Embed Size (px)
Citation preview
CASE REPORT
Class III subdivision malocclusion correctedwith asymmetric intermaxillary elastics
Guilherme Janson,a Marcos Roberto de Freitas,b Janine Araki,c Eduardo Jacomino Franco,d
and Sergio Estelita Cavalcante Barrosc
Bauru, Brazil
Correcting a Class III subdivision malocclusion is usually a challenge for an orthodontist, especially if the pa-tient’s profile does not allow for any extractions. One treatment option is to use asymmetric intermaxillary elas-tics to correct the unilateral anteroposterior discrepancy. However, the success of this method depends on theindividual response of each patient and his or her compliance in using the elastics. The objectives of this articlewere to present a successful treatment of a Class III subdivision patient with this approach and to illustrate anddiscuss the dentoskeletal changes that contributed to the correction. (Am J Orthod Dentofacial Orthop2010;138:221-30)
Orthodontic treatment of adult Class III patientsis difficult, especially if the malocclusion isasymmetric.1 A precise diagnosis of the
dentoskeletal components of the malocclusion associ-ated with the patient’s primary concern is essentialfor correct treatment planning.2-9 Similar tocorrection of Class II subdivision malocclusions,Class III subdivision malocclusions can havea variety of orthodontic treatment options such asnonextraction protocols with intermaxillary elastics,unilateral extraction of 1 mandibular premolar on theClass III side, or extraction of 2 mandibularpremolar extractions and 1 maxillary premolarextraction on the Class I side.1,10-13 Malocclusioncorrection based on the use of intermaxillary elasticsis difficult and controversial.11,14-20 However, if it iswell indicated in a compliant patient, it can providesatisfactory results.11,17,18 Therefore, the objective ofthis article was to present the successful orthodontictreatment of a Class III subdivision patient withasymmetric intermaxillary elastic forces. This
aProfessor and head, Department of Orthodontics, Bauru Dental School, Univer-
sity of Sao Paulo, Bauru, Sao Paulo, Brazil.bProfessor, Department of Orthodontics, Bauru Dental School, University of
Sao Paulo, Bauru, Sao Paulo, Brazil.cPostgraduate student, Department of Orthodontics, Bauru Dental School,
University of Sao Paulo, Bauru, Sao Paulo, Brazil.dPrivate practice, Bras�ılia, Distrito Federal, Brazil.
The authors report no commercial, proprietary, or financial interest in the
products or companies described in this article.
Reprint requests to: Guilherme Janson, Department of Orthodontics, Bauru
Dental School University of Sao Paulo, Alameda Octavio Pinheiro Brisolla
9-75, Bauru, SP, 17012-901 Brazil; e-mail, [email protected].
Submitted, July 2008; revised and accepted, August 2008.
0889-5406/$36.00
Copyright � 2010 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2008.08.036
procedure allowed obtaining a good and stableocclusal relationship and a better esthetic facialprofile and smile for the patient.
DIAGNOSIS AND ETIOLOGY
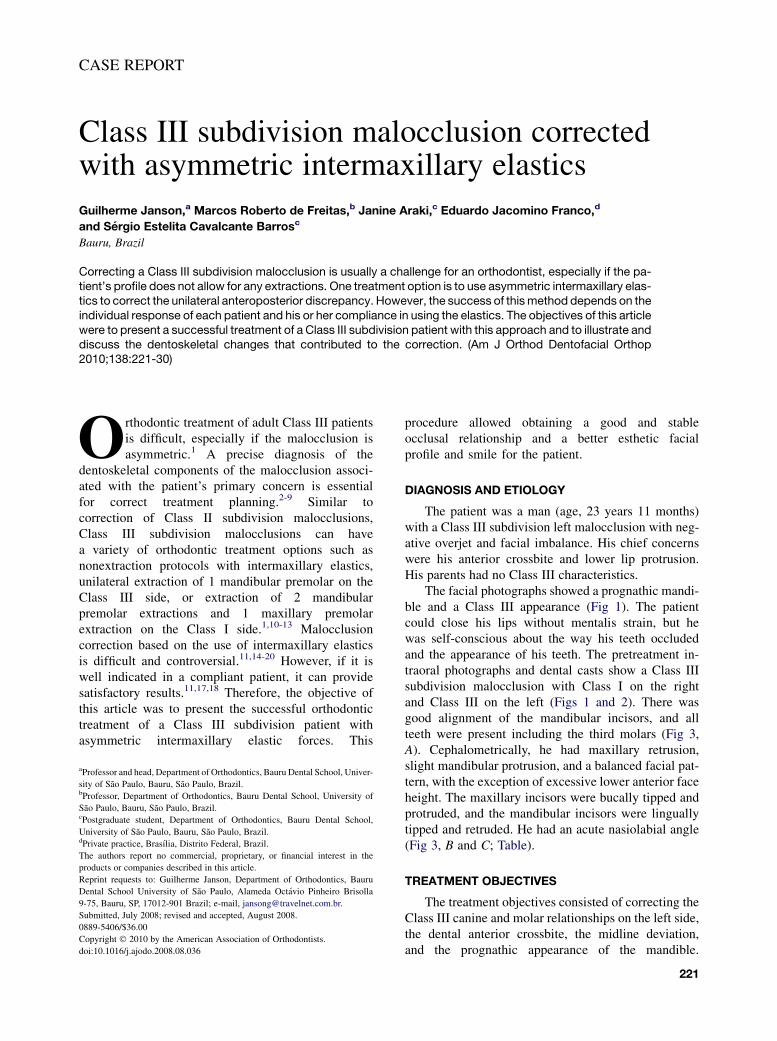
The patient was a man (age, 23 years 11 months)with a Class III subdivision left malocclusion with neg-ative overjet and facial imbalance. His chief concernswere his anterior crossbite and lower lip protrusion.His parents had no Class III characteristics.
The facial photographs showed a prognathic mandi-ble and a Class III appearance (Fig 1). The patientcould close his lips without mentalis strain, but hewas self-conscious about the way his teeth occludedand the appearance of his teeth. The pretreatment in-traoral photographs and dental casts show a Class IIIsubdivision malocclusion with Class I on the rightand Class III on the left (Figs 1 and 2). There wasgood alignment of the mandibular incisors, and allteeth were present including the third molars (Fig 3,A). Cephalometrically, he had maxillary retrusion,slight mandibular protrusion, and a balanced facial pat-tern, with the exception of excessive lower anterior faceheight. The maxillary incisors were bucally tipped andprotruded, and the mandibular incisors were linguallytipped and retruded. He had an acute nasiolabial angle(Fig 3, B and C; Table).
TREATMENT OBJECTIVES
The treatment objectives consisted of correcting theClass III canine and molar relationships on the left side,the dental anterior crossbite, the midline deviation,and the prognathic appearance of the mandible.
221
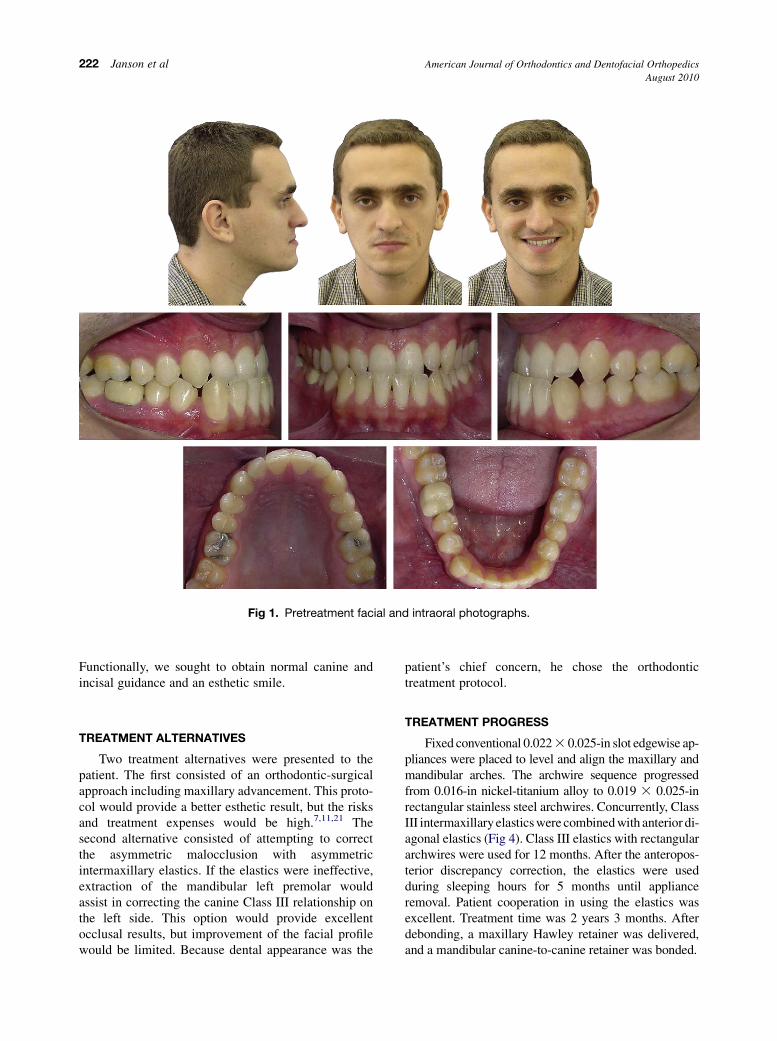
Fig 1. Pretreatment facial and intraoral photographs.
222 Janson et al American Journal of Orthodontics and Dentofacial Orthopedics
August 2010
Functionally, we sought to obtain normal canine andincisal guidance and an esthetic smile.
TREATMENT ALTERNATIVES
Two treatment alternatives were presented to thepatient. The first consisted of an orthodontic-surgicalapproach including maxillary advancement. This proto-col would provide a better esthetic result, but the risksand treatment expenses would be high.7,11,21 Thesecond alternative consisted of attempting to correctthe asymmetric malocclusion with asymmetricintermaxillary elastics. If the elastics were ineffective,extraction of the mandibular left premolar wouldassist in correcting the canine Class III relationship onthe left side. This option would provide excellentocclusal results, but improvement of the facial profilewould be limited. Because dental appearance was the
patient’s chief concern, he chose the orthodontictreatment protocol.
TREATMENT PROGRESS
Fixed conventional 0.022 3 0.025-in slot edgewise ap-pliances were placed to level and align the maxillary andmandibular arches. The archwire sequence progressedfrom 0.016-in nickel-titanium alloy to 0.019 3 0.025-inrectangular stainless steel archwires. Concurrently, ClassIII intermaxillary elastics were combined with anterior di-agonal elastics (Fig 4). Class III elastics with rectangulararchwires were used for 12 months. After the anteropos-terior discrepancy correction, the elastics were usedduring sleeping hours for 5 months until applianceremoval. Patient cooperation in using the elastics wasexcellent. Treatment time was 2 years 3 months. Afterdebonding, a maxillary Hawley retainer was delivered,and a mandibular canine-to-canine retainer was bonded.
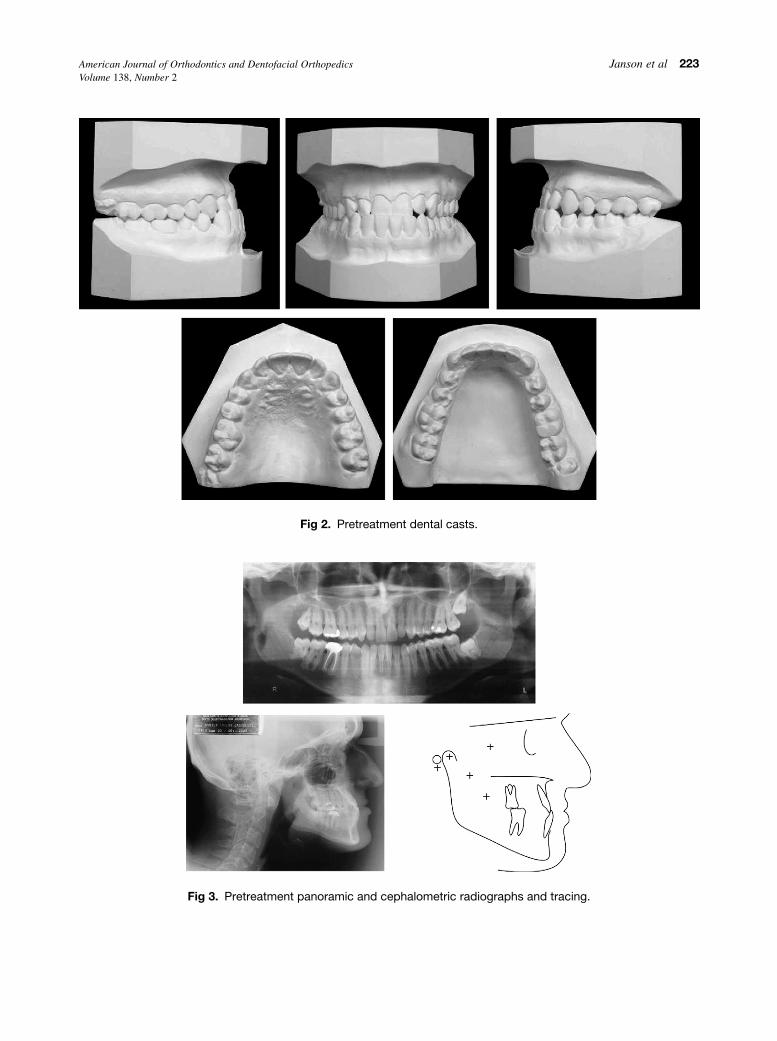
Fig 2. Pretreatment dental casts.
Fig 3. Pretreatment panoramic and cephalometric radiographs and tracing.
American Journal of Orthodontics and Dentofacial Orthopedics Janson et al 223Volume 138, Number 2
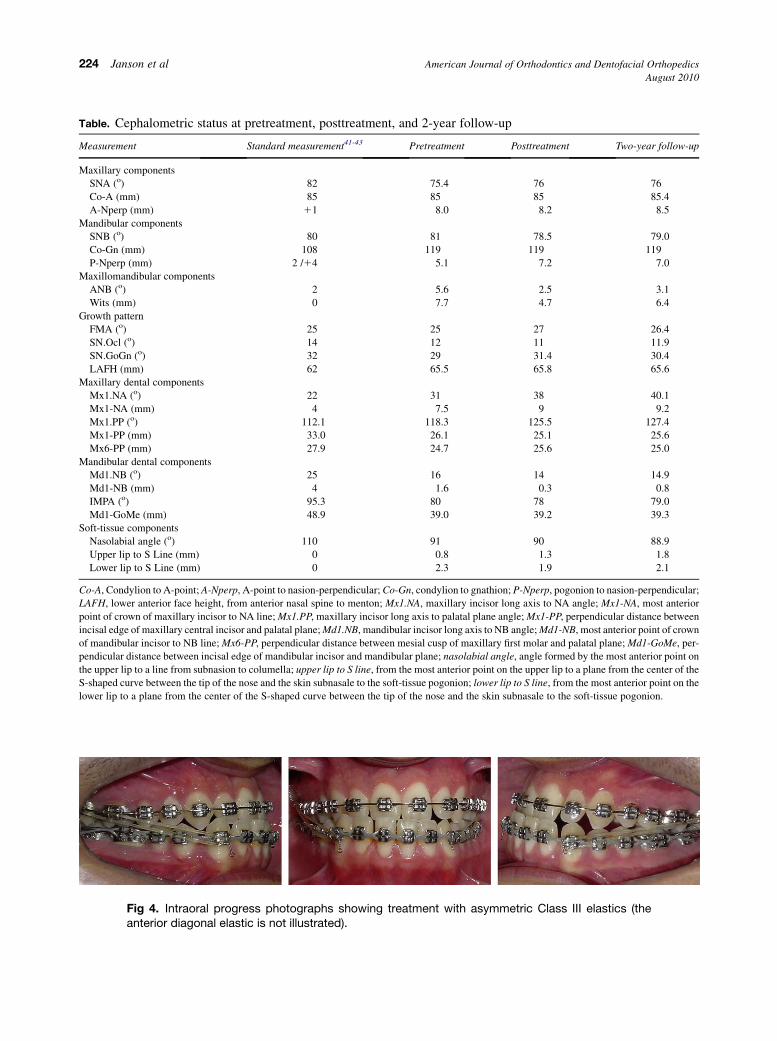
Table. Cephalometric status at pretreatment, posttreatment, and 2-year follow-up
Measurement Standard measurement41-43 Pretreatment Posttreatment Two-year follow-up
Maxillary components
SNA (o) 82 75.4 76 76
Co-A (mm) 85 85 85 85.4
A-Nperp (mm) 11 �8.0 �8.2 �8.5
Mandibular components
SNB (o) 80 81 78.5 79.0
Co-Gn (mm) 108 119 119 119
P-Nperp (mm) �2 /14 �5.1 �7.2 �7.0
Maxillomandibular components
ANB (o) 2 �5.6 �2.5 �3.1
Wits (mm) 0 �7.7 �4.7 �6.4
Growth pattern
FMA (o) 25 25 27 26.4
SN.Ocl (o) 14 12 11 11.9
SN.GoGn (o) 32 29 31.4 30.4
LAFH (mm) 62 65.5 65.8 65.6
Maxillary dental components
Mx1.NA (o) 22 31 38 40.1
Mx1-NA (mm) 4 7.5 9 9.2
Mx1.PP (o) 112.1 118.3 125.5 127.4
Mx1-PP (mm) 33.0 26.1 25.1 25.6
Mx6-PP (mm) 27.9 24.7 25.6 25.0
Mandibular dental components
Md1.NB (o) 25 16 14 14.9
Md1-NB (mm) 4 1.6 0.3 0.8
IMPA (o) 95.3 80 78 79.0
Md1-GoMe (mm) 48.9 39.0 39.2 39.3
Soft-tissue components
Nasolabial angle (o) 110 91 90 88.9
Upper lip to S Line (mm) 0 0.8 1.3 1.8
Lower lip to S Line (mm) 0 2.3 1.9 2.1
Co-A, Condylion to A-point; A-Nperp, A-point to nasion-perpendicular; Co-Gn, condylion to gnathion; P-Nperp, pogonion to nasion-perpendicular;
LAFH, lower anterior face height, from anterior nasal spine to menton; Mx1.NA, maxillary incisor long axis to NA angle; Mx1-NA, most anterior
point of crown of maxillary incisor to NA line; Mx1.PP, maxillary incisor long axis to palatal plane angle; Mx1-PP, perpendicular distance between
incisal edge of maxillary central incisor and palatal plane; Md1.NB, mandibular incisor long axis to NB angle; Md1-NB, most anterior point of crown
of mandibular incisor to NB line; Mx6-PP, perpendicular distance between mesial cusp of maxillary first molar and palatal plane; Md1-GoMe, per-
pendicular distance between incisal edge of mandibular incisor and mandibular plane; nasolabial angle, angle formed by the most anterior point on
the upper lip to a line from subnasion to columella; upper lip to S line, from the most anterior point on the upper lip to a plane from the center of the
S-shaped curve between the tip of the nose and the skin subnasale to the soft-tissue pogonion; lower lip to S line, from the most anterior point on the
lower lip to a plane from the center of the S-shaped curve between the tip of the nose and the skin subnasale to the soft-tissue pogonion.
Fig 4. Intraoral progress photographs showing treatment with asymmetric Class III elastics (theanterior diagonal elastic is not illustrated).
224 Janson et al American Journal of Orthodontics and Dentofacial Orthopedics
August 2010
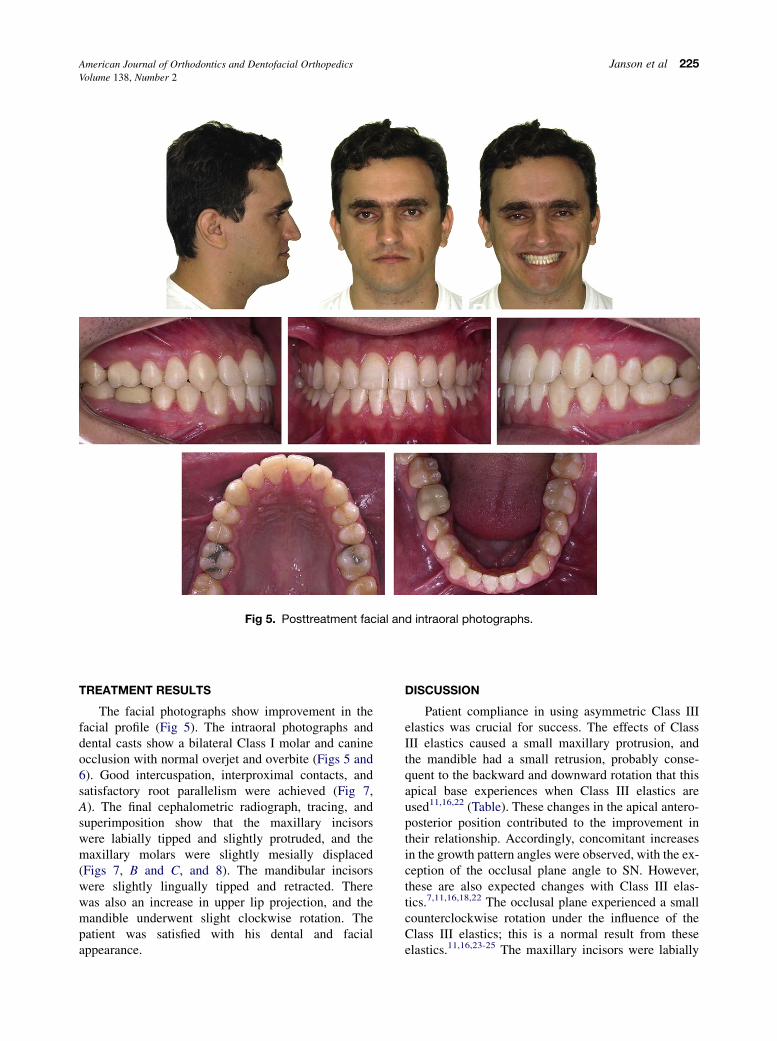
Fig 5. Posttreatment facial and intraoral photographs.
American Journal of Orthodontics and Dentofacial Orthopedics Janson et al 225Volume 138, Number 2
TREATMENT RESULTS
The facial photographs show improvement in thefacial profile (Fig 5). The intraoral photographs anddental casts show a bilateral Class I molar and canineocclusion with normal overjet and overbite (Figs 5 and6). Good intercuspation, interproximal contacts, andsatisfactory root parallelism were achieved (Fig 7,A). The final cephalometric radiograph, tracing, andsuperimposition show that the maxillary incisorswere labially tipped and slightly protruded, and themaxillary molars were slightly mesially displaced(Figs 7, B and C, and 8). The mandibular incisorswere slightly lingually tipped and retracted. Therewas also an increase in upper lip projection, and themandible underwent slight clockwise rotation. Thepatient was satisfied with his dental and facialappearance.
DISCUSSION
Patient compliance in using asymmetric Class IIIelastics was crucial for success. The effects of ClassIII elastics caused a small maxillary protrusion, andthe mandible had a small retrusion, probably conse-quent to the backward and downward rotation that thisapical base experiences when Class III elastics areused11,16,22 (Table). These changes in the apical antero-posterior position contributed to the improvement intheir relationship. Accordingly, concomitant increasesin the growth pattern angles were observed, with the ex-ception of the occlusal plane angle to SN. However,these are also expected changes with Class III elas-tics.7,11,16,18,22 The occlusal plane experienced a smallcounterclockwise rotation under the influence of theClass III elastics; this is a normal result from theseelastics.11,16,23-25 The maxillary incisors were labially

Fig 6. Posttreatment dental casts.
226 Janson et al American Journal of Orthodontics and Dentofacial Orthopedics
August 2010
tipped and protruded, and the mandibular incisors werelingually tipped and retruded. The vertical componentof the elastics produced small extrusions of themaxillary molars and mandibular incisors. Asa consequence of these skeletal and dentoalveolarchanges, there was a decrease in the nasolabial angle,protrusion of the upper lip, and retrusion of the lowerlip, significantly improving his facial profile (Table,Figs 5-8).
If the patient’s compliance had not been good inusing the elastics, another option would have beento extract the mandibular left first premolar. Accord-ing to Class III subdivision malocclusion characteris-tics, with the maxillary midline coincident to themidsagittal plane and the mandibular midline devi-ated to the right, this could be considered the bestchoice to correct the midline deviation and the occlu-sal discrepancy.1 However, this would not be a favor-able treatment alternative for the desired soft-tissuechanges because the anterior crossbite would be cor-rected by retraction of the mandibular incisors withlittle or no protrusion of the maxillary incisors; thiswould cause less improvement in the facial profilethan the nonextraction alternative. On the otherhand, it could be argued that the use of asymmetric
Class III elastics could deviate the maxillary midlineto the right as an unfavorable side effect. Yes, thiscould be possible, but in choosing between these 2treatment options one must select the protocol thatwill fulfill most of the treatment objectives, with thefewest collateral side effects. Based on this, it wasthought that the nonextraction option would providea more favorable profile change, and that the resultingunfavorable maxillary midline deviation would bewithin acceptable limits. According to Johnston etal,26 deviations up to 2 mm of the dental midline tothe midsagittal plane can be clinically satisfactory.The final extraoral smiling photograph confirms this(Fig 5).
It has been stated that anteroposterior intermaxillaryelastics produce significant vertical adverseeffects.16,18,20,25,27,28 This can be true if their use isnot properly monitored. Use of the correct resistanttorques in the maxillary and mandibular incisors tocounteract the Class III elastic forces on these teeth isessential. In this patient, the adverse effects seem tohave been well controlled, because only smallextrusions of the maxillary molars and mandibularincisors were apparent (Fig 8). Inclusion of the secondmolars might also have helped in controlling the adverse
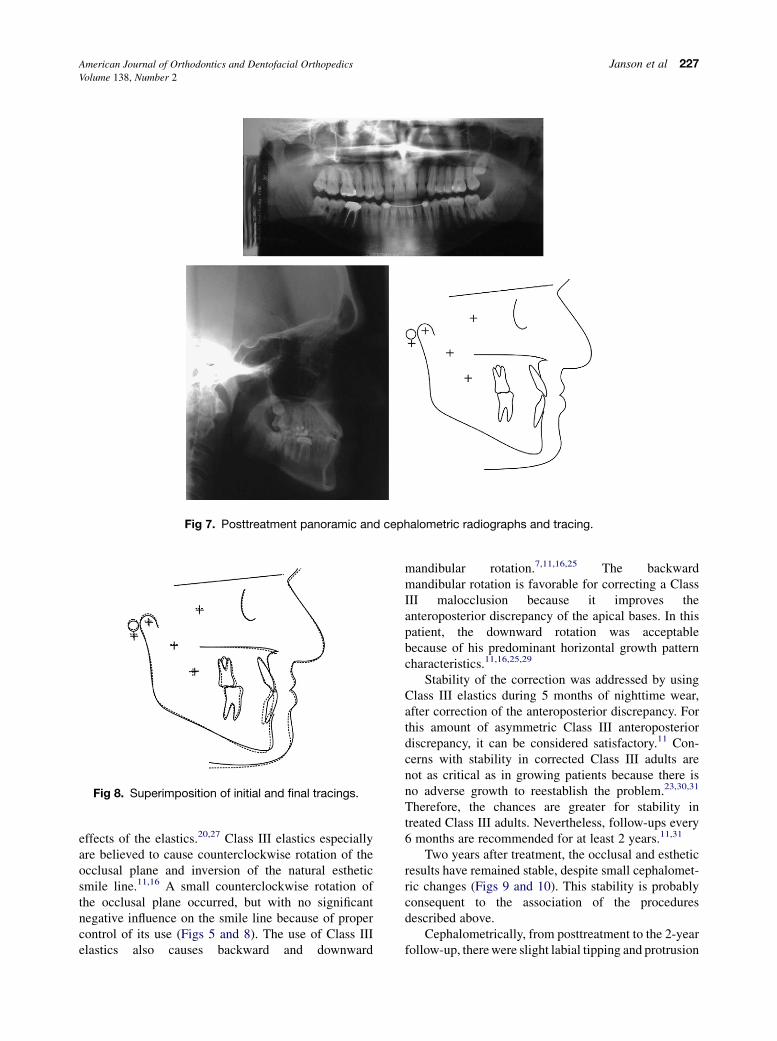
Fig 8. Superimposition of initial and final tracings.
Fig 7. Posttreatment panoramic and cephalometric radiographs and tracing.
American Journal of Orthodontics and Dentofacial Orthopedics Janson et al 227Volume 138, Number 2
effects of the elastics.20,27 Class III elastics especiallyare believed to cause counterclockwise rotation of theocclusal plane and inversion of the natural estheticsmile line.11,16 A small counterclockwise rotation ofthe occlusal plane occurred, but with no significantnegative influence on the smile line because of propercontrol of its use (Figs 5 and 8). The use of Class IIIelastics also causes backward and downward
mandibular rotation.7,11,16,25 The backwardmandibular rotation is favorable for correcting a ClassIII malocclusion because it improves theanteroposterior discrepancy of the apical bases. In thispatient, the downward rotation was acceptablebecause of his predominant horizontal growth patterncharacteristics.11,16,25,29
Stability of the correction was addressed by usingClass III elastics during 5 months of nighttime wear,after correction of the anteroposterior discrepancy. Forthis amount of asymmetric Class III anteroposteriordiscrepancy, it can be considered satisfactory.11 Con-cerns with stability in corrected Class III adults arenot as critical as in growing patients because there isno adverse growth to reestablish the problem.23,30,31
Therefore, the chances are greater for stability intreated Class III adults. Nevertheless, follow-ups every6 months are recommended for at least 2 years.11,31
Two years after treatment, the occlusal and estheticresults have remained stable, despite small cephalomet-ric changes (Figs 9 and 10). This stability is probablyconsequent to the association of the proceduresdescribed above.
Cephalometrically, from posttreatment to the 2-yearfollow-up, there were slight labial tipping and protrusion
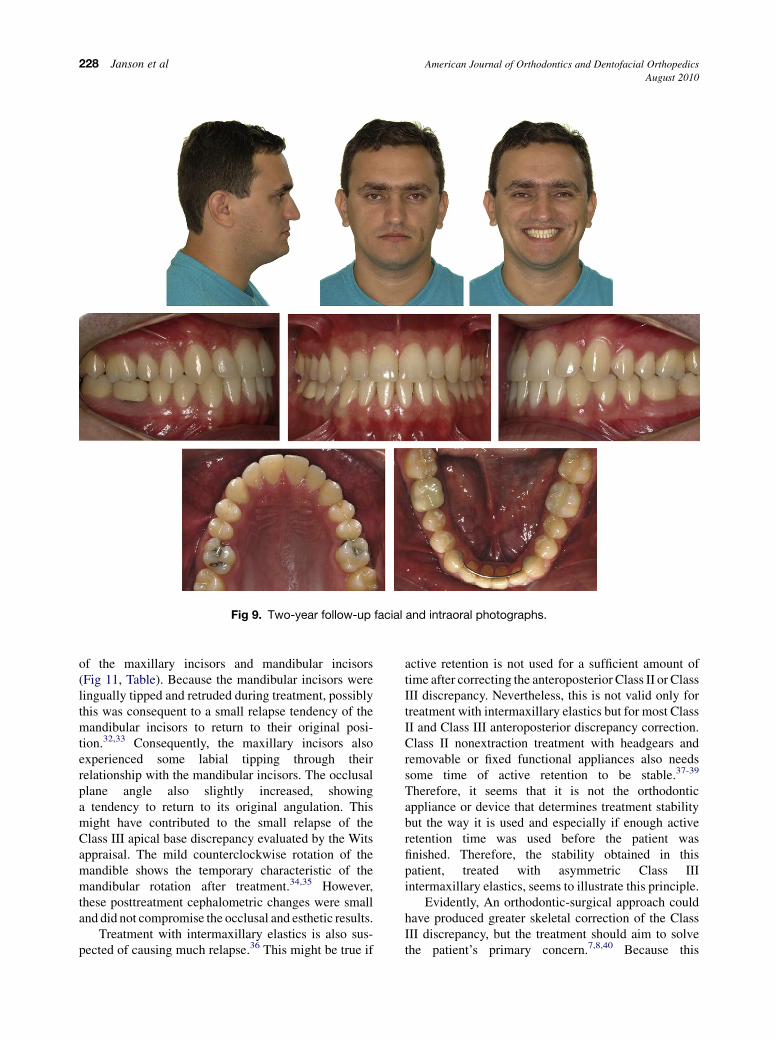
Fig 9. Two-year follow-up facial and intraoral photographs.
228 Janson et al American Journal of Orthodontics and Dentofacial Orthopedics
August 2010
of the maxillary incisors and mandibular incisors(Fig 11, Table). Because the mandibular incisors werelingually tipped and retruded during treatment, possiblythis was consequent to a small relapse tendency of themandibular incisors to return to their original posi-tion.32,33 Consequently, the maxillary incisors alsoexperienced some labial tipping through theirrelationship with the mandibular incisors. The occlusalplane angle also slightly increased, showinga tendency to return to its original angulation. Thismight have contributed to the small relapse of theClass III apical base discrepancy evaluated by the Witsappraisal. The mild counterclockwise rotation of themandible shows the temporary characteristic of themandibular rotation after treatment.34,35 However,these posttreatment cephalometric changes were smalland did not compromise the occlusal and esthetic results.
Treatment with intermaxillary elastics is also sus-pected of causing much relapse.36 This might be true if
active retention is not used for a sufficient amount oftime after correcting the anteroposterior Class II or ClassIII discrepancy. Nevertheless, this is not valid only fortreatment with intermaxillary elastics but for most ClassII and Class III anteroposterior discrepancy correction.Class II nonextraction treatment with headgears andremovable or fixed functional appliances also needssome time of active retention to be stable.37-39
Therefore, it seems that it is not the orthodonticappliance or device that determines treatment stabilitybut the way it is used and especially if enough activeretention time was used before the patient wasfinished. Therefore, the stability obtained in thispatient, treated with asymmetric Class IIIintermaxillary elastics, seems to illustrate this principle.
Evidently, An orthodontic-surgical approach couldhave produced greater skeletal correction of the ClassIII discrepancy, but the treatment should aim to solvethe patient’s primary concern.7,8,40 Because this
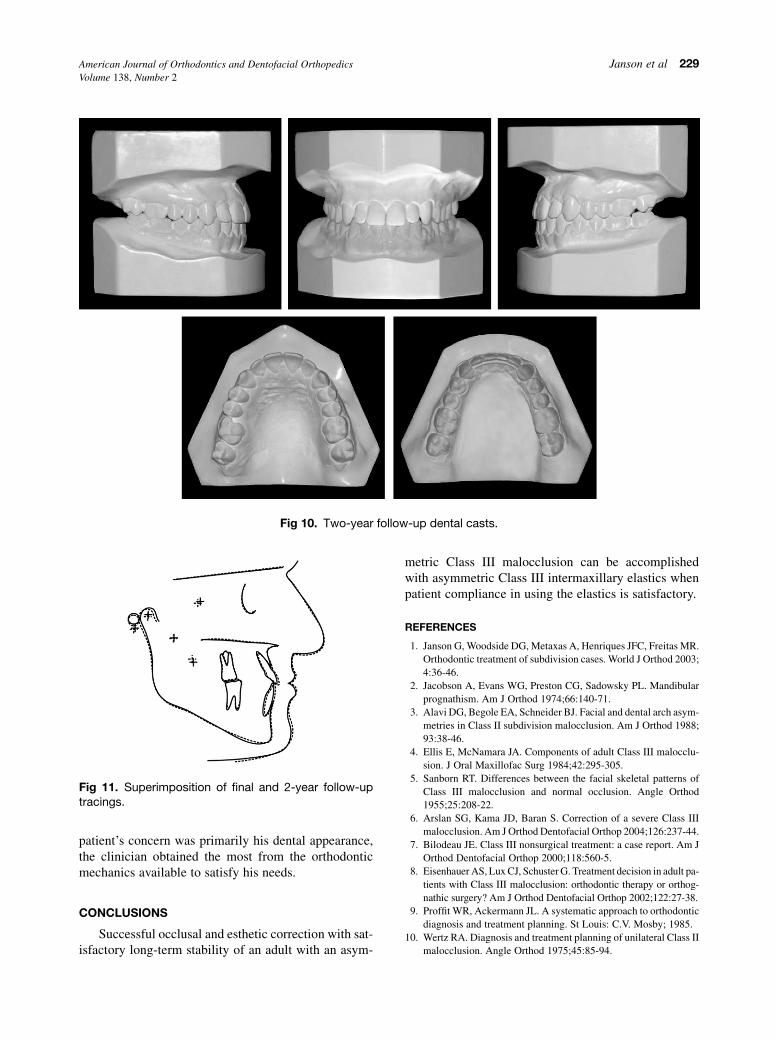
Fig 10. Two-year follow-up dental casts.
Fig 11. Superimposition of final and 2-year follow-uptracings.
American Journal of Orthodontics and Dentofacial Orthopedics Janson et al 229Volume 138, Number 2
patient’s concern was primarily his dental appearance,the clinician obtained the most from the orthodonticmechanics available to satisfy his needs.
CONCLUSIONS
Successful occlusal and esthetic correction with sat-isfactory long-term stability of an adult with an asym-
metric Class III malocclusion can be accomplishedwith asymmetric Class III intermaxillary elastics whenpatient compliance in using the elastics is satisfactory.
REFERENCES
1. Janson G, Woodside DG, Metaxas A, Henriques JFC, Freitas MR.
Orthodontic treatment of subdivision cases. World J Orthod 2003;
4:36-46.
2. Jacobson A, Evans WG, Preston CG, Sadowsky PL. Mandibular
prognathism. Am J Orthod 1974;66:140-71.
3. Alavi DG, Begole EA, Schneider BJ. Facial and dental arch asym-
metries in Class II subdivision malocclusion. Am J Orthod 1988;
93:38-46.
4. Ellis E, McNamara JA. Components of adult Class III malocclu-
sion. J Oral Maxillofac Surg 1984;42:295-305.
5. Sanborn RT. Differences between the facial skeletal patterns of
Class III malocclusion and normal occlusion. Angle Orthod
1955;25:208-22.
6. Arslan SG, Kama JD, Baran S. Correction of a severe Class III
malocclusion. Am J Orthod Dentofacial Orthop 2004;126:237-44.
7. Bilodeau JE. Class III nonsurgical treatment: a case report. Am J
Orthod Dentofacial Orthop 2000;118:560-5.
8. Eisenhauer AS, Lux CJ, Schuster G. Treatment decision in adult pa-
tients with Class III malocclusion: orthodontic therapy or orthog-
nathic surgery? Am J Orthod Dentofacial Orthop 2002;122:27-38.
9. Proffit WR, Ackermann JL. A systematic approach to orthodontic
diagnosis and treatment planning. St Louis: C.V. Mosby; 1985.
10. Wertz RA. Diagnosis and treatment planning of unilateral Class II
malocclusion. Angle Orthod 1975;45:85-94.

230 Janson et al American Journal of Orthodontics and Dentofacial Orthopedics
August 2010
11. Janson G, de Souza JE, Alves FA, Andrade P Jr, Nakamura A, de
Freitas MR, et al. Extreme dentoalveolar compensation in the
treatment of Class III malocclusion. Am J Orthod Dentofacial
Orthop 2005;128:787-94.
12. Cheney EA. The influence of dentofacial asymmetries upon treat-
ment procedures. Am J Orthod 1952;38:934-45.
13. Burstone CJ. Diagnosis and treatment planning of patients with
asymmetries. Semin Orthod 1998;4:153-64.
14. Baker HA. Treatment of protruding and receding jaws by the use
of intermaxillary elastics. Int Dent J 1904;25:344-56.
15. Bien SM. Analysis of the components of forces used to effect the
distal movement of teeth. Am J Orthod 1951;37:514-20.
16. Stewart CM, Chaconas SJ, Caputo AA. Effects of intermaxillary
elastic traction on orthodontic tooth movement. J Oral Rehabil
1978;5:159-66.
17. Hanes RA. Bony profile changes resulting from cervical traction
compared with those resulting from intermaxillary elastics. Am
J Orthod 1959;45:353-64.
18. Ellen EK, Schneider BJ, Sellke T. A comparative study of anchor-
age in bioprogressive versus standard edgewise treatment in Class
II correction with intermaxillary elastic force. Am J Orthod
Dentofacial Orthop 1998;113:430-6.
19. Kanter F. Mandibular anchorage and extraoral force. Am J Orthod
1956;42:194-208.
20. Higley BA, Hill NC. Anchorage in orthodontics. Am J Orthod
1960;46:456-65.
21. Frank C. The nonsurgical orthodontic correction of a Class III
malocclusion. Am J Orthod Dentofacial Orthop 1993;103:107-14.
22. Schudy FF. The control of vertical overbite in clinical orthodon-
tics. Am J Orthod 1968;38:19-39.
23. Kondo E, Ohno T. Nonsurgical and nonextraction treatment of
a skeletal Class III patient with severe prognathic mandible:
long-term stability. World J Orthod 2001;2:115-26.
24. Costa Pinho TM, Ustrell Torrent JM, Correia Pinto JG. Orthodon-
tic camuflage in the case of a skeletal Class III malocclusion.
World J Orthod 2004;5:213-23.
25. Lin J, Gu Y. Preliminary investigation of nonsurgical treatment of
severe skeletal Class III malocclusion in the permanent dentition.
Angle Orthod 2003;73:401-10.
26. Johnston CD, Burden DJ, Stevenson MR. The influence of dental
to facial midline discrepancies on dental attractiveness ratings.
Eur J Orthod 1999;21:517-22.
27. Tweed CH. Philosophy of orthodontic treatment. Am J Orthod
1945;31:74-103.
28. Fischer B. Treatment of Class II,Division 1 differentialdiagnosis and
analysis of mandibular anchorage. Am J Orthod 1948;34:461-90.
29. Lew K. Soft tissue profile changes following orthodontic treat-
ment of Chinese adults with Class III malocclusion. Int J Adult
Orthod Orthognath Surg 1990;5:59-65.
30. Nanda SK. Growth patterns in subjects with long and short faces.
Am J Orthod Dentofacial Orthop 1990;98:247-58.
31. Suri S, Utreja A. Management of a hyperdivergent Class III mal-
occlusion, maxillary midline diastema, and infected mandibular
incisors in a young adult. Am J Orthod Dentofacial Orthop
2003;124:725-34.
32. Kondo E, Aoba TJ. Nonsurgical and nonextraction treatment of
skeletal Class III open bite: its long-term stability. Am J Orthod
Dentofacial Orthop 2000;117:267-87.
33. Westwood PV, McNamara JA Jr, Baccetti T, Franchi L,
Sarver DM. Long-term effects of Class III treatment with
rapid maxillary expansion and facemask therapy followed by
fixed appliances. Am J Orthod Dentofacial Orthop 2003;123:
306-20.
34. Garib DG, Henriques JF, Carvalho PE, Gomes SC. Longitudinal
effects of rapid maxillary expansion. Angle Orthod 2007;77:
442-8.
35. Ferro A, Nucci LP, Ferro F, Gallo C. Long-term stability of
skeletal Class III patients treated with splints, Class III elas-
tics, and chincup. Am J Orthod Dentofacial Orthop 2003;
123:423-34.
36. Riedel RA. A review of the retention problem. Angle Orthod
1960;30:179-99.
37. Janson G, Caffer DC, Henriques JF, de Freitas MR, Neves LS. Sta-
bility of Class II, division 1 treatment with the headgear-activator
combination followed by the edgewise appliance. Angle Orthod
2004;74:594-604.
38. Nanda RS, Nanda SK. Considerations of dentofacial growth in
long-term retention and stability: is active retention needed?
Am J Orthod Dentofacial Orthop 1992;101:297-302.
39. Teuscher U. A growth-related concept for skeletal Class II treat-
ment. Am J Orthod 1978;74:258-75.
40. Bilodeau JE. Correction of a severe Class III malocclusion that re-
quired orthognatic surgery: a case report. Semin Orthod 1996;2:
279-88.
41. McNamara JA. A method of cephalometric evaluation. Am J
Orthod 1984;86:449-69.
42. Scheideman GB, Bell WH, Legan HL, Finn RA, Reisch JS. Ceph-
alometric analysis of dentofacial normals. Am J Orthod 1980;78:
404-20.
43. Steiner CC. The use of cephalometrics as an aid to planning
and assessing orthodontic treatment. Am J Orthod 1960;46:
721-35.