Embed Size (px)
Citation preview
colorectal
cancer
By Dr. Ryan Al.Ghanemi

overview of the lecture
case presentation.
epidemiology of colorectal cancer.
clinical presentation of colorectal cancer.
staging of colorectal cancer.
management of primary colon tumor.
management of rectal tumor.
case presentation
A 65 years old man present with dyspnea on exertion and angina for 3-4 weeks.
He denies any cough, weight loss, git symptoms.
His past medical history is significant for hypertension, stable angina, and colonic polyps
Those were removed 7 to 8 years ago by colonoscopy.

The physical examination reveals a well-nourished man.
The finding from head and neck, cardiopulmonary, and neurologic examinations are Unremarkable.
Examination of the abdomen reveals an obese abdomen without tenderness or Palpable masses .
The rectal examination reveals no masses , a smooth enlarged prostate
Strongly hemoccult positive stool in the vault .
Cbc : hb of 8.7 g/dl hct 29 % and low mcv .
Ecg : normal sinus rhythm and mild lvh.
Normal chest radiograph.

What is the most likely mechanism causing this process?
How would you confirm the diagnosis ?
What is the initial treatment for this pt ?

Most likely mechanism: anemia caused by occult GI tract bleeding .
Confirmation of the diagnosis : EGD and colonscopy.
Initial treatment: blood transfusion.

Epidemiology:
Approximately 148,810 new cases of large bowel cancer are diagnosed each year in the United States, of which 108,070 are colon and the remainder rectal cancers.
Annually, approximately 49,960 Americans die of CRC, accounting for approximately 9 percent of all cancer deaths.
Incidence
Age is a major risk factor for sporadic CRC. It is a rare diagnosis before the age of 40, the incidence begins to increase significantly between the ages of 40 and 50, and age-specific incidence rates increase in each succeeding decade thereafter).

The lifetime incidence of CRC in patients at average risk is about 5 percent, with 90 percent of cases occurring after age 50.
The incidence is higher in patients with specific inherited conditions that predispose them to the development of CRC.

A gradual shift toward right-sided or proximal colon cancers has been observed both in the United States and internationally.
The greatest increase in incidence is in cecal primaries.
why this changes?
This change in the anatomic distribution of CRCs may be, in part, related to improvements in diagnosis and treatment.
and increased screening by flexible sigmoidoscopy with removal of adenomatous polyps in the descending colon .
but there also appears to be a true increase in the incidence of ascending colon and cecal cancers .
Consistent with this hypothesis, five-year survival rates have improved significantly for left and transverse colon cancers, but not for right-sided tumor.

Risk factors :
Environmental and genetic factors can increase the likelihood of developing CRC.
Although inherited susceptibility results in the most striking increases in risk.
the majority of CRCs are sporadic rather than familial .

Personal or family history of sporadic cancers or adenomatous polyps — Patients with a personal history of CRC or adenomatous polyps are at risk for the development of a future large bowel cancer
FAP
Hereditary nonpolyposis colorectal cancer
A personal history of large (>1 cm) adenomatous polyps and polyps with villous or tubulovillous histology also increase the risk of CRC, particularly if multiple . The relative risk ranges from approximately 3.5 to 6.5 in such patients

Family history is also an important risk factor in sporadic disease, with a single affected first-degree relative (parent, sibling, or child) increasing the risk 1.7-fold of that in the general population
A family history of a large (>1 cm) or histologically advanced colonic adenoma appears to carry the same significance as a positive family history of colorectal cancer

Inflammatory bowel disease
Diabetes mellitus and insulin resistance obesity
Cholecystectomy - Alcohol
A history of radiation therapy for prostate cancer was associated with an increased risk of rectal cancer in a large database study . The magnitude of risk was similar to that observed in patients with a family history of colonic adenomas

protective factors
Diet
Fiber
Calcium supplementation has been recommended for the primary or secondary prevention of colonic adenomas by the American College of Gastroenterology
Aspirin and NSAIDs
Hormone replacement therapy

Omega 3 fatty acids — Consumption of omega 3 fatty acids (mainly as fish oil) has been associated with a reduced incidence of colorectal cancer in observational studies
Screening:
Patient surveillance can most effectively be accomplished by colonoscopy.
For average risk individuals ACG colonoscopy every 10 years beginning at 50 years of age .
If adenomatous polyp is identified and removed repeat colonoscopy should be done every 3 years when the colon is clear every 5 years .
What if he has high risk factor , eg early family history ?
Clinical presentations:
• Abdominal pain — 44 percent
• Change in bowel habit — 43 percent
• Hematochezia or melena — 40 percent
• Weakness — 20 percent
• Anemia without other gastrointestinal symptoms — 11 percent
Weight loss — 6 percent

A meta-analysis of 15 studies concluded that the sensitivity of alarm features (such as weight loss) was poor (ranging from 5 to 64 percent).
However, the specificity for some alarm symptoms (including dark red rectal bleeding and abdominal mass) was greater than 95 percent.

Abdominal pain can be caused by a partial obstruction, peritoneal dissemination, or intestinal perforation leading to generalized peritonitis.
tenesmus caused by a rectal cancer may involve pelvic floor muscles.
a locally advanced lesion may involve the sciatic or obturator nerve, leading to a neuropathic pain syndrome
Hematochezia is more often caused by a rectal rather than colon cancer
A change in bowel habits is a more common presenting symptom for left-sided cancers because fecal contents are liquid in the proximal colon and are therefore less likely to be associated with obstructive symptoms
Metastatic disease — Approximately 20 percent of patients have distant metastatic disease at the time of presentation
The presence of right upper quadrant pain, abdominal distention, early satiety, supraclavicular adenopathy, or periumbilical nodules usually signals advanced disease.

Because the venous drainage of the intestinal tract is via the portal system, the first site of hematogenous dissemination is usually liver
tumors arising in the distal rectum may metastasize initially to the lungs because the inferior rectal vein drains into the inferior vena cava rather than into the portal venous system.

Unusual presentations — There are also a variety of unusual presentations of CRC. These include:
Local invasion or a contained perforation causing malignant fistula formation into adjacent organs
Fever of unknown origin
CRC ultimately proves to be the origin of approximately 6 percent of adenocarcinomas of unknown primary sites
Impact of symptoms on prognosis
— The presence of symptoms and their particular type appear to be of some prognostic importance:
• Patients who are symptomatic at diagnosis have a somewhat worse prognosis . In one report, the five-year survival rate for symptomatic and asymptomatic patients was 49 versus 71 percent.
the duration of symptoms is not an accurate predictor of prognosis.

• Obstruction and/or perforation, although uncommon, carry a poor prognosis, independent of stage .
• Tumors presenting with hemorrhage have been thought to have a better prognosis because of their tendency to be diagnosed earlier; however, bleeding is not an independent predictor of outcome .

LOCATION OF COLORECTAL MALIGNANCIES
Synchronous cancers — Synchronous CRCs:
defined as two or more distinct primary tumors separated by normal bowel and not due to direct extension or metastasis, occur in 3 to 5 percent of patients with colon cancer
Metachronous cancers :
Metachronous CRCs, defined as nonanastomotic new tumors developing at least six months after the initial diagnosis.
develop in 1.5 to 3 percent of patients in the first five years postoperatively, rising to up to 9 percent after several decades in survivors of the primary cancer

DIAGNOSIS
CRC may be suspected from one or more of the symptoms and signs described above or may be asymptomatic and discovered by routine screening of average and high risk subject
Colonoscopy and BE
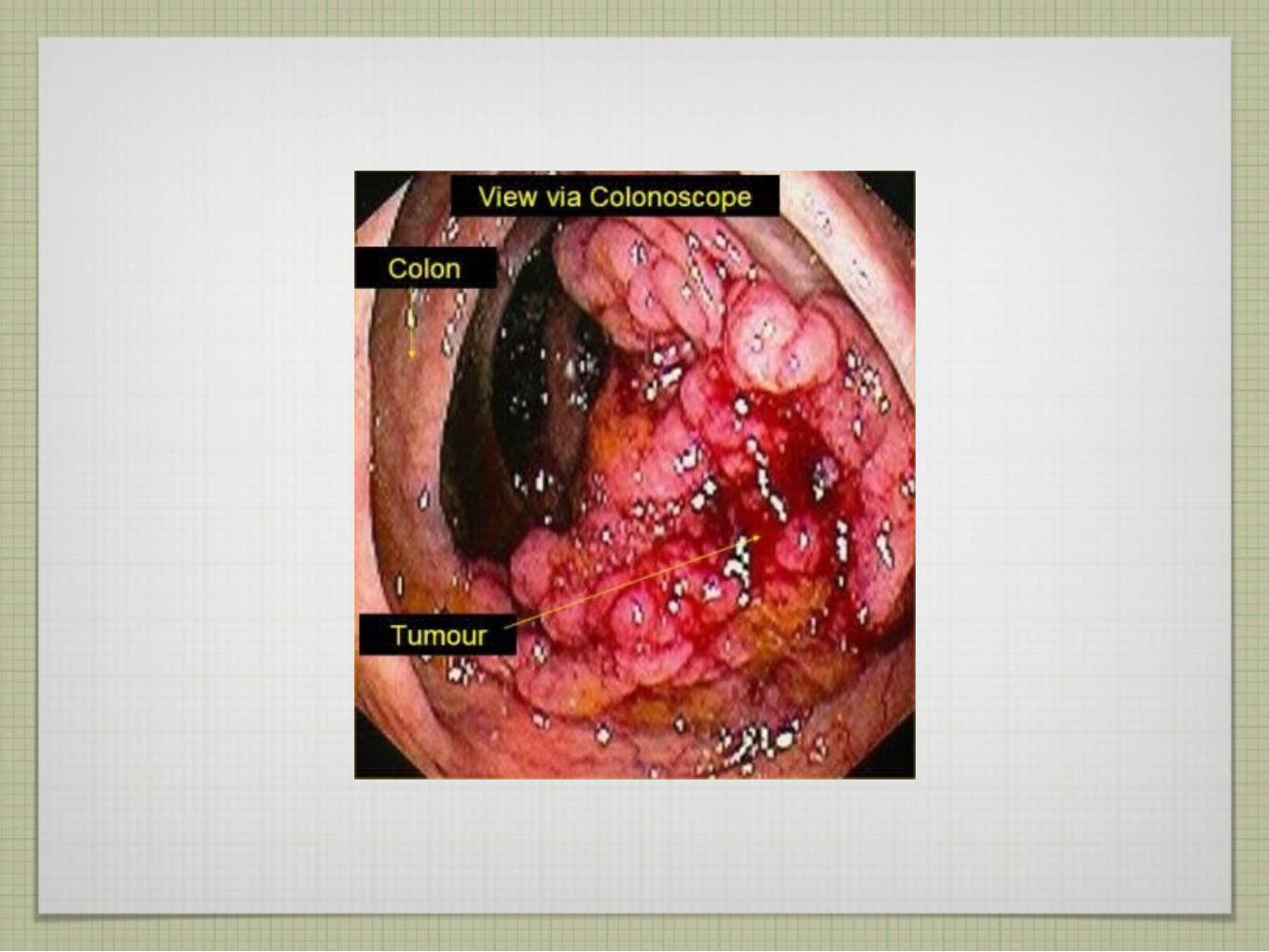
The vast majority of colon and rectal cancers are endoluminal adenocarcinomas that arise from the mucosa. Colonoscopy is the single best diagnostic test in symptomatic individuals, since it can localize lesions throughout the large bowel, biopsy mass lesions, detect synchronous neoplasms, and remove polyps
The air contrast barium enema (BE), supplemented with flexible sigmoidoscopy, is also used to evaluate symptomatic patients

A direct evaluation of the total colonic mucosa is necessary to exclude carcinoma with certainty
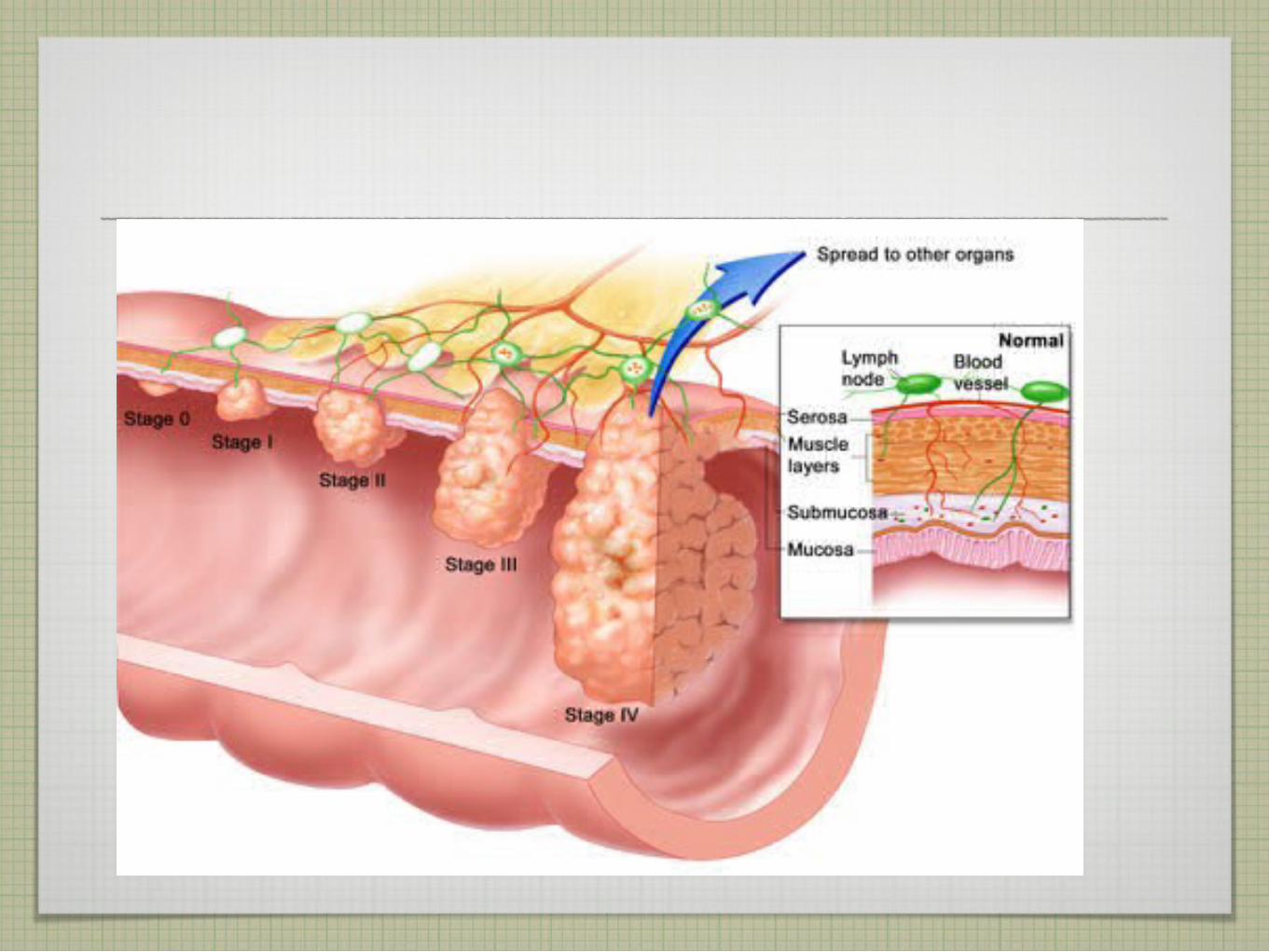
staging
Tx: No description of the tumor's extent is possible because of incomplete information.
Tis: The cancer is in the earliest stage. It involves only the mucosa. It has not grown beyond the muscularis mucosa (inner muscle layer).
T1: The cancer has grown through the muscularis mucosa and extends into the submucosa.
T2: The cancer has grown through the submucosa and extends into the muscularis propria (outer muscle layer).

T3: The cancer has grown through the muscularis propria and into the subserosa but not to any neighboring organs or tissues.
T4: The cancer has grown through the wall of the colon or rectum and into nearby tissues or organs.
N categories for colorectal cancer
N categories indicate whether or not the cancer has spread to nearby lymph nodes and, if so, how many lymph nodes are involved.
Nx: No description of lymph node involvement is possible because of incomplete information.
N0: No lymph node involvement is found.
N1: Cancer cells found in 1 to 3 nearby lymph nodes.
N2: Cancer cells found in 4 or more nearby lymph nodes.
M categories for colorectal cancer
M categories indicate whether or not the cancer has spread to distant organs, such as the liver, lungs, or distant lymph nodes.
Mx: No description of distant spread is possible because of incomplete information.
M0: No distant spread is seen.
M1: Distant spread is present.
Stage 0
Tis, N0, M0: The cancer is in the earliest stage. It has not grown beyond the inner layer (mucosa) of the colon or rectum. This stage is also known as carcinoma in situ or intramucosal carcinoma.
Stage I
T1, N0, M0 or T2, N0, M0: The cancer has grown through the muscularis mucosa into the submucosa (T1) or it may also have grown into the muscularis propria (T2). It has not spread to nearby lymph nodes or distant sites.
Stage IIA
T3, N0, M0: The cancer has grown into the outermost layers of the colon or rectum but has not reached nearby organs. It has not yet spread to the nearby lymph nodes or distant sites.
Stage IIB
T4, N0, M0: The cancer has grown through the wall of the colon or rectum and into other nearby tissues or organs. It has not yet spread to the nearby lymph nodes or distant sites.
Stage IIIA
T1, N1, M0 or T2, N1, M0: The cancer has grown through the mucosa into the submucosa (T1) or it may also have grown into the muscularis propria (T2). It has spread to 1 to 3 nearby lymph nodes but not to distant sites.
Stage IIIB
T3, N1, M0 or T4, N1, M0: The cancer has grown into the outermost layers of the colon or rectum but has not reached nearby organs (T3) or the cancer has grown through the wall of the colon or rectum and into other nearby tissues or organs (T4). It has spread to 1 to 3 nearby lymph nodes but not distant sites.

Stage IIIC
Any T, N2, M0: The cancer may or may not have grown through the wall of the colon or rectum, but it has spread to 4 or more nearby lymph nodes. It has not spread to distant sites.
Stage IV
Any T, Any N, M1: The cancer may or may not have grown through the wall of the colon or rectum, and it may or may not have spread to nearby lymph nodes. It has spread to distant sites such as the liver, lung, peritoneum (the membrane lining the abdominal cavity), or ovary.

An increase in colorectal cancer screening has been associated with an earlier stage at which colorectal cancer is diagnosed. The following results were observed in a large database study
• Localized — confined to the primary site and to the mucosa, submucosa, and muscle layer (Dukes' A or B or TNM stage I or II ) — 40 percent
• Lymph node involvement (Dukes' C or TNM stage III) — 37 percent
• Distant metastases (Dukes' D or TNM stage IV) — 19 percent
As a general rule, the stage of rectal cancer at diagnosis tends to be slightly earlier than the stage in the colon probably because rectal cancers are more likely to cause symptoms.
In patients with four or fewer hepatic lesions, resection may be curative, with five-year relapse-free survival rates of 24 to 38 percent
Intraoperative evaluation — Even if preoperative clinical staging evaluation fails to show evidence of metastatic spread.
intraoperative evaluation is an essential component of the clinical staging process.
CT scan is not a reliable diagnostic test for low volume tumor on peritoneal surfaces.

EUS for rectal cancer — Preoperative knowledge of the depth of invasion and nodal status is critically important for planning therapy of a rectal cancer.
Neoadjuvant combined modality approaches utilizing both chemotherapy and radiation are associated with less toxicity and a higher likelihood of sphincter preservation, particularly for distal transmural tumors.

Tumor markers :
An expert panel on tumor markers in breast and colorectal cancer convened by the American Society of Clinical Oncology (ASCO) recommended that serum CEA nor CA 19-9 levels not be used as a screening test for colorectal cancer . A similar recommendation has been made by the European Group on Tumor Markers .
However, serum levels of CEA do have prognostic utility in patients with newly diagnosed CRC. Patients with preoperative serum CEA >5 ng/mL have a worse prognosis, stage for stage, than those with lower levels

PROGNOSIS :
Colon cancer — Five-year survival rates in a contemporary series of over 119,000 patients treated between 1991 and 2000 stratified according to the most recent modification of the TNM staging system were as follows:
• Stage I (T1-2N0) — 93 percent
• Stage IIA (T3N0) — 85 percent
• Stage IIB (T4N0) — 72 percent
• Stage IIIA (T1-2 N1)— 83 percent
• Stage IIIB (T3-4 N1) — 64 percent
• Stage IIIC (N2) — 44 percent
Stage IV — 8 percent

Survival rates in patients with stage II and III disease are variable and depend on the number of lymph nodes analyzed .
Rectal cancer — Five-year survival rates for rectal cancer tend to be somewhat lower and are heavily dependent upon case mix .
In particular, the survival of patients with stage III disease is variable and depends upon the T stage (ie, T1-2 versus 3-4) and the extent of nodal disease. As an example, when data from the National Cancer Database were stratified according to subsets of stage III disease, the following five-year survival rates were reported :

• Stage IIIA (T1-2, N1) — 55.1 percent (n = 1043 patients)
• Stage IIIB (T3-4, N1) — 35.3 percent (n = 2856 patients)
• Stage IIIC (Any T, N2) — 24.5 percent (n = 2088 patients)
Surgical management of primary colon cancer
Surgery is the only curative modality for localized colon cancer. Surgery also provides a potentially curative option for selected patients with limited metastatic disease in liver and/or lung.
PREOPERATIVE EVALUATION :
A complete history and physical examination should be performed in all patients presenting with a newly diagnosed colon cancer
The preoperative evaluation should also include a complete blood count, serum electrolytes, liver enzymes, and carcinoembryonic antigen (CEA), urinalysis, coagulation profile, electrocardiogram, chest x-ray, and computed tomography (CT) scan of the abdomen and pelvis
Ideally, each patient should have a colonoscopic examination of the entire colon prior to surgery.

Endoscopic ultrasound — Endoscopic ultrasound (EUS) is not routinely used in the preoperative or staging workup of colon cancer (in contrast to rectal cancer, where it is routinely used).

GENERAL SURGICAL PRINCIPLES
The goal of colon cancer surgery is complete removal of the tumor along with the major vascular pedicle feeding the affected colonic segment and the lymphatic drainage basin
En bloc resection of contiguous structures is indicated if there is attachment or adhesion of the tumor to any organ or structure.
Bowel preparation
Preoperative mechanical bowel preparation (MBP) reduces both the fecal content and bacterial count in the bowel lumen . The use of MBP in conjunction with prophylactic antibiotics has been reported to decrease the incidence of wound infection and intraabdominal abscess after colorectal surgery .
Some have questioned the need for routine MBP prior to elective colon cancer surgery.

In an early systematic review of randomized trials of preoperative MBP versus no MBP in 1592 patients (nine trials) undergoing elective colorectal surgery, there was no significant difference in the anastomotic leakage rate between patients who had versus did not have MBP (2.9 versus 1.6 percent, respectively) .
Furthermore, there was a nonsignificant trend toward a higher incidence of wound infection in patients who received MBP (7.4 versus 5.4 percent).
Resection margins — Proximal and distal resection margins should be at least 5 cm from the tumor .
Regional lymphadenectomy — Regional lymphadenectomy provides important prognostic information that guides adjuvant treatment and is of therapeutic value as well.
SURGICAL TECHNIQUES
Right hemicolectomy : A right hemicolectomy is usually performed for tumors of the cecum and ascending colon, and for some hepatic flexure. In a classic right hemicolectomy, the ileocolic, right colic, and right branch of the middle colic vessels are divided and removed with the contiguous mesentery.
Care must be taken to identify the right ureter, the ovarian or testicular vessels, and the duodenum. If the omentum is attached to the tumor, it should be removed en bloc with the specimen.
Extended right hemicolectomy
An extended right hemicolectomy can be performed for proximal, mid, or even distal transverse colon cancers, although tumors of the distal transverse colon are more often resected with a left hemicolectomy.
In the extended right hemicolectomy, the ileocolic, right colic, and middle colic vessels with their contiguous mesentery are divided and removed. The inferior mesenteric vein may be divided and included in the specimen. Care must be taken to protect the duodenum and the pancreas

Transverse colectomy
A transverse colectomy may be undertaken for mid transverse colon cancers as long as satisfactory resection margins and an adequate lymphadenectomy can be obtained. The transverse colon is resected along with the middle colic vessels and its mesentery. At times, the inferior mesenteric vein is also divided and included in the resected specimen. Both the hepatic and splenic flexures may need to be mobilized in order to achieve a tension-free anastomosis. When mobilizing the splenic flexure, care must be taken not to apply much traction to the omentum or colon, as this will invariably result in splenic capsule tears.
Left hemicolectomy
A left hemicolectomy is appropriate for tumors in the distal transverse or descending colon and for selected patients with proximal sigmoid colon cancer. The left branch of the middle colic vessels, the inferior mesenteric vein, and the left colic vessels along with their mesenteries are included with the specimen.
In some cases, a segmental colectomy may be performed as long as adequate resection margins and lymphadenectomy are achieved .
Sigmoid colectomy
For sigmoid colon cancers, segmental or sigmoid colectomy is appropriate. The inferior mesenteric artery is divided at its origin, and dissection proceeds just under the superior rectal vessels toward the pelvis until adequate margins are obtained.
As with right-sided tumors, care must be taken while mobilizing the sigmoid and descending colon to identify the left ureter and the left ovarian or testicular vessels.

Subtotal and total colectomy
A subtotal or a total abdominal colectomy is indicated if there are synchronous neoplasms on the right and left sides of the colon. Occasionally these procedures are performed in patients presenting with obstructing-left sided tumors.
For patients with hereditary nonpolyposis colorectal cancer (HNPCC) who present with a colon cancer, total abdominal colectomy is the procedure of choice. .

Locally advanced primary lesions — Approximately 10 percent of patients with colon cancer have invasion of contiguous organs or inflammatory adhesions involving neighboring structures

Benefit of postoperative RT
There is a paucity of high-quality evidence addressing the role of adjuvant RT (with or without concurrent chemotherapy) in patients with resected locally advanced colon cancer
current treatment recommendations suggest that adjuvant RT be offered to the following subgroups of patients who have an estimated risk of local recurrence that is 30 percent or higher: T4 disease, positive resection margins, disease complicated by perforation or abscess formation
Neoadjuvant chemoradiotherapy
Neoadjuvant (preoperative) chemoradiotherapy may represent an alternative approach for selected patients with locally advanced colon cancer invading into adjacent organs. However, there is no consensus as to which patients are suitable for this approach.
Although commonly used for locally advanced rectal cancers.
patients with obstruction
Optimal management for an obstructing cancer depends upon the condition of the patient and the tumor location.
If the patient is a candidate for surgery, surgical treatment alternatives for obstructing colon cancers include resection of the tumor with a primary anastomosis with or without a temporary proximal diversion, resection without an anastomosis and with an end colostomy, and proximal diversion with a mucous fistula or a loop colostomy, to temporize the situation with an elective definitive resection at a second operation
patients with perforation
The management of perforated tumors has to be individualized. Treatment alternatives will depend on the patient's overall condition and whether peritonitis is localized or generalized. If the patient is stable and peritonitis is not generalized, tumor resection with a primary anastomosis can be performed.
As noted above, primary anastomosis is not recommended if there is diffuse peritonitis or free perforation and/or the patient is medically unstable.

For an unstable patient, percutaneous drainage or a proximal diverting colostomy can be performed.
Chemotherapy — Obstructed and perforated colon cancers are considered at high risk for recurrence. Guidelines from ASCO suggest the use of adjuvant chemotherapy in these settings, even for node-negative disease.

LAPAROSCOPIC COLECTOMY
Laparoscopic-assisted colectomy (LAC) was first described in 1991 . However, because of concerns over port site recurrences and the adequacy of the oncologic procedure, LAC was not accepted by the surgical community until the completion of multiple studies comparing safety and oncologic equivalency to open colectomy
At least six large (100 or more patients) prospective randomized controlled trials have now been reported, and none suggest a significant detrimental impact on recurrence or survival for laparoscopic as compared to open resection
In the earliest trial from Barcelona ( a median follow-up of 94 months, overall and disease-free survival were similar in both groups institution study),

In the largest trial, the United States Intergroup
At a median follow-up of seven years, there were also no significant differences in the five-year disease-free survival (69 versus 68 percent in the LAC and open colectomy groups, respectively) or overall survival (76 versus 75 percent).
Both concluded that laparoscopic colectomy provides oncologic outcomes (cause-specific survival, disease recurrence, number of lymph nodes harvested) that are comparable to those achieved with an open approach.

MANAGEMENT OF CARCINOMA IN A POLYP
Endoscopic resection alone is a reasonable approach for favorable-risk early stage colon cancers arising in a polyp. The presence of any of the following factors should prompt consideration of radical surgery, as they indicate a higher risk of residual cancer and/or nodal metastases:

• Poorly differentiated histology
• Lymphovascular invasion
• Cancer at the resection or stalk margin
• Invasion into the muscularis propria of the bowel wall (T2 lesion)
• Invasive carcinoma arising in a sessile (flat) polyp
• Invasive carcinoma with incomplete polypectomy
• Lymphovascular invasion
• Cancer at the resection or stalk margin
• Invasion into the muscularis propria of the bowel wall (T2 lesion)
Surgical management of rectal cancer
Physical and endoscopic examination — Digital rectal examination (DRE) and rigid sigmoidoscopy are essential to the surgical decision-making process
The type of operation offered to a patient with rectal cancer depends on tumor stage and location
If sphincter preservation is to be achieved, the tumor has to be located high enough above the top of the anorectal ring to allow for an adequate distal margin.
This is more likely with midrectal and upper rectal tumors than for distal tumors (within 5 cm of the anal verge),
although preoperative chemoradiotherapy may permit sphincter preservation in some patients with low-lying tumors.

GENERAL SURGICAL PRINCIPLES
After establishing the diagnosis and completing the staging workup, a decision is made whether to pursue immediate resection or attempt preoperative chemoradiotherapy .
The benefits of preoperative chemoradiotherapy were best demonstrated in the German Rectal Cancer Study Group trial that randomly assigned 823 patients with rectal cancer to preoperative versus postoperative chemoradiotherapy .
The following results were noted:
• Patients treated preoperatively had similar survival rates but a significantly lower pelvic relapse rate compared to those receiving postoperative chemoradiotherapy.
Overall rates of sphincter preservation were similar in both groups (APR required by 26 and 23 percent of preoperatively and postoperatively treated patient.
Goals of surgery:
The primary goal of surgery is complete removal of the primary tumor along with the regional lymphatics and the superior hemorrhoidal artery pedicle. The surgical specimen should contain at least 12 lymph nodes

SELECTION OF APPROPRIATE SURGERY
The surgeon has three major curative options for rectal cancer: local excision, sphincter-preserving abdominal surgery (low anterior resection or LAR), and abdominal perineal resection (APR).
The depth of tumor invasion into the rectal wall, the presence or absence of regional lymph node metastases, the size and macroscopic appearance of the cancer, and tumor location are all critical in determining the best surgical option
Abdominal perineal resection (APR):
An APR requires incisions in both the abdomen and perineum. It entails removal of the primary tumor along with a complete proctectomy, resulting in the need for a permanent colostomy.
APR has long been considered the gold standard for surgical therapy of distal rectal cancers.
Oncologic outcomes following LAR are not significantly different from those after APR .
However, compared to LAR, APR is associated with higher procedure-related morbidity and mortality . and an inferior quality of life (QOL), mainly related to depression and changes in body image .

Sphincter-sparing procedures : Sphincter-sparing approaches for distal rectal cancers have evolved along two
pathways:
For larger or more invasive tumors of the distal rectum (eg, T3 or T4 lesions), preoperative or neoadjuvant chemoradiotherapy may facilitate the conversion of a planned APR to a LAR by promoting tumor regression
For small rectal cancers that are confined to the rectal wall, local excision techniques may offer local control and survival rates that are comparable to APR, while preserving sphincter function
Low anterior resection — Most invasive rectal cancers involving the upper third of the rectum can be adequately treated by a LAR, preserving the anal sphincter.
Even for patients with midrectal and some distal (lower third) rectal cancers, LAR has become increasingly prevalent as the safety and efficacy has been established
THANK YOU Dr. Ryan Al.Ghanemi























