Embed Size (px)
Citation preview
Classification & Risk Factors for
Diabetes Mellitus
Frank Schwartz, MD FACEProf. of Endocrinology
J O Watson Chair for Diabetes ResearchDirector: The OU Diabetes Institute
Objectives of Lecture
Present an overview of the common forms of Diabetes Mellitus
Review the pathogenesis of each
Describe the risk factors for developing each
Definition of Diabetes Mellitus
A chronic disorder of carbohydrate & fat
metabolism….. due to absolute/or relative deficiency in
insulin secretion……. &/or ineffective biological responses
to insulin….. resulting in hyperglycemia
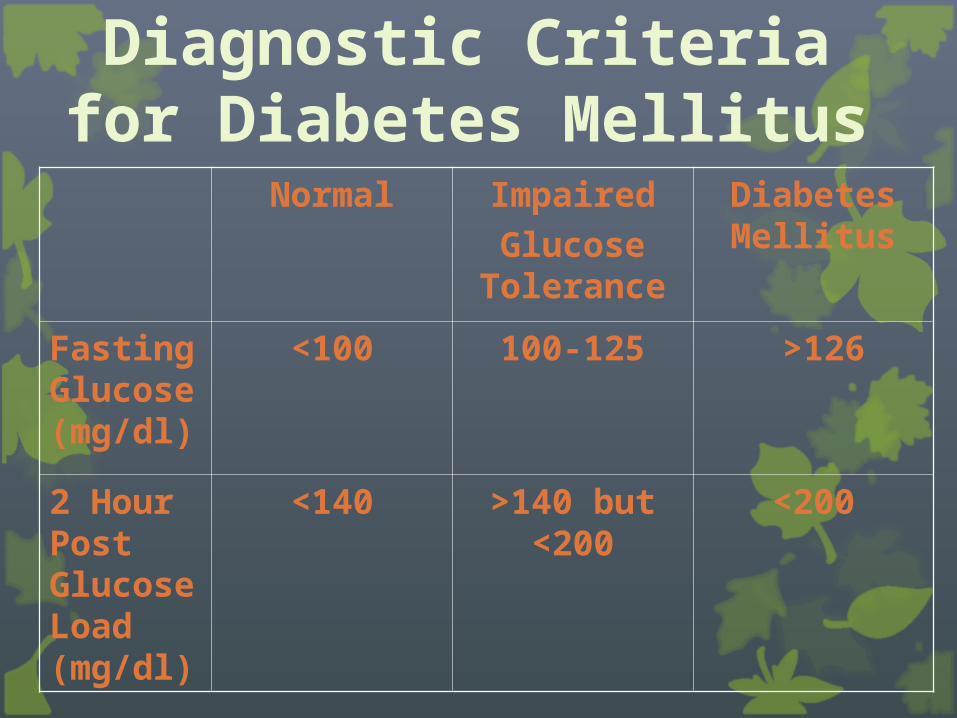
Diagnostic Criteria for Diabetes Mellitus
Normal Impaired
Glucose Tolerance
Diabetes Mellitus
Fasting Glucose (mg/dl)
<100 100-125 >126
2 Hour Post Glucose Load (mg/dl)
<140 >140 but <200
<200
Classification of Diabetes Mellitus
Two Major Forms of Diabetes Mellitus
Type 1 Diabetes (T1DM)-Absolute insulin deficiency resulting from beta-cell destruction….. usually caused by an autoimmune process
Type 2 Diabetes (T2DM) -Biological ineffectiveness of insulin action (Insulin resistance) and/or beta cell secretory defects…..a major factor is thought to be acquisition of visceral obesity in genetically susceptible individuals
Type 1 Diabetes Mellitus (T1DM)
• Caused by beta cell destruction
-Pattern A: autoimmune process-Pattern B: unknown cause (viral?)
• Occurs most commonly during childhood, adolescence, & early adulthood….. but can occur at any age including persons > 40 Latent Autoimmune Diabetes of Adulthood (LADA)
Type 2 Diabetes Mellitus T2DM)
Most common form of diabetes accounting for >90 % of all cases
Occurs most commonly in adulthood, but prevalence in children & adolescents is increasing rapidly
Risk is highly correlated with acquisition of visceral obesity …. resulting in insulin resistance & “relative” insulin deficiency
Other Common Forms of Diabetes Mellitus
Impaired Glucose Tolerance (IGD)-Abnormal glucose levels but not fulfilling criteria for diagnosis of type 2 diabetes-> 50 % risk of going on to develop DM
Gestational Diabetes (GD)-Development of DM during pregnancy which usually resolves following pregnancy
Secondary Diabetes-Glucose intolerance induced by another disease which resolves when condition is treated/corrected
Gestational Diabetes (GD)
Defined as onset of diabetes induced by pregnancy which resolves following the pregnancy
50% life-time risk of progression to T2DM during lifetime
Can be prevented with life-style intervention
Both T1DM & T2DM can also occur during pregnancy
Secondary Diabetes
Diabetes & glucose intolerance induced by another medical
condition, which then resolves following the resolution of that
medical condition
Overlapping Forms of Diabetes Mellitus
Double Diabetes or Diabetes 1.5
• The occurrence of insulin deficiency & insulin resistance in same patient
• Children who have T1DM….but with a family history of T2DM….. are more prone to obesity & insulin resistance
• Tend to have much greater insulin requirements than other patients their age @ which is especially accelerated at puberty
What Causes T1DM?
Pathogenesis of T1DM
Viral or immune cell mediated destruction of β-Cell which results in a rapid or progressive decline in Insulin production
“Immune markers” for T1DM may occur years before the onset of disease
Factors Contributing To Development of T1DM
Genetic susceptibilityEnvironmental triggersAbnormalities in immune
regulation (inherited vs acquired?)
Loss of self tolerance (inherited vs acquired?)
Family History & Risk For Developing T1DM
0.4% occurrence rate in persons with no family history of T1DM
6-11% in offspring of person with T1DM
5% in siblings of person with T1DM
30-40% in identical twins
> 90% of individuals with new-onset T1DM have no family
history!!!
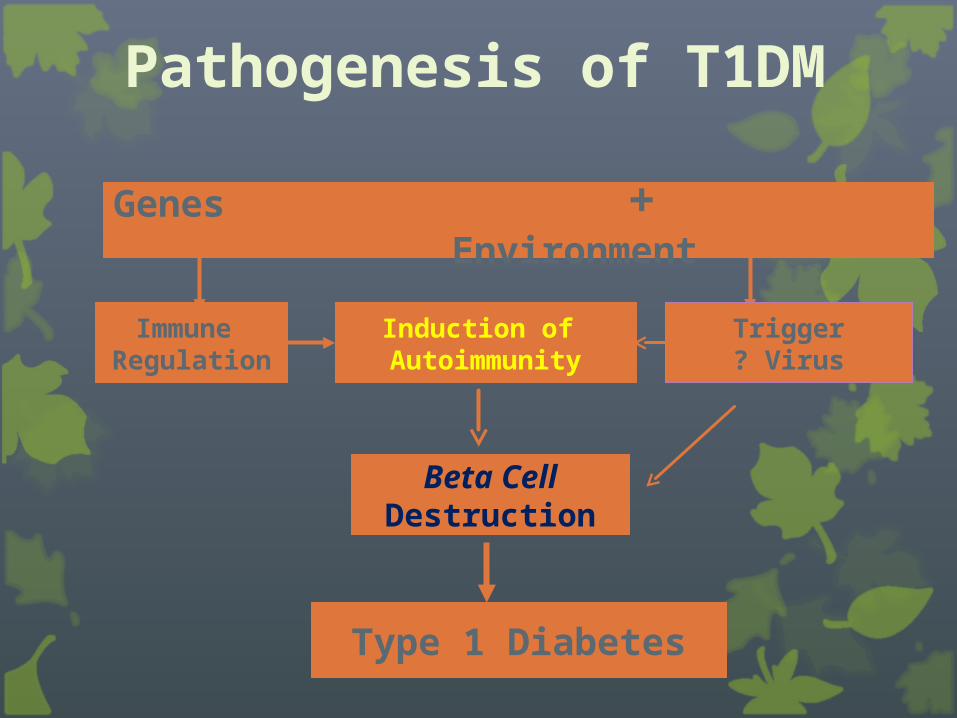
Pathogenesis of T1DM
Genes + Environment
Type 1 Diabetes
Beta Cell Destruction
Induction of Autoimmunity
Immune Regulation
Trigger? Virus
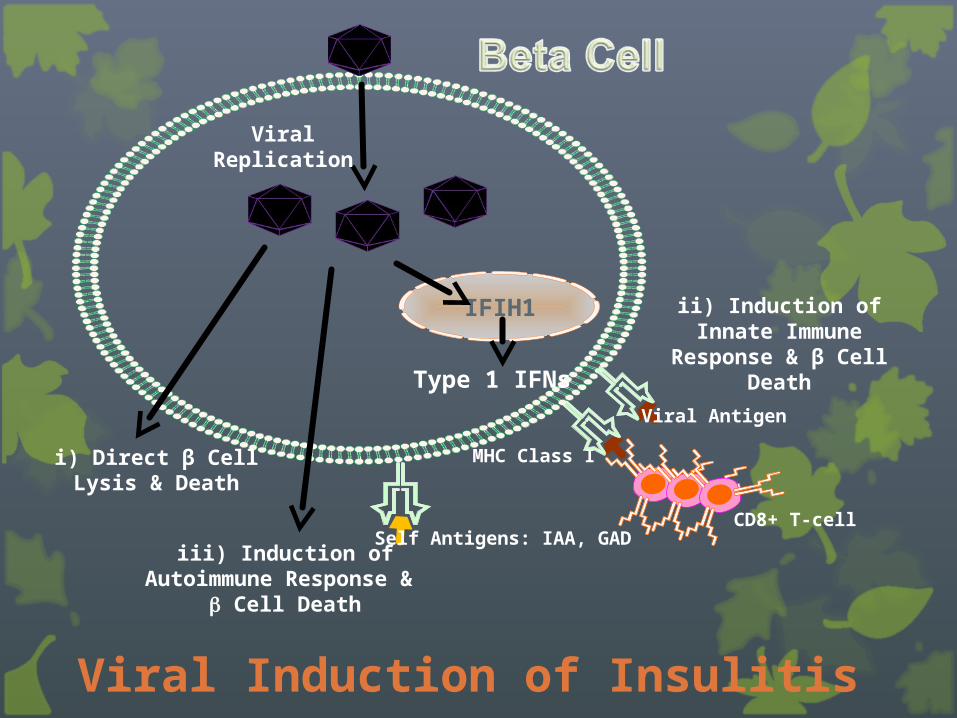
Viral Replication
i) Direct β CellLysis & Death
iii) Induction of Autoimmune Response & Cell Death
IFIH1 ii) Induction of Innate Immune Response & β
Cell DeathType 1 IFNs
MHC Class I
CD8+ T-cell
Viral Antigen
Self Antigens: IAA, GAD
Viral Induction of Insulitis
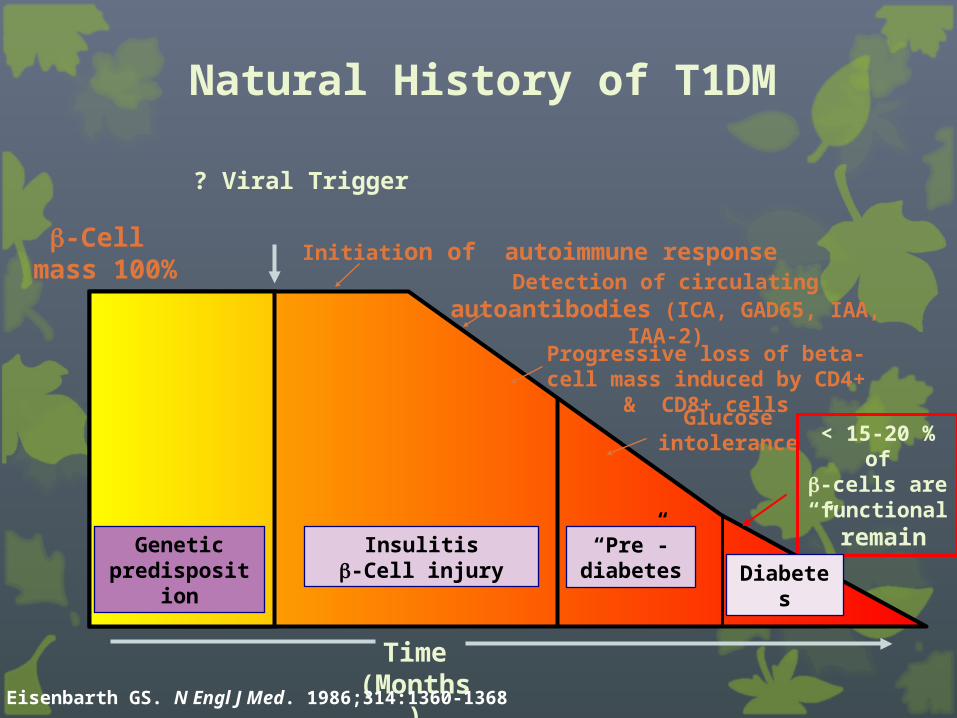
? Viral Trigger
Detection of circulating autoantibodies (ICA, GAD65, IAA, IAA-2)
Initiation of autoimmune response
Progressive loss of beta-cell mass induced by CD4+ & CD8+
cellsGlucose
intolerance < 15-20 % of-cells are
“functional” remain
Time(Months)
-Cell mass 100%
“Pre”-diabetes
Geneticpredisposition
Insulitis-Cell injury
Eisenbarth GS. N Engl J Med. 1986;314:1360-1368
Diabetes
Natural History of T1DM
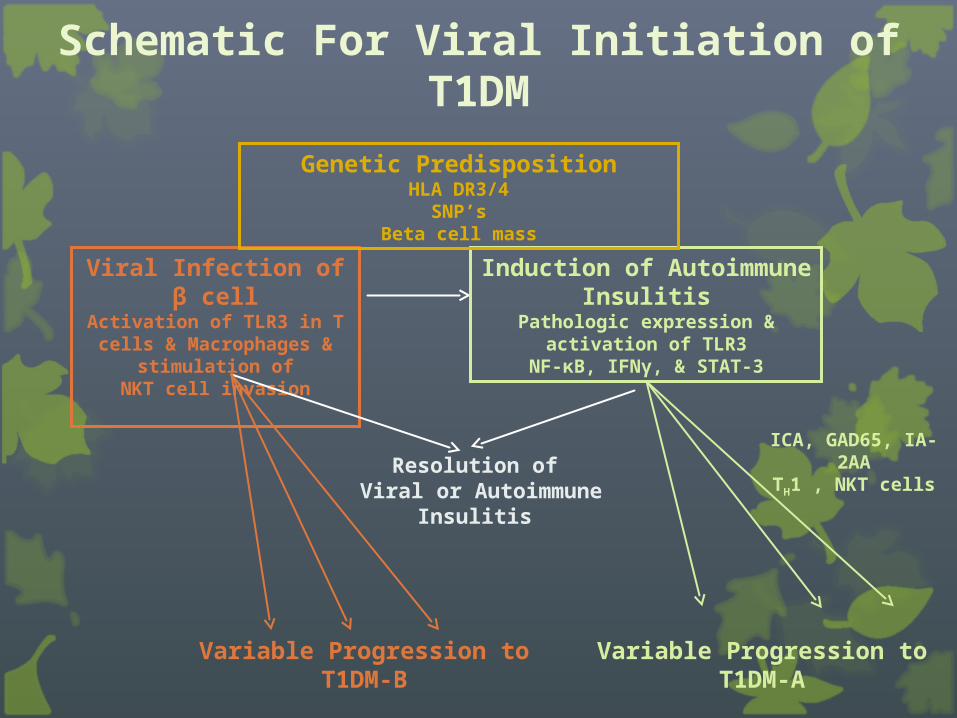
Schematic For Viral Initiation of T1DM
Viral Infection of β cellActivation of TLR3 in T cells
& Macrophages & stimulation of
NKT cell invasion
Variable Progression to T1DM-B
Induction of Autoimmune Insulitis
Pathologic expression & activation of TLR3
NF-κB, IFNγ, & STAT-3
Resolution of Viral or Autoimmune Insulitis
Variable Progression to T1DM-A
Genetic PredispositionHLA DR3/4
SNP’sBeta cell mass
ICA, GAD65, IA-2AATH1 , NKT cells
Prevention of T1DM: How Can We Approach This?
There are no specific genetic markers
Most patients with new-onset T1DM have no family history
Detection of Islet-Cell antibodies (ICA’s) are not 100% specific…. & these are usually only checked in first degree relatives of persons with diabetes
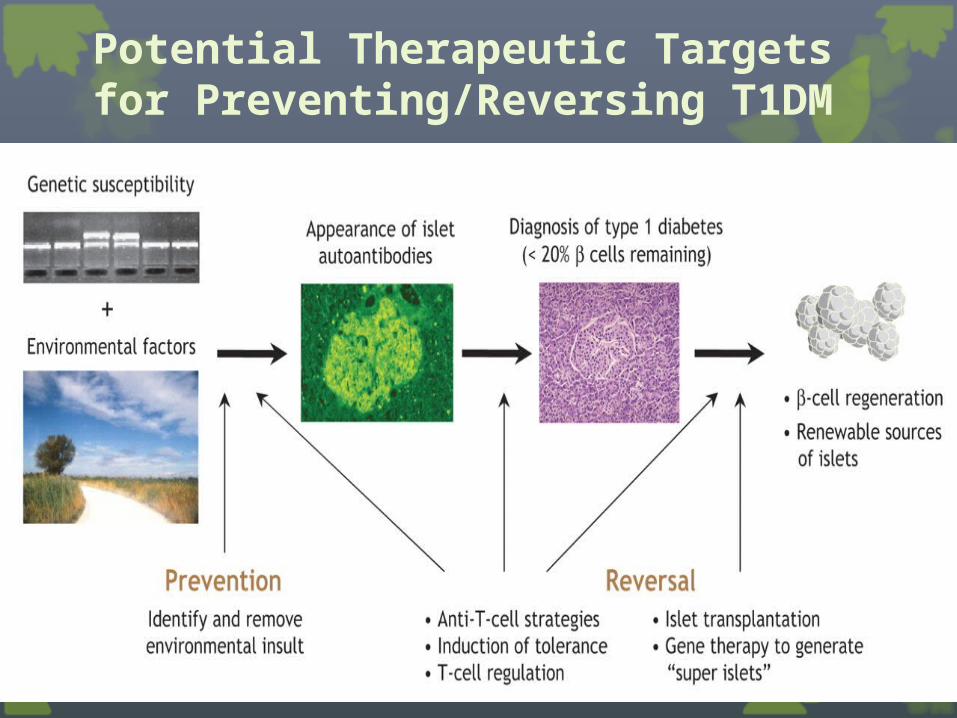
Potential Therapeutic Targets for Preventing/Reversing T1DM
Conclusions
There are at least two patterns of T1DM…one is autoimmune mediated (Pattern A) & the other (Pattern B) is probably viral mediated
Onset of T1DM following initiation of insulitis is variable & spontaneous recovery can occur
These patients require life-long insulin therapy
What Causes T2DM?
Risk Factors for T2DM
Family history/genetics
Obesity
Western life-style
Tobacco use
Lack of exercise
Hypertension & Hyperlipidemia
Gestational diabetes
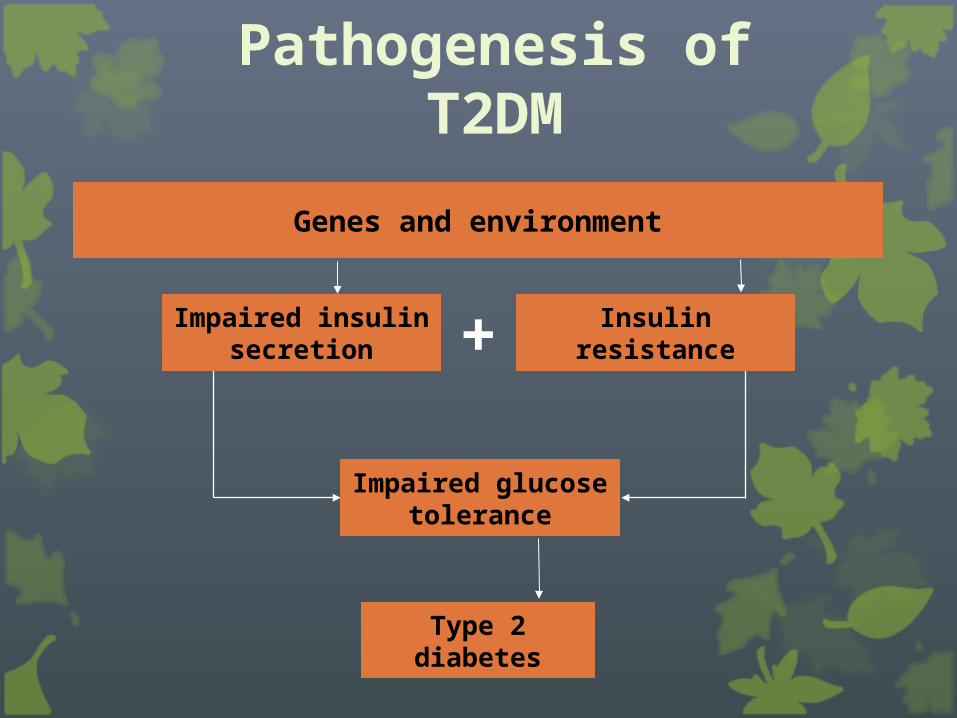
Pathogenesis of T2DM
Genes and environment
Type 2 diabetes
Impaired glucose tolerance
Impaired insulin secretion
Insulin resistance+
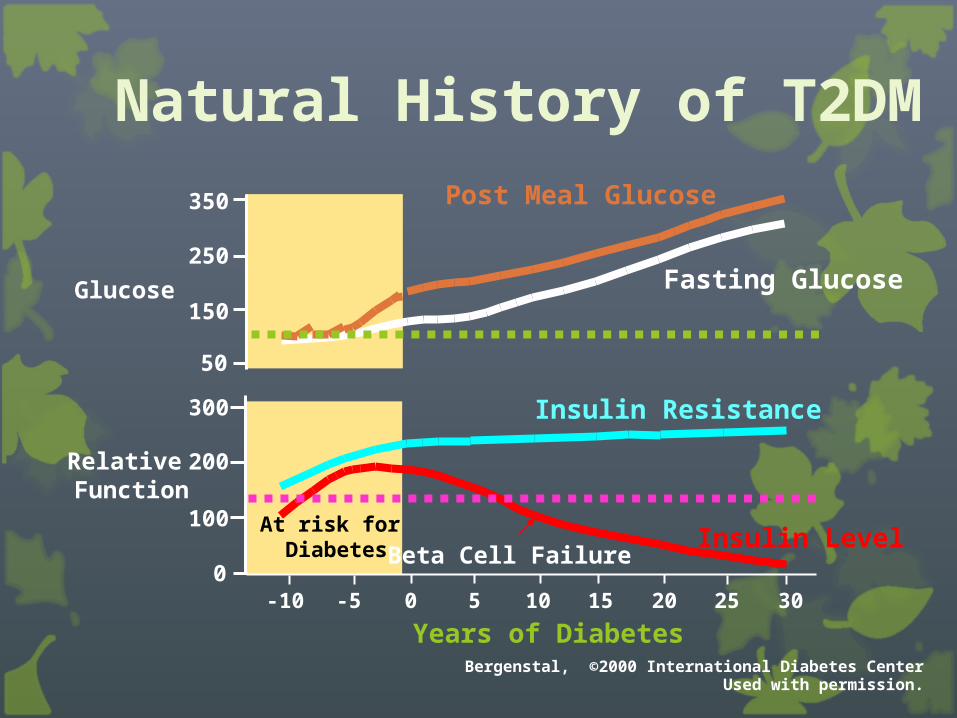
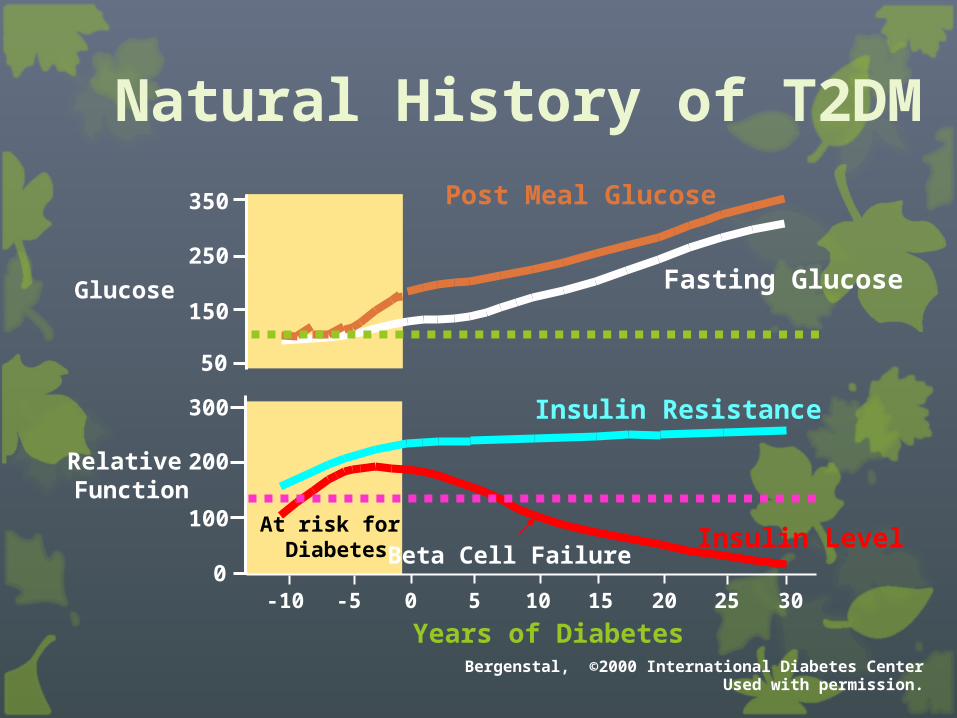
Natural History of T2DM
0
100
200
300
-10 -5 0 5 10 15 20 25 30
50
150
250
350
At risk for Diabetes
Glucose
Relative Function
Post Meal Glucose
Fasting Glucose
Insulin Resistance
Insulin LevelBeta Cell Failure
Years of DiabetesBergenstal, ©2000 International Diabetes Center
Used with permission.
Major Factors Involved In Pathogenesis of T2DM
Insulin Resistance
-Acquisition of visceral obesity…leads to Lipotoxicity, & impaired Insulin signaling
Beta Cell Secretory Defects
-Impaired first phase insulin release
secondary to Lipotoxicity, Glucotoxicity, & loss of Incretion secretion
Visceral Fat Topography
Visceral Fat
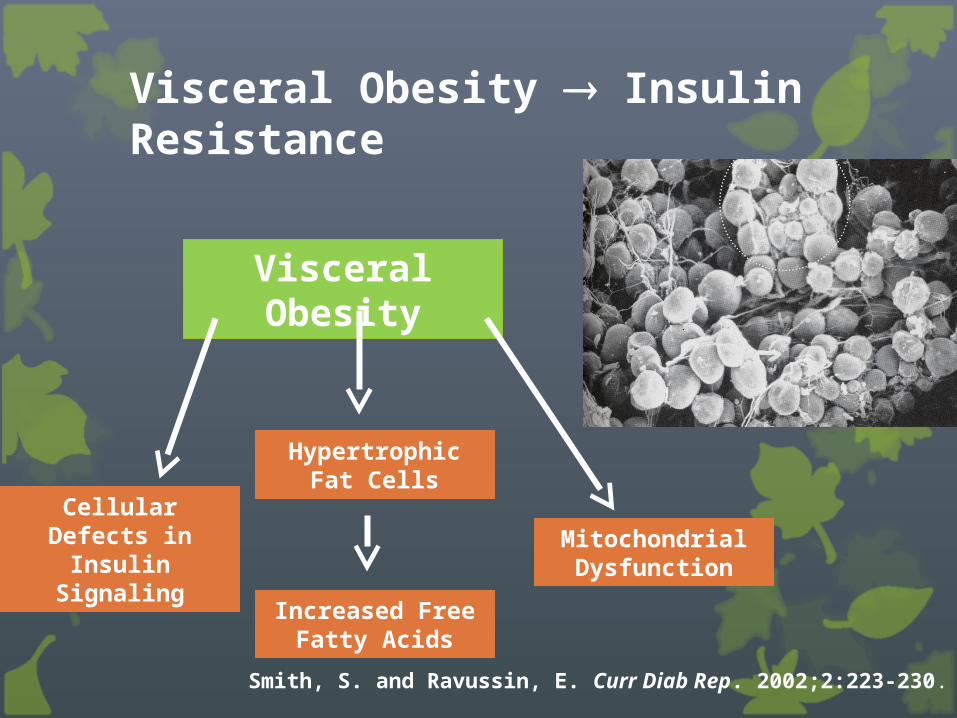
Visceral Obesity Insulin Resistance
Smith, S. and Ravussin, E. Curr Diab Rep. 2002;2:223-230.
Visceral Obesity
Cellular Defects in Insulin Signaling
Hypertrophic Fat Cells
Increased Free Fatty Acids
Mitochondrial Dysfunction
Lipotoxicity
The pathologic changes in organs resultant from elevated fat levels in blood or tissues,
as in the diabetic liver.
http://www.medilexicon.com/medicaldictionary.php?t=50859
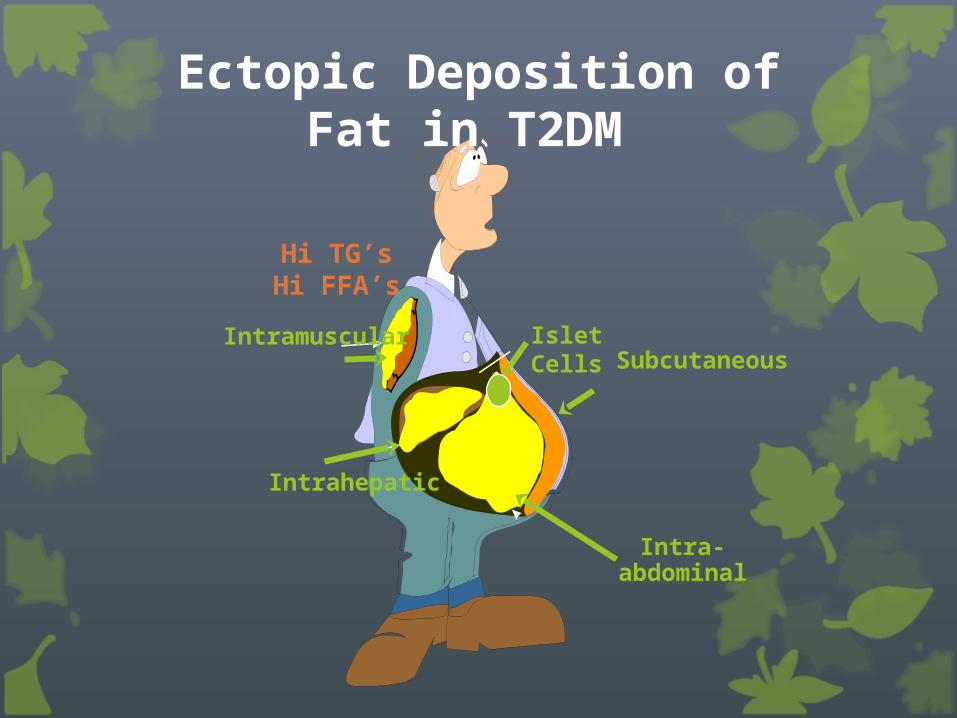
Ectopic Deposition of Fat in T2DM
Hi TG’sHi FFA’s
Intramuscular
Intrahepatic
Subcutaneous
Intra-abdominal
Islet Cells
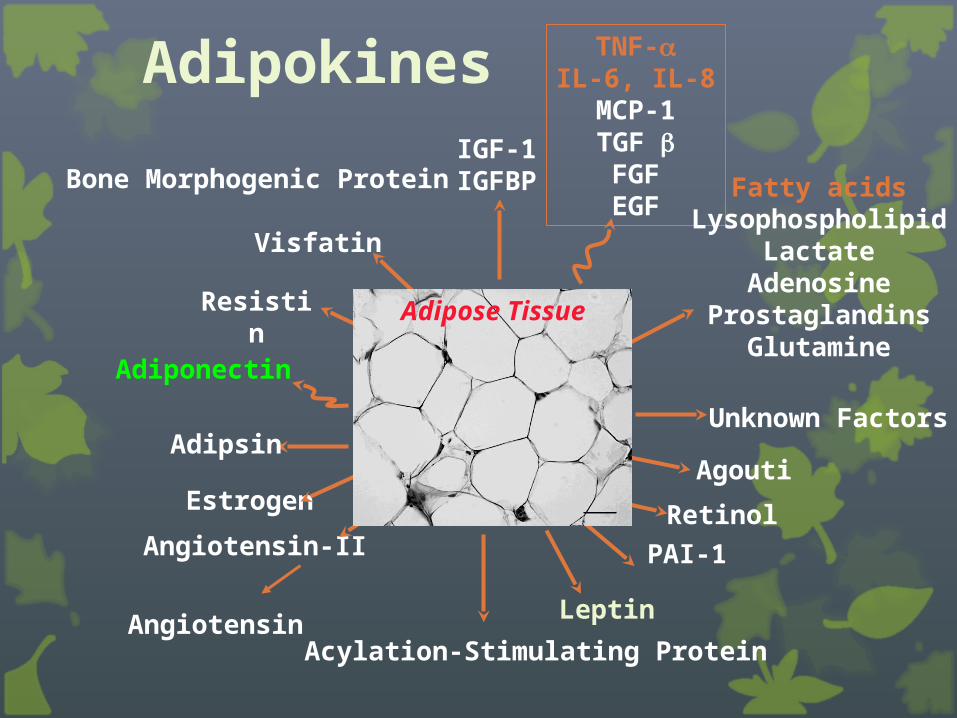
Unknown Factors
Agouti
Retinol
PAI-1
Leptin
Acylation-Stimulating ProteinAngiotensin
Angiotensin-II
Adiponectin
Adipsin
Resistin
Bone Morphogenic ProteinIGF-1IGFBP
TNF-IL-6, IL-8MCP-1TGF FGFEGF
Fatty acidsLysophospholipid
LactateAdenosine
ProstaglandinsGlutamine
Estrogen
Visfatin
Adipose Tissue
Adipokines
Insulin Signaling Defects in T2DM
Mechanism of Insulin Resistance
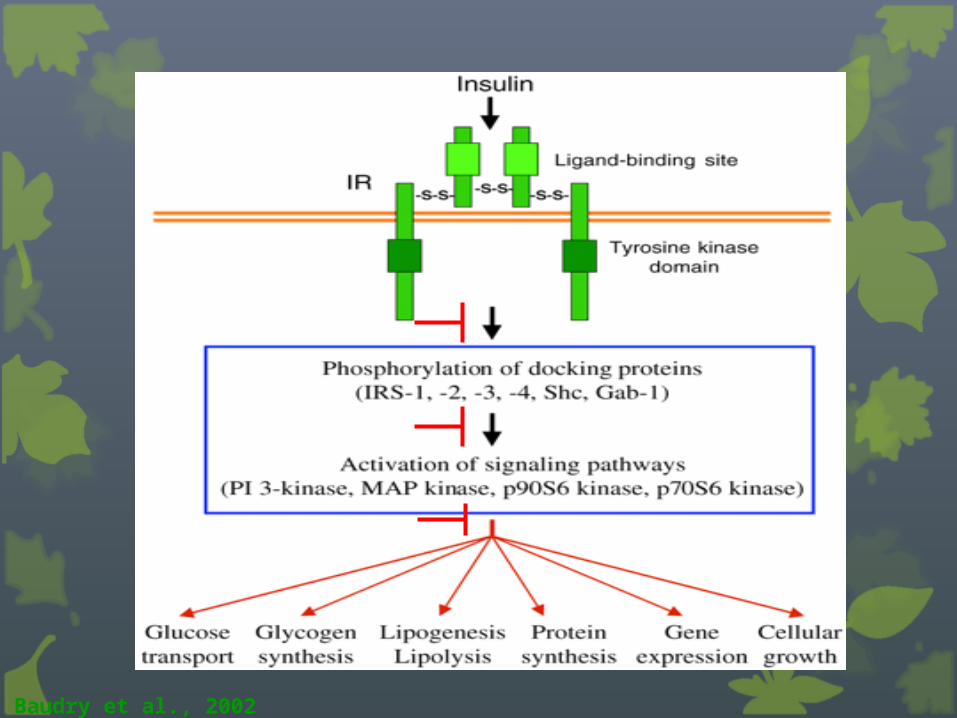
Baudry et al., 2002
Natural History of T2DM
0
100
200
300
-10 -5 0 5 10 15 20 25 30
50
150
250
350
At risk for Diabetes
Glucose
Relative Function
Post Meal Glucose
Fasting Glucose
Insulin Resistance
Insulin LevelBeta Cell Failure
Years of DiabetesBergenstal, ©2000 International Diabetes Center
Used with permission.
Glucotoxicity
As the beta cell begins to decompensate, post-prandial & then fasting glucose levels rise
Once BS’s are elevated…..Hyperglycemia itself has an adverse effect on insulin release from beta cell
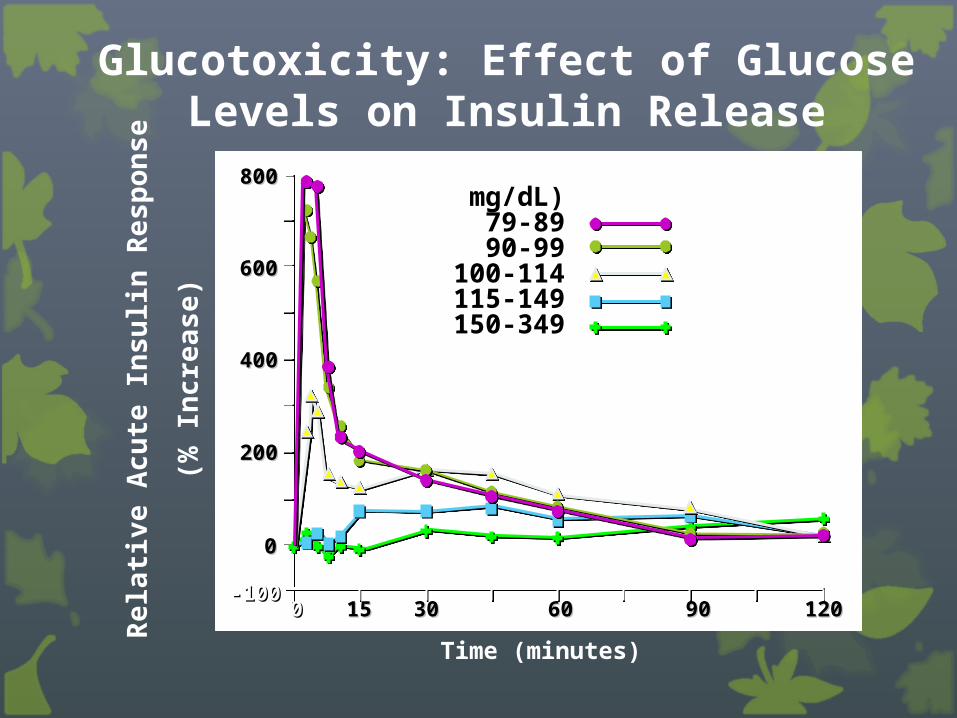
Glucotoxicity: Effect of Glucose Levels on Insulin Release
FPG (mg/dL)79-8990-99
100-114115-149150-349
N2420
73
12
800800
600600
400400
200200
00
-100-10000 1515 3030 6060 9090 120120
Rel
ativ
e A
cute
In
suli
n R
esp
on
se
(% I
ncr
ease
)
Time (minutes)
Summary
Acquisition of visceral obesity, ectopic fat deposition in liver, muscle, & beta cells are major factors in pathogenesis of T2DM
Excessive adipokine production by visceral adipocytes are key contributors to the development of Lipotoxicity & Insulin Resistance
Summary
Glucotoxicity contributes to impaired insulin release
Impaired incretin secretion contributes to impaired insulin release & excessive glucagon secretion
Eventual β-Cell exhaustion & cell death are the final result of this process
Most persons with T2DM exhibit insulin deficiency by 8 years
Summary





























