Embed Size (px)
Citation preview
Managing Your DiabetesA Resource Book for Our Families
THE SECTION OF ENDOCRINOLOGY, METABOLISM AND DIABETES

A Message for our Patients and Their Families . . .You have been given this book because you or someone you care about has been diagnosed with diabetes. It is our goal that people with diabetes and their families have the knowledge and skills to make informed decisions about how to live life with diabetes.
There are many members of your Diabetes Team at Nationwide Children’s Hospital. You will learn about diabetes from each diabetes team member. They can serve as a resource and guide in your journey with diabetes. We hope that this book will be a resource and guide to you also.
© Nationwide Children’s Hospital 2015
Table of Contents1What is Diabetes ...................................1
2Healthy Coping .....................................8
3Monitoring Blood Glucose ...................12
4Insulin ................................................19
5Taking Insulin .....................................21
6Insulin Injections ................................26
7Calculating Bolus Insulin Doses ..........30
8Insulin Dose Changes .........................33
9High Blood Glucose(Hyperglycemia) and Ketones ..............38
10Low Blood Glucose(Hypoglycemia) ...................................45
11Glucagon and Mini-Dose Glucagon ......49
12Sick Days............................................53
13Nutrition .............................................55
14Being Active ........................................72
15School ................................................76
16Clinic Visits .........................................80
17Complications .....................................85
18Special Situations ...............................87
19Resources ..........................................90
20Common Terms ...................................92

1
What is diabetes?
When you have diabetes, your body does not make enough insulin or does not use insulin well. The body is made up of many cells. Each cell needs sugar (glucose) for energy. Glucose comes from the foods you eat. Insulin is the key that allows glucose to get into the cells to make energy. Insulin is made in your pancreas.
What kind of diabetes do I have?There are different kinds of diabetes that children can have. The most common are:
• Type 1 diabetes
• Type 2 diabetesYou can also have both types of diabetes. Sometimes your doctor will know right away what type of diabetes you have. Sometimes your doctor will need to see the results of lab tests before they know which type of diabetes you have. This can take many weeks.
1
2
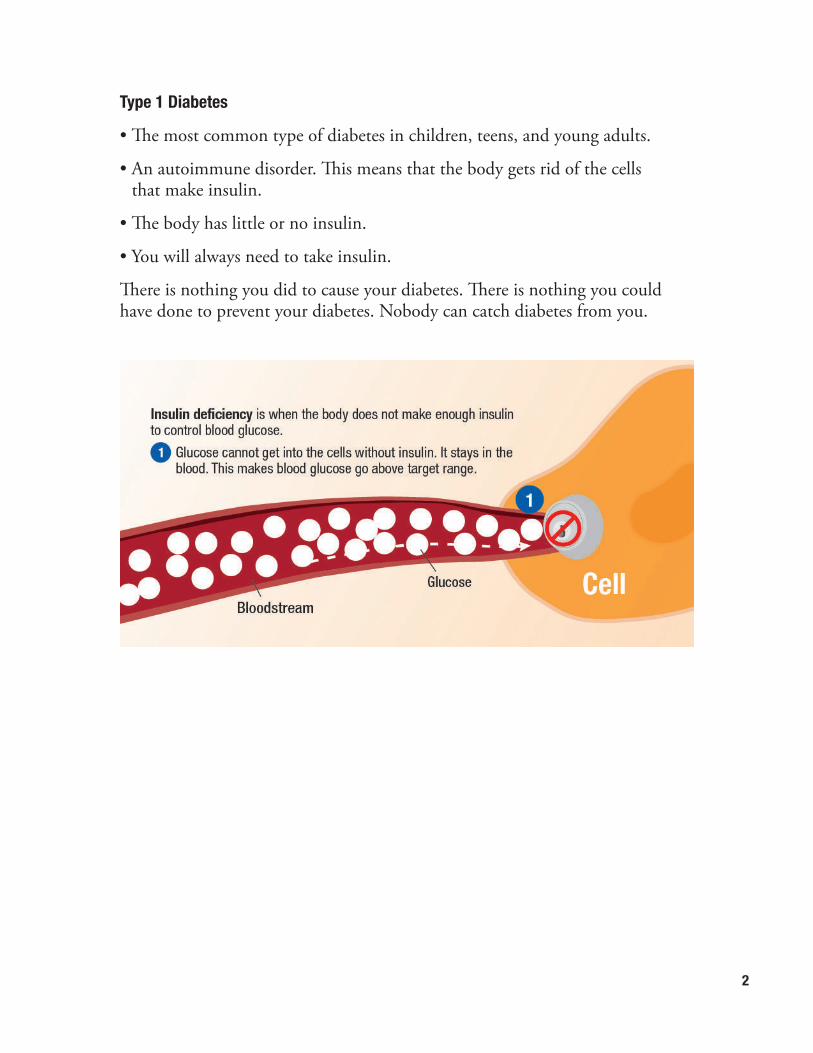
Type 1 Diabetes
• The most common type of diabetes in children, teens, and young adults.
• An autoimmune disorder. This means that the body gets rid of the cells that make insulin.
• The body has little or no insulin.
• You will always need to take insulin.
There is nothing you did to cause your diabetes. There is nothing you could have done to prevent your diabetes. Nobody can catch diabetes from you.
3
Type 2 Diabetes
• It is more common in adults.
• Some children and teens can develop Type 2 diabetes.
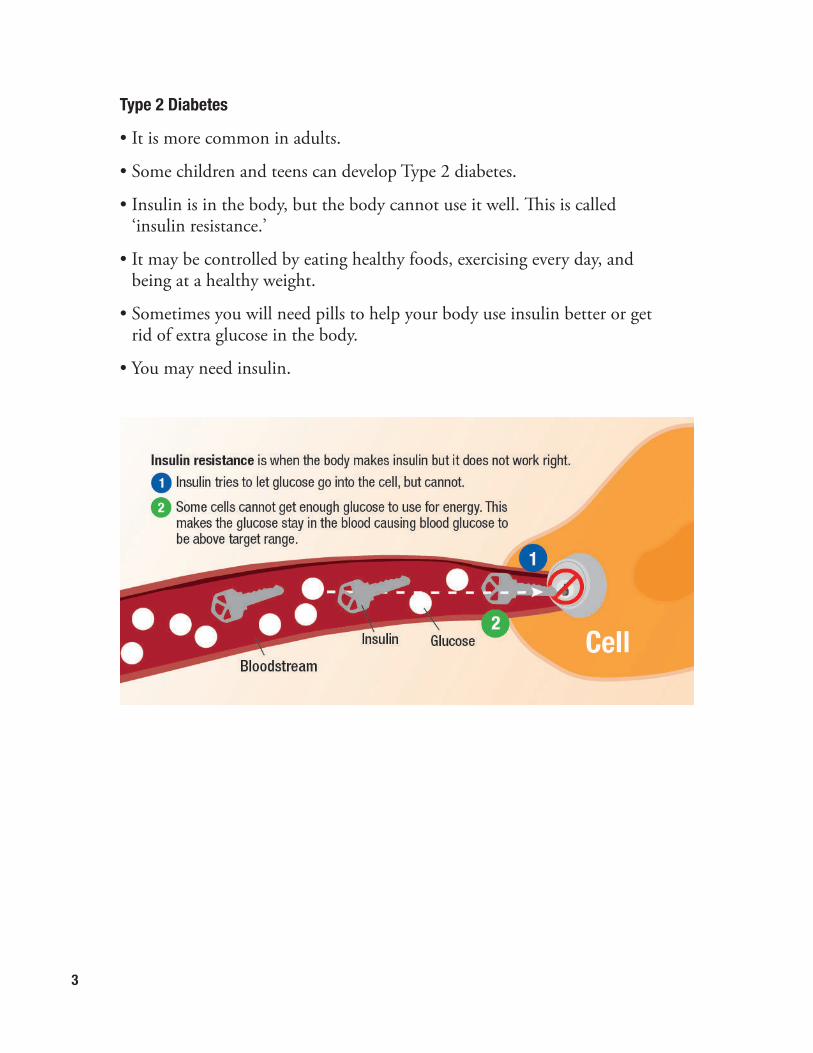
• Insulin is in the body, but the body cannot use it well. This is called ‘insulin resistance.’
• It may be controlled by eating healthy foods, exercising every day, and being at a healthy weight.
• Sometimes you will need pills to help your body use insulin better or get rid of extra glucose in the body.
• You may need insulin.
4
What happens when I have diabetes?When there is not enough insulin or insulin does not work well:
• The glucose stays in the blood. à
• When the blood glucose gets too high, some glucose leaves the body through the urine. à
• Water leaves the body with the glucose. à
When your blood glucose is high you may:
• Feel thirsty
• Go to the bathroom a lot
• Have a dry mouth
• Wet the bed
When glucose cannot get into the cells:
• The body starts to use fat for energy. à
• When fat is used for energy, your body makes ketones. à
• Ketones are in the blood and in the urine. à
• Ketones cause the blood to have more acid. à
• Acid in the blood leads to diabetic ketoacidosis (DKA). This can make you very sick. à
5
When you cannot use glucose for energy you:
• Feel tired
• Lose weight
When you have ketones in your blood you:
• May have a stomach ache
• May throw up (vomit)
When you have diabetic ketoacidosis (DKA) you:
• Feel Sick
• Start to breathe fast
• Have a fruity smell to your breath
• Can be hard to wake up
What signs did you have before you learned you had diabetes?
1. _________________________________________________________
2. _________________________________________________________
3. _________________________________________________________
4. _________________________________________________________
5. _________________________________________________________
6
Food Activity
Honeymoon When you find out you have diabetes and start to take insulin, your body does not have to work as hard to make insulin. Some of the cells that were not making insulin may begin to make some insulin again. This is called a honeymoon phase. This does not happen for everyone. If it does, then it happens soon after you find out you have diabetes.
The honeymoon phase lasts for a few weeks or longer. There is no way to know how long it will last. Taking insulin is the best way to stay in the honeymoon phase.
What do I need to do if I have diabetes?Keep your blood glucose as close to normal as you can. A normal blood glucose is 70 to 120 mg/dl.
How do I keep my blood glucose in a normal range?You can learn to manage your diabetes by learning to think like a pancreas. When your pancreas is working well it gives your body the amount of insulin you need for the food you eat and your activity level at that time.
This keeps your blood glucose in a normal range.
Think and act like a pancreas by:
• Checking your blood glucose at least 4 times each day
• Taking insulin at least 4 times each day
• Counting carbohydrates in the foods you eat
• Learning what makes your blood glucose change and making changes to keep your blood glucose in target range
7
Why do I need to take care of diabetes? There are health problems that can happen when your blood glucose is too low or too high. We will teach you what to do when this happens.
Having diabetes does not cause permanent problems, but high blood glucose over many years can cause permanent problems.
Will diabetes stop me from doing things I want to do?You will still be able to do all of the things you did before you had diabetes.
• You will need to plan so you have time to check your blood glucose, count carbohydrates, and take insulin.
• You will need to be ready for times when your blood glucose is too low or too high.
Your family, your healthcare team, and this book will help you learn what you need to know to take care of your diabetes.
All images credited to: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health
8
Healthy Coping 2Diabetes is a Family AffairDiabetes should not define your life. It is only a part of your life. There are many changes that you and your family will need to make. We are here to help you make those changes. It is our goal that you live well and continue with your regular activities.
The Grief ResponseAny major life change can cause a grief process. Grief is the emotional response to a loss or a life-changing event. The person diagnosed with diabetes and his or her family members can all respond differently.
Stages in the grief process may include:
• Shock - “How could this be possible?”
• Sadness -“I feel different from my friends”
• Denial - “Maybe the doctors are wrong.”
• Helplessness -“I have no control.”
• Anger - “This isn’t fair!”
• Anxiety - “Will I be able to play basketball?”
• Adjustment - “I can still eat this snack. I just need to take insulin.”
• Acceptance - “This is my life now, so I will carry on.”
Image credited to: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health
9
Healthy Ways to Cope with Diabetes and Grief• Talking to others and sharing your thoughts
• Writing down your feelings
• Being open to learning about diabetes
• Remembering the positive things
• Working together with family
Unhealthy Ways to Cope with Grief Process• Avoiding the fact that you have diabetes
• Staying away from other people
• Using drugs or drinking alcohol
• Yelling at and fighting with friends, family, or other children at school
DepressionDepression can happen with diabetes. Common signs of depression include:
• Changes in appetite
• Sleeping more or having trouble sleeping
• Less energy
• Not wanting to do activities you usually enjoy
• Having a hard time concentrating
• Getting annoyed easily
• Sadness
• Hopelessness
• Feeling bad about yourself
If you have any of these signs of depression or are feeling “burned out” and overwhelmed with diabetes, it is important you ask for help to find ways to cope. It is normal to feel this way and struggle with diabetes at the same time. Many people can get help by talking to someone, like a member of your Diabetes Team or a counselor.
10
Counseling Resources are Available at:
• Nationwide Children’s Hospital Psychology
• Nationwide Children’s Behavioral Health Center
• Other local mental health agencies
• If there is an emergency needing immediate mental health attention, please call Netcare Access at 614-276-2273 or your local county mental health crisis line.
Family and Parenting
• Family rules should not change because of diabetes. If a child was given certain privileges or restrictions before diagnosis, those should continue after diagnosis.
• Rules and privileges should be based on the child’s age, developmental stage, family needs and parenting style.
• Children and teens with diabetes can play sports, participate in community activities, and pursue a career of their choice (there are restrictions for military service, commercial pilots and truck drivers).
• Children and families are often better at managing diabetes when everyone works as a team.
People with Diabetes
• Jackie Robinson – First African American to play professional baseball
• Justice Sonia Sotomayor – Supreme Court judge
• Jay Cutler – Chicago Bears quarterback
• George Lucas – Creator and director of Star Wars
• Nick Jonas – Jonas Brothers singer
• Halle Berry – Storm in the X-Men movies
You can do amazing things just like them!
11
Health Insurance and Financial Assistance Many families have questions about money and finances when a child is diagnosed with diabetes. Below are some of the options that may be available to help you and your child get the resources you need.
Commercial insurance is usually gotten through the employer of one of the parents. Your insurance company can tell you how your coverage works. Many commercial insurance plans have a list of accepted providers. Call the member services number on your insurance card to find an accepted provider and benefit coverage.
Healthy Start/Medicaid is insurance from the government for families who meet income guidelines. If the family is approved, the coverage will be for all children in the home under 19 years of age. Healthy Start may be available for families with commercial insurance if they meet the income guidelines. For qualifying families, Medicaid can pay any expense (or co-pay) for all of the child’s medical needs. Medicaid also covers counseling services, as well as dental and vision care.
Bureau for Children with Medical Handicaps (BCMH) is another resource for children with diabetes. There are two parts to the program.
The Diagnostic Program is available to every child who is a resident of the state of Ohio, no matter how much money the family makes. The plan pays out-of-pocket expenses for the diagnostic process, including the hospital stay when diabetes is diagnosed. It does not pay for prescriptions and supplies.
The Treatment Program is for families who meet income guidelines. It covers all out-of-pocket expenses related to diabetes care, including prescriptions and supplies. Commercial insurance and Medicaid must always be billed first before BCMH will cover any expenses.
Family Medical Leave Act (FMLA) may be available for parents who need to take time off work to help manage their child’s diabetes. Our office can help you get FMLA forms if the parent is eligible. Part of the form is filled out by you. Then, the doctor or nurse practitioner will fill out the rest.
The social worker is available to talk with you about your concerns or questions. He or she will give information to help the family get used to the diabetes diagnosis. The social worker will also help find community resources to meet family needs, deal with insurance or financial concerns, and help with ideas to manage behavior changes, including referrals to counseling if needed.
12
Monitoring Blood Glucose 3Blood sugar is also called blood glucose.
Why do I need to check my blood glucose?• To keep you safe
• To help you and your health care team manage your blood glucose levels
• To help you change your insulin doses
• To help you manage your daily activities, like school, work, exercise, and the food you eat
Always check at these times:
• Before breakfast, lunch, and dinner
• Before bed
• When you have signs of low blood glucose (see ‘Low Blood Glucose’ on page 46)
• Each time you get in a car to drive
Sometimes you will need to check at these times:
• Middle of the night
• Before, during, and after exercise
Check more often:
• When you are sick
Check blood glucose between 2 a.m. and 4 a.m. if there is a chance your blood glucose may be low.
• Check for 2 to 3 nights after changing your Lantus® insulin dose.
• When you have an unusual amount of exercise late in the day.
• When you are sick.
• When your blood glucose is low before bed.

13
What supplies do I need?
Blood glucose meter Blood glucose test strips
Lancet device Lancets
Container for used lancets (sharps container or a container made of thick plastic, like a detergent bottle or bleach bottle)
14
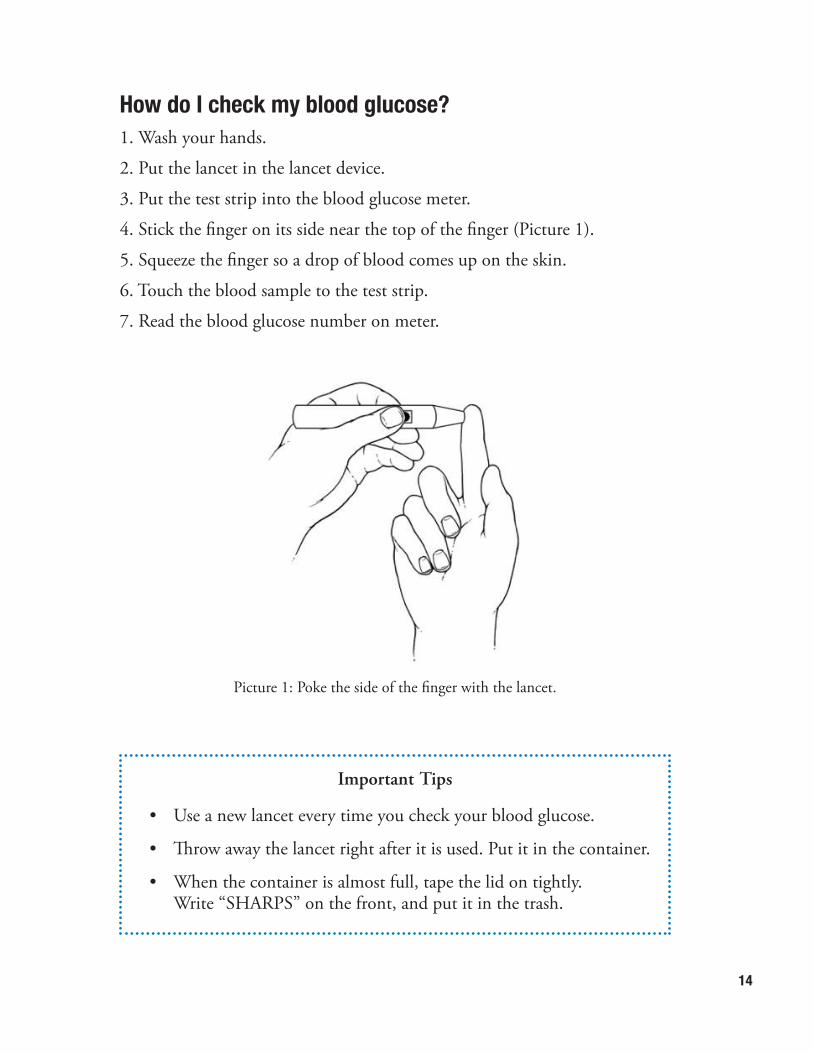
How do I check my blood glucose?1. Wash your hands.
2. Put the lancet in the lancet device.
3. Put the test strip into the blood glucose meter.
4. Stick the finger on its side near the top of the finger (Picture 1).
5. Squeeze the finger so a drop of blood comes up on the skin.
6. Touch the blood sample to the test strip.
7. Read the blood glucose number on meter.
Picture 1: Poke the side of the finger with the lancet.
Important Tips
• Use a new lancet every time you check your blood glucose.
• Throw away the lancet right after it is used. Put it in the container.
• When the container is almost full, tape the lid on tightly. Write “SHARPS” on the front, and put it in the trash.

15
What number should my blood glucose be?Blood glucose is measured in mg/dl. The normal range for blood glucose for people without diabetes is 70 to 120 mg/dl. The Diabetes Center has guidelines for blood glucose readings. This is called a target range. There may be times when your healthcare provider gives you a different target range, like for bedtime, with exercise, or after eating.
Nationwide Children’s Hospital Diabetes Center Target Blood Glucose Ranges
The goal is to keep the blood glucose within the target range most of the time.
What should I do after I check my blood glucose?
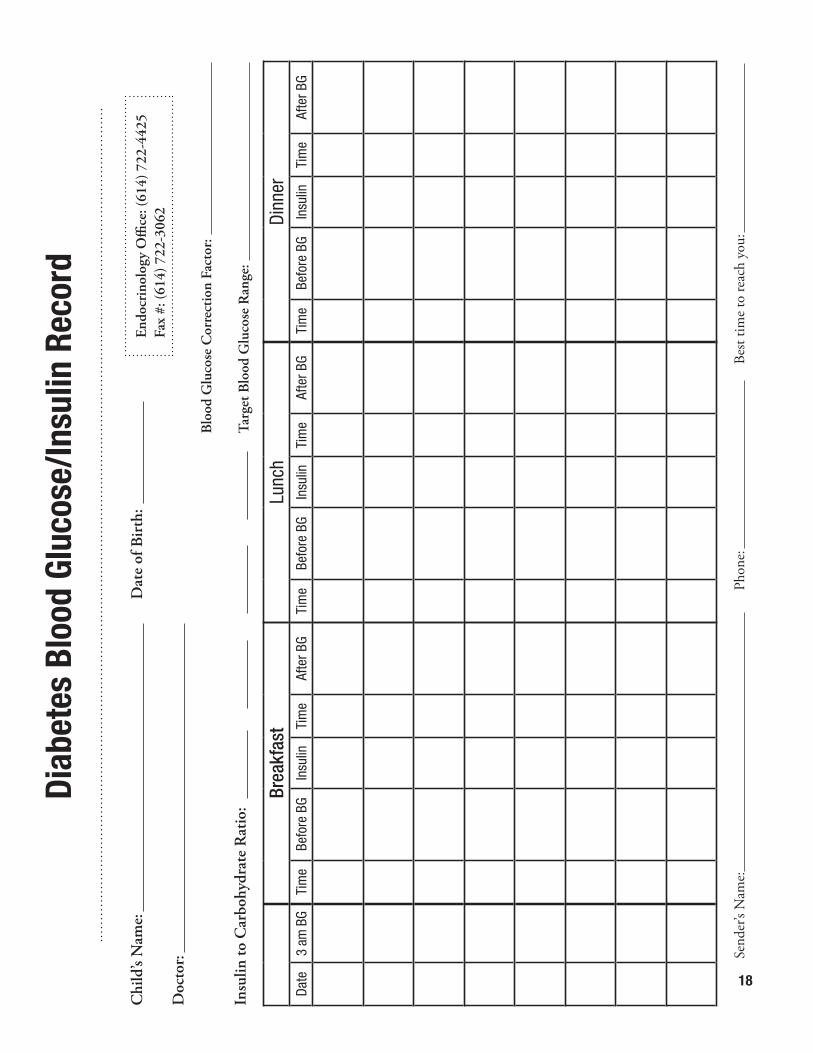
Write the blood glucose number in a log book or on a log sheet (page 18), and:
• Include all of your blood glucose numbers.
• Write a comment if there is a reason the blood glucose is above or below target.
Age Blood Glucose mg/dl
0 to 5 years old 100 to 180
6 to 9 years old 80 to 140
10 years old or more 70 to 120
16
Important Tips
• Take your blood glucose meter with you when you are away from home.
• Know your blood glucose numbers when you call the clinic or the doctor.
• Bring your blood glucose meter and blood glucose records to all your appointments.
• Bring a list of any questions that you may have.
How do I take care of my blood glucose meter?• Set the date and time when you get a new meter.
• Make sure the date and time are right each time you use your meter.
• Use the control solution as needed. This will let you know the meter and test strips are working right. Use it:
o When you get a new meter.
o When you get new test strips.
o When you think that the meter is not giving you the right blood glucose number.
• Keep the meter and test strips out of very hot or very cold temperatures. This can cause blood glucose numbers to be wrong.
• Keep meter and test strips in a case, away from sunlight.
• Keep test strips in the container they come in. Keep the lid closed.
• Keep extra batteries with your meter.
• There is a phone number on the back of each blood glucose meter. Call that number if your meter is not working or you have questions about how to use your meter.
17
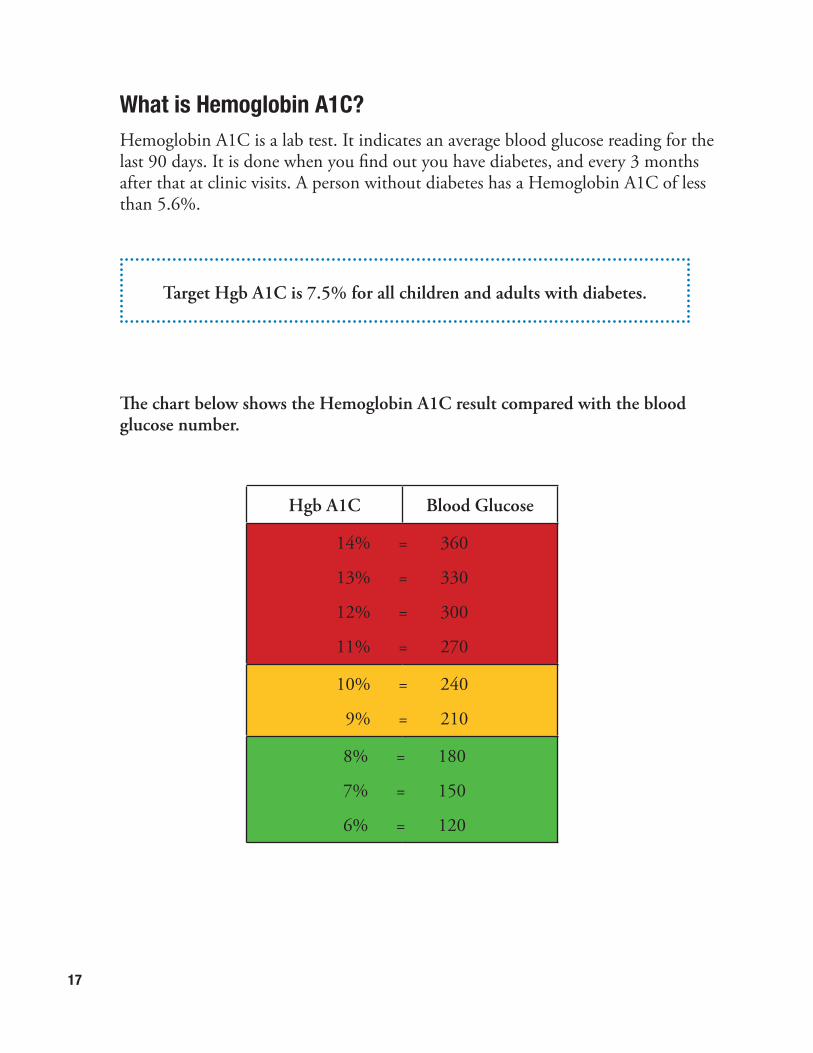
What is Hemoglobin A1C?Hemoglobin A1C is a lab test. It indicates an average blood glucose reading for the last 90 days. It is done when you find out you have diabetes, and every 3 months after that at clinic visits. A person without diabetes has a Hemoglobin A1C of less than 5.6%.
The chart below shows the Hemoglobin A1C result compared with the blood glucose number.
Hgb A1C Blood Glucose
14% = 360
13% = 330
12% = 300
11% = 270
10% = 240
9% = 210
8% = 180
7% = 150
6% = 120
Target Hgb A1C is 7.5% for all children and adults with diabetes.
18
Diab
etes
Blo
od G
luco
se/In
sulin
Rec
ord
Chi
ld’s
Nam
e:
D
ate
of B
irth
:
Doc
tor:
Insu
lin to
Car
bohy
drat
e R
atio
:
Brea
kfas
tTi
me
Befo
re B
GIn
sulin
Tim
eAf
ter B
G
Lunc
hTi
me
Befo
re B
GIn
sulin
Tim
eAf
ter B
G
Dinn
erTi
me
Befo
re B
GIn
sulin
Tim
eAf
ter B
GDa
te3
am B
G
Blo
od G
luco
se C
orre
ctio
n Fa
ctor
:
Targ
et B
lood
Glu
cose
Ran
ge:
Endo
crin
olog
y O
ffice
: (61
4) 7
22-4
425
Fax
#: (6
14) 7
22-3
062
Send
er’s
Nam
e:
Pho
ne:
Bes
t tim
e to
reac
h yo
u:
19
Insulin 4When you have type 1 diabetes, your body cannot make its own insulin. You will need insulin shots (injections) every day. Many people with type 2 diabetes also need insulin injections. You cannot take insulin by mouth or in any other form than injections.
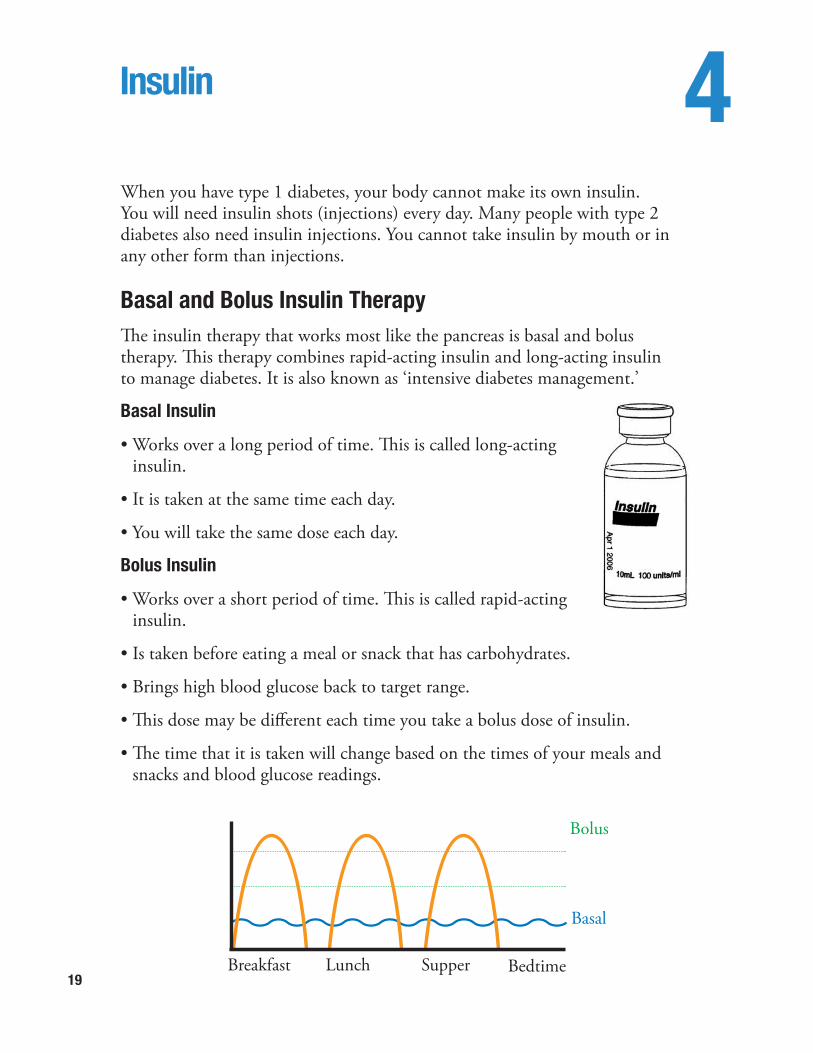
Basal and Bolus Insulin TherapyThe insulin therapy that works most like the pancreas is basal and bolus therapy. This therapy combines rapid-acting insulin and long-acting insulin to manage diabetes. It is also known as ‘intensive diabetes management.’
Basal Insulin
• Works over a long period of time. This is called long-acting insulin.
• It is taken at the same time each day.
• You will take the same dose each day.
Bolus Insulin
• Works over a short period of time. This is called rapid-acting insulin.
• Is taken before eating a meal or snack that has carbohydrates.
• Brings high blood glucose back to target range.
• This dose may be different each time you take a bolus dose of insulin.
• The time that it is taken will change based on the times of your meals and snacks and blood glucose readings.
Breakfast Lunch Supper Bedtime
Basal
Bolus
20
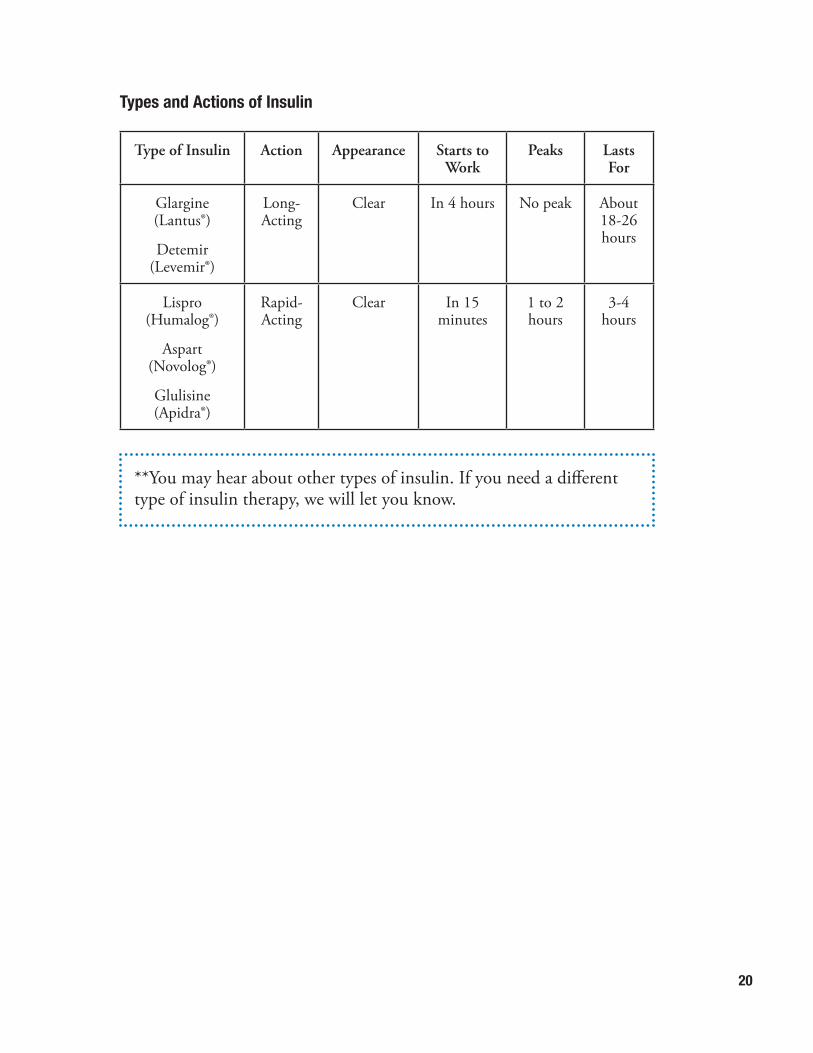
Types and Actions of Insulin
Type of Insulin Action Appearance Starts to Work
Peaks Lasts For
Glargine (Lantus®)
Detemir (Levemir®)
Long-Acting
Clear In 4 hours No peak About 18-26 hours
Lispro (Humalog®)
Aspart (Novolog®)
Glulisine (Apidra®)
Rapid-Acting
Clear In 15 minutes
1 to 2 hours
3-4 hours
**You may hear about other types of insulin. If you need a different type of insulin therapy, we will let you know.
21
Taking Insulin 5You can use a syringe, an insulin pen, or an insulin pump to take insulin. Insulin comes in a bottle (vial) or in an insulin pen.
Before you leave the pharmacy and each time you give an insulin injection:
ü Check to make sure you have the right type of insulin.
ü Check the expiration date.
ü Check the look of the insulin (appearance). It should be clear.
ü Check that you have the right form of insulin. This means the insulin could come in a vial, disposable pen, or cartridge.
Throw away insulin and use a new vial, pen, or cartridge if:
• Insulin has been left where it is very hot or very cold.
• Insulin is cloudy or contains particles.
• It is later than the expiration date on the vial, pen, or cartridge.
• It has been more than 28 days since you began using the vial, pen, or cartridge .
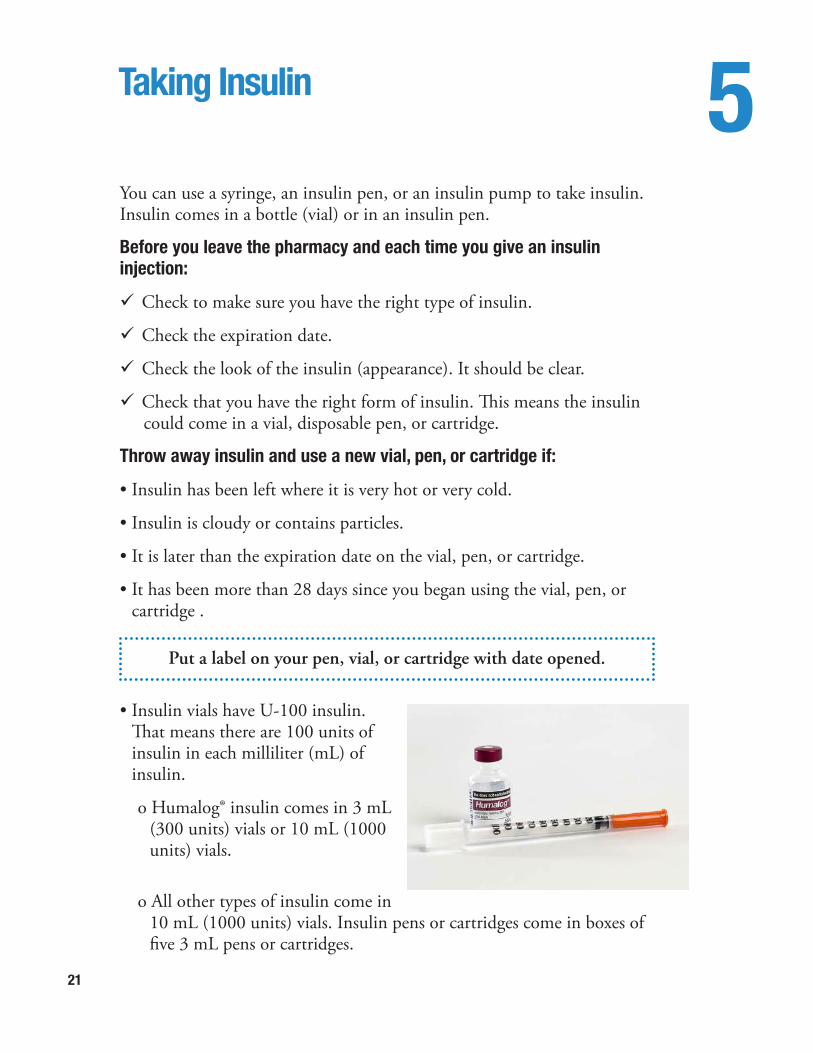
• Insulin vials have U-100 insulin. That means there are 100 units of insulin in each milliliter (mL) of insulin.
o Humalog® insulin comes in 3 mL (300 units) vials or 10 mL (1000 units) vials.
o All other types of insulin come in 10 mL (1000 units) vials. Insulin pens or cartridges come in boxes of five 3 mL pens or cartridges.
Put a label on your pen, vial, or cartridge with date opened.
22
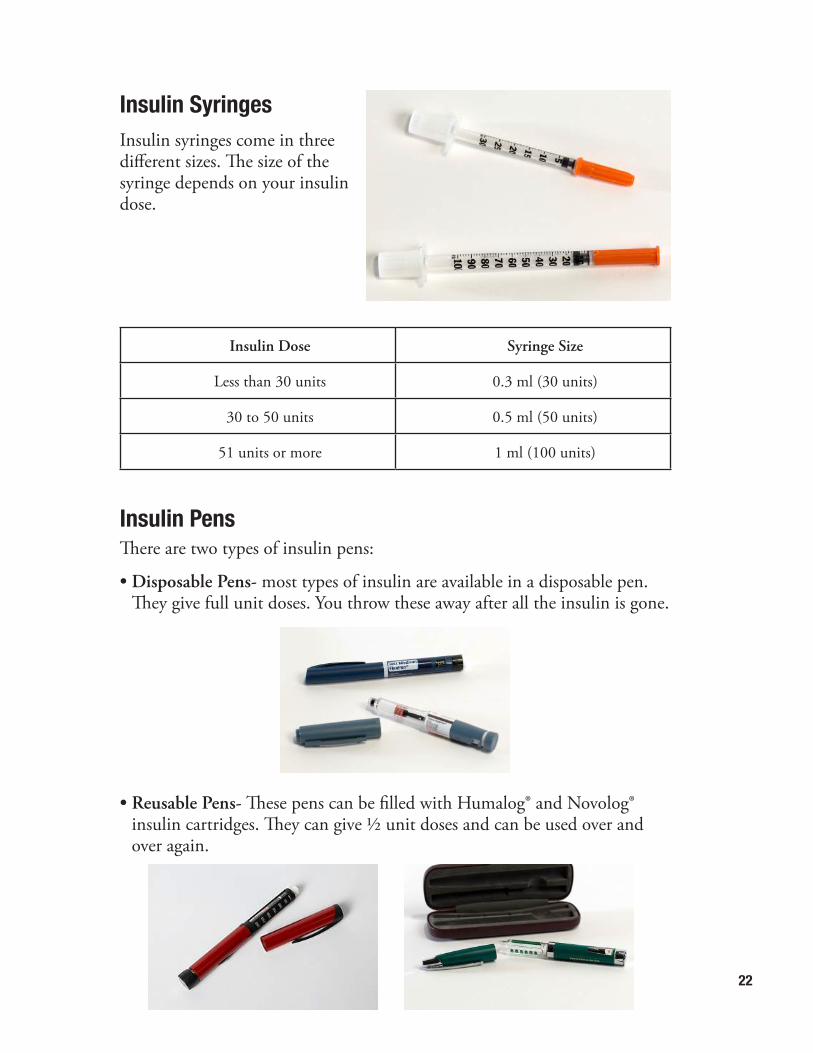
Insulin SyringesInsulin syringes come in three different sizes. The size of the syringe depends on your insulin dose.
Insulin Dose Syringe Size
Less than 30 units 0.3 ml (30 units)
30 to 50 units 0.5 ml (50 units)
51 units or more 1 ml (100 units)
Insulin PensThere are two types of insulin pens:
• Disposable Pens- most types of insulin are available in a disposable pen. They give full unit doses. You throw these away after all the insulin is gone.
• Reusable Pens- These pens can be filled with Humalog® and Novolog® insulin cartridges. They can give ½ unit doses and can be used over and over again.
23
Syringes and Insulin Pen NeedlesSyringes and needles come in different thickness and lengths. The doctor will prescribe the size for you.
• ‘Gauge’ means the thickness of the needle. The higher the number meansthe thinner the needle.
• Needle lengths include: ½ inch (12.7 mm), 5/16 inch (8 mm), 3/16 inch (5 mm), and 5/32 inch (4 mm). Your healthcare team will tell you the needle length that is best for you. When using an insulin vial with U-100 insulin, you need to use an insulin syringe that says “For use with U-100 insulin.”
How do I store insulin?
Insulin Before opening After opening
Vial Store in refrigerator. Good until expiration date on vial.
Store at room temperature. Throw away 28 days after first use.
Levemir® insulin pen Store in refrigerator. Good until expiration date on insulin pen.
Store at room temperature. Throw away 42 days after first use.
Humalog®, Novolog®, or Lantus® insulin pen or Humalog® or Novolog® insulin cartridge
Store in refrigerator. Good until expiration date on insulin pen or cartridge.
Store at room temperature. Throw away 28 days after first use.
*Source: These are the manufacturer’s recommendations.
• When storing insulin in the refrigerator, the temperature should be between 36 degrees F and 46 degrees F.
•When storing insulin at room temperature, temperature should be between 36 degrees F and 86 degrees F.
24
Insulin Pump TherapyInsulin pump therapy is basal and bolus insulin therapy. An insulin pump is a small device that gives you rapid-acting insulin (Novolog®, Humalog®, or Apidra®) all the time. This is the basal and bolus insulin.
• The user can give a bolus dose of rapid-acting insulin when needed. This is for carbohydrates eaten and for bringing high blood glucose back to target.
• A small flexible tube (cannula) is inserted under the skin to give the insulin. This is the infusion set. You or a family member needs to change the infusion set every 2 to 3 days.
• Insulin pump therapy is not the right choice for everyone. The healthcare providers at the Diabetes Center want you to think about the following things before starting insulin pump therapy:
o For the school age or older child, both the parent and child must want an insulin pump and be willing to learn about insulin pump therapy.
o For the younger child, the parent must be willing to learn about insulin pump therapy.
o You must go to clinic visits every 3 months.
o You must be willing to check blood glucose at least 4 times a day.
o You must look for blood glucose patterns to manage diabetes.
o You must have good carbohydrate counting skills.
o The family must be comfortable with basic diabetes management skills.
25
If you think you might want insulin pump therapy, talk with your healthcare provider to decide if it is a good choice. We offer classes to make it easier to start insulin pump therapy. Here at Nationwide Children’s Hospital, we recommend you stay on shots (injections) for at least six months before thinking about insulin pump therapy. Your doctor and educator want to make sure that you have a good understanding of basic diabetes care. You also need to be comfortable with the injections and calculating your insulin doses. If the pump does not work, then you must be able to go back to injections and insulin dose calculations.
26
Insulin Injections 6How do I prepare an insulin pen?1. Calculate your insulin dose (see page 30).
2. Wash your hands.
3. Read the label on the insulin pen to make sure you have the right pen.
4. Take the cap off of the pen. Use alcohol to clean the rubber seal on the end of the pen.
5. Remove paper tab from the pen needle.
6. Push the capped needle onto the pen. Tighten needle by screwing clockwise.
7. Pull off the outer needle shield. Save this shield. Pull off the inner needle shield and throw it away.
8. Dial 2 units by turning the dose knob to “2.”
9. Point the pen needle upwards. Tap the pen so air moves to the top of pen.
10. With the needle pointing up, push the dose button until it stops. A stream of insulin should appear. If it does not, repeat steps 7 to 9. This is called priming the pen. This gets air out of the needle.
11. Dial the dose knob to the right number of insulin units that you need. You are now ready to give the injection.
12. After giving the injection, put the outer shield back on the needle. Unscrew the used needle, and throw it away.
How do I prepare an insulin injection by syringe?1. Calculate your insulin dose (see page 30).
2. Wash your hands.
3. Read the label on the insulin bottle (vial) to make sure you have the right type of insulin.
4. Clean the top of the insulin vial with alcohol.
5. Take the white cap off of the bottom of the syringe.
27
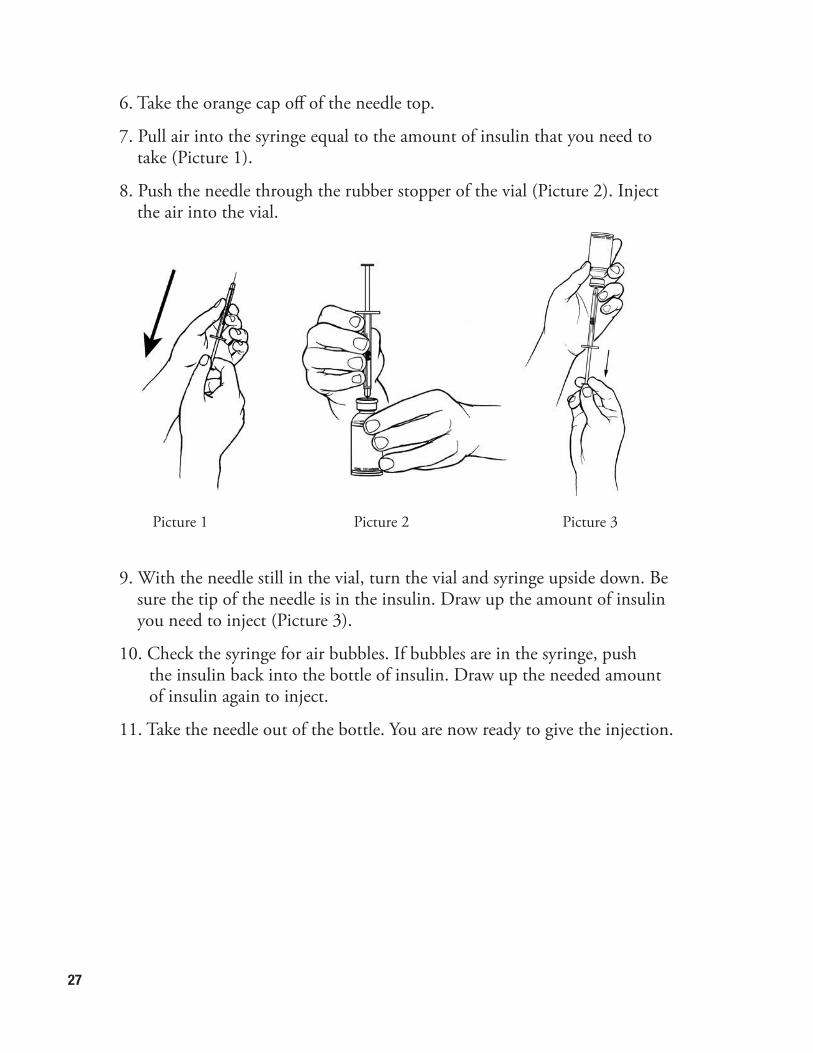
6. Take the orange cap off of the needle top.
7. Pull air into the syringe equal to the amount of insulin that you need to take (Picture 1).
8. Push the needle through the rubber stopper of the vial (Picture 2). Inject the air into the vial.
9. With the needle still in the vial, turn the vial and syringe upside down. Be sure the tip of the needle is in the insulin. Draw up the amount of insulin you need to inject (Picture 3).
10. Check the syringe for air bubbles. If bubbles are in the syringe, push the insulin back into the bottle of insulin. Draw up the needed amount of insulin again to inject.
11. Take the needle out of the bottle. You are now ready to give the injection.
Picture 1 Picture 2 Picture 3
28
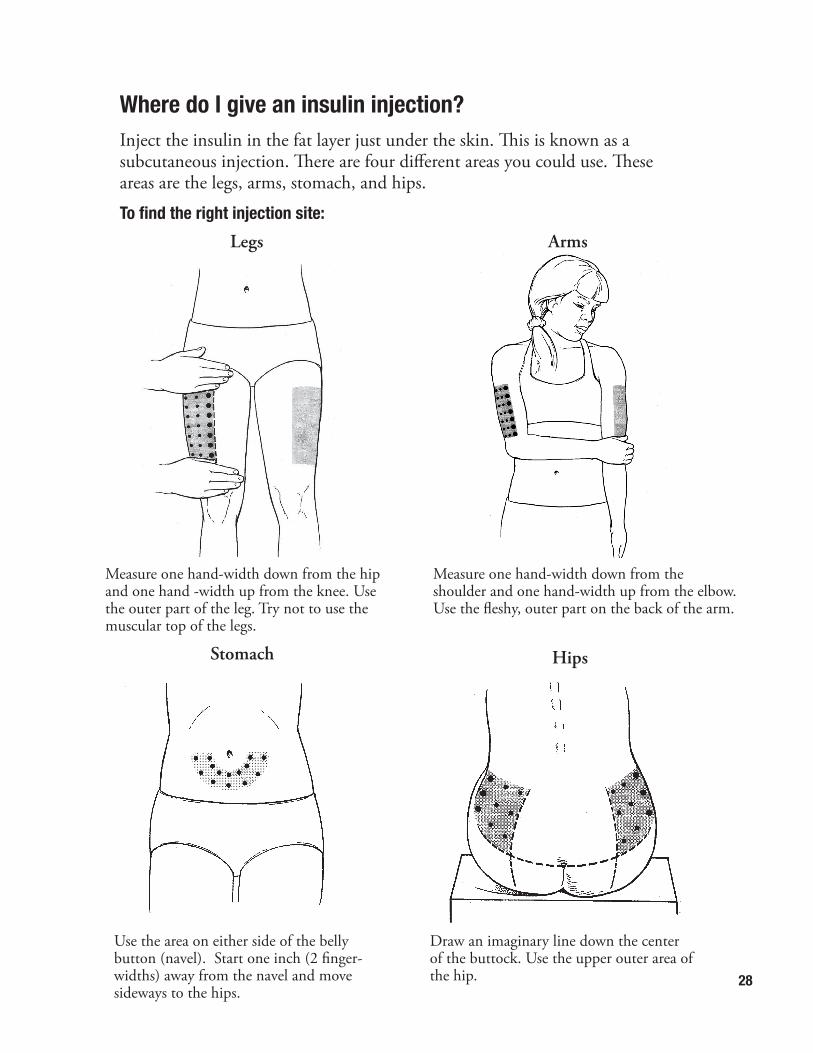
Where do I give an insulin injection?Inject the insulin in the fat layer just under the skin. This is known as a subcutaneous injection. There are four different areas you could use. These areas are the legs, arms, stomach, and hips.
To find the right injection site:
Legs Arms
Stomach Hips
Measure one hand-width down from the hip and one hand -width up from the knee. Use the outer part of the leg. Try not to use the muscular top of the legs.
Measure one hand-width down from the shoulder and one hand-width up from the elbow. Use the fleshy, outer part on the back of the arm.
Use the area on either side of the belly button (navel). Start one inch (2 finger-widths) away from the navel and move sideways to the hips.
Draw an imaginary line down the center of the buttock. Use the upper outer area of the hip.
29
How do I keep from getting scar tissue?Use different areas of your body and different places (sites) within each area. If one site is used too much you may get scar tissue. This may look like swelling or a hard lump. It is hard to inject insulin into scar tissue. If you use the area with scar tissue, insulin may leak out. Even if it does not leak, you may see higher blood glucose levels at your next blood glucose check. This is because your body is not getting enough insulin. If you have scar tissue, do not use that site for at least 3 months. When you start using that site again, look at the next blood glucose after using that site. If that blood glucose is higher than expected, there may still be scar tissue.
How do I give an insulin injection?
1. Pick the injection site.
2. Clean the area with alcohol or soap and water. If you use alcohol, allow the skin to dry to prevent stinging.
3. Insert the needle straight into the skin. Push the plunger on the syringe or the button on the insulin pen until all insulin is injected.
4. Count slowly to 10.
5. Remove the needle from the skin.
6. Check the site to see if insulin leaks out. If this happens, make a note in your logbook. Your next blood glucose may be higher than expected.
30
Calculating Bolus Insulin Doses 7How do I calculate my bolus insulin doses?You will need to figure out (calculate) your bolus insulin dose based on carbohydrate eaten, blood glucose level or both added together. Calculating a bolus dose for carbohydrate (meal bolus)
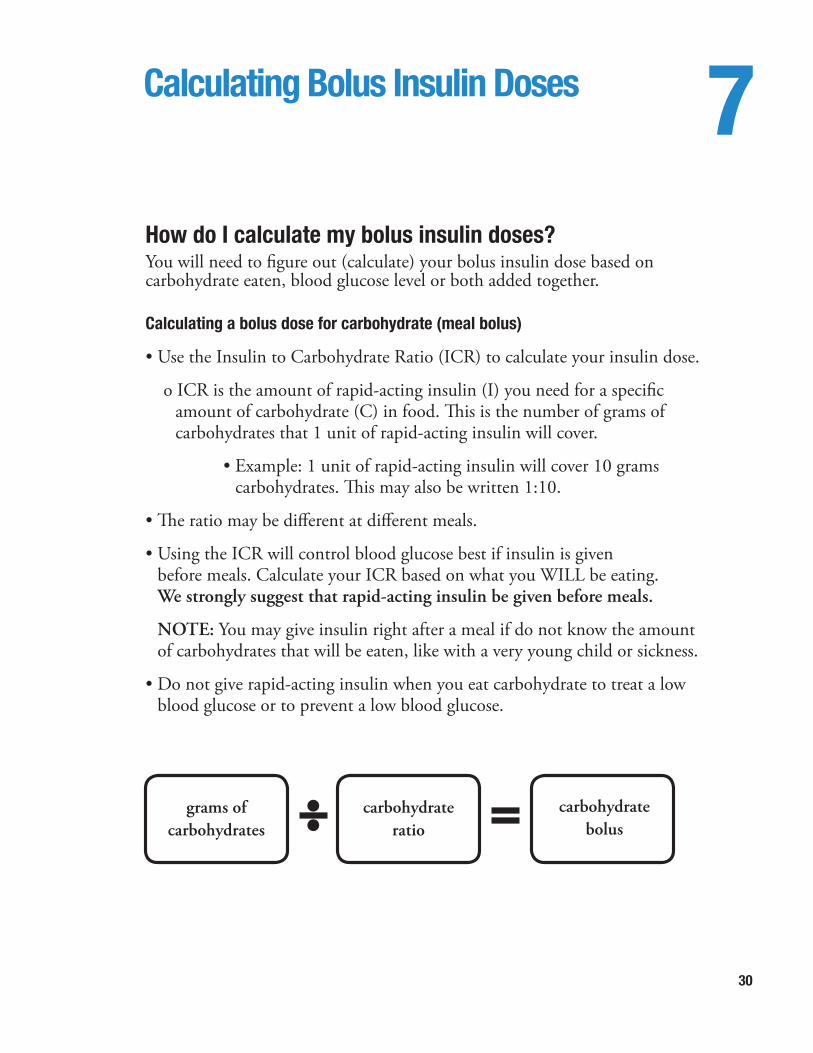
• Use the Insulin to Carbohydrate Ratio (ICR) to calculate your insulin dose.
o ICR is the amount of rapid-acting insulin (I) you need for a specific amount of carbohydrate (C) in food. This is the number of grams of carbohydrates that 1 unit of rapid-acting insulin will cover.
• Example: 1 unit of rapid-acting insulin will cover 10 grams carbohydrates. This may also be written 1:10.
• The ratio may be different at different meals.
• Using the ICR will control blood glucose best if insulin is given before meals. Calculate your ICR based on what you WILL be eating. We strongly suggest that rapid-acting insulin be given before meals.
NOTE: You may give insulin right after a meal if do not know the amount of carbohydrates that will be eaten, like with a very young child or sickness.
• Do not give rapid-acting insulin when you eat carbohydrate to treat a low blood glucose or to prevent a low blood glucose.
grams of carbohydrates
carbohydrateratio
carbohydratebolus
31
Example:
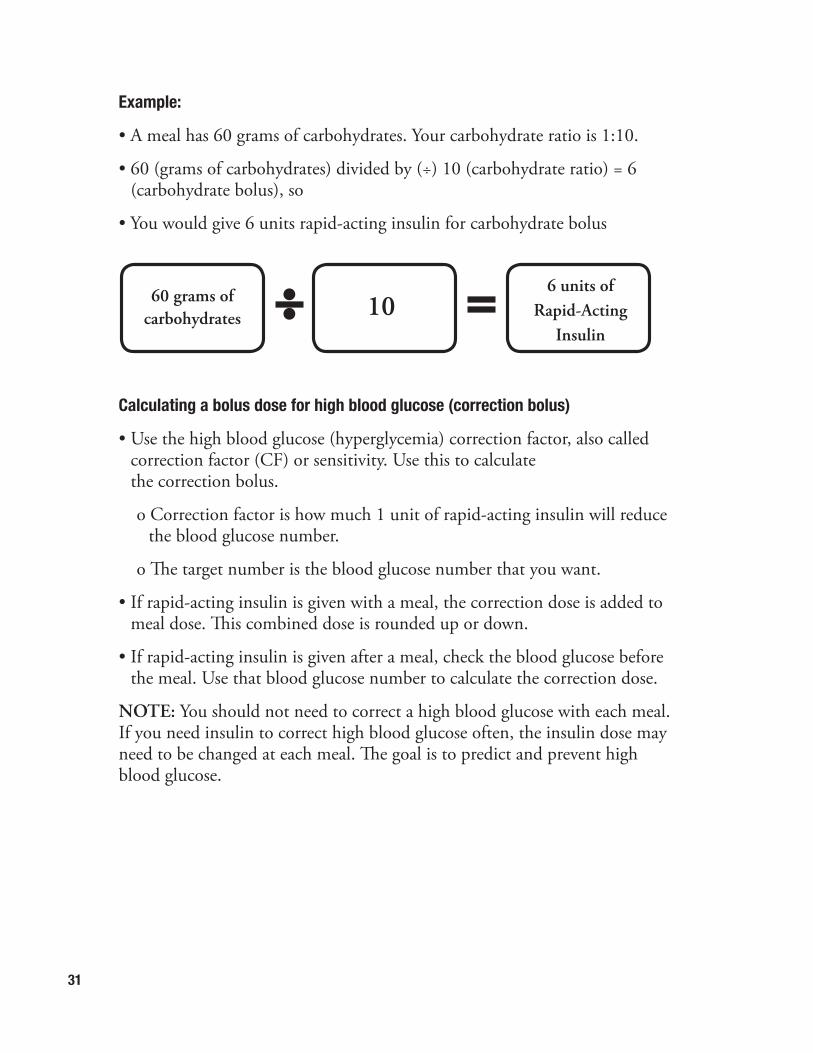
• A meal has 60 grams of carbohydrates. Your carbohydrate ratio is 1:10.
• 60 (grams of carbohydrates) divided by (÷) 10 (carbohydrate ratio) = 6 (carbohydrate bolus), so
• You would give 6 units rapid-acting insulin for carbohydrate bolus
Calculating a bolus dose for high blood glucose (correction bolus)
• Use the high blood glucose (hyperglycemia) correction factor, also called correction factor (CF) or sensitivity. Use this to calculate the correction bolus.
o Correction factor is how much 1 unit of rapid-acting insulin will reduce the blood glucose number.
o The target number is the blood glucose number that you want.
• If rapid-acting insulin is given with a meal, the correction dose is added to meal dose. This combined dose is rounded up or down.
• If rapid-acting insulin is given after a meal, check the blood glucose before the meal. Use that blood glucose number to calculate the correction dose.
NOTE: You should not need to correct a high blood glucose with each meal. If you need insulin to correct high blood glucose often, the insulin dose may need to be changed at each meal. The goal is to predict and prevent high blood glucose.
60 grams of carbohydrates 10
6 units of Rapid-Acting
Insulin
32
Example:
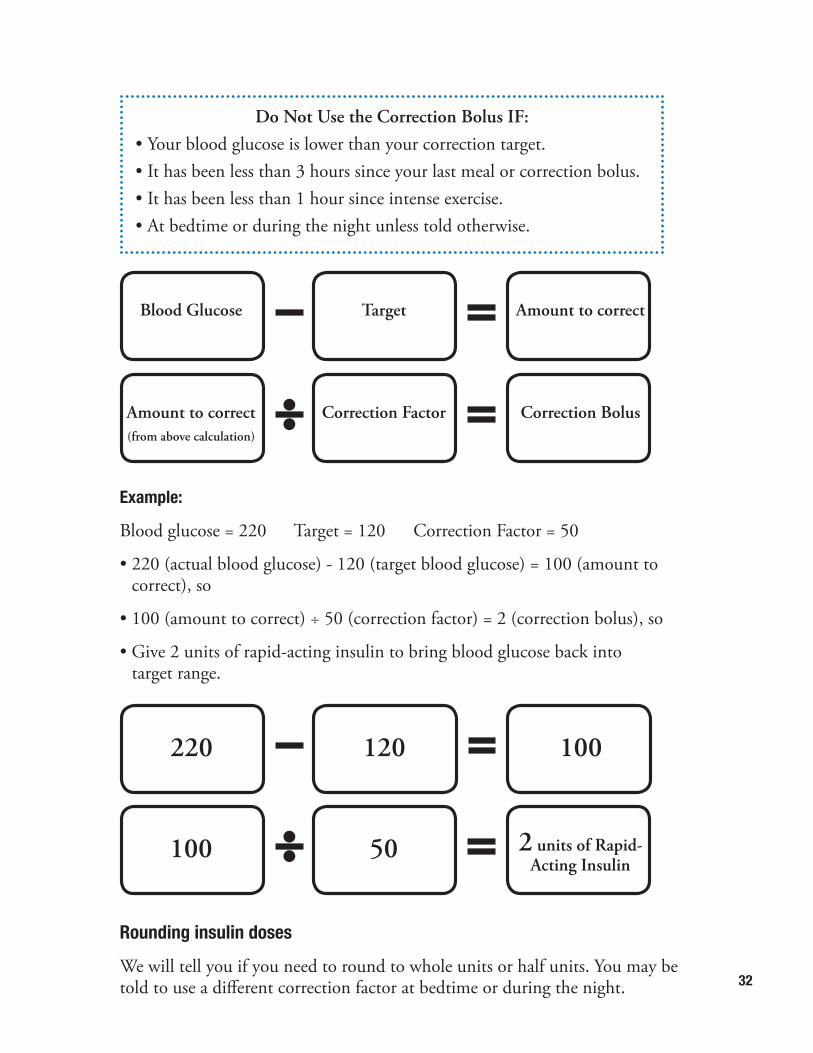
Blood glucose = 220 Target = 120 Correction Factor = 50
• 220 (actual blood glucose) - 120 (target blood glucose) = 100 (amount to correct), so
• 100 (amount to correct) ÷ 50 (correction factor) = 2 (correction bolus), so
• Give 2 units of rapid-acting insulin to bring blood glucose back into target range.
Rounding insulin doses
We will tell you if you need to round to whole units or half units. You may be told to use a different correction factor at bedtime or during the night.
Blood Glucose Target Amount to correct
Do Not Use the Correction Bolus IF:• Your blood glucose is lower than your correction target.• It has been less than 3 hours since your last meal or correction bolus.• It has been less than 1 hour since intense exercise. • At bedtime or during the night unless told otherwise.
Amount to correct(from above calculation)
Correction Factor Correction Bolus
100 50 2 units of Rapid-Acting Insulin
220 120 100
33
Insulin Dose Changes 8For children with diabetes, blood glucose levels can go up and down a lot. Often, these changes happen at the same time of day, like at meal times or bedtime. As time goes on, you will be able to find these patterns in blood glucose changes more easily. It is important that you know how to make the right changes to your child’s or your own basal and bolus insulin doses for these patterns. This will help keep blood glucose levels in the right place (target range). The Diabetes Team will work with you and your family to help make the right insulin dose changes.
What You NeedBefore you start you will need to have these supplies and information ready.
You will need to:
• Have a blood glucose log – Record your blood glucose results here. You should be checking blood glucose before all three meals and before going to bed.
• Know your insulin doses – You will have two different types of insulin doses:
o Basal insulin – This is the Lantus® insulin that works over a long period of time.
o Bolus insulin – This is the Novolog® or Humalog® insulin that is based on how many carbohydrates you are eating and how high your blood glucose is.
• Know your target blood glucose range for your age
o Birth to 5 years: 100-180 mg/dL
o 6 to 9 years: 80-140 mg/dL
o 10 years and older: 70-120 mg/dL
34
How to Find Blood Glucose PatternsMany different things can make blood glucose go up or down, like exercise, food, or stress.
1. Review the past week’s blood glucose levels in your log. Look at the same times of day tested for each day of the week, like breakfast, lunch, dinner, or bedtime.
2. Look for blood glucose numbers that are above or below your target range.
3. Look for patterns in the blood glucose numbers.
• Are they below target range? Are they below target at a certain time of day?
• Are they above target range? Are they above target at a certain time of day?
• Is there no clear pattern?
4. Look to see if blood glucose levels are out of range after a certain event, like after a high blood glucose correction, bolus, exercise, or birthday parties or special events.
5. Look for other things that may make blood glucose numbers out of range unexpectedly. These may not be good reasons to change an insulin dose.
• Unplanned activity/exercise
• Dirty fingers at the time of testing
• Wrong carbohydrate counting or eating more or less than expected
• Timing of meals
• Expired insulin or test strips
• Meter not working
6. A change in the insulin dose may be needed if:
• You are using the correction factor often.
• You are treating low blood glucose often.
35
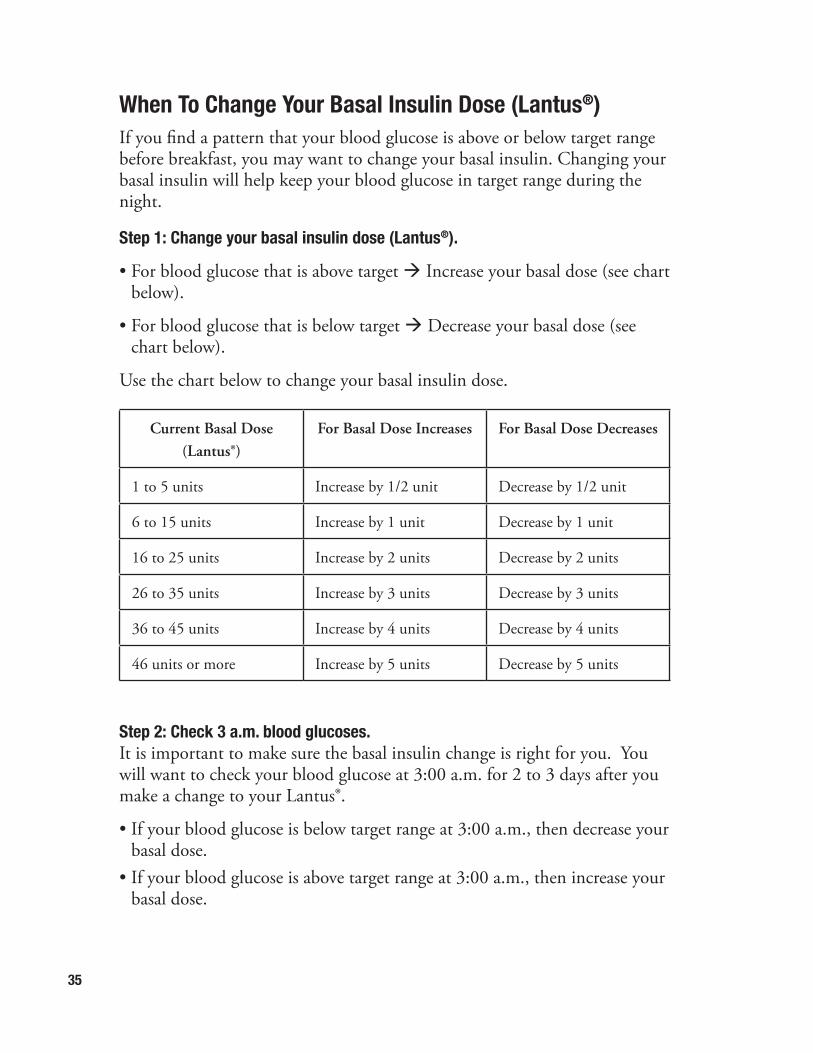
When To Change Your Basal Insulin Dose (Lantus®)If you find a pattern that your blood glucose is above or below target range before breakfast, you may want to change your basal insulin. Changing your basal insulin will help keep your blood glucose in target range during the night.
Step 1: Change your basal insulin dose (Lantus®).
• For blood glucose that is above target à Increase your basal dose (see chart below).
• For blood glucose that is below target à Decrease your basal dose (see chart below).
Use the chart below to change your basal insulin dose.
Current Basal Dose (Lantus®)
For Basal Dose Increases For Basal Dose Decreases
1 to 5 units Increase by 1/2 unit Decrease by 1/2 unit
6 to 15 units Increase by 1 unit Decrease by 1 unit
16 to 25 units Increase by 2 units Decrease by 2 units
26 to 35 units Increase by 3 units Decrease by 3 units
36 to 45 units Increase by 4 units Decrease by 4 units
46 units or more Increase by 5 units Decrease by 5 units
Step 2: Check 3 a.m. blood glucoses.It is important to make sure the basal insulin change is right for you. You will want to check your blood glucose at 3:00 a.m. for 2 to 3 days after you make a change to your Lantus®.
• If your blood glucose is below target range at 3:00 a.m., then decrease your basal dose.
• If your blood glucose is above target range at 3:00 a.m., then increase your basal dose.
36
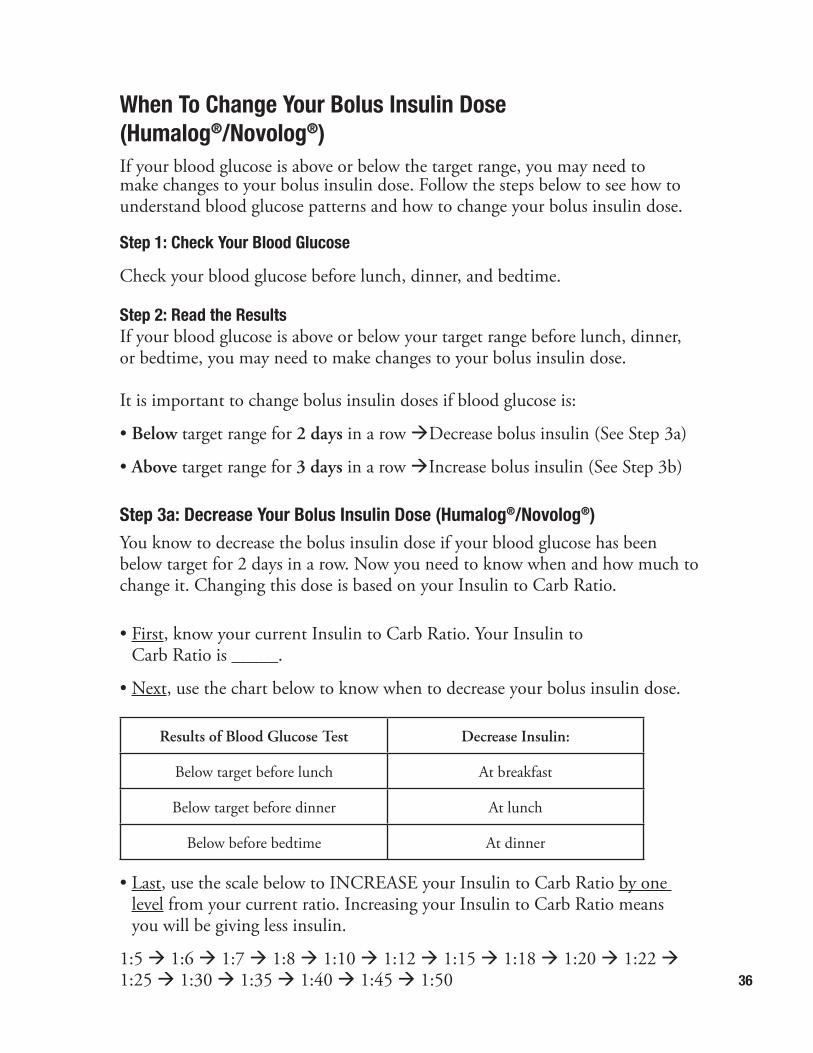
When To Change Your Bolus Insulin Dose (Humalog®/Novolog®)If your blood glucose is above or below the target range, you may need to make changes to your bolus insulin dose. Follow the steps below to see how to understand blood glucose patterns and how to change your bolus insulin dose.
Step 1: Check Your Blood Glucose
Check your blood glucose before lunch, dinner, and bedtime.
Step 2: Read the ResultsIf your blood glucose is above or below your target range before lunch, dinner, or bedtime, you may need to make changes to your bolus insulin dose. It is important to change bolus insulin doses if blood glucose is:
• Below target range for 2 days in a row àDecrease bolus insulin (See Step 3a)
• Above target range for 3 days in a row àIncrease bolus insulin (See Step 3b) Step 3a: Decrease Your Bolus Insulin Dose (Humalog®/Novolog®)You know to decrease the bolus insulin dose if your blood glucose has been below target for 2 days in a row. Now you need to know when and how much to change it. Changing this dose is based on your Insulin to Carb Ratio. • First, know your current Insulin to Carb Ratio. Your Insulin to
Carb Ratio is _____.
• Next, use the chart below to know when to decrease your bolus insulin dose.
Results of Blood Glucose Test Decrease Insulin:
Below target before lunch At breakfast
Below target before dinner At lunch
Below before bedtime At dinner
• Last, use the scale below to INCREASE your Insulin to Carb Ratio by one level from your current ratio. Increasing your Insulin to Carb Ratio means you will be giving less insulin.
1:5 à 1:6 à 1:7 à 1:8 à 1:10 à 1:12 à 1:15 à 1:18 à 1:20 à 1:22 à 1:25 à 1:30 à 1:35 à 1:40 à 1:45 à 1:50
37
• Last, use the scale below to DECREASE your Insulin to Carb Ratio by one level from your current ratio. Decreasing your Insulin to Carb Ratio means you will be giving more insulin.
1:50 à 1:45 à 1:40 à 1:35 à 1:30 à 1:25 à 1:22 à 1:20 à 1:18 à 1:15 à 1:12 à 1:10 à 1:8 à 1:7 à 1:6 à 1:5
What To Do After an Insulin ChangeContinue to monitor blood glucose levels.
• If glucoses continue to be below target range after 2 days, decrease insulin again.
• If glucoses continue to be above target range after 3 to 5 days, increase insulin again.
When To Call The DoctorAlways call the doctor if you are not sure about how to change your basal or bolus insulin doses.
• You can FAX your blood glucose log or pump/meter download to 614-722-3062.
• You can CALL in your blood glucose log to 614-722-4425.
• You can SEND in your blood glucose log using your “myChart” account.
Step 3b: Increase Your Bolus Insulin Dose (Humalog®/Novolog®).You know to increase the bolus insulin dose if your blood glucose has been above target for 3 days in a row. Now you need to know when and how much to change it. Changing this dose is based on your Insulin to Carb Ratio.
• First, know your current Insulin to Carb Ratio. Your Insulin to Carb Ratio is _____.
• Next, use the chart below to know when to increase your bolus insulin dose.
Results of Blood Glucose Test Increase Insulin:
Above target before lunch At breakfast
Above target before dinner At lunch
Above target before bedtime At dinner
38
High Blood Glucose (Hyperglycemia) and Ketones 9Hyperglycemia (said like: hi per glie SEE mee ah) is also called high blood glucose. It happens when blood glucose numbers are higher than 120 mg/dl.
What causes high blood glucose?• Eating more carbohydrates than you calculated for your insulin dose
• Not enough insulin is taken
• Stress
• Illness
How do I prevent high blood glucose?• Count your carbohydrate closely.
• Give the right insulin dose based on your meal and blood glucose number.
• Change the insulin doses when you see a pattern of high blood glucose levels.
• Give insulin for all the carbohydrate you eat.
How will I feel when my blood glucose is high?• Thirsty
• Need to go to the bathroom a lot
• Need to get up at night to go to the bathroom
• Tired
• Dry lips and mouth
39
What should I do if my blood glucose is high?• Drink fluids that do not have carbohydrates. Try to drink 1 full glass
(8 ounces) every 30 to 60 minutes.
• Use the high blood glucose correction dose.
• Check your urine or blood for ketones if blood glucose is higher than 300 mg/dl.
Why would I have ketones?You need glucose in every cell in your body to use for energy. Your body needs glucose and insulin in your blood. When there is not enough glucose or not enough insulin, your cells will not have glucose to use for energy.
When cells do not have glucose to use for energy:
• The body starts to use fat for energy. à
• Ketones are made when fat is used for energy. à
• Ketones are in the blood and in the urine. à
• Ketones are acids. à
What 2 things does your body need to prevent ketones?
1. _________________________________________________________
2. _________________________________________________________
High blood glucose, by itself, is not an emergency. High blood glucose and small, moderate, or large ketones IS something you
should take care of right away.
40
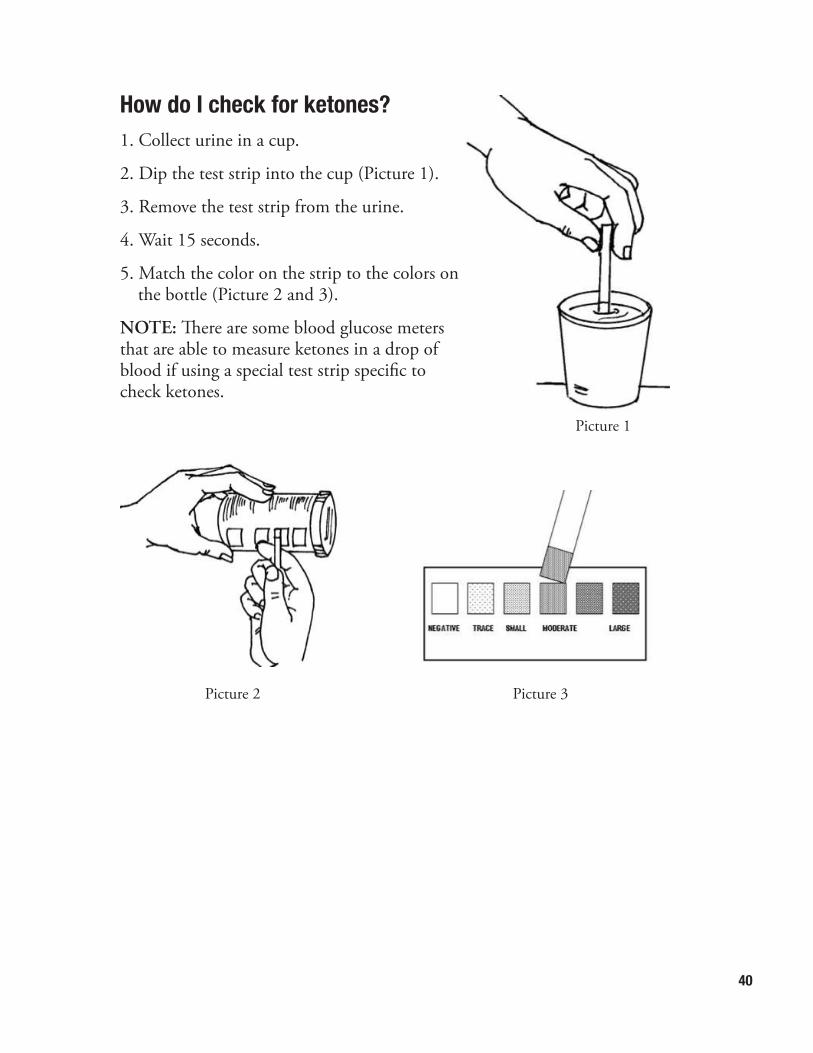
How do I check for ketones?1. Collect urine in a cup.
2. Dip the test strip into the cup (Picture 1).
3. Remove the test strip from the urine.
4. Wait 15 seconds.
5. Match the color on the strip to the colors on the bottle (Picture 2 and 3).
NOTE: There are some blood glucose meters that are able to measure ketones in a drop of blood if using a special test strip specific to check ketones.
Picture 1
Picture 2 Picture 3
41
Expires May: 2008
What do I do if I have ketones that are small, moderate, or large?You will need more rapid-acting insulin (Humalog®, Novolog®, or Apidra®). This is called a ketone bolus.
A ketone bolus is:
Based on your daily Lantus® basal dose or your total daily basal insulin dose on your pump.
• If you have small ketones, give 5% (0.05) of your Lantus® dose.
• If you have moderate or large ketones, give 10% (0.1) of your Lantus® dose.
Dose is based on Lantus® dose, but use Humalog®/Novolog® for ketone bolus.
Tips
• Check the expiration date on the bottle of test strips. Do not use them if it is past the date.
• Once the ketone bottle is opened, get new ketone test strips after 6months.
• Keep the ketone test strips in the bottle that they come in with the lid on.
42
Example: Your daily Lantus dose is 20 units.
• 20 x 0.05 = 1, so:
o Give 1 unit of Humalog® or Novolog® for small ketones.
• 20 x 0.1 = 2, so:
o Give 2 units of Humalog® or Novolog® for moderate or large ketones.
Your rapid-acting insulin dose at that time will have three parts:
• Meal bolus
• Correction bolus
• Ketone bolus
All three bolus doses are added together to equal the rapid-acting insulin dose.
What is your Lantus® insulin dose?
________________________________________________________
What is 10% of your Lantus® insulin dose?
________________________________________________________
What is your ketone bolus dose for small ketones?
________________________________________________________
What is your ketone bolus dose for moderate or large ketones?
________________________________________________________
Refer to the Diabetes SOS: Sick Day Self-Management guidelines and ketone correction Bolus Worksheet on page 94.
Use one of the following flow sheets that most closely fits your symptoms:
• Sick day when you are able to drink.
• Sick day when you are vomiting and not able to drink.
43
Important to Remember
Do not exercise if you have ketones that are small, moderate, or large.
Are ketones a problem?Ketones can make you very sick. When there are ketones in the blood, the blood can become acidotic. This is called Diabetic Ketoacidosis (DKA).
Signs of ketoacidosis:
• Fast breathing
• Fruity smell to the breath
• Hard to wake up
• Feeling sick to the stomach (nausea) or having belly pain
How do I prevent diabetic ketoacidosis (DKA)? • Check ketones if blood glucose is higher than 300 mg/dl and when you
are sick.
• Give the right amount of ketone bolus if you have small, moderate, or large ketones.
Important to Remember if You Have Ketones
• If signs of ketoacidosis are present, contact the Diabetes Center right away or go to your local emergency department.
• If you have ketones, check your blood glucose and ketones every 3 hours.
• Give a ketone bolus every 3 hours until ketones are negative.
• Keep eating carbohydrates and take extra Humalog®/Novolog® with meals (ketone bolus).
• Take the same dose of long-acting Lantus® insulin that you usually take.
• Drink 1 full cup (8 ounces) of water every 30 to 60 minutes.
44
• Call the Endocrinology office or doctor on call when:
o You have used a ketone bolus for moderate or large ketones twice and your ketones are still moderate or large.
o You have treated a low blood glucose twice and your blood glucose is still low.
o You have thrown up (vomited) 3 times.
Important to Remember
• DKA is dangerous!!
• When you have signs of DKA, you need to act quick by:
o Calling the endocrinology office or doctor on call, OR
o Going to the local emergency department.
45
Low Blood Glucose (Hypoglycemia) 10Hypoglycemia (said like: hi poe glie SEE mee ah), or low blood glucose, is the most common problem with insulin therapy. Low blood glucose is when the blood glucose falls below 70 mg/dl. Hypoglycemia can happen very quickly.
What causes low blood glucose? • Not enough carbohydrates eaten
• Too much insulin given
• More exercise than normal
How do I prevent low blood glucose?• The best way to prevent low blood glucose is to take insulin based on the
amount of carbohydrates you are eating, your blood glucose level, and your planned activity level.
• Plan ahead if you know you will be doing more activity than normal.
• Test your blood glucose regularly.
What do I need to be ready for a low blood glucose?• Know YOUR signs of low blood glucose. Your family and friends will also
need to learn your signs of low blood glucose so they can help you treat it.
• Always keep some form of sugar with you.
• Always keep your blood glucose meter with you.
• Always have a Glucagon Emergency Kit (see page 49).
• Always wear a medical necklace or bracelet, or carry a medical ID card in your wallet.
46
What are the signs of low blood glucose?Because sugar (glucose) is the main fuel for the brain, a sudden drop in the glucose level can cause the following symptoms:
Early Signs Late Signs Signs While Sleeping
• Shakiness
• Nervousness
• Stomach ache
• Weakness
• Blurry vision
• Dizziness
• Pale skin
• Sweating
• Headache
• Personality change
• Seizures
• Confusion
• Irritability, crankiness
• Unconsciousness
• Nightmares
• Waking up suddenly
• Sweating; wet clothes or sheets
• Fast heart beat
• Can’t fall back to sleep; restless
How do I treat low blood glucose with the 15/15 Rule?Step 1: Stop what you are doing if you have any signs of low blood glucose, and check your blood glucose. You may have to:
• Let your coach know you need a break.
• Leave class in the middle of a lesson and go to the nurse’s office.
Step 2: Read the results.
• For children up to 1 year old, treat blood glucose of 90 or below.
• For children 1 to 4 years old, treat a blood glucose of 80 or below.
• For children 5 years old or more, treat a blood glucose of 70 or below.
47
Step 3: Treat the low blood glucose with a 15 gram carbohydrate snack that works fast (Picture 1). This is called a fast-acting carbohydrate. If your blood glucose is low, your body needs sugar quickly. If these symptoms are not treated, seizures and/or unconsciousness can happen.
Eat a 15 gram fast-acting carbohydrate. One of the following would be a good choice:
• 4 ounces of 100% fruit juice
• 3 to 4 glucose tablets
• 1 tube of glucose gel
• Candy, like Skittles or gummy bears.
Do not use candy bars or other candy that has fat.
Step 4: Check your blood glucose again in 15 minutes. Do this even if you feel better.
• If your blood glucose is still below target range (70 - 80 mg/dl), repeat steps 3 and 4.
• If your blood glucose is above target range (70-80 mg/dl) and it is more than 1 hour until your next meal, eat another 15 gram carbohydrate snack with protein. This can be any of the following:
o Peanut butter or cheese and crackers
o Half of a sandwich
o Granola bar
o One glass of milk
Picture 1: Always carry some kind of glucose with you, like glucose tablets or fruit juice.
48
What do I do about low blood glucose at nighttime?It is a good idea to keep small boxes or cans of juice at your bedside to treat low blood glucose in the middle of the night. Make sure to follow up with a snack of 15 grams of complex carbohydrate and protein before going back to bed. Cheese and crackers are a good choice. You do not need to eat a full meal.
Important to Remember
• Remember, if blood glucose is below target before a meal, treat before you eat. When blood glucose is above 70 mg/dl, take your insulin before you eat a meal or another snack.
• If you have signs of low blood glucose, but cannot test your blood, you should treat for low blood glucose anyway. Use the 15/15 Rule, giving yourself 15 grams of carbohydrate and checking your blood glucose in 15 minutes.
• Have a signal for your teacher or your coach that lets them know you are having signs of low blood glucose.
49
Glucagon and Mini-Dose Glucagon 11GlucagonFood or drink should not be given to a person with low blood glucose if there is a chance he or she might choke. Glucagon is a hormone the body makes that allows sugar that is stored in the body to be released. Glucagon comes in an emergency kit that has liquid in a syringe and powder in a vial.
Give glucagon by injection if the person with low blood glucose:
• Cannot swallow
• Is unconscious
• Is seizing (uncontrollable jerking movements)
How to give glucagon by injection:
1. Remove the cap from the vial with the glucagon powder.
2. Remove the cap from the needle on the syringe.
3. Inject all of liquid in the syringe into the vial with the powder (Picture 1).
4. Keep the syringe in the vial while you roll or swirl the vial gently. Do this until the solution is clear. Picture 1
50
5. If your child is older than 5 years and weighs more than 45 pounds, draw up all of medicine into the syringe. If your child is younger than 5 years or weighs less than 45 pounds, draw up the medicine to the 0.5 mg mark on syringe (Picture 2).
6. Inject the medicine under the skin or into the muscle where you would give an insulin injection (See Chapter 6, Insulin Injections, page 28).
7. Turn the person on their side. Throwing up (vomiting) may happen after glucagon is given.
8. Call 911 (Picture 3).
After giving glucagon:
• Check blood glucose every 15 minutes.
• When the person is awake and can take food or drink, give 15 grams ofcarbohydrate.
• When you can, call the endocrinology office or doctor on call. Insulin doses often need to be changed.
Picture 2 Picture 3
Glucagon is a safe medicine to give. If in doubt, give it.
51
Mini-Dose GlucagonIf a person has signs of mild to moderate low blood glucose and cannot eat or is vomiting, a small dose of glucagon may be given to raise the blood glucose. This is called mini-dose glucagon.
Mini-dose glucagon will usually raise blood glucose 50 to 100 mg/dl (points) in 30 minutes without causing nausea.
How to give mini-dose glucagon:
1. Open the glucagon emergency kit.
2. Mix the liquid with powder as instructed on the lid of the kit.
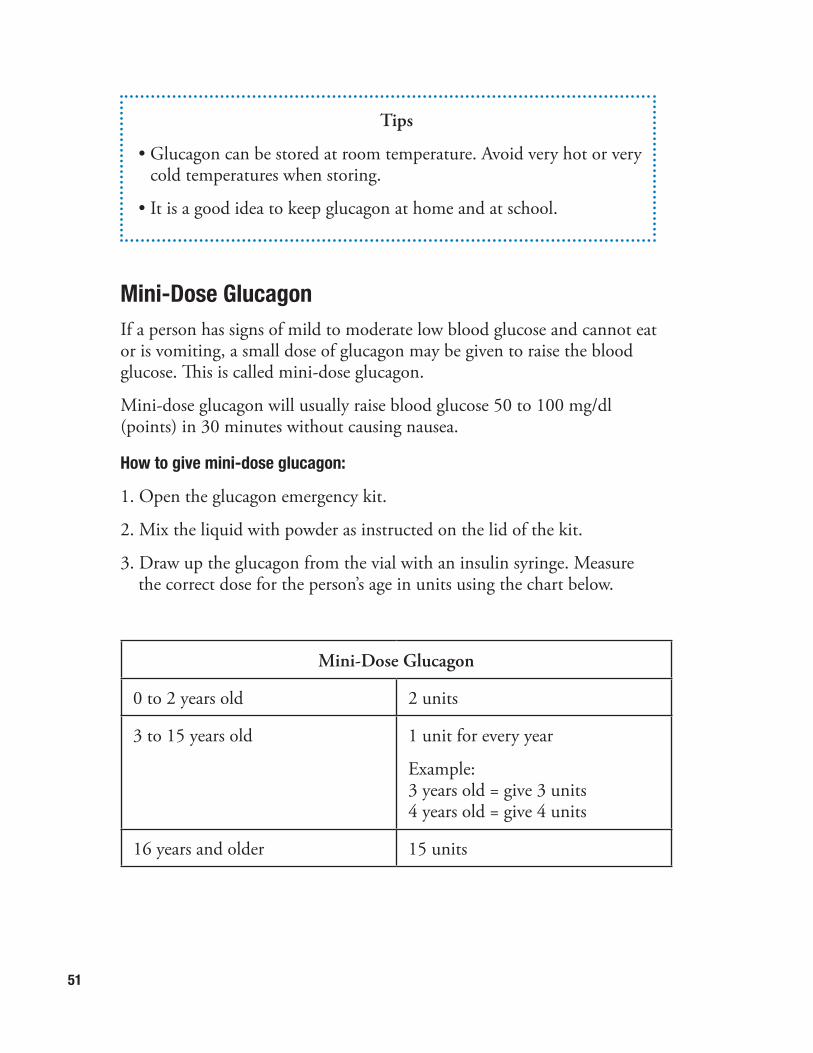
3. Draw up the glucagon from the vial with an insulin syringe. Measure the correct dose for the person’s age in units using the chart below.
Mini-Dose Glucagon
0 to 2 years old 2 units
3 to 15 years old 1 unit for every year
Example:3 years old = give 3 units4 years old = give 4 units
16 years and older 15 units
Tips
• Glucagon can be stored at room temperature. Avoid very hot or very cold temperatures when storing.
• It is a good idea to keep glucagon at home and at school.

52
4. Inject the mini-dose of glucagon the same way you would inject insulin (See Chapter 6, Insulin Injections, page 29).
5. Store the leftover glucagon in the refrigerator.
6. Check the blood glucose every 15 minutes. If the blood glucose has not started to rise at 15 minutes or is not above 80 mg/dl at 30 minutes, repeat the mini-dose. Make sure this second dose is double the amount of mini-dose glucagon you gave the first time.
7. Give the same amount of mini-dose glucagon injection you gave the first time, every hour as needed, to keep the blood glucose above 80 mg/dl.
8. The glucagon vial can be used for 24 hours after mixing if it is kept in the refrigerator.
9. Throw the mixed glucagon vial away after 24 hours.
53
Sick Days 12Blood glucose levels are often harder to control when a person with diabetes is sick. Illness makes the body release stress hormones. This causes high blood glucose numbers. Illness is a common reason people with diabetes get ketones in their blood and urine. Decreased appetite or throwing up (vomiting) can lead to low blood glucose. Ketones can form even when blood glucose numbers are in target or low. Good control of blood glucose is not usually possible during illness. The goal is to keep from having very high or very low blood glucose and to prevent or treat ketones.
General Rules• If you do not feel like eating much, carbohydrates may be given in the
form of liquids instead of solid food.
• Keep taking your usual dose of long-acting insulin (Lantus® or Levemir®). Do this even when you are vomiting or do not want to eat.
• Check blood glucose every 3 hours during the day and night.
• Check ketones every 3 hours. Keep checking until you have no ketones and the result on your ketone strip stays negative.
• Give insulin for ketones every 3 hours.
• Drink a lot of fluids. Try to drink 8 ounces (1 full glass) every 30 to 60 minutes.
• Follow your Diabetes SOS: Sick Day Self-Management guidelines (see page 94) for help managing your diabetes.
Image credited to: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health
54
Carbohydrates for Sick Days
Foods Liquids
• Bread or Toast
• Crackers
• Applesauce
• Regular Jello®
• Pedialyte®
• Gatorade®
• Regular Popsicles
• Soup broth
Medicines
Many prescription and over-the-counter medicines have sugar and carbohydrates in them. Ask your pharmacist if you can get the medicine in a sugar-free form. If your child is taking a medicine that might raise his or her blood glucose, make a note of it in the logbook. Keep giving the medicine your child’s regular doctor tells you to give to treat the illness or fever.
Surgery & Diabetes
Your child’s insulin dose may need to be changed if your child has surgery or a procedure that needs anesthesia. The dose will depend on how long the surgery is and how long he or she is without food and drink before the surgery. This includes dental procedures. If possible, your child’s surgery should be done first thing in the morning.
Call the Diabetes Center office as soon as you know that a surgery has been scheduled. The diabetes doctor and surgeon will need to make a plan for your child’s diabetes before, during, and after the procedure.
55
Nutrition 13Children need good nutrition to grow into healthy adults. The American Academy of Pediatrics recommends healthy eating for children of all ages. Nutrition recommendations may be different depending on age and gender.
While your child is in the hospital, a registered dietitian (RD) will meet with you and your family to talk about the different kinds of foods eaten at home. The dietitian will ask about the foods and drinks your child has at breakfast, lunch, dinner, and snacks. Your family will then learn about healthy eating so that diabetes can be better managed. It is important to remember that nutrition recommendations for type 1 diabetes and type 2 diabetes may be different.
Nutrition and CarbohydratesAs part of the education, a dietitian will give your family instructions on how to count grams of carbohydrates. This is important because carbohydrates are the part of food which raises blood glucose. Carbohydrates are in grains, like bread, rice, and pasta. They are also in milk, fruits, and vegetables. Carbohydrates are in foods with added sugar, like cake, cookies, and sweets.
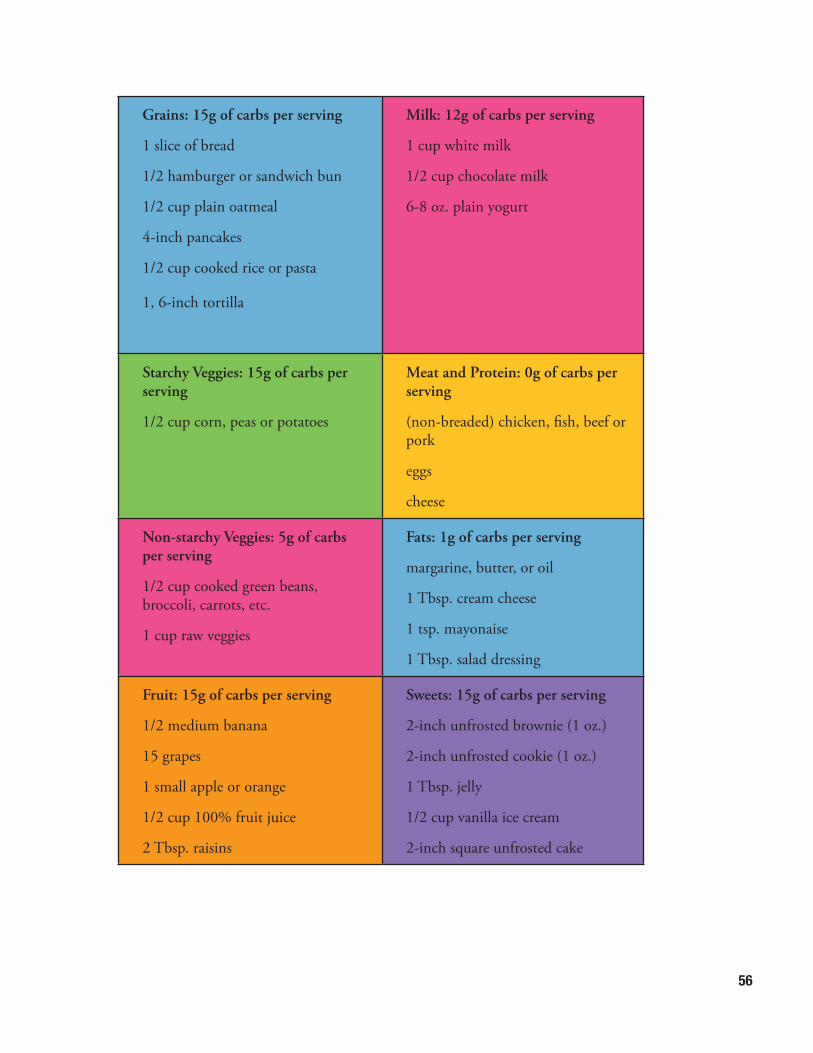
The chart on the next page will help your family learn about the carbohydrate amounts in different foods.
56
Grains: 15g of carbs per serving
1 slice of bread
1/2 hamburger or sandwich bun
1/2 cup plain oatmeal
4-inch pancakes
1/2 cup cooked rice or pasta
1, 6-inch tortilla
Milk: 12g of carbs per serving
1 cup white milk
1/2 cup chocolate milk
6-8 oz. plain yogurt
Starchy Veggies: 15g of carbs per serving
1/2 cup corn, peas or potatoes
Meat and Protein: 0g of carbs per serving
(non-breaded) chicken, fish, beef or pork
eggs
cheese
Non-starchy Veggies: 5g of carbs per serving
1/2 cup cooked green beans, broccoli, carrots, etc.
1 cup raw veggies
Fats: 1g of carbs per serving
margarine, butter, or oil
1 Tbsp. cream cheese
1 tsp. mayonaise
1 Tbsp. salad dressing
Fruit: 15g of carbs per serving
1/2 medium banana
15 grapes
1 small apple or orange
1/2 cup 100% fruit juice
2 Tbsp. raisins
Sweets: 15g of carbs per serving
2-inch unfrosted brownie (1 oz.)
2-inch unfrosted cookie (1 oz.)
1 Tbsp. jelly
1/2 cup vanilla ice cream
2-inch square unfrosted cake
57
After you learn how to count carbohydrates, the meal plan can be much more flexible. It is important to know how to count carbohydrates, and we want to help. Our dietitians will work with your family while your child is in the hospital and at follow-up clinic visits. You will be given written information that will help your family learn more about carbohydrate counting.
Free FoodsA ‘free food’ is a food that is very low in carbohydrates. Typically, these foods have 5 grams (g) of carbohydrate or less per serving. Your child can have free foods for snacks to avoid giving an extra insulin injection.
Here are some examples of free foods:
• Sugar-free Jell-O® topped with 2 Tbsp whipped topping
• 1 cup low-fat microwave popcorn
• Celery with 1 Tbsp natural peanut butter or cream cheese
• Pickles
• 1/2 cup cooked, non-starchy vegetables, like green beans, broccoli, or cauliflower
• 1/2 cup low-fat cottage cheese
• 1 sugar-free popsicle
• 1/2 cup raw vegetables, dipped in 1/4 cup salsa or 2 Tbsp guacamole
• String cheese
• Eggs
• Turkey jerky
• 1/4 cup peanuts
• 20 almonds (Picture 1)
• Deli meat
• Chicken salad or tuna salad with celery sticks or in a lettuce wrap
Be careful of portion sizes of some free foods. They may be high in calories and fat. For healthy eating, try to stick with one snack between meals.
Picture 1
58
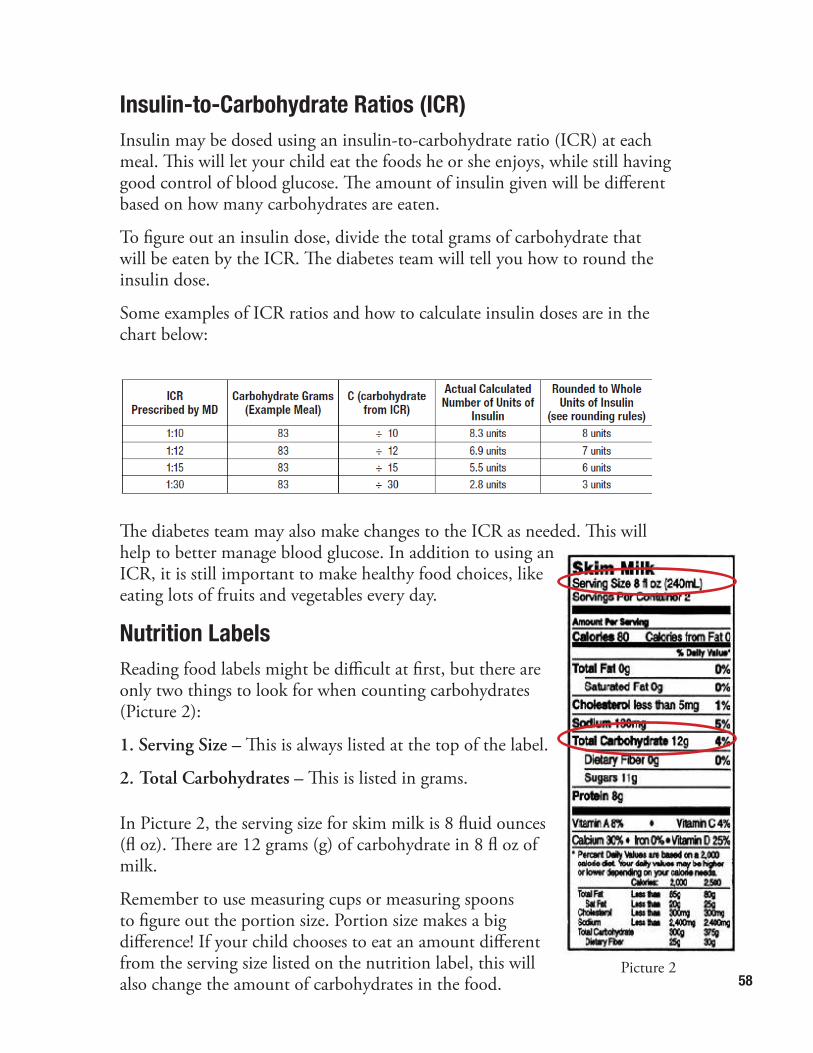
Insulin-to-Carbohydrate Ratios (ICR)Insulin may be dosed using an insulin-to-carbohydrate ratio (ICR) at each meal. This will let your child eat the foods he or she enjoys, while still having good control of blood glucose. The amount of insulin given will be different based on how many carbohydrates are eaten.
To figure out an insulin dose, divide the total grams of carbohydrate that will be eaten by the ICR. The diabetes team will tell you how to round the insulin dose.
Some examples of ICR ratios and how to calculate insulin doses are in the chart below:
The diabetes team may also make changes to the ICR as needed. This will help to better manage blood glucose. In addition to using an ICR, it is still important to make healthy food choices, like eating lots of fruits and vegetables every day.
Nutrition LabelsReading food labels might be difficult at first, but there are only two things to look for when counting carbohydrates (Picture 2):
1. Serving Size – This is always listed at the top of the label.
2. Total Carbohydrates – This is listed in grams.
In Picture 2, the serving size for skim milk is 8 fluid ounces (fl oz). There are 12 grams (g) of carbohydrate in 8 fl oz of milk.
Remember to use measuring cups or measuring spoons to figure out the portion size. Portion size makes a big difference! If your child chooses to eat an amount different from the serving size listed on the nutrition label, this will also change the amount of carbohydrates in the food.
Picture 2
59
Example: How many grams of carbohydrates would you count if drinking 2 cups (16 fl oz) of milk?
1 cup (8 fl oz) = 12g carbohydrate
12g carbohydrate x 2 cups = 24g of carbohydrate
Once your family feels comfortable with doing this, the dietitian may go over harder label reading at future clinic appointments.
Other Foods to Think AboutAn ICR gives flexibility with the foods someone with diabetes can eat. However, there are a few things that the dietitians strongly encourage not eating. These foods include regular soda, pop, and syrup, like maple syrup or pancake syrup. This is because they are made of a lot of sugar. These two things can make blood glucoses go very high, very quickly. There are many other options! Choose drinks with zero grams of carbohydrate, like diet soda pop, sugar-free powdered drink mixes, or flavored water. Plain water is always one of the healthiest options you can give your child as a drink to hydrate. Try adding slices of fresh fruit to plain water, like oranges, lemons, or limes. This adds a lot of flavor! Look for sugar-free syrup at the grocery store, or think about putting jam, butter or peanut butter on top of pancakes or waffles. Remember, “sugar-free” does not always mean “carbohydrate-free.” Always check the nutrition label.
Additional ResourcesThere are many resources to help with carbohydrate counting. The Calorie King® book provides the carbohydrate amount of thousands of foods and drinks (Picture 3). It has nutrition information from popular chain restaurants. Your family will get a copy of the Calorie King® book to take home, but extra copies can be bought from many book stores or grocery stores. There are also many apps for smartphones and tablets to help count carbohydrates. Ask the Diabetes Team members for help with this.
Picture 3
60
Eating OutKeep these tips in mind before going out to eat:
• Plan ahead – Remember to take a carbohydrate counting reference book to look up serving sizes and carbohydrate amounts. You can also use an app to find this information. Many restaurants also give nutrition facts for their food online or in a brochure. Think about looking this up ahead of time.
• Watch serving sizes – Know serving sizes by practicing measuring skills at home. This helps your family be sure that portion sizes are right when dining out. If the portion size served is too large, take the extra food home. This is important because restaurants usually serve very large portions.
• Ask about ingredients and preparation – If you do not know how an item on the menu is made, ask the waiter or waitress. For lower fat choices, avoid fried foods and cut the fat off of meats. If you do choose to eat fried foods, remember to count the carbohydrates in the breading and flour coating. Sauces, like ketchup, BBQ, sweet and sour, and honey mustard have carbohydrates. Think about asking for sauces and dressingsto be served on the side. This helps you easily control and measure the
amount the amount you eat.
• Continue to avoid sweetened drinks like you would at home.
Counting Carbohydrates in Homemade RecipesThere are a few extra steps involved when calculating the amount of carbohydrates in a home cooked meal. Follow the steps (below) to do this.
1. Make a list of each ingredient and how many grams of carbohydrate are in each. Use nutrition labels, the Calorie King® book, or phone apps for this step.
Example: If the recipe calls for a 14 ounce (oz) can of tomatoes, the label may state the serving size is ½ cup and that there are 3.5 servings per container.
a. Read the label for total carbohydrates.
• Ex. Each ½ cup serving contains 4g of carbohydrate
b. Multiply the number of servings (3.5) by the number of carbs per serving (4g) to find the total carbohydrates in 1 can of tomatoes.
• Ex. 3.5 x 4 g = 14 g carbohydrates for the entire can of tomatoes
61
2. Add up the total grams of carbohydrate for all ingredients in the entire recipe.
3. Divide the total grams of carbohydrate by the number of servings in the recipe.
4. This will give you the grams of carbohydrate per serving.
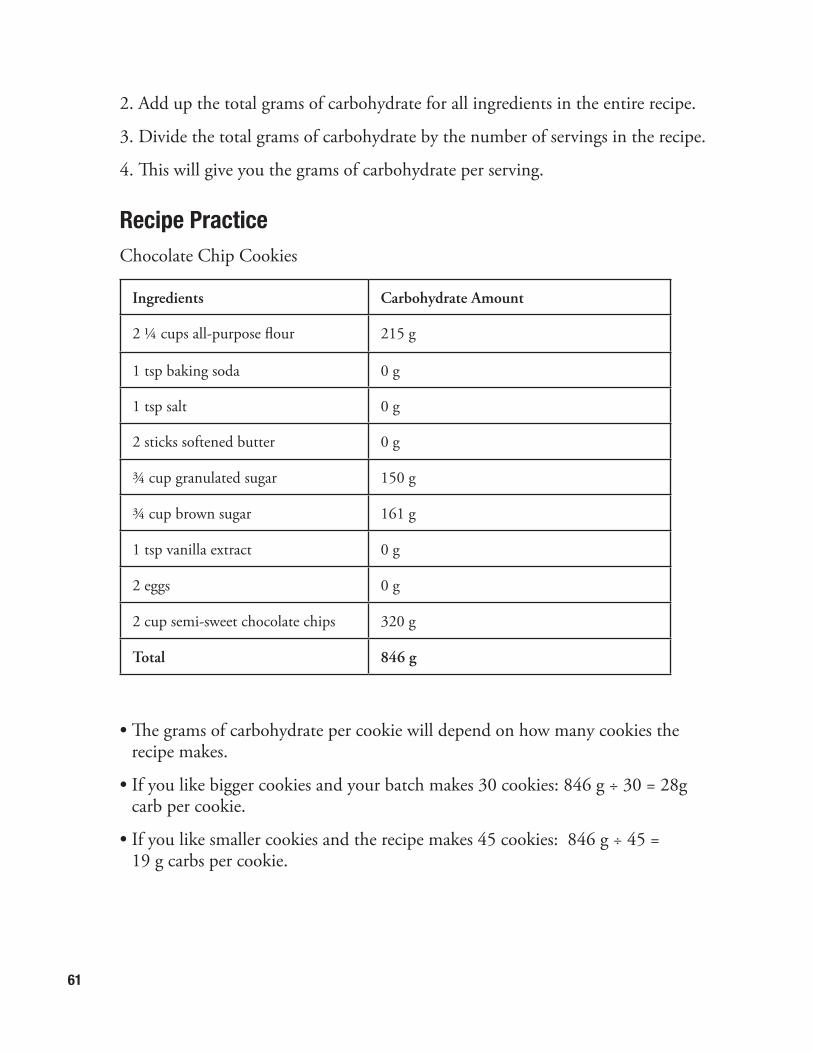
Recipe PracticeChocolate Chip Cookies
Ingredients Carbohydrate Amount
2 ¼ cups all-purpose flour 215 g
1 tsp baking soda 0 g
1 tsp salt 0 g
2 sticks softened butter 0 g
¾ cup granulated sugar 150 g
¾ cup brown sugar 161 g
1 tsp vanilla extract 0 g
2 eggs 0 g
2 cup semi-sweet chocolate chips 320 g
Total 846 g
• The grams of carbohydrate per cookie will depend on how many cookies the recipe makes.
• If you like bigger cookies and your batch makes 30 cookies: 846 g ÷ 30 = 28g carb per cookie.
• If you like smaller cookies and the recipe makes 45 cookies: 846 g ÷ 45 = 19 g carbs per cookie.
62
Healthy EatingIn addition to managing diabetes, it is important to remember to make healthy food choices for good nutrition. Even people who do not have diabetes need to eat a healthy, balanced diet. This includes eating foods from each of the five food groups: grains, dairy, meat and protein, fruits, and vegetables.
Fruits and Vegetables
Try to include different fruits and vegetables at every meal. Fruits and vegetables are not only low in calories, but they have many vitamins and minerals to keep us healthy. They also have fiber, which helps keep us feeling full. Make a goal for half of the plate to be filled with fruits and vegetables at meals.
Dairy
Try to include three servings of dairy each day. Dairy has calcium, a mineral that helps keep bones strong. Milk, yogurt, and cheese are good sources of calcium. One cup of milk is considered one serving of dairy. Low-fat or reduced-fat dairy products can help you keep a healthy weight.
Meats and Proteins
Choose lean meats for heart health. Lean meats include chicken, turkey, fish and ground beef that is at least 90% lean. These items are lower in calories and fat. Meat is a good source of protein and iron to keep strong muscles. Other good sources of protein include beans, lentils, nuts, seeds, tofu, and eggs.
Grains
The best choices from the grains group are whole grains. Whole grains offer more nutrition and are also higher in fiber. Look for items at the store that list whole grains as the first ingredient on the nutrition label.
Portion Size
Portion control is important to help stay at a healthy weight. For example, one serving of meat is 3 ounces, or about the size of a deck of cards. Use the plate model below as a map to help guide portion sizes at meals. For more information, visit www.choosemyplate.gov.
63
Sweeteners
In the past, people with diabetes were told to stay away from high-sugar foods because they were thought to cause high blood glucose. Now, studies suggest that total grams of carbohydrate are more important than how much sugar is in the food. People with diabetes can now enjoy foods with sugar as long as insulin is given to cover these carbohydrates. However, it does not mean that sweets can be eaten in unlimited amounts!
There are several types of sweeteners you can use. The differences between these products are described on the next page.
Important to Remember about Sweets
Remember, someone with diabetes can still have sweets, but should try to eat them in moderation. This means that they should not be eaten every day. Many baked goods, like cake and cookies, have extra sugar. They do not have much nutritional value. Carbohydrates are the body’s main way of getting energy, but it is important to choose healthy carbohydrates, like fruits, veggies, whole grains, and low-fat dairy. These will give the body the best fuel.
Facts to Remember
• Foods high in sugar are often high in both calories and fat.
• Most foods high in sugar have poor nutritional value because they are not good sources of vitamins, minerals, and protein.
• Foods high in sugar are high in carbohydrates; therefore, the portions tend to be small.
• A food labeled “sugar-free” does not always mean it is “carbohydrate-free”.
64
Artificial Sweeteners
An artificial sweetener does not have calories or carbohydrates.
It will not change blood glucose levels.
Right now, five artificial sweeteners are approved by the Food and Drug Administration (FDA) as safe to eat:
• Acesulfame-K: Brand names include Sweet-One® and Sunett®. It may be used in cooking and baking. It does not leave an after-taste.
• Aspartame: Brand names include Equal® and Nutrasweet®. It is protein-based and leaves no after-taste. It loses its sweet taste after being in high temperatures for long periods of time. This means it may not be the best choice for cooking and baking.
• Saccharin: Brand names include Sugar-Twin® and Sweet-n-Low®. It comes in a powder, liquid, or tablet form. It may have a bitter after-taste. Use it in small amounts and/or at the end of cooking.
• Sucralose: Brand name is Splenda®. It is made from sugar. It is stable at high temperatures, so it is good for baking. Sucralose tastes the most like sugar.
• Neotame: Neotame is not used often in foods. Since it is heat stable, it can also be used in cooking and baking. Not very much is needed to sweeten foods.
The American Diabetes Association states that artificial sweeteners are okay for people with diabetes to use because they are safe for all people.
65
Sugar Alcohols
Sugar alcohols have less calories and carbohydrate than regular sugar, but they do still have carbohydrates. This means they will still raise blood glucose. They are in “sugar-free” cookies, candy, chewing gum, breath mints, low-sugar granola bars, and even ice cream. They may cause diarrhea or stomach aches when eaten in large amounts because of the way they are digested by the body. Make sure to read nutrition labels for the total grams of carbohydrates, even when foods are labeled as sugar-free.
Common sugar alcohols that you may see in a list of ingredients include:
• Sorbitol
• Mannitol
• Xylitol
• Isomalt
• Hydrogenated starch hydrolysates
Sugar
Sugar comes in many forms. All forms have calories and carbohydrates. Here are some other common names for sugar:
• Refined sugar
• High fructose corn syrup
• Honey
• Concentrated fruit juice
• Maple, brown, or powdered sugar
• Dextrose
• Agave
66
Tips for School
School Lunch
It is your choice if you want to take a lunch to school or eat the school lunch.
Here are some hints for school lunches:
• Visit with school cafeteria staff to find out portion sizes and the substitution policy.
• Ask for nutrition information for school meals.
• Find out if the school offers single food items by themselves. Set guidelines for which are okay for your child to choose and when.
• Review the school lunch menu ahead of time to see which days you may need to pack a lunch from home.
• If you are packing a lunch, write down the total grams of carbohydrate for the meal and put it in the lunch box. This helps the school staff calculate insulin doses.
Parties at School
Here are some tips for handling school parties:
• Tell the teacher that you want to know ahead of time when there will be a school party, if possible, and what will be served.
• Make sure your child’s teacher knows about any foods with carbohydrates that may need insulin coverage. Even something as small as one piece of candy can affect blood glucose.
• If the school staff cannot give insulin during the time of the party or do not feel comfortable, encourage your child save party snacks to enjoy when he or
she gets home.
• Send “free foods” or desserts with a known carbohydrate count to school for your child and his or her class to eat during the party.
67
Common Measurements
Liquid (Fluid Ounces [oz.]) Measurements
½ oz. = 1/16 cup = 1 tablespoon1 oz. = ⅛ cup = 2 tablespoons2 oz. = ¼ cup = 4 tablespoons4 oz. = ½ cup = 8 tablespoons6 oz. = ¾ cup = 12 tablespoons8 oz. = 1 cup = 16 tablespoons16 oz. = 2 cups = 1 pint32 oz. = 4 cups = 1 quart Weight Measurements
½ oz. = 1/32 lb. = 15 grams1 oz. = 1/16 lb. = 30 grams2 oz. = ⅛ lb. = 57 grams4 oz. = ¼ lb. = 113 grams8 oz. = ½ lb. = 226 grams16 oz. = 1 lb. = 454 grams32 oz. = 2 lb. = 903 grams
Other Measurements
3 teaspoons (tsp.) = 1 tablespoon (Tbsp.)⅓ cup = 5 ⅓ tablespoons⅛ teaspoon = Dash½ teaspoon = 30 drops3 tablespoons = 1 ½ ounces (oz)1 gallon = 4 quarts = 8 pints = 16 cups = 128 oz
68
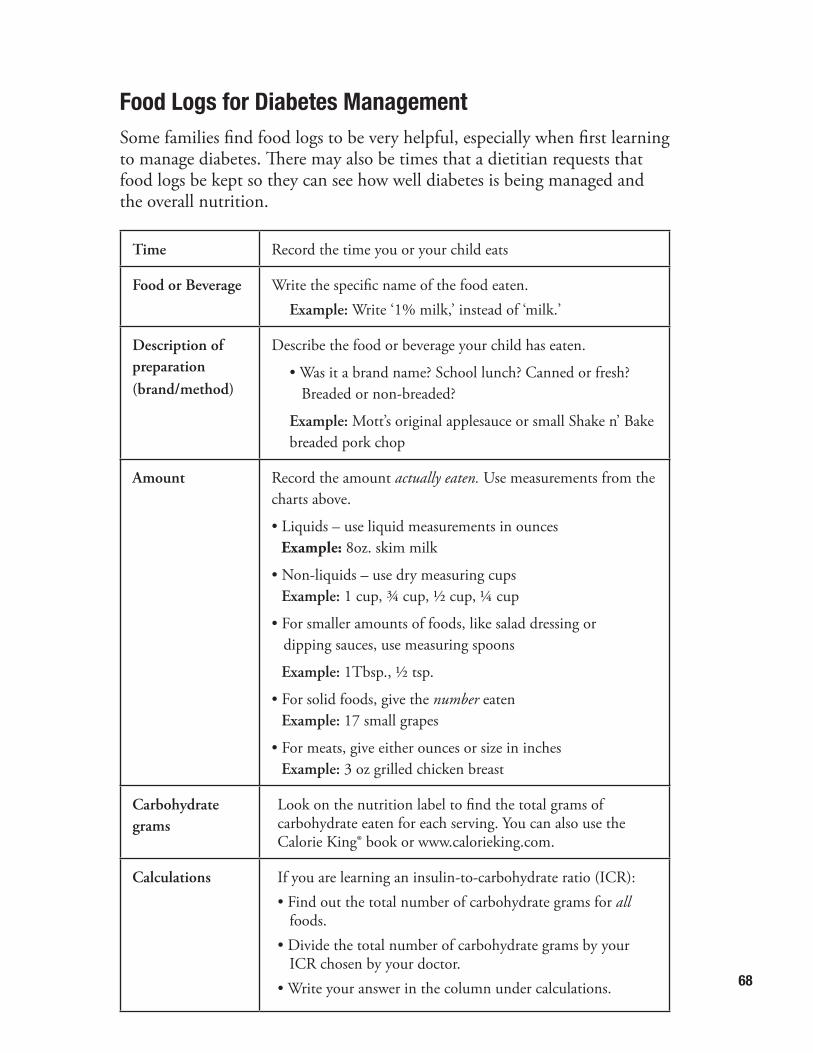
Food Logs for Diabetes ManagementSome families find food logs to be very helpful, especially when first learning to manage diabetes. There may also be times that a dietitian requests that food logs be kept so they can see how well diabetes is being managed and the overall nutrition.
Time Record the time you or your child eats
Food or Beverage Write the specific name of the food eaten. Example: Write ‘1% milk,’ instead of ‘milk.’
Description of preparation (brand/method)
Describe the food or beverage your child has eaten.
• Was it a brand name? School lunch? Canned or fresh? Breaded or non-breaded?
Example: Mott’s original applesauce or small Shake n’ Bake breaded pork chop
Amount Record the amount actually eaten. Use measurements from the charts above.
• Liquids – use liquid measurements in ounces Example: 8oz. skim milk
• Non-liquids – use dry measuring cups Example: 1 cup, ¾ cup, ½ cup, ¼ cup
• For smaller amounts of foods, like salad dressing or dipping sauces, use measuring spoons
Example: 1Tbsp., ½ tsp.
• For solid foods, give the number eaten Example: 17 small grapes
• For meats, give either ounces or size in inches Example: 3 oz grilled chicken breast
Carbohydrate grams
Look on the nutrition label to find the total grams of carbohydrate eaten for each serving. You can also use the Calorie King® book or www.calorieking.com.
Calculations If you are learning an insulin-to-carbohydrate ratio (ICR):• Find out the total number of carbohydrate grams for all
foods.• Divide the total number of carbohydrate grams by your
ICR chosen by your doctor.• Write your answer in the column under calculations.
69
Important to Remember
• Write down all the information IMMEDIATELY after eating. It is easy to forget what foods were eaten if you wait until the end of the day to log or record it.
• Be sure to include drinks.
• Don’t forget sauces like ketchup, salad dressing, sour cream, and gravy.
• Make sure to record any nutritional supplements used, like Carnation Instant Breakfast® or vitamins.
• Use measuring cups and spoons as often as possible.
• Look at how much is left on the plate. Record only what was actually eaten.
• Ask babysitters, teachers, or other caregivers to help keep records when necessary.
• If it is difficult to figure out what to record for a specific food, attach the food label to the logs that will be mailed or faxed to the dietitian.
• Try to be as specific as possible and write down the food item being eaten, the amount or portion eaten, and the carbohydrate grams. It is also helpful to include specific brand names.
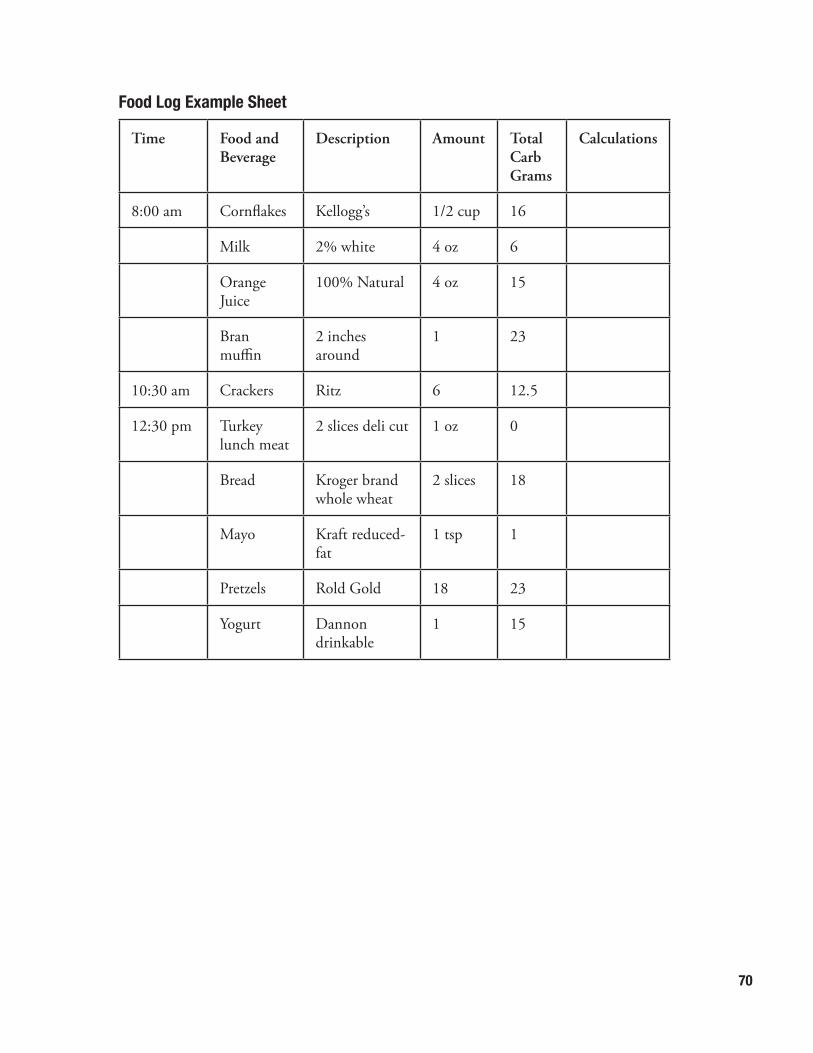
70
Food Log Example Sheet
Time Food and Beverage
Description Amount Total Carb Grams
Calculations
8:00 am Cornflakes Kellogg’s 1/2 cup 16
Milk 2% white 4 oz 6
Orange Juice
100% Natural 4 oz 15
Bran muffin
2 inches around
1 23
10:30 am Crackers Ritz 6 12.5
12:30 pm Turkey lunch meat
2 slices deli cut 1 oz 0
Bread Kroger brand whole wheat
2 slices 18
Mayo Kraft reduced-fat
1 tsp 1
Pretzels Rold Gold 18 23
Yogurt Dannon drinkable
1 15
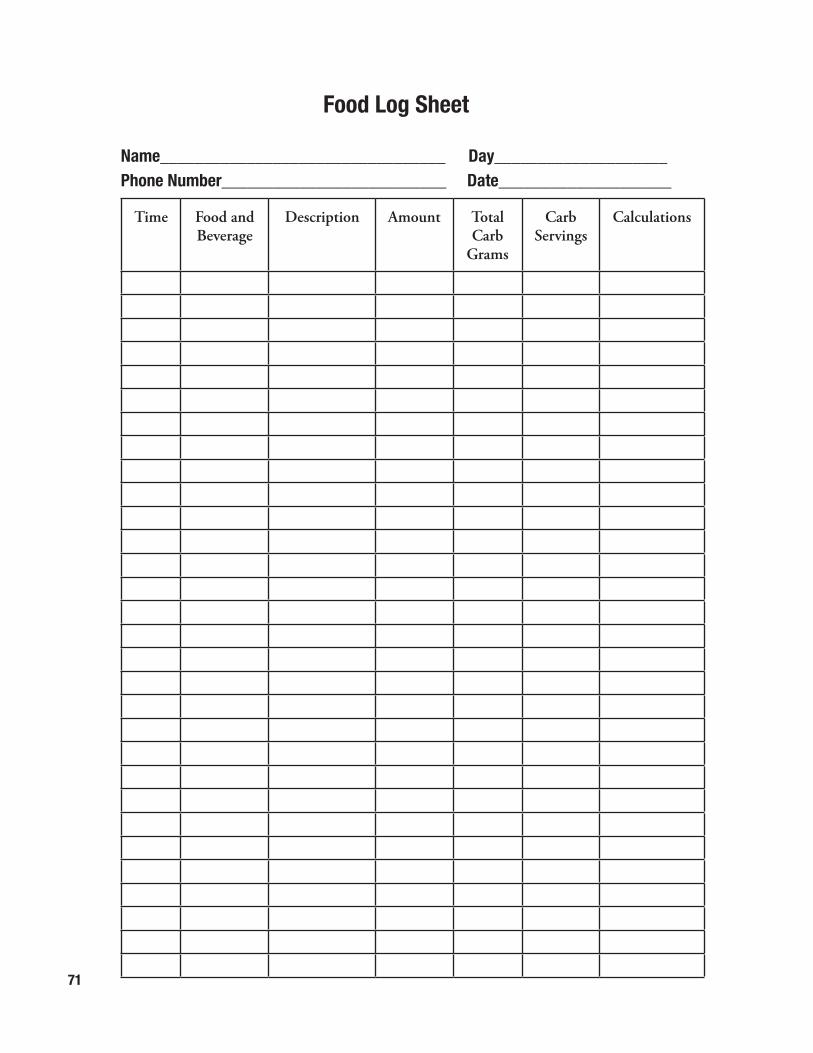
71
Food Log Sheet
Name_________________________________ Day____________________Phone Number__________________________ Date____________________
Time Food and Beverage
Description Amount Total Carb
Grams
CarbServings
Calculations
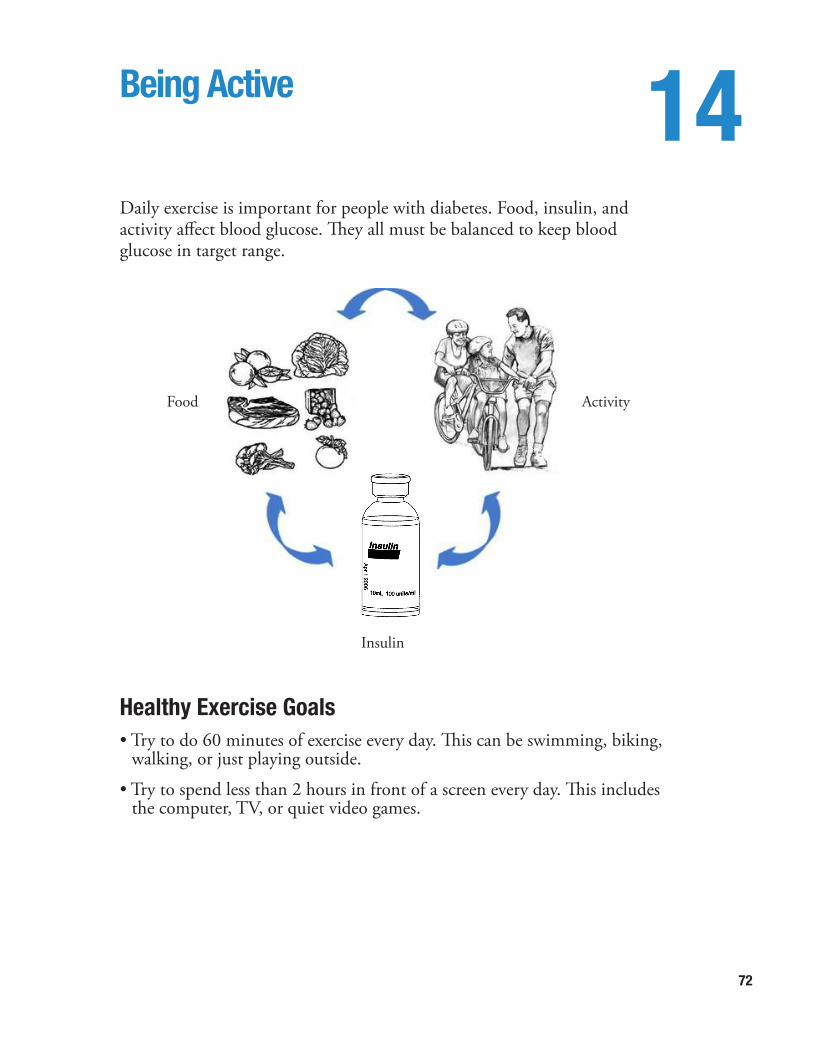
72
Being Active 14Daily exercise is important for people with diabetes. Food, insulin, and activity affect blood glucose. They all must be balanced to keep blood glucose in target range.
Healthy Exercise Goals• Try to do 60 minutes of exercise every day. This can be swimming, biking,
walking, or just playing outside.
• Try to spend less than 2 hours in front of a screen every day. This includes the computer, TV, or quiet video games.
Food Activity
Insulin
73
Exercise and Diabetes• Exercise makes your body more sensitive to insulin.
• Exercise may cause low blood glucose:
o During exercise
o After exercise
o Many hours after exercise
• Sometimes blood glucose may be higher in the first hour after exercise.
• Different types of exercise may cause different changes in blood glucose.
How Exercise Affects Blood Glucose• Check blood glucose at the following times:
o Before starting exercise
o Every 30 to 60 minutes during exercise
o After exercise
o During the night (between 2 a.m. and 3 a.m.) if exercise is late in the day
• Keep an exercise/activity log (see Exercise and Diabetes Blood Glucose Log on page 75)
Low Blood Glucose with Exercise:Take action to prevent low blood glucose if any of the following happen:
• Blood glucose is lower than 100 mg/dl before starting exercise.
• You have a history of low blood glucose with exercise.
• When starting a new type of exercise.
• When increasing your normal amount of exercise.
• When starting a new sports season.
Important!
It is best to prevent low blood glucose if you know when it will happen.
74
How to Prevent Low Blood Glucose During Exercise• Check blood glucose before, during, and after exercise.
• If blood glucose is less than 100, eat or drink a 15 gram carbohydrate and protein snack.
• Depending on the activity and blood glucose number, you may need to eat or drink a carbohydrate and protein snack every 30 to 60 minutes.
• Do not give insulin for exercise snacks.
• Know YOUR common signs of low blood glucose (see page 46).
• Do not give an insulin injection in the area you will be using during exercise
o Example: Do not use your leg for a dinner injection if you plan to run after dinner.
Keep Yourself Safe During Exercise
• Be prepared by keeping your testing supplies and glucagon emergency kit nearby.
• Keep a low blood glucose treatment with you, like juice or glucose tablets.
• Wear a diabetes medical ID like a bracelet or necklace.
• Exercise with a buddy. Tell others about your signs of low blood glucose.
• Do not exercise if you have ketones (small, moderate, or large).
• Drink a lot of fluids during exercise
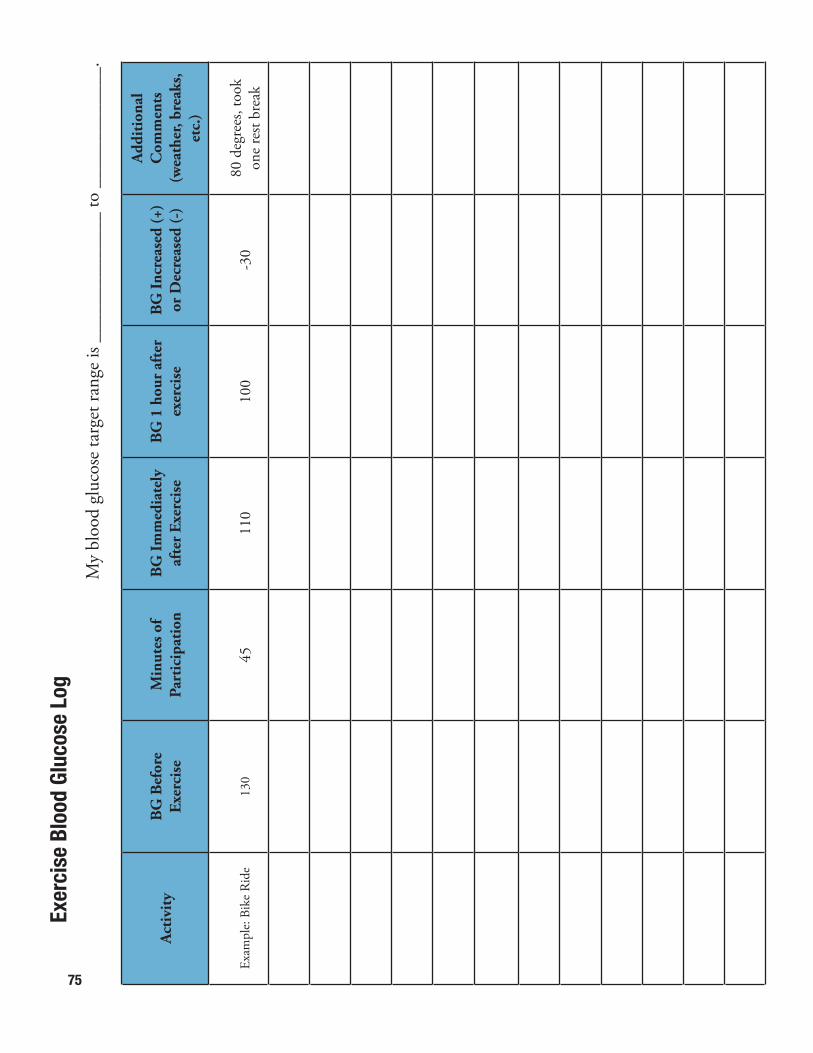
75
Act
ivit
yB
G B
efor
e Ex
erci
seM
inut
es o
f Pa
rtic
ipat
ion
BG
Imm
edia
tely
af
ter
Exer
cise
BG
1 h
our
afte
rex
erci
seB
G In
crea
sed
(+)
or D
ecre
ased
(-)
Add
itio
nal
Com
men
ts
(wea
ther
, bre
aks,
et
c.)
Exam
ple:
Bik
e R
ide
130
4511
010
0-3
080
deg
rees
, too
k on
e re
st br
eak
Exer
cise
Blo
od G
luco
se L
ogM
y bl
ood
gluc
ose
targ
et ra
nge
is __
____
____
____
to _
____
____
____
.
76
School 15Children need adult help to manage their diabetes during the school day. Children with chronic medical conditions, like diabetes, have a legal right to go to school and do school-related activities. The school, parent, child, and healthcare provider all help make a school health plan for diabetes so children can go to school and do school activities.
At home or at school, the treatment goals for children with diabetes include:
• Good blood glucose control
• Normal growth and development
• Good emotional health
• Learning to the best of their ability
Diabetes management during the school day should support these goals.
How to Work With School Staff
School staff will need information about diabetes and about the special needs of each child with diabetes. The role of the school nurse and teacher will be different at different ages. The school nurse should be the first contact to help prepare a diabetes management plan for your child.
It can be stressful for parent and child to return to school. We suggest the following to prepare for the return to school:
1. Meet with the school nurse or the person who will help with diabetes care at school. Do this before starting the school year to talk about your child’s needs. You may want to include any or all of the following school staff:
• Nurse’s aide/medicine monitor
• Teacher(s)
• Principal
• Food service manager
• Bus driver
• Guidance counselor
• Gym teacher/coach
77
2. During your meeting, you may want to talk about the following topics:
• Who will help my child test blood glucose?
• Who will help give my child insulin, if it is needed?
• Where will the diabetes supplies be kept?
• How will I know when more diabetes supplies are needed?
• What is the best way to reach the school nurse or staff member in charge of diabetes management?
• Who is able to give glucagon in case of an emergency?
• What time is gym or recess?
• What is the process to keep my child safe when there is a low blood glucose? Who can walk with my child if he or she need to leave class because of low blood glucose?
• How and when are blood glucoses communicated to the parent?
• Who tells the parent and makes special arrangements when there are parties or field trips?
3. Give the school a school healthcare plan for your child. We will give you a school health care plan packet during your first hospital stay and at your spring or summer clinic visit. This packet has general instructions for diabetes management.
4. Bring the packet with you to your meeting. We ask that you tell the school staff your child’s current insulin dose. Fill out the “MUST BE COMPLETED BY PARENT” section on the last page of the school packet. The last page of your packet is an insulin dose order form. You can also find this on the Diabetes Center website, www.nationwidechildrens.org/diabetes. A parent or guardian needs to fill out the form. If the school needs a signed order, then fax (or have the school fax) the form to the Diabetes Center. We will sign and return the form to the school or parent.
5. Bring the diabetes supplies your child will need at school. Use the checklist below:
o Blood Glucose Meter
o Blood Glucose Test Strips
o Lancet Device
o Lancets
o Ketone Test Strips
o Glucagon Emergency Kit
o Insulin
o Syringes or Insulin Pen Needles
o Food or Drink to treat or prevent low blood sugar
78
For many children, the school healthcare plan and open communication with the school nurse are all that is needed. Some parents like more detailed, written instructions. It is your right to make a 504 plan or an Individualized Education Plan (IEP) for your child. There is a sample 504 plan on the American Diabetes Association website at www.diabetes.org/advocacy/school.
504 Plan: Outlines a specific plan to make sure that chronic illness is managed safely during the school day.
IEP (individualized education plan): Outlines a specific plan for a child who has problems that affect ability to learn.
ResourcesThere may be times that you need to give school staff education about diabetes care or the rights of children with diabetes. Your school nurse is often a good resource to help educate other staff members.
You may also find the following resources helpful:
American Diabetes Association
Information about rights and responsibilities at school; sample 504 B Plan
Juvenile Diabetes Research Foundation (JDRF)
School Advisory Toolkit for Families; free resource
National Diabetes Education Program
Guide called Helping the Student with Diabetes Succeed: A Guide for School Personnel; free resource
79
Legal RightsThere are many federal laws that protect the rights of children with chronic illness, including diabetes. Public schools must make accommodations to make sure these children get a fair and equal education. Private schools and charter schools that do not get federal funding are not held to the same legal standards.
Individuals with Disabilities Education Act (IDEA)
Protects children who may have learning problems due to a disability. This is the law that supports the making of an IEP.
Section 504
Section 504 of the Rehabilitation Act of 1973 is a civil rights law that protects children with physical or mental disability and prohibits discrimination because of the disability. A Section 504 Plan may need to be made between the parents and the school so the child’s special needs related to their diabetes care in school are met.
Americans with Disabilities Act
This is a civil rights law. Like Section 504, it protects students with disabilities. This law applies to all students in public or private schools, except those run by religious organizations.
Ohio House Bill 264
State law which protects students with diabetes and the school employees who help those students. The law supports the following:
• Allows school staff without formal medical training to get education so they can care for children with diabetes. If staff volunteer, the school must let them be trained. No staff will be forced to give diabetes care if they are not comfortable doing so.
• Allows students who are able to manage their diabetes by themselves to carry diabetes supplies with them. The student’s parent or guardian must make this request. There must be a written doctor’s note for this request. The right may be taken away by the school if the student misuses the diabetes supplies.
• Students with diabetes must be allowed to go to the school they went to before diagnosis.
80
Clinic Visits 16Clinic AppointmentsThe American Diabetes Association (ADA) recommends that every 3 months anyone with diabetes should be seen by a healthcare provider who can help manage diabetes. There may be times more frequent clinic visits are suggested.
You will have a team of healthcare professionals to help manage diabetes at each clinic visit. Your team members include:
• Pediatric endocrinologist – a doctor who has specialized in the medical management of children with endocrine problems, including diabetes
• Mid-level practitioner – a nurse practitioner or physician assistant who gives medical care to children under the direction of a doctor
• Diabetes nurse educator – a nurse who specializes in helping families manage diabetes on a daily basis
• Dietitian – an expert in everything about diet and nutrition
• Social work – a person trained to help with barriers to healthcare and mental health issues
Diabetes clinic visits are often longer than other clinic visits. Plan on 2 hours for each visit. The visit will focus on issues specific to diabetes and the endocrine system. Your child should keep seeing a primary care doctor for regular healthcare needs. This includes well child visits and immunizations. It is also important to see a dentist every 6 months. People with diabetes are more likely to have some dental problems.
A legal guardian or an adult who has written permission from the legal guardian must come with any child under age 18 to clinic visits. If you have concerns about sensitive issues and would like to speak to a healthcare professional alone, let us know when you register for your visit.
If you need to cancel a clinic visit, let us know as soon as possible. Clinic times fill up quickly.
81
What to Expect• Review of growth and development. This includes height, weight, body
mass index (BMI), and stage of sexual development.
• Blood pressure
• Hemoglobin A1C. This will be taken from a drop of blood in clinic. You will have results by the end of the clinic visit.
• Review of current diabetes management. This includes blood glucose monitoring, medicine management, and nutrition.
• Review of blood glucose patterns. The doctor may make changes to insulin doses if needed.
• Problems or struggles you or your child may have with diabetes management.
• What to expect as your child grows.
How to Get the Most Out of Your Visit• Bring completed blood glucose records, logbook, and blood glucose meter.
This includes printing off the most recent downloaded meter readings.
• Review your records before your clinic visit to look for blood glucose patterns or problem areas.
• Write down any questions or concerns you or your child may have.
• Come ready to talk about your or your child’s health goals and the things that stand in the way of good health habits.
How to Help• Bring the pharmacy name, phone number, and address with you.
• Check to see that you have enough refills to last until your next visit.
• Bring the complete list of medicines your child takes.
82
Continuing Care for Living a Healthy LifeThere are some medical problems that are more common with diabetes or after you get diabetes. The ADA recommends the following screenings, so that problems can be treated early if they do happen.
At diagnosis:
• Celiac screen - Celiac disorder is an allergy to wheat. If the screen is positive, a referral to a gastrointestinal (GI) doctor will be recommended. Celiac disorder is managed by eating a gluten-free diet.
• Thyroid screen – If your child has thyroid disorder, it is managed with a daily pill.
• Insulin antibodies - Confirms type 1 diabetes diagnosis.
• Hemoglobin A1C – Gives the average blood glucose over the last 3 months.
Once each year:
• Thyroid screen
• Dilated eye exam - Can find vision problems related to diabetes. Start getting this exam when the child starts puberty or is 10 years old (whichever happens first) and has had type 1 diabetes for 3 years.
• Urine microalbumin – Finds any early kidney problems. Start getting this test when the child starts puberty or is 10 years old (whichever happens first) and has had type 1 diabetes for 5 years.
• Lipid profile (cholesterol)- Start when the child is older than 18 years of age.
NOTE: For type 2 diabetes, dilated eye exam, lipid profile, and urine microalbumin should be done every year, starting at diagnosis or once child is 10 years old.
Once every 5 years:
• Lipid profile (cholesterol) – Screening should start around puberty (around 10 years old). If there is a family history of early heart disease or high cholesterol, screening should start earlier. If the results are normal, the screen is repeated every 5 years. The doctor will decide what to do if results are abnormal.
83
After Clinic VisitsWe can help you best when your prescription refills and form requests are done at clinic visits. We understand that you may need our help between clinic visits. Most problems can be handled during office hours by calling 614-722-4425. Office hours are 8 a.m. to 4:30 p.m., Monday through Friday.
After regular office hours call the Nationwide Children’s Hospital Operator at 614-722-2000 and ask to speak with the Endocrinologist on call. There is always a doctor on call after hours to help with urgent problems.
You will get an After Visit Summary (AVS) before leaving your clinic visit. DO NOT leave your visit until you have received your AVS. Your AVS will include the following information to help in the care of your child:
Patient Instructions
You may see recommendations from the diabetes educator, the registered dietitian, the social worker, and/or the doctor here. The information will review what they talked about with you at your clinic visit.
Plan
The plan is written by the doctor, nurse practitioner, and/or physician assistant who saw you at that visit. The plan will include:
1. The A1C taken at this visit. If lab work is needed, you will be sent to the lab to get this done.
2. The type of insulin and the amount that you need to take.
3. Blood glucose testing recommendations.
4. Other medicines your child is taking, if any.
5. Office contact information for any other questions or concerns, before your next clinic visit.
6. Your next scheduled clinic visit date, time, and place.

84
Cancelling Your VisitRegular office visits are very important in good management of your child’s diabetes. There may not be many available visits to reschedule your child in a timely manner.
We know that emergencies may happen and keep you from coming to your child’s scheduled appointment. Please give us at least 24 hour notice if you cannot make your appointment. Call Nationwide Children’s Hospital Central Scheduling at 614-722-6200 to reschedule your appointment.
85
Complications 17When you have diabetes it is possible to get acute problems or chronic problems (complications). The best way to lower the risk of complications is to use what you have learned about diabetes to keep your blood glucose in your target range as much as you can.
Acute ComplicationsAcute complications are problems that happen in a short period of time. They can also be fixed in a short period of time. The two major acute complications of diabetes that need urgent action are:
• Diabetic ketoacidosis (DKA)
• Severe hypoglycemia
Chronic Complications
Chronic complications are health changes that happen when blood glucoses have been high for many years. These can happen 3 to 5 years after high blood glucoses start. In the beginning, it is possible for some problems to be reversed. In some cases, these become permanent health problems.
Some examples of chronic complications include:
• Poor growth
• Diabetic retinopathy (an eye problem that can lead to blindness)
• Nephropathy (kidney problems that can lead to kidney failure)
• Neuropathy (damage to nerves)
• Heart and blood vessel problems
There is good news. Treatment options for diabetes, today, are much better than they were in the past. It is possible to manage your diabetes in a way that lowers the chance of developing chronic complications.
A large research study completed in 1993, called the Diabetes Control and Complications Trial (DCCT), stated that lower Hgb A1C numbers led to far fewer chronic complications.
If chronic complications are found early, they can sometimes be reversed.
86
To find problems early:
• Have a dilated eye exam or retinal scan every year. Start when you start puberty or when you are 10 years old (whichever happens first) and have had diabetes for 3 years.
• Have a urine test called urine microalbumin. This checks for early kidney problems.
• Check your feet often for changes or sores that are not healing well.
87
Special Situations 18Travel• Be prepared.
• Have extra diabetes supplies with you.
• Store medicine where it will not be in a very hot or very cold temperature.
o Do not store medicine inside the car or in the trunk of the car.
o Do not put medicine in baggage that will be checked.
• Keep diabetes supplies in their original container with the pharmacy label intact.
• Carry a travel letter that states you have diabetes and need to carry diabetes supplies with you. We can provide you with a travel letter.
• Have phone numbers for the endocrinology office with you.
• Wear medical ID.
DrivingIn Ohio, people with diabetes must have a form signed by their diabetes doctor that says that diabetes will not stop them from being a safe driver. The form will be given to you by the Bureau of Motor Vehicles (BMV). A low blood glucose while you are driving can be dangerous to you and to others. Your doctor will want to know you are managing your diabetes well to limit your risk of having an accident due to a low blood glucose. You will need to agree to follow safe driving practices before your diabetes doctor will sign the form.
88
Safe driving practices include:
• Check blood glucose before driving.
• If you have signs of low blood glucose while driving, pull off the road, and stop the car. Treat the low blood glucose before driving again.
• Carry food or drink with you in your car to treat low blood glucose.
• Wear a medical ID
Safe diabetes management includes:
• Check blood glucose 4 times a day.
• Keep written records.
Pregnancy and DiabetesIt is possible to have a healthy pregnancy and baby when the mother has diabetes. However, pregnancy in women with diabetes is considered high risk. A high risk obstetrician (pregnancy doctor) should be used, as there are risks to both mother and baby:
Risks to mother:
• Large baby
• Increased chance of C-section.
• Chance of worsening retinopathy, if retinopathy is already present.
• Chance of worsening kidney damage, if kidney damage is already present.
Risks to baby:
• Birth defects if blood glucose is high during pregnancy.
o Baby is especially at risk during the first 3 months of pregnancy.
• Low blood glucose problems just after birth.
89
How to Prevent Problems with Pregnancy
• Planned pregnancy is best.
• Schedule an appointment with a high risk obstetrician before becoming pregnant.
• Keep blood glucoses as close to normal as possible.
• If you find out you are pregnant, call the endocrinology office. They can refer you to a high risk obstetrician.
Cigarette or Smokeless Tobacco UseSmoking or using chewing tobacco can cause some of the same problems that diabetes can cause. If you do not smoke, do not start to smoke. If you do smoke, let us know so that we can help you quit.
AlcoholAlcohol can make it hard for your body to release stored glucose. This can lead to low blood glucose. Drinking alcohol can make it harder for you to feel signs of low blood glucose, which may lead to severe low blood glucose.
90
Resources 19Community Agencies Central Ohio Diabetes Association (CODA) is a local organization that gives some educational resources for families with diabetes. They also organize summer camps for children with diabetes.
The Juvenile Diabetes Research Foundation (JDRF) is an organization that raises funds for research to find a cure for juvenile diabetes. They also have a newsletter and magazine which share up-to-date diabetes research information.
The American Diabetes Association (ADA) has many written resources for families. They also raise money for research and support of local programs for families with diabetes.
Helpful Phone Numbers, Publications and Websites
Phone Numbers
American Diabetes Association (local office) 614-436-1917
American Diabetes Association (national office) 800-342-2383
Bureau for Children with Medical Handicaps (BCMH) 614-466-1700
Central Ohio Diabetes Association 614-884-4400
Juvenile Diabetes Research Foundation (local-JDRF) 614-464-2873
National Juvenile Diabetes Research Foundation (JDRF) 800-223-1138
Nationwide Children’s Hospital Endocrinology 614-722-4425
Nationwide Children’s Clinical Services and 614-722-6300 Care Coordination (social worker contact; 614-722-4425ask for Endo Social worker)
Nationwide Children’s Behavioral Health Intake 614-355-8080
Nationwide Children’s Hospital Psychology Department 614-722-4700
91
Netcare (Mental Health Emergency) 614-273-2273
Ohio Coalition for the Education of 800-374-2806Children with Disabilities
Ohio Healthy Start 800-324-8680 (Medicaid Consumer Hotline)
Publications
There are many publications and web sites that deal with issues related to diabetes. Some resources will be more helpful than others, depending on your needs. Here is a partial list of those resources:
Diabetes Forecast (Published by the ADA)
Diabetes Countdown (Published by JDRF)
Diabetes Care (ADA)
Diabetes in the News (ADA Online News Feed)
Diabetes Self-Management Magazine
Websites
American Diabetes Association (ADA), www.diabetes.org
Juvenile Diabetes Research Foundation (JDRF), www.jdrf.com
Children with Diabetes, www.childrenwithdiabetes.com
Central Ohio Diabetes Association (CODA), www.diabetes.ohio.org
Bureau for Children with Medical Handicaps, www.odh.ohio.gov
Children’s Diabetes Foundation, www.childrensdiabetesfoundation.org
National Diabetes Education Program, www.ndep.nih.gov
Nationwide Children’s Hospital Section of Endocrinology,www.nationwidechildrens.org/diabetes
92
Common Terms 20Acanthosis nigricans – darkened area on the neck or in the armpit; this means there may be insulin resistance
Acidosis – unhealthy elevated level of acid in blood; in diabetes, it happens when ketones are in blood
Acute complication – a problem that occurs in a short period of time; is fixed in a short period of time
Cholesterol – a type of fat that the body needs in small amounts, but elevated levels can help cause heart disease
Chronic complication – health change that happens after many years; in some cases can be reversed; but often is a permanent health change
Complex carbohydrate – Food with a slow release form of carbohydrate
Dawn phenomenon – rise in blood glucose from evening to morning caused by hormone production during the night; results in insulin resistance
DKA – Diabetes Ketoacidosis; life-threatening acute complication of diabetes; caused when the body is not able to use glucose for energy
Fasting – state of the body when it has been at least 6 hours since last eating or drinking; certain lab work needs to be done when a person is fasting
Glucagon – hormone that is released by the pancreas when blood glucose is too low; can also be given by injection; lets stored glucose be released from the liver into the blood
Glucose – sugar that is present in the blood after eating; the body uses glucose for energy
Glycogen – stored form of glucose; extra glucose is stored in the liver as glycogen.
Hemoglobin A1C (Hgb A1C) – lab test that measures the amount of glucose attached to hemoglobin in the body; gives an idea of the average glucose levels over the last 3 months
Heredity – Traits (ex. color of eyes); likeliness to get certain health conditions that are passed from parent to child
93
Honeymoon phase – Period of time soon after the diagnosis of diabetes when the body temporarily makes a small amount of insulin
Hormone – chemical that is made in a part of the body that affects other areas of the body; insulin and glucagon are hormones
Hyperglycemia – High blood glucose
Hyperlipidemia – High levels of fat (lipids) in the blood
Hypoglycemia – Low blood glucose
Insulin – a hormone made by the beta cells in the pancreas; lets the body use glucose for energy
Insulin resistance – a condition in which the body cannot use insulin as well as it normally does; found in people with type 2 diabetes; may be found in people with unhealthy weight
Intramuscular injection – injection given into the muscle
Ketoacidosis – see DKA
Ketones – produced when the body breaks down fat; can lead to ketoacidosis
Ketonuria – ketones in the urine
Kussmaul respirations – rapid, shallow breathing; present in ketoacidosis; the body’s attempt to restore acid base balance in the blood
Lancet – a fine, sharp needle device; used to puncture the skin to get a drop of blood
Lipid – another word for fat; two types of lipids are triglycerides and cholesterol
Pancreas – a gland behind the liver; one of its functions is to make insulin
Proteinuria – protein in the urine; may be an early sign of kidney disease
Renal – relates to the kidneys
Simple Carbohydrate – food that is made of rapid-release form of carbohydrates
Subcutaneous injection – injection into the fatty tissue between the muscle and the skin
Triglyceride – a kind of fat that is carried in the blood and stored in the body
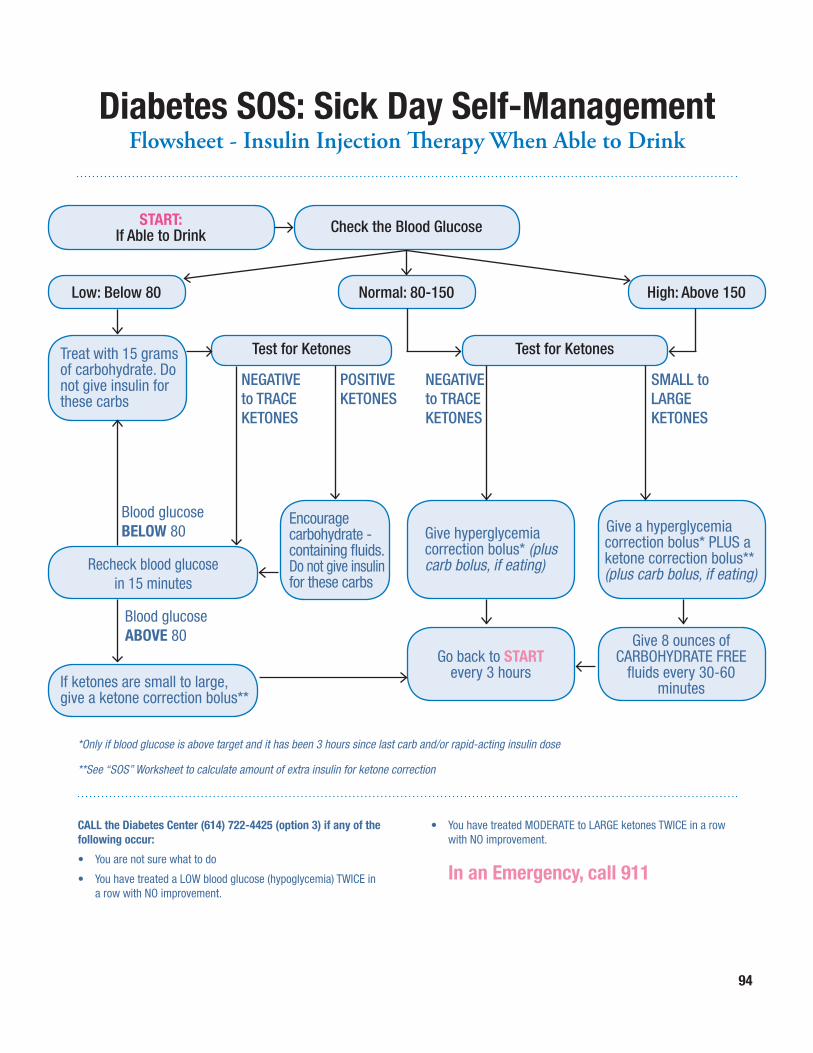
94
CALL the Diabetes Center (614) 722-4425 (option 3) if any of the following occur:
• You are not sure what to do
• You have treated a LOW blood glucose (hypoglycemia) TWICE in a row with NO improvement.
• You have treated MODERATE to LARGE ketones TWICE in a row with NO improvement.
In an Emergency, call 911
Check the Blood Glucose
Low: Below 80 Normal: 80-150 High: Above 150
Give a hyperglycemia correction bolus* PLUS a ketone correction bolus** (plus carb bolus, if eating)
Give 8 ounces of CARBOHYDRATE FREE
fluids every 30-60 minutes
Go back to START every 3 hours
Test for KetonesTest for Ketones
NEGATIVE to TRACE KETONES
POSITIVEKETONES
Blood glucose BELOW 80
Blood glucose ABOVE 80
NEGATIVEto TRACEKETONES
SMALL to LARGE KETONES
*Only if blood glucose is above target and it has been 3 hours since last carb and/or rapid-acting insulin dose
**See “SOS” Worksheet to calculate amount of extra insulin for ketone correction
Diabetes SOS: Sick Day Self-Management Flowsheet - Insulin Injection Therapy When Able to Drink
Treat with 15 grams of carbohydrate. Do not give insulin for these carbs
START:If Able to Drink
Encourage carbohydrate - containing fluids. Do not give insulin for these carbs
Recheck blood glucose in 15 minutes
If ketones are small to large, give a ketone correction bolus**
Give hyperglycemia correction bolus* (plus carb bolus, if eating)
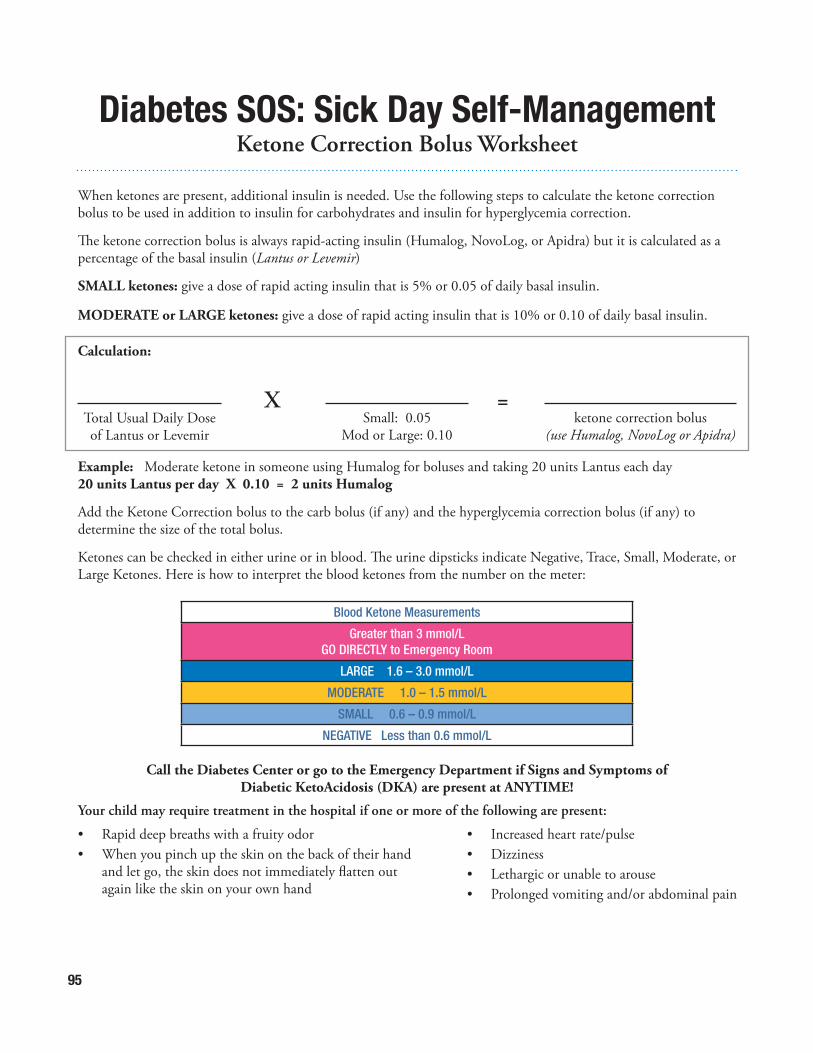
95
When ketones are present, additional insulin is needed. Use the following steps to calculate the ketone correction bolus to be used in addition to insulin for carbohydrates and insulin for hyperglycemia correction.
The ketone correction bolus is always rapid-acting insulin (Humalog, NovoLog, or Apidra) but it is calculated as a percentage of the basal insulin (Lantus or Levemir)
SMALL ketones: give a dose of rapid acting insulin that is 5% or 0.05 of daily basal insulin.
MODERATE or LARGE ketones: give a dose of rapid acting insulin that is 10% or 0.10 of daily basal insulin.
Calculation:
Example: Moderate ketone in someone using Humalog for boluses and taking 20 units Lantus each day20 units Lantus per day X 0.10 = 2 units Humalog
Add the Ketone Correction bolus to the carb bolus (if any) and the hyperglycemia correction bolus (if any) to determine the size of the total bolus.
Ketones can be checked in either urine or in blood. The urine dipsticks indicate Negative, Trace, Small, Moderate, or Large Ketones. Here is how to interpret the blood ketones from the number on the meter:
Total Usual Daily Dose of Lantus or Levemir
Small: 0.05 Mod or Large: 0.10
ketone correction bolus (use Humalog, NovoLog or Apidra)
X =
Call the Diabetes Center or go to the Emergency Department if Signs and Symptoms of Diabetic KetoAcidosis (DKA) are present at ANYTIME!
Your child may require treatment in the hospital if one or more of the following are present:
• Rapid deep breaths with a fruity odor• When you pinch up the skin on the back of their hand and let go, the skin does not immediately flatten out again like the skin on your own hand
• Increased heart rate/pulse• Dizziness• Lethargic or unable to arouse• Prolonged vomiting and/or abdominal pain
Blood Ketone Measurements
Greater than 3 mmol/LGO DIRECTLY to Emergency Room
LARGE 1.6 – 3.0 mmol/L
MODERATE 1.0 – 1.5 mmol/L
SMALL 0.6 – 0.9 mmol/L
NEGATIVE Less than 0.6 mmol/L
Diabetes SOS: Sick Day Self-Management Ketone Correction Bolus Worksheet
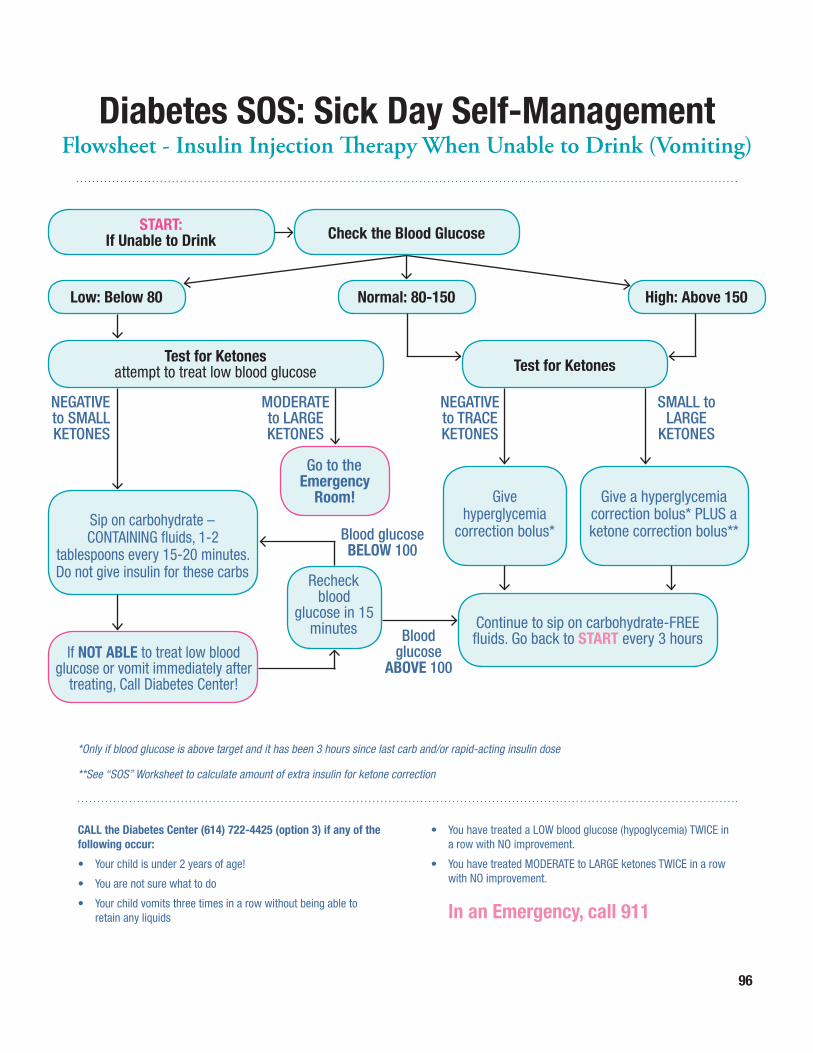
96
CALL the Diabetes Center (614) 722-4425 (option 3) if any of the following occur:
• Your child is under 2 years of age!
• You are not sure what to do
• Your child vomits three times in a row without being able to retain any liquids
• You have treated a LOW blood glucose (hypoglycemia) TWICE in a row with NO improvement.
• You have treated MODERATE to LARGE ketones TWICE in a row with NO improvement.
In an Emergency, call 911
*Only if blood glucose is above target and it has been 3 hours since last carb and/or rapid-acting insulin dose
**See “SOS” Worksheet to calculate amount of extra insulin for ketone correction
Diabetes SOS: Sick Day Self-Management Flowsheet - Insulin Injection Therapy When Unable to Drink (Vomiting)
START:If Unable to Drink Check the Blood Glucose
Low: Below 80 Normal: 80-150 High: Above 150
Sip on carbohydrate – CONTAINING fluids, 1-2
tablespoons every 15-20 minutes. Do not give insulin for these carbs
Go to the Emergency
Room!
Recheck blood
glucose in 15 minutes
Give a hyperglycemia correction bolus* PLUS a ketone correction bolus**
Give hyperglycemia
correction bolus*
Continue to sip on carbohydrate-FREE fluids. Go back to START every 3 hours
Test for KetonesTest for Ketonesattempt to treat low blood glucose
NEGATIVE to SMALL KETONES
Blood glucose BELOW 100
Blood glucose
ABOVE 100
MODERATE to LARGEKETONES
NEGATIVEto TRACEKETONES
SMALL to LARGE
KETONES
If NOT ABLE to treat low blood glucose or vomit immediately after
treating, Call Diabetes Center!
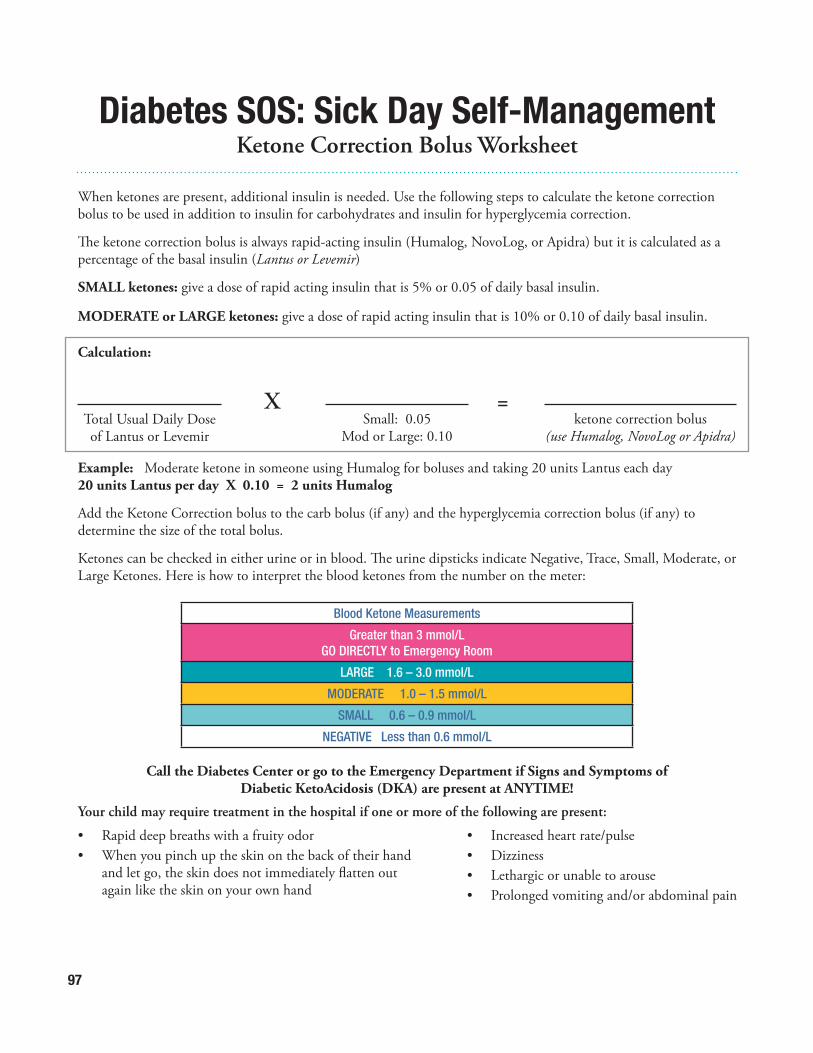
97
When ketones are present, additional insulin is needed. Use the following steps to calculate the ketone correction bolus to be used in addition to insulin for carbohydrates and insulin for hyperglycemia correction.
The ketone correction bolus is always rapid-acting insulin (Humalog, NovoLog, or Apidra) but it is calculated as a percentage of the basal insulin (Lantus or Levemir)
SMALL ketones: give a dose of rapid acting insulin that is 5% or 0.05 of daily basal insulin.
MODERATE or LARGE ketones: give a dose of rapid acting insulin that is 10% or 0.10 of daily basal insulin.
Calculation:
Example: Moderate ketone in someone using Humalog for boluses and taking 20 units Lantus each day20 units Lantus per day X 0.10 = 2 units Humalog
Add the Ketone Correction bolus to the carb bolus (if any) and the hyperglycemia correction bolus (if any) to determine the size of the total bolus.
Ketones can be checked in either urine or in blood. The urine dipsticks indicate Negative, Trace, Small, Moderate, or Large Ketones. Here is how to interpret the blood ketones from the number on the meter:
Total Usual Daily Dose of Lantus or Levemir
Small: 0.05 Mod or Large: 0.10
ketone correction bolus (use Humalog, NovoLog or Apidra)
X =
Call the Diabetes Center or go to the Emergency Department if Signs and Symptoms of Diabetic KetoAcidosis (DKA) are present at ANYTIME!
Your child may require treatment in the hospital if one or more of the following are present:
• Rapid deep breaths with a fruity odor• When you pinch up the skin on the back of their hand and let go, the skin does not immediately flatten out again like the skin on your own hand
• Increased heart rate/pulse• Dizziness• Lethargic or unable to arouse• Prolonged vomiting and/or abdominal pain
Blood Ketone Measurements
Greater than 3 mmol/LGO DIRECTLY to Emergency Room
LARGE 1.6 – 3.0 mmol/L
MODERATE 1.0 – 1.5 mmol/L
SMALL 0.6 – 0.9 mmol/L
NEGATIVE Less than 0.6 mmol/L
Diabetes SOS: Sick Day Self-Management Ketone Correction Bolus Worksheet
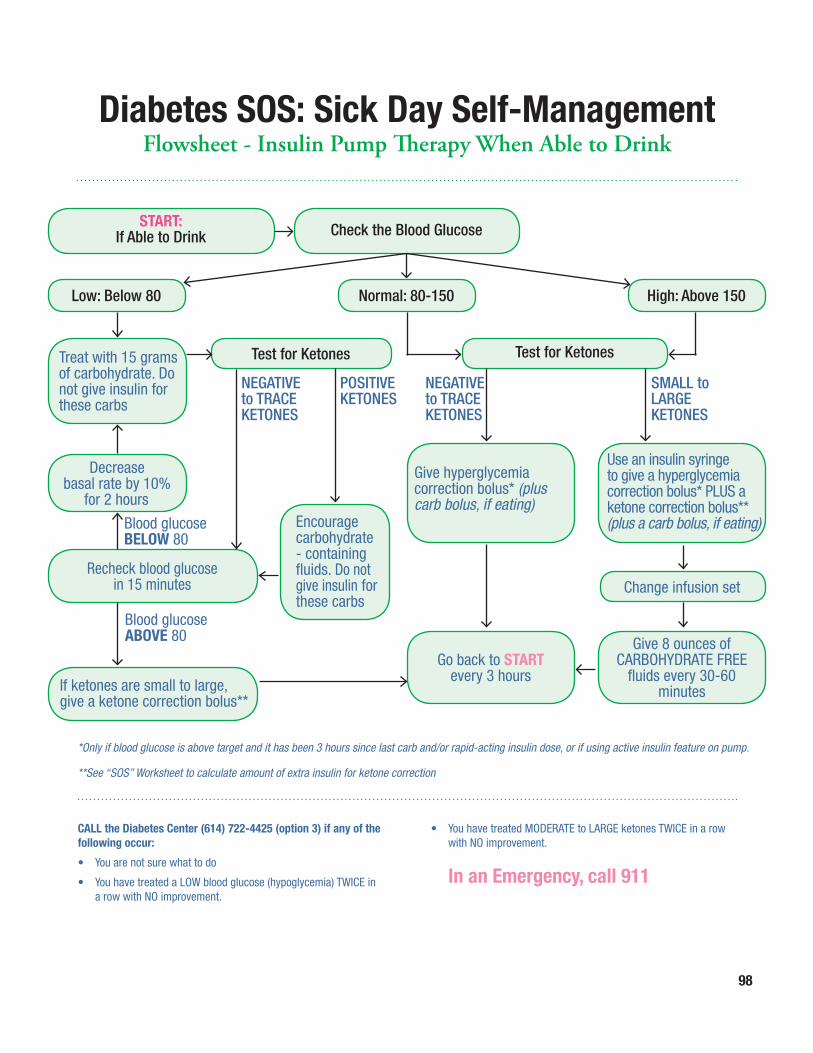
98
CALL the Diabetes Center (614) 722-4425 (option 3) if any of the following occur:
• You are not sure what to do
• You have treated a LOW blood glucose (hypoglycemia) TWICE in a row with NO improvement.
• You have treated MODERATE to LARGE ketones TWICE in a row with NO improvement.
In an Emergency, call 911
START:If Able to Drink Check the Blood Glucose
Low: Below 80 Normal: 80-150 High: Above 150
Decrease basal rate by 10%
for 2 hours
Recheck blood glucose in 15 minutes
Give hyperglycemia correction bolus* (plus carb bolus, if eating)
Go back to START every 3 hours
Test for Ketones
Change infusion set
Test for Ketones
NEGATIVE to TRACE KETONES
POSITIVEKETONES
Blood glucose BELOW 80
Blood glucose ABOVE 80
NEGATIVEto TRACEKETONES
SMALL to LARGE KETONES
*Only if blood glucose is above target and it has been 3 hours since last carb and/or rapid-acting insulin dose, or if using active insulin feature on pump.
**See “SOS” Worksheet to calculate amount of extra insulin for ketone correction
Diabetes SOS: Sick Day Self-Management Flowsheet - Insulin Pump Therapy When Able to Drink
Treat with 15 grams of carbohydrate. Do not give insulin for these carbs
If ketones are small to large, give a ketone correction bolus**
Use an insulin syringe to give a hyperglycemia correction bolus* PLUS a ketone correction bolus** (plus a carb bolus, if eating)
Give 8 ounces of CARBOHYDRATE FREE
fluids every 30-60 minutes
Encourage carbohydrate - containing fluids. Do not give insulin for these carbs
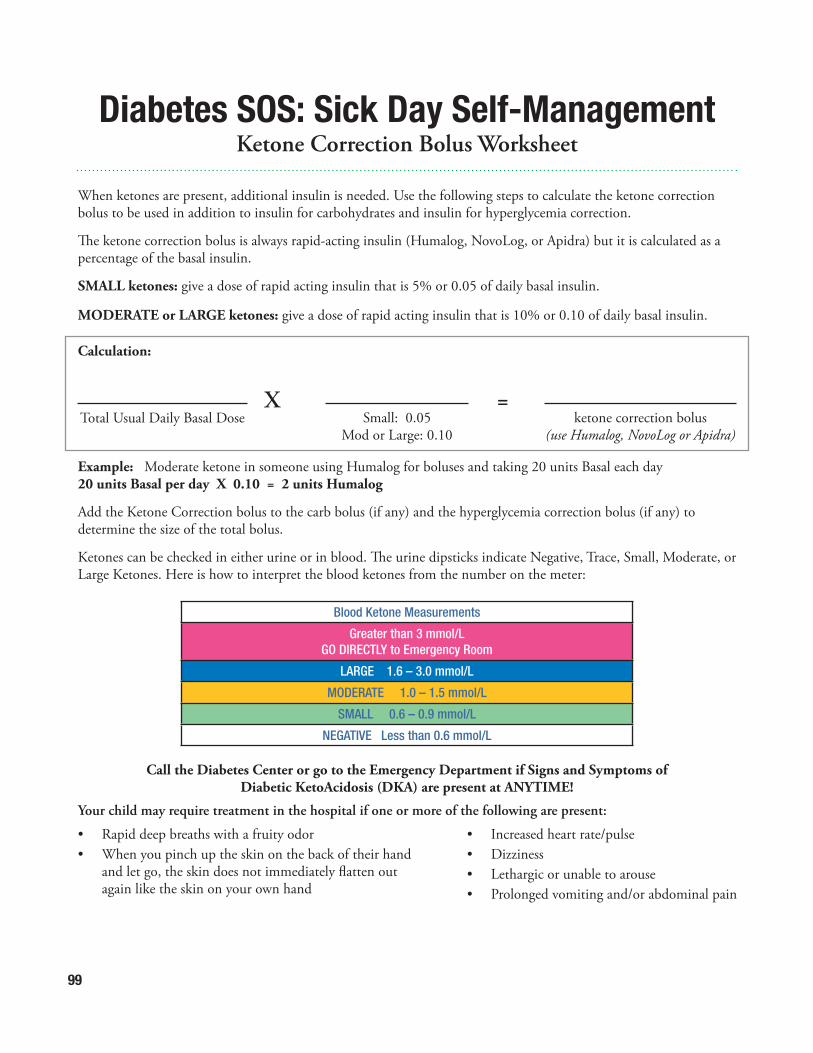
99
When ketones are present, additional insulin is needed. Use the following steps to calculate the ketone correction bolus to be used in addition to insulin for carbohydrates and insulin for hyperglycemia correction.
The ketone correction bolus is always rapid-acting insulin (Humalog, NovoLog, or Apidra) but it is calculated as a percentage of the basal insulin.
SMALL ketones: give a dose of rapid acting insulin that is 5% or 0.05 of daily basal insulin.
MODERATE or LARGE ketones: give a dose of rapid acting insulin that is 10% or 0.10 of daily basal insulin.
Calculation:
Example: Moderate ketone in someone using Humalog for boluses and taking 20 units Basal each day20 units Basal per day X 0.10 = 2 units Humalog
Add the Ketone Correction bolus to the carb bolus (if any) and the hyperglycemia correction bolus (if any) to determine the size of the total bolus.
Ketones can be checked in either urine or in blood. The urine dipsticks indicate Negative, Trace, Small, Moderate, or Large Ketones. Here is how to interpret the blood ketones from the number on the meter:
Total Usual Daily Basal Dose Small: 0.05 Mod or Large: 0.10
ketone correction bolus (use Humalog, NovoLog or Apidra)
X =
Call the Diabetes Center or go to the Emergency Department if Signs and Symptoms of Diabetic KetoAcidosis (DKA) are present at ANYTIME!
Your child may require treatment in the hospital if one or more of the following are present:
• Rapid deep breaths with a fruity odor• When you pinch up the skin on the back of their hand and let go, the skin does not immediately flatten out again like the skin on your own hand
• Increased heart rate/pulse• Dizziness• Lethargic or unable to arouse• Prolonged vomiting and/or abdominal pain
Blood Ketone Measurements
Greater than 3 mmol/LGO DIRECTLY to Emergency Room
LARGE 1.6 – 3.0 mmol/L
MODERATE 1.0 – 1.5 mmol/L
SMALL 0.6 – 0.9 mmol/L
NEGATIVE Less than 0.6 mmol/L
Diabetes SOS: Sick Day Self-Management Ketone Correction Bolus Worksheet
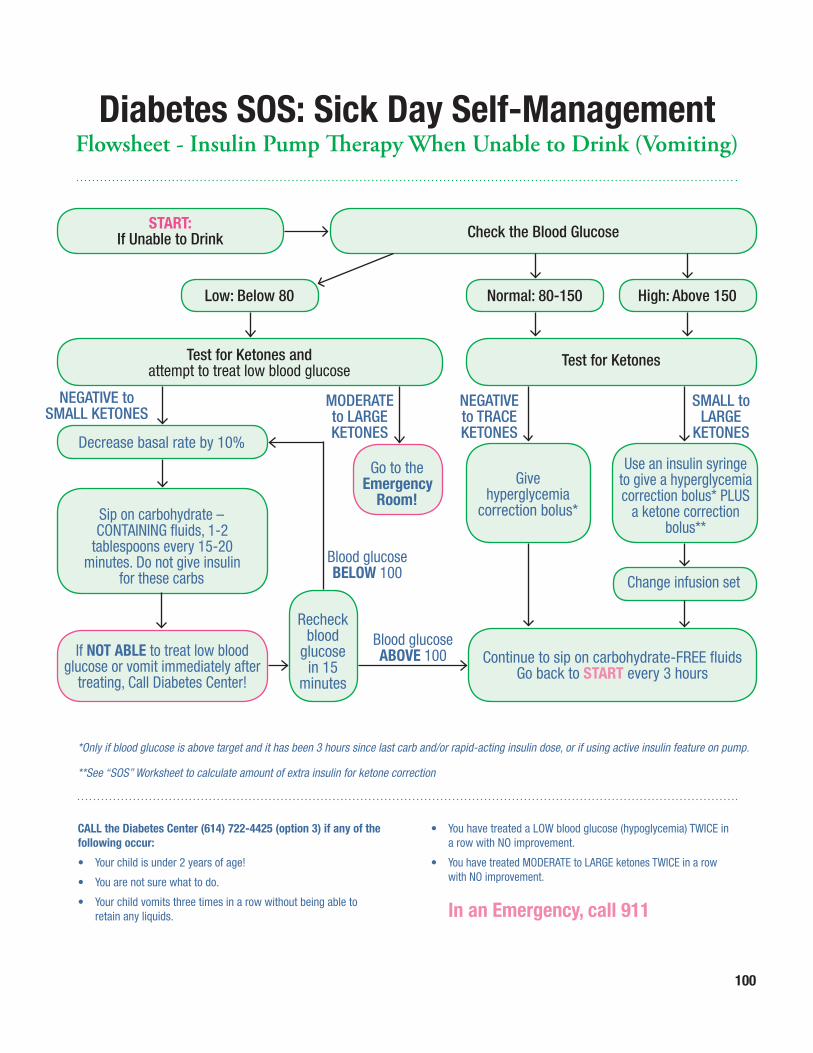
100
CALL the Diabetes Center (614) 722-4425 (option 3) if any of the following occur:
• Your child is under 2 years of age!
• You are not sure what to do.
• Your child vomits three times in a row without being able to retain any liquids.
• You have treated a LOW blood glucose (hypoglycemia) TWICE in a row with NO improvement.
• You have treated MODERATE to LARGE ketones TWICE in a row with NO improvement.
In an Emergency, call 911
*Only if blood glucose is above target and it has been 3 hours since last carb and/or rapid-acting insulin dose, or if using active insulin feature on pump.
**See “SOS” Worksheet to calculate amount of extra insulin for ketone correction
Diabetes SOS: Sick Day Self-Management Flowsheet - Insulin Pump Therapy When Unable to Drink (Vomiting)
START:If Unable to Drink Check the Blood Glucose
Low: Below 80
Decrease basal rate by 10%
Sip on carbohydrate – CONTAINING fluids, 1-2
tablespoons every 15-20 minutes. Do not give insulin
for these carbs
Go to the Emergency
Room!
Recheck blood
glucose in 15
minutes
Give hyperglycemia
correction bolus*
Continue to sip on carbohydrate-FREE fluidsGo back to START every 3 hours
Test for Ketones and attempt to treat low blood glucose
Normal: 80-150 High: Above 150
Change infusion set
Test for Ketones
NEGATIVE to SMALL KETONES
Blood glucose BELOW 100
Blood glucose ABOVE 100
MODERATE to LARGEKETONES
NEGATIVEto TRACEKETONES
SMALL to LARGE
KETONES
Use an insulin syringe to give a hyperglycemia correction bolus* PLUS
a ketone correction bolus**
If NOT ABLE to treat low blood glucose or vomit immediately after
treating, Call Diabetes Center!
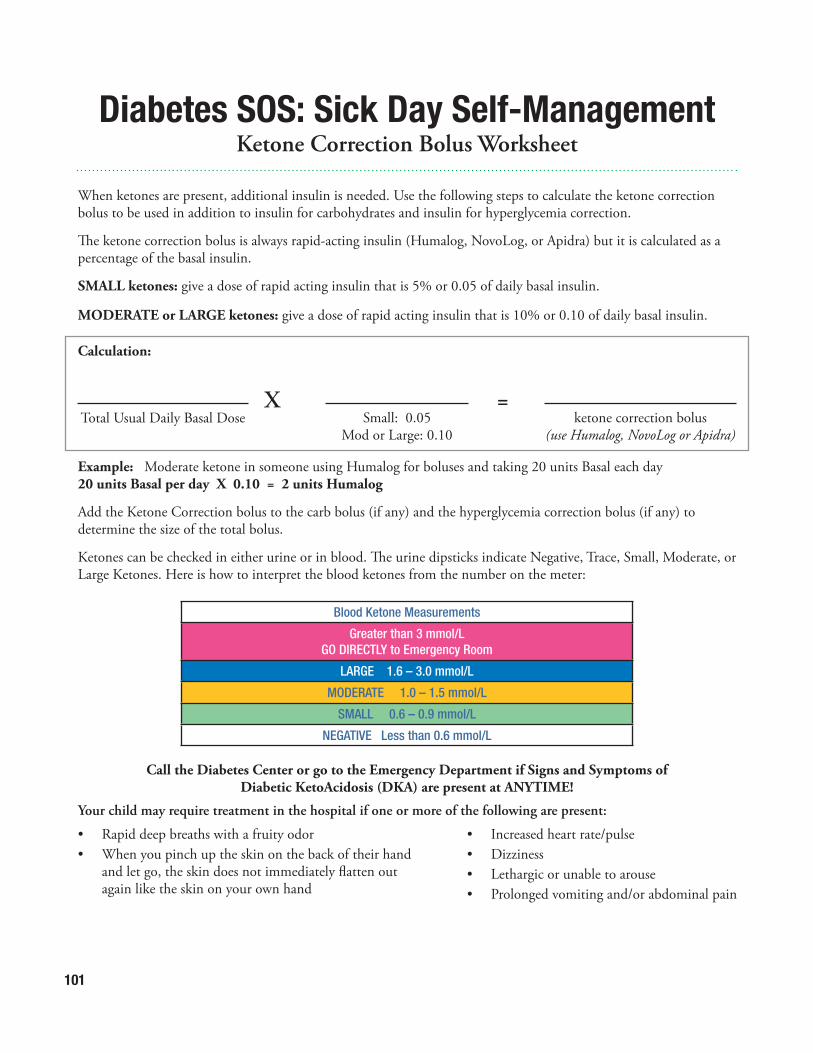
101
When ketones are present, additional insulin is needed. Use the following steps to calculate the ketone correction bolus to be used in addition to insulin for carbohydrates and insulin for hyperglycemia correction.
The ketone correction bolus is always rapid-acting insulin (Humalog, NovoLog, or Apidra) but it is calculated as a percentage of the basal insulin.
SMALL ketones: give a dose of rapid acting insulin that is 5% or 0.05 of daily basal insulin.
MODERATE or LARGE ketones: give a dose of rapid acting insulin that is 10% or 0.10 of daily basal insulin.
Calculation:
Example: Moderate ketone in someone using Humalog for boluses and taking 20 units Basal each day20 units Basal per day X 0.10 = 2 units Humalog
Add the Ketone Correction bolus to the carb bolus (if any) and the hyperglycemia correction bolus (if any) to determine the size of the total bolus.
Ketones can be checked in either urine or in blood. The urine dipsticks indicate Negative, Trace, Small, Moderate, or Large Ketones. Here is how to interpret the blood ketones from the number on the meter:
Total Usual Daily Basal Dose Small: 0.05 Mod or Large: 0.10
ketone correction bolus (use Humalog, NovoLog or Apidra)
X =
Call the Diabetes Center or go to the Emergency Department if Signs and Symptoms of Diabetic KetoAcidosis (DKA) are present at ANYTIME!
Your child may require treatment in the hospital if one or more of the following are present:
• Rapid deep breaths with a fruity odor• When you pinch up the skin on the back of their hand and let go, the skin does not immediately flatten out again like the skin on your own hand
• Increased heart rate/pulse• Dizziness• Lethargic or unable to arouse• Prolonged vomiting and/or abdominal pain
Blood Ketone Measurements
Greater than 3 mmol/LGO DIRECTLY to Emergency Room
LARGE 1.6 – 3.0 mmol/L
MODERATE 1.0 – 1.5 mmol/L
SMALL 0.6 – 0.9 mmol/L
NEGATIVE Less than 0.6 mmol/L
Diabetes SOS: Sick Day Self-Management Ketone Correction Bolus Worksheet