Embed Size (px)
Citation preview

PANI ellll. : BANCROFflAN FILARIASIS IN RELATION TO MICROfiLARAEMIA AND DEC THERAPY 9
21 Dalla DV. Bhagwat AG. Idiopathic portal hypertension-Areview. Bull PGIMER 1981;15:173--92.
22 Foster JH. Conkle OM. Crane JM. Burko H. Splenoportography:An assessment of its value and risk. Ann Surg 1974;5:773--81.
23 Burchanh F. Aagaard J. Sorensen TIA. Christensen U. Jensen L1.Comparison of splenoponography and transhepatic portography inthe diagnosis ofponal vein thrombosis. J Hepalo/1986;2:351-7.
24 Groszmann RJ. Atterbury CEo Clinical applications of the measure-ment of portal pressure. Clin GaslroenleroI1980;2:379-86.
25 Staritz M. Poralla T. Meyer Zum Buschenfelde K-H. Intravascularoesophageal variceal pressure (IOVP) assessed by endoscopic fineneedle puncture under basal conditions. Valsalva's manoeuvre andafter glyceryl trinitrate application. GUI1985;26:525-30.
26 Sarin SK. Sethi KK. Nanda R. Measurement and correlation of
wedged hepatic. intrahepatic, intrasplenic and intravariceal pressuresin patients with cirrhosis of liver and non-cirrhotic portal fibrosis.GUI1987;18:26(}...{j.
27 Burcharth F. Alsner T. Bertheussen K. Rosendal T. Nielsen SE.Influence of general anaesthesia on portal pressure in liver cirrhosisand portal hypertension. A eta Anaesthesiol Scand 1979;23:248--52.
28 Bhatia SJ, Deshmukh H, Abraham P, et al. Effect of sublingualisosorbide dinitrate in portal hypertension. Indian J Gastroenterol1990;9:113--15.
29 Navasa M. Chest a J. Bosch J. Rodes J. Reduction of portal pressureby isosorbide-5-mononitrate in patients with cirrhosis. Effects onsplanchnic and systemic hemodynamics and liver function. Gastro-enterotogy 1989;96:11Ja-18.
Clinical manifestations of Bancroftian filariasis in relationto microfilaraemia and diethylcarbamazine therapyS. P. PANI, A. SRIVIDYA, P. K. RAJAGOPALAN
ABSTRACTWe studied the clinical manifestations of Bancroftianfilariasis in relation to microfilaraemia and diethylcarba-mazine (DEC) therapy in three groups of individualsin Pondicherry. In 3170 persons examined in a door-to-door survey (Group I), the prevalence of disease was foundto be independent of microfilaria (mf) status (the diseaserate was 13.4% in mf carriers and 13.6% in amicrofilaraemicpersons). There was no association between the occurrenceof disease (and individual manifestations), and mf status andits intensity in 1103 mf carriers examined in the filariasisclinic (Group II). Clinical manifestations, however, were ageand sex dependent in Group II. Change in mf status in a five-year period (1981 to 1986) with and without DEC therapy didnot influence the clinical manifestations in 1024 individuals(Group III). Though the disease rate in mf carriers whodiscontinued DEC (22.2%) and in those who completed onecourse of DEC (14.8%) was higher than those who did notreceive DEC (10.6%), statistical analysis did not show anysignificant difference between the groups. The study con-firms that the dynamics of infection and filarial disease arecomplex, and other associated factors need to be investigated.
Vector Control Research Centre, Medical Complex,Indira Nagar, Pondicherry 605006, India
S. P. PANI, A. SRIVIDYA, P. K. RAJAGOPALAN
Correspondence to P. K. RAJAGOPALAN
© The National Medical Journal of India IWI
INTRODUCTIONLymphatic filariasis is a major public health problem inIndia.' Several gaps still exist in our understanding of itsnatural history and its relation to microfilaraemia andclinical disease. 2.3 The dynamics of infection and filarialdisease are complex. 4 The appearance of clinical manifes-tations is a slow process and most microfilaraemic personsare asymptomatic while many symptomatic individualsare amicrofilaraemic .•.5 As a result, in any stable endemicarea only a minority of the affected population is both mfand disease positive. Therefore, a longitudinal follow upof the population is required which, besides being timeconsuming and difficult, poses ethical problems as mfcarriers once detected need to be treated. In the absenceof uniform criteria for clinical diagnosis, the comparisonof results between studies is difficult. Studies of mfcarriers which have included cases with lymphadenopathy(which may be due to several causes other than filariasis)without any other associated filarial symptoms havereported high disease rates of up to 94 %.6.7 Geographicalvariations in the clinical picture also occur=? and the longterm effects of DEC on disease status are not clear. to Wereport the results of detailed analyses on the relationshipof microfilaraemia with disease status, and also theoccurrence of disease in relation to long term changes inmf status and D EC therapy.

10
PATIENTS AND METHODSPondicherry town in south India is a stable endemic areafor Bancroftian filariasis. II A five-year integrated vectormanagement (IVM) project was undertaken in the townby the Vector Control Research Centre (VCRC). Door-to-door random surveys of mf carriers were carried outduring the pre- (1981) and post-control (1986) periods'<"and the following three groups were identified.
Group I consisted of 3170 randomly selected personsexamined clinically and for microfilaraemia by door-to-door visits in 1986. The data from this group wereanalysed for prevalence of disease in relation to micro-filaraemia.
Group II: Since there were limitations in the detailedanalyses of the relationship of microfilaraemia and clinicalstatus in group I (as there were only 27 mf carriers whohad clinical filariasis in this group), 1103 mf carriersdetected in the door-to-door mass blood survey in 1986,12were examined clinically at the VCRC filariasis clinic tostudy the association of microfilaraemia and diseasestatus.
Group III consisted of 1024 persons examined formicrofilaraemia both in 1981 and 1986 (out of 7525 personscovered in both the surveys!') and examined clinically atthe filariasis clinic. All those who were mf carriers in 1981were asked whether they had received DEC therapy. Thetreatment status in 1981 was confirmed from the cardsissued by the state filaria control unit. The data wereanalysed for clinical outcome in relation to DEC therapyand also in relation to change in mf status over the five-year period (1981 to 1986).
Standard criteria were followed for clinical examinationof the individuals." Both acute and chronic manifesta-tions were recorded after detailed clinical examination bya physician. Only the detection of one or more specificmanifestations (Table I) was used for calculation ofdisease rate. Persons who bad lymphadenopathy withoutany other specific filarial manifestation were not includedas enlarged lymph nodes may occur from bacterial infec-tions due to walking barefoot and from several otherendemic diseases such as tuberculosis. Any person whohad developed clinical manifestations of the diseasebefore 1981 was excluded from groups II and III.
Statistical analysesThe Chi-square and Fisher's exact tests were used tocompare proportion positivity in different groups. Logodds ratio interaction test was also used for comparison ofdifferent groups for the development of disease in relationto treatment and microfilaraemia status. A test for lineartrend in proportions was used to study the relationshipbetween the occurrence of clinical disease at different mfcounts.P The 't' independent test was used to study thedifference in mean mf counts between symptomatic andasymptomatic individuals in different age classes.
RESULTSRelationship between microfilaraemia and clinical statusOfthe 3170 persons examined in group I, 6.3% (201) weremicrofilaraemic and 13.6% (432) were diseased. Clinical
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. 4, NO.1
TABLE I. Comparison of clinical manifestations between mfcarriers and microfilaraemic persons (Group I)
Microfilaraemia status Significant
Clinical mf+ve mf-vedifferencebetween
manifestations (n=201) (n=2969) mf +ve and
No.+ve (%ofn) No.+ve (% ofn) mf-ve(p value")
SpecificA. AcuteFilarial fever 8 (3.98) 213 (7.17) 0.11Lymphangitis 1 (0.50) 19 (0.64) 0.63Funiculitis I (1.19)· 12 (1.18)" 0.63Epididymo-orchitis 3 (3.57)' 19 (1.86)' 0.22
B. ChronicHydrocele 15 (17.86)" 112 (10.97)· 0.08Lymphoedema 1 (0.50) 54 (1.82) 0.13Lymph varix 2 ( 1.(0) 2 (0.07) 0.02'·'Scrotum lymph 0 (0.00)' 3 (0.10)" 0.78Chyluria 6 (2.99) 34 (1.15) 0.05
Non-specificLymphadenitis 17 (8.46) 188 (6.33) 0.30
• only males considered•• Chi square/Fisher's exact .test done
••• Difference significant
Q)300c
Q)
tU>Q)•...o,Q)
20CJ)CO-CCD0•...Q)Q.
10
40
O~~~--~--~----r---~--~---o 20 40
Age in Years60
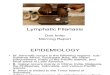
FIG 1. Age-specific prevalence of disease in microfilaraemicand amicrofilaraemic population (Group I)

PANI a al: : BANCROITIAN FILARIASIS IN RELATION TO MICROFILARAEMIA AND DEC THERAPY 11
TABLE II. Comparison of clinical manifestations between microfilaraemic females andmales (Group II)
Clinical Males Females pvalue Age (years) mfcountmanifestations ~ n=m- (') Range Median Range Median
(%ofn) (%ofn)
SpecificA. AcuteFilarial fever 26(4.6) 16(3.0) 0.21 7-58 24 1-45 3.5Lymphangitis 14(2.5) 17(3.2) 0.61 6-60 19 1~ 4Funiculitis 6(1.1) 21-37 23.5 2-46 5.5Epididymo-orchitis 11(1.9) 15-46 32 1-46 6
B. ChronicLymphoedema 4(0.9) 14(2.6) O.OIt 12-74 35 1-44 3Hydrocele 58(10.2) 15-76 39.5 1-90 3.5Lymph varix 3(0.5) 1(0.2) 0.33 24-43 30 1-5 2.5Scrotum lymph 1(0.2) 54" 29"Chyluria 12(2.1) 15(2.8) 0.65 12-74 30 1-49 8
Non-specificLymphadenitis 143(25.3) 293(54.6) o.oOt 5-76 20 1-211 4
• Significant difference between males and females done using Chi square/Fisher's exact test•• Single caset Difference significant
TABLE III. Distribution of symptomatic and asymptomatic mFcarriers according to mf count (Group II)
mf Symptomatic Asymptomaticcount Male Female Male Female
<10 85 45 328 353
Male11-20 12 10 66 6421-30 5 2 25 3031-40 3 I 9 14>41 8 2 25 16
Total 113 60 453 477
40
30Q)-IIIa:Q)ClIII- 20cQ)o...Q)o,
10 Female
o ~~h----.----~---.----~---.--o 20 40
Age in Years60
FIG 2. Disease rates in female and male microfilaria carriers(Group II)
manifestations of filariasis were recorded in 27 mf carriers(13.4%) and in 405 (13.6%) amicrofilaraemic persons(12=0.005; p=0.98). The comparison of the clinicalspectrum in the two groups is shown in Table I. The age-specific patterns of disease prevalence of the mf carriers
and amicrofilaraemic persons (Fig. 1) showed a clear agedependent rise in both groups and there was no significantdifference in any age class (p>0.05).
Of the 1103 mf carriers in group II,,173 (15.7%) hadmanifestations of disease and there was no significantdifference between the disease rate in this group and thatin the mf carriers of grpup I (X2=0.50; p=0.47). Thedisease rate in females (11.2%) was significantly lower(12=15.45; p=O.OOOI) than males (20%). There was asignificant difference in the occurrence of lymphoedemaand lymphadenitis between males and females (Table II).Age-specific disease rates (Fig. 2) were similar in bothsexes and showed a monotonic rise till about 30 years. Asignificant difference in disease rates between the sexeswas observed in persons over 40 years of age (p<0.05).
The age-specific patterns of individual manifestations(Fig. 3) showed that lymphangitis was common in childrenand there was also a distinct age dependent monotonicincrease in the, hydroceles. Lymphoedema appearedearlier in females than males (Fig. 3, Table II) and therewas no association between mf density and clinical out-come (Table III) in either sex (males: z=0.1846,

12
151413121110
••7•5 1432I
• 0
ii 0
a::•aIII
30-C• ae 21
" 24Q.222011
"141210
••420
0 20
THE NATIONAL MEDICAL JOURNAL OF INDIA
1514
A. MALE ACUTE 1312 1II
10
••7•
2 I4:I2
1 I
00
30
C. MALE CHRONIC 2.21
4 24222011I.
1411210.
:~5 :~
eo 0
Age In Years
B. FEMALE ACUTE
20
D. FEMALE CHRONIC
FIG3. Age-specific patterns of acute and chronic manifestations in mf carriers (Group II: Lymphangitis 1,Filarial fever 2, Funiculitislepididymo-orchitis 3, Hydrocoele 4, and Lymphoedema 5)
TABLE IV. Age-specific mean mf counts among symptomatic and asymptomatic carriers(Group II)
Male FemaleAgeclass Symptomatic Asymptomatic Symptomatic Asymptomatic(in years) mean±s.e mean±s.e mean±s.e mean±s.e
0-14 12.7±S.82 10.3±1.43 10.8±2.99 13.4±1.4215-29 10.2±2.S7 9.7±1.l0 7.6±2.07 8.9±1.l730-44 11.l±3.24 11.5±2.0S 6. I± 1.53 8.3±1.29>45 10.3±2.60 11.0±1.96 8.4±4.34 7.5±1.23
Total 10.7±1.S6 10.3±0.74 7.9±1.26 9.6±O.75
Comparison of mean mf counts between symptomatic and asymptomatic for both sexes in each class was notsignificant(t-independent test, p>O.05).
TABLE V. Comparison (%) of mf carriers positive for different clinical manifestations in relation tomf count (Group II)
mf Sample Filarial Lymphangitis Funiculitis Epididymo- Hydrocele Lymphoedema Chyluriacount size fever orchitis
~10 811 4.19 2.71 0.97 1.94 11.14 1.60 2.2211-20 152 3.29 3.29 1.28 2.56 5.13 1.97 2.6321-30 62 3.23 3.23 0.00 0.00 3.33 0.00 1.6131-40 27 0.00 3.70 0.00 0.00 16.67 3.70 0.00~41 51 1.96 1.96 3.03 3.03 15.15 1.96 7.84
Total 1103 3.81 2.81 1.06 1.94 10.25 1.63 2.45
VOL. 4, NO.1
2
5

PANI ~I al. : BANCROFrlAN FILARIASIS IN RELATION TO MICROFILARAEMIA AND DEC THERAPY 13
p=0.4268; females: z=0.4937, p=0.3108). The mean mfcounts in different age classes did not show any significantdifference between symptomatic and asymptomaticindividuals (Table IV). There was no significant difference(p>0.05) in the occurrence of any individual manifesta-tion below and above an mf count of 20 (Table V).
Clinical consequences of long term changes in mf statusand DEe therapyAll mf carriers detected in the pre-control survey in 1981were referred to the local filariasis clinic under the stateauthorities for treatment, since chemotherapy was notdone under the IVM programme. However, only a smallproportion of these mf carriers received one course ofDEC.12.16Though not intended, this gave us an opportunityto examine the clinical consequences in relation tochanges in mf status and DEC therapy over the five-yearperiod.
Of the 1024 persons in group III (examined for mfstatus both in 1981 and 1986),293 were microfilaraemic in1981. Treatment details were available for 286 of these-(a) 207 (73%) had not received DEC, (b) 61 (21%) hadreceived a single course of D EC (6 mg/kg of body weigh tfday for 21 days), and (c) 18 (6%) discontinued DEC(between the second and fifth day) due to its side-effects.The disease rates in these three categories were 10.6%,14.8% and 22.2% respectively and were significantlydifferent (a v. b: 12=0.432, p=O.Sl; a v. c: Fisher'sp=0.14; b v. c: Fisher's p=0.34). Application of log oddsratio also did not reveal any significant difference in theabove categories (z<1.96, p>O.OS).
The 1024 persons in group III were classified into 4 subgroups: (a) mf positive both in 1981 and 1986 (n=155),(b) mf positive in 1981 but negative in 1986 (n= 138),(c) mf negative both in 1981 and 1986 (n=613), and(d) mf negative in 1981 but mf positive in 1986 (n= 118).
In these subgroups 12.3%,12.3%, 12.4% and 14.4%respectively had developed clinical manifestations withinthe five-year period. Comparison of the occurrence ofdisease between subgroup 'c' and the other subgroups didnot reveal any significant difference in disease rates (c v.a: 12=0.007; p=0.92; c v. b: 12=0.01; p=0.91; c v. d:'XP=O.20; p=0.65). The acute disease rates were 3.2%,5.8%,4.9% and 5.4%, and the chronic disease rates were9.0%,5.8%,7.5% and 8.5% respectively and these alsodid not show any significant difference (p>O.OS). Appli- .cation of log odds ratio test for the above analyses did notshow any significant difference for total, acute or chronicdisease (z<1.96; p>0.05).
DISCUSSIONThe results of the present study indicate that the prevalenceof filarial disease was related to the age of the person butneither to mf status (group I) nor the mf counts (group II).Previously it had been believed that clinical manifesta-tions could be related to the age and mf count. 17However,studies on sub-periodic Bancroftian filariasis in Tonga"and on periodic Wuchereria bancrofti in Haiti" had shownthe occurrence of disease to be independent of mf status.
The chronic manifestations of lymphatic filarial infec-
tion are believed to be due to the presence of adultworms 19 and mf apparently have no role in theirpathogenesis-". Using a mathematical model it has alsobeen 'shown that non-fecund infections (single worm!single sex) could result in the development of disease,"which would imply that microfilaraemia is not alwaysessential to produce disease manifestations. The presentstudy suggests no direct relation of mf status on clinicalmanifestations. However, its possible role in. thepathogenesis of chronic manifestations cannot be ruledOUt.21
Neither the changes in mf status nor treatment withDEC over a five-year period influenced the occurrence ofdisease. Though statistical analyses did not show anysignificant difference, those who received D EC (partial orcomplete course) therapy, recorded higher disease ratesthan those who did not receive DEC at all. The long termadverse effects of DEC on onchocerciasis are wellrecorded but there is no specific report of such effects inlymphatic filariasis. to It has been observed that someasymptomatic mf carriers develop clinical manifestationsfollowing DEC therapy. 22Similar observations have alsobeen made at the VCRC clinic (unpublished data). Astudy on the long term effects of DEC on patients withlymphoedema due to both Bancroftian and Malayanfilariasis has shown that while in some cases there wasregression of the oedema volume, in others it increased inspite of therapy. 1.23 Thus the exact mode of action and theprophylactic value of DEC are still not clear. 24The clinicalconsequences of infection and DEC therapy in mf carriersmay, therefore, depend on several other factors includinghost immune status, degree of exposure to infective vectorbites and these may vary from individual to individual.Simultaneous clinical, parasitological, immunologicaland chemotherapeutic studies in an endemic populationneed to be carried out to understand the complexdynamics of infection and disease manifestations offilariasis.
REFERENCES1 Anonymous. Filariasis in India. Natl Med J India 1990;3:1~.2 Fourth report of the WHO expert committee on filariasis. Lymphatic
filariasis. WHO Tech Rep Ser 1984;702:16-25.3 Ottesen EA. Introduction. In: Filariasis. Ciba Foundation
Symposium. 1987;127:1~.4 Hairston NG, Jackowski LA. Analysis of the Wuchereria bancrofti
population in the people of American Samoa. Bull WHO1968;38:29-59.
5 Ottesen EA. Immunological aspects of lymphatic filariasis andonchocerciasis in man. Tram R Soc Trop Med Hyg 1984;78 (suppl):9-18.
6 Raccurt CP, Mojon M, Hodges WHo Parasitological, serological,and clinical studies of Wuchereria bancrofti in Lirnbe, Haiti. Am JTrop Med Hyg 1984;33:1124-9.
7 Udonsi JK. Bancroftian filariasis in the Igwun Basin, Nigeria. Anepidemiological, parasitological, and clinical study in relation to thetransmission dynamics. Acta Tropica 1988;45:171-9.
8 Rao CK, Sen T, Narasimhan MVVL, Krishna Rao C, Sharma SP.Variation in clinical pattern of Bancroftian filariasis in Kerala andUttar Pradesh. J Commun Dis 1977;9:203-5.
9 Pani SP, Krishnamoorthy K, Rao AS, Prathibha J. Clinical manifes-tations in Malayan filariasis infection with special reference tolymphoedema grading. Indian J Med Res (A) 1990;91:200-7.
10 Ottesen EA. Efficacy of diethylcarbamazine in eradicating infec-

14
tion with lymphatic-dwelling filariae in humans. Rev Infect Dis1985;7:341-56.
11 Rajagopalan PK, Das PK, Subramanian S, Vanamail P. RamaiahKD. Bancroftian filariasis in Pondicherry, South India. 1. Pre-control epidemiological observations. Epidemio! Infect 1989;103:685-92.
12 Subramanian S, Pani SP, Das PK, Rajagopalan PK. Bancroftianfilariasis in Pondicherry, South India. 2. Epidemiological evaluationof the effect ofvector control. Epidemiollnfect 1989;103:693-702.
13 Vanamail P, Subramanian S, Das PK; et al. Estimation of age-specific rates of acquisition and loss of Wuchereria bancrofti infec-tion. Trans R Soc Trop Med Hyg 1989;83:689-93.
14 World Health Organisation. Lymphatic pathology andimmunopathology in filariasis: Report of the twelfth meeting of thescientific working group of filariasis. TDR/F1L-SWG (12)/85.31985:1-33.
15 Snedecor GW, Cochran WG. Statistical Methods. lowa:lowa StateUniversity Press, 1967:246.
16 Vanamail P, Subramanian S, Das PK, Pani SP, Rajagopalan PK.Estimation of fecundic life span of Wuchereria bancrofti from alongitudinal study of human infection in an endemic area ofPondicherry (South India). Indian J Med Res (A) 1990;91:293-7.
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. 4, NO.1
17 Kimura E, Penaia L, Spears GFS. Epidemiology of sub periodicBancroftian filariasis in Samoa 8 years after control by mass treat-ment with diethylcarbamazine. Bull WHO 1985;63:869-80.
18 Desowitz RS, Berman SJ, Puloka T. Hyperendemic subperiodicBancroftian filariasis: A search for clinical and immunologicalcorrelates of microfilaraemia. Bull WHO 1976;54:565-71.
19 Partono F. The spectrum of disease in lymphatic filariasis. In:Filariasis. Ciba Foundation Symposium. 1987;1l7:15-31.
20 Raghavan NGS. Clinical features and some epidemiological aspectsof filariasis in India. J Commun Dis 1976;1:189-92.
21 Pattanayak S, Arora DD, Das M. Clinical manifestations,pathogenesis and chemotherapy in filariasis. J Commun Dis1969;1:45-53.
22 Turner LH. Studies on filariasis in Malaya. Treatment ofWuchereria malayi filariasis with diethylcarbamazine in single dailydoses. Ann Trop Med Parasito/1959;S3:180--8.
23 Pani SP, Krishnamoorthy K, Pratibha J, Rao AS. Diethylcarbamazineand supportive measures for the treatment of Brugian filariasis. NatlMed J India 1989;2:2ID-3.
24 Subrahmanyam D. Antifilarials and their mode of action. In:Filariasis. Ciba Foundation Symppsium. 1987;1l7:246-64.
Tcelllymphomas in north Indian adults: Clinical features,diagnosis and treatment outcome in 20 patientsP. BAMBERY, B. KUMAR, S. .vARMA, U. KAUR, S. SEHGAL,S. KAUR, S. D. DEODHAR
ABSTRACTMalignant diseases of T lymphocytes in adults are uncommon.Special difficulties arise both in establishing a diagnosis and intherapy. We describe our experience with 20 patients admittedto the Nehru Hospital, Chandigarh between 1980 and 1989.They had mycosis fungoides (8), Lennert's lymphoma (3),lymphoblastic lymphoma (8) and human T Iymphotrophic virus 1related adult T cell lymphoma (1). All patients had advanceddisease at the time of presentation and were prescribedchemotherapeutic regimens which they could afford. Their
Postgraduate Institute of Medical Education and Research,Chandigarh 160012, India
P.BAMBERY, B.KUMAR, S.VARMA, U.KAUR, S.SEHGALS. KAUR, S. D. DEODHAR Departments oflnternal Medicine,Dermatology, Experimental Medicine and Immunopathology
Correspondence to P. BAMBERY Department oflnternal Medicine
© The National Medical Journal of India 1991
outcome was poor; most patients died within a year of firstbeing seen.
Treatment of patients with T cell lymphomas in India ishampered by the late presentation of patients and the cost of thenewer, more effective chemotherapeutic regimens.
INTRODUCTIONMalignant disorders of T lymphocytes exhibit remarkablediversity in clinical manifestations.' The course of thedisease may end fatally within a few months? or last for afew decades.! The diagnosis is important because theseconditions often do not provide for long term survivaleven though the initial response to chemotherapy may beencouraging.' The common origin from T cells, of severalunrelated malignancies, has been demonstrated onlyrecently.' We describe our experience with the diagnosisand treatment of 20 patients with malignant Tcell disease.
























![Filariasis by Cj[1]](https://img.pdfslide.us/doc/110x75/577cdbff1a28ab9e78a9973c/filariasis-by-cj1.jpg)


