Embed Size (px)
Citation preview
CNS InfectionsCNS Infections
ELSELS
Wednesday, August 6th 2008Wednesday, August 6th 2008
Amal Al-HashmiAmal Al-Hashmi
OutlineOutline
Viral meningitisViral meningitis Viral encephalitisViral encephalitis Bacterial meningitisBacterial meningitis
• EtiologyEtiology• PathophysiologyPathophysiology• Clinical PresenationClinical Presenation• PathophysiologyPathophysiology• Diagnostic toolsDiagnostic tools
CT, MRI head, LP,EEGCT, MRI head, LP,EEG
• TreatmentTreatment
Viral meningitisViral meningitis
DefinitionDefinition
an inflammatory response to viral an inflammatory response to viral infection of leptomeningeal cells and infection of leptomeningeal cells and the subarachnoid spacethe subarachnoid space
account for the majority, at least account for the majority, at least 70%, of cases of aseptic meningitis70%, of cases of aseptic meningitis
EtiologyEtiology
In Europe and USIn Europe and US
nonpolio enteroviruses are the most nonpolio enteroviruses are the most common case of viral meningitis ( Kupila common case of viral meningitis ( Kupila et al 2006) for both children & adultset al 2006) for both children & adults
(coxsackie & enteric cytopathogenic human (coxsackie & enteric cytopathogenic human orphan virus [echovirus]), are the most orphan virus [echovirus]), are the most common causal agentscommon causal agents
EtiologyEtiology
followed by followed by
mumpsmumps
arbovirusesarboviruses
herpesvirusesherpesviruses
lymphocytic choriomeningitislymphocytic choriomeningitis
HIV at the time of seroconversionHIV at the time of seroconversion
Clinical presentationClinical presentation
Children under 2 years of age show Children under 2 years of age show fever, irritability, or seizures , but fever, irritability, or seizures , but may never develop signs of may never develop signs of meningeal irritationmeningeal irritation
Adult pts present with fever, Adult pts present with fever, malaise, headache, nausea, malaise, headache, nausea, vomiting, nuchal rigidity, & vomiting, nuchal rigidity, & photophobiaphotophobia
CSFCSF
1- slightly elevated opening pressure1- slightly elevated opening pressure
2- mild to moderate pleocytosis with 2- mild to moderate pleocytosis with 10–500 white blood cells (WBC)/µl, 10–500 white blood cells (WBC)/µl, predominantly lymphocytespredominantly lymphocytes
3- mildly elevated protein (<100 3- mildly elevated protein (<100 mg/dl),mg/dl),
4- normal glucose 4- normal glucose
CSFCSF
RT-CRP has now replaced viral RT-CRP has now replaced viral cultures as diagnostic procedure of cultures as diagnostic procedure of choice for establishing enteroviral choice for establishing enteroviral infections ( Ramers et al 2000) infections ( Ramers et al 2000)
computed tomography or magnetic computed tomography or magnetic resonance imaging (MRI) scans in resonance imaging (MRI) scans in general are normalgeneral are normal
Viral EncephalitisViral Encephalitis
EtiologyEtiology C/FC/F CSF findings CSF findings Neuroimaging Neuroimaging
Viral EncephalitisViral Encephalitis Most common cause are herpes simplex and Most common cause are herpes simplex and
arbovirusesarboviruses HSV-1 most common cause of fetal encephalitis HSV-1 most common cause of fetal encephalitis
in USin US accounting for 10% overall& 90% in adultaccounting for 10% overall& 90% in adult frequency 1/250,000frequency 1/250,000
HSV-2 more commonly isolated in monophasic or HSV-2 more commonly isolated in monophasic or recurrent meninigitis & congenitally acquired recurrent meninigitis & congenitally acquired neonatal HSV meningoencephalitisneonatal HSV meningoencephalitis
Viral EncephalitisViral Encephalitis C/FC/F Fever 90%Fever 90% Headache 80%Headache 80% Altered mentation 70%Altered mentation 70% Personality changes 70-80%Personality changes 70-80% Seizures 40-67%Seizures 40-67% Memory disturbance 25-45%Memory disturbance 25-45% Motor deficit 30-40%Motor deficit 30-40% Aphaisa 33%Aphaisa 33% Olfactory hallucinationOlfactory hallucination
Viral EncephalitisViral Encephalitis
No set of signs or symptoms is No set of signs or symptoms is pathognomonic of HSEpathognomonic of HSE
(Whitly 2006)(Whitly 2006)
CSFCSF
increased opening pressureincreased opening pressure Normal glucoseNormal glucose Moderalty elevated protien Moderalty elevated protien Lymphocytic pleocytosis Lymphocytic pleocytosis
10-1000/microlitter10-1000/microlitter Xanthochromia and red cells may Xanthochromia and red cells may
occur occur Cultures negative in 95%Cultures negative in 95%
CSFCSF
PCR of HSE is the diagnostic PCR of HSE is the diagnostic procedure of choice ( lakeman & procedure of choice ( lakeman & whitely 1995)whitely 1995)
False negative ( Weil et al. 2002)False negative ( Weil et al. 2002)
NeuroimagingNeuroimaging
particularly MRI,may show particularly MRI,may show temporaltemporal or or orbitofrontal cortex enhancement or orbitofrontal cortex enhancement or edema in HSE ( Raschilas et al 2002)edema in HSE ( Raschilas et al 2002)
In most other acute viral encephalitis, In most other acute viral encephalitis, neuroimaging findings are nonspecific neuroimaging findings are nonspecific
Brain MRI or CT serve to exclude brain Brain MRI or CT serve to exclude brain abscess, subdural empyema, cranial abscess, subdural empyema, cranial extradural abscess, or septic venous extradural abscess, or septic venous thrombosisthrombosis
EEGEEG
Diffuse slowing Diffuse slowing Focal abnormalities in the temporal Focal abnormalities in the temporal
region ( 75% with +ve PCR)region ( 75% with +ve PCR) PLEDSPLEDS
Brain BiopsyBrain Biopsy
Atypical casesAtypical cases Poor response to treatmentPoor response to treatment Findings:Findings:
hemorrahgic necrosishemorrahgic necrosis
HSV antigen in infected neuronsHSV antigen in infected neurons
acidophilic intranuclear inclusionsacidophilic intranuclear inclusions
TreatmentTreatment
Empiric therapy with acyclovir Empiric therapy with acyclovir should be started should be started immediatelyimmediately
Stander Rx course is IV acyclovir Stander Rx course is IV acyclovir
10mg/kg Q8h in adults10mg/kg Q8h in adults
20mg/kg Q8h in neonate and children 20mg/kg Q8h in neonate and children Duration 14-21 daysDuration 14-21 days
TreatmentTreatment
Steroid ?Steroid ? Retrospective studies suggested no obvious Retrospective studies suggested no obvious
harm and be some benefit harm and be some benefit ( Kamie et al 2006)( Kamie et al 2006)
Controlled clinical trails are neededControlled clinical trails are needed
PrognosisPrognosis
MortalityMortality rate in untreated cases is rate in untreated cases is 70%70% which reduced to 19-27% which reduced to 19-27% with with rxrx
Morbidity remains high only 37% of Morbidity remains high only 37% of all pt PCR proven and treated with all pt PCR proven and treated with acyclovir survive with no or mild acyclovir survive with no or mild residual deficits (Raschilas et al2002)residual deficits (Raschilas et al2002)
PrognosisPrognosis
Clinical relapse can occur and more Clinical relapse can occur and more often in children and neonateoften in children and neonate
Consider Consider Foscarnet Foscarnet in cases of in cases of acyclovir resistant stains or in who acyclovir resistant stains or in who are allergicare allergic
Bacterial meningitisBacterial meningitis
Incidence of 3-5/100 000/year in US Incidence of 3-5/100 000/year in US (quagliarello 1997)(quagliarello 1997)
More than 1500 death/yr in USMore than 1500 death/yr in US
Etiology - GeneralEtiology - General
Pneumococcus (Streptococcus Pneumococcus (Streptococcus Pneumoniae)Pneumoniae)• Most common in adults >20Most common in adults >20• Account for ½ of reported casesAccount for ½ of reported cases• 22° to pneumonia/otitis, ° to pneumonia/otitis,
splenectomy/DM2splenectomy/DM2 ’’ing incidence of pen-resistance in ing incidence of pen-resistance in
pneumococcus (25-45% to pen, 10% to pneumococcus (25-45% to pen, 10% to Ceph,+ to chloramphenicol)Ceph,+ to chloramphenicol)
Etiology - GeneralEtiology - General
HiB (Haemophilus Influenzae type B)HiB (Haemophilus Influenzae type B)
• Before vaccination, most common case in US Before vaccination, most common case in US 45% of meningitis caused by Hib 45% of meningitis caused by Hib
• Now accounts for less than 10%–Now accounts for less than 10%–
• still in elderly, HIV ptsstill in elderly, HIV pts
Etiology - GeneralEtiology - General
Meningococcus (Neisseria Meningococcus (Neisseria Meningitidis)Meningitidis)• Mainly children and young adults Mainly children and young adults
(army/college)(army/college)• 22° to asymptomatic nasopharyngeal ° to asymptomatic nasopharyngeal
colonizationcolonization
Etiology – Special PopulationsEtiology – Special Populations
NeonateNeonate• GBS, E. coli & other gram neg., Listeria GBS, E. coli & other gram neg., Listeria
(10%)(10%) Post head trauma/NeurosurgeryPost head trauma/Neurosurgery
• Staph Aureus & CNS, Enteric gram neg.Staph Aureus & CNS, Enteric gram neg. ElderlyElderly
• Listeria and Hib Listeria and Hib
Listeria = Impaired cellular immunityListeria = Impaired cellular immunity• Pregnancy, Chronic disease, Elderly, AlcoholPregnancy, Chronic disease, Elderly, Alcohol

Clinical PresentationClinical Presentation
Triad of Headache, fever and neck Triad of Headache, fever and neck stiffness: 85% of patientsstiffness: 85% of patients
N/V, photophobia, myalgia ( common)N/V, photophobia, myalgia ( common) Alteration in LOC, Seizures (40%)Alteration in LOC, Seizures (40%) Nuchal rigidity: resistance to passive Nuchal rigidity: resistance to passive
flexionflexion Kernig’s: extension of the knee with thigh Kernig’s: extension of the knee with thigh
flexedflexed pain, neck flexion pain, neck flexion Brudzinsky’s Brudzinsky’s
• Flexion of neck causes hip flexionFlexion of neck causes hip flexion
Clinical PresentationClinical Presentation
Cranial nerve palsies 3Cranial nerve palsies 3rdrd, 6, 6thth , 7 , 7thth (10- (10-20%)20%)
Occasionally focal neurological deficit Occasionally focal neurological deficit
hemiparesis, dysphasiahemiparesis, dysphasia
Clinical PresentationClinical Presentation
Classical c/f are commonly absent in Classical c/f are commonly absent in neonates neonates
look for high pitched crying, refusal look for high pitched crying, refusal to feed, irritabilityto feed, irritability
In elderly less act onset of lethrgy, In elderly less act onset of lethrgy, mild or no fevermild or no fever
Certain clinical featuresCertain clinical features
Promient rash particually extrimities Promient rash particually extrimities ((Meningococcus)Meningococcus)
erythemaous, macular evolving into erythemaous, macular evolving into petechial petechial
Rhinorrhea or otorrhea with S Rhinorrhea or otorrhea with S pneumoniaepneumoniae
PathophysiologyPathophysiology
Bacteria spread by droplets and Bacteria spread by droplets and colonize nasopharynxcolonize nasopharynx
bacteremia then meningeal spread bacteremia then meningeal spread thru chroroid plexus epithelial cellsthru chroroid plexus epithelial cells
Multiply rapidly because of absence Multiply rapidly because of absence of immune cellsof immune cells
Lysis of bacterial cell wall in SASLysis of bacterial cell wall in SAS Stimulate microglia inflammatory Stimulate microglia inflammatory
cytokine production of IL-1 and TNFcytokine production of IL-1 and TNF
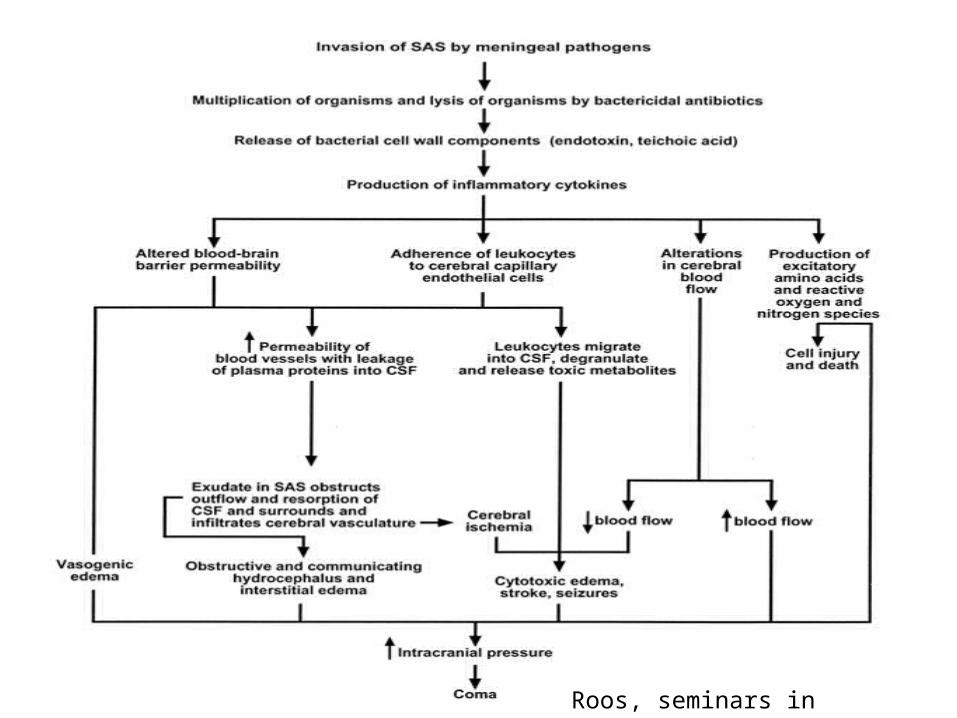
Roos, seminars in neurology 2000
PathophysiologyPathophysiology
Alteration of BBB w/ vasogenic Alteration of BBB w/ vasogenic edema + loss of autoregulation AND edema + loss of autoregulation AND entry of PMN w/ cytotoxic edema SO entry of PMN w/ cytotoxic edema SO formation of purulent exudate formation of purulent exudate
HydrocephalusHydrocephalus
narrows arteries in SAS and invades narrows arteries in SAS and invades wall (vasculitis; leads to CVA)wall (vasculitis; leads to CVA)
Continous rise of ICP and comaContinous rise of ICP and coma
CSFCSF
↑↑ pressure 20-50 mm H20pressure 20-50 mm H20 ↑↑ WBC (100-10000 wbc/mm3, WBC (100-10000 wbc/mm3,
mainly PMN)mainly PMN) ↓↓ glucose (less than 40% of serum glucose (less than 40% of serum
glu)glu) ↑↑ Protein (1.0-5.0 mg/dl)Protein (1.0-5.0 mg/dl) Positive gram stain/culture in 70-90%Positive gram stain/culture in 70-90%
• Less if Abx before; sterile only after 12hLess if Abx before; sterile only after 12h Bx if skin lesionsBx if skin lesions
DiagnosisDiagnosis
Blood Cultures (50%)Blood Cultures (50%) Abx before LP if CT/LP delay Tx Abx before LP if CT/LP delay Tx
(no change in WBC +/- in (no change in WBC +/- in sterility for hours)sterility for hours)
+/- Decadron+/- Decadron CT head (?)CT head (?) Lumbar PunctureLumbar Puncture

CT Head before LP?CT Head before LP?• CT will be abnormal, if you have :CT will be abnormal, if you have :
Seizure Seizure clinical evidence of increased ICPclinical evidence of increased ICP Hx of CNS diseaseHx of CNS disease Immuncompromised statusImmuncompromised status Age>60Age>60 Abnormal neurological exam (including Abnormal neurological exam (including
mental status)mental status)
Hasbun et al. CT head before LP in suspected meningitis. NEJM 345:1727, 2001 Kastenbauer et al. CT head before LP in suspected meningitis. NEJM 346:1248, 02
CT SCAN PRIOR TO LUMBAR CT SCAN PRIOR TO LUMBAR PUNCTURE IN SUSPECTED PUNCTURE IN SUSPECTED
MENINGITISMENINGITIS 235 patients with suspected meningitis 235 patients with suspected meningitis
underwent CTunderwent CT 56/235 (24%) had abnormal CT; 11 (5%) 56/235 (24%) had abnormal CT; 11 (5%)
with mass effectwith mass effect
Hasbun et al. NEJM 2001;345:1727.Hasbun et al. NEJM 2001;345:1727.
CT SCAN PRIOR TO LUMBAR CT SCAN PRIOR TO LUMBAR PUNCTURE IN SUSPECTED PUNCTURE IN SUSPECTED
MENINGITISMENINGITIS 96 patients without above features 96 patients without above features
who underwent CTwho underwent CT• 93 had normal CT; 1 had mass 93 had normal CT; 1 had mass
effecteffect• All had lumbar puncture with no All had lumbar puncture with no
evidence of brain herniationevidence of brain herniation
Hasbun et al. NEJM 2001;345:1727.Hasbun et al. NEJM 2001;345:1727.
CT before LPCT before LP
• Kastenbauer: Nothing predicts Kastenbauer: Nothing predicts herniation (Abnormal CT in 2/10 herniation (Abnormal CT in 2/10 herniations and 27/65 w/ no herniation)herniations and 27/65 w/ no herniation)
of Kastenbauer et al. N Engl J Med of Kastenbauer et al. N Engl J Med 2002;346(16):1248-1251. (189K)2002;346(16):1248-1251. (189K)
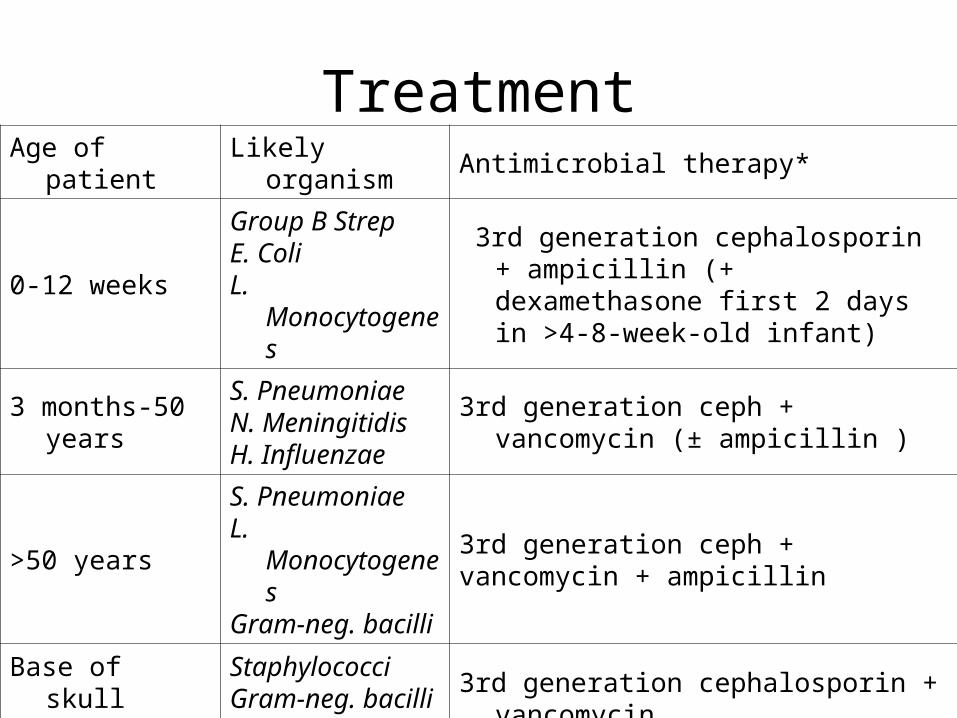
Age of patient Likely organism Antimicrobial therapy*
0-12 weeksGroup B StrepE. ColiL. Monocytogenes
3rd generation cephalosporin + ampicillin (+ dexamethasone first 2 days in >4-8-week-old infant)
3 months-50 yearsS. PneumoniaeN. MeningitidisH. Influenzae
3rd generation ceph + vancomycin (± ampicillin )
>50 yearsS. PneumoniaeL. MonocytogenesGram-neg. bacilli
3rd generation ceph + vancomycin + ampicillin
Base of skull fracture
StaphylococciGram-neg. bacilliS. pneumoniae
3rd generation cephalosporin + vancomycin
Immunocompromised state
L. MonocytogenesGram-neg. bacilliS. PneumoniaeH. Influenzae
Vancomycin + ampicillin + ceftazidime
Treatment
TreatmentTreatment
Based on ageBased on age Always bactericidalAlways bactericidal Consider intrathecal VancoConsider intrathecal Vanco Alternatives: Alternatives:
• Cefepime or meropenem instead of 3rd Cefepime or meropenem instead of 3rd generation Cephgeneration Ceph
• If severe Pen allergy: Vanco + chloramphenicol If severe Pen allergy: Vanco + chloramphenicol or Vanco + septra (listeria)or Vanco + septra (listeria)
3rd generation Cephalosporin3rd generation Cephalosporin• Ceftriaxone 2g q12h – jaundice in neonatesCeftriaxone 2g q12h – jaundice in neonates• Cefotaxime 2g q4hCefotaxime 2g q4h• Ceftazidime 2g q 8h Ceftazidime 2g q 8h
Tx of contactsTx of contacts
Contact Public Health for Contact Public Health for meningococcus and HiBmeningococcus and HiB
Need to treat close contacts Need to treat close contacts (potentially share secretions)(potentially share secretions)• Rifampin bid for two days CRifampin bid for two days C• Or Cipro 500mg once Or Cipro 500mg once • Or zithromax 500mg onceOr zithromax 500mg once
PreventionPrevention
Pneumovax for surgical or functional Pneumovax for surgical or functional asplenia (sickle cell, chronic illness, asplenia (sickle cell, chronic illness, immunosuppression, older age…)immunosuppression, older age…)
SteroidsSteroids
Morbidity and mortality of meningitis Morbidity and mortality of meningitis related of inflammatory reaction related of inflammatory reaction rather than bacteria themselvesrather than bacteria themselves
Decadron inhibits IL-1 and TNF m-Decadron inhibits IL-1 and TNF m-RNA production and RNA production and CSF outflow CSF outflow resistance and stabilizing BBBresistance and stabilizing BBB
Lots of small studies 1950’s-2002; Lots of small studies 1950’s-2002; big studies are rare, especially in big studies are rare, especially in adults. adults.
SteroidSteroid
The available evidence on adjunctive The available evidence on adjunctive dexamethasone therapy confirms a dexamethasone therapy confirms a benefit for treating H influenza type benefit for treating H influenza type b in reducing audiological sequelae b in reducing audiological sequelae and suggest benefit in reducing the and suggest benefit in reducing the audiological and neurological audiological and neurological sequelae in H influenza type b and sequelae in H influenza type b and pneumococcal in children pneumococcal in children
(sebire et al 2006) …….( weisfelt et al 2006)(sebire et al 2006) …….( weisfelt et al 2006)
Cochrane Review 2003Cochrane Review 2003 18 RCT18 RCT Mainly kidsMainly kids General General
• Lower mortality RR 0.76 [.59-.98]Lower mortality RR 0.76 [.59-.98]• Hearing loss 0.36 [.22-.60]Hearing loss 0.36 [.22-.60]• Neuro Sequelae 0.66 [.44-.99]Neuro Sequelae 0.66 [.44-.99]
In ChildrenIn Children• Lower hearing loss in non Hib meningitis 0.42 Lower hearing loss in non Hib meningitis 0.42
[.2 - .89][.2 - .89] In adultsIn adults
• Lower mortality 0.48 [0.24-0.96]Lower mortality 0.48 [0.24-0.96]
Systematic Review in adultsSystematic Review in adults
5 RCT in adults5 RCT in adults• Overall mortality and neuro sequelae Overall mortality and neuro sequelae
0.60.6• Pneumococcus mortality 0.5Pneumococcus mortality 0.5• Meningococcal sequelae 0.5 and Meningococcal sequelae 0.5 and
mortality 0.9mortality 0.9 No increased side effects with No increased side effects with
steroidssteroids
Vanco level controversyVanco level controversy
Experimental evidence of decreased Experimental evidence of decreased absorption if steroids givenabsorption if steroids given
One RCT study in children One RCT study in children demonstarted reliable penetration of demonstarted reliable penetration of vanco if 60mg/kg doses used.vanco if 60mg/kg doses used.
4/11 pts in adults failed vanco with 4/11 pts in adults failed vanco with steroids but used lower dosagessteroids but used lower dosages
SteroidsSteroids
Do not use if immunosuppressedDo not use if immunosuppressed
Thank You!
Questions?