Embed Size (px)
Citation preview

SCIENTIFIC ARTICLE
Comparison of a NewMultifilament Stainless Steel
Suture with Frequently Used Sutures for Flexor
Tendon Repair
Erik McDonald, BS, Joshua A. Gordon, BS, Jenni M. Buckley, PhD, Leonard Gordon, MD
Purpose To investigate the mechanical properties of some common suture materials currentlyin use and compare them with a new multifilament stainless steel suture.
Methods We investigated the mechanical properties of 3-0 and 4-0 Fiberwire, 3-0 Supramid,3-0 Ethibond, and a new 3-0 and 4-0 multifilament stainless steel suture. All suture materialwas tested in a knotted configuration and all but the Supramid was tested in an unknottedconfiguration. We measured the load, elongation at failure, and stiffness during both tests.
Results The 4-0 multifilament stainless steel showed the least elongation, whereas the 3-0multifilament stainless steel withstood the highest load of any material in both the knottedand unknotted tests. There was no difference in stiffness between the 3-0 and 4-0 multifil-ament stainless steel when untied; however, the 3-0 multifilament stainless steel was stifferwhen tied. Soaking in a saline solution had no significant effect on the ultimate load,elongation at failure, or stiffness of any of the sutures. The 3-0 Fiberwire and 3-0 Ethibondrequired at least 5 throws to resist untying.
Conclusions Multifilament stainless steel exhibited promising mechanical advantages over theother sutures tested. More research is needed to determine how this material will affect theclinical outcomes of primary flexor tendon repair.
Clinical relevance With a secure attachment to the tendon, the multifilament stainless steel’s lowerelongation and better knot-holding ability may result in a higher force to produce a 2-mm gap anda higher ultimate tensile strength in a tendon repair. (J Hand Surg 2011;36A:1028–1034.Copyright © 2011 by the American Society for Surgery of the Hand. All rights reserved.)
Key words Biomechanics, Ethibond, Fiberwire, flexor tendon, mechanical properties.
upbiug
TWO OF THE BIOMECHANICAL properties used topredict the success of a tendon repair are theultimate tensile strength and the ability to resist
gapping.1–10 The characteristics of the suture material
FromtheUCSF/SFGHOrthopaedicTraumaInstitute,andtheDepartmentofAnatomyandOrthopaedicSurgery, University of California, San Francisco; and the David Geffen School of Medicine, University ofCalifornia, Los Angeles, Los Angeles, CA.
Received for publication September 30, 2010; accepted in revised form March 22, 2011.
Funding and hardware for this study were provided by Core Essence Orthopaedics, Fort Washing-ton, PA. L.G. owns stock and receives royalties from Core Orthopaedics.
Corresponding author: Leonard Gordon, MD, Department of Anatomy and OrthopaedicSurgery, University of California, 2299 Post Street, San Francisco, CA 94115; e-mail:[email protected].
0363-5023/11/36A06-0011$36.00/0
doi:10.1016/j.jhsa.2011.03.0331028 � © ASSH � Published by Elsevier, Inc. All rights reserved.
sed for a repair have a noteworthy effect on thesearameters, and a number of new suture materials haveeen developed.11–28 Some of the characteristics of andeal suture material include nonbioreactivity, a highltimate tensile strength, and the ability to resist elon-ation, handle and tie easily, and hold knots well.
In 1929, Bunnell29 advocated the use of silk orchromatic catgut, but by 194030 he had begun to sug-gest monofilament stainless steel in a crisscross config-uration for primary flexor tendon repair. This suturewas difficult to handle and was ultimately discarded infavor of monofilament nylon and subsequently Ethi-bond (EB), a multifilament polyester (Ethicon, Somer-ville, NJ). More recently Fiberwire (FW) (Arthrex, Na-
ples, FL) has demonstrated some advantageous
MULTIFILAMENT STAINLESS STEEL SUTURE 1029
properties but has some disadvantages including a poorability to hold knots.20,27,31,32
Recently, a multifilament stainless steel (MFSS) su-ture was developed for use in flexor tendon repair.Whereas the use of stainless steel as suture material is
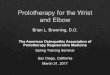
FIGURE 1: A Side view of the 3-0 MFSS suture (magnificationfilaments used in the MFSS suture material.
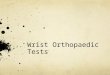
FIGURE 2: Test setup showing the load cell and sutureclamps.
not a new idea, the configuration of the stainless steel
JHS �Vol A,
filaments in this design produces a suture that is easierto handle than the monofilament designs.30,33 The me-chanical properties of MFSS may be advantageous inproducing strong repairs with secure knots.
The purposes of this study were to investigate themechanical properties of some common suture materi-als currently in use and to compare them with a newMFSS suture.
MATERIALS AND METHODS
Suture material physical properties
We investigated the mechanical properties of the fol-lowing 4 suture materials: FW, a multifilament, ultra-high-molecular-weight polyethylene core with abraided polyester jacket; Supramid (SM), a multifila-ment nylon core with a nylon jacket (S. Jackson, Inc.,Alexandria, VA); EB, a multifilament polyester su-ture; and an MFSS suture (Core Essence Orthopae-dics, Fort Washington, PA). The SM and EB weretested in the 3-0 size, whereas the FW and MFSSwere tested in 3-0 and 4-0 configurations.
The MFSS cable is composed of 49 filaments of316L stainless steel. The filaments in the 3-0 size are0.034 mm in diameter, with a total suture diameter of0.31 mm. The 4-0 filaments are 0.024 mm in diameterand the total suture diameter is 0.21 mm. The suture isarranged in 7 bundles of 7 filaments each; althoughtechnically a cable, it functions as a suture (Fig. 1).
Untied suture testing
We evaluated the ultimate tensile strength of 5 different
.3). B Diagram showing the configuration of the 7 bundles of 7
�6suture materials: 3-0 and 4-0 MFSS, 3-0 and 4-0 FW,
June

thro
1030 MULTIFILAMENT STAINLESS STEEL SUTURE
and 3-0 EB. The SM suture was only available as a loopof suture with a needle attached. When the suture wasremoved from the needle, the length of remaining su-ture was insufficient to be attached to the testingclamps. We therefore tested the SM suture only in thetied configuration.
A total of 25 strands were tested, 5 of each material.To test the ultimate tensile strength and elongation ofthe sutures, each suture was loaded in uniaxial tensionat 1 mm/s using a servohydraulic testing machine (MTSMini-Bionix 858; Eden Prairie, MN) until failure. Astrand of suture was attached to the MTS by a set ofclamps (Fig. 2). The suture was wrapped around eachspool 3 times and then held securely with a clamp oneach side. Wrapping the suture around the spools en-sured that the load was applied to the center of thesuture, which had a length of 3 cm between spools. A5-N preload was applied and the suture was subjected to10 cycles from 5 to 10 N to allow the suture to settle andeliminate any slack from the system. A load cell(INTERFACE SSM-500, Scottsdale, AZ) recordedforce data and the MTS displacement transducer re-corded displacement. The ultimate load, elongation atfailure, and stiffness were measured for each specimen.Stiffness represents the force per unit displacement andwas calculated as the slope of a best fit line from 15 to
FIGURE 3: A Representative knot showing 3 total
30 N on the force versus displacement curve.
JHS �Vol A,
Knotted suture testing
To test the strength of the suture in a knotted configu-ration, we tied the suture around a 7.6-cm-diametercylinder to ensure consistent lengths using a surgeon’sknot with 1 additional throw, for a total of 3 throws (2� 1 � 1) (Fig. 3). In addition, we tested 3-0 FW and3-0 EB with a surgeon’s knot with 3 additional throws,for a total of 5 throws (2 � 1 � 1 � 1 � 1) (Fig. 3).The 3-0 SM was tied after cutting the suture loopoff of the needle. The loop of suture was placedaround the 2 spools for testing. The suture loopswere cyclically loaded 10 times from 5 to 10 N,then immediately tested to failure at 1 mm/s. Aswith the untied suture, this cyclic preloading al-lowed the suture to settle and removed any slackfrom the system. We tested 6 samples of eachmaterial and configuration.
We also tested 6 samples of each suture after soakingthem in a physiological saline solution at room temper-ature for 10 minutes. The ultimate load and elongationat failure were measured for each specimen. Stiffnesswas calculated for specimens in which the suture failedby breakage, and not calculated for specimens thatfailed by untying. As with the untied suture, the stiff-ness was calculated as the slope of a best fit line from 15
ws. B Representative knot showing 5 total throws.
to 30 N on the force versus displacement curve.
June

MULTIFILAMENT STAINLESS STEEL SUTURE 1031
Statistical analysis
To determine which factors significantly affect the me-chanical behavior during bench-top testing, stepwiselinear regression was conducted with the followinginitial predictor variables: (1) suture material, (2) suturegauge, (3) number of knots (knotted only), and (4)wet/dry suture material. We ran the stepwise algorithmwith p � .10 as the exclusion criteria. Pairwise com-parisons were then made between suture constructsusing Student’s t-test with Tukey’s posthoc adjustmentfor multiple comparisons. We set p � .05 as the cutofffor significance; only statistically significant findingsare reported in the Results section unless otherwisenoted.
RESULTS
Suture only
The ultimate load of the 3-0 MFSS was the highest ofany suture material tested (Table 1). The ultimate loadof the 4-0 MFSS was not statistically different from the3-0 or 4-0 FW. The EB had the lowest ultimate tensile
TABLE 1. Ultimate Load, Elongation at Failure, an
Suture Material SizeUltimate Load (N)
(mean � SD)
MFSS 3-0 73.8 � 0.7
FW 3-0 41.9 � 3.3
MFSS 4-0 39.9 � 1.3
FW 4-0 36.6 � 2
EB 3-0 27.3 � 2.4
Elongation at Failure (mm)(mean � SD)
EB 3-0 13.8 � 1.7
FW 4-0 11.9 � 1.1
FW 3-0 11.6 � 0.3
MFSS 3-0 5 � 0.8
MFSS 4-0 2.3 � 0.9
Stiffness (N/mm)(mean � SD)
MFSS 3-0 18.5 � 2.8
MFSS 4-0 16.8 � 1.5
FW 3-0 3.4 � 0.2
FW 4-0 2.8 � 0.1
EB 3-0 1.6 � 0.1
*Rows not connected by the same letter are statistically different (p �
strength.
JHS �Vol A,
The elongation at failure was highest for EB, whichwas statistically greater than any other suture (Table 1).The 3-0 and 4-0 FW had equivalent elongations atfailure. The 4-0 MFSS had the least elongation at fail-ure. The 3-0 MFSS had an elongation that was statis-tically greater than the 4-0 MFSS but less than any othersuture material tested.
There was no difference in stiffness between the 3-0and 4-0 MFSS (p � .05); however, both were greaterthan all other suture materials tested (p � .05) (Table1).
Knotted suture
When tied, the 3-0 MFSS withstood 121 N beforerupture (Table 2). When tied with 5 throws, the 3-0 FWsustained 53 N before failure, which was not statisti-cally different from the 4-0 MFSS. The double-strandedSM was also not statistically different from the 3-0 FWwith 5 knots.
The 4-0 MFSS had the least elongation of any ma-terial tested; however, it was not different from the 3-0
iffness Results for Unknotted Suture
LowerConfidence
Interval
Upper95% Confidence
Interval *
72.5 75.0 A
40.1 43.6 B
38.2 41.7 B C
34.9 38.4 C
25.5 29.1 D
12.9 14.7 A
10.9 12.8 B
10.7 12.6 B
4.4 5.7 C
1.4 3.3 D
17.4 19.7 A
15.2 18.4 A
1.8 5.0 B
1.1 4.4 B
0.0 3.2 B
. N � 5 for all groups.
d St
95%
.05)
MFSS. When tied with 5 throws, the 3-0 FW failed at
June

1032 MULTIFILAMENT STAINLESS STEEL SUTURE
an elongation greater than those with only 3 throws;however, the ultimate load was also greater. The dou-ble-stranded SM showed the most elongation.
The 3-0 MFSS was the stiffest material, followed by4-0 MFSS and 3-0 FW with 5 throws. The 3-0 EB andSM were the least stiff of the materials tested.
Both the 3-0 and 4-0 MFSS failed exclusively bybreakage at the knot with only 3 throws. With only 3throws, the 3-0 and 4-0 FW and 3-0 EB typically untiedinstead of breaking. When tied with 5 throws, the 3-0FW and EB broke at the knot instead of untying. TheSM broke at the knot.
DISCUSSIONThe results of this study indicate MFSS has some fa-
TABLE 2. Ultimate Load, Elongation at Failure, an
Suture Material Size ThrowsUltimate Load (N)
(mean � SD)
MFSS 3-0 3 121 � 3.2
FW 3-0 5 53 � 15.8
MFSS 4-0 3 49.6 � 9.3
EB 3-0 5 41.3 � 3.4
EB 3-0 3 32.5 � 12
SM 3-0 3 30.1 � 8.1
FW 3-0 3 23 � 6.3
FW 4-0 3 18.4 � 3
Elongation at Failure (mm(mean � SD)
MFSS 4-0 3 2.6 � 1.6
MFSS 3-0 3 2.8 � 0.3
FW 4-0 3 4.2 � 0.7
FW 3-0 3 4.3 � 0.9
FW 3-0 5 6.6 � 1.6
EB 3-0 3 10.7 � 3.2
EB 3-0 5 11 � 1
SM 3-0 3 16.6 � 3.7
Stiffness (N/mm)(mean � SD)
MFSS 3-0 3 47.1 � 6.9
MFSS 4-0 3 31.4 � 3.8
FW 3-0 5 8.7 � 0.8
EB 3-0 5 2.9 � 0.2
SM 3-0 3 1.8 � 0.1
*Rows not connected by the same letter are statistically different (p �
vorable mechanical properties compared with several
JHS �Vol A,
suture materials currently in clinical use. The elongationof the MFSS was significantly lower than any of theother suture materials, and the stiffness was signifi-cantly higher. When tied, the MFSS only required 3throws to resist untying, whereas Fiberwire needed 5throws. We are not the first investigators to concludethat Fiberwire has the potential for untying at lowloads.20,27,31,32 A metallic suture material may offerbenefits of nonviscoelastic properties. Polymer sutureshave been shown to exhibit stress relaxation and creep,unlike stainless steel, which does not have these prop-erties.34 In addition, stainless steel may offer otherbenefits, such as being secured by a means other than aknot—for example, crimping.
We are also not the first study to investigate stainless
iffness Results for Knotted Suture
Lower95% Confidence
Interval
Upper95% Confidence
Interval *
115.2 126.8 A
47.7 58.3 B
44.3 54.9 B C
36.0 46.6 C D
27.3 37.8 D E
24.3 35.9 D E
17.7 28.3 E
10.9 25.8 E
1.4 3.8 A
1.6 4.1 A
2.5 5.8 A B
3.1 5.4 A B
5.5 7.8 B
8.9 11.2 C
9.8 12.2 C
15.3 17.9 D
44.9 49.3 A
29.4 33.5 B
6.7 10.9 C
0.9 4.9 D
–0.6 4.1 D
. N � 12 for all groups.
d St
)
.05)
steel for use in primary flexor tendon repair. Trail et al33
June

MULTIFILAMENT STAINLESS STEEL SUTURE 1033
in 1989 investigated multiple suture materials andfound that whereas MFSS offered many advantagesover the polymer-based sutures they tested, the authorsultimately did not recommend it based on its handlingcharacteristics. This has been a consistent problem withMFSS. Although we did not directly address the han-dling properties in this study, we noted that the MFSSdoes not have the memory that makes monofilament sodifficult to work with and tie. The configuration of theindividual filaments creates an overall construct thatdoes not plastically deform or kink when handled. Thisdesign creates a suture that has completely differenthandling characteristics from monofilament designsused in the past.
In 2005, Lawrence and Davis21 compared a braidedstainless steel suture with 4 other materials includingFW. They concluded that FW and stainless steel werethe most biomechanically suitable when performingflexor tendon repairs. Their study was limited in that theauthors only investigated 4-0 suture and only in the tiedconfiguration, but their study supports the hypothesisthat an MFSS suture could be a viable option for flexortendon repair.
Additional research is necessary to determine howthis particular MFSS suture will perform in vivo. Futurestudies should investigate how the ultimate load andgapping of a tendon repair is affected by the MFSS, aswell as the ability of this construct to pass unimpededthrough the tendon pulley system. Greater stiffness isgenerally regarded as an advantage to limit gapping.Nevertheless, studies should be conducted to determinewhether the increased stiffness of the MFSS wouldshield the tendon from tensile forces during healing atthe risk of causing tenomalacia.
Although we did not perform a formal power anal-ysis, we determined the sample sizes based on numbersused by previous investigators. This is a limitation ofthe study. Our final data sets were 5 samples per groupfor the suture only and 12 samples per group for theknotted suture. The straight suture sample sizes are thesame as those of Lawerence and Davis,21 who used 5samples per group when investigating tied suture,which one would expect to have greater variability. Forour tied comparisions, we used 12 samples per group.Again, our outcomes were similar to those of Lawrenceand Davis, who tested FW, MFSS, and EB, amongother materials. Some of our comparisons did not reachsignificance but we did observe some trends. One ex-ample is the lack of significant differences in elongationat failure between the MFSS and FW when tied. How-ever, in cases like these, one should also consider the
mode of failure. The mode of failure for the MFSS wasJHS �Vol A,
the suture breaking at the knot, whereas the FW failedby untying.
With a secure attachment to the tendon, the lowerelongation and better knot-holding ability of the MFSSmay result in higher force to produce a 2-mm gap andhigher ultimate tensile strength in tendon repair. Moreresearch is needed to determine how this material willaffect actual clinical outcomes of primary flexor tendonrepair.
REFERENCES1. Amadio PC. Friction of the gliding surface. Implications for tendon
surgery and rehabilitation. J Hand Ther 2005;18:112–119.2. Barrie KA, Tomak SL, Cholewicki J, Wolfe SW. The role of
multiple strands and locking sutures on gap formation of flexortendon repairs during cyclical loading. J Hand Surg 2000;25A:714–720.
3. Bhatia D, Tanner KE, Bonfield W, Citron ND. Factors affecting thestrength of flexor tendon repair. J Hand Surg 1992;17B:550–552.
4. Momose T, Amadio PC, Zhao C, Zobitz ME, An KN. The effect ofknot location, suture material, and suture size on the gliding resis-tance of flexor tendons. J Biomed Mater Res 2000;53:806–811.
5. Moriya T, Zhao C, An KN, Amadio PC. The effect of epitendinoussuture technique on gliding resistance during cyclic motion afterflexor tendon repair: a cadaveric study. J Hand Surg 2010;35A:552–558.
6. Tang JB, Wang B, Chen F, Pan CZ, Xie RG. Biomechanical eval-uation of flexor tendon repair techniques. Clin Orthop Relat Res2001;38:252–259.
7. Walbeehm ET, De Wit T, Hovius SE, McGrouther DA. Influence ofcore suture geometry on tendon deformation and gap formation inporcine flexor tendons. J Hand Surg 2009;34B:190–195.
8. Winters SC, Gelberman RH, Woo SL, Chan SS, Grewal R, Seiler JGIII. The effects of multiple-strand suture methods on the strength andexcursion of repaired intrasynovial flexor tendons: a biomechanicalstudy in dogs. J Hand Surg 1998;23A:97–104.
9. Zhao C, Amadio PC, Momose T, Couvreur P, Zobitz ME, An KN.The effect of suture technique on adhesion formation after flexortendon repair for partial lacerations in a canine model. J Trauma2001;51:917–921.
10. Zhao C, Amadio PC, Tanaka T, Kutsumi K, Tsubone T, Zobitz ME,et al. Effect of gap size on gliding resistance after flexor tendonrepair. J Bone Joint Surg 2004;86A:2482–2488.
11. Aoki M, Manske PR, Pruitt DL, Kubota H, Larson BJ. Caninecadaveric study of flexor tendon repair using tendon splint: tensilestrength and the work of flexion. Nippon Seikeigeka Gakkai Zasshi1995;69:332–341.
12. Aoki M, Manske PR, Pruitt DL, Larson BJ. Tendon repair usingflexor tendon splints: an experimental study. J Hand Surg 1994;19A:984–990.
13. Barrie KA, Tomak SL, Cholewicki J, Merrell GA, Wolfe SW. Effectof suture locking and suture caliber on fatigue strength of flexortendon repairs. J Hand Surg 2001;26A:340–346.
14. Barrie KA, Wolfe SW, Shean C, Shenbagamurthi D, Slade JF III,Panjabi MM. A biomechanical comparison of multistrand flexortendon repairs using an in situ testing model. J Hand Surg 2000;25A:499–506.
15. Gill RS, Lim BH, Shatford RA, Toth E, Voor MJ, Tsai TM. Acomparative analysis of the six-strand double-loop flexor tendonrepair and three other techniques: a human cadaveric study. J HandSurg 1999;24A:1315–1322.
16. Gordon L, Tolar M, Rao KT, Ritchie RO, Rabinowitz S, Lamb RP.Flexor tendon repair using a stainless steel internal anchor. Biome-chanical study on human cadaver tendons. J Hand Surg 1998;
23B:37–40.June

1034 MULTIFILAMENT STAINLESS STEEL SUTURE
17. Greenwald D, Shumway S, Albear P, Gottlieb L. Mechanical com-parison of 10 suture materials before and after in vivo incubation.J Surg Res 1994;56:372–377.
18. Karjalainen T, Goransson H, Viinikainen A, Jamsa T, Ryhanen J.Nickel-titanium wire as a flexor tendon suture material: an ex vivostudy. J Hand Surg 2010;35B:469–474.
19. Kim JC, Lee YK, Lim BS, Rhee SH, Yang HC. Comparison oftensile and knot security properties of surgical sutures. J Mater SciMater Med 2007;18:2363–2369.
20. Komatsu F, Mori R, Uchio Y. Optimum surgical suture material andmethods to obtain high tensile strength at knots: problems of con-ventional knots and the reinforcement effect of adhesive agent.J Orthop Sci 2006;11:70–74.
21. Lawrence TM, Davis TR. A biomechanical analysis of suture ma-terials and their influence on a four-strand flexor tendon repair.J Hand Surg 2005;30A:836–841.
22. Scherman P, Haddad R, Scougall P, Walsh WR. Cross-sectional areaand strength differences of Fiberwire, Prolene, and Ticron sutures.J Hand Surg 2010;35A:780–784.
23. Su BW, Protopsaltis TS, Koff MF, Chang KP, Strauch RJ, Crow SA,et al. The biomechanical analysis of a tendon fixation device forflexor tendon repair. J Hand Surg 2005;30A:237–245.
24. Vigler M, Palti R, Goldstein R, Patel VP, Nasser P, Lee SK.Biomechanical study of cross-locked cruciate versus Stricklandflexor tendon repair. J Hand Surg 2008;33A:1821833.
25. Viinikainen A, Goransson H, Huovinen K, Kellomaki M, Tormala P,Rokkanen P. Material and knot properties of braided polyester (Ti-cron) and bioabsorbable poly-L/D-lactide (PLDLA) 96/4 sutures. J
Mater Sci Mater Med 2006;17:169–177.JHS �Vol A,
26. Wada A, Kubota H, Hatanaka H, Miura H, Iwamoto Y. Comparisonof mechanical properties of polyvinylidene fluoride and polypropyl-ene monofilament sutures used for flexor tendon repair. J Hand Surg2001;26B:212–216.
27. Waitayawinyu T, Martineau PA, Luria S, Hanel DP, Trumble TE.Comparative biomechanic study of flexor tendon repair using Fiber-Wire. J Hand Surg 2008;33A:701–708.
28. Wolfe SW, Willis AA, Campbell D, Clabeaux J, Wright TM. Biome-chanic comparison of the Teno Fix tendon repair device with thecruciate and modified Kessler techniques. J Hand Surg 2007;32A:356–366.
29. Bunnell S. Treatment of Injuries of the Hand. Cal West Med 1929;30:1–5.
30. Bunnell S. Primary repair of severed tendons: the use of stainlesssteel wire. Am J Surg 1940;47:502–516.
31. Ilahi OA, Younas SA, Ho DM, Noble PC. Security of knots tied withethibond, fiberwire, orthocord, or ultrabraid. Am J Sports Med2008;36:2407–2414.
32. Wust DM, Meyer DC, Favre P, Gerber C. Mechanical and handlingproperties of braided polyblend polyethylene sutures in comparisonto braided polyester and monofilament polydioxanone sutures. Ar-throscopy 2006;22:1146–1153.
33. Trail IA, Powell ES, Noble J. An evaluation of suture materials usedin tendon surgery. J Hand Surg 1989;14B:422–427.
34. Vizesi F, Jones C, Lotz N, Gianoutsos M, Walsh WR. Stress relax-ation and creep: viscoelastic properties of common suture materialsused for flexor tendon repair. J Hand Surg 2008;33A:241–
246.June