Embed Size (px)
Citation preview

at SciVerse ScienceDirect
DERMATOLOGICA SINICA 32 (2014) 113–114
Contents lists available
Dermatologica Sinica
journal homepage: http: / /www.derm-sinica.com
CORRESPONDENCE
Coexisting staphylococcal scalded skin syndrome and acute generalizedexanthematous pustulosis
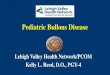
Figure 1 (A) Perioral exudation and crusting with radial fissures; (B) pinhead-sizedpustules with underlying erythematous base and desquamation.
Dear Editor,
Staphylococcal scalded skin syndrome (SSSS) is caused by epi-dermolytic toxins produced by Staphylococcus aureus and charac-terized by blistering and superficial desquamation.1 Acutegeneralized exanthematous pustulosis (AGEP) is most often causedby drugs and is characterized by the rapid occurrence of many ster-ile, nonfollicular pustules, usually arising on an edematous ery-thema and often accompanied by leukocytosis and fever.2 Wepresent a case of a 3-year boywith initial SSSS, who then developedAGEP due to erythromycin.
A 3-year-old boy presented with fever, sore throat, desquama-tion in the neck, and progressive malaise. His family physicianthus prescribed erythromycin and ibuprofen suspension. However,pustular lesions erupted on his neck the day after the first intake ofmedication, and grew to involve the other major skin folds thefollowing day. The child grew increasingly lethargic and com-plained of periorbital pain. He was brought to our emergencydepartment and was admitted on suspicion of SSSS.
On physical examination, the child’s temperature was 38.2�Cand he appeared acutely ill. The white blood cell count was20,900/mL. The patient had periorbital erythema that was tenderon palpation, and perioral exudation and crusting, with radial fis-sures around the mouth (Figure 1A), but no lesions on the oral mu-cosa. Desquamation as well as pinhead-sized pustules overlying theerythematous base was observed around the neck, axilla, and thegroin region (Figure 1B). Bacterial cultures of a pustule weredone, which were later found to be negative. A skin biopsy wastaken from his neck. The specimen demonstrated two histologicalpatterns: the left side of the specimen contained a subcorneal cleftand the right side showed intraepidermal pustules (Figure 2A). Thesubcorneal cleft, under higher magnification, showed acantholysiswith minimal inflammation, which is consistent with SSSS(Figure 2B). On the other side of the specimen, the intraepidermalspongiform pustules were infiltrated by abundant neutrophils inthe papillary dermis, findings consistent with AGEP (Figure 2C).Thus, the biopsy showed two distinct disease processes, SSSS andAGEP, in accordance to history and clinical presentation.
The patient was started on intravenous oxacillin 500 mg q6hand clindamycin 150 mg q8h, and antibiotic treatment continuedthroughout hospitalization (8 days). The intermittent feverresolved on Day 6; desquamation on the trunk improved bydischarge on Day 8. The patient was discharged on cloxacillin250 mg q8h and clindamycin 150 mg q8h for the remainder ofthe course. There has been no recurrence to date.
1027-8117/$ – see front matter Copyright � 2013, Taiwanese Dermatological Associatiohttp://dx.doi.org/10.1016/j.dsi.2013.04.004
The clinical and pathologic features of the case point to an initialSSSS with subsequent development of AGEP, according to thecriteria proposed by Roujeau et al.3 Tracing back the medical his-tory, ibuprofen had been previously administered and no adverseevents had occurred. Erythromycin was thus considered the culpritdrug for AGEP.
This is an unusual case of SSSS coexisting with AGEP. The exfo-liative phase of SSSS is often heralded by perioral exudation andcrusting with large radial fissures, but does not involve the mucosalmembranes, as occurred in our patient. There is usually no historyof drug exposure. The most reliable diagnostic tool remains a skinbiopsy.1 Our biopsy specimen showed a large subcorneal cleft for-mation, with acantholysis in the superficial epidermis and no trace
n. Published by Elsevier Taiwan LLC. All rights reserved.

Figure 2 (A) Biopsy specimen shows a subcorneal cleft on the left and intraepidermalpustules on the right; (B) a subcorneal cleft with acantholysis with minimal inflamma-tion; (C) intraepidermal spongiform pustules with abundant neutrophils in the papil-lary dermis. (Hematoxylin and eosin; A, 20�; B and C, 200�.)
Correspondence / Dermatologica Sinica 32 (2014) 113–114114
of neutrophils in the bullae; a finding consistent with SSSS but un-explainable by AGEP.
There arefive criteria forAGEP: (1) sudden eruptionof numerous,small (<5mm) non-follicular pustules; (2) fever� 38�C; (3) neutro-philia and/or mild eosinophilia; (4) histological evidence of subcor-neal or intraepidermal pustules; and (5) acute evolution withspontaneous resolution in <15 days.2,3 Our case met all the clinicalcriteria and the biopsy specimen showed histological changesconsistent with AGEP.
AGEP is induced by drugs in >90% of cases.2 Various drugs havebeen implicated in AGEP,4 with antibiotics (such as
aminopenicillins and macrolides including erythromycin) beingthe most common triggers.4 Antibiotics implicated in AGEP gener-ally have a short latent period of 1 day to 3 days from drug admin-istration to pustular eruption, compared with 11 days for all otherassociated drugs.4 In our case, the AGEP occurred 1 day followingthe intake of erythromycin, which had not been previously taken,making it the most likely culprit.
Collating the clinical and histological findings in our case, wesurmise that the rhino-pharyngitis in this 3-year-old boy provideda distant, extracutaneous focus of S. aureuswith subsequent releaseof exotoxin, resulting in SSSS, and erythromycin initiated secondaryAGEP.
In conclusion, this case illustrates the importance of obtaining agood history, as well as being alert to possible AGEP occurring sub-sequent to initial treatment for an unrelated disease. Also, the rightdiagnosis and subsequent treatment are in contradiction to eachother in this case. If one were to treat this case as purely SSSS,then the offending antibiotics would have been continued with apotentially disastrous consequence. By contrast, if one erroneouslythought this was simply AGEP, then no additional medicationwould have been given for SSSS, and additional systemic corticoste-roids would have caused a worse outcome. Therefore, cliniciansshould include AGEP as a differential diagnosis once pustular erup-tion appears following antibiotics treatment for SSSS. Promptrecognition and discontinuation of the suspected culprit antibioticare imperative for optimal outcome.
Thomas Waitao ChuDepartment of Dermatology, Far Eastern Memorial Hospital, New Taipei City, Taiwan
Oriental Institute of Technology, New Taipei City, Taiwan
Shu-Hui WangDepartment of Dermatology, Far Eastern Memorial Hospital, New Taipei City, Taiwan
Oriental Institute of Technology, New Taipei City, Taiwan
Ching-Chi ChiDepartment of Dermatology, Chang Gung Memorial Hospital, Chiayi, Taiwan
College of Medicine, Chang Gung University, Taoyuan, Taiwan
Cheng-Hsiang HsiaoDepartment of Pathology, Cheng Hsin General Hospital, Taipei, Taiwan
Lin-Hui Su*
Department of Dermatology, Far Eastern Memorial Hospital, New Taipei CIty, Taiwan
*Corresponding author. Department of Dermatology, Far Eastern MemorialHospital, No. 21, Sec. 2, Nanya S. Rd, New Taipei City 220, Taiwan.
E-mail address: [email protected]
Conflicts of interest: The authors declare that they have no financial or nonfinancialconflicts of interest related to the subject matter or materials discussed in this article.
References
1. Ladhani S, Joannou CL. Difficulties in diagnosis and management of the staphy-lococcal scalded skin syndrome. Pediatr Infect Dis J 2000;19:819–21.
2. Sidoroff A, Halevy S, Bavinck JN, Vaillant L, Roujeau JC. Acute generalized exan-thematous pustulosis (AGEP)–a clinical reaction pattern. J Cutan Pathol 2001;28:113–9.
3. Roujeau JC, Bioulac-Sage P, Bourseau C, et al. Acute generalized exanthematouspustulosis. Analysis of 63 cases. Arch Dermatol 1991;127:1333–8.
4. Sidoroff A, Dunant A, Viboud C, et al. Risk factors for acute generalized exan-thematous pustulosis (AGEP)-results of a multinational case-control study(EuroSCAR). Br J Dermatol 2007;157:989–96.
Received: Jan 9, 2013Revised: Apr 8, 2013
Accepted: Apr 26, 2013