Embed Size (px)
Citation preview

Companion animal praCtiCe
150 In Practice April 2010 | Volume 32 | 150–155
Cytological examination of the lower respiratory tract in dogs and cats
John Dunn
doi:10.1136/inp.c1433
John Dunn graduated from the Royal (Dick) School of Veterinary Studies. He spent five years at the University of Saskatchewan, Canada, where he completed a master’s degree in small animal medicine, after which he worked as a lecturer in small animal medicine and clinical pathology at Cambridge. He is a diplomate of the European Colleges of Veterinary Internal Medicine and Veterinary Clinical Pathology. He is currently senior clinical pathologist at Axiom Veterinary Laboratories in South Devon.
Cytological examination of tracheal wash or bronchoalveolar lavage samples offers a convenient means of diagnosing inflammatory, infectious and, to a lesser extent, neoplastic disorders involving the lower respiratory tract of dogs and cats. Both procedures are relatively safe and easy to perform, and are minimally invasive. This article outlines the techniques for obtaining quality cytological specimens from the lower respiratory tract and describes basic interpretation of cytological findings, which should take into account the history, clinical findings and any radiographic abnormalities that may be present. It is also important to recognise when a sample is non-representative (eg, one that is contaminated by oropharyngeal material during collection) in order to avoid misleading cytological interpretation and culture results.
Collection techniques
Cytological examination of the respiratory tract involves analysis of samples obtained from a tracheal wash (TW) and/or bronchoalveolar lavage (BAL). Cytology samples should be collected into an EDTA tube. If bacteriology is required, a second sample should be collected into a sterile plain glass or plastic tube as EDTA has bacteriostatic properties.
TW and BAL collect material from the tracheo-bronchial tree. Interstitial lesions, therefore, may not be diagnosed. Transthoracic fine-needle aspiration (see box on page 151) may be a more appropriate tech-nique for the investigation of interstitial masses identi-fied by radiography or ultrasonography.
The main indication for TW and BAL is when there is radiographic evidence of tracheobronchial or pul-monary disease resulting in a chronic cough or res-piratory distress. It may be useful to perform a full cardiological investigation beforehand to exclude cardiogenic causes for the respiratory signs or radio-graphic lesions observed. TW and BAL are useful techniques for diagnosing hypersensitivity reactions, inflammation/infection (eg, bacteria, fungi, parasitic larvae and protozoa) and neoplasia.
TW and BAL both induce a neutrophilic inflam-matory response that peaks around 24 hours after the wash. If a sample is not of diagnostic quality the proce-dure should either be repeated immediately or after 48 hours, as any wash-induced inflammatory changes may complicate cytological interpretation.
Potential complications arising from TW and BAL are rare, but include subcutaneous emphysema, pneumo mediastinum, haemorrhage, hypoxia and nee-dle tract infection.
Tracheal washTW is easier to perform in large dogs and usually does not require anaesthesia, so the cough reflex remains intact (light sedation may be necessary in small dogs and cats). The sample is less likely to be contaminated by oropharyngeal material.
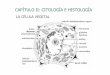
techniqueClip and aseptically prepare the skin. Infiltrate the subcutaneous tissue with local anaesthetic and insert the needle through the cricothyroid ligament (use an 18 gauge jugular catheter or 14 gauge needle with a 3·5 French gauge urinary catheter). Flush 1 to 2 ml of saline/5 kg and aspirate immediately. The use of
Tracheal wash. Insert an 18 gauge jugular catheter or a 14 gauge needle with a 3·5 French gauge urinary catheter through the cricothyroid ligament. Flush 1 to 2 ml of saline/5 kg through the catheter and aspirate immediately. (Reproduced, with permission, from Cowell and others 1999)
150-155 Cytology.indd 150 31/3/10 10:01:57

Companion animal praCtiCe
151In Practice April 2010 | Volume 32 | 150–155
1 to 2 ml of saline/5 kg and aspirate immediately. A larger volume of saline (eg, 1 to 3 ml/kg) may help to negate the dead space in the catheter, which may be a significant factor, particularly in small animals (use of a smaller volume of saline may result in a hypo- or acellular BAL).
Bronchial washings can also be collected through a rigid or fibre-optic bronchoscope. This allows visuali-sation of the bronchi and different collection sites, and biopsies can also be collected if necessary.
Cytological evaluation
Total and differential cell counts are of little diagnos-tic significance. The cells should be concentrated by centrifugation (five minutes at 1000 to 1500 rpm) and the sediment resuspended in a drop of supernatant. Prepare the smear using line smear concentration or
warmed saline may help to prevent airway constric-tion during sampling. The aspirated fluid should be collected into EDTA (for cytology) and sterile plain (for bacteriology) tubes. A gauze wrap applied over the puncture site may help to prevent the formation of subcutaneous emphysema.
Bronchoalveolar lavageBAL is the preferred technique for collecting cytology samples in small dogs and cats. BAL is more reliable than TW for obtaining diagnostic material from the lower airways. The drawbacks are that general anaes-thesia is required and that there is a greater risk of oropharyngeal contamination of the sample. If pos-sible, the depth of anaesthesia should be such that it does not inhibit the cough reflex. The endotracheal tube should be passed directly into the trachea avoid-ing contact with the oropharynx and arytenoid carti-lage in order to minimise pharyngeal contamination.
techniquePass a long 14 gauge urinary catheter down the endotra-cheal tube (note that the catheter must be longer than the endotracheal tube by at least 5 to 7·5 cm). Flush
Bronchoalveolar lavage (BAL). Under general anaesthesia, pass a 14 gauge urinary catheter through the endotracheal tube and flush 1 to 2 ml saline/5 kg and aspirate immediately. The technique can be performed through a rigid or fibre-optic endoscope, which allows visualisation of collection sites. (Reproduced, with permission, from Cowell and others 1999)
Mucus stains as an eosinophilic background deposit and can have a ‘fern-like’ appearance on direct smears. Increased amounts of mucus can be seen in cases of inflammation or infection. Wright’s Giemsa stain, magnification x100
Curschmann’s spirals are thought to be casts of inspissated mucus from small bronchioles and can be seen in any lower airway disease resulting in the excessive production of mucus. Wright’s Giemsa stain, magnification x100
Transthoracic fine-needle aspiration
Transthoracic fine-needle aspiration may be a more useful technique for the investigation of discrete and, to a lesser extent, diffuse interstitial lesions, particularly if the mass is located adjacent to the thoracic wall.
Fine-needle aspiration of the lung may potentially give rise to more complications, particularly pulmonary laceration, haemorrhage and pneumothorax. The technique can be performed with the animal standing or in sternal recumbency, and should preferably be carried out under ultrasound guidance. Sedation may be required if the animal is struggling or showing signs of severe respiratory distress.
Local anaesthetic is injected into the anterior edge of the intercostal space immediately caudal to the rib. With diffuse interstitial lesions, the right diaphragmatic lung lobe is generally aspirated between the seventh and ninth ribs, one-third of the distance down from the vertebral bodies to the costochondral junction.
In the case of discrete masses, if ultrasound is unavailable, the lesion is located from at least two radiographic views. Lesions close to the thoracic wall may be aspirated using a 22 to 25 gauge x 5 cm needle attached to a 5 or 10 ml syringe; deeper lesions may require a longer 22 gauge spinal needle to reach the site of interest. The needle is inserted through the costochondral space at a 90° angle to the thoracic wall. Once the thoracic cavity has been entered, negative pressure is applied to the syringe and the needle is advanced into the lesion. The chances of obtaining an adequate sample are maximised if the needle is withdrawn and advanced two or three times in a slightly different direction while maintaining negative pressure at all times. The needle is then withdrawn and the negative pressure released just before the needle exits the thoracic cavity. Only a small amount of material may be present in the needle or the hub of the syringe and this should be expelled onto a glass slide after detaching the syringe from the needle and filling it with air. A smear is prepared in the usual way (fluid samples are handled in a manner similar to that described for TW or BAL).
150-155 Cytology.indd 151 31/3/10 10:01:58

Companion animal praCtiCe
152 In Practice April 2010 | Volume 32 | 150–155
Increased numbers of goblet cells can be seen with conditions resulting in chronic airway irritation and overproduction of mucus (eg, chronic bronchitis and feline bronchial asthma).
alveolar macrophagesAlveolar macrophages may be the predominant cell type found in TW/BAL samples from clinically normal animals. The cytoplasm becomes vacuolated and may contain phagocytosed debris when these cells become activated.
neutrophilsNeutrophils normally constitute less than 5 per cent of the total nucleated cell population. Increased num-bers are seen in cases of inflammation, infection or tissue necrosis (a variable number of macrophages may also be present). The presence of neutrophils showing degenerative changes is more indicative of bacterial infection or tissue necrosis.
eosinophilsEosinophils are normally present in very low numbers (<5 per cent of the total nucleated cell population) in dogs but the figure may be as high as 20 per cent in some apparently healthy cats. An increased number of eosinophils with variable numbers of neutrophils and macrophages may be seen in the case of hypersensitiv-ity reactions or parasitism (lymphocytes, plasma cells
blood film techniques. A squash preparation may be helpful if the wash contains flocculent tissue flecks.
MucusMost washes contain a small amount of mucus that stains as an eosinophilic background deposit. Increased amounts of mucus may be expected with inflam-mation or infection. Mucus can assume a ‘fern-like’ appearance on direct smears. Curschmann’s spirals are casts of inspissated mucus from the small bronchi-oles and are frequently seen in conditions resulting in the excessive production of mucus.
Normal cell typesKnowledge of the normal cellular elements is essential in order to appreciate abnormal cytological patterns.
epithelial cellsCiliated columnar epithelial cells line the trachea and bronchi and often appear poorly preserved. Ciliated and non-ciliated cuboidal epithelial cells line the bronchioles and may be present as single cells or clusters. If viewed end-on, the ciliated and columnar/cuboidal features of these cells may be difficult to appreciate.
Goblet cellsGoblet cells are mucus-producing bronchial cells and contain large deeply basophilic mucin granules.
Goblet cells are mucus-producing bronchial cells and may be seen in increased numbers in the presence of conditions causing chronic airway irritation and producing excessive mucus. Wright’s Giemsa stain, magnification x500
Ciliated columnar epithelial cells line the trachea and bronchi. Wright’s Giemsa stain, magnification x1000
Cuboidal epithelial cells line the bronchioles and are often arranged in clusters. Wright’s Giemsa stain, magnification x1000
The presence of superficial squamous epithelial cells (arrowhead) in a TW or BAL sample indicates oropharyngeal contamination. Numerous ciliated columnar epithelial cells and one goblet cell (arrow) can also be seen. Wright’s Giemsa stain, magnification x500
150-155 Cytology.indd 152 31/3/10 10:01:59

Companion animal praCtiCe
153In Practice April 2010 | Volume 32 | 150–155
either a granulomatous or pyogranulomatous inflam-matory response. The latter is characterised by an increased number of reactive alveolar macrophages and a variable number of neutrophils. Lymphocytes, plasma cells and eosinophils may be present in low numbers. A granulomatous inflammatory response is characterised by an increased number of reactive epithelioid macrophages. Large multinucleated giant cells may also be present.
BAL cytology from dogs and cats with chronic bronchitis tends to be less specific. The inflammatory response may be relatively mild and there may be evi-dence of increased mucus production. The distribu-
and mast cells may also be present in low numbers). Some eosinophils may appear morphologically atypi-cal, with the nucleus being round or oval-shaped rather than segmented.
lymphocytesLymphocytes are present in low numbers in normal dogs and cats (5 to 14 per cent). Increased numbers can be seen in patients with airway hypersensitivity and in response to antigenic stimulation (eg, viral diseases and chronic infections). Some lymphocytes may trans-form into plasma cells.
mast cellsMast cells are rarely seen in TW/BAL samples from healthy dogs and cats (less than 2 per cent of the total nucleated cell population). The number may be slightly increased in the case of some hypersensitivity reactions.
Inflammation
neutrophilic inflammationPossible causes of a neutrophilic (purulent) inflam-matory response include tracheobronchitis (eg, ken-nel cough), bronchopneumonia, inhaled bronchial/pulmonary foreign bodies, aspiration pneumonia, a pulmonary abscess or a large necrotic tumour (eg, pri-mary lung tumours involving a single lung lobe).
Mycobacterial infections (especially in cats) and mycotic or protozoal infections most frequently elicit
BAL sample consisting of a large number of reactive alveolar macrophages. Pyogranulomatous or granulomatous inflammation is a feature of myobacterial, fungal or protozoal infections. Variable numbers of neutrophils, lymphocytes, plasma cells, eosinophils and large multinucleated giant cells may also be seen. Wright’s Giemsa stain, magnification x1000
(left) BAL sample consisting of a large number of degenerate neutrophils. Wright’s Giemsa stain, magnification x500. (right) Many of these contain ingested bacterial organisms. Wright’s Giemsa stain, magnification x1000. This cytological appearance is consistent with bronchopneumonia
(left) Cluster of epithelioid macrophages in a BAL sample from a cat containing thin negative-staining mycobacterial organisms. Wright’s Giemsa stain, magnification x500. (right) These stain acid-fast positive with Ziehl-Neelsen stain. Magnification x500
150-155 Cytology.indd 153 31/3/10 10:02:01

Companion animal praCtiCe
154 In Practice April 2010 | Volume 32 | 150–155
tion of nucleated cells is more consistent with a chronic active or mixed inflammatory response, although in many cases macrophages may predominate.
eosinophilic inflammationAs a general guideline, an inflammatory response is considered to have a significant eosinophilic com-ponent if the number of eosinophils is greater than 10 per cent of the total nucleated cell population. In some cases, the number of mast cells may also be slightly increased. Differential diagnoses include feline bronchial asthma and pulmonary infiltrate with eosinophils, which includes allergic bronchitis, eosinophilic bronchopneumonia, pulmonary eosino-philic granuloma associated with Dirofilaria immitis infection, and neoplasia (eg, lymphomas, mast cell tumours). Parasit ism (eg, involving Oslerus osleri, Angio strongylus vasorum, Crenosoma vulpis and Aelurostrongylus abstrusus [cats]) also frequently elicits an eosinophilic response.
Intrapulmonary haemorrhageThe presence of macrophages containing red blood cells or haemoglobin breakdown products, such as haemosiderin (haemosiderophages) or haematoidin crystals, indicates previous intrapulmonary haemor-rhage. Possible causes include trauma, the presence of a pulmonary foreign body, infectious (bacterial, fungal, protozoal or parasitic) diseases, lung lobe tor-
sion, feline bronchial asthma, congestive heart failure, pulmonary thromboembolism, coagulopathies (eg, dicoumarol toxicity) or primary/metastatic neoplasia.
Oropharyngeal contaminationThe presence of superficial squamous epithelial cells in a TW or BAL sample indicates oropharyngeal con-tamination. Bacteria (eg, Simonsiella species) often adhere to the surface of these cells. A variable number of neutrophils may also be present.
(left) Haemosiderophages are macrophages that contain phagocytosed haemoglobin breakdown products such as haemosiderin or haematoidin crystals. Wright’s Giemsa stain, magnification x1000. (right) Haemosiderin stains as bluish-black material with Prussian blue stain. Magnification x500
(left) Eosinophilic inflammation is usually diagnosed when the number of eosinophils is greater than 10 per cent of the total nucleated cell population (although this figure may be as high as 20 per cent in some apparently healthy cats). There may be evidence of secondary bacterial infection. Wright’s Giemsa stain, magnification x500. (right) Significant numbers of degenerate neutrophils and intra- and extracellular bacteria can be seen. Wright’s Giemsa stain, magnification x1000
Oropharyngeal contamination. Superficial squamous epithelial cells are often covered with bacterial organisms (eg, Simonsiella species), seen here as large bullet-shaped striated organisms. Wright’s Giemsa stain, magnification x500
Simonsiella species
150-155 Cytology.indd 154 31/3/10 10:02:02

Companion animal praCtiCe
155In Practice April 2010 | Volume 32 | 150–155
Atypical cell types
Dysplastic epithelial cellsColumnar and cuboidal epithelial cells can become dysplastic in response to inflammation or chronic irritating stimuli (eg, dust, smoke). Chemotherapy can also induce severe dysplastic changes. It may be difficult to differentiate between dysplastic and neoplastic cells.
Squamous metaplasiaNormal columnar or cuboidal epithelial cells may be replaced by stratified squamous epithelial cells, which represent an adaptive response to chronic inflamma-tion or irritation.
primary or metastatic neoplasiaPrimary lung tumours and lymphosarcomas are more likely to involve the bronchial tree and, as a result, may exfoliate cells in TW or BAL samples. In contrast, metastatic lung tumours tend to produce interstitial lesions and neoplastic cells are rarely seen. Fine-needle
Pulmonary carcinoma in a dog. Tumours involving the bronchial tree (eg, primary pulmonary carcinomas or bronchial carcinomas) are more likely to exfoliate cells in BAL samples. The cells present in this BAL sample are showing obvious morphological features of malignancy, which include anisocytosis, anisokaryosis, variation in nuclear:cytoplasmic ratio and also variation in the size, shape and number of nucleoli within each nucleus. Wright’s Giemsa stain, magnification x1000
aspiration cytology of discrete pulmonary masses may be more rewarding in many cases where pulmonary neoplasia is suspected.
Further readingVILLIERS, E. & BLACKWOOD, L. (2005) Manual of Small Animal Clinical Pathology, 2nd edn. Quedgeley, BSAVA PublicationsBAKER, R. & LUMSDEN, J. H. (2000) Colour Atlas of Cytology of the Dog and Cat. Missouri, MosbyCOWELL, R. L., TYLER, R. D. & MEINKOTH, J. H. (1999) Diagnostic Cytology of the Dog and Cat, 2nd edn. Missouri, MosbyRASKIN. R. E. & MEYER, D. J. (2001) Atlas of Canine and Feline Cytology. Philadelphia, W. B. SaundersFOURNEL-FLEURY, C., MAGNOL, J. & GUELFI, J. (1994) Colour Atlas of Cancer Cytology of the Dog and Cat. Paris, Conférence Nationale des Vétérinaires Spécialisés en Petits Animaux
First larval stage of metastrongyle species in a BAL sample from a five-year-old Irish setter. Wright’s Giemsa stain, magnification x100
150-155 Cytology.indd 155 31/3/10 10:02:04