Embed Size (px)
DESCRIPTION
odontologiaevaluacion de desensibilizantes mediante el barrido electronico
Citation preview
Comparative evaluation of the effectiveness of desensitizingagents in dentine tubule occlusion using scanning electronmicroscopy
CL Chen,* A Parolia,* A Pau,* IC Celerino de Moraes Porto†
*School of Dentistry, International Medical University, Bukit Jalil, Kuala Lumpur, Malaysia.†Department of Restorative Dentistry, Federal University of Alagoas, Macei�o, Alagoas, Brazil.
ABSTRACT
Background: Dentine hypersensitivity (DH) occurs on exposed dentine and is dependent on the patency of dentinaltubules. This study compared the effectiveness of red propolis extract (RPE), calcium sodium phosphosilicate (Novamin)and arginine-calcium carbonate (ACC) in occluding dentine tubules.Methods: Eighty dentine discs from extracted human molars were randomly divided into four groups (n = 20): Group 1– RPE; Group 2 – Novamin; Group 3 – ACC; Group 4 – saline. The discs were etched with 37.5% phosphoric acid andtreated with the test agents. Ten treated discs from each group were then exposed to 6% citric acid challenge. The extentof tubule occlusion was assessed using scanning electron microscopy (SEM). Three blinded assessors scored each SEMimage on the degree of tubule occlusion. Differences in occlusion were tested using ANOVA and Tukey adjustment.Results: Discs treated with ACC demonstrated more tubule occlusion, followed by RPE and Novamin, and were greaterin statistical significance when compared to discs treated with saline. Following acid challenge, RPE treated discs main-tained more occlusion, followed by ACC and Novamin.Conclusions: All three agents demonstrated tubule occlusion. Although ACC showed more occlusion following treat-ment, RPE demonstrated a higher degree of occlusion following acid challenge.
Keywords: Arginine-calcium carbonate, calcium sodium phosphosilicate, dentine hypersensitivity, red propolis extract, scanningelectron microscopy.
Abbreviations and acronyms: ACC = arginine-calcium carbonate; DH = dentine hypersensitivity; PBS = phosphate buffered saline;SEM = scanning electron microscopy; RP = red propolis; RPE = red propolis extract.
(Accepted for publication 14 May 2014.)
INTRODUCTION
Dentine hypersensitivity (DH) is characterized byshort sharp pain arising from exposed dentine inresponse to stimuli typically thermal, evaporative,tactile, osmotic or chemical and which cannot beascribed to any other form of dental defect or pathol-ogy.1 DH is a common occurrence and is often oneof the main reasons why patients seek dental treat-ment. The reported prevalence of DH varies from4% to 57%.2,3 The discomfort of DH experiencedby the patients is highly subjective and can vary sub-stantially between individuals. For some patients, thediscomfort is perceived as a low grade pain, of slightconcern, but for others the discomfort may presentas a disturbing, severe pain which can affect theirquality of life.4 To avert stimulation of the hypersen-sitive areas, patients tend to avoid certain food and
drinks in their diet and avoid cleaning their teeth.Inability to maintain adequate plaque control maylead to increased risk of caries development and peri-odontal problems. Therefore, effective and long-last-ing treatment is of great interest to both patients anddental professionals. Three major mechanisms of den-tinal sensitivity have been proposed in the literature:neural theory, odontoblastic transduction theory andhydrodynamic theory. The most widely acceptedtheory is the hydrodynamic theory proposed byBr€annstr€om, who suggested that exposed dentinewith patent tubules allows the movement of tubulefluid which leads to dentine sensitivity.5 Scanningelectron microscopy (SEM) has shown that tubules inclinically characterized ‘sensitive’ exfoliated teeth areeight times more numerous, two times wider indiameter and more penetrable, whereas tubules in‘non-sensitive’ teeth are fewer, smaller and usually
© 2015 Australian Dental Association 65
Australian Dental Journal 2015; 60: 65–72
doi: 10.1111/adj.12275
Australian Dental JournalThe official journal of the Australian Dental Association

blocked.6 This suggests that agents which have theability to occlude patent dentinal tubules and/or areadhesive to dentine surfaces and hence achieve sur-face coverage and seal most tubules, would be idealto relieve DH. There has been a significant advance-ment in understanding DH, and various agents andtherapies have been developed to combat the prob-lem.7 However, none of the treatment regimens havebeen completely efficient in treating DH. Therefore,the continued development of new desensitizingagents is required.8 Recently, calcium sodium phos-phosilicate (Novamin) has been found to be veryeffective for occluding dentinal tubules. When intro-duced into the oral environment, Novamin releasessodium, calcium and phosphate ions, which theninteract with saliva and result in the deposition of acrystalline hydroxycarbonate apatite layer over theexposed dentine and within the dentinal tubules.9–12
Continued efforts have recently resulted in a noveltechnology that uses 8% arginine-calcium carbonate(ACC) for treating DH, which has shown instant andlasting relief of DH.13 It is unique in that two of itskey components, arginine and calcium, are foundnaturally in saliva, and that the arginine and calciumcarbonate work together to accelerate the naturalmechanisms of occlusion to deposit a dentine-likemineral, containing calcium and phosphate, withinthe dentinal tubules and in a protective layer on thedentine surface.14 Propolis is a natural resinous sub-stance collected from plant buds or exudates by Apismellifera bees. The composition of propolis variesaccording to its botanical origin. Generally it con-tains a mixture of resin, essential oils, wax mixedwith bee glue (the salivary secretions of bees), aminoacids, minerals, ethanol (alcohol), vitamins A, B com-plex, E, zinc, pollen and the highly active biochemi-cal substance known as bioflavonoids. Bioflavonoidsare well known plant compounds which have anti-bacterial, antifungal, antiviral, antioxidant and anti-inflammatory proprieties.15,16 Brazilian propolis isclassified into 12 types according to their physio-chemical characteristics and related to geographiclocations.16 Red propolis (RP) is a newly classified13th type. The RP variety is obtained in north-eastBrazil. Bees collect reddish exudates from Dalbergiaecastophyllum (L) Taub (Leguminosae) to make redpropolis.17,18 RP has been reported to have a highconcentration of phenolic acids and flavonoids whichhave been associated with a variety of health bene-fits.19,20 Propolis has been used in the treatment ofDH and found to be effective.21–25 However, nostudy has compared the effect of red propolis extract(RPE) with other desensitizing agents in relievingDH. The objective of this experimental study wasto evaluate and compare the effectiveness of RPE,Novamin and ACC in occluding dentinal tubules.
MATERIALS AND METHODS
Sample preparation
Eighty dentine discs were prepared from extractedhuman permanent molars. The crown was sectionedwith a diamond saw (IsoMet® 1000 Percision Saw;Buehler, Lake Bluff, IL, USA), perpendicular to thelong axis of the tooth, to create dentine discs with athickness of 1.0 � 0.1 mm from the mid coronal den-tine. The occlusal enamel was removed from eachtooth, exposing the middle dentine. The disc surfacewas free of enamel and pulp horns. The dentine discswere polished using 600 grit silicon carbide paper(CarbiMetTM, Buehler, Lake Bluff, IL, USA) to createan even and uniform surface. The polished sampleswere then placed in a jar of distilled water and soni-cated for 10 minutes to remove the polishing abrasive.After sonication, the samples were rinsed with saline.The dentinal tubules were opened by etching the den-tine discs in a Petri dish with 37.5% phosphoric acid(Gel Etchant; Kerr Corp., Orange, CA, USA) for30 seconds. After etching, the samples were rinsedwith distilled water, then placed in a jar of distilledwater and finally sonicated once again for five min-utes. The etched and sonicated samples were stored inphosphate buffered saline (PBS, pH = 7) for subse-quent SEM analysis without coating.
Experimental design
The dentine discs were randomly divided into fourgroups, each containing 20 discs: Group 1 – 10% redpropolis extract (Apic Flora, Maceio, Alagoas, Brazil);Group 2 – paste containing Novamin (NUPRO® Sens-odyne®, Dentsply Corp., Smile Way York, PA, USA);Group 3 – paste containing arginine-calcium carbon-ate (Colgate® Sensitive Pro-ReliefTM, Colgate OralPharmaceuticals Inc., New York, NY, USA); andGroup 4 – saline (negative control).
Treatment of samples
Double-sided tape was used to fasten the samplesonto microscope slides with the polished side facingup. Group 1 samples were wetted with PBS bufferand then the test product (RPE) was applied onto thedentine surface using a rubber cup in slow speedhandpiece (GENTLE power LUX 20LP, KaVo DentalCorp., Fruehauf Drive, Charlotte NC, USA). At lowspeed, the test product was gently applied onto thesurface for one minute. For samples in Groups 2 and3, test products were applied according to the manu-facturers’ instructions (in-office treatment). The sam-ples were left undisturbed for five minutes at roomtemperature. Thereafter, the samples were immersed
66 © 2015 Australian Dental Association
CL Chen et al.

in a jar of PBS for five minutes while stirring. Thesamples were then gently rinsed with distilled waterto ensure removal of any excess product from the sur-faces. This treatment was repeated three times. Tenspecimens were randomly selected from each group tobe coated with a layer of gold/palladium using a minisputter coater (Emitech SC7620, Quorum Technolo-gies Ltd, Lewes, East Sussex, UK) for subsequentSEM analysis.
Acid challenge
The remaining 10 treated samples from each groupwere immersed in 6% citric acid (pH 2) in a Petri dishfor one minute, followed by rinsing in saline for twominutes. The samples were coated with a layer ofgold/palladium for subsequent SEM analysis.
Evaluation of occlusion
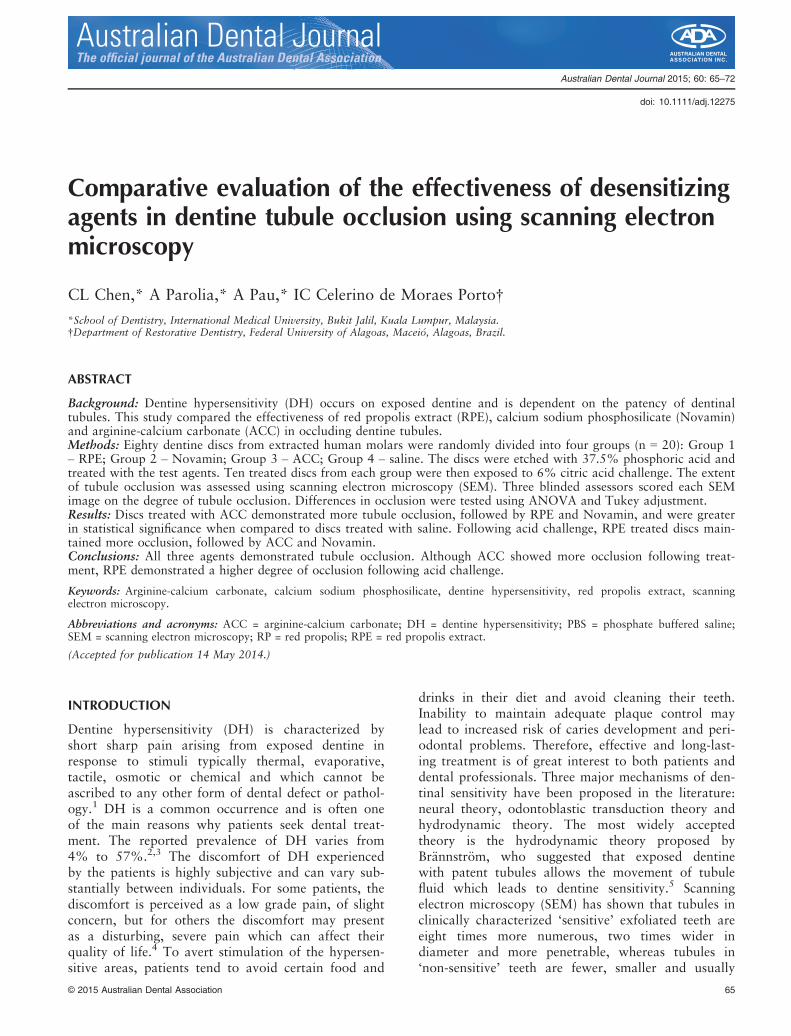
The extent of dentinal tubule occlusion was assessedusing SEM (TM3000 Tabletop Microscope, Hitachi,Tokyo, Japan). Dentine samples were coated to aidconductivity. The samples were examined at an oper-ating voltage of 5 kV in Shadow 2 image mode. TheSEM micrographs were obtained at a magnificationof 2000X. Dentine samples were examined after eachof the following situations: (1) after etching withphosphoric acid – to ensure that the dentinal tubulesare in an open unoccluded state; (2) after applicationof test agent – to determine the effect of the testagents on dentinal tubule occlusion; (3) after acidchallenge – to determine the susceptibility of thetreatment to acid challenge. SEM visual assessmentmay present a concern of subjectivity. To minimizethe subjectivity, four representative images of eachtreated dentine surface of each specimen were cap-tured. The images were then assessed independentlyby three well trained blinded reviewers to score thelevel of tubule occlusion (on a categorical scale of 1–5), in accordance with the tubule occlusion classifica-tion scoring system:26,27 (1) occluded (100% oftubules occluded); (2) mostly occluded (50–<100% oftubules occluded); (3) partially occluded (25–<50%of tubules occluded); (4) mostly unoccluded (<25%of tubules occluded); (5) unoccluded (0%, no tubuleocclusion).The mean score of tubule occlusion by the three
blinded reviewers was taken and used for analysis.Figure 1 summarizes the experimental design.
Statistical methods
The primary objective was to evaluate and comparethe effectiveness between the desensitizing agents inoccluding dentinal tubules. Data were entered into
SPSS 17.0 (SPSS Inc., Chicago, IL, USA). The mean oftubule occlusion score was analysed using ANOVA.All pair-wise treatment comparisons were performedwith a Tukey adjustment for multiplicity; treatmentdifferences and p-values were presented. The signifi-cant level was set at p < 0.05.
RESULTS
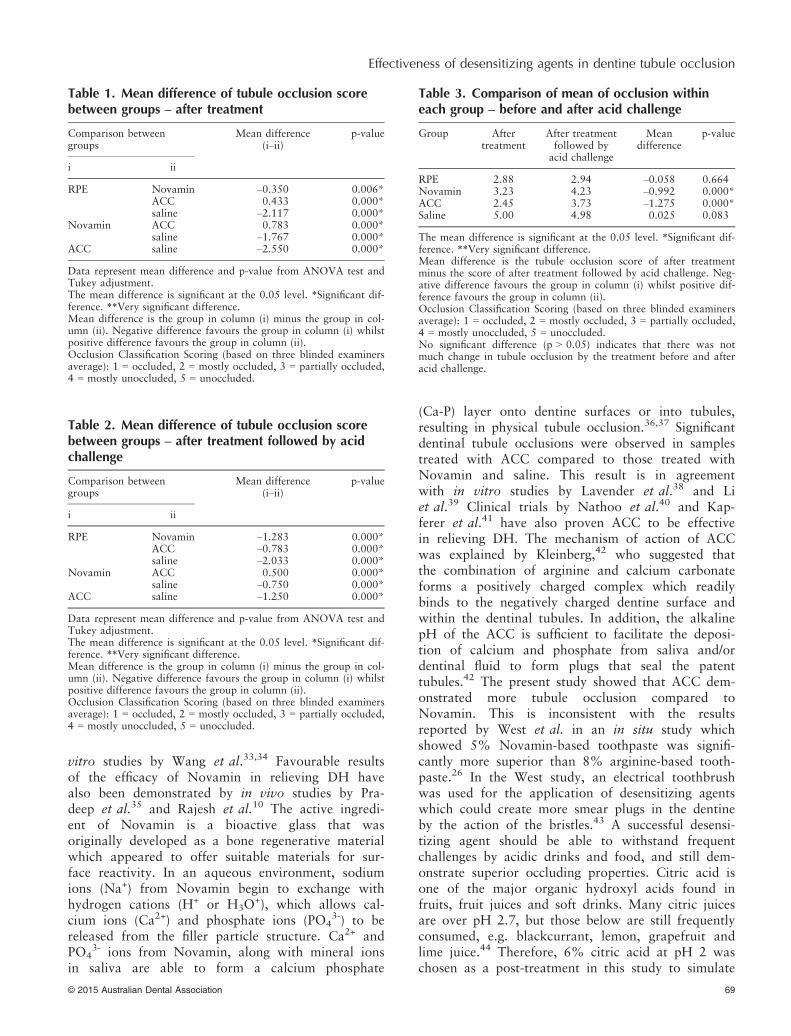
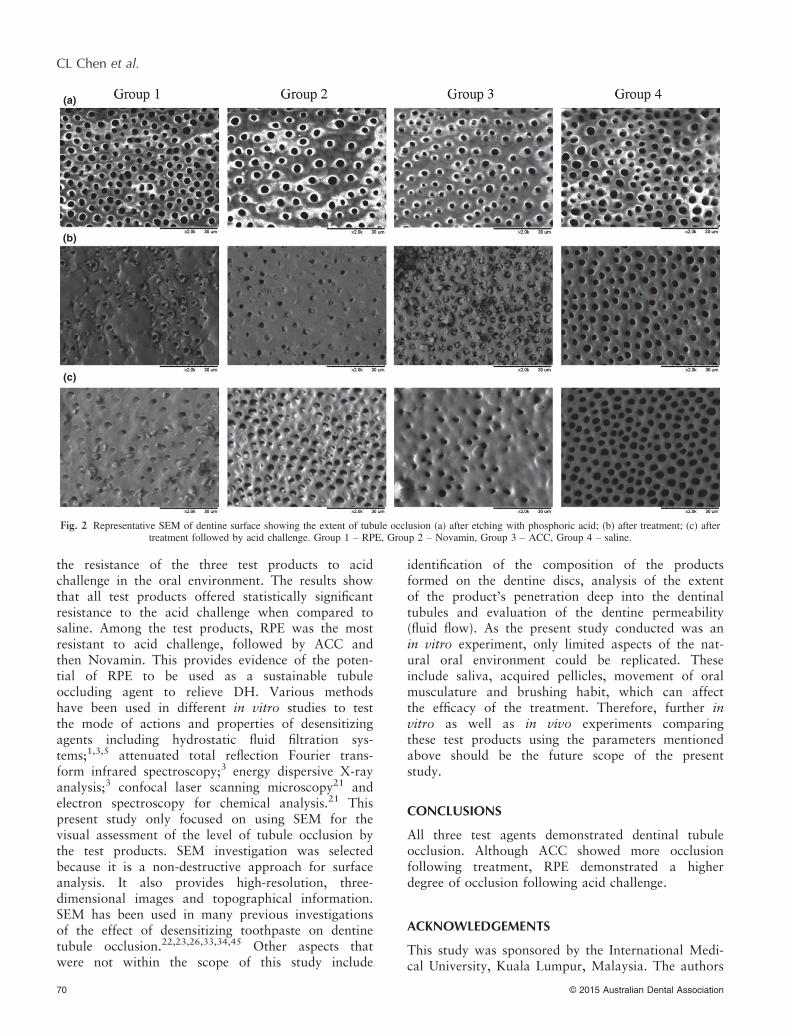
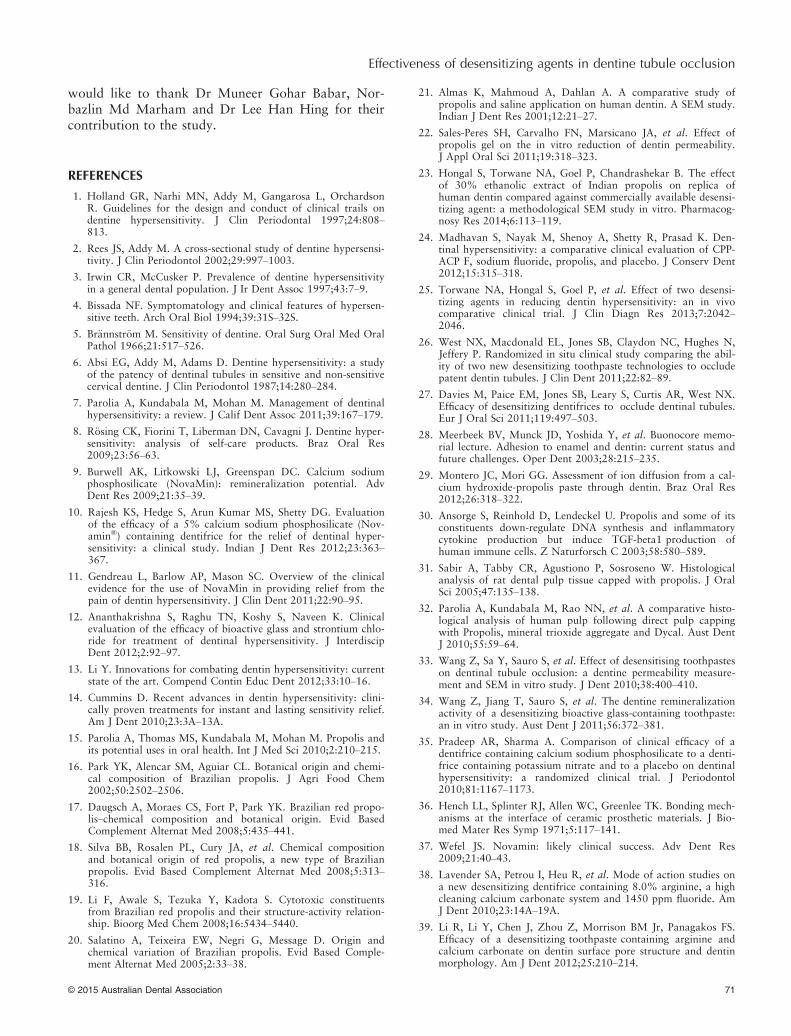
Treatment with test products from all groupsshowed statistically significant differences from eachother. All three test agents presented significantlysuperior tubule occlusion and acid resistance whencompared to saline (Tables 1 and 2). Samples thatwere treated with ACC demonstrated significantlymore tubule occlusion when compared to RPE(p = 0.001) and Novamin (p = 0.001) (Table 1).After treatment with acid challenge, RPE showedsignificantly more resistance to acid challenge whencompared to ACC (p = 0.001) and Novamin(p = 0.001) (Table 2). Post-treatment with acid chal-lenge resulted in more openings of dentinal tubulesof the treated samples from all groups (Table 3).However, only RPE showed no statistically signifi-cant difference between the tubule occlusion beforeand after acid challenge (p = 0.664). In contrast, sig-nificant differences were observed within the groupof Novamin (p = 0.001) and ACC (p = 0.001). TheSEM micrographs of etched dentine surface by phos-phoric acid demonstrated fully patent dentinaltubules (Fig 2a). Examination of dentine surfacetreated with RPE showed dentine surface coverageand peritubules particle depositions by the product(Fig 2b, Group 1). After treatment with Novamin,some tubules remained completely occluded whilstsome remained open (Fig 2b, Group 2). All thetubules of the samples treated with ACC wereoccluded by crystal-like depositions (Fig 2b,Group 3). After acid challenge, tubules observed inthe samples treated with RPE remained mostlyoccluded (Fig 2c, Group 1). In contrast, more open-ings of tubules were observed in the samples treatedwith Novamin and ACC (Fig 2c, Group 2 and 3).The tubules of samples treated with saline remainedcompletely open after treatment as well as after acidchallenge (Fig 2b and c, Group 4).
DISCUSSION
Saliva naturally occludes patent dentinal tubules bytransporting calcium and phosphate ions into thetubules to induce tubule plugging and by forming asurface protective layer of salivary glycoproteinwith calcium and phosphate.14 However, this pro-cess of natural tubule occlusion is very slow andthe tubule plugging is easily removed by dietary
© 2015 Australian Dental Association 67
Effectiveness of desensitizing agents in dentine tubule occlusion
acid and physical insult, thus rendering it neithereffective nor reliable in providing lasting relief ofDH. Therefore, successful treatment regimens whichcan provide rapid, long-lasting tubule occlusion andresistance to the challenges in the oral environmentare needed. Results from the present study showthat RPE was significantly effective in dentinaltubule occlusion in comparison to saline. This is inagreement with in vitro studies by Almas et al.21
and Sales-Peres et al.22 Propolis has also recentlybeen proven to be clinically effective in reducingDH.24,25 This may be attributed to the interactionbetween the high content of flavonoids in RPE andthe dentine, forming crystals that are able to adhereto the dentine surface and occlude the dentinaltubules.22 Other possible factors could be the pres-ence of natural resinous substances in propolis thatshow a bonding mechanism similar to dental adhe-sive materials such as composite resin or varnish.Resin adhesives are capable of bonding to the toothsurface by diffusion and mechanical interlocking in
microporosities, and therefore may have the poten-tial to provide surface coverage, occlude dentinaltubules and prevent fluid movement.28 Moreover,propolis may provide a durable occlusion because ofits diffusion deep inside dentinal tubules that maybe difficult to remove and therefore prolong painrelief.29 However, the mechanism of action of RPEis still unclear. Propolis has been shown to stimulatethe production of transforming growth factor(TGF)-b1, a growth factor known to be importantfor odontoblast-like cell differentiation.30 Studieshave reported that when direct pulp capping wasperformed with propolis-derived flavonoids, partialdentine bridge formation was detected beneath thepulp-capping material after four weeks.31,32 Thesestudies have shown that flavonoids stimulate repara-tive dentinogenesis which is believed to contributeto the process of dentinal tubule occlusion.Novamin in this study has been shown to have asignificant effect in dentinal tubule occlusion com-pared to saline. This is consistent with previous in
Fig. 1 Summary of experimental design to prepare dentine specimens for different treatments and SEM observations.
68 © 2015 Australian Dental Association
CL Chen et al.
vitro studies by Wang et al.33,34 Favourable resultsof the efficacy of Novamin in relieving DH havealso been demonstrated by in vivo studies by Pra-deep et al.35 and Rajesh et al.10 The active ingredi-ent of Novamin is a bioactive glass that wasoriginally developed as a bone regenerative materialwhich appeared to offer suitable materials for sur-face reactivity. In an aqueous environment, sodiumions (Na+) from Novamin begin to exchange withhydrogen cations (H+ or H3O
+), which allows cal-cium ions (Ca2+) and phosphate ions (PO4
3-) to bereleased from the filler particle structure. Ca2+ andPO4
3- ions from Novamin, along with mineral ionsin saliva are able to form a calcium phosphate
(Ca-P) layer onto dentine surfaces or into tubules,resulting in physical tubule occlusion.36,37 Significantdentinal tubule occlusions were observed in samplestreated with ACC compared to those treated withNovamin and saline. This result is in agreementwith in vitro studies by Lavender et al.38 and Liet al.39 Clinical trials by Nathoo et al.40 and Kap-ferer et al.41 have also proven ACC to be effectivein relieving DH. The mechanism of action of ACCwas explained by Kleinberg,42 who suggested thatthe combination of arginine and calcium carbonateforms a positively charged complex which readilybinds to the negatively charged dentine surface andwithin the dentinal tubules. In addition, the alkalinepH of the ACC is sufficient to facilitate the deposi-tion of calcium and phosphate from saliva and/ordentinal fluid to form plugs that seal the patenttubules.42 The present study showed that ACC dem-onstrated more tubule occlusion compared toNovamin. This is inconsistent with the resultsreported by West et al. in an in situ study whichshowed 5% Novamin-based toothpaste was signifi-cantly more superior than 8% arginine-based tooth-paste.26 In the West study, an electrical toothbrushwas used for the application of desensitizing agentswhich could create more smear plugs in the dentineby the action of the bristles.43 A successful desensi-tizing agent should be able to withstand frequentchallenges by acidic drinks and food, and still dem-onstrate superior occluding properties. Citric acid isone of the major organic hydroxyl acids found infruits, fruit juices and soft drinks. Many citric juicesare over pH 2.7, but those below are still frequentlyconsumed, e.g. blackcurrant, lemon, grapefruit andlime juice.44 Therefore, 6% citric acid at pH 2 waschosen as a post-treatment in this study to simulate
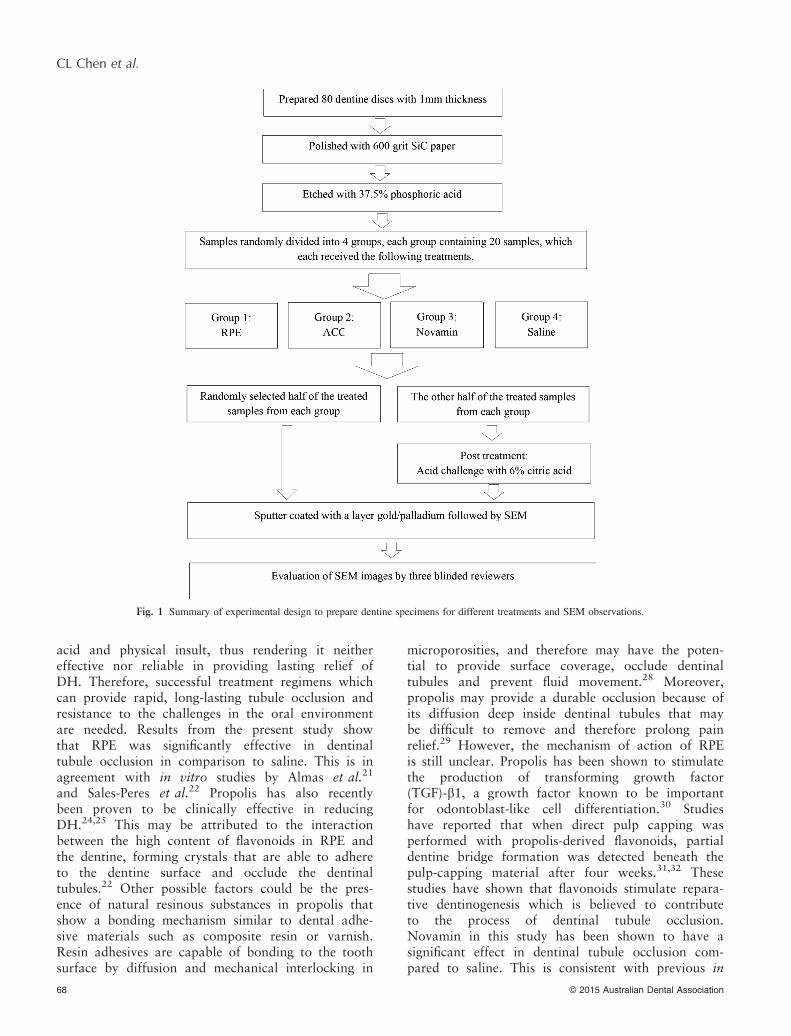
Table 1. Mean difference of tubule occlusion scorebetween groups – after treatment
Comparison betweengroups
Mean difference(i–ii)
p-value
i ii
RPE Novamin –0.350 0.006*ACC 0.433 0.000*saline –2.117 0.000*
Novamin ACC 0.783 0.000*saline –1.767 0.000*
ACC saline –2.550 0.000*
Data represent mean difference and p-value from ANOVA test andTukey adjustment.The mean difference is significant at the 0.05 level. *Significant dif-ference. **Very significant difference.Mean difference is the group in column (i) minus the group in col-umn (ii). Negative difference favours the group in column (i) whilstpositive difference favours the group in column (ii).Occlusion Classification Scoring (based on three blinded examinersaverage): 1 = occluded, 2 = mostly occluded, 3 = partially occluded,4 = mostly unoccluded, 5 = unoccluded.
Table 2. Mean difference of tubule occlusion scorebetween groups – after treatment followed by acidchallenge
Comparison betweengroups
Mean difference(i–ii)
p-value
i ii
RPE Novamin –1.283 0.000*ACC –0.783 0.000*saline –2.033 0.000*
Novamin ACC 0.500 0.000*saline –0.750 0.000*
ACC saline –1.250 0.000*
Data represent mean difference and p-value from ANOVA test andTukey adjustment.The mean difference is significant at the 0.05 level. *Significant dif-ference. **Very significant difference.Mean difference is the group in column (i) minus the group in col-umn (ii). Negative difference favours the group in column (i) whilstpositive difference favours the group in column (ii).Occlusion Classification Scoring (based on three blinded examinersaverage): 1 = occluded, 2 = mostly occluded, 3 = partially occluded,4 = mostly unoccluded, 5 = unoccluded.
Table 3. Comparison of mean of occlusion withineach group – before and after acid challenge
Group Aftertreatment
After treatmentfollowed byacid challenge
Meandifference
p-value
RPE 2.88 2.94 –0.058 0.664Novamin 3.23 4.23 –0.992 0.000*ACC 2.45 3.73 –1.275 0.000*Saline 5.00 4.98 0.025 0.083
The mean difference is significant at the 0.05 level. *Significant dif-ference. **Very significant difference.Mean difference is the tubule occlusion score of after treatmentminus the score of after treatment followed by acid challenge. Neg-ative difference favours the group in column (i) whilst positive dif-ference favours the group in column (ii).Occlusion Classification Scoring (based on three blinded examinersaverage): 1 = occluded, 2 = mostly occluded, 3 = partially occluded,4 = mostly unoccluded, 5 = unoccluded.No significant difference (p > 0.05) indicates that there was notmuch change in tubule occlusion by the treatment before and afteracid challenge.
© 2015 Australian Dental Association 69
Effectiveness of desensitizing agents in dentine tubule occlusion
the resistance of the three test products to acidchallenge in the oral environment. The results showthat all test products offered statistically significantresistance to the acid challenge when compared tosaline. Among the test products, RPE was the mostresistant to acid challenge, followed by ACC andthen Novamin. This provides evidence of the poten-tial of RPE to be used as a sustainable tubuleoccluding agent to relieve DH. Various methodshave been used in different in vitro studies to testthe mode of actions and properties of desensitizingagents including hydrostatic fluid filtration sys-tems;1,3,5 attenuated total reflection Fourier trans-form infrared spectroscopy;3 energy dispersive X-rayanalysis;3 confocal laser scanning microscopy21 andelectron spectroscopy for chemical analysis.21 Thispresent study only focused on using SEM for thevisual assessment of the level of tubule occlusion bythe test products. SEM investigation was selectedbecause it is a non-destructive approach for surfaceanalysis. It also provides high-resolution, three-dimensional images and topographical information.SEM has been used in many previous investigationsof the effect of desensitizing toothpaste on dentinetubule occlusion.22,23,26,33,34,45 Other aspects thatwere not within the scope of this study include
identification of the composition of the productsformed on the dentine discs, analysis of the extentof the product’s penetration deep into the dentinaltubules and evaluation of the dentine permeability(fluid flow). As the present study conducted was anin vitro experiment, only limited aspects of the nat-ural oral environment could be replicated. Theseinclude saliva, acquired pellicles, movement of oralmusculature and brushing habit, which can affectthe efficacy of the treatment. Therefore, further invitro as well as in vivo experiments comparingthese test products using the parameters mentionedabove should be the future scope of the presentstudy.
CONCLUSIONS
All three test agents demonstrated dentinal tubuleocclusion. Although ACC showed more occlusionfollowing treatment, RPE demonstrated a higherdegree of occlusion following acid challenge.
ACKNOWLEDGEMENTS
This study was sponsored by the International Medi-cal University, Kuala Lumpur, Malaysia. The authors
(a)
(b)
(c)
Fig. 2 Representative SEM of dentine surface showing the extent of tubule occlusion (a) after etching with phosphoric acid; (b) after treatment; (c) aftertreatment followed by acid challenge. Group 1 – RPE, Group 2 – Novamin, Group 3 – ACC, Group 4 – saline.
70 © 2015 Australian Dental Association
CL Chen et al.
would like to thank Dr Muneer Gohar Babar, Nor-bazlin Md Marham and Dr Lee Han Hing for theircontribution to the study.
REFERENCES
1. Holland GR, Narhi MN, Addy M, Gangarosa L, OrchardsonR. Guidelines for the design and conduct of clinical trails ondentine hypersensitivity. J Clin Periodontal 1997;24:808–813.
2. Rees JS, Addy M. A cross-sectional study of dentine hypersensi-tivity. J Clin Periodontol 2002;29:997–1003.
3. Irwin CR, McCusker P. Prevalence of dentine hypersensitivityin a general dental population. J Ir Dent Assoc 1997;43:7–9.
4. Bissada NF. Symptomatology and clinical features of hypersen-sitive teeth. Arch Oral Biol 1994;39:31S–32S.
5. Br€annstr€om M. Sensitivity of dentine. Oral Surg Oral Med OralPathol 1966;21:517–526.
6. Absi EG, Addy M, Adams D. Dentine hypersensitivity: a studyof the patency of dentinal tubules in sensitive and non-sensitivecervical dentine. J Clin Periodontol 1987;14:280–284.
7. Parolia A, Kundabala M, Mohan M. Management of dentinalhypersensitivity: a review. J Calif Dent Assoc 2011;39:167–179.
8. R€osing CK, Fiorini T, Liberman DN, Cavagni J. Dentine hyper-sensitivity: analysis of self-care products. Braz Oral Res2009;23:56–63.
9. Burwell AK, Litkowski LJ, Greenspan DC. Calcium sodiumphosphosilicate (NovaMin): remineralization potential. AdvDent Res 2009;21:35–39.
10. Rajesh KS, Hedge S, Arun Kumar MS, Shetty DG. Evaluationof the efficacy of a 5% calcium sodium phosphosilicate (Nov-amin®) containing dentifrice for the relief of dentinal hyper-sensitivity: a clinical study. Indian J Dent Res 2012;23:363–367.
11. Gendreau L, Barlow AP, Mason SC. Overview of the clinicalevidence for the use of NovaMin in providing relief from thepain of dentin hypersensitivity. J Clin Dent 2011;22:90–95.
12. Ananthakrishna S, Raghu TN, Koshy S, Naveen K. Clinicalevaluation of the efficacy of bioactive glass and strontium chlo-ride for treatment of dentinal hypersensitivity. J InterdiscipDent 2012;2:92–97.
13. Li Y. Innovations for combating dentin hypersensitivity: currentstate of the art. Compend Contin Educ Dent 2012;33:10–16.
14. Cummins D. Recent advances in dentin hypersensitivity: clini-cally proven treatments for instant and lasting sensitivity relief.Am J Dent 2010;23:3A–13A.
15. Parolia A, Thomas MS, Kundabala M, Mohan M. Propolis andits potential uses in oral health. Int J Med Sci 2010;2:210–215.
16. Park YK, Alencar SM, Aguiar CL. Botanical origin and chemi-cal composition of Brazilian propolis. J Agri Food Chem2002;50:2502–2506.
17. Daugsch A, Moraes CS, Fort P, Park YK. Brazilian red propo-lis–chemical composition and botanical origin. Evid BasedComplement Alternat Med 2008;5:435–441.
18. Silva BB, Rosalen PL, Cury JA, et al. Chemical compositionand botanical origin of red propolis, a new type of Brazilianpropolis. Evid Based Complement Alternat Med 2008;5:313–316.
19. Li F, Awale S, Tezuka Y, Kadota S. Cytotoxic constituentsfrom Brazilian red propolis and their structure-activity relation-ship. Bioorg Med Chem 2008;16:5434–5440.
20. Salatino A, Teixeira EW, Negri G, Message D. Origin andchemical variation of Brazilian propolis. Evid Based Comple-ment Alternat Med 2005;2:33–38.
21. Almas K, Mahmoud A, Dahlan A. A comparative study ofpropolis and saline application on human dentin. A SEM study.Indian J Dent Res 2001;12:21–27.
22. Sales-Peres SH, Carvalho FN, Marsicano JA, et al. Effect ofpropolis gel on the in vitro reduction of dentin permeability.J Appl Oral Sci 2011;19:318–323.
23. Hongal S, Torwane NA, Goel P, Chandrashekar B. The effectof 30% ethanolic extract of Indian propolis on replica ofhuman dentin compared against commercially available desensi-tizing agent: a methodological SEM study in vitro. Pharmacog-nosy Res 2014;6:113–119.
24. Madhavan S, Nayak M, Shenoy A, Shetty R, Prasad K. Den-tinal hypersensitivity: a comparative clinical evaluation of CPP-ACP F, sodium fluoride, propolis, and placebo. J Conserv Dent2012;15:315–318.
25. Torwane NA, Hongal S, Goel P, et al. Effect of two desensi-tizing agents in reducing dentin hypersensitivity: an in vivocomparative clinical trial. J Clin Diagn Res 2013;7:2042–2046.
26. West NX, Macdonald EL, Jones SB, Claydon NC, Hughes N,Jeffery P. Randomized in situ clinical study comparing the abil-ity of two new desensitizing toothpaste technologies to occludepatent dentin tubules. J Clin Dent 2011;22:82–89.
27. Davies M, Paice EM, Jones SB, Leary S, Curtis AR, West NX.Efficacy of desensitizing dentifrices to occlude dentinal tubules.Eur J Oral Sci 2011;119:497–503.
28. Meerbeek BV, Munck JD, Yoshida Y, et al. Buonocore memo-rial lecture. Adhesion to enamel and dentin: current status andfuture challenges. Oper Dent 2003;28:215–235.
29. Montero JC, Mori GG. Assessment of ion diffusion from a cal-cium hydroxide-propolis paste through dentin. Braz Oral Res2012;26:318–322.
30. Ansorge S, Reinhold D, Lendeckel U. Propolis and some of itsconstituents down-regulate DNA synthesis and inflammatorycytokine production but induce TGF-beta1 production ofhuman immune cells. Z Naturforsch C 2003;58:580–589.
31. Sabir A, Tabby CR, Agustiono P, Sosroseno W. Histologicalanalysis of rat dental pulp tissue capped with propolis. J OralSci 2005;47:135–138.
32. Parolia A, Kundabala M, Rao NN, et al. A comparative histo-logical analysis of human pulp following direct pulp cappingwith Propolis, mineral trioxide aggregate and Dycal. Aust DentJ 2010;55:59–64.
33. Wang Z, Sa Y, Sauro S, et al. Effect of desensitising toothpasteson dentinal tubule occlusion: a dentine permeability measure-ment and SEM in vitro study. J Dent 2010;38:400–410.
34. Wang Z, Jiang T, Sauro S, et al. The dentine remineralizationactivity of a desensitizing bioactive glass-containing toothpaste:an in vitro study. Aust Dent J 2011;56:372–381.
35. Pradeep AR, Sharma A. Comparison of clinical efficacy of adentifrice containing calcium sodium phosphosilicate to a denti-frice containing potassium nitrate and to a placebo on dentinalhypersensitivity: a randomized clinical trial. J Periodontol2010;81:1167–1173.
36. Hench LL, Splinter RJ, Allen WC, Greenlee TK. Bonding mech-anisms at the interface of ceramic prosthetic materials. J Bio-med Mater Res Symp 1971;5:117–141.
37. Wefel JS. Novamin: likely clinical success. Adv Dent Res2009;21:40–43.
38. Lavender SA, Petrou I, Heu R, et al. Mode of action studies ona new desensitizing dentifrice containing 8.0% arginine, a highcleaning calcium carbonate system and 1450 ppm fluoride. AmJ Dent 2010;23:14A–19A.
39. Li R, Li Y, Chen J, Zhou Z, Morrison BM Jr, Panagakos FS.Efficacy of a desensitizing toothpaste containing arginine andcalcium carbonate on dentin surface pore structure and dentinmorphology. Am J Dent 2012;25:210–214.
© 2015 Australian Dental Association 71
Effectiveness of desensitizing agents in dentine tubule occlusion

40. Nathoo S, Delgado E, Zhang YP, DeVizio W, Cummins D,Mateo LR. Comparing the efficacy in providing instant relief ofdentin hypersensitivity of a new toothpaste containing 8.0%arginine, calcium carbonate, and 1450 ppm fluoride relative toa benchmark desensitizing toothpaste containing 2% potassiumion and 1450 ppm fluoride, and to a control toothpaste with1450 ppm fluoride: a three-day clinical study in New Jersey,USA. J Clin Dent 2009;20:123–130.
41. Kapferer I, Pflug C, Kisielewsky I, Giesinger J, Beier US, Dum-fahrt H. Instant dentin hypersensitivity relief of a single topicalapplication of an in-office desensitizing paste containing 8%arginine and calcium carbonate: a split-mouth, randomized-controlled study. Acta Odontol Scand 2013;71:994–999.
42. Kleinberg I. SensiStat. A new saliva-based composition for sim-ple and effective treatment of dentinal sensitivity pain. DentToday 2002;21:42–47.
43. Prati C, Venturi L, Valdr�e G, Mongiorgi R. Dentin morphologyand permeability after brushing with different toothpastes inthe presence and absence of smear layer. J Periodontol2002;73:183–190.
44. West NX, Hughes JA, Addy M. The effect of pH on the ero-sion of dentine and enamel by dietary acids in vitro. J OralRehabil 2001;28:860–864.
45. Gillam DG, Tang JY, Mordan NJ, Newman HN. The effects ofa novel Bioglass dentifrice on dentine sensitivity: a scanningelectron microscopy investigation. J Oral Rehabil 2002;29:305–313.
Address for correspondence:Dr Abhishek Parolia
Senior LecturerSchool of Dentistry
International Medical UniversityBukit Jalil 57000
Kuala LumpurMalaysia
Email: [email protected]
72 © 2015 Australian Dental Association
CL Chen et al.