Embed Size (px)
Citation preview

98 Journal of The Association of Physicians of India ■ Vol. 64 ■ December 2016
Pericardial Effusion with Cardiac Tamponade as a form of presentation of Primary HypothyroidismArun Agarwal1, Nikhil Chowdhury2, Ankit Mathur3, Samiksha Sharma4, Aakanksha Agarwal5
AbstractHypothyroidism is a rare cause of pericardial effusion (PE). Pericardial effusion secondary to hypothyroidism remains a diagnostic challenge for clinicians because of its inconsistency between symptoms and amount of pericardial effusion. We report an atypical case that presented with ascites and was diagnosed to have cardiac tamponade secondary to primary hypothyroidism. Besides repeated pericardiocentesis she eventually required surgical management and optimization of medical therapy to manage the massive pericardial effusion.
1Consultant and Head, Department of Internal Medicine, 2Senior Consultant, Department of Cardiology, 3Senior Consultant, Depatment CTVS, 4Consultant, Department of Pathology, Narayana Multispeciality Hospital, Jaipur, Rajasthan; 5Intern, BJ Medical College, Ahmedabad, GujaratReceived: 27.11.2015; Revised: 05.05.2016; Re-revised: 26.07.2016; Accepted: 08.08.2016
Introduction
Hypothyroidism can have atypical modes of presentations like pre-
eclampsia in pregnancy, acute massive macroglossia and pericardial effusion (PE) as a sole manifestation. Patients with massive amount of pericardial effusion secondary to hypothyroidism may be asymptomatic or have few symptoms. Cardiac tamponade as a complication of hypothyroidism is very rare. This is probably due to the slow accumulation of fluid and to cardiac distensibility. Pericardial effusion has a high concentration of protein and, like other serous effusions of hypothyroidism, its pathogenesis is not fully understood. Controversy exists regarding the form of drainage of cardiac tamponade which shall be discussed here.
Case Report
A 40 year female, known case of depression since 2003 and not a known case of hypothyroidism had a history of feverishness, gradually increasing abdominal distention, weakness, and decreased appetite for 2 months. She was initially admitted at a government hospital from 10.09.2015 to 16.09.2015. She was discharged on thyroxine 100 ug, diuretics, oleanzapine and supportive treatment with a diagnosis of anemia, hypothyroidism and high gradient ascites. She was later referred to our institution for further work-up in view of persistent abdominal symptoms. She had no history of shortness of breath, chest pain, vomiting, arthralgia or recent travel. Vital signs on admission
suggestive of Dengue fever. There were no features of capillary leak syndrome. The pericardial fluid bacterial culture and tuberculosis/non-tuberculosis (TB/NTB) real time PCR were negative. Blood, urine and pericardial f luid cultures, malarial antigen, scrub typhus IgM, serology and MT were negative. All other causes of cardiac tamponade except hypothyroidism were ruled out. Thyroxine dose was optimized.However , there was a pers i s tent collection of pericardial fluid and daily 200-350 ml fluid was being aspirated. A repeat echocardiography on 08.10.2015 showed persistent moderate size PE, RA and RV collapse and thickened, shaggy visceral pericardium. NCCT and CECT chest were done (Figure 2A). Cardio thoracic and vascular surgery (CTVS) consult was taken and it was decided to do a surgical procedure with a diagnostic and therapeutic intent in view of recurrent PE. Pericardiectomy a n d p e r i c a r d i a l p l e u r a l w i n d o w formation was done on 12.10.2015. Intra-operatively pericardium was found to be thickened and adherent to the heart. Bilateral pleural effusions were drained, mediastinal and bilateral pleural drains were placed and biopsy was sent. She evolved favorably during the post operative period. She was discharged on 21 .10 .2015.A chest x-ray taken at discharge showed that the cardiac silhouette had returned to normal size with minimal left pleural effusion (Figure 2C). The pericardium biopsy showed chronic non specific inflammation, fibrosis and congested vessels . (F igure 3) . The pat ient i s currently receiving follow-up care through the outpatient department. When last seen in February 2016, she was asymptomatic, X ray chest and inflammatory markers were normal, and thyroxine dosage were adjusted. She is off antidepressants now.
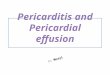
we r e t e m p e r a t u r e 9 9 . 4 °F ; b l o o d pressure 100/64 mmHg; heart rate regular at 110 beats/min; respiratory rate 20/min. There was no pulsus paradoxus. Physical examination found coarse hair, dry skin, elevated jugular venous pressure, muffled heart sounds, bilaterally decreased basal air entry in lungs, non tender hepatomegaly (2 cms below costal margin), moderate ascites, mild pitting edema of the legs bilaterally, and a non-palpable thyroid gland. Chest roentgenogram showed globular enlargement of the cardiac silhouette (Figure 1A). An electrocardiogram revealed low P wave and QRS complexes (Figure 1B). An echocardiogram demonstrated normal heart size but with massive pericardial effusion and signs of early systolic right atrium (RA) and early diastolic right ventricle (RV) collapse (Figure 1C). Cardiac tamponade was diagnosed and pericardiocentesis was done on 29.09.2015 via sub costal approach using 6F pigtail catheter which was left in situ. 700 ml of golden brown color fluid was drained. After the procedure, her heart rate decreased in the range of 50-60 beats/min and blood pressure remained around 100/60 mm Hg. Her hematology, biochemistry and other reports are mentioned in tables 1 and 2 respectively. The test for Dengue IgM antibody was also positive but she had no symptoms

99Journal of The Association of Physicians of India ■ Vol. 64 ■ December 2016
Fig. 1: (A) Chest roentgenogram upon admission showing globular cardiac enlargement. (B) 12 lead electrocardiogram showing low voltage trace. (C) Four chamber view with two-dimensional echocardiography shows collapse of the right ventricle and right atrial free wall (arrow)
Fig. 2: (A) CECT chest dated 09.10.2015 before surgery showing pericardial effusion and bilateral pleural effusion. (B) Chest roentgenogram at discharge shows normal cardiac silhouette with minimal left pleural effusion
Fig. 3: Pericardial biopsy: H&E stain. Arrow 1 show congested vessel, arrow 2 show inflammation and arrow 3 show fibrosis. No evidence of Granuloma or malignancy is seen
A B
Discussion
Pericardial ef fusion (PE) as an initial clinical presentation of primary hypothyroidism has been reported in literature.1,2 Our patient had severe hypothyroidism with undetectable T3,T4 and markedly raised TSH. As discussed she had massive PE with features of cardiac tamponade and the fluid had a high concentration of protein and was an exudate (Table 3). Though the Light’s criteria had been described for pleural effusions it has
Table 1: Hematology and biochemistry
Hb(gm/dl)
Platelet count(x103/cmm)
TLC(x103/cmm)
BUN(mg/d)
Creat(mg/dl)
AST/ALT(IU/ml)
T.Prot/Alb(gm/dl)
ESR(mm 1st hour)
CRP(U/L)
10.09.2015 5.6 127 5.26 1.19 38/16 7.3/3.829.09.2015 8.2 123 3.9 0.63 32/26 6.46/3.03 35 0.9701.10.2015 9.3 142 5.907.10.2015 9.4 230 11.8 120 19.2608.10.2015 8.5 203 8.7 16.8 0.5311.10.2015 9.9 188 7.113.10.2015 9.0 236 8.1 9.0 0.6015.10.2015 9.6 161 6.3 0.5802.02.2016 11.9 160 4.9 32/51 15 0.32
Hb: Hemoglobin (12.0 -15.0), TLC: Total leucocyte count (4.0 – 10.0), BUN: Blood urea nitrogen (7.0 – 17.0), Creat: Creatinine (0.6 – 1.0), AST: Aspartate transaminase (15.0-37.0), ALT: Alanine transaminase (30.0 – 65.0), T. Prot/Alb: Total proteins/Albumin (6.4 – 8.2 / 3.4 – 5.0), ESR: Erythrocyte sedimentation rate (0.0-12.0), CRP:C reactive protein (< 1.0).
been applied for other serous effusions too to classify them as exudates or transudates.3 She had been treated for depression for a long period but it appears that her symptoms had been treated but her clinical picture had never been investigated.
PE in hypothyroidism is a part of the generalized polyserositis and t h e p a t h o p h y s i o l o g i c a l c h a n g e s responsible are capillary dysfunction, albumin leak into interstitial and extra cellular space, reduced lymph clearance
probab ly due to poor lymphat i c tone, and disturbances in electrolyte metabolism.2,4 The term “Gold Paint Effusion” has been used to describe the golden brown appearance of the pericardial fluid due to the shimmering satin cholesterol crystals. Changes in l ipid metabol ism are probably responsible for the high cholesterol content of the fluid. The case discussed had high total cholesterol (47 mg/dl) in pericardial fluid. A churning action of the heart may play a role in the precipitation of cholesterol from pericardial fluid or the poor absorptive capacity of the pericardium may be a major factor.1,4 Mercedes Camprubi et al5 reported a case of cholesterol pericarditis with hypothyroidism. However no such crystals could be demonstrated in the pericardial biopsy of our patient, though the fluid did had golden brown appearance. Having ruled out an infectious process a tumor or an underlying immunologic disorder and because of the persistence of the effusion a surgical approach was

100 Journal of The Association of Physicians of India ■ Vol. 64 ■ December 2016
Table 2: Investigations (Special)
Date Test Result11.09.2015 USG Abdomen Mild Hepatomegaly,Gross Ascites.12.09.2015 Thyroid Function Tests FT3 0.00pg/ml/undetectable (normal 1.8-4.2),FT4 0.07 ng/dl (Normal
0.89-1.76),TSH > 150 uIU/ml(normal 0.4-4.0)15.09.2015 Ascitic fluid Analysis Total proteins 5.0 gm/dl,Albumin 2.3 gm/dl,Glucose 81 mg/dl,Total
cells 300/cmm,differential P20% L80%,ADA 8.9 U/L,gross appearance yellowish.SAAG > 1.1(High gradient)
28.092015 TSH 13.9 uIU/ml (normal 0.40-5.50)28.092015 Dengue Profile NS1 not detected ; IgM antibody detected; IgG antibody not detected29.09.2015 Pericardial fluid
analysisTotal cells 300/cmm, differential P10% L90%,total proteins 6.58 gm/dl, albumin 1.86 gm/dl, glucose 96.6 mg/dl, cholesterol 47 mg/dl, ADA 6.60 U/L,LDH 151U/L; Stains (Grams, AFB and KOH) negative ;TB/NTM real time PCR not detected; Cytology smears show low cellularity, comprising of few reactive mesothelial cells in a pinkish background..No other specific pathology or malignancy noted.
Table 3: Sensitivity of tests to distinguish exudative from transudative effusions3
Test Patients value
Sensitivity for exudate
(%)
Specificity for exudate
(%)Light’s criteria (one or more of the following three) : 98 83Ratio of pleural-fluid protein level to serum protein level >0.5 1.01 86 84Ratio of pleural-fluid LDH level to serum LDH level >0.6 0.843 90 82Pleural-fluid LDH level >two thirds the upper limit of normal for serum LDH level
< 2/3rd 82 89
Pleural-fluid cholesterol level >60 mg/dl (1.55 mmol/liter) 47 mg/dl 54 92Pleural-fluid cholesterol level >43 mg/dl (1.10 mmol/liter) 47 mg/dl 75 80Ratio of pleural-fluid cholesterol level to serum cholesterol level >0.3 0.44 89 81Serum albumin level - pleural fluid albumin level < 1.2 g/dl 1.17 g/dl 87 92
LDH denotes lactate dehydrogenase.
considered and a pericardial biopsy was performed. In our case diagnosis was based on clinical and echocardiography findings and hypothyroidism as a cause for pericardial effusion and tamponade was diagnosed by an exclusion criteria.6
The data from pathologic study showed enlarged pericardium with chronic non specific inflammation and fibrosis.
The management varies depending on size of effusion and hemodynamic stability of the patient. Management strategy ranges from conservative management with close monitoring a n d t h y r o x i n e r e p l a c e m e n t t o pericardiocentesis or creation of a pericardial window.6 The advantages of pericardial window are possible
tissue biopsy and prevention from recurrences. On literature search we could find only one case report of a case of cardiac tamponade secondary to hypothyroidism being managed with surgical intervention.6
The bilateral pleural effusion and ascites were due to congestive heart failure and not a part of capillary leak syndrome (CLS). In CLS in dengue fever, the fluid clears rapidly within a week’s time, is associated with some degree of thrombocytopenia in all cases, bleeding manifestations, and other clinical and sonography features such as edematous gall bladder wall which were not present in the case discussed. Further, Pericardial effusion,
though reported in dengue fever, is not massive and the pericardial biopsy features of chronic inflammation also rules out acute febrile tropical illness as a likely etiology in the present case. We did not find any evidence in favor of dengue fever which could have caused or complicated the patient illness and positive serology for dengue fever could be the result of a subclinical infection that may have occurred in the preceding 2 to 3 months period or a false positive test due to cross reactivity with other flaviviruses.
Conclusion
Hypothyroidism presenting with mass ive per icardia l e f fus ion and cardiac tamponade is an uncommon and rare presentation as in the present case report. Mild pericardial effusion respond to thyroxine supplementation over a long period.Pericardiocentesis is necessary only when it is massive and tamponade develops. Very rarely in recurrent PE surgical management such as pericardiectomy and/or pericardial pleural window is needed as in the present case reported.
References1. Patil VC, Patil HV, Agrawal V, Patil S. Cardiac tamponade in
a patient with primary hypothyroidism. Indian J Endocrinol Metab 2011; 15:S144-S146.
2. Radheshyam Purkait, Anand Prasad, Ramchandra Bhadra, Arindam Basu. Massive pericardial effusion as the only manifestation of primary hypothyroidism. Journal of Cardiovascular Disease Research 2013; 4:248-250.
3. Light RW. Clinical practice. Pleural effusion. N Engl J Med 2002; 346:1971-7.
4. Chou SL, Chern CH, How CK, Wang LM, Huang CI, Lee CH. A rare case of massive pericardial effusion secondary to hypothyroidism. J Emerg Med 2005; 28:293–6.
5. Mercedes Camprubí, A Jordi Mercé and Antoni Raventosb. Pericardial Constriction Secondary to Cholesterol Pericarditis. Rev Esp Cardiol 2006; 59:289-91
6. Auguet T, Vázquez, Nolla J, Solsona JF. Cardiac tamponade and hypothyroidism. Int Care Med 1993; 19:241.










![Challenges in Management of Pericardial Effusion in ... · [5,6]. It has been demonstrated that cardiac tamponade, a serious hemodynamic medical emergency as a result of pericardial](https://img.pdfslide.us/doc/110x75/5ceb108588c993886b8bfeff/challenges-in-management-of-pericardial-effusion-in-56-it-has-been-demonstrated.jpg)