Embed Size (px)
Citation preview
4/22/15
1
Common Pediatric Infec0ons
Susannah Kussmaul, MD Pediatric Infec<ous Diseases
Kaiser Permanente, Central Bay Area UCSF Volunteer Faculty
April 22, 2015
No disclosures
4/22/15
2
A 7 year-‐old boy has missed 3 weeks of school due to school’s no-‐nit policy. The family tried Permethrin 1% (Nix®) crème rinse at 0 and 7 days for 2 separate treatment cycles, but he is s<ll itchy and infested. You confirm that they used the Nix® correctly and that live lice are present. Which of the following is a recommended next step? A. Treatment with RID® (pyrethrin/piperonyl butoxide) shampoo B. Treatment with Lindane C. Treatment with Benzyl Alcohol 5% (Ulesfia®) D. Treatment with mayonnaise
Head Lice (Pediculosis Capitis) • Incidence: 1 in 4 elementary school children – 2nd only to the
common cold – Females > Males – Less common among black children
• Transmission: – Direct head contact à lice crawl; they do not hop/fly – Not spread by swimming or pets – Rarely through pillows, hats, combs/brushes
• Es<mated costs up to $1 billion yearly • Lice infesta<ons:
– Unrelated to hygiene or socioeconomic status – Not affected by brushing – though people who brush frequently may have
fewer lice in their infesta<on – Do not spread disease (unlike body lice) à no health risk
• Lice can be treated with OTC remedies , but health professionals increasingly involved
4/22/15
3
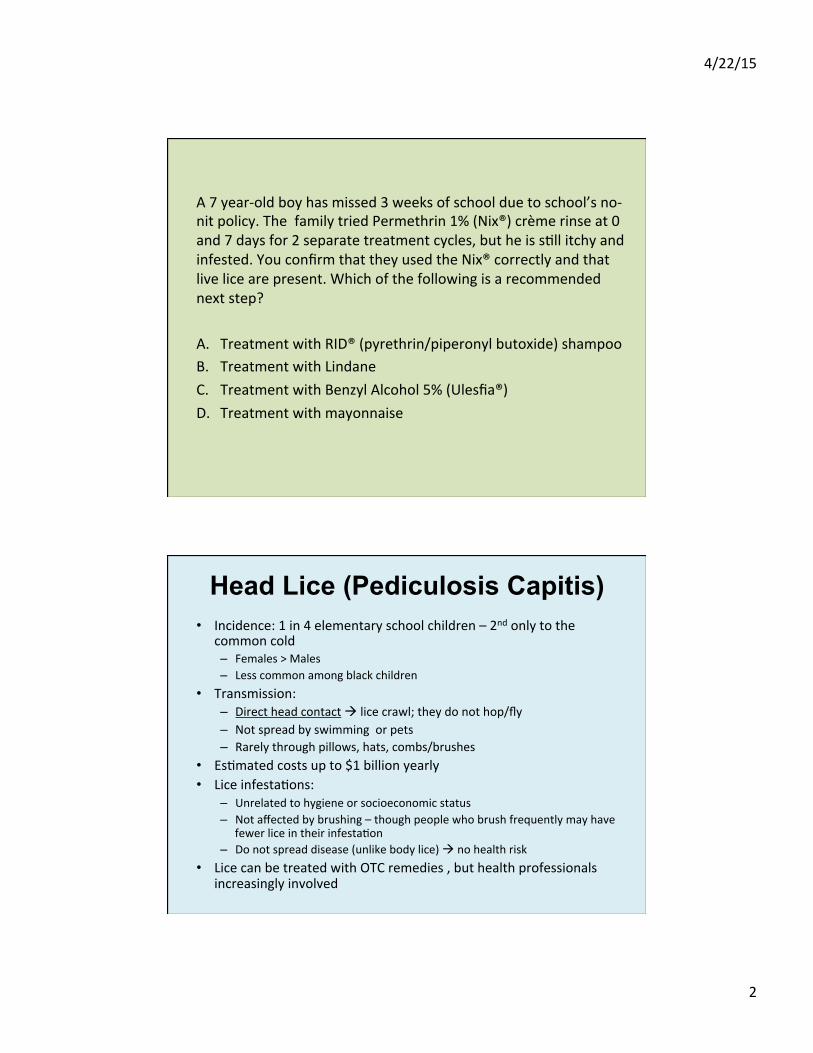
Pediculus humanus capitus • Adults: sesame seed with 6 legs
– Tan/greyish white • Darker aker ea<ng or from pigment (camouflage)
– Claws to alach to hair – Can live 30 days; mature females can lay 8 eggs/day – Several blood meals daily, or die within 1-‐2 days
• Eggs: firmly alached (glue-‐like substance) – 0.8 x 0.3 mm – 4 mm from scalp (usually viable within 6 mm)
• Hair grows ~1 cm/month
– Hatch in 8-‐9 days (range 7-‐12) – Incubated by body heat
• Viable up to 1 week in environment but won’t hatch at ambient temperatures
• Nymphs – Several blood meals daily, or die quickly – Molt 3 <mes, mature aker 7 days
www.cdc.gov/parasites
Head Lice (Pediculosis Capitis) • Symptoms:
– Oken asymptoma<c – Itching occurs from hypersensi<vity to saliva, an<coagulants etc… during blood meal
• May be a late sign, especially in the first infesta<on • May last weeks, even aker successful treatment
– Irritability / sleep disrup<on – Sensa<on of something crawling on scalp – Superinfec<on, local adenopathy can occur
4/22/15
4
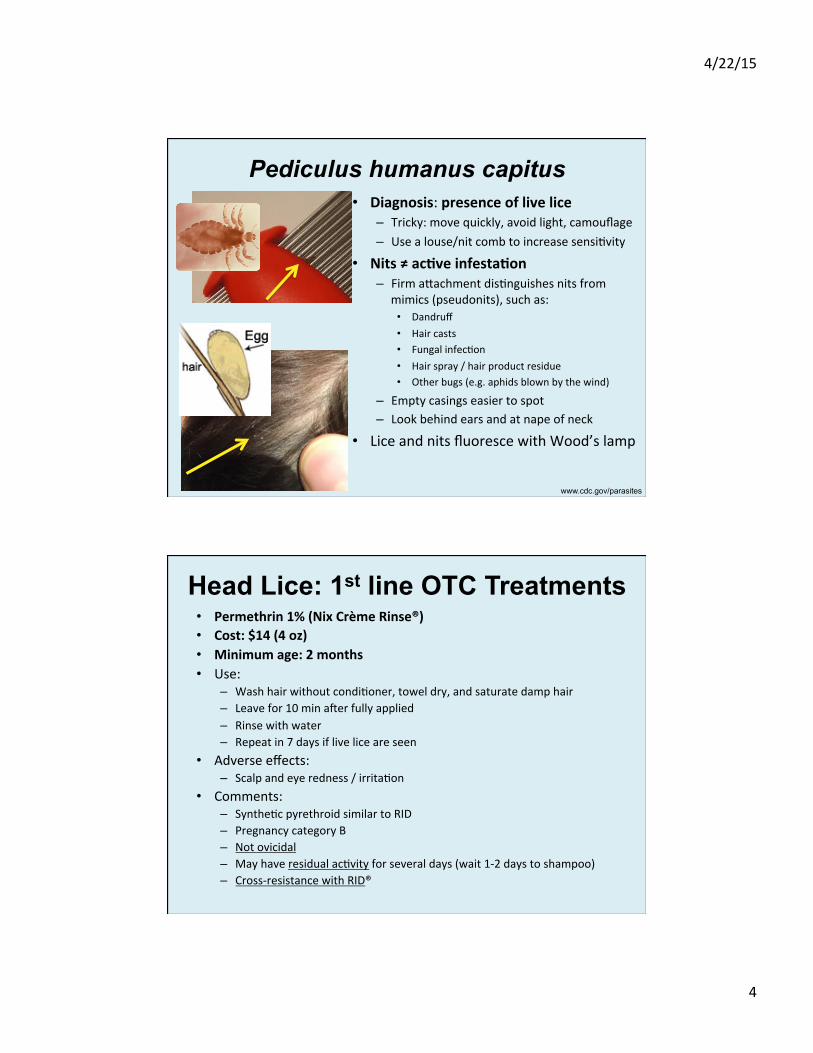
Pediculus humanus capitus • Diagnosis: presence of live lice
– Tricky: move quickly, avoid light, camouflage – Use a louse/nit comb to increase sensi<vity
• Nits ≠ ac0ve infesta0on – Firm alachment dis<nguishes nits from
mimics (pseudonits), such as: • Dandruff • Hair casts • Fungal infec<on • Hair spray / hair product residue • Other bugs (e.g. aphids blown by the wind)
– Empty casings easier to spot – Look behind ears and at nape of neck
• Lice and nits fluoresce with Wood’s lamp
www.cdc.gov/parasites
Head Lice: 1st line OTC Treatments • Permethrin 1% (Nix Crème Rinse®) • Cost: $14 (4 oz) • Minimum age: 2 months • Use:
– Wash hair without condi<oner, towel dry, and saturate damp hair – Leave for 10 min aker fully applied – Rinse with water – Repeat in 7 days if live lice are seen
• Adverse effects: – Scalp and eye redness / irrita<on
• Comments: – Synthe<c pyrethroid similar to RID – Pregnancy category B – Not ovicidal – May have residual ac<vity for several days (wait 1-‐2 days to shampoo) – Cross-‐resistance with RID®
4/22/15
5
Head Lice: 1st line OTC Treatments • Pyrethrins/piperonyl butoxide (RID®) shampoo or mousse • Cost: $9 (4 oz) • Minimum age: 2 years • Use:
– Saturate dry hair / scalp – Leave for 10 min aker fully applied – Rinse with water – Repeat in 9-‐10 days (no residual ac<vity)
• Adverse effects: – Scalp and eye redness / irrita<on
• Comments: – Pregnancy category C – Not ovicidal – Derived from chrysanthemums – cau<on if allergy to those, or ragweed – Cross-‐resistance with Nix®
• Malathion (Ovide®) • Cost: $150 for 2 oz • Minimum age: 6 years • Use:
– Saturate dry hair/scalp and allow to air-‐dry, uncovered – Wash hair aker 8-‐12 hours – Reapply aker 7-‐9 days if live lice seen
• Adverse effects: respiratory distress if ingested • Comments:
• Organophosphate pes<cide • ~8% systemic absorp<on • Pregnancy category B • Par<ally ovicidal – one treatment may be sufficient • Flammable – avoid hair dryers, curling irons, smoking • Bad smell • Gel formula<on in the works (30 min applica<on)
Head Lice: Alternative Rx Treatments
4/22/15
6
• Benzyl alcohol 5% (Ulesfia®) • Cost: $50 for 227 grams – may require several boZles • Minimum age: 6 months • Use:
– Saturate dry hair for 10 min aker fully applied – Use appropriate amount (up to 6 bolles for long hair) – Reapply aker 7-‐9 days (no residual ac<vity)
• Adverse effects: – Scalp itching/irrita<on/redness; eye irrita<on – Gasping syndrome in infants < 6 months
• Comments: – Approved 2009 – Pregnancy category B – Non-‐neurotoxic – Not ovicidal – Smells good – Some systemic absorp<on
Head Lice: Alternative Rx Treatments
• Spinosad (Natroba®) • Cost: $210 for 4 oz • Minimum age: 4 years (Effec<ve in children >6 mo, but safety not reported)
• Use: – Saturate dry hair star<ng at scalp and leave for 10 min aker fully applied – Reapply aker 7 days if live lice seen
• Adverse effects: – Scalp redness/irrita<on, eye redness; – Rare (<1%: dry skin, alopecia, exfolia<on) – Contains benzyl alcohol – gasping syndrome a concern – don’t use in kids < 6 months
• Comments: – Approved 2011 – Pregnancy category B; pump & dump – Non-‐synthe<c deriva<ve of a soil bacterium; non-‐toxic to humans – Ovicidal – Cross resistance with RID/Nix not expected – different MOA
– Combing is not necessary: ~85% efficacy without combing compared to ~45% efficacy of permethrin (with combing) in a RCT
Head Lice: Alternative Rx Treatments
Stough et al, Pediatrics 2009
4/22/15
7
• Ivermec0n lo0on (Sklice®) • Cost: $300 for 4 oz • Minimum age: 6 months • Use:
– Saturate dry hair and leave for 10 min aker fully applied – Rinse with water – Intended for single use
• Adverse effects: – Eye redness / irrita<on – Skin burning sensa<on, dry skin, dandruff
• Comments: – Pregnancy category C – Not ovicidal – but nymphs die quickly when hatched due to toxicity – Compared to placebo, 95% vs. 31% effec<ve on day #2; 85% vs 21%
effec<ve on day #8, and 74% vs. 18% effec0ve on day #15
Head Lice: Prescription Treatments
• Oral ivermec0n (Stromectol®) • Not FDA-‐approved for this indica<on • AAP: alterna<ve when resistant to all topical agents • Cost: $15 for average single dose • Minimum age: children > 15 kg • Use:
– Single dose of 200 mcg/kg, repeat aker 9-‐10 days
• Adverse effects: diarrhea, nausea • Comments:
– Not ovicidal
Head Lice: Prescription Treatments
4/22/15
8
• Mul<center, cluster-‐randomized (by household) controlled trial (double-‐blind, double dummy) – 376 households / 812 pts > 2 years old and > 15 kg with live lice despite using topical insec<cide within 2-‐6 weeks before enrollment
– Ivermec<n 400 mcg/kg vs malathion on days 1 and 8, given at study site
– Endpoint: lice-‐free on day #15
• Results: – ITT analysis: eradica0on in 95.2% (ivermec0n) vs. 85% (malathion)
• Absolute difference of 10.2% (95% CI 4.6 – 15.7%, p<0.001) – No significant differences in adverse events
Oral Ivermectin vs. Malathion 0.5%
Chosidow et al, NEJM 2010; 362:896-905.
• Permethrin 5% lo0on – Used for scabies – Not FDA approved for this indica<on – Anectodally recommended for difficult-‐to-‐treat lice – If resistant to permethrin 1% (Nix®) or RID®, may not be successful
• Trimethoprim-‐sulfa – Not FDA-‐approved for this indica<on – Toxic effect vs. killing the lice’s symbio<c gut bacteria – May increase effec<veness of other treatments – Risks outweigh benefits – not recommended if there are alterna<ves
• Lindane: don’t use it – Black box warning: should not be used in neonates, infants, children, people
< 50 kg, the elderly, pa<ents with HIV or seizure disorders, or pregnant/nursing women
– Neurotoxic, ?carcinogenic, ?teratogenic – though bad outcomes typically from incorrect use
– Banned in Canada, California
Head Lice: Prescription Treatments
4/22/15
9
• Remember: “natural products” may s<ll have toxic chemicals but are not regulated by the FDA
• Occlusive agents – Some reported success with petroleum jelly “helmet” overnight with showercap
• Takes 7-‐10 days of intensive shampooing to remove – may account for its succss
– Cetaphil cleanser (Nuvo lo<on): used like petroleum jelly, easier to remove
• Apply à blow dry à adherent film à louse suffoca<on • Even without nit removal, 95% successful in an open clinical trial • No neurotoxins
– Mayonnaise, margarine/buler, olive oil: not effec<ve in one small study
Head Lice: Home Remedies
Takano-‐Lee et al, J Ped Nurs 2004
Pearlman, Pediatrics 2004
4/22/15
10
• Shaving head – buzz cut vs. shaving à psychological stress? • Wet-‐combing: manual nit removal with nit comb
– Retreatment makes this unnecessary à kills nymphs before they lay eggs – Can be helpful, reduces burden of “disease” – Benefit:
• Decreases diagnos<c confusion • May be necessary for schools with “no-‐nit” policies
• Wet-‐combing without medical therapy: – Bug-‐ bus<ng campaigns in UK: twice weekly rigorous combing – Mixed results in studies – likely depends on host’s hair, and diligence of
comber • Desicca0on: the LouseBuster
– 30 min applica<on is 95% effec<ve – Hot air delivered through patented high-‐flow applicator, lower temperature
than hair dryer – Costly (~ $100 per treatment; 2 treatments recommended) – www.kidsheadlice.com for a list of salons
Head Lice: Non-Pharmacologic Approaches
“Herculean cleaning measures are not beneficial” – AAP guidance 2010
How to kill lice: temperatures > 130 F • Wash in hot wash cycle • 15 min in hot clothes dryer
A reasonable approach: • Wash bedding, towels, clothing, hats if used within 48 hours • Furry toys: put in the dryer, or seal in a bag for 14 days. • Vacuum couches, rugs – remember, lice die in 2 days
DO NOT: • Use hairdryers (i.e. homemade LouseBuster at home) – might burn scalp
– May make lice airborne – Dangerous with some treatments (malathion)
• Treat pets, or use animal products on children • Use shielding shampoos: no RCTs to support efficacy • Use environmental sprays: chemical exposures, and lice die quickly (just vacuum) • Use vinegar based products with permethrin– interferes with its residual ac<vity
Head Lice: Additional Measures
4/22/15
11
• Proper iden<fica<on of live lice and nits • Instruc<ons on nit combing • Treat based on live lice – not nits
– May treat household contacts prophylac<cally • Proper applica<on of treatments • Pi{alls
– Decreased effec<veness because of use with condi<oner – Did not saturate / use enough – Did not leave on long enough – Reinfesta<on – Resistance
• Nonpharmacologic measures – Environmental (cleaning) – Combing – Desicca<on
• Tell schools, friends, etc… so they can check their families • CDC has a nice FAQs page for parents on their website
Head Lice: Caregiver Education
• No nit policies are not recommended (AAP, CDC, American Associa<on of School Nurses) “No-‐nit” policies requiring that children be free of nits before they return to a child care facility or school have not been effec3ve in controlling head lice transmission and are not recommended. (AAP Red Book, 2012) – Low contagion within classrooms – Result in a lot of missed school and work
• 12-‐24 million school days missed per year • $4-‐8 million per year in work / caregiver costs
• No-‐nit policies adds to stress and causes parents to hide what is going on because of s0gma/shame – which makes it harder to control
Head Lice: Prevention
4/22/15
12
• Frankowski et al, Pediatrics 2010 Aug;126(2):392-‐403 (Head lice guidance) • Eisenhower et al; J Ped HC 2012, Volume 26 , Issue 6 , 451 -‐ 461 • Speare et al, Int J Derm 2003 Aug;42(8):626-‐9. • Takano-‐Lee et al, J Ped Nurs 2004 Dec;19(6):393-‐8. • Stough et al, Pediatrics 2009 • Pearlman, Pediatrics 2004 • Chosidow et al, NEJM 2010; 362:896-‐905. • www.cdc.gov • American Academy of Pediatrics, 2012 Red Book
Head Lice: References
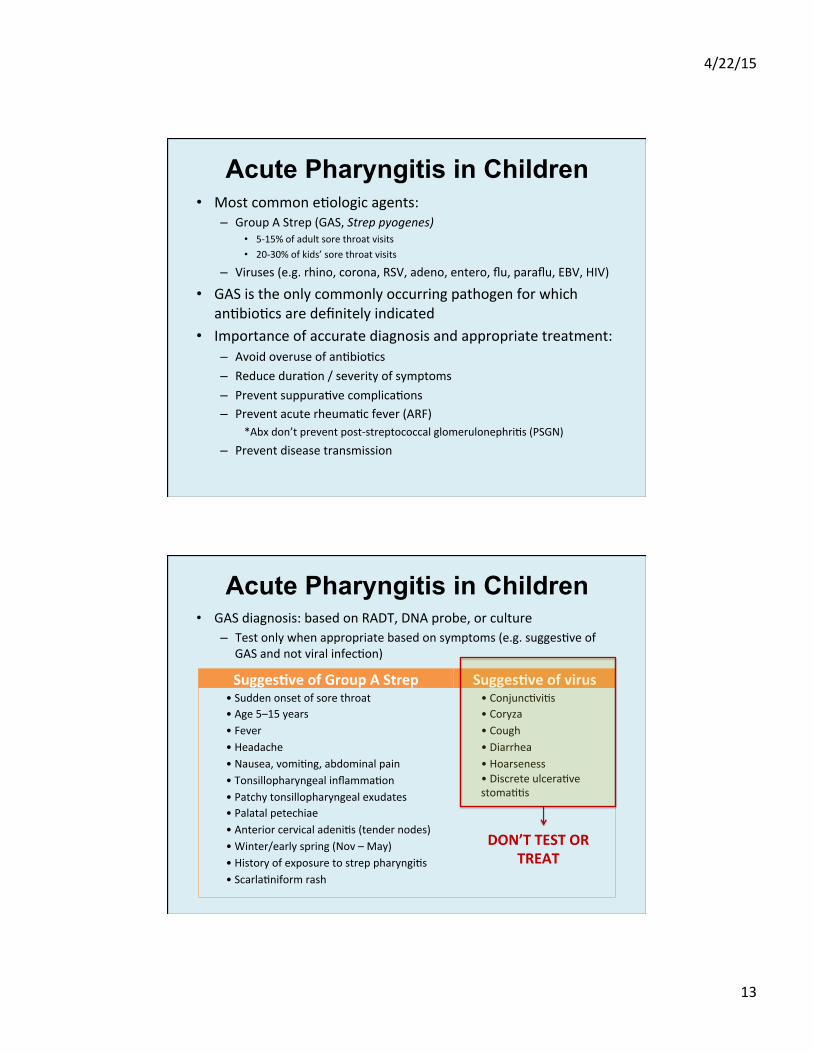
What are your next steps? A. Treat for GAS B. Test for GAS and treat later if
results posi<ve C. Test for GAS, treat now, and
discon<nue if results nega<ve D. Test for GAS, treat now, and
con<nue regardless of results since pa<ent has maximum McIsaac score of 5
Modified Centor Score (McIsaac)
Criteria Points
Temp > 38 C 1
Absence of cough 1
Swollen, tender anterior cervical nodes
1
Tonsillar swelling or exudate
1
Age 3-‐14 years 1
Age >45 years -‐1
You are seeing a 9 year-‐old boy with acute onset sore throat, fever to 39 C, headache, and abdominal pain. There is no cough or rhinorrhea. On exam he has exuda<ve tonsilli<s with tender anterior cervical nodes à McIsaac score of 5 (Centor 4)
McIsaac et al, JAMA 2004
4/22/15
13
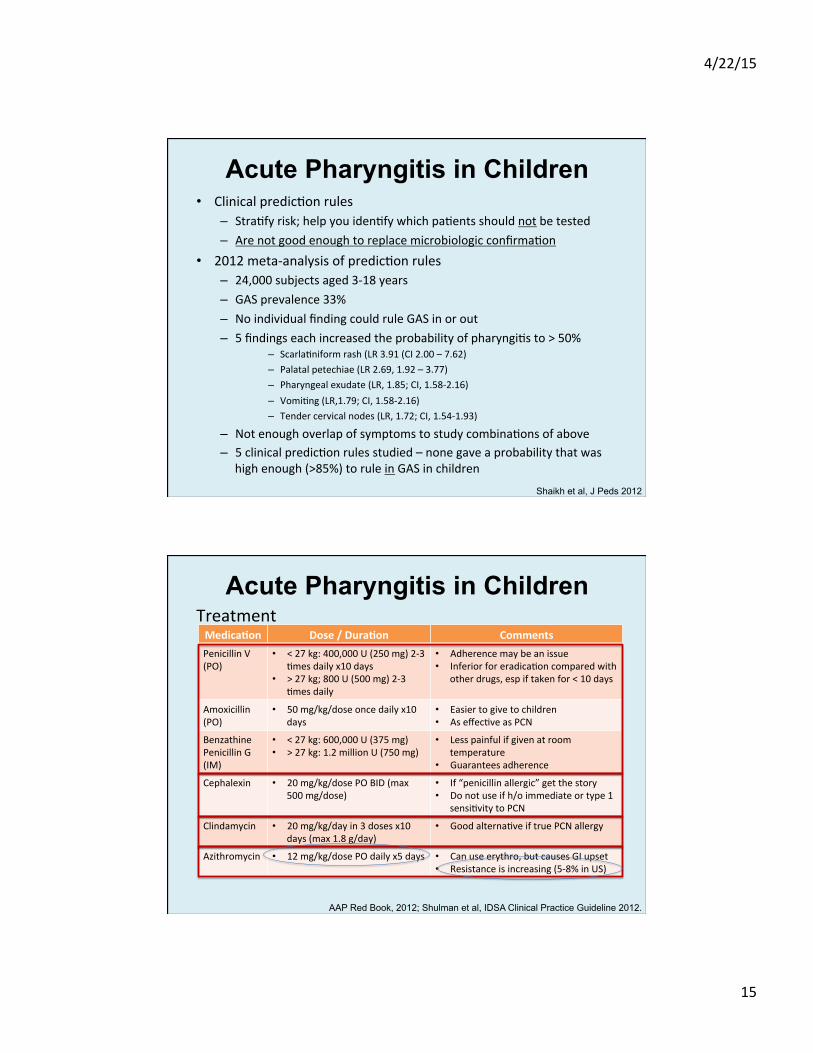
• Most common e<ologic agents: – Group A Strep (GAS, Strep pyogenes)
• 5-‐15% of adult sore throat visits • 20-‐30% of kids’ sore throat visits
– Viruses (e.g. rhino, corona, RSV, adeno, entero, flu, paraflu, EBV, HIV) • GAS is the only commonly occurring pathogen for which
an<bio<cs are definitely indicated • Importance of accurate diagnosis and appropriate treatment:
– Avoid overuse of an<bio<cs – Reduce dura<on / severity of symptoms – Prevent suppura<ve complica<ons – Prevent acute rheuma<c fever (ARF)
*Abx don’t prevent post-‐streptococcal glomerulonephri<s (PSGN)
– Prevent disease transmission
Acute Pharyngitis in Children
• GAS diagnosis: based on RADT, DNA probe, or culture – Test only when appropriate based on symptoms (e.g. sugges<ve of
GAS and not viral infec<on)
Acute Pharyngitis in Children
Sugges0ve of Group A Strep Sugges0ve of virus • Sudden onset of sore throat • Age 5–15 years • Fever • Headache • Nausea, vomi<ng, abdominal pain • Tonsillopharyngeal inflamma<on • Patchy tonsillopharyngeal exudates • Palatal petechiae • Anterior cervical adeni<s (tender nodes) • Winter/early spring (Nov – May) • History of exposure to strep pharyngi<s • Scarla<niform rash
• Conjunc<vi<s • Coryza • Cough • Diarrhea • Hoarseness • Discrete ulcera<ve stoma<<s
DON’T TEST OR TREAT

4/22/15
14
• Survey of 423 pediatricians and 525 family prac<ce physicians in 2004
• Two clinical scenarios presented – Viral pharyngi0s scenario (6 yo with 2 days of sore throat, coryza, and
no cough; has non-‐exudaIve pharyngiIs and no LAD on exam) • 81% of pediatricians and 82% of FPs would test and/or start an<bio<cs • Why is this inappropriate? à 2-‐26% GAS carriage rates depending on the cohort studied
– GAS scenario (6 yo with 2 days of sore throat and headache, without cough or coryza; exudaIve pharyngiIs + tender cervical LAD on exam):
• 42% of physicians would start an<bio<cs before test results available, and con<nue despite nega<ve results
What are your colleagues doing?
Park et al, Pediatrics 2006
• How to diagnose GAS pharyngi<s: – Not a clinical diagnosis; this has been well-‐studied
IDSA clinical prac<ce guideline, 2012: Swabbing the throat and tes<ng for GAS pharyngi<s by rapid an<gen detec<on test (RADT) and/or culture should be performed because the clinical features alone to not reliably discriminate between GAS and viral pharyngi<s except when overt viral features like rhinorrhea, cough, oral ulcers, and/or hoarseness are present
– Use RADT, DNA probe, culture depending on age • Nega<ve RADT tests in children should be backed up by a culture • Backup culture not necessary in adults (prevalence lower, ARF so rare)
– Serology (e.g. ASO, DNaseB) not helpful in acute infec<on – Note: even one dose of an<bio<cs can make a culture nega<ve
• Do not – Test asymptoma<c close contacts (unless high risk for ARF or PSGN) – Test pa<ents who just completed therapy (as a test of cure) – Test pa<ents with signs and symptoms of viral infec<on
Acute Pharyngitis in Children
4/22/15
15
• Clinical predic<on rules – Stra<fy risk; help you iden<fy which pa<ents should not be tested – Are not good enough to replace microbiologic confirma<on
• 2012 meta-‐analysis of predic<on rules – 24,000 subjects aged 3-‐18 years – GAS prevalence 33% – No individual finding could rule GAS in or out – 5 findings each increased the probability of pharyngi<s to > 50%
– Scarla<niform rash (LR 3.91 (CI 2.00 – 7.62) – Palatal petechiae (LR 2.69, 1.92 – 3.77) – Pharyngeal exudate (LR, 1.85; CI, 1.58-‐2.16) – Vomi<ng (LR,1.79; CI, 1.58-‐2.16) – Tender cervical nodes (LR, 1.72; CI, 1.54-‐1.93)
– Not enough overlap of symptoms to study combina<ons of above – 5 clinical predic<on rules studied – none gave a probability that was
high enough (>85%) to rule in GAS in children
Acute Pharyngitis in Children
Shaikh et al, J Peds 2012
Acute Pharyngitis in Children
AAP Red Book, 2012; Shulman et al, IDSA Clinical Practice Guideline 2012.
Medica0on Dose / Dura0on Comments Penicillin V (PO)
• < 27 kg: 400,000 U (250 mg) 2-‐3 <mes daily x10 days
• > 27 kg; 800 U (500 mg) 2-‐3 <mes daily
• Adherence may be an issue • Inferior for eradica<on compared with
other drugs, esp if taken for < 10 days
Amoxicillin (PO)
• 50 mg/kg/dose once daily x10 days
• Easier to give to children • As effec<ve as PCN
Benzathine Penicillin G (IM)
• < 27 kg: 600,000 U (375 mg) • > 27 kg: 1.2 million U (750 mg)
• Less painful if given at room temperature
• Guarantees adherence
Cephalexin • 20 mg/kg/dose PO BID (max 500 mg/dose)
• If “penicillin allergic” get the story • Do not use if h/o immediate or type 1
sensi<vity to PCN
Clindamycin • 20 mg/kg/day in 3 doses x10 days (max 1.8 g/day)
• Good alterna<ve if true PCN allergy
Azithromycin • 12 mg/kg/dose PO daily x5 days • Can use erythro, but causes GI upset • Resistance is increasing (5-‐8% in US)
Treatment
4/22/15
16
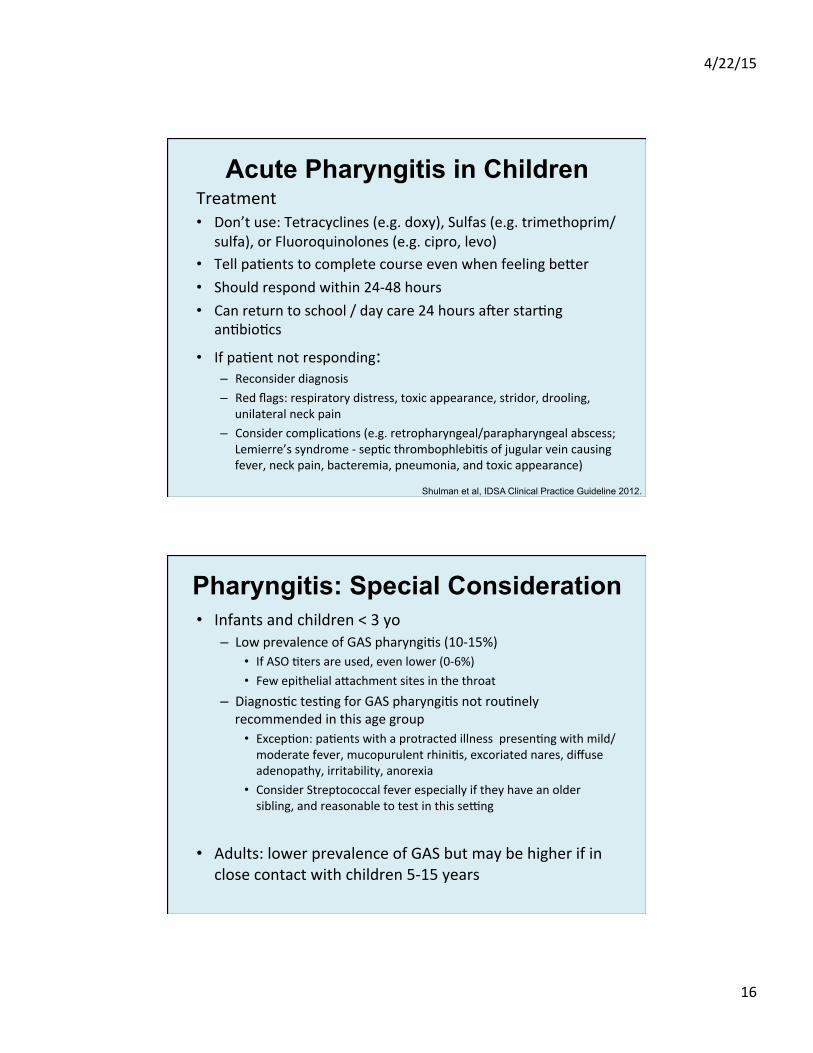
Treatment • Don’t use: Tetracyclines (e.g. doxy), Sulfas (e.g. trimethoprim/
sulfa), or Fluoroquinolones (e.g. cipro, levo) • Tell pa<ents to complete course even when feeling beler • Should respond within 24-‐48 hours • Can return to school / day care 24 hours aker star<ng
an<bio<cs
• If pa<ent not responding: – Reconsider diagnosis – Red flags: respiratory distress, toxic appearance, stridor, drooling,
unilateral neck pain – Consider complica<ons (e.g. retropharyngeal/parapharyngeal abscess;
Lemierre’s syndrome -‐ sep<c thrombophlebi<s of jugular vein causing fever, neck pain, bacteremia, pneumonia, and toxic appearance)
Acute Pharyngitis in Children
Shulman et al, IDSA Clinical Practice Guideline 2012.
• Infants and children < 3 yo – Low prevalence of GAS pharyngi<s (10-‐15%)
• If ASO <ters are used, even lower (0-‐6%) • Few epithelial alachment sites in the throat
– Diagnos<c tes<ng for GAS pharyngi<s not rou<nely recommended in this age group
• Excep<on: pa<ents with a protracted illness presen<ng with mild/moderate fever, mucopurulent rhini<s, excoriated nares, diffuse adenopathy, irritability, anorexia
• Consider Streptococcal fever especially if they have an older sibling, and reasonable to test in this se�ng
• Adults: lower prevalence of GAS but may be higher if in close contact with children 5-‐15 years
Pharyngitis: Special Consideration
4/22/15
17
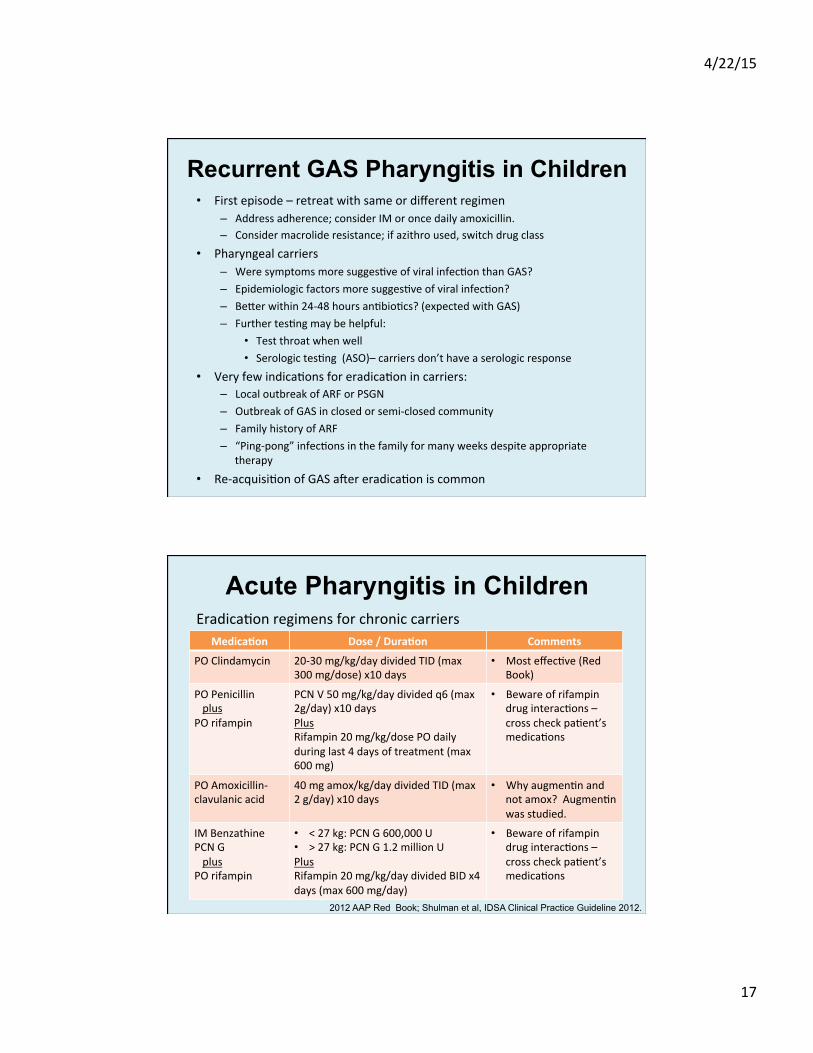
• First episode – retreat with same or different regimen – Address adherence; consider IM or once daily amoxicillin. – Consider macrolide resistance; if azithro used, switch drug class
• Pharyngeal carriers – Were symptoms more sugges<ve of viral infec<on than GAS? – Epidemiologic factors more sugges<ve of viral infec<on? – Beler within 24-‐48 hours an<bio<cs? (expected with GAS) – Further tes<ng may be helpful:
• Test throat when well • Serologic tes<ng (ASO)– carriers don’t have a serologic response
• Very few indica<ons for eradica<on in carriers: – Local outbreak of ARF or PSGN – Outbreak of GAS in closed or semi-‐closed community – Family history of ARF – “Ping-‐pong” infec<ons in the family for many weeks despite appropriate
therapy
• Re-‐acquisi<on of GAS aker eradica<on is common
Recurrent GAS Pharyngitis in Children
Eradica<on regimens for chronic carriers
Acute Pharyngitis in Children
Medica0on Dose / Dura0on Comments
PO Clindamycin 20-‐30 mg/kg/day divided TID (max 300 mg/dose) x10 days
• Most effec<ve (Red Book)
PO Penicillin plus PO rifampin
PCN V 50 mg/kg/day divided q6 (max 2g/day) x10 days Plus Rifampin 20 mg/kg/dose PO daily during last 4 days of treatment (max 600 mg)
• Beware of rifampin drug interac<ons – cross check pa<ent’s medica<ons
PO Amoxicillin-‐clavulanic acid
40 mg amox/kg/day divided TID (max 2 g/day) x10 days
• Why augmen<n and not amox? Augmen<n was studied.
IM Benzathine PCN G plus PO rifampin
• < 27 kg: PCN G 600,000 U • > 27 kg: PCN G 1.2 million U Plus Rifampin 20 mg/kg/day divided BID x4 days (max 600 mg/day)
• Beware of rifampin drug interac<ons – cross check pa<ent’s medica<ons
2012 AAP Red Book; Shulman et al, IDSA Clinical Practice Guideline 2012.
4/22/15
18
• Shaikh et al, J Peds 2012 • Shulman et al, IDSA Clinical Prac<ce Guideline 2012 • McIsaac et al, JAMA 2004 • www.cdc.gov • American Academy of Pediatrics, 2012 Red Book
Acute Pharyngitis in Children: References
In an otherwise healthy child with acute o<<s media, observa<on without star<ng an<bio<cs is a reasonable op<on for which of the following pa<ents?: A. 3 year-‐old with temperature of 102.4 (39.1 F) and mild
unilateral TM bulging B. 10 month old with temperature 101.3 F (38.5 C) and mild
unilateral TM bulging C. 10 month old with temperature 101.3 F (38.5 C) and mild
bulging of the bilateral TMs D. None of the above
4/22/15
19
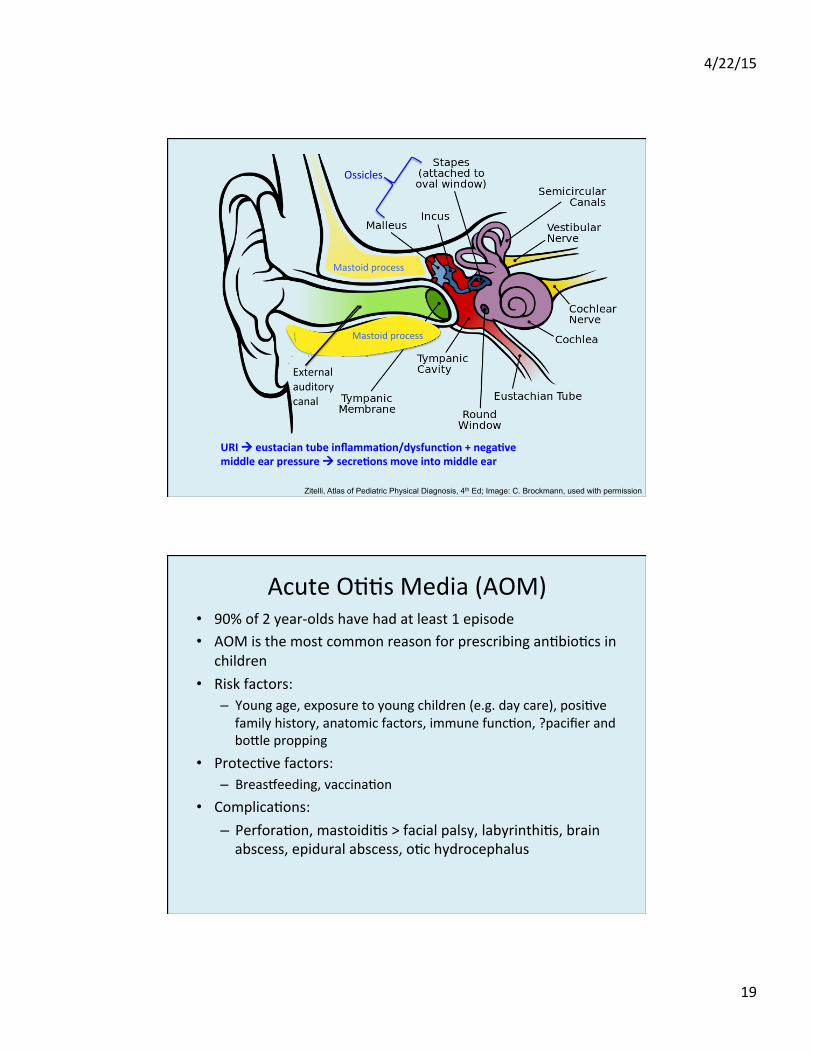
Zitelli, Atlas of Pediatric Physical Diagnosis, 4th Ed; Image: C. Brockmann, used with permission
Ossicles
Mastoid process
Mastoid process
External auditory canal
URI à eustacian tube inflamma0on/dysfunc0on + nega0ve middle ear pressure à secre0ons move into middle ear
Acute O<<s Media (AOM) • 90% of 2 year-‐olds have had at least 1 episode • AOM is the most common reason for prescribing an<bio<cs in
children • Risk factors:
– Young age, exposure to young children (e.g. day care), posi<ve family history, anatomic factors, immune func<on, ?pacifier and bolle propping
• Protec<ve factors: – Breas{eeding, vaccina<on
• Complica<ons: – Perfora<on, mastoidi<s > facial palsy, labyrinthi<s, brain abscess, epidural abscess, o<c hydrocephalus
4/22/15
20
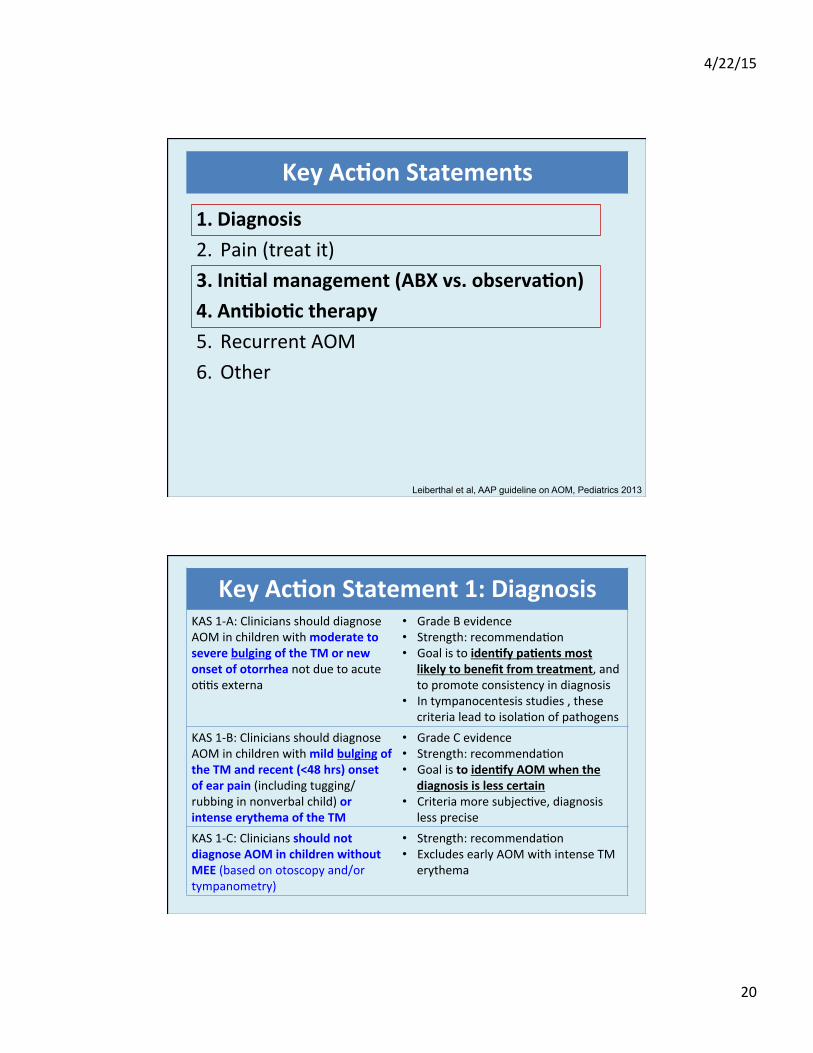
1. Diagnosis 2. Pain (treat it) 3. Ini0al management (ABX vs. observa0on) 4. An0bio0c therapy 5. Recurrent AOM 6. Other
Leiberthal et al, AAP guideline on AOM, Pediatrics 2013
Key Ac0on Statements
Key Ac0on Statement 1: Diagnosis KAS 1-‐A: Clinicians should diagnose AOM in children with moderate to severe bulging of the TM or new onset of otorrhea not due to acute o<<s externa
• Grade B evidence • Strength: recommenda<on • Goal is to iden0fy pa0ents most
likely to benefit from treatment, and to promote consistency in diagnosis
• In tympanocentesis studies , these criteria lead to isola<on of pathogens
KAS 1-‐B: Clinicians should diagnose AOM in children with mild bulging of the TM and recent (<48 hrs) onset of ear pain (including tugging/rubbing in nonverbal child) or intense erythema of the TM
• Grade C evidence • Strength: recommenda<on • Goal is to iden0fy AOM when the
diagnosis is less certain • Criteria more subjec<ve, diagnosis
less precise KAS 1-‐C: Clinicians should not diagnose AOM in children without MEE (based on otoscopy and/or tympanometry)
• Strength: recommenda<on • Excludes early AOM with intense TM
erythema
4/22/15
21
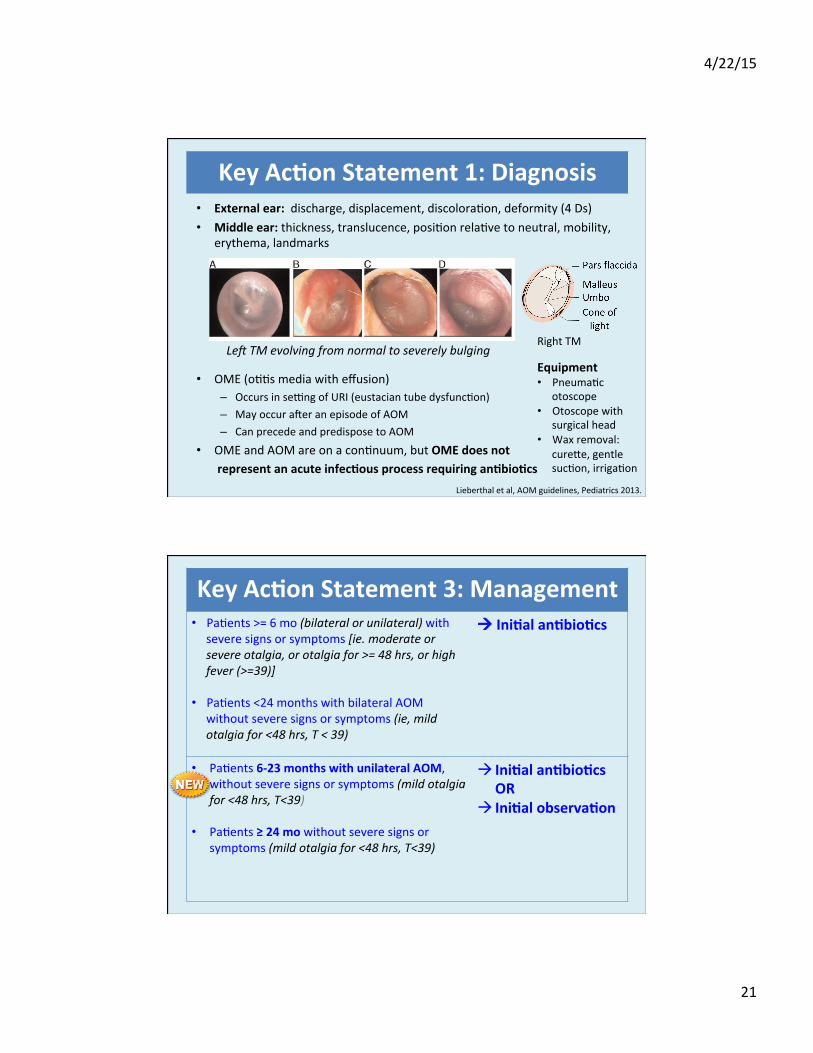
• External ear: discharge, displacement, discolora<on, deformity (4 Ds) • Middle ear: thickness, translucence, posi<on rela<ve to neutral, mobility,
erythema, landmarks
LeO TM evolving from normal to severely bulging
• OME (o<<s media with effusion) – Occurs in se�ng of URI (eustacian tube dysfunc<on) – May occur aker an episode of AOM – Can precede and predispose to AOM
• OME and AOM are on a con<nuum, but OME does not represent an acute infec0ous process requiring an0bio0cs
Lieberthal et al, AOM guidelines, Pediatrics 2013.
Key Ac0on Statement 1: Diagnosis
Right TM
Equipment • Pneuma<c
otoscope • Otoscope with
surgical head • Wax removal:
curele, gentle suc<on, irriga<on
Key Ac0on Statement 3: Management • Pa<ents >= 6 mo (bilateral or unilateral) with
severe signs or symptoms [ie. moderate or severe otalgia, or otalgia for >= 48 hrs, or high fever (>=39)]
• Pa<ents <24 months with bilateral AOM without severe signs or symptoms (ie, mild otalgia for <48 hrs, T < 39)
à Ini0al an0bio0cs
• Pa<ents 6-‐23 months with unilateral AOM, without severe signs or symptoms (mild otalgia for <48 hrs, T<39)
• Pa<ents ≥ 24 mo without severe signs or symptoms (mild otalgia for <48 hrs, T<39)
à Ini0al an0bio0cs OR
à Ini0al observa0on
4/22/15
22
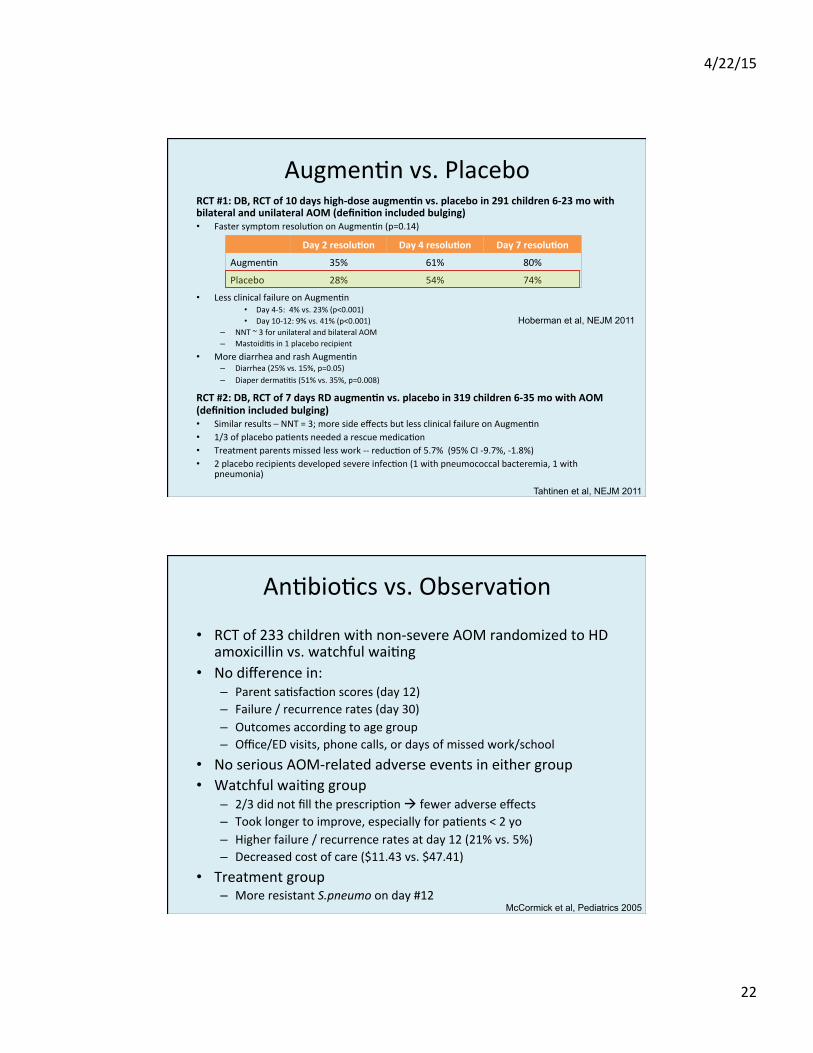
Augmen<n vs. Placebo RCT #1: DB, RCT of 10 days high-‐dose augmen0n vs. placebo in 291 children 6-‐23 mo with bilateral and unilateral AOM (defini0on included bulging) • Faster symptom resolu<on on Augmen<n (p=0.14)
• Less clinical failure on Augmen<n • Day 4-‐5: 4% vs. 23% (p<0.001) • Day 10-‐12: 9% vs. 41% (p<0.001)
– NNT ~ 3 for unilateral and bilateral AOM – Mastoidi<s in 1 placebo recipient
• More diarrhea and rash Augmen<n – Diarrhea (25% vs. 15%, p=0.05) – Diaper derma<<s (51% vs. 35%, p=0.008)
RCT #2: DB, RCT of 7 days RD augmen0n vs. placebo in 319 children 6-‐35 mo with AOM (defini0on included bulging) • Similar results – NNT = 3; more side effects but less clinical failure on Augmen<n • 1/3 of placebo pa<ents needed a rescue medica<on • Treatment parents missed less work -‐-‐ reduc<on of 5.7% (95% CI -‐9.7%, -‐1.8%) • 2 placebo recipients developed severe infec<on (1 with pneumococcal bacteremia, 1 with
pneumonia)
Hoberman et al, NEJM 2011
Day 2 resolu0on Day 4 resolu0on Day 7 resolu0on
Augmen<n 35% 61% 80%
Placebo 28% 54% 74%
Tahtinen et al, NEJM 2011
An<bio<cs vs. Observa<on
• RCT of 233 children with non-‐severe AOM randomized to HD amoxicillin vs. watchful wai<ng
• No difference in: – Parent sa<sfac<on scores (day 12) – Failure / recurrence rates (day 30) – Outcomes according to age group – Office/ED visits, phone calls, or days of missed work/school
• No serious AOM-‐related adverse events in either group • Watchful wai<ng group
– 2/3 did not fill the prescrip<on à fewer adverse effects – Took longer to improve, especially for pa<ents < 2 yo – Higher failure / recurrence rates at day 12 (21% vs. 5%) – Decreased cost of care ($11.43 vs. $47.41)
• Treatment group – More resistant S.pneumo on day #12
McCormick et al, Pediatrics 2005
4/22/15
23
• Bolom line – safe to observe some pa<ents with AOM; appropriate for: 1. Nonsevere unilateral findings/symptoms in kids < 24 mo 2. Nonsevere findings/symptoms in kids > 24 mo
à No increased risk of suppura<ve complica<ons if good follow-‐up and rescue an<bio<c given when needed
• Ini<al observa<on should be part of a larger strategy including pain meds, parent informa<on/educa<on
Key Ac0on Statement 3: Management
• AOM composi<on: – 66% bacteria + virus – 27% bacteria alone – 4% virus alone
• Usual suspects: S.pneumo, nontypeable H.flu, Moraxella – Widespread use of PCV7 (2000), has affected coloniza<on / pathogens – Currently nontypeable H.flu ≈ non-‐PCV7 S.pneumo strains – Will con<nue to evolve with use of PCV13 – Think H.flu if o<<s-‐conjunc<vi<s syndrome (or is it adenovirus…?)
• GAS, Staph aureus in <5% of cases – More common in older children – More aggressive, more likely to rupture or progress to mastoidi<s
Key Ac0on Statement 4: An0bio0cs

4/22/15
24
• Different mechanisms of resistance: – S.pneumo: penicillin binding proteins
• Overcome with higher dose of amoxicillin (“high dose amox” = S.pneumo dosing)
– H.flu and Moraxella: beta-‐lactamase • Overcome by adding beta-‐lactamase inhibitor (amox + clav) • 60-‐80% of H.flu are suscep<ble to amoxicillin • 100% of Moraxella in the upper resp tract produce B-‐lactamase, but:
– high rate of resolu<on spontaneously or on amoxicillin – Rarely progresses to mastoidi<s or intracranial infec<ons – Suggests not very virulent
– Bolom line – when using Augmen<n, H.flu is the key for expanded coverage (Moraxella kind of wimpy and will probably go away on its own)
Key Ac0on Statement 4: An0bio0cs
Key Ac0on Statement 4: An0bio0cs Ini0al Immediate or Delayed An0bio0c Treatment 1st Line Alterna<ve (PCN-‐allergic)
• Amox • Amox/clav (Augmen0n), if
• Purulent conjunc<vi<s • Amox within 30 days • Repeated failures on amox
• Cefdinir (3rd gen) • Cefuroxime (2nd gen) • Cefpodoxime (3rd gen) • Cewriaxone (3rd gen; IV/IM)
Treatment awer 48-‐72 hours if Failing Ini0al Management 1st Line Alterna<ve (PCN-‐allergic)
• Amox/clav • Cewriaxone (3rd gen; IV/IM)
• Cewriaxone (3rd gen; IV/IM) • Clindamycin +/-‐ 3rd gen cephalosporin • Tympanocentesis • Consult specialist
Don’t use: macrolides (azithro, erythro); erythro-‐sulfisoxazole; trimethoprim-‐sulfa Dura0on uncertain, not well-‐established; typically:
– 10 days for kids < 2 years with severe symptoms – 7 days for kids 2-‐5 years – 5-‐7 days for kids > 5 years
• Don’t have to follow-‐up at 10-‐14 days
• Persistent effusion is common – don’t treat it
4/22/15
25
An<bio<c dosing • Amoxicillin: 80-‐90 mg/kg/day in 2 doses
• “high dose amox” = Strep pneumo dosing • Amox/clav: 90 mg/kg/day amox + 6.4 mg/kg/day clav [ra<o 14:1] in 2 doses
• Expanded coverage of H.flu and Moraxella • 14:1 ra<o less likely to cause diarrhea
• Cefdinir (3rd gen): 14 mg/kg/day in 1 or 2 doses • Cefuroxime (2nd gen): 30 mg/kg/day in 2 doses • Cefpodoxime (3rd gen): 10 mg/kg/day in 2 doses • Cewriaxone (3rd gen): 50 mg/kg/day IM/IV in 1 dose for 1or 3 days
• Limited data – 3 days probably beler than 1 • Clindamycin 30-‐40 mg/kg/day in 3 doses
• For possible penicillin-‐resistant Strep pneumo; also Staph aureus
Keep different suscep<bility palerns in mind • Amox slightly beler against S.pneumo than cefdinir or cefuroxime • Cefdinir, cefurox beler against H.flu than amox • Augmen<n = cephalosporins against H.flu • Clinda does not cover Gram-‐nega<ves (e.g. H.flu, Moraxella)
Key Ac0on Statement 4: An0bio0cs Yuck list
Clindamycin Cefuroxime Cefpodoxime *try chocolate, nutella
• Recurrent AOM – Consider tympanocentesis with culture of middle ear fluid – Consider clindamycin (+/-‐ H.flu coverage with cefdinir, cefixime, or cefuroxime)
– Consider nasopharyngeal specimen as alterna<ve to tympanocentesis
• PPV of NP culture during AOM – 22-‐44% for S.pneumo – 50-‐71% for nontypeable H.flu – 17-‐19% for Moraxella
• NPV for all three ranges from 95-‐99%
Key Ac0on Statement 4: An0bio0cs
4/22/15
26
Otitis Media: References • Lieberthal et al, Clinical Prac<ce Guideline (AAP); Pediatrics 2013. • Karma et al, Int J Ped Otorhino 1989 • Laine et al, Pediatrics 2010 • Shaikh et al, PIDJ 2009 • Hoberman et al, NEJM 2011 • McCormick et al, Pediatrics 2005 • Palmu et al, Ped ID J, 2001
Pinworm can be diagnosed in the following ways: A. Stool O&P B. Serologic tes<ng (Enterobius an<body) C. Microscopic examina<on of sample collected from perianal
area using scotch tape D. Microscopic examina<on of sample collected from under
fingernails E. C and D
4/22/15
27
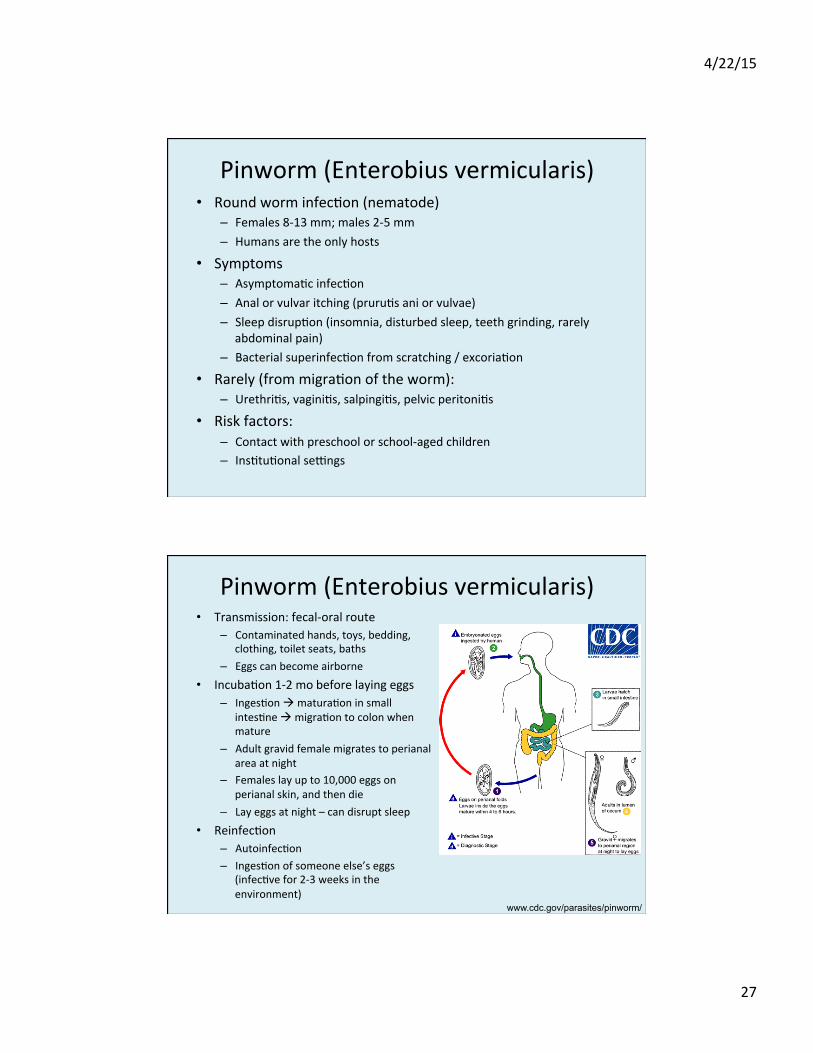
Pinworm (Enterobius vermicularis) • Round worm infec<on (nematode)
– Females 8-‐13 mm; males 2-‐5 mm – Humans are the only hosts
• Symptoms – Asymptoma<c infec<on – Anal or vulvar itching (pruru<s ani or vulvae) – Sleep disrup<on (insomnia, disturbed sleep, teeth grinding, rarely
abdominal pain) – Bacterial superinfec<on from scratching / excoria<on
• Rarely (from migra<on of the worm): – Urethri<s, vagini<s, salpingi<s, pelvic peritoni<s
• Risk factors: – Contact with preschool or school-‐aged children – Ins<tu<onal se�ngs
Pinworm (Enterobius vermicularis) • Transmission: fecal-‐oral route
– Contaminated hands, toys, bedding, clothing, toilet seats, baths
– Eggs can become airborne
• Incuba<on 1-‐2 mo before laying eggs – Inges<on à matura<on in small
intes<ne à migra<on to colon when mature
– Adult gravid female migrates to perianal area at night
– Females lay up to 10,000 eggs on perianal skin, and then die
– Lay eggs at night – can disrupt sleep • Reinfec<on
– Autoinfec<on – Inges<on of someone else’s eggs
(infec<ve for 2-‐3 weeks in the environment)
www.cdc.gov/parasites/pinworm/
4/22/15
28
Pinworm (Enterobius vermicularis) • Diagnosis
– Direct visualiza<on of adult worms in the perianal region – Best viewing <me is 2-‐3 hours aker child falls asleep – or whenever
they wake up screaming and crying – Scotch tape:
• Apply transparent (not translucent) adhesive tape to the perianal area in the morning aker waking and before toile<ng/washing
• Apply tape to glass slide • Eggs can be seen under a low-‐power lens • Ideally obtain 3 specimens on 3 consecu<ve mornings
– Alterna<ve: analyze samples from under fingernails
• Not used: – O&P: very few eggs are in the intes<nal lumen / stool – Serologic tes<ng not available – CBC: does not cause eosinophilia
Pinworm (Enterobius vermicularis)
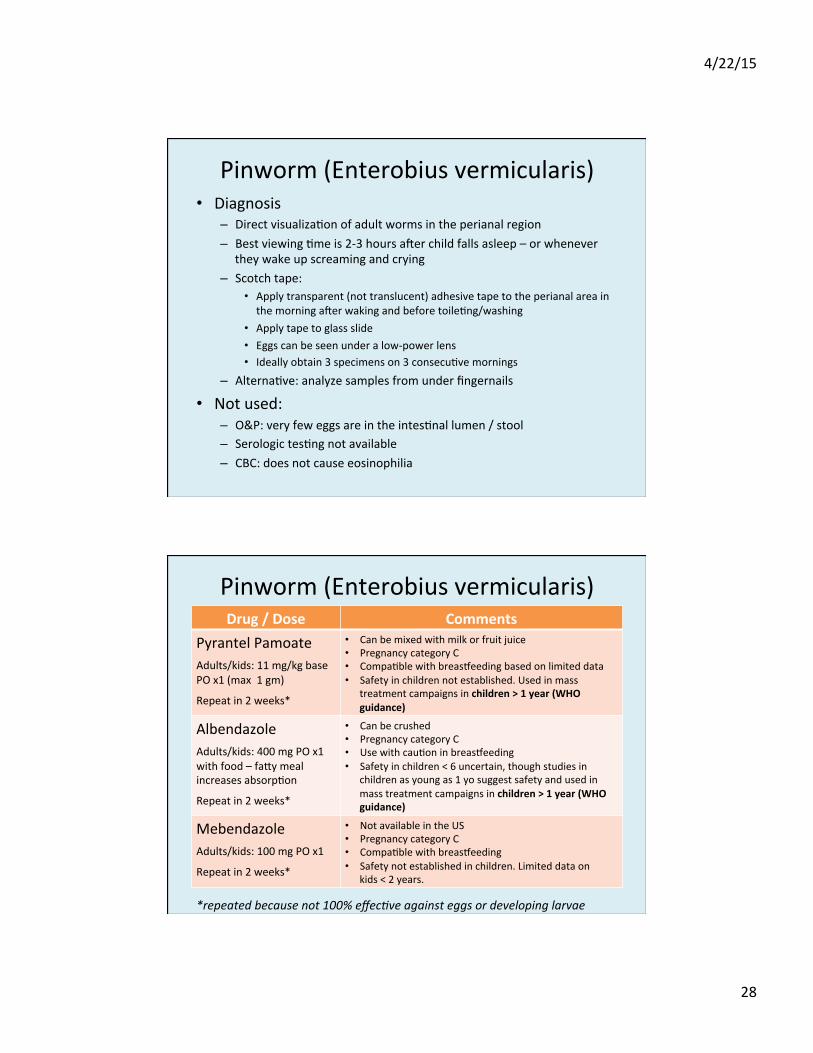
*repeated because not 100% effecIve against eggs or developing larvae
Drug / Dose Comments Pyrantel Pamoate
Adults/kids: 11 mg/kg base PO x1 (max 1 gm)
Repeat in 2 weeks*
• Can be mixed with milk or fruit juice • Pregnancy category C • Compa<ble with breas{eeding based on limited data • Safety in children not established. Used in mass
treatment campaigns in children > 1 year (WHO guidance)
Albendazole
Adults/kids: 400 mg PO x1 with food – faly meal increases absorp<on
Repeat in 2 weeks*
• Can be crushed • Pregnancy category C • Use with cau<on in breas{eeding • Safety in children < 6 uncertain, though studies in
children as young as 1 yo suggest safety and used in mass treatment campaigns in children > 1 year (WHO guidance)
Mebendazole
Adults/kids: 100 mg PO x1
Repeat in 2 weeks*
• Not available in the US • Pregnancy category C • Compa<ble with breas{eeding • Safety not established in children. Limited data on
kids < 2 years.
4/22/15
29
Pinworm (Enterobius vermicularis) • Environmental measures
– Bathe in the morning (egg burden highest) – May be helpful to frequently change underwear, PJs, and bedding
– Hand hygiene before ea<ng or preparing food, aker using toilet – Short fingernails – Avoid / discourage nail-‐bi<ng – Try not to scratch perianal region (good luck with a 3 year-‐old)
• Treat household contacts – If repeated symptoma<c infec<ons occur – If mul<ple members infected – usually the case – Reasonable to treat bed mates, bath mates