Embed Size (px)
Citation preview

Endemic Bancroftian Filariasis in Thailand: Detectionby Og4C3 Antigen Capture ELISA and the PolymeraseChain Reaction
SURANG NUCHPRAYOON, M.D., M.P.H., Ph.D.*,SONGPUN SANGPRAKARN, B.Sc.*,
SUTIN YENTAKAM*,ALISA JUNPEE, B.Sc.*
Abstract
Lymphatic filariasis, mainly caused by Wuchereria bancrofti and Brugia malayi, has beentargeted for elimination by the World Health Organization by the year 2020. To achieve this goal,highly sensitive and specific diagnostic tests are necessary for close monitoring and evaluation ofthe control program. We employed an ELISA to detect the Og4C3 antigen and a polymerase chainreaction-basedassay for diagnosis of W bancrofti infection, among the Thai-Karen population in Takprovince, Thailand. We found that this endemic area had a microfilarial rate of 10 per cent, whilethe antigen assay could detect cases about two fold as many (23%). The repeated PCR for the detec-tion of Ssp I of W.bancrofti was positive in 12 per cent of the population under this study. Our dataemphasizethe need for using highly sensitive and specific assays for assessment of the real burden ofthe disease.
Key word: Wuchereria bancrofti, Ssp I repeat, Og4C3 Antigen, PCR, Antigen Detection Assay
NUCHPRAYOON S, YENTAKAM S,SANGPRAKARN S, JUNPEE AJ Med Assoc Thai 2001; 84: 1300-1307
Lymphatic filariasis has been estimated toaffect more than 120 million people in endemiccountries(1). More than 90 per cent of the diseaseburden is due to Wuchereria bancrofti. The diseasehas been targeted by the Wodd Health Organizationfor elimination as a public health problem by theyear 2020(2). In Thailand, as assessed by using a
conventional microscopic method which has lowsensitivity, the disease has been controlled to theprevalence of 0.99 per 100,000 population(3). Forbancroftian filariasis in Thailand, the active trans-mission areas are limited to 3 provinces (Tak, Kan-janaburi, and Mae-Hong-Son) bordering Thailandarid Myanmar. To achieve the goal to eliminate the
* Department of Parasitology, Faculty of Medicine, Chulalongkom University, Bangkok 10330, Thailand.

Vol.84 No.9 BANCROFflAN FILARIASIS IN THAILAND 1301
disease, it will be necessary for a lymphatic fila-riasis control program to assess the real burden of thedisease. Part of the control strategies will includeannual mass treatment with diethylcarbamazine andivermectin or albendazole(4). Therefore, evaluationof infection in communities is necessary beforeinitiating mass treatment(5). Close monitoring andassessment of the intervention programs requirehighly sensitive and specific diagnostic assays.
The routine method for diagnosis of lym-phatic filariasis is to detect microfilariae in peri-pheral nocturnal blood by microscopic method. Thistime-consuming and tedious method is difficult todifferentiate one filarial species from another(6).Furthermore, conventional para,>itologicalproceduresfail to identify amicrofilaremic infections or indivi-duals with very low microfilaria levels(7). Assaysthat detect circulating W. bancrofti antigen can alsodetect nocturnal periodic infections in day blood, aswell as other occult infections(8,9). The Og4C3monoclonal antibody has been used to diagnosemicrofilaremicindividuals, as well as amicrofilaremicindividuals, with high specificity and sensitivity(9-11).
A polymerase chain reaction (PCR)-basedassay for diagnosis of W. bancrofti infectio~ usingspecies-specific deoxyribonucleic acid (DNA)probes, has been reported by several authors(12-14).Subsequently, a very sensitive and specific PCR,based on a highly repeated DNA sequence (Ssp Irepeat), has been developed(15).The PCR can detectW. bancrofti genomic DNA in blood samples(16),mosquitoes(17-19), as well as in paraffin-embeddedtissues(20), and urine samples(21).
We describe here the assessment of ban-
croftian filariasis in an endemic area of Thailand byusing the ELISA for Og4C3 antigen and a PCR-based assay to detect W. bancrofti DNA in bloodsamples collected from Thai-Karenpopulation, livingin the endemic area of Tak province, Thailand.
MATERIAL AND METHODStudy areas and populations
Recruited for the study were 196 Thai-Karens residing in Mae Chan sub-district, Umphangdistrict, Tak province, at the Thai-Myanmar border.The Umphang district is 60 km from Mae Sot dis-trict of Tak province. The Vector-borne DiseasesControl Center is located in Mae Sot 500 km north-
west of Bangkok. The study was organized in f;:OOpe-ration with the Filariasis Division, and the Vector-
borne Diseases Control Center 18 (Mae Sot dis-trict), Department of Communicable Disease Con-trol, Ministry of Public Health, Thailand. As almostnone of the Thai-Karens speak and read Thai orEnglish, verbal informed consent was obtained fromeach individual, or parents or guardians of childrenrecruited in the study, in the presence of two wit-nesses. We had a translator for Thai and Karenlanguages for the communication. Each individualwas informed as to the purpose and scope of thestudy. Individuals were also educated about lym-phatic filariasis and how to prevent the disease.Individuals who were microfilaremic were treated
with standard treatment (diethylcarbamazine, DEC).This study was approved by the Ethics Committeeof the Faculty of Medicine, Chulalongkorn Univer-sity, Bangkok, Thailand.
. Collection of specimensCollection of blood specimens was per-
formed as previously described(19,22,23). Two tofive ml of blood samples were collected from eachindividual between 8.00-12.00 p.m. Approximately60 III of blood samples were smeared onto micro-scope slides in duplicate, air-dried and stained withGiemsa's stain. Identification of the parasite specieswas established. All of the microfilaria-positivespecimens were the larvae of W. bancrofti.
Detection of specific Og4C3 antigenThe ELISA for detecting and quantifying
the W bancrofti-specific Og4C3 antigcm was per-formed according to the manufacturer's instructions(Trop-Ag W bancrofti, lCU Tropical BiotechnologyPty Ltd, Townsville, Queensland, Australia). Theassay was performed on the polystyrene 96-wellmicrotiter plates coated with Og4C3 monoclonalantibody that was blocked with nitrogen casein. Onehundred microliters of each serum sample was boiledwith 300 III of sample diluent (0.1 M Na2EDTA,pH 4.0) for 5 minutes. After centrifugation, thesupernatant was recovered and 50 III was added toeach well, and kept in a humid container at roomtemperature for 90 minutes or at 4.C overnight.After washing with 0.01 M Phosphate bufferedsaline with Tween 20, pH 7.4 (PBS, 0.05% Tween20), 50 III of diluted anti-Onchocercaantibody wereadded to each well and kept at room temperature for1 hour. After another wash, 50 III of diluted sheepanti-rabbit immunoglobulin-horseradish peroxidase(HRP) conjugate were added to each well. The sam-

1302 S. NUCHPRAYOON et al.
pIe, hyperimmune rabbit antibody, and conjugatewere each diluted with a blocking solution (PBSrr,0.5% high nitrogen casein). Plates were kept atroom temperature for one hour. After washing, 100III of ABTS substrate was added to each well. Theplates were kept at room temperature for 30 minutes.The reaction was stopped with 50 III of 2N H2S04'The absorbance was read spectrophotometrically at405 nm. The positive samples had antigen titersmore than 100 units/ml.
Extraction of parasite DNA from blood samplesThe DNA was extracted as previously des-
cribed(24). Briefly, 100 III of human blood wasmixed with 500 III of TE buffer and centrifuged.Thepellet was then washed with 500 III of TB buffer,resuspended in 500 III red-cell-lysis buffer (RCLB)and incubated for 5 min to lyse red blood cells.After centrifugation, the red blood cells digestionstep was repeated, then resuspended in 200 III ofDSP buffer (20 mM Tris, pH 8.0, 50 mM KCl, 2.5
mM MgC12'0.15 mg/ml Proteinase K, 0.5% Tween20). Incubation in DSP was performed at 60°C for3 h to lyse the microfilariae and release the DNA.The proteinase K in DSP was then inactivated byincubating the samples at 90°C for 10 min. Follow-ing brief centrifugation to pellet debris, the super-natant was kept for PCR analysis.
The polymerase chain reactionThe PCR was performed with 1 or 2 III of
the extracted DNA as template in a final volumeof 50 Ill. The reaction included 2 units of Taqpolymerase, 400 pM each of NVl and NV2 pri-mers, and 200 IlM of each deoxynucleotide tripho-sphate in 50 mM KCl, 10 mM Tris-HCl, pH 9.0,0.1 per cent Triton X-lOO, and 1.5 mM MgC12'
J Med AssocThai September 2001
The sequences of NV1 and NV2 were 5'-CGTGATGGCATCAAAGTAGCG- 3' and 5'-CCCTCACTTACCATAAGACAAC- 3', respectively. TheDNA was denatured at 94°C for 5 min, followedby 35 cycles of 1 min at 94°C, 1 min at 55°C, 1min at noc, and a final 10 min extension at noc.The 188bp PCRproduct(SspI repeat)wasresolvedand visualized on a 2 per cent ethidium bromide-stained agarose gel. The positive control DNA wasprepared from adult W. bancrofti (kindly providedby Dr. N Raghavan).
Data analysisData were recorded and analyzed by using
Microsoft Excel 6.0 program. The unpaired t-testwas used to test statistically the significant diffe-rence.
RESULTSCharacteristics of the study population
Among the 196 Thai-Karens living in MaeChan, 114 (58%) were males and 82 (42%) females.The mean age was 28 I 13 (1-69) years. Themajority (53%) of the subjects were in the age group>15-30 years (Table 1). There was a total of 20microfilaremic cases accounting for the prevalenceof 10 per cent. Most microfilaremicindividuals werein the age group >15-30 years (17%) and >30-45years (17%). Women had a slightly higher micro-filarial infection rate than men (11% compared to10%, respectively).
Prevalence of lymphatic filariasis assessed byusing Og4C3 antigenemia
The ELISA for the specific circulatingantigen (Og4C3) to assess the situation of bancrof-tian filariasis in this population identified 44 anti-
Table 1. Microfilaremia and Og4C3 antigenemia in Thai-Karens stratified by age and sex.
Age-group Male Female Total
(years) Total Mf+ Ag+ Total Mf+ Ag+ Total % Mf+ % Ag+ %
S;15 17 1 2 4 0 1 21 11 1 5 3 14> 15-30 56 4 11 49 4 8 105 53 8 8 19 18> 30-45 27 5 9 20 3 6 47 24 8 17 15 32> 45-60 12 1 3 8 2 4 20 10 3 15 7 35>60 2 0 0 1 0 0 3 2 0 0 0 0
Total (%) 114 11 25 82 9 19 196 100 20 10 44 23
Note: Mf+ and Ag+ indicate microfilaremic and antigenemic patients, respectively.

Vol.84 No.9 BANCROFI1AN FILARIASIS IN THAILAND 1303
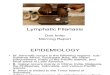
Detection of 188-bp Ssp I repeat by a PCR assay on a 2% ethiduim bromide-stained agarose gel.Lane 1: lOO-bp marker, lane 2: positive control using W. bancrofti genomic DNA, lane 3: negativecontrol using blood sample from non-infected healthy volunteers, lanes 5-8: five representativesamples positive for Ssp I repeat by the PCR.
Fig. 1.
genic cases in total (Table 1). All of the microfila-remic cases were positive for Og4C3 antigenemia.The antigen detection assay was positive for 24individuals in the amicrofilaremic group. The num-ber accounted for a 23 per cent prevalence of anti-genemia (Table 1). The antigen test could detectmore positive cases than the conventional micro-scopic method. The majority of the antigenic caseswere in the age group> 45 -60years (35%). Thosewho were in the age group < 15 years, > 15-30years, > 30-45 years and> 60 years had antigene-mic rates of 14 per cent, 18 per cent, 32 per centand 0 per cent, respectively.
Polymerase chain reaction (PCR) for diagnosisof lymphatic fdariasis
The molecular biology technique usingPCR to detect genetic material, DNA, of infectious
organisms has been used widely. For lymphaticfilariasis, the DNA region named Ssp I repeat wasused in the polymerase chain reaction (PCR) forthe detection of the filarial parasite, Wuchereriabancrofti. The PCR result showed the 188-bp Ssp Irepeat as shown in Fig. 1. All blood samples frommicrofilaremic patients were positive when testedby the PCR. In addition, four more subjects who hadbeen earlier classified in the amicrofilaremic groupwere found positive for the Ssp I repeat. Therefore,the PCR was positive in 12 per cent of the studypopulation.
High Og4C3 antigen levels among microfdare-mic individuals
To study the correlation between the Og4C3antigen level and microfilaremic status, we analysedthe data and it was tested with unpaired t-test. The

1304 S. NUCHPRAYOON et al. J Med Assoc Thai September 2001
Mf+
Fig. 2.
Mf- PCT{+ PCR-
The antigen units classified by microfilaremic status and detection of Ssp I repeat. Mf+: micro-filaremic group, Mf-: amicrofilaremic group, PCR+: Ssp I-positive group, PCR- : Ssp I-negativegroup.
range of the antigen level was 10 - 3,156 units inthe amicrofilaremics, and 439- 321,907 units in themicrofilaremics (Fig. 2). The level of Og4C3 anti-gen among microfilaremics (GM = 11,507 units)was higher than those in amicrofilaremics (GM =23 units) with statistic significance (unpaired I-test,p = 3.9 x 10-11).
For analysis of the PCR results, we foundthat those who were positive for Ssp I repeat alsohad higher antigen levels (14 - 321,907 units; GM =8,359 units) than those who were negativefor theSsp I repeat (l0 - 389 units; GM = 13 units) (un-paired I-test, p = 3.5 x 10-10).
DISCUSSION
The data from the Filariasis Division,Department of Communicable Disease Control,Ministry of Public Health show that Thailand hascontrolled lymphatic filariasis to a prevalence rateof 0.99 per 100,000(3). Our study, however, showed
a much higher microfilarial rate in the endemic areaof Tak province. The microfilarial rate (10%) in aThai-Karen population living in Mae Chan sub-dis-trict, Umphang'district was much higher. Therefore,this endemic area is considered a high-risk areawith active transmission(25). The continuous moni-toring and annual mass treatment as control strate-gies are necessary for the area. Advanced diag-nostic techniques were found useful as indicatorsfot assessment the real prevalence of the disease.The data also indicated that the specific Og4C3antigen assay was a good indicator of an activeinfection. Although the PCR did not detect as manycases as the antigen assay, its detection of theparasite in mosquito vectors has been proved suc-cessful(19).
The PCR did not detect the W. bancrofti-infected cases as high as the antigen detectionassay. Therefore, the PCR for detection of Ssp Irepeat is less sensitive than the Og4C3 antigen
1000000I
Q ID- .100000 6 I
! 8A-- +8 A
10000 X -.. 0"1 )le.':::::: 0
;:J 1000 X:::
I
-()
t)l) ()
":: 100 ,.:::B
10 -1.- . -+-

Vol.84 No. 9 BANCROFTIAN FILARIASIS IN THAILAND 1305
assay. Together with the difficulty in the applica-tion of this technique in the endemic areas, the PCRhas obviously less applicability for the field studythan the antigen detection assay. Another advan-tage of the antigen detection assay is that it directlycorrelated with the current active infection(26).
The high prevalence of bancroftian fila-riasIs assessed by the detection of microfilariae,Og4C3 antigen and Ssp I repeat found among thispopulation deserves considerable attention from thepublic heath community in Thailand. The collecteddata demonstrated the real burden of bancroftianfilariasis as assessed by the Og4C3 antigen assay,which is an indicator of active infection. The highprevalence of the disease in the endemic area in-vites closer monitoring and control strategies forthe disease.
Part of the reason for such a high preva-lence of lymphatic filariasis is that this remote areais difficult to access by health personnel. Further-more, the local villagers are not well educated;being.unaware of its danger and prone to infection.Poverty is another major hindrance preventing thispopulation from access to health care services.
To eliminate the disease successfully,healthpersonnel need to have access to the remote areasas well as to provide health education.
ACKN0 WLEDG EMENTS
This work was supported by ThailandResearch Fund (TRF), and Molecular Biology Pro-gram, Research Affairs, Faculty of Medicine, Chula-longkorn University, and the Special Programmefor Research and Training in Tropical Diseases ofthe World Health Organization (TDR/WHO). Theauthors wish to thank Associate Professor Dr. Som-chai Jongwutiwes, Dr. Saravudh Suwannadabba andMs. Kobkan Kanjanopas for their kind advice. Wealso thank Associate Professor Dr. Apiwat Mutiran-gura for the laboratory facilities, Ms. Junpen Prom-thong, Ms. Kamonwan Chuenta, Ms. Juntharut Krai-nara for their laboratory assistance, and Ms. Kun-wadee Sai-Im for data entry. We also thank all thehealth personnel from the Vector-borne DiseasesControl Center 18, Filariasis Division, Ministry ofPublic Heath, and all the staff at the Department ofParasitology, Faculty of Medicine, ChulalongkornUniversity for their technical support.
(Received for publication on April 28, 2001)
REFERENCES
1. Michael E, Bundy DAP. Global mapping oflymphatic filariasis. Parasitol Today 1997'; 13:472-6. .
Behbehani K. Candidate parasitic diseases. BullWorld Health Organ 1998;76 (Supp12): 64-7.Filariasis Division. Annual Report, Filariasis Divi-sion, CDC Department, Ministry of Public Health,Bangkok, Thailand. 1999 (in Thai).Ottesen EA, Duke BOL, Karam M, Behbehani K.Strategies and tools for the control/eliminationof lymphatic filariasis. Bull World Health Organ1997; 75: 491-503.
Ottesen EA, Ramachandran CP. Lymphatic fila-riasis infection and disease: Control strategies.Parasitol Today 1995; 11: 129-31.Poole CB, Williams SA. A rapid DNA assay forthe species-specific detection and quantificationof Brugia in blood samples. Mol Biochem Para-sitoll990; 40: 129-36.Chanteau S, Plichart R, Spiegel A, Martin PM,Cartel JL. Diagnostic values of ELISA-IgG4 as
2.
3.
4.
5.
6.
7.
8.
compared to ELISA-IgG and indirect immuno-fluorescence, for the routine diagnosis of ban-croftian filariasis in the South Pacific. Applicationon capillary blood collected on filter paper. TropMed Parasitoll991; 42: 339-42.Weil GJ, Jain DC, Santhanam S, et al. A mono-clonal antibody-based enzyme immunoassay fordetecting parasite antigenemia in bancroftian fila-riasis. J Infect Dis 1987; 156: 350-5.Turner P, Copeman B, Gerisi D, Speare R. Acomparison of the Og4C3 antigen capture ELISA,the Knott test, an IgG4 assay and clinical signs,in the diagnosis of bancroftian filariasis. TropMed Parasitoll993; 44: 45-8.More SJ, Copeman DB. A highly specific andsensitive monoclonal antibody-based ELISA forthe detection of circulating antigen in bancroftianfilariasis. Trop Med Parasitoll990; 41: 403-6.Triteeraprapab S, Thumpanyawat B, SangprakamS. Wuchereria bancrojti-specific circulating anti-gen for diagnosis of bancroftian filariasis. ChulaMedJ 1998;42: 267-77.
9.
10.
11.

1306 S. NUCHPRAYOON et al.
12. Dissanayake S, Min X, Piessens WF. Detectionof amplified Wuchereria bancrofti DNA in mos-quitoes with a nonradioactive probe. Mol Bio-chem Parasitol1991; 45: 49-51.Theodore JG, Kaliraj P, Jayachandran S, Jaya-raman K. Cloning, over-expression and evalua-tion of a recombinant fusion protein of Wuche-reria bancrofti towards its application as a diag-nostic agent for bancroftian filariasis. Parasito-logy 1993; 106: 413-20.Siridewa K, Karunanayake EH, ChandrasekharanNV, et al. Cloning and characterizationof a repeti-tive DNA sequence specific for Wuchereria ban-crofti. Am J Trop Med Hyg 1994; 51: 495-500.Zhong M, McCarthy J, Bierwert L, et al. A poly-merase chain reaction assay for detection of theparasite Wuchereria bancrofti in human bloodsamples. Am J Trop Med Hyg 1996;54: 357-63.Williams SA, Nicolas L, Lizotte-Waniewski M,et al. A polymerase chain reaction assay for thedetection of Wuchereria bancrofti in blood sam-ples from French Polynesia. Trans R Soc TropMed Hyg 1996;90: 384-7.Chanteau S, Luquiaud P, Failloux AB, WilliamsSA. Detection of Wuchereria bancrofti larvae inpools of mosquitoes by the polymerase chainreaction.TransR Soc Trop Med Hyg 1994;88:665-6.
Nicolas L, Luquiaud P, Lardeux F, Mercer DR.A polymerase chain reaction assay to determineinfection of Aedes polynesiensis by Wuchereriabancrofti. Trans R Soc Trop Med Hyg 1996; 90:136-9.Triteeraprapab S, Kanjanopas K, SuwannadabbaS, Sangprakarn S, Poovorawan Y, Scott AL.Transmission of the nocturnal periodic strain ofWuchereria bancrofti by Culex quinquefasciatus:
13.
14.
15.
16.
17.
18.
19.
J Med Assoc Thai September 2001
20.
establishing the potential for urban filariasis inThailand. Epidemiol Infect 2000; 125: 207-12.McCarthyJS, Zhong M, Gopinath R, Ottesen EA,Williams SA, Nutman TB. Evaluation of a poly-merase chain reaction-based assay for diagnosisof Wuchereria bancrofti infection. J Infect Dis1996; 173: 1510-4.Lucena WA, Dhalia R, Abath FG, Nicolas L,Regis LN, Furtado AF. Diagnosis of Wuchereriabancrofti infection by the polymerase chainreaction using urine and day blood samples fromamicrofilaraemic patients. Trans R Soc Trop MedHyg 1998; 92: 290-3.Triteeraprapab S, Songtrus 1. High prevalenceof bancroftian filariasis in Myanmar-migrantworkers: A study in Mae Sot District, Tak Pro-vince, Thailand. J Med Assoc Thai 1999; 82: 734-9.Triteeraprapab S, Nuchprayoon I. Eosinophilia,anemia, and parasitism in a rural region of north-west Thailand. Southeast Asian J Trop Med PublicHealth 1998;29: 584-90.Williams SA, Nicolas L, Lizotte-Waniewski M,et al. A polymerase chain reaction assay for thedetection of Wuchereria bancrofti in blood sam-ples from French Polynesia. Trans R Soc TropMed Hyg 1996;90: 384-7.Filariasis Division. Elimination program for lym-phatic filariasis. Filariasis Division, CDC Depart-ment, Ministry of Public Health, Thailand 2000(in Thai).Chanteau S, Glaziou P, Luquiaud P, Plichart C,Moulia-Pelat JP, Cartel JL. Og4C3 circulatingantigen, anti-Brugia malayi IgG and IgG4 titersin Wuchereria bancrofti infected patients, accord-ing to their parasitological status. Trop Med Para-sito11994; 45: 255-7.
21.
22.
23.
24.
25.
26.

Vol.84 No.9 BANCROFTIAN FILARIASIS IN THAILAND 1307
1"'L 'r11,n~t 'ULL~~~ 1""n1'1-l'ElUh::L 'Y1fiT1 'Y1!J:
Og4C3 LL~::tJtjffi!J1\1n 1,JI'WaLJ.lElii,s
n1'1U~Q!J1~!J1aD1~~..!
L'WEI~1
ffj'NR U'lflh::!Ij, W.1J., MP. H., lh.~. *, m1U dJurh"1173J*,. . " .mmnnJ LLI:V.:JI.h::nn?'YI.1J.*, fififf7 iJ~un{U, ?'YI.1J. *
hi'lL~l'lil~i1mL'l1(;)'I1~mn'nnw£JlBT1i'lL~l'lil~Wuchereria bancroft! LLG'I::Brugia malay! ~~j:jm1LLw'h::tJlW!< ~T"'T ..I'~ 1" 1.1 1 :'1 1 ..1.'1.J'... 'fl..l
eNi'lm1f)'I.Il),ltlLG'lm-l1.JLtltJltl'Yl"1::nl"'1W! 'I1'11),1W!u11ltl 'I.Iu W.A". 2563 '1.1m 1'Yl"1::m1fj Lul'l1).Jl tI'I.I),Ii'lll),l"1lLu'l.l'Yl"1::
~f)~ml'!tlm11ij"1Qtlyjj:ji'lll),l 11LLG'I::i'lll),l~lLWl::~~1'1.1m1~w!(;1l),lLLG'I::U1::LiJ'I.ITi'l1~nl1i'llUfJ),I T11'l Cdl.rtl1W!1'lflBii1G'1'lfl
1'1.1m1(;111"lLLf)'I.I~L"1'1.1 Og4C3 LLG'I::Hu~n1£Jl'.jnHTw~L),If)fL11;'f1'1.1m11ij"1QtlT11'l~W!L:5f)W£JlBhI'lL~l'lil~ W. bancroft!
1 .1 ..I ~n. ..I'..I..I"'T ~ ~ .1 1 ,...~ .l'
l T::1 ...'I.Iu1::'D'lm'YlmA"tlf)~ 'I.IW'l.l'Yl'Yl),lL1i'l~n~),IL'lI(;1"1~'I11w!(;1ln'lm~u1::LYlA"YltI WUll),lf)W!1lnl1(;111"1WUL'D'f) ),ILI'l1I"1G'1lL1t1 10%
1'1.1'l1ru::yjm1(;111"1LLf)'I.I~L"1'1.11;'fl),ll1()(;111"1m1~W!L:5f)ML.yJ),I~'I.IU1::),Ilru 2 L'Yh (23%) LLG'I::15ulii'i1£Jl'.jflTiTw~L),If.)fL11;'f
(;111"1!'tl'l.l Sspl repeat wuM 12% 'lIm;!G'I~~mhlL1.!'I.I1'f1iii'l.ll'lll),l~lLiJ'I.I.yj"1::~f.)~1'lfl51ij"1QtI.yjj:jl'lll),l11LLG'I::i'l1l),l~lLWl::
~~ 1 'I.Im1u1::Li~'I.Ii:~m'l.lm1ru'1W!tI(;1l),l i'lll),lL iJ'I.I"11~
Ihtlicy : 2!<JfiJL=Jt)!!w'/.Jl'lww11i1, Ssp I repeat, Lm'l.l~L"1'1.1Og4C3, U~n1£Jl'.jflTilw~L),If.)fL1!'1'. m1(;111"1LLf)'I.I~L"1'1.1
CfTloQfi'~""h::(I" f{ilu Liium,n~.
'rI,oQYn1a1LLRuh::rm. Dim iu'rIftJ
'i"'I1~!JL'I1'1moQLL'W'rIrf., 2544; 84: 1300-1307
. mI'11'J1lu'j~~1Y1t1l. I'1ru::LLW'Y1t1l'fl<l~{~~lG'l~f1'jcl).J\111'Y1t11atl. f11~L'Y1W"1 10330










![Filariasis by Cj[1]](https://img.pdfslide.us/doc/110x75/577cdbff1a28ab9e78a9973c/filariasis-by-cj1.jpg)