Embed Size (px)
Citation preview

Circulation of the GiraffeBy EOBERT H. GOETZ, M.D., JAMES V. WARREN, M.D., OTTO II. GAUER, M.D.,
JOHN L. PATTERSON, JR. , M.D., JOSEPH T. DOYLE, M.D., E. N. KEEN, M.D.,
AND MAURICE MCGREGOR, M.D.
With the technical assistance of L. M. Tiller, M. Smith and E. Mance
THE long neck of the giraffe presents aunique problem in the regulation of the
systemic arterial blood pressure and in themaintenance of the cerebral circulation. In1954, Goetz and Budtz-Olsen succeeded inmeasuring the arterial blood pressure in astanding, unanesthetized giraffe.1'2 In thisanimal, approximately 13 feet tall, the carotidarterial mean pressure was found to be 200mm. Hg at the base of the brain. The presentstudy was undertaken 2 years later as asequel to this preliminary observation to pro-vide detailed information concerning the cir-culation of the giraffe. Concomitant studiesof respiratory function will be reportedseparately.
MethodIn January, 1956, 4 wild giraffes, about 2 years
of age, were captured and confined to a stockadeon the Hans Merensky Farm, Northern Transvaal,Union of South Africa. The 3 largest animalswere kept together; the fourth, the victim ofmultiple cutaneous tumors of low grade malig-nancy and of unknown identity, was penned sepa-rately. The animals were fed their usual her-bivorous diet and, with the exception of the sickgiraffe, appeared healthy. None of the animalsbecame entirely tame. At the time of the study,in October, 1956, the 3 larger animals ranged inheight from 12 to 13 feet, whereas the small onewas only 9 feet tall.
For physiologic study, the giraffe was lured
From the Department of Surgery, Albert EinsteinCollege of Medicine, Yeshiva University, New York,N. Y.
Supported by grunts received from the U. S. Officeof Naval Research, Contract no. Nonr. 1153(00),Washington, D. C.; the National Heart Institute,National Institutes of Health, U. S. Public HealthService (H-1217); the South African Council forScientific and Industrial Research, Pretoria; theDeutsche Forschungs Gemoinschaft, Bad-Godesberg,Germany; and the New York Heart Association, N. Y.
Received for publication June 3, 1960.
and driven into a narrow chute or "crush pen".When the gate to the chute was closed, the animalcould move neither forward nor backward. Aftera blindfold and a halter had been applied, theanimal could be led into a latticework of 3-inchsteel pipes firmly imbedded in the ground.3 Thegiraffe was secured in the standing position byhobbling the feet to the pipes and by placing aleather sling under the abdomen to prevent theanimal from lying down. The head was controlledby 2 men positioned on the scaffolding at headlevel. The clamps which secured the pipes couldbe easily released so that the anesthetized animalcould be rapidly lowered to the lateral decubitus.
Needle electrodes were inserted into the skinover the shoulders and a third into the neck forelectrocardiographic monitoring.
The jugular vein and the carotid artery wereexposed through a generous incision made alongthe lateral border of the sternohyoid muscle about50 cm. above the juguluin. Xylocain (lidocaine)was used for local anesthesia. Since the skin isabout 1.5 cm. thick in this region, a linoleumcutter was required to effect the cutdown. At thislevel in the neck the jugular vein was found to beabout 2.5 cm. in diameter and in a state of col-lapse ; the diameter of the carotid artery was about1.2 cm. Bleeding from tiny arteries was difficultto control because of the,high intraluminal pressure.
In each animal an extra-long woven nyloncatheter (240 cm.) was passed centrally throughthe isolated jugular vein. The pulmonary arterycould be catheterized in 2 animals by blindlyadvancing the catheter. In the other 2 animalsthe catheter tip could not be passed beyond theright ventricle. A cannula was inserted, into thecarotid artery for blood samplings. Intravasoularpressures were measured from this cannula orfrom nos. 90 or 60 polyethylene tubing attachedto Statham P23D or P23G strain gages placedin most cases at the level of the incision.
In each animal venous eatheterization waseffected both with a single and a double lumencatheter, 1 lumen of which carried at its tip amodified Wetterer miniature manometer.4 The useof this type of manometer permitted direct measure-ment of pressures at heart level. In 2 animals,a catheter of this latter type was also passedfrom the carotid artery into the aorta and into
Circulation Research, Volume VIII, September 1960 1049
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

1050 GOETZ, ET AL.
the left ventricle without incident. Pressures andelectrocardiograms were recorded simultaneouslyon a Sanborn M-150 direct-writing polyoscillographor optically with Heiland Type G galvanometersand a camera housed in a light-tight prefabri-cated shack.
The pressures recorded at heart level were cor-rected to brain level by subtracting a hydrostaticcorrection calculated with the assumption that thespecific gravity of giraffe blood is not significantlydifferent from man:
Hydrostatic correction = 1.055 X cm. elevation(mm.Hg) L36
The cardiac output was measured, utilizing theFick principle and the indicator-dilution method,in all animals using T 1824.n- 6 The dye was in-jected through the cardiac catheter. Arterial bloodsamples were collected in heparinized tubes at 1-second intervals. Subsequently at intervals up to30 minutes blood samples were obtained for esti-mation' of the general blood volume. The dyeconcentration of the plasma was read on a ColemanJunior spectrophotometer. The mean dye con-centration, the mean circulation time, the cardiacoutput and the central blood volume were obtainedfrom the time-concentration dye curve and thehematoerit reading and the total blood volume byextrapolating the dye disappearance curve back tozero. The high environmental temperature causedhemolysis in a number of the blood samples.
Arterial and venous blood samples were collectedanaerobically for the measurement of oxygen con-tent by a modified Haldane method, for directoxygen and carbon dioxide tensions and for bloodpH with the Beckman Model G pH-meter. Expiredgas samples were analyzed for O.< and C02 con-centration with the Scholander Microgasanalyzer.Oxygen consumption was measured by the open-circuit method. Expired gas was collected with aSpecially constructed mask for periods of 2 to 3minutes. Pulmonary blood flow (cardiac output)was calculated from the oxygen consumption andthe arterio-mixed venous blood oxygen difference.
After initial observations general anesthesia wasinduced in the fourth animal by injecting sodiumthial-barbital (Kemithal) through the cardiaccatheter. Prior to this the animal had been given500 mg. chlorpromazine intravenously in an un-successful effort to reduce struggling.
ResultsOnce confined in the steel scaffolding the
giraffe remained quiet and apparently calmfor periods as long as 10 or 15 minutes. Theanimal would then, for a moment and atirregular intervals, buck and thrash about."' The first and largest animal was immo-
bilized only with great difficulty; the dissec-tion was long and difficult; the day wasextremely hot, and the animal bucked repeat-edly and violently, each time apparentlyaggravating a severe angulation of the neck.After 4 hours the animal began to show signsof respiratory distress, the muzzle becamepale, and during the injection of T-1824 dye,it suddenly collapsed and died. The dyesamples were visually evaluated because of thesmall volume of individual blood samples. Thetimes from onset and from midpoint of thedjre injection to the peak concentration were4 to 6 seconds, respectively. This rapid circu-lation rate suggested that the animal's hypo-tension resulted from vasodilatation ratherthan from inadequate cardiac action.7 It is,therefore, possible that the animal developedorthostatic syncope, irreversible because ofits immobilization in the standing position.At autopsy the total weight of the disarticu-lated limbs, neck and body was 570 Kg.
Carotid Arterial Pressure
Technically satisfactory pressure tracingswere obtained both with the miniature ma-nometer and the Statham transducer usingPE 90 polyethylene tubing. The pulse con-tour was essentially the same. In each animal,except giraffe no. 3, a tall high-frequencyspike was recorded during the early ejectionphase followed by a domelike plateau preced-ing the incisura (fig. 1). With the rise insystolic blood pressure during struggling thisinitial spike decreased in height in animalno. 1 and completely disappeared in animalno. 2.
The intravascular pressure measurements(at heart level) are summarized in table 1.As it was felt that the initial spike contrib-uted little to the mean pressures, the pres-sures are recorded by 3 readings. The firstrefers to the initial spike, the second to theplateau or dome following the spike and thethird to the end diastolic pressure (fig. 1).In all 4 animals the arterial pressure wasextraordinarily high as judged by humanstandards. Even in the smallest animal whichwas not quite 9 feet tall the arterial pressure
Circtilation Research, Volume VIII, September 1960
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

CIRCULATION OF GIRAFFE 1051
1 *l-l\\1 '
Figure 1Catheterization of right heart in the standing nonanesthetieed giraffe with miniaturemanometer. Pressures in right atrium (A) and right ventricle (B) simultaneously re-corded with arterial pressure in carotid artery and electrocardiogram. (C) Changes incarotd artery and right ventricular pressure on lowering the head for 150 cm. Notethe increase in the short initial spike and the lowering of the mean pressure in thecarotid artery.
was not much lower than in the larger ani-mals. The highest systolic pressure recordedin a quiet animal was 353 mm. Hg and thehighest diastolic pressure 303 mm. Hg. Exceptfor the pressure taken before the syncope ingiraffe no. 1, the lowest recorded pressuresin a standing healthy animal were 260 mm.Hg systolic and 158 mm. Hg diastolic. Inthe calm, standing animal, the pressures variedrelatively little, but on struggling, both thesystolic and diastolic pressures often rose bymore than 100 mm. Hg. The arterial bloodpressure in 1 anesthetized giraffe in thelateral decubitus was 262/225/188 mm. Hg.Pulse Wave Velocity
The velocity of the arterial pulse wave wascalculated in 1 standing and 1 anesthetizedrecumbent animal from a pressure recordingmade during the withdrawal of the minia-ture manometer for a measured distance fromthe left ventricle to the carotid artery, usingthe electrocardiogram as a reference point(fig. 2). In the standing giraffe the pulse
Circulation Research, Volume VIII, September 1960
wave velocity was about 5 M/second whereasin the anesthetized and recumbent animal itmeasured 4.0 M/second.Changes in Arterial Pressure Pattern
The changes in the arterial pressure patternrecorded with the miniature manometer dur-ing withdrawal from the left ventricle intothe carotid artery are illustrated in figure 3.The R waves of the electrocardiogram havebeen superimposed on the corresponding pres-sure pulses. An initial spike in the left ven-tricular pressure contour is noted. It is alsorecorded in the aortic pressure pulse imme-diately after the manometer passes throughthe aortic valve (A). As the distance fromthe aortic valve increases, this initial spikegradually disappears (B). As the manometeris further withdrawn a new pattern developswith a dip in pressure preceding systole anda progressively more prominent spike in earlysystole. This increases in height with increas-ing distance from the aorta (D). On furtheranalysis it appears that the initial peak in
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

1052 GOETZ, ET AL.
l|!lllllll!!l|lll!|lllllll|Mlillll"|IMilllllllli|||IMIIIIIII!llllllllllllllll!llll!l|l!l!l!Mllllllllllllll|iii|I i ' < i ! f I i i i •
I M I H I I I I I I I I I I M I M I
MMMlllMI' l
Figure 2Withdrawal of miniature manometer from tlie left ventricle via aorta and for 70 cm. alongthe carotid artery in a standing nnanesthetized giraffe. Pressure simultaneously recordedwith electrocardiogram. 'The electrocardiogram has been erased but for the li wave,as in the original record it teas superimposed over the pressure tracing. Time = 0.1second. A, B, C and I) refer to the pulses reproduced in figure 3.
(A) coincides witli a small presystolic dip in(C) and the systolic dip following the initialspike in (A) with the early systolic peak in(D).
The drop in diastolic pressure during with-drawal of the miniature manometer is prac-tically linear and uneventful.
Ventricular PressuresThe left ventricular pressure was measured
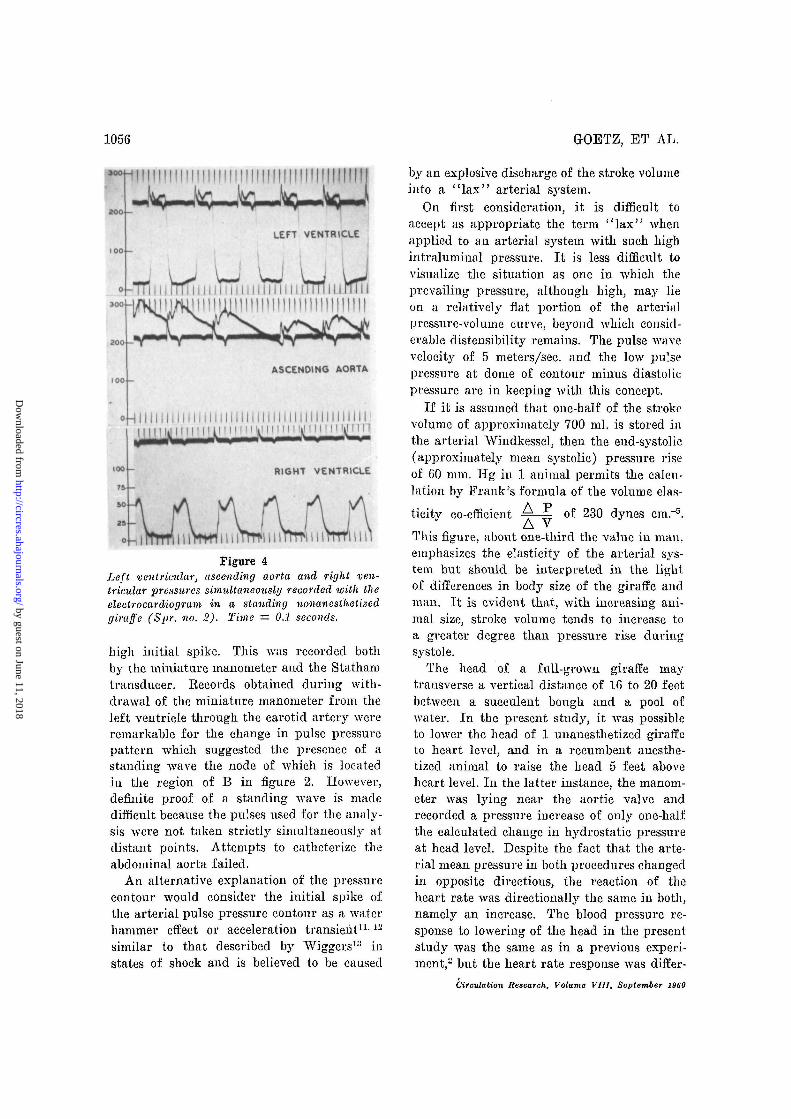
in 1 standing and in 1 recumbent giraffe byretrograde arterial catheterization with theminiature manometer. Atrial premature beatsoccurred regularly when the catheter trav-ersed the aortic A'alve. In the standing animalthe left ventricular systolic pressure variedbetween 260 to 286 mm. Hg and the enddiastolic pressure between 10 to 18 mm. Hg(fig. 4). The maximal rate of left ventricularpressure ascent was about 6,000 mm. Hg/sec.In the recumbent anesthetized small animal(no. 4) the left ventricular pressure was 170/0mm. Hg.
Right ventricular pressures were recordedin all 4 animals with the Statham transducerand in 2 with the miniature manometer. Theright ventricular systolic pressures variedbetween 40 and 75 mm. Hg and the enddiastolic pressures between 5 and 20 mm. Hg(figs. 1 and 4). Large fluctuations were pro-duced by respiration. The maximal rate ofpressure ascent in the right ventricle was1,200 mm. Hg per second.
The right ventricular pressure was alsorecorded with the miniature manometer asthe head was lowered in 1 giraffe (fig. 1).There was a marked increase in the respira-tory fluctuations with a maximum systolicfluctuation of 20 mm. Hg during inspiration.The end-diastolic pressure remained essen-tially the same.
Pulmonary Arterial Pressure
The pulmonary arterial pressure recordedin giraffe no. 3 varied between 38/13 mm.Hg and 48/22 mm. Hg. In this animal, itwas possible to eatheterize the right ventriclewith the miniature manometer and then ad-vance the catheter well into the pulmonaryartery. There was a drop in pressure as thecatheter passed through the valve, the gra-dient between systolic pressures in the 2 areasbeing 10 mm. Hg. In giraffe no. 2 the sameprocedure was followed, but the catheter tiplodged in the region of the pulmonic valveand the gradient and the pulmonic pressures,although apparently of comparable magni-tude to those found in giraffe no. 3, couldnot be determined with precision. Convincingpulmonary capillary venous pressures couldnot be obtained in any of the animals.
Central Venous Pressures
The right atrial pressure in 3 animals wasessentially atmospheric but varied greatlywith the phase of respiration (fig. 1). For
Circulation Research, Volume VIII, September 1960
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

CIRCULATION OF GIRAFFE 1053
Table 1Systemic Arterial Blood Pressure and Heart Rate in Four Conscious Standing Giraffes"
RitaNo. 1
SpogterNo. 2
SpriiigkiinnNo. 3
WisslossNo. 4
Pressure at heart level (mm. Hg)Animal calm Animal struggling
Psp/Ps/Pd
282/240/158to
340/285/220280/240/185
to353/315/240260/220/190
to353/340/303315/255/200
to330/270/210
Pmt
210to
265217to
285205to
325245to
255
Psp/Ps/Pd Pm323/310/250 285
to to384/360/284 325
350/385/300 322
Animal recumbentanesthetized
262/225/188 215
Brain levelMean pressure at
mm. HgAnimal calm
Pm
77to
13277to
15598to
208139to
149
Heartrate80to
10860to12560tono
60to75
*With exception of animal no. 4, column 2.tHighest and lowest readings are given of spike (Psp), systolic (Ps), end-diastolic pressures
(Pd) and Pm = mean pressure determined by planimetry.
technical reasons it was impossible to meas-ure the jugular venous pressure at head level.In the standing animal this vessel appearscollapsed. From the rapid filling on compres-sion it appears possible that the lumen stillhad an appreciable open cross section. How-ever, the existence of an open lumen in atruly collapsible external jugular vein is un-likely to produce a negative venous pressureat the base of the skull.8 As a syphon effectmay still be produced through the deep non-collapsible venous channels, it is believedthat at head level the venous pressure isprobably subatmospheric.
Cardiac OutputThe data are summarized in table 2. The
indicator-dilution procedure in giraffes nos.2 and 3 were technically satisfactory. Thecardiac output in these 2 animals compareswell with similar determinations in dairy cowsof about the same weight.9 From the dyecurves the circulation time and the generaland central blood volume were also available(table 2). The values for general blood vol-ume, when related to estimated body weight,are very much the same as in the cow.
Cardiac output determinations, utilizingthe Fick principle, were obtained in animalsnos. 2, 3 and 4. The agreement between dyeand Fick outputs in animal no. 3 was quite
Circulation Research, Volume VIII, September 1960
good but poor in the second animal dueto the time differences in blood, expired gasand dye sampling. It should be noted thatin animal no. 3 the mixed venous bloodsample was believed to have been obtainedfrom the right atrium. It is, therefore, pos-sible that this sample contained a relativelyhigh proportion of coronary sinus blood, whichwould have produced a falsely high mixedvenous-systemic arterial oxygen difference anda falsely low cardiac output. There was astriking fall in cardiac output in animal no.4 with change from the upright unanesthetizedto the recumbent anesthetized condition. Bothof the Fick determinations were done withgood correspondence of gas and blood sam-pling times and the results are regarded withconfidence.Heart Bate
Considering the size of the animal the heartrates were high in all animals. They variedgreatly, increasing rapidly whenever the ani-mal showed signs of restlessness. When theanimal appeared calm, the rate was about 60.The experimental conditions in blindfoldingand restraint must obviously be consideredwhen interpreting these data.Circulatory Effects of Changes in Posture
In 1 giraffe the arterial pressure was con-tinuously recorded while the head was force-
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

1054 GOETZ, ET AL.
» f ' I I f f !
i I I I 1 I I 1 1 1 1 1Figure 3
Changes in the arterial pressure pattern recordedduring withdraival of minature manometer fromleft ventricle along the carotid artery in a standingnonanesthetised giraffe (Spr. no. 2). At V themanometer was lying within the left ventricle.
ably lowered by 150 cm. (fig. 5). As thehead went down there occurred a markedincrease in the pulse pressure resulting froma rise in the systolic and a conspicuous fallin the diastolic pressures (fig. 1). The meanarterial pressure at heart level fell approxi-mately 50 mm. Hg. There was a concomitantrise iu heart rate from 65 to 105 beats perminute.
Of particular interest was the response ofthe aortic pressure in the anesthetized re-cumbent animal when the head was passivelyraised a distance of 150 cm. above heart levelas the minature manometer lay in the acend-ing aorta. As is shown in figure 6, there wasan immediate rise of 50 mm. Hg in systolicand of 60 mm. Hg in diastolic pressure. Thepulse pressure, therefore, decreased. Thispressure response was the exact opposite ofthat observed when the head was loweredbut the change iu heart rate was in the samedirection, i.e. there was an increase in heartrate with elevation of the head. The observedrise iu pressure of only 50 mm. Hg obvi-ously did not suffice to keep the pressure atbrain level constant since the calculatedhydrostatic increase in pressure at the rootof the aorta must have amounted to approxi-mately 110 mm. Hg.
DiscussionThe observations reported here must be
viewed in the light of the prevailing experi-mental conditions. Facilities were limited com-pared with an established laboratory, being300 miles from the nearest city, and trans-portation facilities were slow and irregular.Furthermore, the experiments were restrictedto the 4 anima'.s available, although studieson a larger series of animals clearly wouldhave been desirable.
The systemic arterial pressure of the giraffeis the highest of auj' animal thus far studied.Even the lowest pressure recorded in theseanimals, with the exception of the pre-syncopal pressure in 1, would be adequate
A, B, C and D refer to the respective pulses infigure 2. The arroios indicate the R wave of theelectrocardiogram. Time = 0.1 seconds.
Circulation Research, Volume V1I1, September 2960
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

CIRCULATION OF GIRAFFE 1055
Table 2Cardiac Output and Belated Functions
Animal
No. 2Spogter
No. 3Springkiiiui
No. 4Wissless
Cardiac outputL./min.«
Dye Fick
75t 39t
32t 22t
41121t
Systemicarterial
mixed venous0= dift.
ml./lOO ml.
10.8
10.4§
4.05.4
Circulationtimesec.
11
10
9 5||II
Generalblood
volumeL.
39.9
35.3
Centralblood
volume(Q)L.
13.9
8.4
Timeof componentsof procedures(hour of day)
Fickarterial andvenous bloodsamplesexpired gasdye
Fickvenous bloodexpired gasarterial bloodFick1
expired gasarterial bloodvenous bloodFick2
venous bloodexpired gasarterial blooddye
09.1011.3510.42
10.3010.4010.56
13.28 V213.2913.32
11.5211.52%11.5213.39'/i
"Bounded figures,t Standing and unanesthetized.tHecumbcnt and anesthetized.§Venous sample believed to have been right atrial.||Cardiac output for this indicator-dilution curve not given because syringe broke and some
dye lost.
to maintain perfusion of the brain withoutrecourse to any auxiliary mechanisms. Theblood pressure showed a minimal tendency tofall, even over the longest periods duringwhich the animal was quiet and not subjectedto manipulation. Recent observations on moretractable domestic cattle have demonstratedconsiderable fluctuations in A'ascular functionsrelated to environmental conditions.10 Of pos-sible relevance to the question of the effectof environmental influences is the recordingin 1 animal of almost identical diastolic pres-sures before and after general anesthesia. In-deed, the hydrostatic situation would prob-ably not permit a significant fall in peripheralresistance and in arterial pressure if an ade-quate cerebral perfusion pressure were to bemaintained. In. this respect the anatomicalstructure of the large vessels is perhaps ofconsiderable significance, with the arteriesbelow heart level showing greater muscularityand smaller lumens.3
The values obtained for cardiac output
Circulation Research, Volume VIII, September 1960
(table 2), while variable, are similar to thoseobtained in domestic cattle of about thesame weight. Despite technical difficulties,some confidence is gained for the outputvalues by the dye technic, in the case ofanimals nos. 2 and 3, by the reasonable valuesobtained for blood volume. Based on an esti-mated weight of 1,100 pounds (500 Kg.) foranimal no. 2 and 1,000 pounds (455 Kg.)for animal no. 3, the blood volumes of theseanimals represented, respectively, 73 and 78ml./Kg. body weight. The cardiac outputvalues for animal no. 4 are also viewed withconsiderable confidence, taking into accountthe temporal closeness of the blood and ex-pired gas samples, and the approximate agree-ment of the values for arteriovenous oxygendifference with those obtained in cattle.
Our data do not permit a precise analysisof the elastic state of the arterial system, butcertain phenomena provide a basis for specu-lation. The pressure contours in the left ven-tricle and in the carotid artery display a
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from
1056
»0O4—|
<4-7Tii300
LEFT VENTRICLE
i r T T T i i i i i i i i i i i i i i i i i i i i r T T T T 1 LArTTTi
ASCENDING AORTA
HII I I I I I I I I I I I I INI I I I I I I I IMI I I I I I I I IMI I I I 1
I M l Mil 11 M 111 i M 1111 i \ i H II11 t̂ t 111 It 11̂ 1 TI FT
RIGHT VENTRICLE
i i rftrn 11 iWt 111 mm 111WiFigure 4
Left ventricular, ascending aorta and right ven-tricular pressures simultaneously recorded with theelectrocardiogram in a standing nonanestlietizedgiraffe (Spr. no. 2). Time = 0.1 seconds.
high initial spike. This was recorded bothby the miniature manometer and the Stathamtransducer. Eecords obtained during with-drawal of the miniature manometer from theleft veutricle through tlie carotid artery wereremarkable for the change in pulse pressurepattern which suggested the presence of astanding wave the node of which is locatedin the region of B in figure 2. However,definite proof of a standing wave is madedifficult because the pulses used for the analy-sis were not taken strictly simultaneously atdistant points. Attempts to catheterize theabdominal aorta failed.
An alternative explanation of the pressurecontour would consider the initial spike ofthe arterial pulse pressure contour as a waterhammer effect or acceleration transient11-12
similar to that described by Wiggers1'1 instates of shock and is believed to be caused
GOETZ, ET Ah.
by an explosive discharge of the stroke volumeinto a " lax" arterial system.
On first consideration, it is difficult toaccept as appropriate the term "lax" whenapplied to an arterial system with such highintraluminal pressure. It is less difficult tovisualize the situation as one in which theprevailing pressure, although high, may lieon a relatively flat portion of the arterialpressure-volume curve, beyond which consid-erable distensibility remains. The pulse wavevelocity of 5 meters/sec, and the low pulsepressure at dome of contour minus diastolicpressure are in keeping with this concept.
If it is assumed that one-half of the strokevolume of approximately 700 ml. is stored intlie arterial Windkessel, then the end-systolic(approximately mean systolic) pressure riseof 60 mm. Tig in 1 animal permits the calcu-lation by Frank's formula of the volume elas-ticity co-efficient ^-^ of 230 dynes cm."5.
This figure, about one-third the value in man.emphasizes the elasticity of the arterial sys-tem but should be interpreted in the lightof differences in body size of the giraffe andman. It is evident that, with increasing ani-mal size, stroke volume tends to increase toa greater degree than pressure rise duringsystole.
The head of a full-grown giraffe maj'transverse a vertical distance of 16 to 20 feetbetween a succulent bough and a pool ofwater. In the present study, it Avas possibleto lower the head of 1 unanesthetized giraffeto heart level, and in a recumbent anesthe-tized animal to raise the head 5 feet aboveheart level. In the latter instance, the manom-eter was lying near the aortic valve andrecorded a pressure increase of only one-halfthe calculated change in hydrostatic pressureat head level. Despite the fact that the arte-rial mean pressure in both procedures changedin opposite directions, the reaction of theheart rate was direetionally the same in both,namely an increase. The blood pressure re-sponse to lowering of the head in the presentstudy was the same as in a previous experi-ment,2 but the heart rate response was differ-
Circulation Research, Volume VIII, September 1960
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

CIRCULATION OF OIRAPPE 1057
t HEAD GOING UP
Figure 5Blood pressure in the giraffe during lowering of head for 150 cm. Chart prepared fromcontinuous pressure recording by plotting the height of the initial spike and the systolicdome of each pulse (Wis. no. 4).
ent, inasmuch as a slowing of the heart ratehad been observed previously. The explana-tion perhaps lies in the fact that in theearlier study the animal voluntarily loweredits head in order to drink, whereas in the pres-ent study, the animal's head was loweredagainst its own will. The changes in heartrate are in any case small considering thelarge distance transversed by the head. Thisis in keeping with anatomical findings thatthe giraffe does not have a carotid sinus. Evenif it is considered that carotid sinus functionmay have been taken over by an occipitalsinus,14 reflex activity still appears to be atlow level. In this respect, the relatively highheart rates observed in these animals duringthe present and earlier investigations are ofconsiderable interest, although admittedly theenvironmental situation may have producedan elevation in the rate.
In the giraffe, there is a relatively greatdifference between the right ventricular andleft ventricular maximal rates of pressureascent, the left ventricular rate of ascentbeing 5 times that calculated for the rightventricle. This reflects a number of factors,of which the enormous thickness of the leftventricular musculature previously reportedis probably the main one, besides differencesin the resistances of the 2 major vascularbeds.
It is regrettable that the jugular venouspressure at head level could not have beenmeasured simultaneously with arterial pres-sure. On theoretical grounds it appears prob-able that when the head is moved betweenheart and ground level, cerebral perfusionpressure remains relatively constant. With a
Figure 6Behavior of blood pressure on elevating the headof an anesthetized giraffe for 150 cm. Miniaturemanometer in root of aorta.
distended venous system changes in venousand arterial pressure at brain level withchange in head position should be of similarmagnitude. On the other hand, the situationm&y be somewhat different in the case ofhead positions between heart level and the"normal" high position of the head. Inman, when the body position is changed fromhorizontal to upright, the average fall invenous pressure in the jugular bulb is only0.38 X the fall in arterial pressure at thesame level.15 This is believed to be due topartial collapse of the veins with a corre-sponding increase in resistance to blood flow.In the giraffe the same mechanism would beexpected to operate, probably in exaggerateddegree.
SummaryObservations on the circulatory functions
of 4 giraffes are recorded. Both the rightand the left heart were catheterized underlocal anesthesia with a miniature manometer.
Circulation Research, Volume VIII, September I960
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from
1058 GOETZ, ET Ah.
Cardiac output was determined by employingboth indicator dilution method and the Fickprinciple. Other parameters, such as the cir-culation time, blood volume, velocity, rightand left ventricular pressure ascent as wellas the changes in blood pressure occurringwith changes in the posture of the head wererecorded. The difficulties of the experimentscreated certain limitations in their interpreta-tion. The arterial b'.ood pressure is high byhuman standards and adequate to maintaincerebral perfusion without other means ofsupport. The arterial pressure pulse contoursuggests a relatively lax vascular bed withconsiderable reserve extensibility. Values forcardiac output aud blood volume were roughlycomparable to those recorded in domesticcattle of the same approximate weight.
AcknowledgmentThe authors are particularly grateful to Mr. T. J.
Steyn, Director of the Department for the Conser-vation of Flora and Fauna, Pretoria, South Africa,who with his staff gave invaluable assistance, capturedthe animals and cared for them for many months priorto the experiment. Their hospitality and help inrestraining the animals and in the preparation of theexperiment is gratefully acknowledged.
The authors gratefully acknowledge the assistancereceived from Protea Holdings, Johannesburg, SouthAfrica, for making a Sanborn Polyviso recordingapparatus available for field studies and the valuablehelp received from Caltex, Johannesburg, who throughMr. Lewis Lewis of Cape Town, assisted with thephotography, and Baum and Company, New York,who presented us with a special Baumanometer read-ing up to 600 mm. Hg.
Summario in InterlinguaEs registrate observationes relative al functiones
circulatori in 4 girafas. Le corde dextere e le cordesinistre esseva catheterisate sub anesthesia local permedio de un manometro micro-dimensional. Le rendi-mento cardiac esseva determinate per medio delmethodo a dilution de indicator e etiam secundo leprincipio de Pick. Le altere parametros que essevaregistrate include le tempore de circulation, le volu-mine de sanguine, le velocitate del fluxo, le asceuditadel tension dextero- e sinistro-ventricular, e etiam lealterationes in le tension sanguinee que occurre conalterationes in le postura del capite. Le difficultatesdel experimentos creava certe limitationes del inter-pretation de lor resultatos. Le tension de sanguinearterial es alte in comparation con standards human.Illo suffice a mantener le perfusion cerebral sin altere
medios de supporto. Le contorno del pulso de tensionarterial siiggere le existentia de un relativemontelaxe vasculatura con considernbile reservas de distensi-bilitate. Le valores pro le rendimento cardiac e levolumine de sanguine esseva grossiormente compara-bile ill valores registrate in bestial domestic do npprox-imsitivemcnte le inesme statura.
^References1. GOETZ, E. H., AND BUDTZ-OLSEN, 0.: Scientific
safari: Circulation of the giraffe. SouthAfrican M. J. 29: 773, 1955.
2. —: Preliminary observations on circulation in .the giraffe. T. Am. Coll. of Cardiol. 5: 239,195S.
3. —, AND KEEN, B. N.: Some aspects of circula-tory system of the giraffe. Angiology 8: 542,1957.
4. GAUER, O. H., AND GIENAPP, E.: Miniature pres-
sure recording device. Science 112: 404, 1950.5. HAMILTON, "W. P., MOORE, J. "W., KINSMAN,
J. M., AND SPURLING, E. G.: Studies on thecirculation. IV. Further analysis of injectionmethod and of changes in hemodynamics underphysiological and pathological conditions. Am.J. Physiol. 99: 534, 1932.
6. DOYLE, J. T., WILSON, J. S., LEPINE, C, ANDWARREN, J. V.: Evaluation of measurementof cardiac output and of so-called pulmonaryblood volume by dye dilution method. J . Lab.& Clin. Med. 41: 29, 1953.
7. WEISSLER, A. M., AND WARREN, J. V.: Vaso-
pressor syncope. Am. Heart J. 57: 786, 1959.8. HOLT, J. P. : Flow of liquids through "collaps-
ible" tubes. Circulation Research 7: 342, 1959.9. REYNOLDS, M.: Plasma and blood volume in the
cow using the T-1824 hematocrit method. Am.J. Physiol. 175: 118, 1948.
10. DOYLE, J. T., PATTERSON, J. L., JR., WARREN,J. V., AND DETWEILER, D. K.: Observations onthe circulation of domestic cattle. CirculationResearch 8: 4, 1960.
11. ALEXANDER, R. S.: Factors determining the con-tour of pressure pulses recorded from the aorta.Fed. Proc. 11: 738, 1952.
12. PETERSON, L. H.: Certain physical characteristicsof the cardiovascular system and their signifi-cance in the problem of calculating strokevolume from the arterial pulse. Fed. Proc.11: 762, 1952.
13. WIGGERS, C. J.: Physiology of Shock. New Tork,Commonwealth Fund, 1950.
14. ADAMS, W. E.: Comparative Morphology of theCarotid Body and Carotid Sinus. Springfield,111., Charles C Thomas, 1958.
15. PATTERSON, J. L. JR., AND WARREN, J. V.:Mechanisms of adjustment in cerebral circul-tion upon assumption of upright position. J.Clin. Invest. 31: 653, 1952.
Circulation Research, Volume VIII, September 1960
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

ManceJOSEPH T. DOYLE, E. N. KEEN, MAURICE McGREGOR, L. M. TILLER, M. SMITH and E. ROBERT H. GOETZ, JAMES V. WARREN, OTTO H. GAUER, JOHN L. PATTERSON, JR.,
Circulation of the Giraffe
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1960 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.8.5.10491960;8:1049-1058Circ Res.
http://circres.ahajournals.org/content/8/5/1049World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Research Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from





























