Embed Size (px)
Citation preview

CLReview
Metabolic response to sepsis andtrauma
Br. J. Surg. 1989, Vol. 76, February,115-122
This review examines current knowledge regarding the metabolicresponses to trauma and sepsis. The factors which may mediate theresponses are discussed and the potential value of pharmacological ornutritional manipulation is reviewed.Keywords: Metabolic response, sepsis, trauma
R. G. Douglas andJ. H. F. ShawDepartment of Surgery, AucklandHospital, Park Road, Auckland,New Zealand
Correspondence lo:Associate Professor J. H. F. Shaw
may algo playa part in these changes3. Despite extensiveinvestigation there remains much conjecture about the nature ofthe link between tissue insult and the resultant metabolicresponse.
The accelerated breakdown of skeletal muscle following signifi-cant injury was first identified by Cuthbertson more than 50years ago1. He divided the response into a short-lived 'ebb'phase, corresponding to the period of hypovolaemia andsympathetic activity immediately after injury, and a moreprolonged 'flow' phase which is characterized by a negativenitrogen balance. A catabolic state similar to the flow phase oftrauma algo occurs in patients with established sepsis, and manyparallels can be drawn between the metabolic profile of theseverely injured and septic patient. This article is a review of thepresent knowledge of the metabolic responses to trauma andsepsis. Contention persists over some aspects of the nature ofthese responses and the factors which mediate them, and dataand interpretations of the polemical issues will be presented.
The consequences of a prolonged catabolic response are nowseen more frequently as intensive cart facilities prolong thesurvival of multiply injuréd and seve;rely septic patients.Although modero techniques of enteral and parenteral nutritionare able to reduce the cate of consumption of protein and energyreserves it is not Jet possible to achieve a positive nitrogenbalance in severely ~tressed patients2. The last section of thisreview discusses the impact of intravenous nutrition on themetabolism of septic and trauma patients and summarizes theresults of experimental work with agents which promote proteinconservation in this s.etting.
Mediators oí the metabolic response to sepsis and trauma
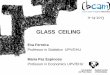
It is well established that the neuroendocrine response to sepsisand trauma effects many oftheobserved changes in metabolism(Figure 1). More recent work has suggested that inflammatorymediators released from the wound itself or from a septic focus
p,O'C..,..
G-- Glucagon G
C?> Insulin e
G>- Alpha-adrenergic--GStimulation
Beta-adrenergic--QStimulation, Glu.cagon
(
The neuroendocrine response
Injury is followed by an outpouring of sympathetic activity anda clearly positive relationship has been established between theinjury severity score4 (ISS) and the plasma concentration ofadrenaline, noradrenaline and dopamineS,6, The plasma cat-echo lamine levels are maximal shortly after injury, but thisresponse is short lived and the plasma levels have usuallyretumed to the normal range within 24 h 7. Although it ispossible to relate plasma hormonallevels to the ISS score wehave recently demonstrated that there is no correlation betweenthe ISS score and the degree of metabolic abnormality seen inpatients after blunt traumaS, The metabolic response in thesepatients appears to be an 'all or none' response-the patientwith an ISS of 15 is metabolically similar to the patient witha score of 50,
At the same time as the sympathetic nervous system re-sponse, the hypothalamic-pituitary axis is al so activated, How-ever, the relationship between injury severity and plasmacortisol is not direct: cortisollevels peak at an ISS of 12 and thenbecome lower with more severe injury9, In addition, the cortisolresponse is transient and the plasma cortisollevel falls to normalwithin a few days of injury. Furthermore, the correlationbetween hormonal changes and metabolic abnormalities isdifficult to show; for example we have found no correlationbetween the plasma cortisollevel and the degree of alteration ineither glucose or protein kinetics8,
The plasma concentration of growth hormone is raised for24 h after injury10, as is that of prolactin, Following thermalinjury antidiuretic hormone levels have been reported to be tentimes control values11, Aldosterone is increasedl2, therenin-angiotensin system is activated 13 and glucagon levels rise
markedlyabout 12h after major injury14,Thus, the ebb phase of injury is associated with increased
sympathetic activity and an outpouring of counter-regulatoryhormones. However, during the stage of maximal nitrogen lossin the flow phase (about 7-10 days after injury) the cat-echolamine, glucagon and cortisol plasma le veIs are notraised 13, This is, however, the time when the plasma insulin levelrises to a peak IS.
Although the catabolic response during the postinjury flowphase and established sepsis is similar, there exist difTerences inthe hormonal milieu between these two conditions; the counter-regulatory hormones remain high in septic patients and theelevation of insulin levels is not a consistent featurel3.
There has been a recent attempt to simulate the hormonalresponses associated with injury in normal volunteers t,oelucidate the role of hormones as mediators of the metabollcchange seen following traumal6. Nine volunteers receiveda continuous 74-h infusion of the three 'stress' hormones
,::7Figure 1 An overriew of lhe imporlanl hormonal regulalory faclors inlhe regulalion of melaholi.~m in .~eplic and injured palienls. FF A. free
fally acid
115

Metabolic response to sepsis and trauma: R. G. Douglas and J. H. F. Shaw
However, the plasma glucose level gives little indication ofglucose turnover and this has been the subject of much recentinvestigation. It is generally agreed that in septic and f1ow phasetrauma patients, glucose turnover is increased and thatgluconeogenesis is enhanced despite freely available plasmaglucose, but there is controversy over changes in glucoseoxidation in these situations31.
GluconeogenesisIn health, gluconeogenesis is effectively inhibited by an in creasein blood glucose levels. However, hepatic glucose production ismaintained at normal or elevated rates during the high flowresponse to trauma or sepsis32-34 despite the hyperglycaemiacharacteristic of such severely ill patients. The suppression ofgluconeogenesis by glucose infusion is very much less effective inseptic and trauma patients than in normal volunteers35-37. Thisreduction in the suppressibility of gluconeogenesis is probablycaused by the increased availability orgluconeogenic substratesoccurring in a favourable hormonal milieu23.26.2S. In severelystressed patients, muscle glycogenolysis and the metabolism ofhypoxic tissues produce lactate, glycerol is released fromadipose tissue, and plasma alanine levels are increased as a resultof enhanced proteolysis34.3S. In burn patients it has beendetermined that lactate is quantitatively the most importantgluconeogenic substrate23. Previously wehave demonstrated anincrease of 40 per cent in the rate of appearance of alanine anda 100 per cent increase in the rate of appearance of gIycerol andavailability of lactate in trauma patientss. On the basis of 2 molof either alanine, glycerol or lactate being required to produce1 mol of glucose it is likely that this substalJtial increase in threecarbon substrates would be adequate to explain the observedihcrease in basal glucose appearance seen in these patients.
However, in recent work by Jahoor et al.39 in burn patientsin which both insulin and glucagon concentrations werelowered simultaneously by infused somatostatin, hepaticglucose production decreased despite an increase in the deliveryof alanine to the liver. These results suggest that gIucoseproduction is controlled at the liver and not by precursorsupply.
Glucose oxidationAlthough most investigators report that glucose oxidation isincreased during the high flow phase and sepsis in absoluteterms, there remains disagreement over whether glucose isoxidized as efficiently as in healthy volunteers4O. The Manches-ter Trauma Unit researchers have found an increase in glucoseoxidation in relation to plasma glucose in injured patients,which they interpreted as a consistent response of substratemobilization and oxidation3°. However, the situation is far fromclear: there exists a considerable body of data derived fromisotopically labelled substrate studies which suggests thatglucose is oxidized less efficiently in septic and traumapatientsS,29.31,41-43. The recently reported reduced activity ofthe pyruvate dehydrogenase complex in septic rats suggests thatintracellular derangements in enzymatically controlled path-ways may account for the observed reduced efficiency of glucosemetabolism44.
It is germane to the interpretation of the data reported onglucose kinetics that the rate of glucose clearance from theplasma is not related to the rate of glucose oxidation or even tothe percentage of glucose uptake oxidized45. Therefore, it isunlikely that reduced glucose oxidation is simply a consequenceof the prevailing insulin resistance.
(cortisol, glucagon and adrenaline) at arate which producedplasma le veIs similar to those seen following mild to moderateinjury. The infusion resulted in a significantly raised basalmetabolic cate, hyperglycaemia, hyperinsulinaemia and insulinresistance, and a negative nitrogen balance. Further studies withsingle hormone infusion indicate that there is a synergistic actionbetween the three hormones. The researchers concluded that thesimultaneous release of stress hormones may be responsible formediating the metabolic response to injury.
Injlammatory mediators
It is not possible to explain the complete spectrum ofmetabolicchanges seen in septic and injured patients by the neuroendo-crine response as it is presently understood. This has provokedthe search for other mediators. Recent research has suggestedthat interleukin 1, a protein released by macrophages at sites ofinflammation, plays a part in the atTerent link between damagedtissue and the central nervous system. This new work isdiscussed further in relation to protein metabolism (see below).Wilmore has recently described synergism in the action ofinflammatory and endocrine mediators and concluded that bothare integral factors of the metabolic response to sepsis andtrauma3.
Energy productionCuthbertson's appealingly simple description of a hypo-metabolic ebb phase and hypermetabolic flow phase17 hasundergone substantial modification in the light ofmore contem-porary research. There is little evidence from clinical studies tosuggest that heat production is reduced during the ebb phasel8,and it is likely that the in crease in metabolic cate during the flowphase is not as large as previously thoughp3. None the lessa modest increase in resting energy expenditure in the flow phaseis commonly observed and, in the extreme case of extensive burninjury, this increase may be as great as 100 per centl9. Themaximal increase in resting energy expenditure coincides withthe maximal cate of protein catabolism and occurs around1 week after injury.
Numerous factors have been proposed to account for theextra heat production, such as the increased oxygen consump-tion of the injured tissues, increased energy expenditure by theheart, the QI0 etTect of raised body temperature, the thermic etTectof accelerated protein breakdown and the heat of evaporationlost from burn surfaces 13.2°. The matter has been the subject of aconcise review by little who concludes that the underlyingmechanism is probably a resetting of hypothalamic regulatorycontroJ21. Yet a furtherexplanation has recently been advanced:it is known that in trauma patients there is an increased cate ofsubstrate recycling in which triglyceride is hydrolysed and thenre-esterified, and glucose and its glycolytic intermediates arerecycled. As there is no net production of free fatty acid orglucose during these cycles but A TP is hydrolysed, suchrecycling represents an energy drain. Wolfe et al. have recentlyquantified the energy dissipated by such substrate recycling and,although their methodology grossly underestimates the extentof these processes, they conclude that it is possible that thesecycles provide the principal biochemical explanation for theincreased heat production seen in trauma patients22.
Glucose metabolism
The post-traumatic ebb phase and the earliest stage of sepsis areboth characterized by hyperglycaemia23. This rapidly estab-lished response is initially the result of enhanced glycogenoly-SiS24 and later a consequence of increased glucose productioncoupled with reduced peripheral utilization23. Sympatheticactivity and circulating adrenaline provide the stimulus forhepatic glycogenolysis and encourage glucagon release whilesimultaneously inhibiting insulin release from the endocrinepancreas2S~27. The release of cortisol probably plays a facili-tatory part in this response28. The plasma glucose levelssubsequently fatI during the post-traurnic flow phase to lesselevated or normal level$29.3O.
lnsu/inAlthough changes in insulin release and responsiveness in septicand trauma patients have been well documented46 4&, the Tole ofthis hormone in the metabolic changes associated with theseconditions remains to be clearly defined.
.The sympathetic discharge following severe burns has beenassociated with an inhibition of insulin release2s, although a lowplasma insulin level is not a consistent feature of the immediate
116 Br. J. Surg.. Vol. 76. No. 2. February 1989

Metabolic re:
postinjury period 15. Plasma insulin levels subsequently rise toreach a peak several days after injury of up to three timesbasal levels49. This coincides with the period of maximalcatabolismso.
During the flow phase, the plasma insulin level is inappro-priately high for the plasma glucose concentration30 with thepancreas showing a normal or augmented response to glucoseinfusionSI.S2. However, this phase ofthe metabolic response ischaracterized by insulin resistance.
The high levels ofinsulin fail to suppress glucose production,and there is a reduction in glycogen storage29, lipolysis and fatoxidationS3. Frayn has demonstrated a highly significant corre-lation (r=O.97) between the plasma insulin concentration andnitrogen loss in trauma patients and concludes from this findingthat protein turnover is resistant to the normal anabolic effect ofinsulinls. However, Jahoor et al. have found in burn patient&that insulin acts to conserve protein by restraining the release ofamino acids from peripheral tissues39. Wilmore has similarlydemonstrated a protein anabolic effect of insulin despiteprofound insulin resistance to carbohydrate in the skeletalmuscle ofinjured patientsS4. The nature ofthe changes in insulinreceptors has not been accurately characterized, although it islikely that there are changes at both the receptor and post-receptor levelss. Experimental animal models most clearlyimplicate glucocorticoids as a cause of insulin resistanceS6,although the mechanism of this response is yet to be ful\yelucidated.
The adaptive value of fuel store mobilizationThe mobilization of fuel reserves in trauma and sepsis iscommon to several species of laboratory animal studied and islikely to be of adaptive value. Infusion ofhypertonic glucose hasbeen shown to decreas,e mortality in pigs fol\owing severehaemorrhageS7 and this manoeuvre has al so resulted in a rapidincrease in blood pressure inrecently inju¡;ed battle casualtiess8.It has been suggested that the observed pressor effect is due toa mass action effect of glucose increasing myocardial glucoseuptake and hence the availability of glucose for anaerobicglycolysisS8. Hyperglycaemia wil\ al so compensate for intra-vascular fluid losses.
The increase in gluconeogenesis and its reduced supressi-bility during exogenous glucose administration in the post-trauma flow stage and in sepsis may reflect the influence of thedamaged and reparatíve tissues on the rest of the bodyS9. Thecel\s in volved in inflammation and wound repair rely on glucoseas a primary fuel which they predominately metabolizeanaerobical\y. The wound may be looked upon as a privilegedorgan whose glucose demands can account for most of theapproximate doubling in glucose turnover seen in severelyburned patients. Wilmore concludes that the increased glucoseturnover provides essential fuel for inflammatory and reparativetissue which optimizes host defences and ensures wound re-pairS4.
Ketone metabolism
Simple starvation is attended by ketosis. As ketone bodies canserve as alternative energy substrates for many tissues, theyreduce whole body glucose demand and therefore gluconeogen-esis from protein. However, in severe sepsis and, to a 1esserextent, trauma there is a blunting of the adaptive ketonaemicresponse and its subsequent nitrogen conservation 74. 75. It islikely that the increased insulin levels seen in stressed surgicalpatients are responsible for the impaired production of ketonebodies 76, although reduced activity of hepatic acylcarnitinetransferase has al so been implicated77.
Protejo metabolism
The negative nitrogen balance described by Cuthbertson1 hasbeen similarly demon~trated in septic patients 78. When thisresponse is prolonged, the resultant protein depletion playsa majar part in the pathogenesis of multiple organ failure whichdevelops in severely injured or septic patients 79. A detailedunderstanding ofthe nature and mechanism ofthe protein loss isimportant to provide a basis for giving more effective nutritionalsupport and offers the alluring possibility ofmetabolic manipu-lation in such cases.
Fat metabolismThe complex changes in the mobilization and oxidation offat insepsis and trauma have not been as fully unravelled as those incarbohydrate metabolismo Again it is appropriate to discuss thepost-trauma changes in the ebb and flow phase, and again thereare parallels to be drawn between the flow phase and established
sepsis.Lipolysis is enhanced immediately after injury by the stimu-
lation of the sympathetic innervation of adipose tissues and byraised plasma adrenaline, glucagon and cortisol levels38.Growth hormone may algo playa part in this response6o. Theaccelerated lipolysis occurs des pite the prevailing hyper-glycaemia and raised plasma insulin61. There is, however, littlecorrelation between plasma free fatty acid levels and the severityof the trauma24.62. This is probably a result of the reducedperfusion of adipose tissues which often follows severe trauma,so that the supply of albumin carriers for released free fatty acids
y
Whole body kinelics in sepsis and traumaA net protein loss may result from a relative decrease in' wholebody protein synthesis, an increase in catabolism, or acombination of both mechanisms, The varied responses re-ported following elective surgical procedures, musculoskeletaltrauma, burns and sepsis are summarized in Table 1. The trauma
117
ponse to sepsis and trauma: R. G. Douglas and J. H. F. Shaw
is inadequate63. In addition, the plasma free fatty acid level isIowered further by the lactic acidosis of systemic hypoxia whichencourages re-esterificationb4.
Septic patients have a lower respiratory quotient (RQ) Ibannon-septic controls, and worsening sepsis is frequently accom-panied by progressive falls in RQ. These findings have beencorroborated by isotopic studies and suggest that increased fatoxidation mar be an important feature of the altered metab-olism seen in sepsis6S-67. During the first few days after severeinjury the RQ riges from a value of close to 0.7 to one thatindicates that carbohydrate is the major fuel13. Glucose infusionin normal volunteers inhibits fat oxidation and the RQ risesabove 1.0 as the excess glucose is deposited as triglyceride.However, in patients with severe sepsis, although the RQ risesfollowing glucose infusion it does not reach a vaIue of 1.0indicating that fat continues to be the main substrate foroxidationsl.
Under most circumstances the rate of uptake of free fattyacids is directly proportional to their plasma concentration68.However, the increase in fatty acid oxidation in sepsis andtrauma is not 'substrate led' as the plasma levels offree fatty acidare often quite low3O. This suggests that there are changes in theintraceIlular metabolism of fat in these patients38.
The preference for fat as an energy substrate is morepronounced in septic than in trauma patients66. Using the sepsisseverity scale developed by E1ebute and Stoner69, it has beenshown that there exists a positive relationship between fatoxidation and sepsis severity, whereas there is a negativereIationship with gIucose oxidation66.
Less is known about changes in triglyceride metabolismo Ithas been reported that the concentration of triglyceride inplasma is elevated in Gram-negative sepsis 70 and after injurylS.
There is presentIr no isotopicalIy-labelled triglyceride suitablefor infusion into patients, but studies in septic animals ha vereveaIed that the increase in trigIyceride concentration is owingto an acceIerated rate of production of trigIyceride, and inparticular very Iow density lipoprotein, rather than the responsebeing secondary to a decrease in triglyceride clearance 71. 72. Theincrease in activity of adipose tissue Iipoprotein lipase isconsistent with the postuIated increase in very low densityIipoprotein tumover 73.

Metabolic response to sepsis and trauma: R. G. Douglas and J. H. F. Shaw
Table 1 Protein synthesis and catabo/ism rates in sepsis and after surgery and trauma
Crane et al. 197782 No change
O'Keefe el al. 197480 Infused r4C]leucine ! No change Reduced postoperativecalorie intake2 cancer patients
Postoperative intakemaintained
Kien et al. 197881 Infused [i3NJglycine ! No changet
Rennie and Harrison198488
Elective orthopaedicn=11
Elective abdominal
operationsn=4
Skin reconstruction inchildrenn=6
Abdominal surgeryn=ll
Skeletal muscle effiux of3-methylhistidine andtyrosine
Infused [15N]glycine
!! ! Postoperation all on IVN10 cancer patients
Kien el al. 197883 Burns, childrenn=ll
Multiple trauman=6
Trauman=43
Sepsisn=22
f 11 Controlled nutritionalsupport
Birkhan et al. 198084 Infused r4C]leucine i 11
Shaw and Wolfe8 f tt Sorne on IVN
Shaw et aU986117
Infused r3N]lysine andr4C]ureaInfused r3N]lysine andr4C]urea
t 11 Net protein catabolismcontinued despite IVN
IVN, intravenous nutrition
-I
>-'" lO';ñ "O4/-
.c I...CIc: .x>--'" c:c: ';
'; 'O...LoO Q,Lo -
Q. CI
~
,E ~
.~ 1J
0-.c '0\IV ~'.v ~u CC '0;
'0; 'O...Loo c.Lo ~Cl. 0\
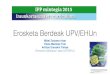
Figure 2 Rates of total protein s}'nthesis. total protein catabolism andnet protein catabolism in normal volunteers. septic patients and in burnedpatients. In septic and burned patients the rate of net protein catabolism issignificantly greater (P < 0'05) than in volunteers. Providing intrarenousnutrition reduces net protein catabolism by significantly increasing totalprotein synthesis. The rate of total protein catabolism remains unchanged(modifiedfrom Shaw and Wolfe.198731. D. Basal nutrirían (post-prandialat I 2 h in normal volunteers); ~. intravenous nutrirían; ..net proteincatabolism
The preceding description of the relative changes in therelationship between net protein synthesis abd catabolism over-simplifies the situation as it exists in the clinical setting as it doesnot include the influence of protein intake. This deficiency isrectified in the model developed by Clague and bis colleagues87,in which they propose that the protein breakdown in response totrauma is largely obligatory, whereas synthesis increases withsubstrate availability. Accordingly, provision ofadequate pro-tein can reduce net nitrogen loss after trauma.
Changes in skeletal muscleSkeletal muscle is the majar site of nitrogen storage and ofnitrogen loss, although the contribution of other tissues such asskin, gut and lungs may not be insubstantial88. The rate ofrelease of 3-methylhistidine, an amino acid derived exclusivelyfrom actin and myosin and excreted unchanged, has been usedas an index of the rate of skeletal muscle breakdown89.Considerable increases in the rate of production of 3-methylhis-tidine have been seen in severely traumatized and septicpatients9°, whereas no increase occurs following orthopaedicoperations and minor injuries91. Although recent doubts havebeen voiced about the specificity of 3-methylhistidine as anindicator of skeletal muscle breakdown92, other investigatorshave provided sound arguments for its continued use93.
In injury, the increased rate of protein release from skeletalmuscle does not simply represent the degradation of damagedtissue; there is increased loss of 3-methylhistidine and changes inskeletal metabolism in muscle undamaged by trauma94.95.
The technique of percutaneous needle biopsy of humanmuscle96 has enabled investigation ofthe intracellular metabolicderangements. The changes in intracellular amino acid concen-tration following elective surgery, trauma and in sepsis aresimilar, suggesting a common response to varying types ofinsult97-99. The response consists of an in crease in essentialamino acids, particularly branched chain amino acids, andreduction in non-essential amino acids largely as a result of a 50per cent decrease in the level of intracellular glutamine97. Thecause of these changes remains a matter for conjecture95~ 1 °°.
of elective surgery results in an inhibition of protein synthesis,whereas catabolism proceeds at an unchanged rateSO-S2. How-ever, in severe trauma involving multiple fractures or burns, orin septic patients, both synthesis and catabolism are increased,with the rate of protein degradation outstripping that ofproductionS,42.83.S4 (Figure 2). The cause of this disparity inresponse is not clear, but it is likely that the postoperativechanges primarily reflect the effect of starvation rather than theresponse to trauma per se. It is noteworthy that the acutemetabolic response to severe injury and sepsis is the directreverse ofthat seen in starvation in which both protein synthesisand degradation are reducedss.S6.
Hepatic protein metabo/ism
The data ofstudies ofwhole body protein metabolism representthe summation of response of the body tissues, but fail to reflectvariation in kinetics between difTerent tissues. In both severetrauma and sepsis, whereas skeletal muscle catabolism exceeds
Surg.. Vol. 76. No. 2. February

Metabolic response to sepsis and trauma: R. G. Douglas and J. H. F. Shaw
synthesis there is a net increase in the production of hepatic Septic and injured patients require approximately 40 kcalstructural and s~cretory prote.insIOI.IO2. ..kg-1 per dayl14 and this energy requirement has traditionalIy
The teleologlcal explanatlon of the autocanrubahsm of been supplied as glucose. Glucose infusion has been de m-muscle tissue in response tc;' ~tress is t.hat th.is mechanis~ alIows onstrated to be a simple and efTective means of conserving badygreat7r than normal quantltl.es of ~ml~o aclds to be avallab~e to protein in severely stressed patients42. However, there has beenthe h~er ~or glucon~og~nesls, oxldatlon and the synthesls of considerable interest in the role of fat as a majar and perhapspro::1~1101~vol~e~ m Immune. defence .and wound. heal- preferred energy .substrate in septic patients and this debate hasmg ...ThlS mcreased hepatlc synthesls occurs at a tIme of recently been revlewed by Longll s. We have used isotopic tracerdepre~sed efficie~cy of .ot~er hepat~c celIul~r fu~ctions~O4.IOS, m~thodology to demonstrate that lipolysis and fatty acidreflectmg the hlgh prlonty of thls functlon m sepsls and oxldation are enhanced in sepsis41.43.67, but whether fat has atraumalO6. greater protein sparing efTect than glucose in this setting is yet to
be resolvedl16.Mechanism 01 protein /oss Despite recent advances in intravenous nutritional supportThe catabolism of muscle protein reserves to provide substrate there are several reports indicating that a positive nitrogenfor increased hepatic synthesis to defend against infection and balance cannot be achieved in septic or severely traumatizedpromote wound healing is an appealing explanation of the patients2,SS. 1ntravenous nutrition (1VN) reduces the net rafechanges in protein metabolism seen in sepsis and trauma. This of loss of protein by increasing the rate of protein synthesis.presents the chalIenge of delineating the neuroendocrine However, the capacity to increase synthesis by providingchanges which mediate this response. substrate falIs short of the increased protein catabolism which
1t is known that physical rest, fever, starvation, glucocor- proceeds uninfluenced by nutritional supportS,l1 7.ticoids and insulin resistance79,SS,IO2 are associated with an The failure of standard 1VN regimens to achieve nitrogenincreased net rafe of protein breakdown, but that none of these retention in severely stressed patients has led to the investigationstimuli induces protein catabolism to the degree seen in sepsis ofmore exotic mixtures. The use ofbranched chain amino acidsand traumalO7. Glucocorticoids cause an increased amino acid to encourage protein anabolism has received much recentrelease, increased oxidation of leucine by skeletal muscle and attention. Branched chain amino acids play an important part infavour hepatic conversion of amino acid to glucose. However, the regulation ofmuscle synthesisllS,119, and muscle biopsies ofit is generalIy believed that glucocorticoids have primarily a injured and septic patients have shown signficant increases in thepermissive role and are not responsible for the overalI protein intracelIular concentration ofbranched chain amino acidsl2O. 1tcatabolism seen in sepsis and trauma26. We have demonstrated has been postulated that this mar provide a stimulus for proteinthat glucagon plays a part in accelerating protein breakdown in synthesis97. Series in which postoperative patients have beentrauma patientslos. infused with branched chain amino acids alonel21, with
Recent work has suggested that factors produced by leuco- ?ranched-chain-amino-acid-enriched 1VNI22 or with lX-keto-cytes mar be central in promoting the changes in protein Isocaproate, the ketoacid breakdown product of leucinel23,metabolism in sepsis and traúma. 1nte?leukin 1, a polypeptide have shown patients to have improved nitrogen balance,synthesized by macrophages as part of the inflammatory presumably on the basis of increased muscle synthesis. As yetresponse, causes rever and leucocytosislO9. Rat muscle incu- there are no data from prospective trials to support the routinebated with interleukin 1 showed a stimulated rate ofproteolysis use of such modified 1VN mixtures.but the protein synthesis rate was unafTectedllO. These efTectsmar be mediated by prostaglandin E2 as the interleukin 1increased prostaglandin E2 production and the catabolic efTectsof interleukin 1 can be abolished by the addition of in-domethacin. When injected into the peritoneal space of rats,interleukin 1 increasecj the rate of synthesis of hepatic secretoryand structural proteinslll.112. The field of inflammatory medi-ators is advancing rapidly as new proteins are isolated and theiractions described. ,
Consequences of a prolonged catabolic stateThe breakdown of skeletal muscle that occurs in septic andtrauma patients may be of adaptive advantage as the cónvales-cing animal is provided with adequate energy substrates andamino acids for hepatic protein synthesis. However, if ibiscatabolic response is prolonged the loss ofbody protein can posea threat to survival by resulting in pulmonary and cardiovascu-lar insufficiency, and impaired immune function and woundhealing26. It is for these reasons thatattempts have been made toreverse or at least slow down protein catabolism in critically illsurgical patients.
The effects of nutritional support
The optimal nutritional support of severely injured and septicpatients has been the subject of intensive investigation. As suchpatients have a basal metabolic expenditure elevated by 20percent or moreabove normal3! and astheycan lose as much as40 g nitrogen a day!!3, they exhaust their energy and proteinreserves much more rapidly than non-stressed patients. AI-though normal hospital food is the most efficient means ofproviding calones and protein to these patients, their gastro-intestinal system is frequently unable to cope and intravenousnutritional support is indicated.
Pharmacological manipulationHormonal blockade
Several approaches have been taken in attempts to attenuate thecatabolic response of severe surgical illness by hormonalblockade. Epidural anaesthesia abolishes the postoperativerelease of catecholamines and cortisol and has been shown toimprove the cumulative nitrogen balance over a S-dar post-operative period in women after hysterectomy124. Using iso-topic tracer methodology we have recently studied the effects ofepidural anaesthesia in 23 patients who had recently undergoneextensive surgical procedures12S. There was a 20 per centdecrease in the Tale of production of glucose with a parallelreduction in glucose oxidation, and net protein catabolism asmeasured by the rateofappearance ofr4C]urea was reduced by11 per cent.
The sympathetic response mar also be attenuated withspecific pharmacological antagonists. Sympatholytic drugs havebeen demonstrated to reduce the degree of hypermetabolism inburn patients 126. In OUT laboratory we have studied the effects of:x and p blockade produced by infusions of phentolamine andpropranolol respectively in stressed patients receiving intra-venous nutrition 127. OUT data demonstrate that the Tole of thesympathetic nervous system in the promotion of endogenousglucose turnover in such patients is primarily a p-adrenergiceffect, whereas the promotion of protein catabolism is mainly an:x-adrenergic effect.
Considerable interest in the Tole of prostaglandins as effec-tors ofthe stress response has been aroused by the recent work oninterleukin l. However, decreasing prostaglandin synthesis withcyclo-oxygenase inhibitors does not reduce muscle catabolismin septic or thermal injury models in animalsl2S.129 or in septicpatients lOS, and their use exposes patients to side-efTects such aspeptic ulceration and impaired haemostasis.
~

Metabolic response to sepsis and trauma: R. G. Douglas and J. H. F. Shaw
I METABt'\1 1'" DATe I i 2. Streat S, Hill GL. Nutritional support in the management ofI nuOL.C RATE I 20 -40% criticallyill patients in surgical intensivecare. Wor/d J Surg 1987;
11: 194-201.I I=t I~I 11TI117 A TI!")'" I i Fat Oxidation 3. ~iI.more. DW. Are the metabolic alterations :associated withI FUEL UTlLlZATION I I cntlcal IlIness related to the hormonal envlronment? C/in
...Glucose Oxidation Nutrition 1986; 5: 9-20.4. Baker SP, O'Neil B, Haddon W, Long WB. The injury severity
score. A method for describing patients \\1th multiple injuries andI I evaluating emergency careo J Trauma 1974; 14: 187-95.
i 5. Frayn KN, Little RA, Maycock PF, Stoner HB. The relationshipof plasma catecholamines to acute metabolic and hormonalresponses to injury in mano Circ Shock 1985; 16: 229-40.
6. Davies CL, Newman Rl, Molyneux SG, Graham-Smith DG.The relationship between plasma catecholamines and severity ofinjury in mano J Trauma 1984; 24: 99-105.
7. Barton RN, Stoner HB, Watson SM. Plasma cortisol and ACTHin the severely injured. Arch Emerg Med 1984; 1: 170.
8. Shaw lHF, Wolfe RR. An integrated analysis of glucose, fat andprotein metabolism in severely traumatised patients: studies inthe basal state and the response to intravenous nutrition. AnnSurg 1989; 207: 63-72.
9. Barton RN, Passingham Bl. ElTect ofbinding to plasma proteinson the interpretation of plasma cortisol concentrations afteraccidental injury. C/in Sci 1981; 61: 399-405.
10. Carey LC, Cloutier CT, Lowery BD. Growth hormone andadrenal cortical response to shock and trauma in the humano AnnSurg 1971; 174: 451-8.
11. Morgan Rl, Martyn lA, Philbin DM, Coggins CH, Burke lF.Water metabolism and antidiuretic hormone (ADH) responsefollowing thermal injury. J Trauma 1980; 20: 468-72.
12. Le Quesne LP, Cochrane lPS, Fieldman NR. Fluid andelectrolyte disturbances after trauma: the Tole of adrenocorticaland pituitary hormones. Br Med Bu//1985; 41: 212-17.
13. Sioner HB. Metabolism after trauma and sepsis. Circ Shock1986; 19: 75-87. -
14. Meguid MM, Brennan MF, Aoki TT, Muller WA, Ball MR,.Moore FD. Hormone-substrate interrelationships following
trauma. Arch Surg 1974; 109: 776-83.15 Frayn KN. Hormonal control of metabolism in trauma and
sepsis. C/in Endocrino/1986; 24: 577-99.16. Bessey PQ, Watters 1M, Black RR, Brooks DC, Aoki TT,
Wilmore DW. Hormonal mechanisms ofinsulin resistance. ArchEmerg Med 1984; 1: 170.
17. Cuthbertson DP. Observations on the disturbance of metab-olism produced by injury to the limbs. Q J ."Ied 1932; 1: 237-46.
18. Little RA, Stoner HB, Frayn KN. Substrate oxidation shortlyafter accidental injury in mano C/in Sci 1981; 61: 789-91.
19. Long CL. Energy balance and carbohydrate metabolism ininfection and sepsis. Am J C/in Nutr 1977; 30: 301-10.
20. Cuthbertson DP. Alterations in metabolism following injury:part l. lnjury 1980; 11: 175-89.
21. Little RA. Heat production after injury. Br -"Ied Bul/ 1985; 41:226-31.
22. Wolfe RR, Herndon DN, lahoor F, Miyoshi H, Wolfe M. TheelTect of severe burn injury on substrate recycling by glucose andfatty acids. N Eng/ J Med 1987; 317: 403-8.
23. Wolfe RR, MiIler HI, Spitzer 11. Glucose and lactate metabolismin burn and shock. Am J Physio/1977; 232: 415-18.
24. Stoner HB, Frayn KN, Barton RN, Threlfall Cl, Little RA. Therelationship between plasma substrates and hormone and theseverity ofinjury in 277 recently injured patients. C/in Sci 1979;56: 563-73.
25. Allison SP, Hinton P, Chamberlain MI. Intravenous glucosetolerance, insulin and free fatty acid le veIs in burned patients.Lancet 1968; ii: 1113-16.
26. Ryan NT. Metabolic adaptations for energy production duringtrauma and sepsis. Surg C/in North Am 1976; 56: 1073-90.
27. Rennie MI, Edwards RHT. Carbohydratemetabolism ofskeletalmuscle and its disorders. In: Dickens F, Randle Pl, Whelan W,eds. Carbohydrate Metabo/ism and lts Disorders. London: Aca-demic Press, 1968; 3: 1-118.
28. Wilmore DW. Hormonal responses and their efTect on metab-olism. Surg C/in North Am 1976; 56: 999-1018.
29. Wolfe RR, Durkot MI, Allsop IR, Burke lF. Glucose metab-olism in severely burned patients. Metabo/ism 1979:28: 1031-39.
30. Frayn KN, Little RA, Stoner HB, Galasko CSB. Metaboliccontrol in non-septic patients with musculo-skeletal injuries.lnjury 1984; ]6: 73-9.
31. Shaw lHF, Wolfe RR. Energy and protein metabolism in sepsisand trauma. Aust N Z J Surg 1987; 57: 41-7.
Acutely
.J, Insulin/Glucagon Ratio
I HORMa'JE STATUS I i Catecholamines
i CortisolFigure 3 Summary o/ the metabolic changes associated with criticalsurgical illness (modified from Sha\~' and Wolfe. 198731)
Anabolic hormonesThe use of anabolic horrnones to attenuate the rate of break-clown of body reserves is an appealing proposition. Insulin hasbeen shown to improve nitrogen balance in trauma patientsl30,but was found to have no effect on the gain of body nitrogen orfat when used as an adjuvant with a 2-week course of IVNI31.Similarly, anabolic steroids have improved the nitrogen balancein postoperative patientsl32, but have not been demonstrated toimprove the efficacy of IVNI33.
Interest in the therapeutic role of human growth hormonehas increased since 1985 when gene recombinant technologyenabled its manufacture on a scale which makes its use asa pharrnacological agent feasible. Several early investigatorsreported improved nitrogen balance in bum patients to whomgrowth hormone was administeredI34-36. More recently Wardand colleagues have demonstrated a favourable influence ofgrowth hormone on protein kinetics in postoperativepatients 13 7. However, the therapeutic rol e of growth horrnone
in catabolic patients awaits further definition.
Discussion (Figure 3)
The increased reIease of hormones, particuIarIy adrenaIine,gIucagon and cortisoI, mediate many of the metaboIic changesseen in sepsis and trauma. The roIe ofinterIeukin 1 has yet to bepreciseIy defined, but there is increasing evidence that substan-ces reIeased from damaged tissue are at Ieast partIr responsibIefor the acceIerated proteoIysis seen in severe surgicaI ilIness.
GIucose turnover is increased in sepsis and trauma, butglucose is oxidized with reduced efficiency. There is evidence tosuggest that fat is the preferred energy substrate in septic and, toa lesser degree, injured patients.
In critical surgical ilIness the rates of both protein synthesisand catabolism are increased. However, the increase in catabol-ism is of greater magnitude resulting in a net breakdown ofprotein and, if prolonged, muscular wasting, cardiopulmonaryinsufficiency and immune compromise.
The provision of sufficient energy substrates and nitrogendoes not reduce the catabolic response but encourages proteinsynthesis, decreasing net catabolism. Numerous substrate,hormonal and pharmacoIogical manipulations have been triedto improve the nitrogen balance in surgical patients who areseverely ilI. To date, the clinical efficacy of non e has been
conclusively proved.
References
1. Cuthbertson DP. The disturbance of metabolism produced bybony and non-bony injury, with notes on certain abnormalconditions ofbone. Biochem J 1930; 24: 1244-63.
Br. J. Surg.. Vol. 76. No. 2. February 1989120

32. Long CL, Spencer JL, Kinney JM, Geiger JW. Cmetabolism in man: e/Tect of elective operation and ]J Appl Ph}'sioI1971; 31: 110-16.
33. Imamura M, Clowes GHA Jr, Blackburn GLmetabolism and gluconeogenesis in trauma and se1975; 77: 868-80.
34. Wilmore DW, Goodwin CW, Aulick LH et al. Enand infection on visceral metabolismo Ann Sur9491-504.
35. Long CL, Kinney JM, Geiger JW. Nonsupplgluconeogenesis by glucose in septic patients. Meta25: 193-200.
36. Shaw JHF, Wolfe RR. Determination of glucose toxidation in normal volunteers and septic patientsand radioisotopes: the response to glucose infusicparenteral nutrition. Aust N Z J Surg 1986; 56: 7~
37. Wolfe RR. Burn trauma and increased glucoseTrauma 1979; 19: 898-9.
38. Frayn KN. Substrateturnover afterinjury. Br Med li232-9.
39. JahoorF,HerndonDN, Wolfe RR. Roleofinsulin althe response of glucose and alanine kinetics in 1:patients. J Clin Im'est 1986; 78: 807-14.
40. Oowes GHA, 0'Donne11 TF, Blackburn GF, Makimetabolism and proteolysis in traumatised and septiClin Norrh Am 1976; 56: 1169-84.
41. Shaw JHF, Wolfe RR. Response to lipid and glucosesepsis: a kinetic analysis. Metabolism 1985; 34: 442
42. Shaw JHF, Klein S, Wolfe RR. Assessment of alanilglucose interrelationships in normal subjects and in ¡:sepsis with stable isotopic tracers. Surgery 1985; 9i
43. Shaw JHF, Januskiewicz J, Horsborough R. Glucand oxidation in normal volunteers, septicaemic ¡:patients with severe pancreatitis. Circ Shock 1985;
44. Yary TC, Siegal JH, Wakatani T, Sato T, Aoyamasepsis on activity ofpyruvate dehydrogenase complemuscJe and liver. Am J Ph}'sioI1986; 13: 634-40.
45. Wolfe RR, O'Donnell TF Jr, Stone MD, RichmondJF. Investigation of factors determining the optirinfusion Tale in total parenteral nutrition. Metabolis892-900.
46. Turinsky J, Saba TM, Scovill W A, Chestnut T. IJinsulin secretion and resistance after burns. J Traurn344-50.
47. Porte D, Robertson RP. Control of insulin secretecholamines, stress and the sympathetic nervous sProc 1973; 32: 1792-6.
48. Yitek Y, Lang DJ, Cowley RA. Admission serumglucose levels in 247 accident victims. Clin Chim Acr93-104.
49. Ryan NT, Blackburn GL, Clowes GHA Jr. Di/Teresensitivity to elevated endogenous insulin le veIs duJmental peritonitis in rats. Metabolism 1974; 23: 108
50. Stoner HB, Frayn KN, Barton RN, Threlfall CJ, Lit!relationships between plasma substrates and horma]severity of injury in 277 recently injured patients. Ch56: 563-73.
51. Black PR, Brooks DC, Bessey PQ, Wolfe RR, WilMechanisms of insulin resistance following injury.1982; 196: 420-9.
52. Gump FE, Long C, Killian P, Kinney JM. Studiesintolerance in septic patients. J Trauma 1974; 14: 3'
53. Askanazi J, Carpentier YA, Elwyn DH et al. Inf1uelparenteral nutrition on fuel utilization in injury amAnn Surg 1980; 191: 40-6.
54. Wilmore DW. The wound as an argaDo In: Frayn KNeds. The Scientific Basis of rhe Care of the Cr.Manchester: Manchester University Press, 1986: 45-
55. Heath DF. SubCellular aspects ofthe response to traurBu111985; 41: 240-5.
56. Barton RN, Passingham BJ. Evidence for a Tolecorticoids in the developmen t of insulin resistance arte]limb injury in the rato J Endocrinol 1986; 86: 363- 7(
57. Stremple JF, Thomas H, Sakach y, Trelka D. TIutilizaton of hypertonic glucose during haemorrhaSurger}' 1976; 80: 4--]2.McNamara JJ, Molot MD, Dunn RA, Stremple JFhypertonic glucose in hypovolemic shock in mano Ann176: 247-50.
--.Wilmore DW, Aulick LH. Metabolicchanges in burneSurg C/in Xorlh Amer ]978; 58: 1173-87.
58
Metabolic response to sepsis and trauma: R. G. Douglas and J. H. F. Shaw
:arbohydrate 60. Frayn KN, Price DA, Maycock PF, Carroll SM. Plasmamajor injury. somatomedin activity after injury in man and its relationship to
other hormonal and metabolic changes. Clin Endocrinol1984;el al. Liver 20: 179-87.psis. Surgery 61. Carpentier Y, Askanazi J, Elwyn DH el al. Effects ofhypercaloric
glucose infusion on lipid metabolism in injury and sepsis.fect of injury J Trauma 1979; 19: 649-54., 1980; 192: 62. Wolfe RR, Miller HI. Cardiovascular and metabolic responses
during burn shock in the guinea pig. Am J Ph)'sioI1976; 231:'essibility of 892-7.bolism 1976; 63. Stoner HB, Matthews J. Studies in the mechanism ofshock. Fat
mobilisation after injury. Br J Exp Parho11967; 48: 58-65.urnover and 64. Miller HI, Issekutz B Jr, Paul P. Effect oflactic acid on plasmausing stable free fatty acids in pancreatectomized dogs. Am J Ph)'sioI1964;m and total 207: 1226-30.15-91. 65. Nanni G, Siegel JH, Coleman B, Fader P, Castglione R.production. Increased lipid fuel dependence in the critically ill septic patient.
J Trauma 1984; 24: 14-30.lu/l1985;41: 66. Stoner HB, Little RA, Frayn KN, Elebute AE, Tresaderm J,
Gross E. The effect ofsepsis on the oxidation of carbohydrate andId glucose in fato Br J Surg 1983; 70: 32-5. .lurn injured 67. Shaw JHF, Wolfe RR. Free fatty acid and glycerol kinetics in
septic patients and in patients with gastrointestinal cancel: theTN. Energy response to glucose infusion and parenteral feeding. Ann Surgic mano Surg 1987; 205: 368-76.
68. Vranic M. Turnover of free fatty acids and triglyceride. Aninfusionsin overview. Fed Proc 1975; 34: 2233-7.
~-9. 69. Elebute AE, Stoner HB. The grading of sepsis. Br J Surg 1983;le, urea and 70: 29-31.latients with 70. Gallin JI, Kaye D, O'Leary WM. Serum lipids in infection. N': 557-67. Engl J Med 1969; 281: 1081-6.ose kinetics 71. Shaw JHF, Wolfe RR. Very low density lipoprotein-fatty acidlatients and kinetics in sepsis. Surg Forum 1984; 35: 128-9.16; 77-8. 72. Wolfe RR, Shaw JHF, Durkot MJ. Effect o[ sepsis on VLDLH. Effect of kinetics: responses in basal state and during glucose infusion. Amx in skeletal .J Physiol1985; 248: 732-40.
73. Robin AP, Grenwood MRC, Askanazi J er al. Influence oftotalDA, Burke parenteral nutrition on tissue lipoprotein lipase activity duringnal glucose chronic and acute illness. Ann Surg 1981; 194: 681-6.m 1980; 29: 74. WannemacherRW Jr.Keyroleofvariousindividualaminoacids
in host response to infection. Am J Clin Nurr 1977; 30: 1269-80..ynamics of ; 75. Birkhan RH, Long CL, Fitkin DL, Bujnardo AC, Geiger JW,la 1977; 17: Blakemore WS. A comparison of the effects of skeletal trauma
and surgery on the ketosis ofstarvation in mano J Trauma 1981'ion by cat- 21: 513-19.ystem. Fed 76. Neufeld HA, Pace JG, Kaninski ML el al. A probable endocrine
basis for the depression of ketone bodies during infections orinsulin and inflammatory state in rats. Endocrinology 1980; 107: 596-601.a 1979; 95: 77. Wannemacher RW, Pace JG, Beall FA, Dinterman RE, Petrella
VI, Neufeld HA. RoJe of the liver in regulation of ketone body'ntial tissue production during sepsis. J Clin In¡;esr 1979; 64: 1565-72.ing experi- 78. Clowes GHA, Randall HT, Cha CJ. Amino acid and energy1-9. metabolism in septic and traumatized patients. JPEN 1980; 4:tle RA. The 195-205.lIes and the 79. Hassett J, Border JR. The metabolic response to trauma and'n Sci 1979; sepsis. World J Surg 1983; 7: 125-31.
80. O'Keefe SJD, Sender PM, James WPT. Catabolic loss of bodymore DW. nitrogen in response to surgery. Lancel 1974; ii: 1035-8.Ann Surg 81. Kien CL, Young VR, Rohrbaugh DK, Burke JF. Whole body
protein synthesis and breakdown in children before and afterof glucose reconstructive surgery of the skin. ,\1erabolism 1978; 27: 27-34.
78-88. 82. Crane CW, Picou D, Smith R, Waterlow JC. Protein turnover inIce of total patients before and after elective orthopaedic operations. Bri infection. J Surg 1977; 64: 129-33.
83. Kien CL, Young VR, Rohrbaugh DK, Burke JF. Increased rates, Little RA, of whole body protejo synthesis and breakdown in childrenilica/ly Il/. recovering from burns. Ann Surg 1978; 187: 383-91.-59. 84. Birkhan RH, Long CL, Fitkin D, Dyger JW, Blakemore WS.Da. Br .\1 ed Effects of major skeletal trauma on whole body protein turnover
in man measured by L-[14C}leucine. Surger)' 1980; 88: 294-9.of gluco- 85. Kinney JM, Elwyn DH. Protein metabolism in the traumatised
rischaemic patient. Acra Chir Scand (supp!) 1985; 522: 45-6.). 86. Millward DJ, Waterlow JC. Effect of nutrition on protein.tyocardial turnover in skeletal muscle. Fed Proc 1978; 37: 2283-90.gic shock. 87. Clague MB, Keir MJ, Wright PD, Johnston IDA. The effects of
nutrition and trauma on who!e-body protejo metabolism in mano'. Effect of Clin Sci 1983; 65: 165-75.Surg 1972; 88. Rennie MJ, Harrison R. Effects of injury, disease and ma!nutri-
tion on protein metabolism in mano Lancer 1984; i: 323-5.:d patients. 89. Young VR, Monro HN. 3-Methy!histidine and muscle protejo
turnover: an overview. Fed Frac 1978; 37: 2291-300.
59
Br. J. Surg.. Vol. 76. No. 2. Februarv 1989 121

Metabolic res pon se to sepsis and trauma: R. G. Douglas and J. H. F. Shaw
t
114. Hill GL, Church J. Energy and protein requirements in generalsurgical patients requiring intravenous nutrition. Br J Surg 1984;71: 1-9.
115. Long CL. Fuel preferences in the septic patient: glucose or lipid?JPEN 1987; 11: 333-5.
116. Shaw JHF. Recent advances in the nutritional management ofcritically ill surgical patients. N Z Med J 1986; 99: 665-7.
117. ShawJHF, WildboreM, WolfeRR.Who]ebodyproteinkineticsin severely septic patients. Ann Surg 1986; 20S: 288-94.
118. Odessey R, Khaiarallah EA, Goldberry AC. Origin and possiblesignificance of alanine production by skeletal muscle. J BiolChem 1974; 249: 7623-32.
119. Buse MG, Reid M. Leucine: a possible regu]ator of proteinturnover in musc]e. J Clin lnrest 1975; SS: 125(}--61.
120. Askanazi J, Carpentier Y, Michelson CB et al. Muscle andplasma amino acids following injury. Ann Surg 1980; 192: 78-85.
121. Freund H, Hover HC, Ataman S, Fischer JE. Infusion of thebranched chain amino acids in postoperative patients. Ann Surg1979; 190: 18-23.
122. Cerra FB, Upson D, Angelico R et al. Branched chains supportpostoperative protein synthesis. Surgery 1982; 92: 192-9.
123. Sapir DG, Stewart DM, Walser M et al. Effects 0(. alpha-ketoisocaproate and of leucine on nitrogen metabolism inpostoperative patients. Lancet 1983; i: 1010-13.
124. Brandt MR, Fernando A, Mordhorst R, Kehlet AH. Epiduralanalgesia improves postoperative nitrogen balance. Br MedJ 1978; i: 1106-8.
125. Shaw JHF, Galler L, Holdaway 1M, Holdaway CM. The effect ofextradural blockage upon glucose and urea kinetics in surgicalpatients. Surg Gynecol Obstet 1987; 16S: 260-6.
126. Wilmore DW, Long JM, Mason AD Jr, Skeen RW, Pruitt BA Jr.Catecholamines: mediators of the hypermetabolic response tothermal injury. Ann Surg 1974; 180: 653-69.
127. Shaw JHF, Holdaway CM, Humberstone DA. Metabolic inter-vention in surgical patients: the effec"ts of alpha- or beta-blockade on glucose and protein metabolism in surgical patientsreceiving total parenteral nutrition. Surgery 1988; 103: 520-5.
128. Hasse]gren P, Ta]amini M, LaFrance R, James JH, Peters JC,Fischer JE. Effect of indomethacin on proteolysis in septicmuscle. Ann Surg 1985; 202: 557-62.
129. Clark AS, Kelly RA, Mitch WE. Systemic response to thermalinjury in rats: accelerated protein degradation and alteredglucose utilization in muscle. J Clin lnvest 1984; 74: 888-97.
130. Woolfson AMJ, Heatly RJ, Allison SP. Insulin to inhibit proteincatabolism after injury. N Engl J Med 1979; 300: 14-17.
131. Macfie J, Yu]e AG, Hill GL. Effect of added insulin on bodycomposition of gastroenterologic patients receiving intravenousnutrition-a controlled clinical trial. Gastroemerology 1981; 81:285-9.
132. Tweedle D, Walton C, Johnston IDA. The effect of an anabolicsteroid on post-operative nitrogen balance. Br J Clin Pract 1973;27: 130-2.
133. Yule AG, Macfie J, Hill GL. Theeffect of an anabolic steroid onbody composition in patients receiving intravenous nutrition.Aust N Z J Surg 1981; SI: 280-4.
134. Prudden JF, Pearson E, Soroff H. Studies on gro"'th hormone.The effect on the nitrogen metabolism of severe]y burnedpatients. Surg G}'necol Obstet 1956; 102: 695-701.
135. Wilmore DW, Moylan JA, BristowBF,Mason AD, Pruitt BA.Anabo]ic effects of human growth hormone and high caloricfeedings following thermal injury. Surg Gynecol Obstet 1974; 138:875-84.
136. Liljedah] S-O, Gemzell C-A, Platin L-O, Birke G. Effect ofgrowth hormone in patients with severe burns. Acta Chir Scand1961; 122: 1-14.
137. Ward HC, Halliday D, Sim AJW. Protein and energy metab-o]ism with biosynthetic human growth hormone after gastro-intestina] surgery. Ann Surg ]987; 206: 56-6].
90. Threlfall CJ, Stoner HB, Galasko CSB. Patterns in the excretionof muscle markers alter trauma and orthopaedic surgery.J Trauma 1981; 21: 140-7.
91. Williamson DH, Farrell R, Kerr A, Smith R. Muscle proteincatabolism alter injury in man, as measured by urinary excretionof 3-methylhistidine. Clin Sci 1977; 52: 527-33.
92. Rennie MJ, Millward DJ. 3-methylhistidine excretion andurinary 3-methylhistidinejcreatinine ratio are poor indicators ofskeletal muscle breakdown. Clin Sci 1983; 65: 217-25.
93. Ballard FJ, Tomas FM. 3-Methylhistidine as a measure ofskeletal muscle protein breakdown in human subjects: the casefor its continued use. Clin Sci 1983; 65: 209-15.
94. Threlfall CJ, Maxwell AR, Stoner HB. Post-traumaticcreatinuria, J Trauma 1984; 24: 516-23.
95. Rennie MJ. Muscle protein turnover and the wasting due toinjury and disease. Br Med Bu111985; 41: 257-64.
96. Bergstrom J. Muscle electrolytes in mano Scand J Clin Lab Invest1962; 14 (Suppl): 1-110.
97. Askanazi J, Furst P, Michelson CB et al. Muscle and plasmaamino acids alter injury: hypocaloric glucose vs amino acidinfusion. Ann Surg 1980; 191: 465-72.
98. Askanazi J, Elwyn DH, Kinney JM et al. Muscle and plasmaamino acids alter injury: the role of inactivity. Ann Surg 1978;188: 797-803.
99. Kurst P, Bergstrom J, Chao 1 et al. InfIuence of amino acidsupply on nitrogen and amino acid metabolism in severe trauma.Acta Chir Scand (suppl) 1979; 494: 136-8.
100. O'Donnell JF, CJowes GHA, Blackburn GL et al. Proteolysisassociated with a deticit of peripheral energy fuel substrates inseptic mano Surgery 1976; 80: 192-200.
101. Van Gool J, Boers W, Ladiges NCJ. Glucocorticoids andcátecholamines as mediators of acute-phase proteins, especiallyrat alpha-macrofoetoprotein. Biochem J 1984; 220: 125-32.
102. Fleck A, Colley CM, Myers MA. Liver export proteins andtrauma. Br Med Bu1l1985; 41: 265-73.
103. Rosenblatt S, Clowes GHA, George BC, Hirsch E, Lindberg B.Exchange of amino acids by muscle and liver in sepsis. Arch Surg1983; 118: 167-75.
104. Cameron DE, Chaudry IH, Schleck S, Baue AE. Hepatocellulardysfunction in early sepsis despite increased hepatic blood fIow.Adv Shock Res 1981; 6: 65-74.
105. Ciernen s MG, Chaudry IH, Dermott P, Baue AE. Depressedhepatic oxidative capability, gluconeogenesis and alpha-adrenergic sensitivity in late sepsis. Circ Shock 1981; 8: 205~10.
106. Pedersen P, Seeman T, Hasselgren P. Protein synthesis anddegradation in liver tissue following induction of septic periton-itis in rats. Acta Chir Scand 1986; 152: 29-34.
107. Clowes GHA, George BC, Villee CA, Sara vis CA. Muscleproteolysis induced by a circulating peptide in patients withsepsis or trauma. N Engl J .~fed 1983; 308: 545-52.
108. Shaw JHF, Wolfe RR. Metabolic intervention in surgicalpatients: an assessment of the efTect of somatostatin, ranitidine,naloxone, diclophenac, dipyridamole or salbutamol infusion onenergy and protein kinetics in surgical patients using stable andradioisotopes. Ann Surg 1988; 207: 274-82.
109. Bernheim HA, Block LH, Atkins E. Fever; pathogenesis,pathophysiology and purpose. Ann Intern Med 1979; 91: 261-70.
110. Baracos V, Rodemann P, Dinarello CA, Goldberg AL. Stimu-lation of muscle protein degradation and prostacyclin El byleukocyte pyrogen (interleukin-I). ."J Engl J Med 1983; 308:553-8.
111. Sztein MB, Vogel SN, Sipe JO et al. The role ofmacrophages inthe acute phase response: SAA inducer is closely related toIymphocyte activating factor and endogenous pyrogen. CellImmunol1981; 63: 164-76.
112. Loda M, Clowes GHA, Oinarello CA, George BC, Lane B,Richardson W. Induction of hepatic protein synthesis by a pep-ti de in blood plasma of patients with sepsis and trauma. Surgery1984; 96: 204-13.
113. Kudsk KA, Stone JM, Sheldon FGF. Nutrition in trauma andburns. Surg Clin North Am J983; 62: 183-92. Paper accepted 8 September 1988
Br. J. Surg.. Vol. 76. No. 2. February 1989122