Embed Size (px)
DESCRIPTION
Norwood
Citation preview

INTRODUCTION
The Norwood-based strategy for single ventricle palliation has improved with technical innova-tions and refinements over the last decades; such as regional cerebral perfusion during aortic arch reconstruction [1], placement of a right ven-tricle-to-pulmonary artery (RV-PA) shunt rather than a systemic-to-pulmonary shunt [2, 3], and the concept of aggressive afterload reduction to maximise oxygen delivery following Norwood procedure [4, 5].
However, Norwood-based palliation continues to have significant early and interstage mortal-ity in the current era with the majority of deaths occurring in the peri-operative period after the Norwood procedure [3, 6, 7]. After Stage I Nor-wood procedures, the presence of a systemic-to-pulmonary shunt contributes to the intrinsic instability of an ‘in-parallel’ circulation in which blood flow distribution may be altered sig-nificantly with perturbations in the ratio of sys-temic to pulmonary vascular resistance and this vulnerability is compounded in the early post-operative period with post-cardioplegia related depression of cardiac output. Cardiopulmonary bypass (CPB) and deep hypothermic circulation arrest (DHCA) contribute to a subsequent sys-temic inflammatory response which also has a negative impact on the Norwood physiology in the early postoperative period.
CORRESPONDENCE
Christopher A. Caldarone, MD, Professor and Chair, Division of Cardiac Surgery, University of Toronto,Watson Family Chair in Cardiovascular Science – Labatt Family Heart Center,Hospital for Sick Children, 555 University Avenue, Toronto, Ontario, Canada, M5G 1X8
Tel: 416-813-6420 Fax: 416-813-7984 E-mail: [email protected]
ISSN 2042-4884
ABSTRACT
Current surgical palliation for neonates with single ventricle physiology includes Norwood-based and Hybrid-based surgical strategies. When transplantation is not available, clinicians must choose between these two strategies with distinctly different learning curves and risk profiles. The Norwood strategy has evolved over several decades while the rising popularity of the Hybrid strategy is a much more recent addition to our therapeutic options. Based upon the premise that avoiding cardio pulmonary bypass in the neonatal period and deferral of aortic arch reconstruction until a second stage procedure have an important influence on outcomes, the Hybrid strategy has compelling theoretical advantages and disadvantages in comparison to the Norwood strategy. The purpose of this review is to summarise the currently available data to support – or refute – the theoretical advantages of the Hybrid strategy within the context of the Norwood strategy.
Comparison of Hybrid and Norwood Strategies in Hypoplastic Left Heart Syndrome
SURGERY | REVIEW
Hideyuki Kato, MD, Osami Honjo, MD, PhD, Glen Van Arsdell, MD, Christopher A. Caldarone, MDDivision of Cardiovascular Surgery, Hospital for Sick Children, Labatt Family Heart Center
Received 12/12/2011, Reviewed 27/12/2011, Accepted 1/1/2012 Key words: Hybrid strategy, Norwood strategy, single ventricle, hypoplastic left heart syndromeDOI: 10.5083/ejcm.20424884.70
Interstage mortality between Stage I and Stage II palliation is also significant (10.5 - 22%) [3, 6] and may be influenced by chronic volume load-ing of the systemic ventricle [8], arrhythmias and shunt-related problems. These intrinsic prob-lems with the Norwood strategy have encour-aged the development of an alternative ‘Hybrid’ strategy.
The hybrid palliative strategy has evolved rap-idly in the last decade [9, 10] and is based on the placement of bilateral pulmonary artery (PA) bands, stenting of the ductus arteriosus, and atrial septostomy as Stage I palliation during the neonatal period, followed by arch reconstruc-tion and bidirectional cavopulmonary shunt as Stage II palliation at the age of four to six months. Stage I hybrid procedures avoid CPB, cardioplegic arrest, and CPB-associated postop-erative systemic inflammatory response.
Furthermore, by deferring aortic arch recon-struction, the hybrid strategy avoids surgical alterations in cerebral blood flow (DHCA and/or regional cerebral perfusion) in the neonatal period when the brain may be more susceptible to neurologic injury [11]. Potential disadvan-tages of hybrid palliation include obstruction of the aortic isthmus by stent deployment, subse-quent coronary and cerebral malperfusion, and mechanical distortion of the branch pulmonary arteries.
60 EUROPEAN JOURNAL OF CARDIOVASCULAR MEDICINE VOL II ISSUE I
61
Several institutions have reported a significant learning curve with the hybrid strategy [9, 12, 13] and we have recently reported measur-able trends toward improvement in outcomes, suggesting that in-stitutional learning is an important component in the development of this strategy.
COMPARISON BETWEEN HYBRID AND NORWOOD STRATEGIES
Early postoperative physiology after Stage I palliation
Pulmonary blood flow after Stage I palliation in Norwood and hy-brid patients is derived from systemic-to-pulmonary artery shunts with the objective of providing pulmonary blood flow which is suf-ficient for pulmonary gas exchange but controlled by the geometry of the shunts/bands to prevent excessive volume loading of the heart. In Norwood patients an aorto-pulmonary or a RV-PA shunt is used, whereas in hybrid patients banding of the proximal branch pulmonary arteries is used to control pulmonary blood flow.
The postoperative haemodynamics after first stage hybrid pallia-tion have not been extensively studied. As the hybrid strategy has evolved, avoidance of cardiopulmonary bypass was postulated to better preserve myocardial function when compared to first stage Norwood palliation. Using respiratory spectrometry, we compared postoperative hemodynamics and oxygen delivery between Stage I hybrid and Norwood patients and noted that the hybrid patients had higher systemic vascular resistance (SVR) during the first post-operative 48 hours after the Stage I procedure [14].
This change was associated with lower cardiac output, low systemic blood flow (Qs) and oxygen delivery. Interestingly, despite bilateral PA banding, total pulmonary vascular resistance and pulmonary blood flow (Qp) were not different between early postoperative Hybrid and Norwood patients.
HYBRID-BASED PALLIATION IN INFANTS WITH SINGLE VENTRICLE PHYSIOLOGY
EUROPEAN JOURNAL OF CARDIOVASCULAR MEDICINE VOL II ISSUE I
The ratio of pulmonary to systemic blood flow (Qp/Qs) after Stage I Norwood palliation was between 0.3 and 3.3 (mean 1.2±0.5) and, despite bilateral pulmonary artery banding, the Qp/Qs ranged from 0.4 to 5.7 (mean 1.7±1.0) after Stage I Hybrid palliation[14]. However, in the absence of post-cardioplegia deficits in myocardial performance, this level of overcirculation appears to be well toler-ated in Hybrid patients with normal myocardial reserve. It is impor-tant to note, however, that this was an uncontrolled comparison and the administration of vasodilators and inotropes was routinely used for the Norwood patients [15] and uncommonly used for the Hybrid patients. The noted differences between the groups may have reflected the management strategy rather than differences in the palliative strategies.
These data suggest that systemic afterload reduction such as milri-none and phenoxybenzamine may be important in the early post-operative period for post-Stage I Hybrid patients. Based on these findings, we have adopted a low threshold to employ systemic afterload reduction and inotropic support for neonates following Hybrid Stage I procedures – especially for those patients known to have diminished preoperative myocardial reserve. We also recog-nize the potential for pulmonary overcirculation in patients with diminished myocardial reserve and utilize standard intensive care unit (ICU) measures to limit pulmonary blood flow in patients with evidence of inadequate distal oxygen delivery.
Survival
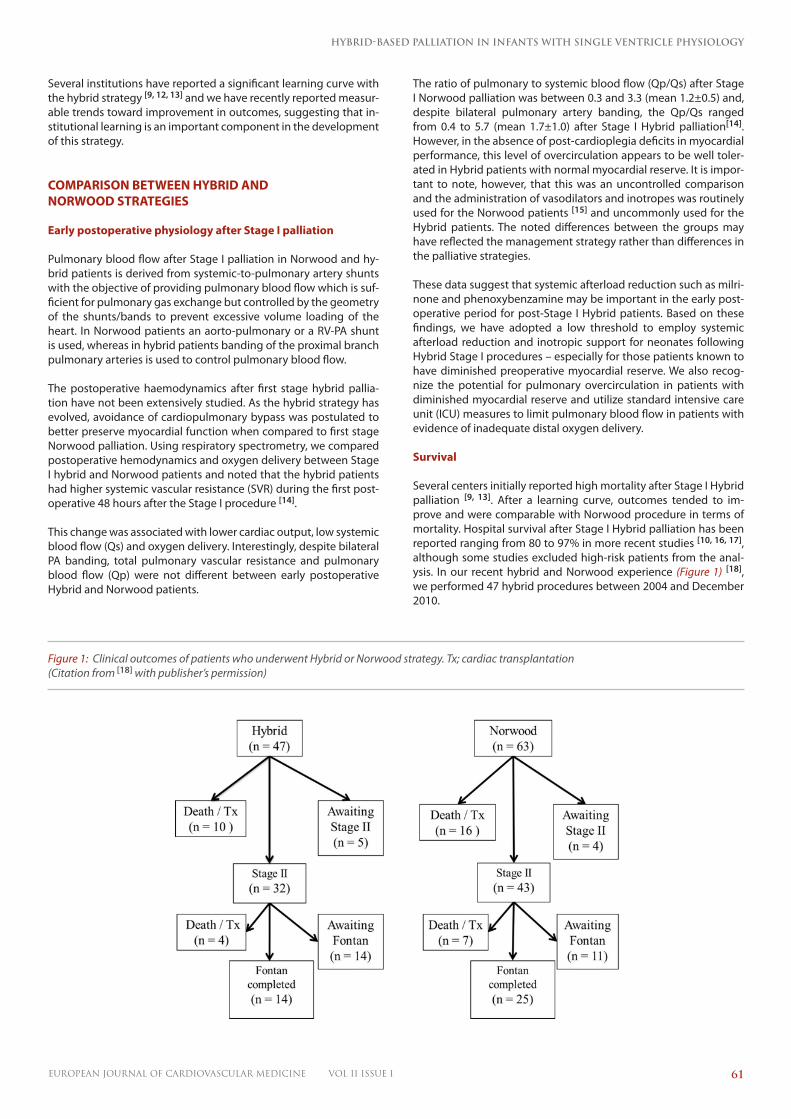
Several centers initially reported high mortality after Stage I Hybrid palliation [9, 13]. After a learning curve, outcomes tended to im-prove and were comparable with Norwood procedure in terms of mortality. Hospital survival after Stage I Hybrid palliation has been reported ranging from 80 to 97% in more recent studies [10, 16, 17], although some studies excluded high-risk patients from the anal-ysis. In our recent hybrid and Norwood experience (Figure 1) [18], we performed 47 hybrid procedures between 2004 and December 2010.
Figure 1: Clinical outcomes of patients who underwent Hybrid or Norwood strategy. Tx; cardiac transplantation (Citation from [18] with publisher’s permission)
HEALTHCARE BULLETIN | SURGERY
62 EUROPEAN JOURNAL OF CARDIOVASCULAR MEDICINE VOL II ISSUE I
These hybrid patients consist of all neonates palliated with the hybrid strategy excluding patients treated as a planned bridge to cardiac transplantation or critically ill patients who underwent the hybrid procedure as a salvage strategy. During the same period, the Norwood procedure was performed in 63 patients.
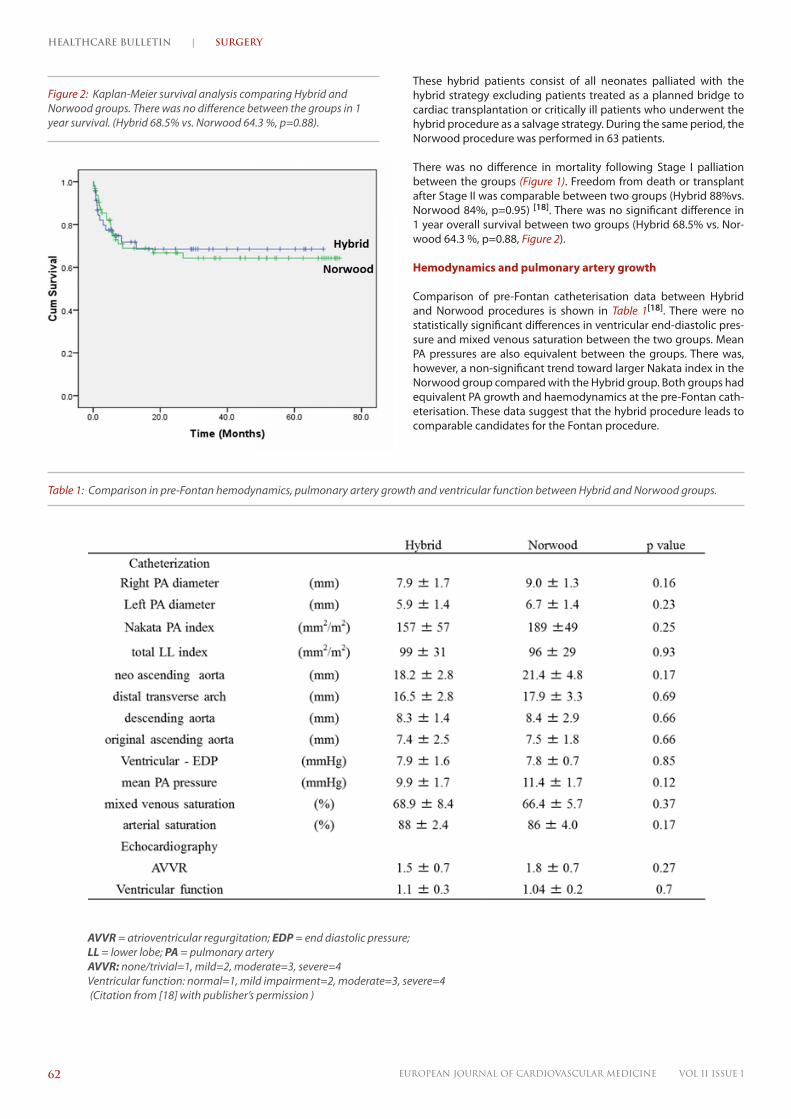
There was no difference in mortality following Stage I palliation between the groups (Figure 1). Freedom from death or transplant after Stage II was comparable between two groups (Hybrid 88%vs. Norwood 84%, p=0.95) [18]. There was no significant difference in 1 year overall survival between two groups (Hybrid 68.5% vs. Nor-wood 64.3 %, p=0.88, Figure 2).
Hemodynamics and pulmonary artery growth
Comparison of pre-Fontan catheterisation data between Hybrid and Norwood procedures is shown in Table 1[18]. There were no statistically significant differences in ventricular end-diastolic pres-sure and mixed venous saturation between the two groups. Mean PA pressures are also equivalent between the groups. There was, however, a non-significant trend toward larger Nakata index in the Norwood group compared with the Hybrid group. Both groups had equivalent PA growth and haemodynamics at the pre-Fontan cath-eterisation. These data suggest that the hybrid procedure leads to comparable candidates for the Fontan procedure.
Figure 2: Kaplan-Meier survival analysis comparing Hybrid and Norwood groups. There was no difference between the groups in 1 year survival. (Hybrid 68.5% vs. Norwood 64.3 %, p=0.88).
Table 1: Comparison in pre-Fontan hemodynamics, pulmonary artery growth and ventricular function between Hybrid and Norwood groups.
AVVR = atrioventricular regurgitation; EDP = end diastolic pressure; LL = lower lobe; PA = pulmonary arteryAVVR: none/trivial=1, mild=2, moderate=3, severe=4Ventricular function: normal=1, mild impairment=2, moderate=3, severe=4 (Citation from [18] with publisher’s permission )

HYBRID-BASED PALLIATION IN INFANTS WITH SINGLE VENTRICLE PHYSIOLOGY
63EUROPEAN JOURNAL OF CARDIOVASCULAR MEDICINE VOL II ISSUE I
Ventricular function and atrioventricular valve regurgitation
Preservation of ventricular function and prevention of atrioven-tricular valve regurgitation (AVVR) are critical determinants in the success of a single ventricle palliative strategy. These parameters may be jeopardised at many points in the Norwood single ventricle management strategy including:
1) myocardial ischemia-reperfusion injury after cardioplegic arrest at Norwood Stage I palliation, 2) volume overloading of the system-ic ventricle during the interstage period, and 3) impairment of the right ventricular function due to ventriculotomy at the site of con-struction of RV-PA conduits in Norwood patients treated with the Sano modification. On the other hand, the Hybrid procedure has potential for diminished myocardial function due to potential for restriction in coronary perfusion due to obstruction of retrograde aortic arch flow through the aortic isthmus after ductal stenting.
The influence of the obstruction of retrograde aortic arch on the Hybrid strategy
Obstruction of retrograde aortic arch flow in patients with dimin-ished prograde aortic flow (e.g. aortic atresia) can be associated with coronary and cerebral ischemia [19]. Obstruction can occur during the Hybrid Stage I procedure immediately after ductal stent deployment or the obstruction can develop in the interstage peri-od due to progressive ingrowth of fibrous tissue as the site of inter-section between the ductal stent and the aortic isthmus [13, 19, 20].
Stoica et al. described a treatment strategy for patients with ret-rograde aortic arch malperfusion based upon surveillance, detec-tion, and catheter-based treatment including retrograde stenting of the aortic isthmus in the subset of patients in whom surveillance resulted in detection of the stenosis. The strategy was associated with a high incidence of death or transplantation among patients in whom retrograde aortic arch obstruction was treated – suggest-ing that a treatment strategy may not be the optimal management plan for addressing retrograde aortic arch obstruction [19]. Because of the lack of success with a treatment strategy, the authors favour the Norwood strategy for patients who are considered at risk for retrograde aortic arch obstruction.
As an alternative to a treatment-based strategy, we have developed a preventative strategy to address potential for retrograde aortic arch obstruction in Hybrid patients. In this strategy, we utilise the creation of prophylactic ‘reverse Blalock-Taussig (BT) shunts’ for patients with restricted antegrade aortic flow and potential retro-grade aortic arch obstruction [21]. Importantly, we have not needed to utilise retrograde stenting of the aortic isthmus as a treatment for arch malperfusion in any of the patients with a prophylactic re-verse BT shunt. The reverse BT shunt may have helped to neutralise the risk of retrograde aortic arch obstruction. Because we have not detected a significant survival disadvantage in the high-risk sub-set of patients with severely diminished prograde arch flow, we are continuing to utilise the reverse BT shunt as a prophylactic compo-nent of our hybrid management strategy in this high- risk group.
Ventricular function and AVVR were not different in a comparison of the hybrid and Norwood groups at the pre-Fontan evaluation as shown in Table 1 (p-value = 0.7 and 0.27 respectively) [18]. These data indicate that the Hybrid strategy has equivalent results with Norwood strategy in terms of preservation of ventricular function and atrioventricular valve function.
Influence upon neurological development Neurological development is a major concern with any treatment strategy for single ventricle palliation. The mean neurocognitive test results in school-aged children with HLHS who underwent the Norwood procedure or cardiac transplantation are significantly below population normative values [22]. In addition, pre-operative brain magnetic resonance imaging revealed that brains of HLHS patients are smaller and less mature before surgery than patients without congenital heart disease [23]. Thus, the impact on neuro-logical development is of critical importance for the single ventricle strategies.
The Hybrid strategy has a potential advantage in terms of preserva-tion of neurologic function in comparison to the Norwood strategy. By delaying aortic arch reconstruction until the second stage proce-dure at four-six months of age for Hybrid patients, there is indirect evidence suggesting that the delay may have a favorable impact on the neurological development. Galli et al reported that the devel-opment of periventricular leukomalacia (PVL) after cardiac surgery is more prevalent in neonates compared with those at the age of more than one month [11] suggesting age-related vulnerability to neurologic injury. PVL in preterm infants is associated with subse-quent cerebral palsy, mental retardation, and learning disabilities. Thus, there is an age-dependent window of vulnerability to brain injury [11] and the Hybrid strategy may have an advantage in delay-ing aortic arch reconstruction from the neonatal period to four-six months of age. Objective demonstration of this advantage, how-ever, will require a controlled clinical trial.
In contrast to the age-related potential neurological advantage of the Hybrid strategy, there is a potential disadvantage with the Hy-brid strategy. As mentioned above, the obstruction of retrograde aortic arch flow can limit cerebral blood flow for four to six months prior to arch reconstruction at the Stage II procedure and long peri-ods of limited cerebral blood flow may be detrimental to neurolog-ic development. If the reverse BT shunt can successfully maintain arch perfusion, it may neutralise this problem. Further long term neurologic evaluation is required to compare the Norwood and Hy-brid strategies in the context of neurologic function.
Intubation time, intensive care unit stay and hospital stay Another potential benefit of Hybrid procedure is that Hybrid pa-tients have shorter total intubation time, ICU stay, and hospital length of stay (combined Stage I and II among survivors) [17, 24]. Galantowicz et al. reported that 85% of Hybrid patients at both Stage I and II were extubated in the first 24 hours [16]. Interestingly, in our experience, we have noted a time-related tendency toward improvement in the intubation time, the length of ICU stay, and hospital stay at the Hybrid Stage II, while concurrent Norwood pa-tients did not have evidence of time-related improvements in these parameters suggesting that we had reached a plateau in terms of refinement of the Norwood strategy [17].
Although there is less consumption of conventional measures of re-source utilisation including intubation time, ICU stay, and hospital length of stay in Hybrid strategy, unplanned reinterventions were more frequent in the Hybrid patients compared with the Norwood patients [18] (Hybrid 31.3% vs. Norwood 9.3%, p=0.016, Figure 3). Any comparison of resource utilisation must include quantification of planned and unplanned hospital admissions, procedures and interventions. Therefore, we are currently undertaking a study to examine total resource utilisation in a comparison of two palliative strategies.

HEALTHCARE BULLETIN | SURGERY
64 EUROPEAN JOURNAL OF CARDIOVASCULAR MEDICINE VOL II ISSUE I
Figure 3: Freedom from unplanned reintervention after Stage II between Hybrid and Norwood groups at 3 years. Unplanned reintervention rate was higher in Hybrid group compared to Norwood group (31.3% vs. 9.3%, p=0.016). This data does not include unplanned reinterventions prior to Stage II (Citation from [18] with publisher’s permission).
CONCLUSIONS
Hybrid palliation is an evolving surgical strategy with comparable survival to reported Norwood-based series. The Hybrid strategy provides equivalent pre-Fontan haemodynamics and pulmonary artery growth, preserves ventricular and atrioventricular valve function, and reduces resource utilisation. The comparative impact of the two different surgical strategies on neurological outcome is not defined and should be a subject of prospective trials.
FUTURE DIRECTIONS
Important questions to frame comparisons of the Hybrid and Nor-wood strategies include:
1. Which strategy is associated with better long term neurodevelopmental outcomes?
There are compelling arguments for and against each strategy. In the past, the timing of arch intervention was immutable – and hy-poplastic aortic arches required repair in the neonatal period. With the Hybrid strategy, it is now possible to defer aortic arch recon-struction and test the hypothesis that age is an important mediator of the vulnerability to injury after aortic arch reconstruction.
2. Which strategy produces the better Fontan candidate?
The Fontan procedure represents the convergence point for both management strategies. Parameters for this comparison include haemodynamics, ventricular function, valvular competence and pulmonary artery growth.
3. Which strategy is associated with the most efficient use of resources when quantifying the entire resource burden from birth to Fontan procedure?
If all other factors are equal, the superior strategy is the one that utilizes the least resources and poses the smallest burden on insti-tutions and families.
Based on demonstration of equivalent survival, a prospective randomised trial should be undertaken to compare the Norwood and Hybrid strategies in the context of these three fundamental questions.
HYBRID-BASED PALLIATION IN INFANTS WITH SINGLE VENTRICLE PHYSIOLOGY
65EUROPEAN JOURNAL OF CARDIOVASCULAR MEDICINE VOL II ISSUE I
REFERENCES Bacha, E.A., S. Daves, J. Hardin, et al., Single-ventricle palliation for high-risk neonates: the emergence of an alternative hybrid stage I strategy. J Thorac Cardiovasc Surg, 2006. 131(1): p. 163-171 e2.
Li, J., G. Zhang, L. Benson, et al., Comparison of the profiles of postoperative systemic hemodynamics and oxygen transport in neonates after the hybrid or the Norwood procedure: a pilot study. Circulation, 2007. 116(11 Suppl): p. I179-87.
Li, J., G. Zhang, B.W. McCrindle, et al., Profiles of hemodynamics and oxygen transport derived by using continuous measured oxygen consumption after the Norwood procedure. J Thorac Cardiovasc Surg, 2007. 133(2): p. 441-8.
Galantowicz, M., J.P. Cheatham, A. Phillips, et al., Hybrid approach for hypoplastic left heart syndrome: intermediate results after the learning curve. Ann Thorac Surg, 2008. 85(6): p. 2063-70; discussion 2070-1.
Honjo, O., L.N. Benson, H.E. Mewhort, et al., Clinical outcomes, program evolution, and pulmonary artery growth in single ventricle palliation using hybrid and Norwood palliative strategies. Ann Thorac Surg, 2009. 87(6): p. 1885-92; discussion 1892-3.
Baba, K., O. Honjo, Y. Kotani, et al., Survival, reintervention, and pulmonary vascular status after Stage II palliation for neonate with Hypoplastic Left Heart Syndrome: Hybrid vs. Norwood strategies. Paper presented at; American Heart Association, Scientific Sessions 2011, November 12-16, 2011; Orland, Florida.
Stoica, S.C., A.B. Philips, M. Egan, et al., The retrograde aortic arch in the hybrid approach to hypoplastic left heart syndrome. Ann Thorac Surg, 2009. 88(6): p. 1939-46; discussion 1946-7.
Egan, M.J., S.L. Hill, B.L. Boettner, et al., Predictors of retrograde aortic arch obstruction after hybrid palliation of hypoplastic left heart syndrome. Pediatr Cardiol, 2011. 32(1): p. 67-75.
Caldarone, C.A., L.N. Benson, H. Holtby, et al., Main pulmonary artery to innominate artery shunt during hybrid palliation of hypoplastic left heart syndrome. J Thorac Cardiovasc Surg, 2005. 130(4): p. e1-2.
Mahle, W.T., K.J. Visconti, M.C. Freier, et al., Relationship of surgical approach to neurodevelopmental outcomes in hypoplastic left heart syndrome. Pediatrics, 2006. 117(1): p. e90-7.
Licht, D.J., D.M. Shera, R.R. Clancy, et al., Brain maturation is delayed in infants with complex congenital heart defects. J Thorac Cardiovasc Surg, 2009. 137(3): p. 529-36; discussion 536-7.
Honjo, O. and C.A. Caldarone, Hybrid palliation for neonates with hypoplastic left heart syndrome: current strategies and outcomes. Korean Circ J, 2010. 40(3): p. 103-11.
13
14
15
16
17
18
19
20
21
22
23
24
Tweddell, J.S., G.M. Hoffman, K.A. Mussatto, et al., Improved survival of patients undergoing palliation of hypoplastic left heart syndrome: lessons learned from 115 consecutive patients. Circulation, 2002. 106(12 Suppl 1): p. I82-9.
Sano, S., K. Ishino, H. Kado, et al., Outcome of right ventricle-to-pulmonary artery shunt in first-stage palliation of hypoplastic left heart syndrome: a multi-institutional study. Ann Thorac Surg, 2004. 78(6): p. 1951-7; discussion 1957-8.
Ohye, R.G., L.A. Sleeper, L. Mahony, et al., Comparison of shunt types in the Norwood procedure for single-ventricle lesions. N Engl J Med, 2010. 362(21): p. 1980-92.
Tweddell, J.S., G.M. Hoffman, R.T. Fedderly, et al., Phenoxybenzamine improves systemic oxygen delivery after the Norwood procedure. Ann Thorac Surg, 1999. 67(1): p. 161-7; discussion 167-8.
De Oliveira, N.C., D.A. Ashburn, F. Khalid, et al., Prevention of early sudden circulatory collapse after the Norwood operation. Circulation, 2004. 110(11 Suppl 1): p. II133-8.
Hehir, D.A., T.E. Dominguez, J.A. Ballweg, et al., Risk factors for interstage death after stage 1 reconstruction of hypoplastic left heart syndrome and variants. J Thorac Cardiovasc Surg, 2008. 136(1): p. 94-9, 99 e1-3.
Gelehrter, S., C.G. Fifer, A. Armstrong, et al., Outcomes of Hypoplastic Left Heart Syndrome in Low-Birth-Weight Patients. Pediatr Cardiol, 2011.
Simsic, J.M., S.M. Bradley, M.R. Stroud, et al., Risk factors for interstage death after the Norwood procedure. Pediatr Cardiol, 2005. 26(4): p. 400-3.
Galantowicz, M. and J.P. Cheatham, Lessons learned from the development of a new hybrid strategy for the management of hypoplastic left heart syndrome. Pediatr Cardiol, 2005. 26(2): p. 190-9.
Akintuerk, H., I. Michel-Behnke, K. Valeske, et al., Stenting of the arterial duct and banding of the pulmonary arteries: basis for combined Norwood stage I and II repair in hypoplastic left heart. Circulation, 2002. 105(9): p. 1099-103.
Galli, K.K., R.A. Zimmerman, G.P. Jarvik, et al., Periventricular leukomalacia is common after neonatal cardiac surgery. J Thorac Cardiovasc Surg, 2004. 127(3): p. 692-704.
Caldarone, C.A., L. Benson, H. Holtby, et al., Initial experience with hybrid palliation for neonates with single-ventricle physiology. Ann Thorac Surg, 2007. 84(4): p. 1294-300.
1
2
3
4
5
6
7
8
9
10
11
12