Embed Size (px)
Citation preview

770 Brief Communications
re-entry due to retrograde dual atrioventricular nodal path- ways. Circulation 56:50, 1977. Zincs DP. deJoseoh RL. Rothbaum A: Unusual oronerties of ac’cessory’pathways. Circulation 49:1200, 1974. - _ Coumel P, Attuel P: Reciprocating tachycardia in overt and latent preexcitation. Influence of functional bundle branch block on the rate of the tachycardia. Eur J Cardiol 1:423, 1974. Wellens HJJ, Durrer D: The role of an accessory atrioventric- ular pathway in reciprocal tachycardia. Observations in natients with and without the Wolff-Parkinson-White svn- drome. Circulation 52:58, 1975. Krikler D, Rowland E: Concealed pre-excitation. J Electro- cardiol 11:209, 1978. Narula OS: Retrograde pre-excitation. Comparison of ante- grade and retrograde conduction intervals in man. Circula- tion 50:1129, 1974. Wu D, Denes P: Mechanism of paroxysmal supraventricular tachvcardia. Arch Intern Med 135437. 1975. De&s P, Wu D, Amat-y-Leon F, Dhingra R, Wyndham CR, Rosen KM: The determinants of atrioventricular nodal re- entrance with premature atria1 stimulation in patients with dual A-V nodal pathways. Circulation 56:25X 1977.
October, 1983
American Heart Journal
17.
18.
19.
20.
21.
22.
23.
Clinical spectrum of pericardial effusion as the presenting feature of hypothyroidism
Joseph Zimmerman, M.D., Joachim Yahalom, M.D., and Hanoch Bar-On, M.D. Jeruslaem, Israel
Pericardial effusion is a common finding in myxedema, occurring in about 30 % of cases.’ However, it is seldom the presenting feature of this disorder. We describe here two patients in whom a large pericardial effusion was the presenting feature of hypothyroidism.
Case 1. A 74-year-old woman was admitted to hospital in 1979 because of an abnormal chest x-ray examination, mild anemia, and increased sedimentation rate, all found on incidental medical examination. In 1972, a chest x-ray examination showed cardiomegaly (Fig. 1). From that time she noted edema of her lower extremities. Apart from cold intolerance she was entirely asymptomatic. On admission, she was in no distress. Blood pressure was 160/90 mm Hg and pulse was 72/min and regular. No pulsus paradoxus was found. There was a cervical conges- tion of 10 cm with a negative Kussmaul sign. Ewart’s sign was positive. The cardiac apex was impalpable and there was a pericardial knock. The liver was normal. There was pitting edema of the lower extremities. Laboratory exam- inations revealed hemoglobin of 11.0 gm/dl and sedimen- tation rate of 46 mm in the first hour. Serum biochemical profile was normal, and tests for rheumatic and collagen diseases were negative. Chest x-ray examination (Fig. 2) revealed globular enlargement of the cardiac silhouette. Serum thyroxine was 1.6 gg/dl, triiodothyronine (T,) resin
From the Department of Internal Medicine B, Hadassah University
Hospital.
Reprint requests: J. Zimmerman. M.D., Dept. of Internal Medicine B, Hadassah University Hospital, P.O.B. 12000, Jerusalem. Israel.
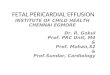
Fig. 1. Case 1. Routine chest x-ray film from 1972, showing a globular cardiac enlargement, suggestive of a pericardial effusion.
Fig. 2. Case 1. Admission chest roentgenogram, showing massive pericardial effusion.
uptake was 44 5%) T, absolute was 10 ng/dl (normal 80 to 200 ng/dl). Serum thyroid-stimulating (TSH) was 87 mu/ml (normal 0 to 5 mu/ml). Pericardiocentesis yielded 900 ml of yellowish turbid fluid that had a protein content of 5.9 gm/dl but was otherwise normal. After this proce- dure, a large residual pericardial effusion was still evident on chest roentgenogram (Fig. 3). After the diagnosis of hypothyroidism was established, treatment with L-thy- roxine was started. Chest x-ray examination in the euthy- roid state, 6 months after institution of thyroid replace- ment, revealed marked decrease in cardiac size (Fig. 4).
Case 2. A 42-year-old woman with a lo-year history of

Volume 106
Number 4, Part 1 Brief Communications 77 1
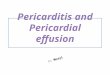
Fig. 3. Case 1. Chest x-ray film after pericardiocentesis, showing a large residual pericardial effusion.
Fig. 4. Case 1. Chest x-ray film in the euthyroid state, after 6 months of thyroid replacement therapy.
psychoneurosis, joint pains, weakness, and cold intoler- ance was admitted to the emergency room because of syncope and persistent hypotentison. Examination revealed a blood pressure of 70/50 mm Hg and a pulse rate of 64/min. No cervical venous congestion ‘was noted. The heart sounds were inaudible. There was minimal hepato- megaly and no peripheral edema. Chest x-ray examination disclosed a huge cardiac silhouette. The diagnosis of pericardial tamponade was suggested, and surgical drain- age of 200 ml of cloudy fluid from the pericardial sac resulted in a prompt rise of blood pressure to 140/80 mm Hg. Laboratory tests revealed a serum thyroxine level of 0.8 N/d& a T3 resin uptake of 32%, and a 24-hour radioiodine uptake of 3%. Tuberculosis and collagen diseases were ruled out by appropriate bacteriologic and serologic tests. Twenty-four hours following her admis-
sion, thyroid replacement was started with marked improvement in the patient’s condition. Chest x-ray examination after a few months of therapy in euthyroid- ism showed marked diminution of cardiac size.
There are some noteworthy features in the two patients presented. In the first case a huge, albeit hemodynamical- ly insignificant pericardial effusion was the most promi- nent feature of hypothyroidism. The usual physical fea- tures of this condition were subtle and a diagnosis of myxedema was not made on clinical grounds alone. This patient was relatively asymptomatic considering the marked degree and the long duration of her illness. It is probable that she had had a pericardial effusion due to hypothyroidism at least 7 years before the diagnosis was established. The eventual diagnosis of her pronounced hypothyroidism only on routine investigation seems to point to the very gradual development of her condition. In the second case, a clinical picture compatible with hypo- thyroidism had been present for some years before the diagnosis was established, when the patient was urgently admitted in shock due to pericardial tamponade. The coexistence of hypotension and relative bradycardia in this case is of interest and served as a clue to the possibility of hypothyroidism complicated by pericardial tamponade. Of major importance in both patients was the rapid response to replacement therapy, resulting in an almost normal cardiac silhouette after a few months. The laboratory features of an increased sedimentation rate and mild anemia, which may point to an inflammatory process, are also common in hypothyroidism.2,” These findings in an elderly patient with asymptomatic pericardial effusion can be misleading and may lead to noncontributory and often invasive procedures, such as pericardiocentesis. Since hypo- thyroidism in the elderly is often oligosymptomatic, we believe that it should be ruled out in every elderly patient presenting with a pericardial effusion before any invasive diagnostic measures are performed.
REFERENCES
1.
2.
3.
Kerber RE, Sherman B: Echocardiographic evaluation of pericardial effusion in myxedema. Circulation 52:823, 1975. Bland JH, Frymoyer JW: Rheumatic syndromes of myxede- ma. N Engl J Med 282:1171, 1970. Carpenter JT, Mohler DN Jr, Thorup OA Jr, Leave11 BS: Anemia in myxedema. In Crispell KR, editor: Current con- cepts in hypothyroidism. New York, 1963, Macmillan Pub- lishing Co, Inc, p 147.
Left ventricular hemangioma masquerading as #ycop/asma pericarditis
William E. Boden, M.D., Erik J. Funk, M.D., Richard A. Carleton, M.D., Ian Benham, M.D., Abdul H. Khan, M.D., Abraham Lasser, M.D., and M. Terry McEnany, M.D. Providence, and Pawtucket, R.I.
From the Departments of Medicine, Pathology and Surgery, The Miriam Hospital; The Memorial Hospital; and Brown University. Reprint requests: William E. Boden, M.D., Division of Cardiology, The Miriam Hospital, 164 Summit Ave., Providence, RI 02906.