Embed Size (px)
Citation preview

Common Pediatric ID Curbsides
Susannah Kussmaul, MD Pediatric Infectious Diseases
Kaiser Permanente, Central Bay Area UCSF Volunteer Faculty
April 2016
No disclosures
Clinical Case
A 3 year-old otherwise healthy, potty-training girl presented to urgent care with fever, abdominal pain and vomiting. She was well-appearing, and her urine
dip was positive. She was started empirically on cephalexin. Now the culture is positive for E.coli that is resistant to cephalexin and ceftriaxone, and is noted to be an ESBL producer. The only oral option appears to
be ciprofloxacin. She still has mild dysuria, but is otherwise well. What should I do?
ESBL E.coli febrile UTI in a 3 year-old girl not improving on keflex:
What is the best management option?
1) Admit for IV antibiotics 2) Continue cephalexin for 1-2 days, then admit
for IV therapy if her symptoms persist 3) Give a dose of IM ceftriaxone 4) Switch to oral ciprofloxacin
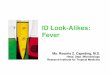
Curbside Question Can I use ciprofloxacin and other
fluoroquinolones in children?
Hampel, et al, Ped Inf Dis J 1997;16(1)
Fluoroquinolones (FQs) in Children • Cartilage damage affecting weight-bearing joints in
beagle puppies (late 1970s) – Dose-dependent – Avoidance of FQs when possible in children
• Accumulation of clinical experience suggested as safe in children as adults – Compassionate use of ciprofloxacin (CF, Staph, GNR
without other options) 2030 treatment courses in 1795 children. Adverse effects: • 1.5% with mild to moderate arthralgia
– 60% of those in patients with CF (long courses) • All resolved off of ciprofloxacin • No reported cartilage damage
≠
• 2006: AAP supports use of IV FQs as alternative therapy for resistant bacterial infections, or PO to avoid hospitalization
Fluoroquinolones (FQs) in Children Fluoroquinolones (FQs) in Children
Boxed warning from the FDA:
Fluoroquinolones are associated with an increased risk of tendinitis and tendon rupture in all ages. This risk is further increased in older patients usually over 60 years of age, in patients taking corticosteroid drugs, and in patients with kidney, heart, or lung transplants
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2004/019537s49_19847s27_19857s31_20780s13toc.cfm
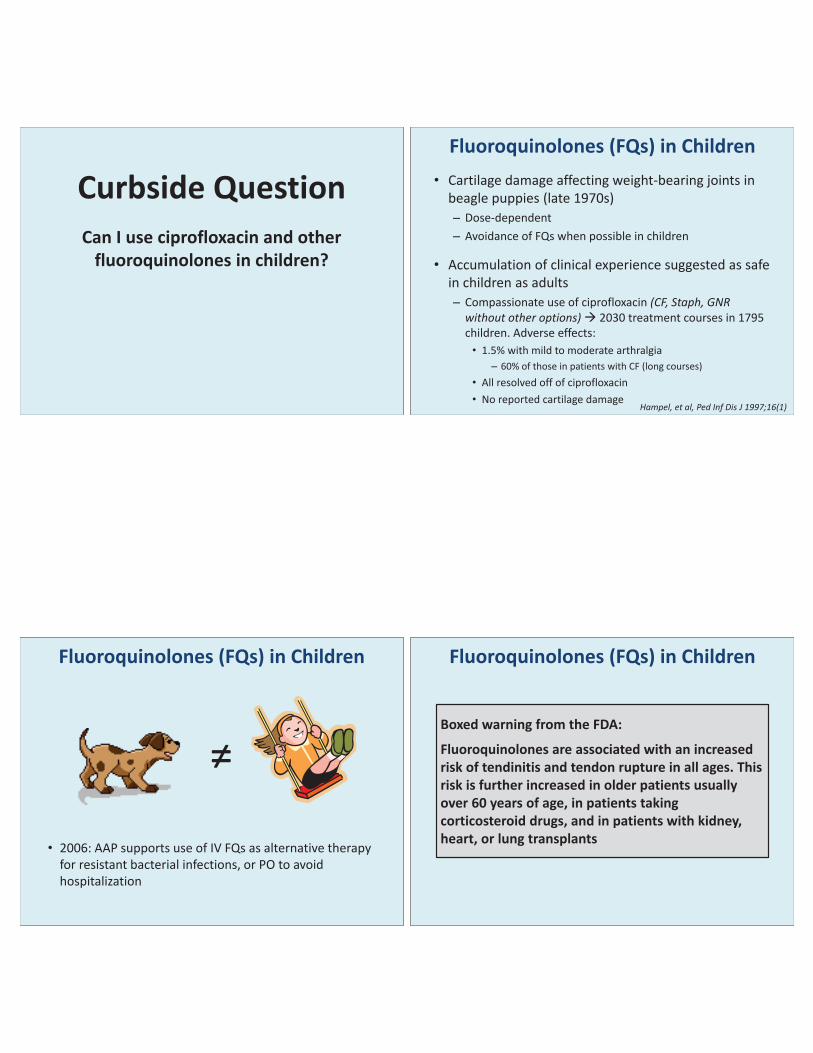
Fluoroquinolones (FQs) in Children • International prospective study • Children 1-17 years old (mean age 6 +/- 4 yrs) with
complicated UTIs or pyelonephritis
• Higher rates of arthropathy seen in the cipro group – MSK effects occurring by 6 weeks resolved, usually within 30 days of
end of treatment.
Arthropathy Rate in Cipro (n=335) vs. Standard (n=349) Treatment Groups
CIPRO COMPARATOR 95% Confidence Interval*
6 weeks 9.3% 6% -0.8% -7.2% 12 months 13.7% 9.5% -.06% - 9.1% *Study designed to demonstrate that the rate of arthropathy in the cipro group did not exceed the comparator group by more than 6% -- findings in the cipro group were not comparable to the comparator group
Noel et al, Ped Inf Dis J 2007; 26:879–891
Fluoroquinolones (FQs) in Children • 2523 children (6 mo–16 yrs) with community acquired
pneumonia or acute otitis media were randomized to receive levofloxacin vs. comparator (non-FQ) antibiotic
• Slight increase in musculoskeletal problems in FQ group (arthralgia, arthritis, tendinopathy, gait abnormality)
– Most were arthralgia (85%) – All resolved without long-term issues (followed to 5 years)
% with MSK complaints FQ group Comparator
group p-value
2 months 2.1% 0.9% <0.05 12 months 3.4% 1.8% <0.05
Bradley et al, Pediatrics 2014; 134:e146-e153
Fluoroquinolones (FQs) in Children • Follow-up to the Noel et al 2007 study enrolled children
with persisting MSK effects, or of concern to the DSMB, for 4 additional years of follow-up – Enrolled 9% of patients in each arm
• Results: – Each group had 1 patient with MSK effects “possibly related”
to FQs at 5 years – No patients with MSK effects “likely related” to FQs
• “If long-term injury occurs with levofloxacin, the rate of these events is low; if injury occurs, it appears to be reversible as assessed at 5 years”
• Limitations: high LTFU rate (~1/2); not blinded
http://idmp.ucsf.edu/news/updated-ucsf-adult-and-pediatric-antibiograms
Fluoroquinolones (FQs) in Children Antibiotic Resistance
OUTPATIENT: % Strains Susceptible to Cipro at UCSF (2014) Pathogen Adults Children
E.Coli (urine) 73% 100% INPATIENT: % Strains Susceptible to Cipro at UCSF (2014)
Pathogen Adults Children Acinetobacter baumanii 73% 100% Citrobacter freundii 80% 95% Enterobacter cloacae 91% 95% E.coli (overall) 72% 89%
E.coli (urine) 73% 91% E.coli (non-urine) 66% 67%
Klebsiella pneumonia 88% 100% Proteus mirabilis 76% 100% Pseudomonas aeruginosa (not CF) 83% 89% Serratia marcescens 100% 100%
Bradley et al, Pediatrics 2011;128;e1034; Choi et al, Kor J Ped 2013:56(5):196-201
Fluoroquinolones (FQs): Review • Bottom line: can use FQs in children
– Musculoskeletal symptoms are feared, but appear transient and relatively uncommon
– Overuse will lead to resistance – don’t use if you have other options – Appropriate if other antibiotics not available or not tolerated,
especially when oral therapy can be used instead of IV therapy
• Characteristics: – Bactericidal – Good bioavailability (70-95%; nearly 100% for levofloxacin) – Good penetration into cells, tissues, CSF
• Most common side effects: – GI symptoms (N/V/D/abdominal pain); risk for C.difficile – Rash, allergies, photosensitivity
Fluoroquinolones (FQs): Spectrum 1st generation: nalidixic acid
• Gram negative rods (Enterobacteriacae) / UTIs • FDA-approved in children > 3 months • Not currently available in the US
2nd generation: ciprofloxacin/ofloxacin, levofloxacin • Greater Gram negative activity (H.flu, Neisseria, Moraxella); Pseudomonas
(cipro>levo); S.aureus (levo>cipro); S.pneumo (levo) • FDA-approved for children 1-17 years old (cipro) and for children >6
months (levo) for certain indications
3rd generation: gemfloxacin • Increased S.pneumo and atypical coverage (e.g. Mycoplasma) • Not FDA-approved in children
4th generation: moxifloxacin • Comparable to levofloxacin for Gram positive and Gram negative
coverage; increased anaerobic and mycobacterial coverage including MTB • Not FDA-approved in children, but used off-label (community acquired
pneumonia, perioperative prophylaxis)
AAP, Pediatrics 2006;118:1287
FQs in Children: Clinical Uses FDA-approved indications
• Nalidixic acid: UTIs • Ciprofloxacin: inhalational
anthrax, complicated resistant E.coli UTI/pyelonephritis
• Levofloxacin: inhalational anthrax
AAP Guidelines
• UTI with resistant organisms – E.coli, Pseudomonas, Enterobacter,
Citrobacter, Serratia • Oral option for Pseudomonas infections
– Cystic fibrosis, chronic suppurative otitis
• Mycobacterial isolates – if susceptibility known
• GI infections – Resistant Shigella, Salmonella,
Campylobacter, Vibrio cholera • Gram-negative bacterial infections in
immunocompromised hosts – When oral therapy indicated or no
other alternative • Sepsis or meningitis from resistant
organism • Serious infections a patient with
anaphylaxis
Bradley et al, Clin Inf Dis Aug 2011
FQs in Children: Clinical Uses • More recent IDSA / PIDS guidelines
– Pediatric community acquired pneumonia (2011) • Use of levofloxacin in children as young as 6 months depending on
allergies and pathogen • First-line agent for highly resistant S.pneumo
– Pediatric bacterial sinusitis (2013) • Use of levofloxacin in patients who are failing treatment with
augmentin – Pediatric otitis media (2013)
• Use of levofloxacin as an “unconventional drug” (in consultation with specialist) for certain highly resistant strains of S.pneumo
Lieberthal et al, Pediatrics 2013;131;e964
Wald et al, Pediatrics 2013;132;e262
Back to the Case
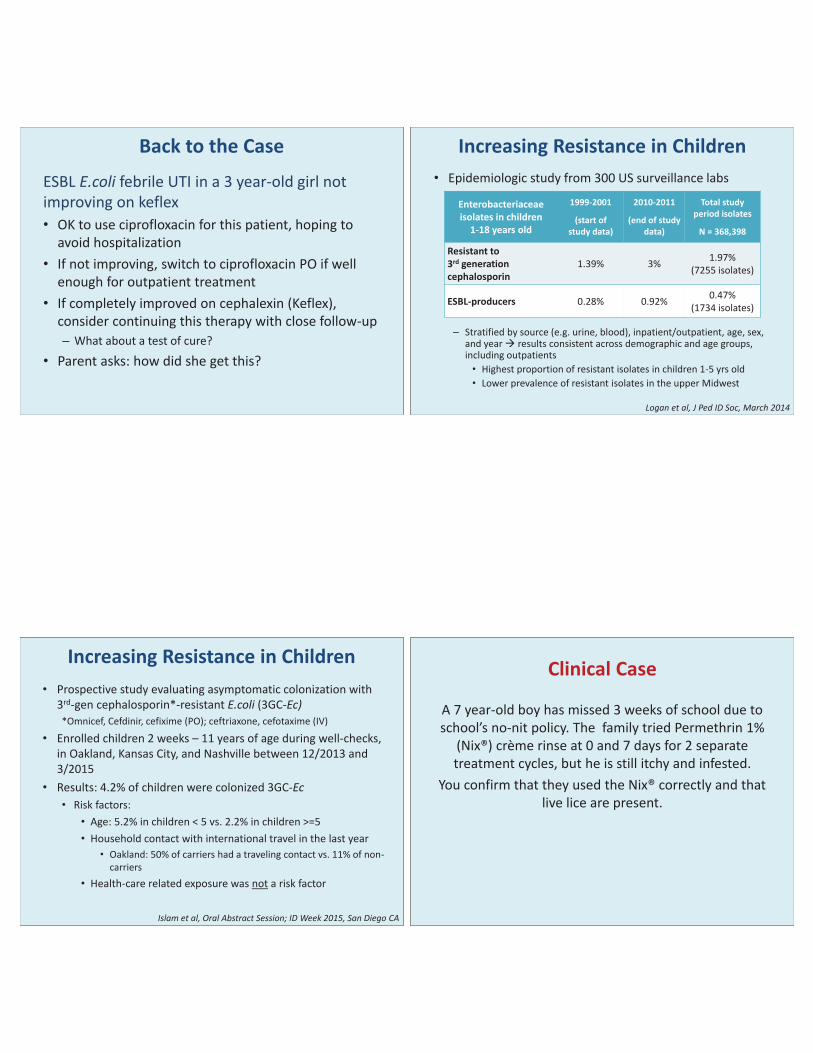
ESBL E.coli febrile UTI in a 3 year-old girl not improving on keflex • OK to use ciprofloxacin for this patient, hoping to
avoid hospitalization • If not improving, switch to ciprofloxacin PO if well
enough for outpatient treatment • If completely improved on cephalexin (Keflex),
consider continuing this therapy with close follow-up – What about a test of cure?
• Parent asks: how did she get this?
• Epidemiologic study from 300 US surveillance labs
– Stratified by source (e.g. urine, blood), inpatient/outpatient, age, sex,
and year results consistent across demographic and age groups, including outpatients • Highest proportion of resistant isolates in children 1-5 yrs old • Lower prevalence of resistant isolates in the upper Midwest
Logan et al, J Ped ID Soc, March 2014
Increasing Resistance in Children
Enterobacteriaceae isolates in children
1-18 years old
1999-2001
(start of study data)
2010-2011
(end of study data)
Total study period isolates
N = 368,398
Resistant to 3rd generation cephalosporin
1.39% 3% 1.97% (7255 isolates)
ESBL-producers 0.28% 0.92% 0.47% (1734 isolates)
• Prospective study evaluating asymptomatic colonization with 3rd-gen cephalosporin*-resistant E.coli (3GC-Ec) *Omnicef, Cefdinir, cefixime (PO); ceftriaxone, cefotaxime (IV)
• Enrolled children 2 weeks – 11 years of age during well-checks, in Oakland, Kansas City, and Nashville between 12/2013 and 3/2015
• Results: 4.2% of children were colonized 3GC-Ec • Risk factors:
• Age: 5.2% in children < 5 vs. 2.2% in children >=5 • Household contact with international travel in the last year
• Oakland: 50% of carriers had a traveling contact vs. 11% of non-carriers
• Health-care related exposure was not a risk factor
Islam et al, Oral Abstract Session; ID Week 2015, San Diego CA
Increasing Resistance in Children Clinical Case
A 7 year-old boy has missed 3 weeks of school due to school’s no-nit policy. The family tried Permethrin 1%
(Nix®) crème rinse at 0 and 7 days for 2 separate treatment cycles, but he is still itchy and infested.
You confirm that they used the Nix® correctly and that live lice are present.
Clinical Case A child with difficult-to-treat lice, whose family has used OTC therapies appropriately. Which of the following treatments is supported by evidence? A. Treatment with Cetaphil gentle cleanser B. Treatment with Benzyl Alcohol 5% (Ulesfia®) C. Treatment with Lindane D. Treatment with mayonnaise E. Either A or B
Case A healthy 3 month old and his 11 month old
cousin are exposed to zoster through Grandma, who is their main caretaker while their parents
work. Grandma recalls that both of their mothers had chicken pox as children.
Do I need to do anything for either of these babies?
3 month old baby whose caretaker has zoster; his mother had chicken pox in
childhood 1) Administer varicella immune globulin 2) Vaccinate early with live varicella vaccine 3) Consider acyclovir prophylaxis if there was
direct mucous membrane contact with lesions 4) Do nothing
11 month old baby whose caretaker has zoster; his mother had chicken pox in
childhood 1) Administer varicella immune globulin 2) Vaccinate early with live varicella vaccine 3) Consider acyclovir prophylaxis if there was
direct mucous membrane contact with lesions 4) Do nothing
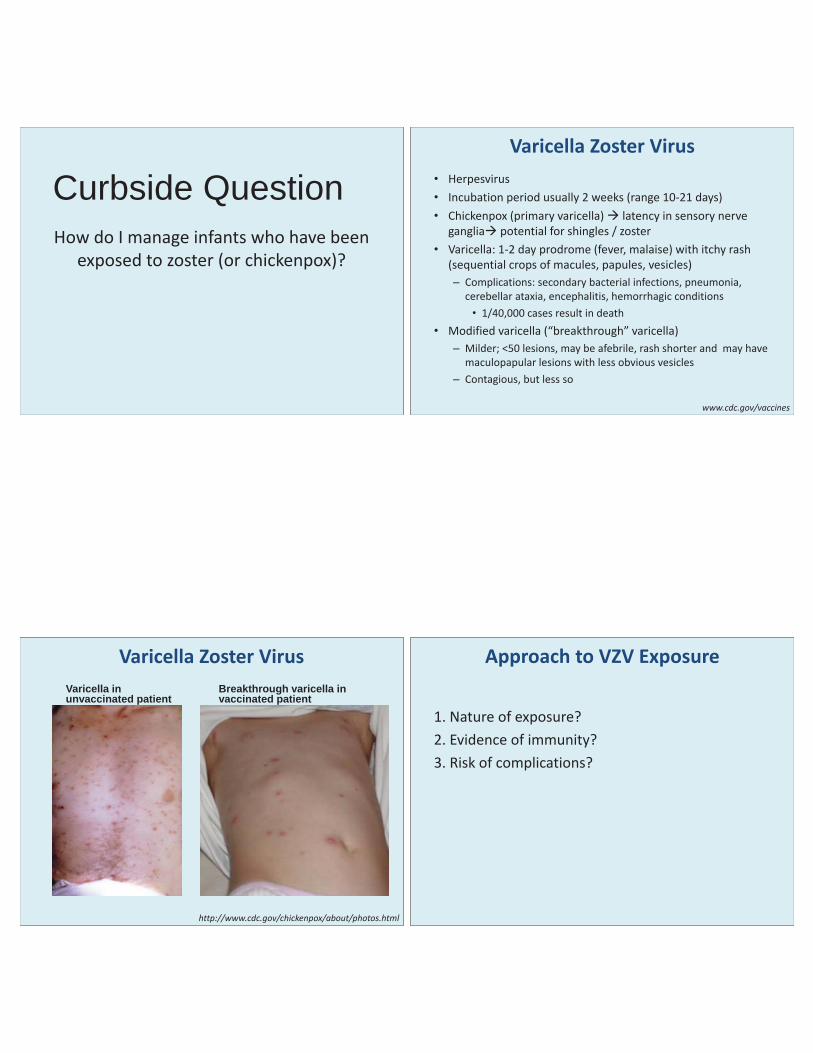
Curbside Question How do I manage infants who have been
exposed to zoster (or chickenpox)?
www.cdc.gov/vaccines
Varicella Zoster Virus • Herpesvirus • Incubation period usually 2 weeks (range 10-21 days) • Chickenpox (primary varicella) latency in sensory nerve
ganglia potential for shingles / zoster • Varicella: 1-2 day prodrome (fever, malaise) with itchy rash
(sequential crops of macules, papules, vesicles) – Complications: secondary bacterial infections, pneumonia,
cerebellar ataxia, encephalitis, hemorrhagic conditions • 1/40,000 cases result in death
• Modified varicella (“breakthrough” varicella) – Milder; <50 lesions, may be afebrile, rash shorter and may have
maculopapular lesions with less obvious vesicles – Contagious, but less so
http://www.cdc.gov/chickenpox/about/photos.html
Varicella Zoster Virus Varicella in unvaccinated patient
Breakthrough varicella in vaccinated patient
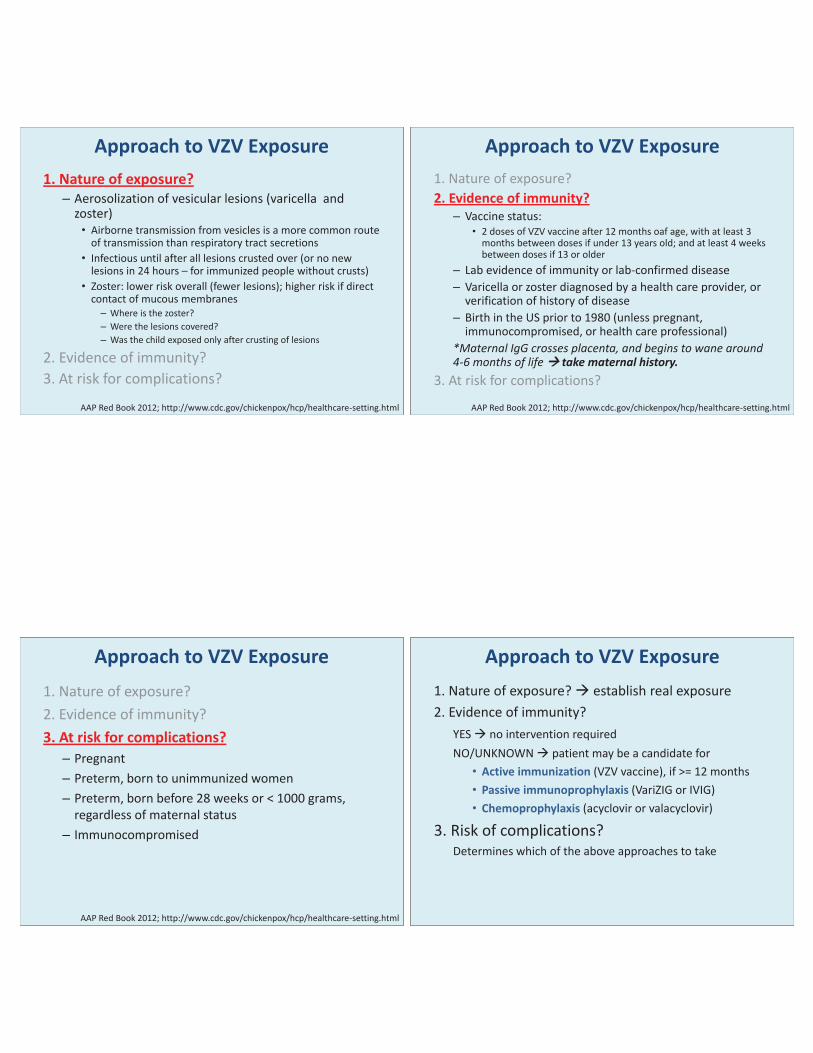
Approach to VZV Exposure
1. Nature of exposure? 2. Evidence of immunity? 3. Risk of complications?
AAP Red Book 2012; http://www.cdc.gov/chickenpox/hcp/healthcare-setting.html
Approach to VZV Exposure 1. Nature of exposure? – Aerosolization of vesicular lesions (varicella and
zoster) • Airborne transmission from vesicles is a more common route
of transmission than respiratory tract secretions • Infectious until after all lesions crusted over (or no new
lesions in 24 hours – for immunized people without crusts) • Zoster: lower risk overall (fewer lesions); higher risk if direct
contact of mucous membranes – Where is the zoster? – Were the lesions covered? – Was the child exposed only after crusting of lesions
2. Evidence of immunity? 3. At risk for complications?
AAP Red Book 2012; http://www.cdc.gov/chickenpox/hcp/healthcare-setting.html
Approach to VZV Exposure 1. Nature of exposure? 2. Evidence of immunity?
– Vaccine status: • 2 doses of VZV vaccine after 12 months oaf age, with at least 3
months between doses if under 13 years old; and at least 4 weeks between doses if 13 or older
– Lab evidence of immunity or lab-confirmed disease – Varicella or zoster diagnosed by a health care provider, or
verification of history of disease – Birth in the US prior to 1980 (unless pregnant,
immunocompromised, or health care professional) *Maternal IgG crosses placenta, and begins to wane around 4-6 months of life take maternal history.
3. At risk for complications?
AAP Red Book 2012; http://www.cdc.gov/chickenpox/hcp/healthcare-setting.html
Approach to VZV Exposure 1. Nature of exposure? 2. Evidence of immunity? 3. At risk for complications? – Pregnant – Preterm, born to unimmunized women – Preterm, born before 28 weeks or < 1000 grams,
regardless of maternal status – Immunocompromised
Approach to VZV Exposure 1. Nature of exposure? establish real exposure 2. Evidence of immunity? YES no intervention required NO/UNKNOWN patient may be a candidate for
• Active immunization (VZV vaccine), if >= 12 months • Passive immunoprophylaxis (VariZIG or IVIG) • Chemoprophylaxis (acyclovir or valacyclovir)
3. Risk of complications? Determines which of the above approaches to take
AAP Red Book 2012:
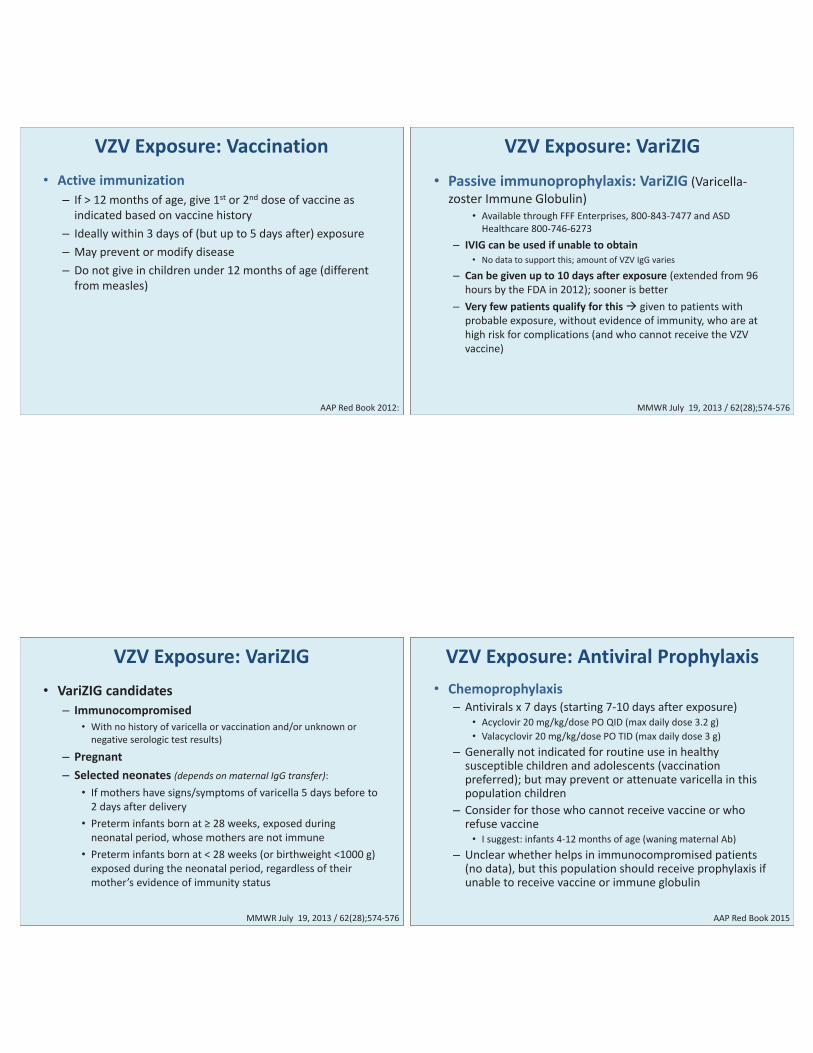
VZV Exposure: Vaccination • Active immunization
– If > 12 months of age, give 1st or 2nd dose of vaccine as indicated based on vaccine history
– Ideally within 3 days of (but up to 5 days after) exposure – May prevent or modify disease – Do not give in children under 12 months of age (different
from measles)
MMWR July 19, 2013 / 62(28);574-576
VZV Exposure: VariZIG • Passive immunoprophylaxis: VariZIG (Varicella-
zoster Immune Globulin) • Available through FFF Enterprises, 800-843-7477 and ASD
Healthcare 800-746-6273 – IVIG can be used if unable to obtain
• No data to support this; amount of VZV IgG varies
– Can be given up to 10 days after exposure (extended from 96 hours by the FDA in 2012); sooner is better
– Very few patients qualify for this given to patients with probable exposure, without evidence of immunity, who are at high risk for complications (and who cannot receive the VZV vaccine)
MMWR July 19, 2013 / 62(28);574-576
VZV Exposure: VariZIG • VariZIG candidates
– Immunocompromised • With no history of varicella or vaccination and/or unknown or
negative serologic test results)
– Pregnant – Selected neonates (depends on maternal IgG transfer):
• If mothers have signs/symptoms of varicella 5 days before to 2 days after delivery
• Preterm infants born at ≥ 28 weeks, exposed during neonatal period, whose mothers are not immune
• Preterm infants born at < 28 weeks (or birthweight <1000 g) exposed during the neonatal period, regardless of their mother’s evidence of immunity status
AAP Red Book 2015
VZV Exposure: Antiviral Prophylaxis • Chemoprophylaxis
– Antivirals x 7 days (starting 7-10 days after exposure) • Acyclovir 20 mg/kg/dose PO QID (max daily dose 3.2 g) • Valacyclovir 20 mg/kg/dose PO TID (max daily dose 3 g)
– Generally not indicated for routine use in healthy susceptible children and adolescents (vaccination preferred); but may prevent or attenuate varicella in this population children
– Consider for those who cannot receive vaccine or who refuse vaccine • I suggest: infants 4-12 months of age (waning maternal Ab)
– Unclear whether helps in immunocompromised patients (no data), but this population should receive prophylaxis if unable to receive vaccine or immune globulin
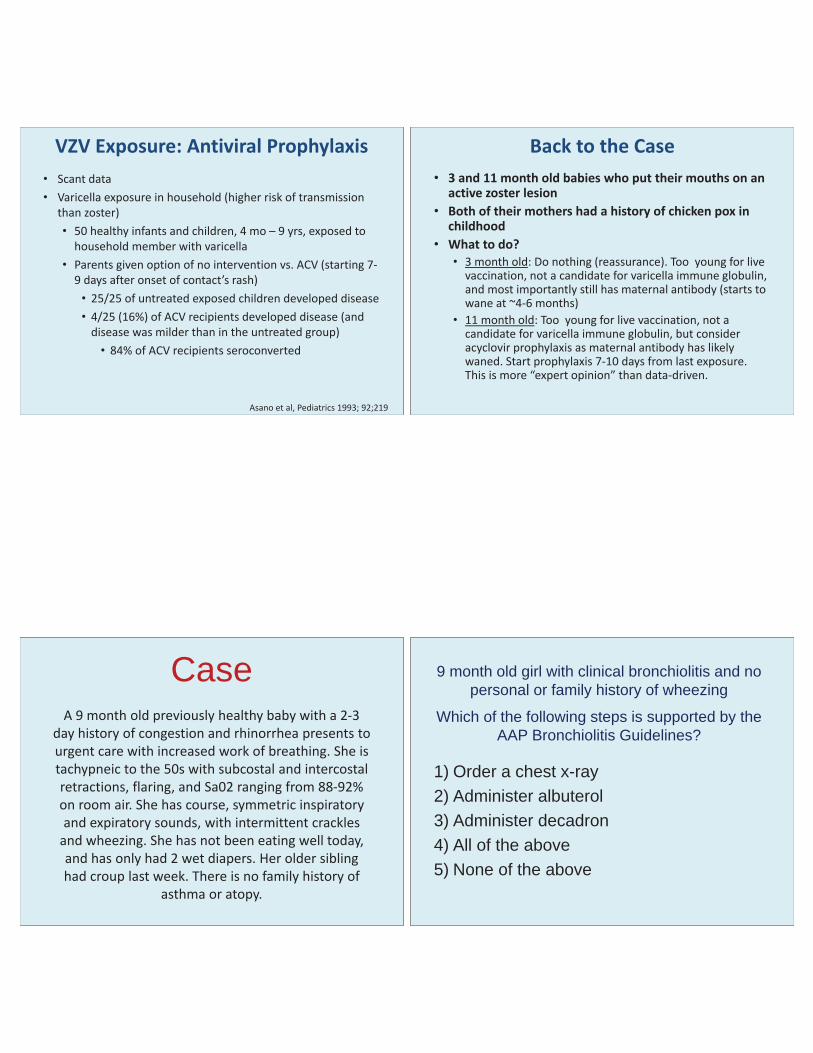
Asano et al, Pediatrics 1993; 92;219
VZV Exposure: Antiviral Prophylaxis • Scant data • Varicella exposure in household (higher risk of transmission
than zoster) • 50 healthy infants and children, 4 mo – 9 yrs, exposed to
household member with varicella • Parents given option of no intervention vs. ACV (starting 7-
9 days after onset of contact’s rash) • 25/25 of untreated exposed children developed disease • 4/25 (16%) of ACV recipients developed disease (and
disease was milder than in the untreated group) • 84% of ACV recipients seroconverted
Back to the Case • 3 and 11 month old babies who put their mouths on an
active zoster lesion • Both of their mothers had a history of chicken pox in
childhood • What to do?
• 3 month old: Do nothing (reassurance). Too young for live vaccination, not a candidate for varicella immune globulin, and most importantly still has maternal antibody (starts to wane at ~4-6 months)
• 11 month old: Too young for live vaccination, not a candidate for varicella immune globulin, but consider acyclovir prophylaxis as maternal antibody has likely waned. Start prophylaxis 7-10 days from last exposure. This is more “expert opinion” than data-driven.
Case A 9 month old previously healthy baby with a 2-3
day history of congestion and rhinorrhea presents to urgent care with increased work of breathing. She is tachypneic to the 50s with subcostal and intercostal retractions, flaring, and Sa02 ranging from 88-92% on room air. She has course, symmetric inspiratory and expiratory sounds, with intermittent crackles
and wheezing. She has not been eating well today, and has only had 2 wet diapers. Her older sibling had croup last week. There is no family history of
asthma or atopy.
9 month old girl with clinical bronchiolitis and no personal or family history of wheezing
Which of the following steps is supported by the AAP Bronchiolitis Guidelines?
1) Order a chest x-ray 2) Administer albuterol 3) Administer decadron 4) All of the above 5) None of the above
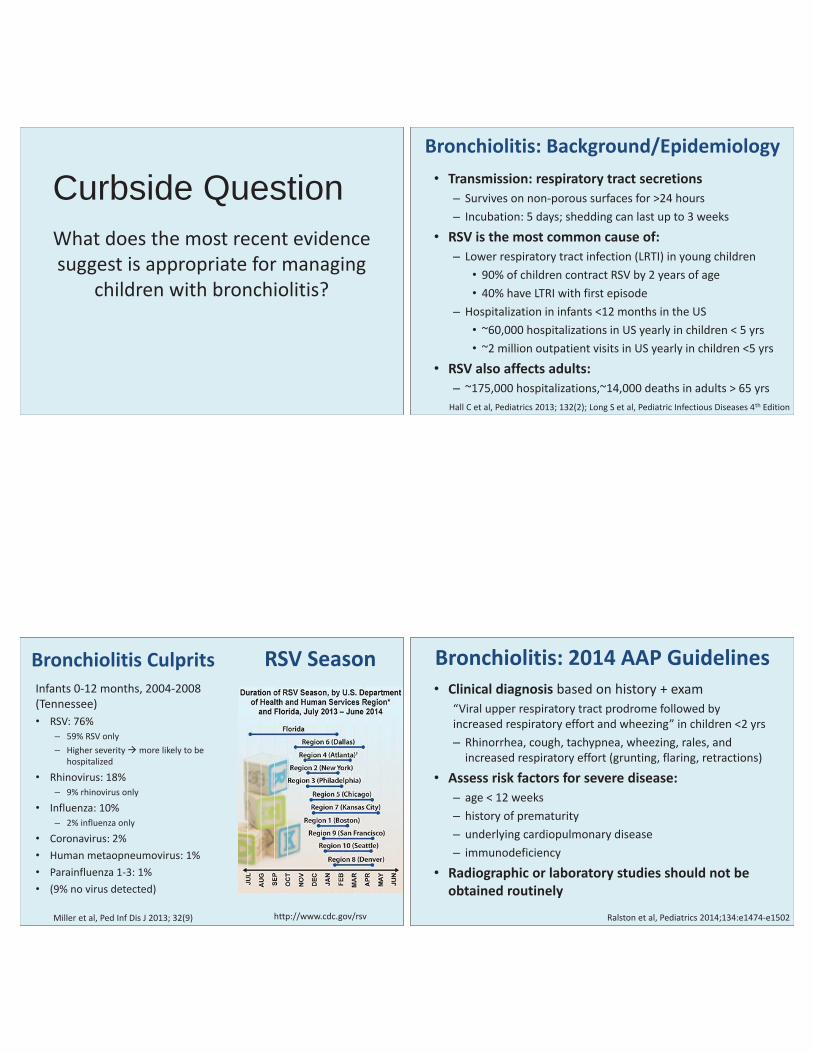
Curbside Question What does the most recent evidence suggest is appropriate for managing
children with bronchiolitis?
• Transmission: respiratory tract secretions – Survives on non-porous surfaces for >24 hours – Incubation: 5 days; shedding can last up to 3 weeks
• RSV is the most common cause of: – Lower respiratory tract infection (LRTI) in young children
• 90% of children contract RSV by 2 years of age • 40% have LTRI with first episode
– Hospitalization in infants <12 months in the US • ~60,000 hospitalizations in US yearly in children < 5 yrs • ~2 million outpatient visits in US yearly in children <5 yrs
• RSV also affects adults: – ~175,000 hospitalizations,~14,000 deaths in adults > 65 yrs
Bronchiolitis: Background/Epidemiology
Hall C et al, Pediatrics 2013; 132(2); Long S et al, Pediatric Infectious Diseases 4th Edition
RSV Season
http://www.cdc.gov/rsv
Bronchiolitis Culprits Infants 0-12 months, 2004-2008 (Tennessee) • RSV: 76%
– 59% RSV only – Higher severity more likely to be
hospitalized
• Rhinovirus: 18% – 9% rhinovirus only
• Influenza: 10% – 2% influenza only
• Coronavirus: 2% • Human metaopneumovirus: 1% • Parainfluenza 1-3: 1% • (9% no virus detected)
Miller et al, Ped Inf Dis J 2013; 32(9)
• Clinical diagnosis based on history + exam “Viral upper respiratory tract prodrome followed by increased respiratory effort and wheezing” in children <2 yrs – Rhinorrhea, cough, tachypnea, wheezing, rales, and
increased respiratory effort (grunting, flaring, retractions)
• Assess risk factors for severe disease: – age < 12 weeks – history of prematurity – underlying cardiopulmonary disease – immunodeficiency
• Radiographic or laboratory studies should not be obtained routinely
Bronchiolitis: 2014 AAP Guidelines
Ralston et al, Pediatrics 2014;134:e1474-e1502
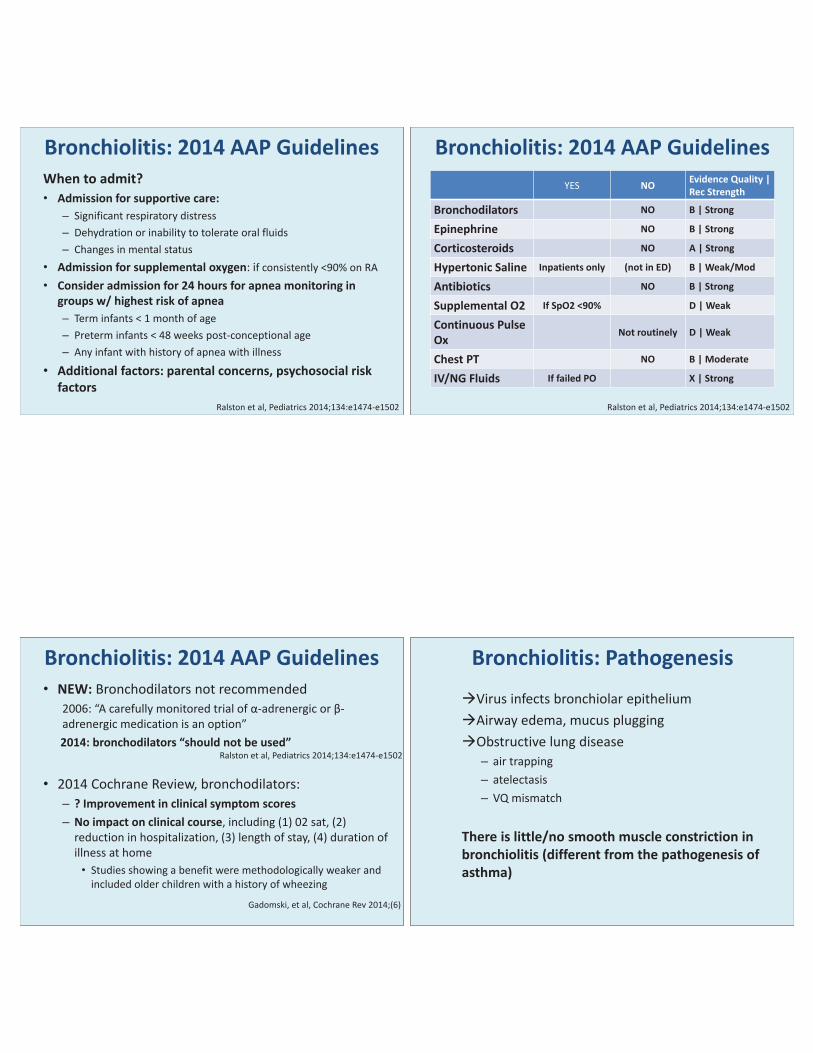
When to admit? • Admission for supportive care:
– Significant respiratory distress – Dehydration or inability to tolerate oral fluids – Changes in mental status
• Admission for supplemental oxygen: if consistently <90% on RA • Consider admission for 24 hours for apnea monitoring in
groups w/ highest risk of apnea – Term infants < 1 month of age – Preterm infants < 48 weeks post-conceptional age – Any infant with history of apnea with illness
• Additional factors: parental concerns, psychosocial risk factors
Bronchiolitis: 2014 AAP Guidelines
Ralston et al, Pediatrics 2014;134:e1474-e1502
YES NO Evidence Quality | Rec Strength
Bronchodilators NO B | Strong
Epinephrine NO B | Strong
Corticosteroids NO A | Strong
Hypertonic Saline Inpatients only (not in ED) B | Weak/Mod
Antibiotics NO B | Strong
Supplemental O2 If SpO2 <90% D | Weak
Continuous Pulse Ox
Not routinely D | Weak
Chest PT NO B | Moderate
IV/NG Fluids If failed PO X | Strong
Bronchiolitis: 2014 AAP Guidelines
Ralston et al, Pediatrics 2014;134:e1474-e1502
• NEW: Bronchodilators not recommended 2006: “A carefully monitored trial of α-adrenergic or β-adrenergic medication is an option” 2014: bronchodilators “should not be used”
• 2014 Cochrane Review, bronchodilators: – ? Improvement in clinical symptom scores – No impact on clinical course, including (1) 02 sat, (2)
reduction in hospitalization, (3) length of stay, (4) duration of illness at home • Studies showing a benefit were methodologically weaker and
included older children with a history of wheezing
Bronchiolitis: 2014 AAP Guidelines
Gadomski, et al, Cochrane Rev 2014;(6)
Ralston et al, Pediatrics 2014;134:e1474-e1502
Bronchiolitis: Pathogenesis
Virus infects bronchiolar epithelium Airway edema, mucus plugging Obstructive lung disease – air trapping – atelectasis – VQ mismatch
There is little/no smooth muscle constriction in bronchiolitis (different from the pathogenesis of asthma)
The AAP bronchiolitis guidelines “seem to be premised on an underlying belief that because bronchiolitis is a short-lived generally non-fatal disease, treatment cannot offer long-term benefit, and that most treatment should therefore be avoided. Emergency physicians’ raison d^etre however is to treat acute conditions; relieving acute respiratory distress and hypoxia using interventions as simple as albuterol and oxygen is … good emergency medicine practice”
Point: symptom relief justifies treatment
Walsh et al, West Jour Emer Med, 2015; 16(1)
Since acute viral bronchiolitis is thus a self-limited disease of relatively good prognosis, the principle of primum non nocere should temper frustrated anxiety to do something – anything – to relieve severe dyspnea. Simple physical exhaustion may determine the fate of an infant laboring to meet his metabolic requirements for oxygen. His energies should not be frittered away by the annoyance of unnecessary or futile medications and procedures. Rest should be treasured.
Counterpoint: do no harm
Wright ae al, Pediatrics 1965; 35(2)
Or: don’t just do something, stand there! • Downsides of albuterol: – Tachycardia (increased metabolic demands for a child
already ill) – Tremors – Hypoxemia – Increased interventions (e.g. steroids or other escalation of
therapy if patient doesn’t turn around quickly on steroids) – Downstream effects of labeling patient a “responder”
• Implications for future illnesses (may be treated like an asthmatic, when they aren’t)
• Increased parental expectations during future illnesses
Counterpoint: do no harm
Quinonez et al, Pediatrics 2015; 135(5)
• “A small subset of children… may have reversible airway obstruction resulting from smooth muscle constriction [but] attempts to define a subgroup of responders have not been successful to date”
• Consider a trial in patients: – With a known h/o wheezing – With a strong family h/o asthma/atopy
• If giving a trial of bronchodilators: – Careful before & after exam:
• Resp rate, wheezing, work of breathing, 02 saturation – Separate from other interventions (antipyretics, suction, IVF) – Interpret response in context of expected exam variability,
and acknowledge that as providers we over-identify “responders” - perhaps they are “responding” to the mist
Bronchiolitis: 2014 AAP Guidelines
Ralston et al, Pediatrics 2014;134:e1474-e1502
• NEW: Corticosteroids 2006: “should not be routinely used” 2014: “should not administer… in any setting”
• 2013 Cochrane Review, corticosteroids (17 trials): – No reduction in hospitalization – No change in length of stay BUT, most studies excluded those with a history of wheezing or asthma
• But steroids + bronchodilators may help some: – Infants with a family h/o asthma or eczema in a 1st degree
relative, salbuterol + dexamethasone shortened time to discharge (18 hours vs. 27 hours, 31% reduction, p = 0.015)
Bronchiolitis: 2014 AAP Guidelines
Fernandes et al, Cochrane Review 2013(6)
Ralston et al, Pediatrics 2014;134:e1474-e1502
Alansari, Pediatrics 2013
• New: Consider hypertonic saline for inpatients – No mention in 2006 guidelines – Proposed mechanism:
• Pull fluid from submucosal and adventitial spaces decrease airway edema • Improve mucociliary clearance (reduce mucus plugging)
– Benefit seen with length of stay, in patients admitted for >3 days • In US, most bronchiolitis admissions are shorter
– Recommendations: • Consider for inpatient (weak/moderate
recommendation) • Not recommended in ED (too short term to help)
Bronchiolitis: 2014 AAP Guidelines
Ralston et al, Pediatrics 2014;134:e1474-e1502
Curbside Question How can I help a family with difficult-to-
treat head lice?
Head Lice (Pediculosis Capitis)
• Incidence: 1 in 4 elementary school children – 2nd only to the common cold
– Most common in summer + after returning from vacation • Transmission: direct head contact lice crawl; they don’t hop/fly
– Not spread by swimming or pets – Rarely through pillows, hats, combs/brushes
• Estimated costs up to $1 billion yearly • Lice infestations:
– Unrelated to hygiene or socioeconomic status – Not affected by brushing – Do not spread disease (unlike body lice) no health risk
• Lice can be treated with OTC remedies , but health professionals increasingly involved

• Symptoms: – Can be asymptomatic – Itching occurs from hypersensitivity to saliva (contains
vasodilators and anticoagulants ) during blood meal • May be a late sign (4-6 weeks into infestation) • May last weeks, even after successful treatment
– Irritability / sleep disruption – Sensation of something crawling on scalp – Superinfection – Local adenopathy can occur
Head Lice (Pediculosis Capitis) • Adults: sesame seed with 6 legs
– Tan/greyish white • Darker after eating or from pigment (camouflage)
– Claws to attach to hair – Can live 30 days; mature females can lay 8 eggs/day – Several blood meals daily, or die within 1-2 days
• Eggs: firmly attached (glue-like substance) – 0.8 x 0.3 mm – 4 mm from scalp (usually viable within 6 mm)
• Hair grows ~1 cm/month
– Hatch in 8-9 days (range 7-12) – Incubated by body heat
• Viable up to 1 week in environment but won’t hatch at ambient temperatures
• Nymphs – Several blood meals daily, or die quickly – Molt 3 times, mature after 7 days
www.cdc.gov/parasites
Head Lice (Pediculosis Capitis)
• Diagnosis: presence of live lice – Tricky: move quickly, avoid light, camouflage – Use a louse/nit comb to increase sensitivity
• Nits ≠ active infestation – Firm attachment distinguishes nits from
mimics (pseudonits), such as: • Dandruff • Hair casts • Fungal infection • Hair spray / hair product residue • Other bugs (e.g. aphids blown by the wind)
– Empty casings easier to spot – Look behind ears and at nape of neck
• Lice and nits fluoresce with Wood’s lamp
www.cdc.gov/parasites
Head Lice (Pediculosis Capitis) Head Lice: OTC Treatments • Piperonyl butoxide (RID®): pyrethrin • Cost: $6 • Efficacy: 30-52% • Documented resistance: yes
– Cross-resistance with Nix® • Ovicidal: no • Minimum age: 2 years • Comments:
– AEs: Scalp and eye redness / irritation – Derived from chrysanthemums – caution if allergic to
chrysanthemums or ragweed – No residual activity – Pregnancy category C
• Use: Saturate dry hair / scalp; leave for 10 min after fully applied; rinse with water; use on day 0, and repeat on day 7-10 if live lice are seen
Devore et al, Pediatrics 2015; 135(5); Kaiser Clinical Guidance

• Permethrin 1% (Nix Crème Rinse®): synthetic pyrethroid – Similar to RID
• Cost: $9 • Efficacy: 45%; cure rate 44-68% • Documented resistance: yes, widespread in the US
– Cross-resistance with RID® • Ovicidal: no • Minimum age: 2 months • Comments:
– Low potential for toxicity (<2% absorbed) – AEs: scalp and eye redness/irritation – Residual activity for several days (don’t wash hair for at least 1-2 days) – Vinegar-based products interfere with activity – Pregnancy category B
• Use: Wash hair without conditioner, towel dry, and saturate damp hair; leave for 10 min after fully applied; rinse with water. Use on day 0, and repeat in 7 days if live lice are seen
Devore et al, Pediatrics 2015; 135(5); Kaiser Clinical Guidance
Head Lice: OTC Treatments • Malathion (Ovide®): organophosphate pesticide • Cost: $107 • Efficacy: 90%; cure rate 85% - 95% • Documented resistance: yes, but not in the US • Ovicidal: yes (partially); one treatment may be sufficient • Minimum age: 6 years
– Safety/efficacy not established in children under 6 years – Contraindicated if <2 years (concern for scalp absorption)
• Comments: • AEs: respiratory distress if ingested • ~8% systemic absorption - concern for scalp absorption in the very
young • Flammable (alcohol): no hair dryers, curling irons, smoking, open flames • Bad smell • Pregnancy category B
• Use: saturate dry hair/scalp and allow to air-dry, uncovered; wash hair after 8-12 hours; apply on day 0, and on day 7-9 days if live lice present
Head Lice: Prescription Treatments
Devore et al, Pediatrics 2015; 135(5); Kaiser Clinical Guidance
• Benzyl alcohol 5% (Ulesfia®): alcohol (non-neurotoxic) • Cost: $53 (short hair), $239 (long hair) • Efficacy: 76%; cure rate 76% • Documented resistance: N/A • Ovicidal: no • Minimum age: 6 months • Comments:
– AEs: scalp itching/irritation/redness; eye irritation; – Some systemic absorption gasping syndrome in infants < 6 months – Smells good – No residual activity – Approved 2009 – Pregnancy category B
• Use: Saturate dry hair for 10 min after fully applied; use appropriate amount (up to 6 bottles for long hair); apply on day 0 and day 7-9.
Devore et al, Pediatrics 2015; 135(5); Kaiser Clinical Guidance
Head Lice: Prescription Treatments • Spinosad (Natroba®): Non-synthetic derivative of a soil bacterium
– Non-toxic to humans
• Cost: $219
• Efficacy: 85-87%
• Documented resistance: No
• Minimum age: 4 years; effective in children >6 mo, but safety not reported
• Comments: – AEs: scalp redness/irritation, eye redness;
• Rare (<1%: dry skin, alopecia, exfoliation) – Contains benzyl alcohol – risk of gasping syndrome in infants < 6 months – Combing not necessary: ~85% efficacy without combing – Approved 2011 – Pregnancy category B
• Use: Saturate dry hair starting at scalp and leave for 10 min after fully applied; apply on day 0 and repeat on day 7 if live lice seen
Stough et al, Pediatrics 2009; Devore et al, Pediatrics 2015; 135(5); Kaiser Clinical Guidance
Head Lice: Prescription Treatments
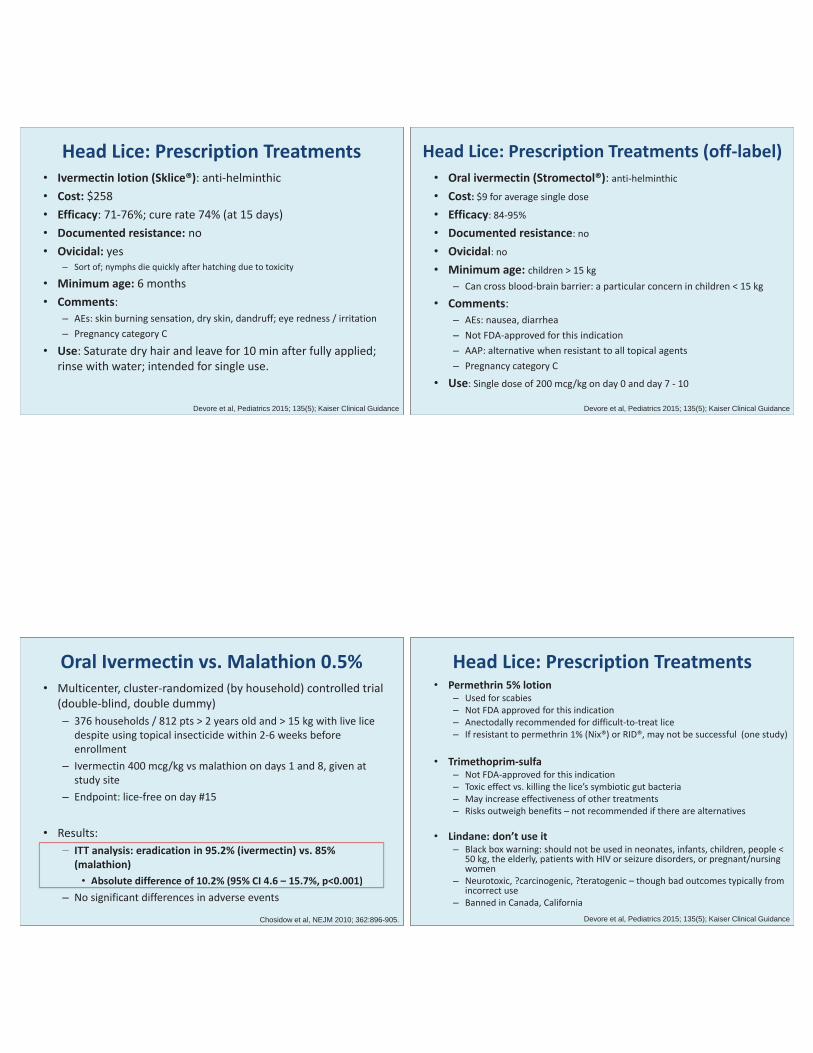
• Ivermectin lotion (Sklice®): anti-helminthic • Cost: $258 • Efficacy: 71-76%; cure rate 74% (at 15 days) • Documented resistance: no • Ovicidal: yes
– Sort of; nymphs die quickly after hatching due to toxicity
• Minimum age: 6 months • Comments:
– AEs: skin burning sensation, dry skin, dandruff; eye redness / irritation – Pregnancy category C
• Use: Saturate dry hair and leave for 10 min after fully applied; rinse with water; intended for single use.
Devore et al, Pediatrics 2015; 135(5); Kaiser Clinical Guidance
Head Lice: Prescription Treatments • Oral ivermectin (Stromectol®): anti-helminthic
• Cost: $9 for average single dose
• Efficacy: 84-95%
• Documented resistance: no
• Ovicidal: no
• Minimum age: children > 15 kg – Can cross blood-brain barrier: a particular concern in children < 15 kg
• Comments: – AEs: nausea, diarrhea – Not FDA-approved for this indication – AAP: alternative when resistant to all topical agents – Pregnancy category C
• Use: Single dose of 200 mcg/kg on day 0 and day 7 - 10
Devore et al, Pediatrics 2015; 135(5); Kaiser Clinical Guidance
Head Lice: Prescription Treatments (off-label)
• Multicenter, cluster-randomized (by household) controlled trial (double-blind, double dummy) – 376 households / 812 pts > 2 years old and > 15 kg with live lice
despite using topical insecticide within 2-6 weeks before enrollment
– Ivermectin 400 mcg/kg vs malathion on days 1 and 8, given at study site
– Endpoint: lice-free on day #15
• Results: – ITT analysis: eradication in 95.2% (ivermectin) vs. 85%
(malathion) • Absolute difference of 10.2% (95% CI 4.6 – 15.7%, p<0.001)
– No significant differences in adverse events
Oral Ivermectin vs. Malathion 0.5%
Chosidow et al, NEJM 2010; 362:896-905.
– ITT analysis: eradication in 95.2% (ivermectin) vs. 85%(malathion) • Absolute difference of 10.2% (95% CI 4.6 – 15.7%, p<0.001)
• Permethrin 5% lotion – Used for scabies – Not FDA approved for this indication – Anectodally recommended for difficult-to-treat lice – If resistant to permethrin 1% (Nix®) or RID®, may not be successful (one study)
• Trimethoprim-sulfa
– Not FDA-approved for this indication – Toxic effect vs. killing the lice’s symbiotic gut bacteria – May increase effectiveness of other treatments – Risks outweigh benefits – not recommended if there are alternatives
• Lindane: don’t use it
– Black box warning: should not be used in neonates, infants, children, people < 50 kg, the elderly, patients with HIV or seizure disorders, or pregnant/nursing women
– Neurotoxic, ?carcinogenic, ?teratogenic – though bad outcomes typically from incorrect use
– Banned in Canada, California Devore et al, Pediatrics 2015; 135(5); Kaiser Clinical Guidance
Head Lice: Prescription Treatments
• Remember: “natural products” may still have toxic chemicals but are not regulated by the FDA
Head Lice: “Natural” Remedies
• Petroleum jelly “helmet” overnight with showercap: some reported success – Takes 7-10 days of intensive shampooing to remove
• Mayonnaise, margarine, olive oil: not effective in one small study
Head Lice: Occlusive Agents
Takano-Lee et al, J Ped Nurs 2004
• Nuvo lotion (Cetaphil Gentle Skin Cleanser) – Apply comb blow dry wash out 8 hours later – Even without nit removal, 95% cure & 6 month remission
rate – Real-life study: families carried out the protocol at home
• Reasonable home measures: (1) clean combs/brushes; (2) change into fresh clothes; (3) heat bedding for 10 min in dryer
– Cheap; and safe (no side effects, not neurotoxic) – Instructions: http://nuvoforheadlice.com – Limitations: open trial, no blinding and no control; potential
conflict of interest (patent) – Not FDA-approved – Alternative 1st line agent at Kaiser (pending approval)
Head Lice: Occlusive Agents
Pearlman, Pediatrics 2004
• Treat only patients with live lice – Also household members with nits
within 1 cm of scalp, and bedmates – 1st line medication at Kaiser: – 1st OTC: RID or Nix, on days 0 and 7 – Alternative: cetaphil cleanser
• Treatment failure or suspected resistance: – Confirm appropriate use / identify non-compliance if present
• Live lice 24 hours after treatment suggests inappropriate application – If resistance suspected; remember RID/Nix cross-resistance – Consider cetaphil cleanser if not used already – Use benzyl alcohol (>6 mo) or malathion (>2 yrs)
• Ivermectin lotion or spinosad are more expensive alternatives – Oral ivermectin if resistant to all topical agents – not FDA approved for
this indication
Approach to Treatment
Kaiser Clinical Guideance – pending approval
Treatment failure associated with reinfestation after 2nd application
Treatment resistance likely if product used correctly, but live lice present 2-3 days later
• Shaving head –not recommended (psychological stress) • Wet-combing: manual nit removal with nit comb
– Retreatment makes this unnecessary kills nymphs before they lay eggs – Can be helpful, reduces burden of “disease” – Decreases diagnostic confusion – May be necessary for schools with “no-nit” policies
• Wet-combing without medical therapy: – Bug- busting campaigns in UK: twice weekly rigorous combing – Mixed results – likely depends on host’s hair, and diligence of comber
• Desiccation: the LouseBuster – 30 min application is 95% effective – Hot air delivered through patented high-flow applicator, lower
temperature than hair dryer – Costly (~ $100 per treatment; 2 treatments recommended) – www.kidsheadlice.com for a list of salons
Head Lice: Non-Pharmacologic Approaches “Exhaustive cleaning measures are not beneficial” – AAP guidance 2015
• Check family members; treat if nits within 1 cm of scalp; consider bedmates
• Treat items in contact with head within 48 hours (limit of lice survival) bedding (especially pillowcases), clothing, headgear, furniture, carpets/rugs, brushes/combs, car seats, etc… – Hot wash cycle, or hot water soak (temp >130 F) for 10 minutes (5 enough) – 15 min in dryer – Vaccuum (remove viable nits) – Other items (though transmission unlikely): seal in a bag for 14 days
• DO NOT: – Use hairdryers (i.e. homemade LouseBuster at home) – might burn scalp; May make
lice airborne – Treat pets, or use animal products on children – Use environmental sprays: chemical exposures, and lice die quickly (vacuum)
• Shielding shampoos: no RCTs to support efficacy
Head Lice: Environmental Measures
• Proper identification of live lice and nits • Instructions on nit combing • Treat based on live lice – not nits
– ? treat household contacts prophylactically – if so, use something cheap and non-toxic (e.g. cetaphil)
• Proper application of treatments • Pitfalls
– Decreased effectiveness because of use with conditioner – Did not saturate / use enough – Did not leave on long enough – Reinfestation – Resistance
• Nonpharmacologic measures – Environmental (cleaning) – Combing – Desiccation
• Tell schools, friends, etc… so they can check their families • CDC has a nice FAQs page for parents on their website
Head Lice: Caregiver Education • No nit policies are not recommended (AAP, CDC, American
Association of School Nurses) “No-nit” policies requiring that children be free of nits before they return to a child care facility or school have not been effective in controlling head lice transmission and are not recommended. (AAP Red Book, 2015) – Low contagion within classrooms – Result in a lot of missed school and work
• 12-24 million school days missed per year • $4-8 million per year in work / caregiver costs
• No-nit policies adds to stress and causes parents to
hide what is going on because of stigma/shame – which makes it harder to control
Head Lice: Prevention

• Devore et al, Pediatrics 2015 May;135(5) – Clinical Head Lice Guidance
• Eisenhower et al; J Ped HC 2012, Volume 26 , Issue 6 , 451 - 461 • Speare et al, Int J Derm 2003 Aug;42(8):626-9. • Takano-Lee et al, J Ped Nurs 2004 Dec;19(6):393-8. • Stough et al, Pediatrics 2009 • Pearlman, Pediatrics 2004 • Chosidow et al, NEJM 2010; 362:896-905. • www.cdc.gov • American Academy of Pediatrics, 2015 Red Book • Kaiser Permanente Clinical Guidance, draft
Head Lice: References
![Reference ID: 3235738...[see Dosage and Administration (2.1)]. Pediatric Patients (2 weeks to 12 years of age) The recommended oral dose of TAMIFLU for treatment of influenza in pediatric](https://img.pdfslide.us/doc/110x75/5e2db8ea7caa5b694e178a78/reference-id-3235738-see-dosage-and-administration-21-pediatric-patients.jpg)