Embed Size (px)
Citation preview

CO-OCCURRENCE OF DEVELOPMENTALDISABILITIES WITH BIRTH DEFECTS
Russell S. Kirby*Department of Obstetrics and Gynecology, Milwaukee Clinical Campus, University of Wisconsin Medical School
This article begins with a discussion of the concepts of comorbidityand co-occurrence of diseases and health conditions. These concepts arethen applied to the literature on the population-based prevalence of devel-opmental disabilities and birth defects. Most of the existing literature fo-cuses on co-occurrence and obtains data from both clinical and administra-tive sources. Developmental disabilities occur more frequently in childrenwith multiple, rather than with isolated, birth defects. More research, withmore sophisticated study designs, will be necessary to further elucidate thecontributions of birth defects to the etiology of developmental disabilities,control for other risk factors, and to identify strategies for prevention andintervention services. © 2002 Wiley-Liss, Inc.MRDD Research Reviews 2002;8:182–187.
Key Words: comorbidity; co-occurrence; epidemiology; birth defects; de-velopmental disabilities
The etiologies of many common developmental disabili-ties are incompletely understood. By studying environ-mental, behavioral, reproductive, and demographic risk
factors among children with a single developmental disorder, incomparison to those with several disabilities or other illnessesand health conditions, researchers may identify etiologic cluesthat facilitate health promotion and primary or secondary pre-vention strategies.
For this article, we reviewed the literature conceptualizingcomorbidity of diseases and health conditions and studies thatapply operational definitions of comorbidity to analyses of ad-ministrative databases, in general, and specifically to pediatrichealth conditions. Population-based studies and clinical caseseries of selected developmental disabilities were examined toidentify findings with a bearing on the issue of comorbidity orco-occurrence with other disabilities and with birth defects. Weconclude with some suggestions for an agenda for future epide-miologic and preventive medicine research into the comorbidityof birth defects and developmental disabilities.
COMORBIDITYCo-occurrence or comorbidity of diseases or health con-
ditions is a rapidly evolving area of research. Unfortunately,many studies lack clarity in their conceptualization of the term“comorbidity” and its formal operationalization in the empiricalcontext. Kraemer identifies three distinct types of comorbidity:epidemiologic, clinical, and familial [Kraemer, 1995]. Clinicalcomorbidity refers to the co-occurrence of other diseases orhealth conditions in individuals with the health condition ofinterest and the differential prognosis these patients have com-
pared to those without other disorders. Clinical comorbidity hasbeen further categorized into the pathogenic, diagnostic, andprognostic with respect to the effect of the comorbid conditionon the patient with the index condition [Feinstein, 1970].Epidemiologic comorbidity refers to the situation in which theprevalence of a comorbid condition differs between those withand without the health condition of interest. A primary differ-ence between epidemiologic and clinical comorbidity, then, isthe focus on groups of study subjects in the former while thelatter focuses on the characteristics of individual patients. It ispossible for epidemiologic comorbidity to exist in the presenceor absence of clinical comorbidity and for clinical comorbidityto be present without evidence of epidemiologic comorbidity.Familial comorbidity describes patterns of comorbidity amongrelatives of the index patient in the presence or absence of thehealth condition of interest. Again, familial comorbidity mayexist between a comorbid condition and the condition of in-terest in the presence or absence of epidemiologic or clinicalcomorbidity. It is also possible that the observed co-occurrenceof two or more disease processes or health conditions is arandom event with no epidemiologic, clinical, familial, or otherknown association to explain the observed pattern.
Researchers have not focused on the study of comorbidityin child or adolescent populations and have typically not appliedKraemer’s concepts of epidemiologic, clinical, and familial co-morbidity in their methodologies. Previous work has focusedlargely on mental health and psychosocial problems and espe-cially on diagnosis and treatment of children with comorbidmental health and chronic conditions [e.g., Sabbeth and Stein,1990; Canning et al., 1992; Canning, 1994]. Primary challengesin studying comorbidity among developmental disabilities inchildhood and birth defects are variability in diagnoses andlimitations deriving from methods of administrative documen-tation. Methodologies for the analysis of comorbidity are muchbetter developed for chronic diseases and diagnoses affectingadults. For example, Elixhauser et al. [1998] created a set of 30comorbidity measures from ICD-9-CM codes. These comor-
*Correspondence to: Dr. Kirby’s present address: Russell S. Kirby, Department ofMaternal and Child Health, School of Public Health, University of Alabama atBirmingham, 320 Ryals Bldg., 1530 3rd Ave. S, Birmingham, AL 35294-0022.E-mail: [email protected] 21 May 2002; Accepted 23 May 2002Published online in Wiley InterScience (www.interscience.wiley.com).DOI: 10.1002/mrdd.10034
MENTAL RETARDATION AND DEVELOPMENTAL DISABILITIESRESEARCH REVIEWS 8: 182–187 (2002)
© 2002 Wiley-Liss, Inc.

bidities were defined as conditions notedon admission not directly related to theprimary reason for the hospitalization butincrease hospital resource use or likeli-hood of poor outcome. Using data fromthe statewide California hospital dis-charge data, the measures were statisti-cally validated. Unfortunately, this studyand others like it [Charlson et al., 1987;Romano et al., 1993] are of limited util-ity in the study of comorbidity in chil-dren with developmental disabilities.First, many of the comorbidities of inter-est are not adequately specified in codingsystems for administrative health data[Virnig and McBean, 2001]. Second,children with developmental disabilitiesmay require hospitalization only occa-sionally, and their disabilities may not benoted on the hospital discharge summary.Third, the outcomes of interest arebroader than those relating to intensity ofhealth care resource use or episode ofcare. Additionally, there are differing le-gal definitions for “special needs chil-dren” and “developmental disabilities”that focus on functional rather than clin-ical criteria, raising impediments to theidentification of children with develop-mental disabilities from clinical as well aseducational or service-based data sources.Pediatric disabilities do not equate withillness or use of health care services, butthese children may require greater re-sources for appropriate management oftheir disabilities.
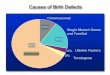
Vessey [1999] provides a usefulmodel for conceptualizing comorbidityin children with chronic conditions. Inthis model, the domains of developmen-tal delay, chronic illness, and mentalhealth concerns overlap, identifying areasof psychological comorbidity. Vesseydefines psychological comorbidity as a“mental health condition existing simul-taneously with an index chronic medicalcondition” [1999]. For thinking aboutcomorbidity in children with develop-mental disabilities, we might representthree overlapping domains of develop-mental disability, birth defects or sequelaeof fetal growth and development and ac-quired chronic illness (Fig. 1). Withineach domain, an infant or child may havea single diagnosis or health condition ormultiple diagnoses. For example, a childwith cerebral palsy may have no otherdisabilities or additional developmentalconditions such as epilepsy or sensoryimpairment. Children with developmen-tal disabilities may also have birth defectsand, again, these may be isolated or mul-tiple defects. Many children with devel-opmental disabilities also have significantchronic illnesses. The most complex
cases may be those infants or childrenwith birth defects, disabilities, and chronichealth conditions. In this review we ex-plore co-occurrences as a proxy for epide-miologic comorbidity within the domainof developmental disabilities and betweenthe domains of developmental disabilitiesand birth defects. Those interested in ex-ploring the relationship between chronicdisease and disabilities in children may wishto consult Newacheck and Taylor [1992].
A widely cited inventory of theprevalence of pediatric chronic illnessesand health conditions in the U.S. pre-sents no statistics concerning comorbidi-ties [Gortmaker and Sappenfield, 1984].Newacheck et al. [1998] used the 1994National Health Interview Survey onDisability to develop an epidemiologicprofile of children with special healthcare needs. While this study provides na-tional estimates by demographic charac-teristics and some health services mea-sures, there is no discussion ofcomorbidity across the domains ofchronic physical, developmental, behav-ioral, and emotional conditions. On theother hand, Boyle et al. [1994] used the1988 NHIS-Child Health Supplement tofocus on the epidemiology of develop-mental disabilities. Their results showthat children with multiple disabilities aremore likely to have fair or poor healthstatus, poor performance in school, andmore physician and hospital visits thanchildren with no disabilities, with an ap-parent dose-response to the number ofdisabilities children have.
Our knowledge of the prevalence,correlates, and public health implicationsof comorbidities among children withdevelopmental disabilities is hindered bya lack of population-based surveillancedata concerning developmental disabili-ties. Boyle [1997] describes several ap-proaches to surveillance and makes astrong case for its relevance to those re-
searching the etiology of developmentaldisorders. There are relatively few at-tempts at comprehensive, population-based surveillance of developmental dis-abilities in childhood in the U.S. Theseinclude the metropolitan Atlanta pro-gram [Yeargin-Allsopp et al., 1992; De-coufle et al., 1995] and a demonstrationproject conducted in Arkansas during theearly 1990s, [Kirby et al., 1995; Brewsteret al., 1998]. Surveillance activities inother countries have typically focused onspecific types of developmental disabilityand emphasized classification of etiolo-gies; these studies include western Aus-tralia [Wellesley et al., 1991; 1992],France [Rumeau-Rouquette et al.,1992], and northern Finland [von Wendtet al., 1985; Louhiala, 1995], among oth-ers. Other studies have focused on a spe-cific type of developmental disability,with examples being cerebral palsy [Gre-ther et al., 1992], mental retardation[Rantakaillo and von Wendt, 1986;McLaren and Bryson, 1987; McDermottet al., 1993], and epilepsy and seizuredisorders [Cowan et al., 1989].
Co-Occurrence of DevelopmentalDisabilities
Two projects conducted in themetropolitan Atlanta region focused onco-occurrence of mental retardation;cerebral palsy; hearing and vision impair-ments; and, in one of the projects, epi-lepsy. The Metropolitan Atlanta Devel-opmental Disabilities Study (MADDS)focused on children at the age of 10during 1985–1987 [Murphy et al., 1993;Murphy et al., 1995a,b; Drews et al.,1995). Co-occurrence of developmentaldisabilities varied across the five catego-ries studied. Three-fourths of cases ofcerebral palsy had at least one other dis-ability, with MR (mental retardation)and epilepsy most commonly co-occur-ring [Murphy et al., 1993], while approx-
Fig. 1. Conceptual model of the overlapping domains of developmental disabilities, birth defects,and chronic illnesses.
183MRDD RESEARCH REVIEWS ● DEVELOPMENTAL DISABILITIES AND BIRTH DEFECTS ● KIRBY

imately one-third of cases of epilepsy hadMR, CP (cerebral palsy), VI (visual im-pairment), or HI (hearing impairment),with 30% co-occurrence between epi-lepsy and MR and higher rates of co-occurrence among children with gener-alized or unclassified seizures [Murphy etal., 1995b]. In a study of a Finnish birthcohort, von Wendt et al. [1985] foundthat 35.5% of children with epilepsy hadone or more other major developmentaldisabilities. Only 22% of children withMR had other developmental disabilities[Murphy et al., 1995a], and a case-con-trol study examining the role of maternaleducation as a risk factor for MR found astrong, inverse association betweenmaternal education and MR onlyamong children with forms of MR notaccompanied by other serious neurolog-ical conditions [Decoufle and Boyle,1995]. A related study found evidencesuggesting a socioeconomic gradientboth for isolated MR and for MR withother neurological conditions [Drews etal., 1995]. Vision and hearing impair-ment also co-occur with other develop-mental disabilities. MR was the mostcommonly co-occurring developmentaldisability with hearing impairment (21%)[Drews et al., 1994]. Co-occurrence wasmore common among children with le-gal blindness (66%); 40% of cases had atleast two other disabilities with MR oc-curring more frequently in combinationwith another disability [Drews et al.,1992].
The Metropolitan Atlanta Devel-opmental Disabilities Surveillance Pro-gram (MADDSP) focused on childrenages 3–10 during calendar year 1991,with surveillance ongoing since thatyear [Boyle et al., 1996]. This studyreports similar findings concerning co-occurrence of developmental disabili-ties, with 22% of MR cases having aco-occurring condition, primarily CP;66% of CP cases (64% MR, 17% VI);23% of HI cases (20% MR); and 73% ofVI cases (69% MR). These findingssuggest that studies of comorbidity be-tween birth defects and developmentaldisabilities should examine differentialpatterns of risk and comorbidity amongchildren with isolated and multiple dis-abilities. One avenue explored withdata from this surveillance system is thecontribution of postnatal causes to theprevalence of developmental disabili-ties [CDC, 1996b], while another is thecomorbidity of developmental disabili-ties in children with sickle cell disease[Ashley-Koch et al., 2001].
Co-Occurrence of Birth Defectsand Developmental Disabilities
Population-based studies of the co-occurrence and comorbidity of develop-mental disabilities and birth defects areinfrequent, in part because there are fewdisabilities surveillance programs con-ducted for populations for which there isalso a birth defects surveillance program.When both exist, it is possible to linkrecords to birth certificates, creating adatabase from which prevalence ratioscan be calculated and case-control studydesigns can be implemented. Generally,however, these studies have focused onco-occurrence of birth defects and devel-opmental disabilities. Drews et al. [1992]studied the 62 cases of legal blindness in10-year-old children in the Atlanta area,using data from the Metropolitan AtlantaCongenital Defects Program (MACDP)in conjunction with the MADDS data-base, and found that 34.5% had birthdefects or genetic conditions associatedwith their visual impairment. Wellesleyet al. [1991] conducted a population-based study of intellectual disabilities inchildren at the ages of 6, 10, and 16 inwestern Australia. When classified by eti-ology, 61% had prenatal origins with 40%of the total genetic and an additional15% of unknown genetic etiology. Fullyone-fifth (21%) of cases had unknownetiologies.
Brewster et al. [1992] used datafrom a birth defects surveillance programto estimate the prevalence of mental re-tardation in public schools. A develop-mental pediatrician and a geneticist inde-pendently estimated the probability ofmental retardation for each specific birthdefect, and these probabilities were ap-plied to the distribution of observed birthdefects, adjusting for mortality. Thestudy suggested that 32%–56% of thecases of mental retardation reported inthe public schools may be due to birthdefects.
Decoufle et al. [2001] linkedrecords from MACDP [Edmonds et al.,1979; James et al., 1995] to data from theMADDSP program described above[Boyle et al., 1996]. Using presence ofdiagnosed birth defects as the startingpoint, prevalence ratios for MR, CP, HI,and VI among 3–10-year-old children inthe Atlanta area with major birth defectsduring 1991–1994. Children born withmajor birth defects had a serious DD(deveopmental diability) prevalence of7.2% compared to 0.9% in children withno major birth defects (prevalence ratioor ratio of prevalence in children with tochildren without major birth defects of8.3 (95% C.I. 7.6–9.0). Children with
isolated birth defects had a lower preva-lence ratio for DD (5.1; 95% C.I. 4.6–5.7). Prevalence ratios also varied mark-edly by birth defect category and werehighest for chromosomal abnormalities,CNS (central nervous system) defects,and defects of the eye and ear. Amongchildren with isolated birth defects, theprevalence ratio for VI was highest(10.2). Prevalence ratios for any DD in-creased monotonically by number ofbirth defects reported and across catego-ries of birth defects by specific DD andfor children with birth defects in three ormore different categories the prevalenceratio for DD was 15.0 (95% C.I. 10.1–22.2).
While this study points the waytoward integrating birth defects anddevelopmental disabilities, the authorsidentify several significant limitations thatwill also affect similar studies in othersettings. By their design, population-based surveillance of both birth defectsand developmental disabilities are of ne-cessity retrospective. Although the finaldata set has the look and feel of a studycohort, due to differential patterns of in-and out-migration, the actual study pop-ulation consists of those children born inthe region and diagnosed with develop-mental disabilities during 1991–1994, aswell as any children born in the regionand diagnosed with a birth defect, to-gether with infants born to residents ofthe region who may or may not stillreside in the region during 1991–1994.While researchers may make educatedguesses as to the net effects of migrationand variable ascertainment of develop-mental disabilities, at present, we do notknow the answer to the question of howthese factors influence the statistical find-ings. A stronger methodological ap-proach would be to identify a cohort ofinfants at birth, or shortly thereafter, andfollow the entire group with clinical ge-netics or developmental pediatric diag-nostic evaluations and then with periodicdevelopmental assessments or throughevaluation of special education adminis-trative records to a specified age, perhapsto the 11th birthday. Only through astudy of this nature could the antecedent-consequent relationship be fully evalu-ated. A study of this nature would bevery expensive, time-consuming, andfraught with logistical difficulties due toHealth Insurance Portability and Ac-countability Act (HIPAA) and FederalEducational Rights and Privacy Act(FERPA) regulations in the UnitedStates. These evolving administrativerules and operating procedures for healthcare and educational providers limit the
184 MRDD RESEARCH REVIEWS ● DEVELOPMENTAL DISABILITIES AND BIRTH DEFECTS ● KIRBY

use of patient- or student-identifiable in-formation and may render the collectionof population-based data for publichealth more difficult in the future [Gos-tin et al., 2001]. One potential setting fora study in the United States population isthe children of active-duty military per-sonnel and their families who receivetheir health services through definedhealth plans.
A population-based surveillancestudy in northwestern Arkansas exam-ined the co-occurrence of developmentaldisabilities in children with birth defectsand the rate of survival to the age of four[Kirby et al., 1995]. Approximately 25%of all children with diagnosed birth de-fects also had a developmental disabilitiesdiagnosis; it should be noted that thiscategory included a larger set of diagnosesthan those employed in the Atlanta stud-ies. By birth defect category, rates of co-occurrence among children surviving toage four ranged from 77% for CNS de-fects to 30% for musculoskeletal defects,with a lower rate (26%) among theheterogeneous “all other birth defects”category.
Croen et al. [2001a] used a case-control study design to examine the as-sociation between congenital anomaliesand cerebral palsy. Cases were identifiedfrom the California cerebral palsy project[Grether et al., 1992], and linked to theCalifornia birth defects registry. Unlikethe study of Decoufle et al. [2001], thisstudy estimates the risk of birth defectsamong children with cerebral palsy. Insingletons, the odds ratio for congenitalabnormalities in children with cerebralpalsy was 5.2 (95% C.I. 2.8– 9.7). Theassociation was stronger for structural ab-normalities of the central nervous sys-tem (OR�16.2, 95% C.I. 5.8–49.3). Bybirth weight, only among singleton birthsof 2500g or more was there an increasedrisk for birth defects among children withcerebral palsy.
In another recent study, Croen etal. [2001b] examined perinatal risk factorsassociated with mental retardation of un-known cause. Cases among childrenborn during 1987– 1994 were identifiedfrom service records and linked to birthcertificates. Among a total of 23,956cases of mental retardation, 11,114 hadno identifiable cause. Of those withdiagnosed causes, approximately 30% hadchromosomal or central nervous systemanomalies, and these constituted 30% ofcases of severe mental retardation and53% of cases of unspecified mental retar-dation. However, this study was notlinked to the state birth defects registryand shares the same limitations imparted
by the use of administrative records fromeducational and service agencies.
An area of growing interest is theepidemiology of autism and pervasivedevelopmental disorder, sometimes re-ferred to as autism spectrum disorder orASD. Here we briefly describe severalrecent studies that examine co-occur-rence of ASD, other developmental dis-abilities, and birth defects. Barton andVolkmar [1998] conducted a retrospec-tive review of a series of 211 patientswith autism, pervasive developmentaldisorder, and other developmental disor-ders. While these patients included someadults, the mean age of subjects withautism was 13.3�8.4 years. Among 68subjects with clinical diagnoses of autism,23 had observed medical conditions; 12(18%) had seizure disorders; and two hadconductive hearing loss. Comparison ofseveral diagnostic systems leads to theconclusion that the prevalence of medicalconditions with a suspected etiologicalassociation with autism is in the range of10%–15%. This study is limited both bythe relatively small series of autism casesand by not employing a case-controlstudy design. Chakrabarti and Fombonne[2001] conducted a population-basedsurvey in Staffordshire, England, to iden-tify children ages 2.5 to 6.5 with symp-toms suggestive of pervasive develop-mental disorder. This study, more oftencited for estimates of the prevalence ofautistic disorders, also has some data oncomorbidities. Of 97 children with ASD,eight had associated medical conditions,including abnormal karyotypes, cerebralpalsy, and tuberous sclerosis. ASD alsohas a large overlap with mental retarda-tion; 24 of the 97 subjects (25.8%) hadsome degree of mental retardation. Astudy of the prevalence of autism in BrickTownship, New Jersey [Bertrand et al.,2001], identified a total of 60 childrenwith ASD among 3–10-year-olds. Amonga subset of these cases, 9% had macro-cephaly, and 30% had dysmorphic fea-tures. Records were not linked to thestate birth defects registry, and while po-tential cases underwent clinical assess-ment by a multidisciplinary team, this didnot include an evaluation by a clinicalgeneticist.
To summarize this brief review ofrecent studies of the descriptive epidemi-ology of autism in pre-adolescent chil-dren, although autism has not commonlybeen included in population-based de-velopmental disabilities surveillance ac-tivities, its prevalence now appears largeenough to warrant inclusion in theseprograms. While autism and ASD posespecial problems for diagnosis, classifica-
tion, and determination of etiology, theseare similar to the problems involved inaccurately classifying seizure disordersand cerebral palsy, conditions often in-cluded in developmental disabilities sur-veillance programs. As innovations indiagnosis increase the likelihood of iden-tification of ASD in children prior to theage of three, it will become possible toidentify ASD in children during orshortly after the period of birth defectsascertainment used in many state pro-grams (generally through the first or sec-ond year of life). That should greatlyenhance our understanding of the co-occurrence of birth defects and ASD and,ultimately, the extent to which specificbirth defects and genetic disorders con-tribute, through natural history or incombination with life events, to theprevalence of ASD.
Defining a Research AgendaSeveral generalizations derive from
this brief review. First, in conceptualizingthe problem, researchers should discon-tinue the interchangeable use of the con-cepts of co-occurrence and comorbidityand differentiate between perinatal out-comes (including birth defects, congeni-tal infections, and trauma), postnatal eti-ologies, and the normative growth anddevelopment of children with specificbirth defects and genetic diseases. Most ofthe current literature examining co-oc-currence of various developmental dis-abilities or birth defects associated withspecific developmental disabilities couldbe improved by greater clarity of focus,especially with respect to incorporatingthe concept of epidemiologic comorbid-ity into the study designs. Second, we arestill grappling with the difficulties im-posed, on the one hand, by coding sys-tems for disease entities that lack thespecificity to identify and differentiatebetween disabilities and birth defects ashealth conditions and, on the other, by afunctional/educational classification forimpairments and handicaps that oftenmaps developmental disorders from acompletely different frame of reference.Third, until there is sufficient experiencewith developmental disabilities surveil-lance in the United States to determinethe most efficient and cost-effectivemethodologies for case ascertainment andmore ongoing surveillance programs, itwill be difficult to advance knowledge inthis area, other than from the handful ofexisting activities. The likelihood thatenvironmental factors play a significantrole in the etiology of developmental dis-orders cannot be underestimated, andthus it is difficult to generalize from the
185MRDD RESEARCH REVIEWS ● DEVELOPMENTAL DISABILITIES AND BIRTH DEFECTS ● KIRBY

studies in Atlanta, New Jersey, Califor-nia, and elsewhere to communitieswhere the prevalence of developmentaldisabilities has not been investigated.Fourth, in examining the association be-tween birth defects and developmentaldisabilities, we must decide which is as-sociated with which. Are birth defects arisk factor for developmental disability, inwhich case a cohort study design makesthe most sense, or should we employcase-control study designs to look retro-spectively at the likelihood that birthdefects occur more frequently amongchildren with specific developmental dis-abilities? To some extent, the answer liesin the underlying purpose of the researchproject. If the goal is to identify whichchildren are at greatest risk for adversedevelopmental outcomes so that theymight be offered the opportunity to par-ticipate in early intervention programs,the retrospective approach might makesense. However, because we know solittle about the prevalence of develop-mental outcomes and the extent towhich they are pediatric sequelae of peri-natal events, the prospective approachalso offers considerable appeal [Kirby,1999]. Finally, it is clear that a multidis-ciplinary approach is essential both in thestudy design and the execution of re-search projects in this field. Ideally weshould include social scientists, epidemi-ologists, developmental specialists from anumber of disciplines, and geneticists inour research teams.
The research agenda requires thesimultaneous surveillance of both birthdefects and developmental disabilities, ifnot by the same program, then at least forthe same target population, using popu-lation-based methods with a careful as-sessment of diagnostic information col-lected. Others have championed the callfor registers and registries [Johnson,1995; Johnson and King, 1999]; it is upto the public health surveillance commu-nity to demonstrate that this is an impor-tant, indeed an essential, public healthfunction where the health of the popu-lation outweighs individual concerns forprivacy and anonymity [Yasnoff et al.,2001; O’Brien and Yasnoff, 1999].However, it is not sufficient to studyco-occurrence and comorbidity; wemust also identify sociodemographic andenvironmental correlates of developmen-tal disabilities [e.g., Schendel et al.,1997], as well as opportunities for sec-ondary and tertiary prevention. Epidemi-ologic research should also link serviceprograms (i.e., Birth to Three, HeadStart, Children with Special Health CareNeeds) with developmental disabilities
and birth defects surveillance data in or-der to evaluate both the ability of theseprograms to find eligible children in needof services and the developmental andeducational outcomes of children whodo participate in these programs.
All in all, the field of developmen-tal disabilities surveillance is in its infancy,but there are exciting opportunities tocontribute to knowledge of etiology, co-morbidity, treatment, and outcomes. f
REFERENCESAshley-Koch A, Murphy CC, Khoury MJ, et al.
2001. Contribution of sickle cell disease tothe occurrence of developmental disabilities: apopulation-based study. Genetics in Medicine3:181–186.
Barton M, Volkmar F. 1998. How commonly areknown medical conditions associated withautism? J Autism Dev Disord 28:273–278.
Bertrand J, Mars A, Boyle C, et al. 2001. Preva-lence of autism in a United States population:the Brick township, New Jersey investigation.Pediatrics 108:1155–1161.
Boyle CA, Decoufle P, Yeargin-Allsopp M. 1994.Prevalence and health impact of developmen-tal disabilities in US children. Pediatrics 93:399–403.
Boyle CA, Yeargin-Allsopp M, Doernberg NS, etal. 1996. Prevalence of selected developmen-tal disabilities in children 3–10 years of age:the metropolitan Atlanta developmental dis-abilities surveillance program, 1991. MorMortal Wkly Rep. CDC Surveill Summ 45:1–14.
Boyle CA. 1997. Surveillance of developmentaldisabilities with an emphasis on special stud-ies. Reprod Toxicol 11:271–274.
Brewster MA, Kirby RS, Cunniff CM, et al. 1992.Predicting needs for special education re-sources for mental retardation from birthdefects records. Public Health Reports 107:290–296.
Brewster MA, Kirby RS, Canino C. 1998. Finalreport: adverse reproductive outcomes in Pu-laski county for years 1980 through 1990,arkansas reproductive health monitoring sys-tem in collaboration with Arkansas Depart-ment of Health. Atlanta, GA: Agency forToxic Substances and Disease Registry,March.
Canning EH, Hanser SB, Shade KA, et al. 1992.Mental disorders in chronically ill children:parent-child discrepancy and physician iden-tification. Pediatrics 90:692–696.
Canning EH. 1994. Mental disorders in chronicallyill children: case identification and parent-child discrepancy. Psychosomatic Med 56:104–108.
Centers for Disease Control and Prevention.1996b. Postnatal causes of developmental dis-abilities in children aged 3–10 years—Atlanta,Georgia 1991. MMWR 45:130–136.
Chakrabarti S, Fombonne E. 2001. Pervasive de-velopmental disorders in preschool children.JAMA 285:3093–3099.
Charlson ME, Pompei P, Ales KL, et al. 1987. Anew method of classifying prognostic comor-bidity in longitudinal studies: Developmentand validation. J Chron Dis 40:373–383.
Cowan LD, Leviton A, Bodensteiner JB, et al.1989. Problems in estimating the prevalenceof epilepsy in children: the yield from differ-ent sources of information. Paediatr PerinatEpidemiol 3:386–401.
Croen LA, Grether JK, Curry CJ, et al. 2001a.Congenital abnormalities among childrenwith cerebral palsy: more evidence for prena-tal antecedents. J Pediatr 138:804–810.
Croen LA, Grether JK, Selvin S. 2001b. The epi-demiology of mental retardation of unknowncause. Pediatrics 107(6). URL: http://www.pediatrics.org/cgi/content/full/107/6/e86.
Decoufle P, Yeargin-Allsopp M, Boyle CA, et al.1995. Developmental disabilities. In: WilcoxLS, Marks JS, eds. From data to action:CDC’s public health surveillance for women,infants, and children. Atlanta: US DHHS.p 335–342.
Decoufle P, Boyle CA. 1995. The relationship be-tween maternal education and mental retar-dation in 10-year-old children. Ann Epide-miol 5:347–353.
Decoufle P, Boyle CA, Paulozzi LJ, Lary JM. 2001.Increased risk for developmental disabilities inchildren who have major birth defects: a pop-ulation-based study. Pediatrics 108:728–734.
Drews CD, Yeargin-Allsopp M, Murphy CC, et al.1992. Legal blindness among 10-year-oldchildren in metropolitan Atlanta: prevalence,1985 to 1987. Am J Public Health 82:1377–1379.
Drews CD, Yeargin-Allsopp M, Murphy C et al.1994. Hearing impairment among 10-year-old children: metropolitan Atlanta, 1985through 1987. Am J Public Health 84:1164–1166.
Drews CD, Yeargin-Allsopp M, Decoufle P, et al.1995. Variation in the influence of selectedsociodemographic risk factors for mental re-tardation. Am J Public Health 85:329–334.
Edmonds LD, Layde PM, James LM, et al. 1979.Congenital malformations surveillance: twoAmerican systems. Intl J Epidemiol 10:247–52.
Elixhauser A, Steiner C, Harris DR, et al. 1998.Comorbidity measures for use with adminis-trative data. Med Care 36:8–27.
Feinstein AR. 1970. The pre-therapeutic classifica-tion of co-morbidity in chronic disease.J Chron Dis 20:455–469.
Gortmaker SL, Sappenfield W. 1984. Chronicchildhood disorders: prevalence and impact.Pediatr Clin NA 31:3–18.
Gostin LO. 2001. National health information pri-vacy: regulations under the Health InsurancePortability and Accountability Act. JAMA285:3015–3021.
Grether JK, Cummins SK, Nelson KB. 1992. TheCalifornia Cerebral Palsy Project. PaediatrPerinat Epidemiol 5:339– 351.
James LM, Erickson JD, McClearn AB. 1995.Prevalence of birth defects. In: Wilcox LS,Marks JS, eds. From data to action: CDC’spublic health surveillance for women, infants,and children. Atlanta: US DHHS. p 203–216.
Johnson A, King R. 1999. Can routine informationsystems be used to monitor serious disability?Arch Dis Child 80:63–66.
Johnson A. 1995. Use of registers in child health.Arch Dis Child 72:474–477.
Kirby RS, Brewster MA, Canino CU, et al. 1995.Early childhood surveillance of developmen-tal disorders by a birth defects surveillancesystem: methods, prevalence estimates, andmortality patterns. J Dev Behav Pediatr 16:318–326.
Kirby RS. 1999. A parable wrapped in an enigma:population-based assessments of outcomesamong high-risk neonates are even less achievable in the age of clinical informatics.Arch Pediatr Adolesc Med 153:789–792.
Kraemer HC. 1995. Statistical issues in assessingcomorbidity. Stat Med 14:721–733.
186 MRDD RESEARCH REVIEWS ● DEVELOPMENTAL DISABILITIES AND BIRTH DEFECTS ● KIRBY

Louhiala P. 1995. Risk indicators of mental retar-dation: changes between 1967 and 1981. DevMed Child Neurol 37:631–636.
McDermott S, Cokert AL, McKeown RE. 1993.Low birthweight and risk of mild mental re-tardation by ages 5 and 9 to 11. PaediatrPerinat Epidemiol 7:195–204.
McLaren J, Bryson SE. 1987. Review of recentepidemiological studies of mental retardation:prevalence, associated disorders, and etiology.Am J Ment Retard 92:243–254.
Murphy CC, Yeargin-Allsopp M, Decoufle P, et al.1993. Prevalence of cerebral palsy among ten-year-old children in metropolitan Atlanta, 1985through 1987. J Pediatr 123:S13–S19.
Murphy CC, Yeargin-Allsopp M, Decoufle P, etal. 1995a. The administrative prevalencemental retardation in 10-year-old children inmetropolitan Atlanta, 1985 through 1987.Am J Public Health 85:319–323.
Murphy CC, Trevathan E, Yeargin-Allsopp M.1995b. Prevalence of epilepsy and epilepticseizures in 10-year-old children: results fromthe Metropolitan Atlanta Developmental Dis-abilities Study. Epilepsia 36:866–872.
Newacheck PW, Taylor WR. 1992. Childhoodchronic illness: prevalence, severity, and im-pact. Am J Public Health 82:364–371.
Newacheck PW, Strickland B, Shonkoff JP, et al.1998. An epidemiologic profile of childrenwith special health care needs. Pediatrics 102:117–123.
O’Brien DG, Yasnoff WA. 1999. Privacy, confi-dentiality, and security in information systemsof state health agencies. Am J Prev Med 16:351–358.
Rantakallio P, von Wendt L. 1986. Mental retar-dation and subnormality in a birth cohort of12,000 children in northern Finland. Am JMent Deficiency 90:380–387.
Romano PS, Roos LL, Jollis JG. 1993. Adapting aclinical comorbidity index for use with ICD-9-CM administrative data: differing perspec-tives. J Clin Epidemiol 46:1075–1079.
Rumeau-Rouquette C, du Mazaubrun C, MlikaA, et al. 1992. Motor disability in children inthree birth cohorts. Intl J Epidemiol 21:359–366.
Schendel DE, Stockbauer JW, Hoffman HJ, et al.1997. Relation between very low birthweight and developmental delay among pre-school children without disabilities. Am JEpidemiol 146:740 –749.
Sabbeth B, Stein REK. 1990. Mental health refer-ral: a weak link in comprehensive care ofchildren with chronic physical illness. J DevBehav Pediatr 11:73–78.
Vessey JA. 1999. Psychological comorbidity inchildren with chronic conditions. Ped Nurs25:211–214.
von Wendt L, Rantakallio P, Saukkonen AL, et al.1985. Epilepsy and associated handicaps in a 1year birth cohort in northern Finland. EurJ Pediatr 144(2):149–151.
Virnig BA, McBean M. 2001. Administrative datafor public health surveillance and planning.Annu Rev Public Health 22:213–230.
Wellesley D, Hockey A, Stanley F. 1991. Theaetiology of intellectual disability in WesternAustralia: a community-based study. DevMed Child Neurol 33:963–973.
Wellesley DG, Hockey KA, Montgomery PD, etal. 1992. Prevalence of intellectual handicapin Western Australia: a community study.Med J Aust 156:94–96, 100, 102.
Yasnoff WA, Overhage JM, Humphreys BL, et al.2001. A national agenda for public healthinformatics: summarized recommendationsfrom the 2001 AMIA spring congress. J AmMed Informatics Assoc 8:535–545.
Yeargin-Allsopp M, Murphy CC, Oakley GP, et al.1992. A multiple-source method for studyingthe prevalence of developmental disabilities inchildren: the Metropolitan Atlanta Develop-mental Disabilities Study. Pediatrics 89:624–630. Erratum 90:1001.
187MRDD RESEARCH REVIEWS ● DEVELOPMENTAL DISABILITIES AND BIRTH DEFECTS ● KIRBY