
Digoxin
Ablation
Ablation
Death
Ablation
Death
Ablation
DeathDeath
Survive
Die
Survive
Die
[+]
[+]
[+]
[+]
[+]
[+]
[+]
[+]
[+]
[+]
Cardioversion + amiodaroneor maintenance amiodarone
Cardioversion + amiodarone
b-Blocker
Response
Failure
AF hospitalization
No AF hospitalization
Survive
Die
HF hospitalization
No HF hospitalization
Pulmonary fibrosis
No pulmonary fibrosis
Hyperthyroidism
No hyperthyroidism
First time
Second time
Ablation
Death
Death
Survive
Die
[+]
[+]
[+]
[+]
b-Blocker ordigoxin orcalcium channel blocker
Response
Failure
AF hospitalization
No AF hospitalization
Survive
Die
HF hospitalization
No HF hospitalization
HF leading to discontinuation of drug
No HF leading to discontinuation of drug
Ablation
Death
Death
Digoxin
Survive
Die
[+]
[+]
[+]
Figure 1. Markov decision analysis model used in our study. Square represents decision node, circle represents chance node, andtriangle represents terminal node. (A) Global structure of the model. Respective subtrees of the collapsed branches of the tree[+] are shown in B and C. (B) Model for rhythm control Markov states. Simulated patients began rhythm control managementand moved to rate control or ablation management based on transition state history. (C) Model for rate control Markov states.For B and C, respective subtrees of the collapsed branches [+] are the same as the chance node directly on top. Simulatedpatients began rate control management and moved to rhythm control or ablation management based on transition state history,so Markov states next to terminal nodes may vary throughout the model. AF = atrial fibrillation; HF = heart failure.
A
B
C

RATE VS RHYTHM CONTROL IN ATRIAL FIBRILLATION AND HEART FAILURE Perez et al
Congestive Heart Failure (AF-CHF)17 and theCanadian Trial of Atrial Fibrillation Investi-gators27 studies. The third study was a post hocanalysis of the Atrial Fibrillation Follow-upInvestigation of Rhythm Management (AFFIRM)28
study. In addition, the AF-CHF study investi-gators were contacted to obtain the frequencies ofhospitalizations due to atrial fibrillation andheart failure, and endocrine and pulmonarytoxicity produced by amiodarone.
Cost and Utilities
Costs of interest were extracted from fivesources. Inpatient costs for atrial fibrillation andheart failure hospitalizations and short-termmanagement of amiodarone-induced hyper-thyroidism were obtained from the HealthcareCost and Utilization Project database onlineaccess tool.29 Costs for electrocardioversion andablation procedures and pulmonary fibrosistreatment were extracted from a published cost-effectiveness analysis.30 Amiodarone costs wereobtained from the 2009 Red Book.31 Costs ofrate-slowing drugs and warfarin were obtainedfrom a pharmacy chain drug discount programthat offered a 90-day supply for a flat fee of $10for selected generic products, so a cost of zerowas assigned to these drugs.32 Warfarin moni-toring costs were obtained from a local pharmacist-run anticoagulation clinic. All costs were adjustedto 2009 U.S. dollars by using the medicalConsumer Price Index (Appendix 3).
Two sources were used to obtain the permanentquality-of-life adjustments or utility scores. Theheart failure utility and cardiac dysrhythmiadisutility were extracted from the Preference-based EQ-5D Index Scores for Chronic Condi-tions in the United States catalog (Appendix 4).33
The cardiac dysrhythmia disutility was added tothe baseline heart failure utility value and assignedto the rate control states because patients in thesestates were assumed to have both conditions.The utility value for the rhythm control stateswas the unmodified heart failure utility becausepatients were assumed to have this condition andbe in normal sinus rhythm. Utility value assump-tions for the short-term adjustment of quality oflife for the hospitalization and severe adverseeffect transition states were obtained from apublished study (adjustment made only forlength of time in transition state; Appendix 5).30
Utility and life expectancy values were used tocalculate QALYs.
Sensitivity Analysis
Deterministic and probabilistic sensitivityanalyses were conducted to test whether resultsand cost-effectiveness conclusions were robust tovariance in the model inputs. One-way sensi-tivity analyses were conducted by varying thecosts, transition probabilities, and utilities withina predetermined range while holding all othervalues constant. Unless a range was given, costsand transition probabilities were varied by 50%and 150% of the base case value. Utilities werevaried within two standard deviations for therespective International Classification of DiseasesNinth Revision code utility value in the catalog.33, 34
Discount rates were varied between 0% and 5%.Starting ages of 55 and 75 years were alsoexamined. A second-order Monte Carlo simulationwas conducted with 10,000 iterations. Beta distri-butions (i.e., continuous probability distributionsthat tend to resemble the normal distribution butare bounded on the interval 0–1) were assignedto all transition probabilities and permanentquality-of-life utility values.35 Costs were assigneda triangular distribution (i.e., a continuousprobability distribution with a set lower limit,mode, and upper limit that takes a triangularshape) in which the likeliest value was theidentified cost and the minimum and maximumvalues were 50% and 150% of the likeliest value.Uncertainty intervals were obtained fromprobabilistic sensitivity analyses. These resultswere also displayed by plotting each iteration onthe incremental cost-effectiveness plane andcreating acceptability curves. Finally, a micro-simulation was performed to evaluate the frequencyof hospitalizations and severe adverse effects.
Results
Base Case Analysis
As the initial treatment strategy, rate controlwas slightly more effective, resulting in 2.395QALYs (95% uncertainty interval [UI] 2.366–2.424 QALYs), than rhythm control, whichresulted in 2.197 QALYs (95% UI 2.155–2.237QALYs). Also, rate control was less costly at$7231 (95% UI $5517–9016) than rhythmcontrol at $16,291 (95% UI $11,033–21,434) asthe initial treatment strategy, making it thedominant alternative. The adjusted Centers forDisease Control and Prevention life tableproduced a probability of survival of 13% at 8years and less than 1% after 14 years.
557

PHARMACOTHERAPY Volume 31, Number 6, 2011
Sensitivity Analyses
One-way sensitivity analyses conducted on allmodel parameters, discount rate, and starting ageshowed that rate control as the initial treatmentstrategy was less costly and more effective thanrhythm control as the initial treatment strategy(data not shown). Probabilistic sensitivityanalysis results supported the base case conclu-sion, such that rate control was found to be lesscostly and more effective than rhythm control asthe initial treatment strategy (Table 1). Figure 2illustrates the probabilistic sensitivity analysisresults in an incremental cost-effective-ness planeand shows all iterations falling in the northwestquadrant where rhythm control is more costlythan rate control (positive incremental cost) andrhythm control is less effective than rate control(negative incremental QALY effect). Finally, theacceptability curve (not shown) showed that theprobability that rhythm control is cost-effectivewas 0% across a range of willingness-to-pay ratios($0–$200,000/QALY), including the most com-monly used reference cases in pharmacoeconomicanalyses ($50,000/QALY and $100,000/QALY).
Similar to the AF-CHF study, the first-orderMonte Carlo simulation (or microsimulation)showed that 19% of those receiving rate controlas the initial treatment strategy failed rate controltreatment, whereas 54% had at least one atrialfibrillation recurrence after 4 years in the alter-nate strategy. In addition, out of 10,000 trials,rhythm control as the initial treatment strategyhad 297 more hospitalizations for atrial fibril-lation, and 43 and 233 more events of pulmonarytoxicity and endocrine abnormalities caused byamiodarone, respectively, when compared withthe alternative. In contrast, rate control as theinitial treatment strategy had 738 morehospitalizations for heart failure and 195 moreepisodes of heart failure leading to the discon-tinuation of the rate control drug.
Discussion
This study found that having patients aged 65years or older with atrial fibrillation and heartfailure who begin rate control before rhythmcontrol produced a lifetime cost savings ofapproximately $9000/patient and an improve-ment in QALYs of approximately 0.19 whencompared with the opposite order of treatment.Based on our literature review, this is the firstpharmacoeconomic evaluation comparing ratecontrol versus rhythm control for the manage-ment of atrial fibrillation with coexisting heartfailure. Our model incorporated crossoverpatterns wherein patients would receive the alter-native therapy should the initial managementstrategy fail. We did so because it reflects bothobservations in clinical trials6, 17 and in currentpractice, and is recommended in the guidelines
558
Table 1. Probabilistic Sensitivity Analysis Results for Rhythm Control versus RateControl as Initial Treatment Strategy
Rhythm Control Rate ControlCost Effect Cost Effect
Statistic ($) (QALY) ($) (QALY)Mean 16,291 2.197 7231 2.395Standard deviation 2717 0.021 896 0.0152.5th percentile 11,033 2.155 5517 2.366Median 16,338 2.197 7225 2.39697.5th percentile 21,434 2.237 9016 2.424QALY = quality-adjusted life-years.
Figure 2. Incremental cost-effectiveness plane shows 10,000incremental cost-effectiveness ratios comparing rhythmcontrol versus rate control as initial treatment strategy fromthe probabilistic sensitivity analysis. Ellipse surrounds 95%of estimates. QALY = quality-adjusted life-years.

RATE VS RHYTHM CONTROL IN ATRIAL FIBRILLATION AND HEART FAILURE Perez et al
for developing decision models.19 In the clinicalsetting, physicians often have a patient begineither rate control or rhythm control and whenconfronted with suboptimal efficacy and/orsevere adverse effects, they are forced to switchthe patient to an alternative treatment.2 In thisstudy, crossover was triggered by treatmentfailure, hospitalizations, and severe adverseeffects. This model was calibrated to reflectsimilar treatment failure patterns observed in theAF-CHF study.17
Specific rate and rhythm control interventions inthe model were chosen based on national atrialfibrillation clinical practice guidelines2 andprotocols from clinical trials.6, 17, 27 Although theatrial fibrillation guidelines recommend the use of�-blockers and digoxin, they caution against theuse of calcium channel blockers for atrialfibrillation management in patients with heartfailure. Nevertheless, some studies have reportedthe use of calcium channel blockers in patientswith heart failure without major complications.15, 28
Also, current atrial fibrillation guidelines recom-mend aggressive rate control, but recommenda-tions might change based on recent findings inwhich lenient rate control is as effective as strictrate control.36 The recently published EuropeanSociety of Cardiology guidelines continue torecommend that the choice to start rhythmcontrol needs to be individualized, and the use ofrate control drugs such as �-blockers and digoxinmay be beneficial in patients with heart failure.37
Finally, a new antiarrhythmic drug, dronedarone,has shown mixed results in mortality outcomes inpatients with coexisting heart failure but has abetter adverse-effect profile than that ofamiodarone.38, 39 Further evidence is needed todetermine whether it is an adequate rhythmcontrol alternative in the population evaluated inthis study.
In the present study model, stroke rates andadverse effects such as hemorrhage were assumedto occur at the same rate across treatmentstrategies for two reasons. First, the AFFIRM,the How to Treat Chronic Atrial Fibrillation(HOT CAFE), and the AF-CHF studies found nosignificant differences in the occurrence of strokeor hemorrhagic events in patients receiving ratecontrol versus rhythm control.6, 9, 17 Second, theatrial fibrillation guidelines recommend that thesame thromboembolic prevention strategies beconsidered for both rate control and rhythmcontrol treatments.2 It was assumed that theentire population in this study was already at ahigher risk of stroke due to age and the coexis-
tence of heart failure, requiring warfarin forstroke prevention.
Several studies have shown no significantdifference in the effect of rate control or rhythmcontrol on life expectancy.6–9 Based on thisevidence, life expectancy in patients with atrialfibrillation was assumed to be the same in bothtreatment strategies in our model and wasadjusted to reflect the presence of heart failure inour hypothetical patient cohort. Consequently,differences in QALY units were driven primarilyby permanent and short-term quality-of-lifeadjustments (utility and disutility scores)assigned to the treatments in our model, whichparallel the differences in quality of life observedin a previously published study.18
The primary cost driver in the model washospital admission, reflecting a high rate ofhospitalization for recurrent atrial fibrillation.Furthermore, the impairment of atrial contrac-tion and fast ventricular rates that accompanyatrial fibrillation could lead to additional decom-pensation of heart failure, resulting in morehospital admissions. The role for the heartfailure hospitalization transition state in themodel was to account for these added costs aswell as short-term quality-of-life adjustment.
In our base case analysis, a cost of zero wasassigned to all rate-slowing drugs and warfarin inour model, assuming that the $10/90-day supplydiscount program offered by many pharmacychains is considered an out-of-pocket cost.32
Deterministic and probabilistic sensitivityanalyses including a maximum of $20 for thesedrug costs did not affect the final results andwere not a major cost driver in the model.Amiodarone was the only drug not included in adrug discount program and was assigned thedrug cost presented in Appendix 3.
We found no studies evaluating the economicimpact of coexisting atrial fibrillation and heartfailure or pharmacoeconomic studies comparinginterventions in this same population. In thegeneral atrial fibrillation literature, economicevaluations have found both rhythm control andrate control strategies to be cost-effective.11–14 In2006, a decision and cost-effectiveness analysiswas performed in patients with atrial fibrillation(without heart failure) by also using secondarydata sources and showed that rhythm controlwith left atrial catheter ablation was more costlybut more effective than pharmacologic rhythmcontrol and rate control in patients withmoderate and low risk of stroke.30 The authorsalso found that pharmacologic rhythm control
559

PHARMACOTHERAPY Volume 31, Number 6, 2011
with amiodarone was more costly and lesseffective than rate control. Although theobservations in that study were similar to ourfindings, a few differences in study design andinputs are worth mentioning. In that analysis,the authors assumed different stroke rates whenin atrial fibrillation or normal sinus rhythm andwhen taking aspirin or warfarin for stroke pre-vention. As a result, some of the cost assump-tions incorporated into their model differed fromthose described herein. Also, those authorsfound that the cost-effectiveness of the therapieswas sensitive to several parameters. By contrast,sensitivity analyses performed in our studyyielded robust results: all parameters weretested, and no critical values were found toinfluence the results of the base case.
Limitations
This study has several limitations. First, thereis potential bias in the underlying data sources.To address this bias, a systematic review of theliterature was conducted to identify the mostrigorous data available and all data sources, datainputs, and assumptions have been clearlydescribed (Appendixes 1–4). Further, deter-ministic and probabilistic sensitivity analyseswere conducted to test this uncertainty, and allsupported the base case results. Second, theassumption that patients in the rate control statesremained in atrial fibrillation may not reflect realclinical scenarios. In practice, patients mayspontaneously convert to sinus rhythm whiletaking rate control drugs, potentially affectingtheir health status and quality of life. However,some evidence suggests that cardiac rhythmstatus fails to demonstrate an effect on mortalityor worsening heart failure.40
Third, patients entering the model wereassumed to have the same symptomatic profile.In practice, however, a treatment strategy may bedetermined based on the severity of a givenpatient’s symptoms. However, the atrial fibril-lation guidelines state that, in “patients withsymptomatic atrial fibrillation lasting manyweeks, initial therapy may be anticoagulation andrate control while the long-term goal is to restoresinus rhythm.”2 Fourth, this study took a third-party payer perspective; however, the societalperspective is the reference standard. Fifth,amiodarone-induced drug toxicities wereassumed to incur only short-term costs anddeficits in quality of life. In reality, they maybecome chronic conditions that increase events
and costs, and may worsen humanistic outcomes.Sixth, emergency room costs and other
ambulatory care costs were assumed to be thesame across groups. Similar to hospitalizationrates, it has been reported that patients receivingrhythm control have had a larger number ofemergency room visits compared with thosereceiving rate control.12 If this is the case, thecost-effectiveness of rhythm control in this studywould be further reduced. Finally, these resultsmay not be extrapolated to atrial fibrillationoccurring in younger patients; those with lone,permanent, or postoperative atrial fibrillation; orthose without heart failure. Further, the effect ofsex on the results was not evaluated.
Conclusion
Based on the findings of this study, werecommend that rate control be given strongconsideration as the initial treatment of choicefor patients with both atrial fibrillation and heartfailure. However, because of limitations in ouranalysis and uncertainty in key estimatesidentified in the literature, we understand thatsome individuals (e.g., those with refractorysymptoms and/or intolerances to rate-slowingdrugs) may be better served by beginning therapywith rhythm control.
Acknowledgments
We would like to acknowledge Ms. Sylvie Levesqueand Dr. Denis Roy from the Montreal Heart InstituteCoordinating Center, Université de Montréal, forproviding us with additional data inputs needed inthis model.
References1. Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease
and stroke statistics—2009 update: a report from the AmericanHeart Association statistics committee and stroke statisticssubcommittee. Circulation 2009;119:480–6.
2. Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006guidelines for the management of patients with atrialfibrillation—executive summary: a report of the AmericanCollege of Cardiology/American Heart Association task force onpractice guidelines and the European Society of Cardiologycommittee for practice guidelines. J Am Coll Cardiol2006;48:854–906.
3. Wu EQ, Birnbaum HG, Mareva M, et al. Economic burden andco-morbidities of atrial fibrillation in a privately insuredpopulation. Curr Med Res Opin 2005;21:1693–9.
4. Wang TJ, Larson MG, Levy D, et al. Temporal relations ofatrial fibrillation and congestive heart failure and their jointinfluence on mortality: the Framingham heart study.Circulation 2003;107:2920–5.
5. Piccini JP, Hernandez AF, Zhao X, et al. Quality of care foratrial fibrillation among patients hospitalized for heart failure. JAm Coll Cardiol 2009;54:1280–9.
6. Wyse DG, Waldo AL, DiMarco JP, et al, for the Atrial
560

RATE VS RHYTHM CONTROL IN ATRIAL FIBRILLATION AND HEART FAILURE Perez et al
Fibrillation Follow-up Investigation of Rhythm Management(AFFIRM) Investigators. A comparison of rate control andrhythm control in patients with atrial fibrillation. N Engl J Med2002;347:1825–33.
7. Van Gelder IC, Hagens VE, Bosker HA, et al. A comparison ofrate control and rhythm control in patients with recurrentpersistent atrial fibrillation. N Engl J Med 2002;347:1834–40.
8. Carlsson J, Miketic S, Windeler J, et al. Randomized trial ofrate-control versus rhythm-control in persistent atrialfibrillation: the strategies of treatment of atrial fibrillation(STAF) study. J Am Coll Cardiol 2003;41:1690–6.
9. Opolski G, Torbicki A, Kosior DA, et al. Rate control vsrhythm control in patients with nonvalvular persistent atrialfibrillation: the results of the Polish how to treat chronic atrialfibrillation (HOT CAFE) study. Chest 2004;126:476–86.
10. Thrall G, Lane D, Carroll D, Lip GY. Quality of life in patientswith atrial fibrillation: a systematic review. Am J Med2006;119:448.e1–19.
11. Hagens VE, Vermeulen KM, TenVergert EM, et al. Rate controlis more cost-effective than rhythm control for patients withpersistent atrial fibrillation: results from the rate control versuselectrical cardioversion (RACE) study. Eur Heart J 2004;25:1542–9.
12. Marshall DA, Levy AR, Vidaillet H, et al. Cost-effectiveness ofrhythm versus rate control in atrial fibrillation. Ann Intern Med2004;141:653–61.
13. Catherwood E, Fitzpatrick WD, Greenberg ML, et al. Cost-effectiveness of cardioversion and antiarrhythmic therapy innonvalvular atrial fibrillation. Ann Intern Med 1999;130:625–36.
14. Eckman MH, Falk RH, Pauker SG. Cost-effectiveness oftherapies for patients with nonvalvular atrial fibrillation. ArchIntern Med 1998;158:1669–77.
15. Al-Khatib SM, Shaw LK, Lee KL, O’Connor C, Califf RM. Isrhythm control superior to rate control in patients with atrialfibrillation and congestive heart failure? Am J Cardiol2004;94:797–800.
16. Hagens VE, Crijns HJ, Van Veldhuisen DJ, et al. Rate controlversus rhythm control for patients with persistent atrialfibrillation with mild to moderate heart failure: results from therate control versus electrical cardioversion (RACE) study. AmHeart J 2005;149:1106–11.
17. Roy D, Talajic M, Nattel S, et al, for the Atrial Fibrillation andCongestive Heat Failure Investigators. Rhythm control versusrate control for atrial fibrillation and heart failure. N Engl J Med2008;358:2667–77.
18. Shelton RJ, Clark AL, Goode K, et al . A randomised,controlled study of rate versus rhythm control in patients withchronic atrial fibrillation and heart failure: CAFE–II study.Heart 2009;95:924–30.
19. Weinstein MC, O’Brien B, Hornberger J, et al. Principles ofgood practice for decision analytic modeling in health-careevaluation: report of the ISPOR task force on good researchpractices—modeling studies. Value Health 2003;6:9–17.
20. Touchette DR, Hartung D. Markov modeling. In: Grauer DW,Lee J, Odom TD, et al, eds. Pharmacoeconomics and outcomes:applications for patient care, 2nd ed. Kansas City: AmericanCollege of Clinical Pharmacy, 2003:206–30.
21. Sonnenberg FA, Beck JR. Markov models in medical decisionmaking: a practical guide. Med Decis Making 1993;13:322–38.
22. Briggs A, Sculpher M. An introduction to Markov modellingfor economic evaluation. Pharmacoeconomics 1998;13:397–409.
23. Miller DK, Homan SM. Determining transition probabilities:confusion and suggestions. Med Decis Making 1994;14:52–8.
24. Siegel JE, Weinstein MC, Russell LB, Gold MR. Recommen-dations for reporting cost-effectiveness analyses: panel on cost-effectiveness in health and medicine. JAMA 1996;276:1339–41.
25. Centers for Disease Control and Prevention. Abridged lifetable. Available from http://www.cdc.gov/nchs/data/nvsr/nvsr58/nvsr58_21.pdf. Accessed June 1, 2009.
26. The Atrial Fibrillation and Congestive Heart FailureInvestigators. Rationale and design of a study assessingtreatment strategies of atrial fibrillation in patients with heartfailure: the atrial fibrillation and congestive heart failure (AF-CHF) trial. Am Heart J 2002;144:597–607.
27. Roy D, Talajic M, Dorian P, et al, for the Canadian Trial ofAtrial Fibrillation Investigators. Amiodarone to preventrecurrence of atrial fibrillation. N Engl J Med 2000;342:913–20.
28. Olshansky B, Rosenfeld LE, Warner AL, et al. The atrialfibrillation follow-up investigation of rhythm management(AFFIRM) study: approaches to control rate in atrialfibrillation. J Am Coll Cardiol 2004;43:1201–8.
29. Agency for Healthcare Research and Quality. Healthcare costand utilization project (HCUP). Available from http://hcupnet.ahrq.gov/HCUPnet.jsp?Id=0D7AE842178B078B&Form=SelDB&JS=Y&Action=%3E%3ENext%3E%3E&_DB=NIS06. AccessedMay 21, 2010.
30. Chan PS, Vijan S, Morady F, Oral H. Cost-effectiveness ofradiofrequency catheter ablation for atrial fibrillation. J AmColl Cardiol 2006;47:2513–20.
31. Thomson Healthcare. Red book: pharmacy’s fundamentalreference, 113th ed. Montevale, NJ: Thomson Reuters, 2009.
32. Walmart.com. Retail prescription program drug list. Availablefrom http://i.walmartimages.com/i/if/hmp/fusion/customer_list.pdf. Accessed May 20, 2010.
33. Sullivan PW, Ghushchyan V. Preference-based EQ-5D indexscores for chronic conditions in the United States. Med DecisMaking 2006;26:410–20.
34. Sullivan PW, Lawrence WF, Ghushchyan V. A national catalogof preference-based scores for chronic conditions in the UnitedStates. Med Care 2005;43:736–49.
35. Briggs AH. Handling uncertainty in cost-effectiveness models.Pharmacoeconomics 2000;17:479–500.
36. Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versusstrict rate control in patients with atrial fibrillation. N Engl JMed 2010;362:1363–73.
37. Camm AJ, Kirchhof P, Lip GY, et al. Guidelines for themanagement of atrial fibrillation: the task force for themanagement of atrial fibrillation of the European Society ofCardiology (ESC). Eur Heart J 2010;31:2369–429.
38. Hohnloser SH, Crijns HJ, van Eickels M, et al. Effect ofdronedarone on cardiovascular events in atrial fibrillation. NEngl J Med 2009;360:668–78.
39. Kober L, Torp-Pedersen C, McMurray JJ, et al. Increasedmortality after dronedarone therapy for severe heart failure. NEngl J Med 2008;358:2678–87.
40. Talajic M, Khairy P, Levesque S, et al. Maintenance of sinusrhythm and survival in patients with heart failure and atrialfibrillation. J Am Coll Cardiol 2010;55:1796–802.
561

PHARMACOTHERAPY Volume 31, Number 6, 2011562
Appendix 1. Studies Identified as Data Sources for Transition Probabilities
Study, Design,Follow-up Period Population TreatmentAF-CHF study, History of atrial fibrillation and NYHA Electrocardioversion + amiodarone 10 mg/kg/dayrandomized controlled, classes II–IV heart failure within (dose rounded up to the nearest 200 mg) x 14 days,3.1 yrs17 previous 6 mo or LVEF ≤ 25%; then 300 mg/day x 4 wks, then 200 mg/day during
mean age 67 yrs follow-up (rhythm control)26
Metoprolol, carvedilol, or bisoprolol with digitalis(rate control)
Canadian Trial of Atrial Symptomatic, paroxysmal atrial Amiodarone 10 mg/kg/day x 14 wks, then 200 mg/dayFibrillation Investigators, fibrillation; mean age 65 yrs during follow-up (rhythm control)randomized controlled,1.3 yrs27
AFFIRM, randomized Atrial fibrillation likely to be �-Blocker with or without digoxin (rate control)controlled, post hoc recurrent with history of heart Calcium channel blocker with or without digoxinanalysis, 3.5 yrs28 failure symptoms or LVEF < 40%; (rate control)
mean age 70 yrs Digoxin alone (rate control)n/N = number of patients in which event occurred/total number of patients in respective intervention group; AF-CHF = Atrial Fibrillation andCongestive Heart Failure; NYHA = New York Heart Association functional classification; LVEF = left ventricular ejection fraction; NA = notapplicable; NR = not reported; R = reported, but not used in the simulation; AFFIRM = Atrial Fibrillation Follow-up Investigation of RhythmManagement.Unless specified, follow-up times were used to calculate transition probabilities.PubMed medical subject heading (MeSH) terms used: (amiodarone OR adrenergic beta antagonists OR digoxin OR calcium channel blockers)AND (atrial fibrillation AND heart failure OR left ventricular dysfunction).EMBASE Emtree terms used: (amiodarone OR beta adrenergic receptor blocking agent OR digoxin OR calcium channel blocking agent) AND(heart atrium fibrillation AND heart failure OR heart left ventricle failure).aValues are presented as reported in each study.bEvents and sample size obtained from AF-CHF study investigators; events defined as number of patients hospitalized at least once duringfollow-up.cDefined by AF-CHF study investigators as endocrine abnormalities caused by amiodarone.dDefined by AF-CHF study investigators as pulmonary toxicity.eProportion of patients with atrial fibrillation during follow-up (failure).fProportion of patients who maintained the target heart rate at 3 years (success).gNumber of patients receiving amiodarone who had first recurrence of atrial fibrillation during follow-up (failure).hProportion of patients with successful rate control at 1 year among those with atrial fibrillation and history of heart failure symptoms or LVEF< 40% (subgroup analysis).iNumber of patients with atrial fibrillation with or without heart failure during follow-up period (main analysis).

RATE VS RHYTHM CONTROL IN ATRIAL FIBRILLATION AND HEART FAILURE Perez et al 563
Appendix 1. (continued)
Treatment Hospitalization Hospitalization Heart FailureSuccess or for Atrial for Heart Pulmonary Leading to Drug
Failure Fibrillation Failure Hyperthyroidism Fibrosis Discontinuation(% or n/N)a (n/N) (n/N) (n/N) (n/N) (n/N)
15% at 1 yr, 18% at 2 yrs, 108/672b 173/672b 25/672b, c 4/672b, d NA25% at 3 yrs, 27% at 4 yrs(Fig 1A)e
88% at 3 yrsf 62/683b 174/683b NA NA NR
71g/201 NR NR R R NA
R NR NR NA NA 14/777i
59%h NR NR NA NA 22/777i
54%h NR NR NA NA 1/777i
Appendix 2. Base Case and Sensitivity Analysis Transition Probabilities
Equivalent 3-Month Low–High Distribution Type3-Month Annual Probability Values for Probabilistic
Transition Transition for One-Way SensitivityProbability Category Probabilities Probabilities Sensitivity Analysis AnalysisRhythm control states
Treatment failureElectrocardioversion + amiodarone17 0.0397 at 1 yr 0.15 at 1 yr 0.02–0.11 Beta
0.0485 at 2 yrs 0.18 at 2 yrs0.0696 at 3 yrs 0.25 at 3 yrs0.0756 at 4 yrsa 0.27 at 4 yrs
Maintenance amiodarone27 0.0804 0.28 0.040–0.121 BetaHospitalization for atrial fibrillation17, b 0.0111 0.04 0.006–0.017 BetaHospitalization for heart failure17, b 0.0188 0.07 0.009–0.028 BetaPulmonary fibrosis17, b 0.0004 0.001 0.0004–0.001 BetaHyperthyroidism17, b 0.0024 0.010 0.003–0.008 Beta
Rate control statesTreatment failure
�-Blocker17 0.0106 0.04 0.005–0.016 BetaDigoxin28 0.1426 0.46 0.071–0.214 BetaCalcium channel blocker28 0.1238 0.41 0.062–0.186 Beta
Hospitalization for atrial fibrillation17, b 0.0060 0.02 0.003–0.009 BetaHospitalization for heart failure17, b 0.0186 0.07 0.009–0.028 BetaDiscontinuation of drug due toheart failure�-Blocker28 0.0013 0.005 0.001–0.002 BetaDigoxin28 0.0001 0.0004 0.00005–0.0001 BetaCalcium channel blocker28 0.0020 0.008 0.001–0.003 Beta
AF-CHF = Atrial Fibrillation and Congestive Heart Failure; AFFIRM = Atrial Fibrillation Follow-up Investigation of Rhythm Management.Calculation of 3-mo transition probabilities: event probabilities were calculated by dividing the number of events of interest in the studypopulation by the sample size of the group of interest. The 3-mo transition probabilities were calculated from event probabilities by using theTreeAge Pro 2009 function ProbtoProb(prob;multiplier). The “prob” in parenthesis represents the event probability obtained from theliterature, and the “multiplier” converts the probability to the time length of interest. This function is equivalent to using the followingequation: P(0.25) = 1 – e –[(–ln(1 – p)/t] • 0.25, where p(0.25) represents the transition probability per 0.25 yrs (3 mo), p represents the eventprobability, and t represents the follow-up time period reported in the individual study.aSame transition probability used after 4 yrs until simulations fall in the absorbing state.bOutcome frequencies were obtained from the AF-CHF study investigators.

PHARMACOTHERAPY Volume 31, Number 6, 2011564
Appendix 3. Base Case and Sensitivity Analysis Costs
3-Month Low-High Values,Base Case One-Way
Variable Value Sensitivity Analysis Base Case Sourcea
Warfarin + anticoagulation monitoring $105 $70–160 Warfarin $10/90-day supply,Warfarin 0 $0–20 considered out-of-pocket cost,32 +Anticoagulation monitoring $105 $70–140 $30/monitoring visit x 3.5 visits in
3-mo period; visit cost varied by± $10/visit
Total inpatient electrocardioversion + amiodarone $4757 $618–7975 $540 ($300–1200) for procedureElectrocardioversion procedure $653 $363–1452 + $3000 ($1800–4800) forTelemetry admission $3630 $0b–5808 telemetry admission30 (2004 USD,
CPI factor 1.21)Amiodarone 800 mg/day x 14 days, then 300 $369 $185–555 Amiodarone AWP $2.53mg/day x 4 wks, then 200 mg/day (146 tablets) ($1.27–3.80)/tablet31
Warfarin + anticoagulation monitoring $105 $70–160
Total maintenance amiodarone $333 $184–502 Amiodarone AWP $2.53Amiodarone 200 mg/day orally (90 tablets) $228 $114–342 ($1.27–$3.80)/tablet31
Warfarin + anticoagulation monitoring $105 $70–160
Total �-blocker $105 $70–180 Metoprolol or carvedilol: $10/90-dayMetoprolol or carvedilol 0 $0–20 supply for any dose, consideredWarfarin + anticoagulation monitoring $105 $70–160 out-of-pocket cost32
Total calcium channel blocker $105 $70–180 Diltiazem or verapamil: $10/90-dayDiltiazem or verapamil 0 $0–20 supply for any dose, consideredWarfarin + anticoagulation monitoring $105 $70–160 out-of-pocket cost32
Total digoxin $105 $70–180 Digoxin: $10/90-day supply for anyDigoxin 0 $0–20 dose, considered out-of-pocket cost32
Warfarin + anticoagulation monitoring $105 $70–160
Total ablation (pulmonary vein or $19,965 $16,335–23,595 Inpatient procedure: $16,500atrioventricular catheter ablation) ($13,500–19,500)30
(2004 USD, CPI factor 1.21)
Total hospitalization for atrial fibrillation $8272 $4136–12,408 Statistics for U.S. communityhospitals, ICD–9 code 427.31,atrial fibrillation for ages 65–84 yrs(n=197,744) $7804 (2007 USD,CPI factor 1.06), mean length ofstay 3.8 days29
Total hospitalization for acute $11,098 $5549–16,647 Statistics for U.S. communitydecompensation of heart failure hospitals, ICD–9 code 428,
heart failure for ages 65–84 yrs(n=426,984) $10,470 (2007 USD,CPI factor 1.06), mean length ofstay 5.3 days29
Total hospitalization for pulmonary toxicity $10,406 $8349–12,584 $8600 ($6900–10,400)(2004 USD, CPI factor 1.21),mean length of stay 14 days30
Total treatment of amiodarone-induced $7046 $3523–10,569 Statistics for US communityhyperthyroidism hospitals, ICD-9 code 242.9,
thyrotoxicosis for ages 65–84 yrs(n=780) $6647 (2007 USD, CPIfactor 1.06), mean length of stay4.2 days29
USD = U.S. dollars; CPI = (medical) Consumer Price Index; AWP = average wholesale price; ICD-9 = International Classification of Diseases,Ninth Revision.All costs are reported in 2009 USD.aDistribution type was triangular for total costs in the probabilistic sensitivity analysis.bMinimum value of $0 to represent outpatient cardioversion costs.

RATE VS RHYTHM CONTROL IN ATRIAL FIBRILLATION AND HEART FAILURE Perez et al 565
Appendix 4. Permanent Quality-of-Life Adjustment
Low–High Values,Base Case One-Way
Category Utilities Sensitivity Analysis Base Case Source33, a
Electrocardioversion + 0.708 0.7012–0.7148 ICD-9 428 (heart failure): 50th percentile EQ-5Damiodarone, normal sinus score, SE 0.0002 and n=284 used to calculaterhythm 2 SDs for sensitivity analysis values
Maintenance amiodarone, 0.708 0.7012–0.7148 ICD–9 428 (heart failure): 50th percentile EQ-5Dnormal sinus rhythm score, SE 0.0002 and n=284 used to calculate
2 SDs for sensitivity analysis values
�-Blocker, atrial fibrillation 0.689 0.6840–0.6940 ICD-9 427 (cardiac dysrhythmias) disutility value(–0.0190) added to ICD-9 428 to represent alower utility, SE 0.0001 and n=649 used tocalculate 2 SDs for sensitivity analysis values
Digoxin, atrial fibrillation 0.689 0.6840–0.6940 ICD-9 427 (cardiac dysrhythmias) disutility value(–0.0190) added to ICD-9 428 to represent alower utility, SE 0.0001 and n=649 used tocalculate 2 SDs for sensitivity analysis values
Calcium channel blocker, 0.689 0.6840–0.6940 ICD-9 427 (cardiac dysrhythmias) disutility valueatrial fibrillation (–0.0190) added to ICD-9 428 to represent a
lower utility, SE 0.0001 and n=649 used tocalculate 2 SDs for sensitivity analysis values
Ablation, normal sinus 0.708 0.7012–0.7148 ICD-9 428 (heart failure): 50th percentile EQ-5Drhythm score, SE 0.0002 and n=284 used to calculate
2 SDs for sensitivity analysis valuesICD-9 = International Classification of Diseases, Ninth Revision; SE = standard error; SD = standard deviation.aDistribution type was beta for all utilities in the probabilistic sensitivity analysis.
Appendix 5. Short-term Quality-of-Life Adjustment forTransition States
Time PeriodCategory Utilities (days)Hospitalization for atrial 0.530 3.829
fibrillationHospitalization for acute 0.530 5.329
decompensation ofheart failure
Pulmonary fibrosis 0.530 1430
Hyperthyroidism 0.530 4.229
Discontinuation of drug 0.530 1a
due to heart failureElectrocardioversion + — 330
amiodarone telemetryadmission
Ablation — 130
aA time period was not assigned to this utility.