Embed Size (px)
Citation preview

1527
Peripheral artery disease (PAD) is initiated by athero-genic mechanisms common to all major vascular terri-
tories but encompasses several distinctly important clinical sequelae.1 The global burden of PAD is large and rising, with substantial morbidity and mortality found in high-, middle-, and low-income countries.2 The atherosclerotic occlusive disease underlying PAD is associated with an
exercise limitation in the majority of patients, whereas the classic symptoms of intermittent claudication, ischemic rest pain, and ischemic ulceration are less common mani-festations.3 Patients with PAD are also at increased risk of myocardial infarction, ischemic stroke, heart failure, re-novascular hypertension, and vascular death reflecting the systemic atherosclerotic burden.4–6 The epidemiology of
Peripheral Artery Disease Compendium
© 2015 American Heart Association, Inc.
Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/CIRCRESAHA.116.303566
Abstract: Patients with peripheral artery disease have a marked reduction in exercise performance and daily ambulatory activity irrespective of their limb symptoms of classic or atypical claudication. This review will evaluate the multiple pathophysiologic mechanisms underlying the exercise impairment in peripheral artery disease based on an evaluation of the current literature and research performed by the authors. Peripheral artery disease results in atherosclerotic obstructions in the major conduit arteries supplying the lower extremities. This arterial disease process impairs the supply of oxygen and metabolic substrates needed to match the metabolic demand generated by active skeletal muscle during walking exercise. However, the hemodynamic impairment associated with the occlusive disease process does not fully account for the reduced exercise impairment, indicating that additional pathophysiologic mechanisms contribute to the limb manifestations. These mechanisms include a cascade of pathophysiological responses during exercise-induced ischemia and reperfusion at rest that are associated with endothelial dysfunction, oxidant stress, inflammation, and muscle metabolic abnormalities that provide opportunities for targeted therapeutic interventions to address the complex pathophysiology of the exercise impairment in peripheral artery disease. (Circ Res. 2015;116:1527-1539. DOI: 10.1161/CIRCRESAHA.116.303566.)
Key Words: exercise ■ metabolism ■ peripheral artery disease ■ peripheral vascular diseases ■ physiopathology ■ therapeutics
Pathogenesis of the Limb Manifestations and Exercise Limitations in Peripheral Artery Disease
William R. Hiatt, Ehrin J. Armstrong, Christopher J. Larson, Eric P. Brass
Circulation Research Compendium on Peripheral Artery Disease
Epidemiology of Peripheral Artery DiseasePathogenesis of the Limb Manifestations and Exercise Limitations in Peripheral Artery DiseaseLower Extremity Manifestations of Peripheral Artery Disease: The Pathophysiologic and Functional Implications of Leg IschemiaThe Genetic Basis of Peripheral Arterial Disease: Current Knowledge, Challenges and Future DirectionsModulating the Vascular Response to Limb Ischemia: Angiogenic and Cell TherapiesPharmacological Treatment and Current Management of Peripheral Artery DiseaseEndovascular Intervention for Peripheral Artery DiseaseSurgical Intervention for Peripheral Arterial Disease
John Cooke, Guest Editor
Original received September 18, 2014; revision received December 8, 2014; accepted December 17, 2014. In February 2015, the average time from submission to first decision for all original research papers submitted to Circulation Research was 13.9 days.
From the Division of Cardiology, Department of Medicine (W.R.H., E.J.A.), CPC Clinical Research (W.R.H.), University of Colorado School of Medicine, Aurora; Cardiovascular & Metabolic Diseases Drug Discovery Unit, Takeda Pharmaceuticals, San Diego, CA (C.J.L.); and Department of Medicine, Harbor-UCLA Center for Clinical Pharmacology, Torrance, CA (E.P.B.).
Correspondence to William R. Hiatt, MD, Division of Cardiology, Department of Medicine, University of Colorado School of Medicine, C/O CPC Clinical Research, 13199 E Montview Blvd, Suite 200, Aurora, CO 80045. E-mail [email protected]
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

1528 Circulation Research April 24, 2015
PAD is linked to that of the other common atherosclerotic processes, such as coronary and cerebral artery diseases, and affects 15% of the adult population aged >45 years.7 Predominant risk factors for PAD include advancing age, smoking, and diabetes mellitus; hypertension and lipid disorders contribute less risk when compared with their association with ischemic stroke and myocardial infarc-tion.2,8 Patients with PAD have cardiovascular outcomes similar to patients with coronary artery disease or isch-emic stroke, with the risk of myocardial infarction, stroke, or vascular death >5% per year.9–15
The diagnosis of PAD can be ascertained by simple hemo-dynamic measurements, in particular, the ankle-brachial index (ABI), a test performed by measuring the systolic blood pres-sure in each arm and the dorsalis pedis and posterior tibial arteries of each ankle. The highest of the dorsalis pedis or posterior tibial artery pressures is the numerator of the ABI specific to each leg, whereas the highest arm pressure on ei-ther side is the denominator. A ratio of <0.90 in either leg is considered hemodynamic evidence of PAD.16 When imaged, PAD can be characterized as one or more arterial stenoses or occlusions involving the distal aorta, iliac, femoral, popliteal, or tibial arteries.17
The underlying mechanisms responsible for the functional limitations in PAD are hemodynamic in origin, which affects the supply of oxygen and substrates to metabolically active tissue: skeletal muscle in the case of intermittent claudication and skin and subcutaneous tissues in the case of critical leg ischemia. However, additional pathophysiologic mechanisms contribute to the limb manifestations, where a reduction in blood flow alone does not fully account for the exercise limita-tion. Recent research into the pathophysiology of this exercise limitation has identified several important sequelae resultant from the chronic hemodynamic deficit. These changes affect-ing the vasculature and skeletal muscle distal to the primary hemodynamic lesions likely contribute to the mechanisms of exercise limitation in PAD. These advances are reviewed here with an additional focus on identifying possible future thera-peutic strategies.
Symptomatic Manifestations and Exercise Limitations in PAD
In the coronary circulation, plaque rupture leading to acute ischemic events is a common clinical presentation; in PAD, progressive atherosclerosis leading to chronic stenosis and occlusion, often in series, in the arteries supplying the lower extremities dominates the symptomatic manifestations.6
Limb SymptomsPatients with PAD may present with a range of limb symp-toms. Most patients are either asymptomatic or have atypical limb symptoms during exercise, whereas only a third have typical symptoms of claudication.18 The clinical character-istics of PAD have been characterized in a longitudinal co-hort study that defined typical and atypical limb symptoms. Typical claudication is defined by exercise-induced calf dis-comfort that is relieved by rest.19 Atypical limb symptoms can be characterized as exertional calf symptoms that do not begin at rest but are otherwise not consistent with classical claudication, such as muscle symptoms that do not include the calves, and pain at rest and pain with exertion.18 These symptoms should not be confused with other causes of atypi-cal limb pain, including statin-induced myalgias, spinal ste-nosis, and other orthopedic conditions. The pathogenesis can usually be differentiated with a careful history and physical examination, although some patients may have PAD concom-itant orthopedic disease.
Atypical exertional leg symptoms are more common than classic claudication and are also associated with decreased overall functional exercise capacity.20 Patients with hemo-dynamic evidence of PAD in the peripheral circulation (eg, low ABI) consistently demonstrate a marked reduction in peak exercise performance and daily ambulatory activity.21–23 Thus, the pathophysiology, which results in reduced exercise performance in PAD, affects a broad spectrum of patients ir-respective of their limb symptoms. In this context, although patients with typical intermittent claudication have been the best studied and the term is in common usage, the mecha-nisms underlying the exercise limitation are likely common to all patients regardless of the nature of their limb symptoms. Therefore, using the term claudication to describe all symp-tomatic patients with PAD is inappropriate, and in this review, the functional deficit associated with PAD will be referred to as an exercise limitation and includes otherwise asymptomatic patients who also have exercise impairment.
Severity of the Exercise ImpairmentThe severity of the functional limitation in PAD has been well characterized. On a population basis, patients with PAD have an ≈50% reduction in peak exercise performance when compared with an age-matched healthy cohort.21 This exer-cise limitation is associated with marked impairments in daily physical activity as assessed by questionnaire and daily ener-gy expenditure.24,25 Patients with PAD also have an accelerated functional decline over time that is related to the underlying hemodynamic severity of the disease in the leg.26 The primary treatment goal for all patients with PAD is cardiovascular risk reduction, whereas on the basis of the above considerations, an additional goal is to improve exercise performance, daily functional activity, and quality of life.
Arterial Hemodynamics in PADThe reduction in blood flow to the lower extremity as a conse-quence of the arterial occlusive disease process is a contribu-tor to the exercise impairment in PAD. Ischemia with exercise followed by reperfusion is also an important initiator of the subsequent pathophysiology in skeletal muscle.
Nonstandard Abbreviations and Acronyms
ABI ankle-brachial index
ERR estrogen related receptor
ETA endothelin receptor A
ETB endothelin receptor B
FFR fractional flow reserve
PAD peripheral artery disease
PPAR peroxisome proliferator–activated receptor
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from
Hiatt et al Exercise Limitation in Peripheral Artery Disease 1529
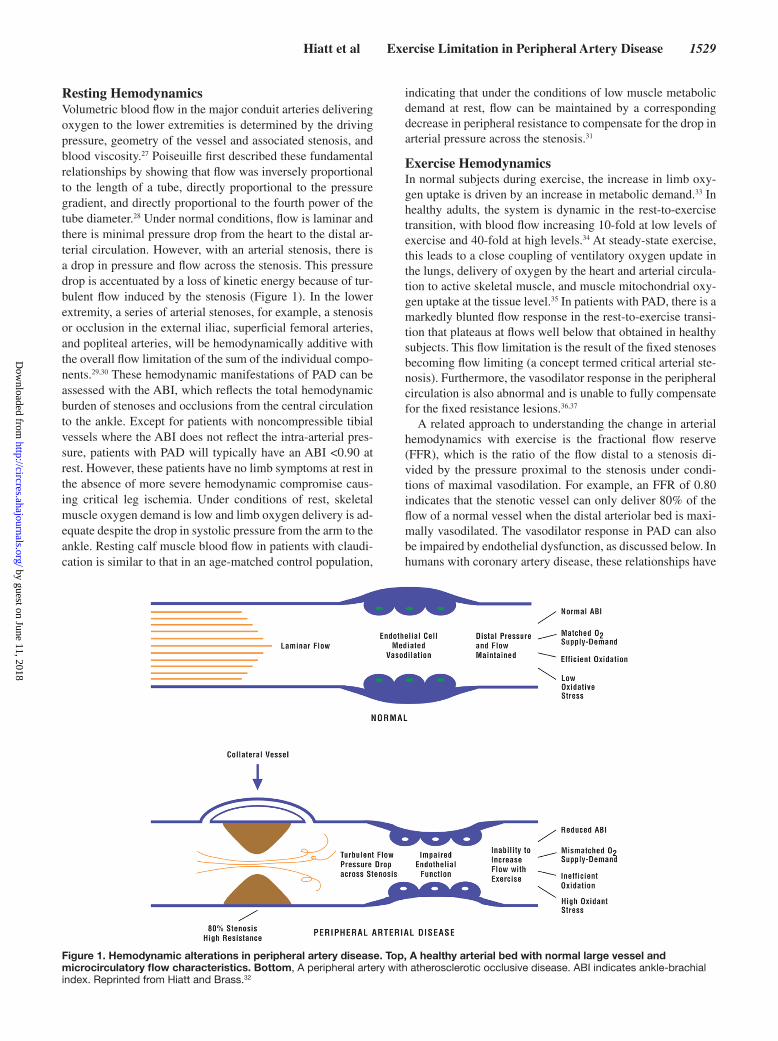
Resting HemodynamicsVolumetric blood flow in the major conduit arteries delivering oxygen to the lower extremities is determined by the driving pressure, geometry of the vessel and associated stenosis, and blood viscosity.27 Poiseuille first described these fundamental relationships by showing that flow was inversely proportional to the length of a tube, directly proportional to the pressure gradient, and directly proportional to the fourth power of the tube diameter.28 Under normal conditions, flow is laminar and there is minimal pressure drop from the heart to the distal ar-terial circulation. However, with an arterial stenosis, there is a drop in pressure and flow across the stenosis. This pressure drop is accentuated by a loss of kinetic energy because of tur-bulent flow induced by the stenosis (Figure 1). In the lower extremity, a series of arterial stenoses, for example, a stenosis or occlusion in the external iliac, superficial femoral arteries, and popliteal arteries, will be hemodynamically additive with the overall flow limitation of the sum of the individual compo-nents.29,30 These hemodynamic manifestations of PAD can be assessed with the ABI, which reflects the total hemodynamic burden of stenoses and occlusions from the central circulation to the ankle. Except for patients with noncompressible tibial vessels where the ABI does not reflect the intra-arterial pres-sure, patients with PAD will typically have an ABI <0.90 at rest. However, these patients have no limb symptoms at rest in the absence of more severe hemodynamic compromise caus-ing critical leg ischemia. Under conditions of rest, skeletal muscle oxygen demand is low and limb oxygen delivery is ad-equate despite the drop in systolic pressure from the arm to the ankle. Resting calf muscle blood flow in patients with claudi-cation is similar to that in an age-matched control population,
indicating that under the conditions of low muscle metabolic demand at rest, flow can be maintained by a corresponding decrease in peripheral resistance to compensate for the drop in arterial pressure across the stenosis.31
Exercise HemodynamicsIn normal subjects during exercise, the increase in limb oxy-gen uptake is driven by an increase in metabolic demand.33 In healthy adults, the system is dynamic in the rest-to-exercise transition, with blood flow increasing 10-fold at low levels of exercise and 40-fold at high levels.34 At steady-state exercise, this leads to a close coupling of ventilatory oxygen update in the lungs, delivery of oxygen by the heart and arterial circula-tion to active skeletal muscle, and muscle mitochondrial oxy-gen uptake at the tissue level.35 In patients with PAD, there is a markedly blunted flow response in the rest-to-exercise transi-tion that plateaus at flows well below that obtained in healthy subjects. This flow limitation is the result of the fixed stenoses becoming flow limiting (a concept termed critical arterial ste-nosis). Furthermore, the vasodilator response in the peripheral circulation is also abnormal and is unable to fully compensate for the fixed resistance lesions.36,37
A related approach to understanding the change in arterial hemodynamics with exercise is the fractional flow reserve (FFR), which is the ratio of the flow distal to a stenosis di-vided by the pressure proximal to the stenosis under condi-tions of maximal vasodilation. For example, an FFR of 0.80 indicates that the stenotic vessel can only deliver 80% of the flow of a normal vessel when the distal arteriolar bed is maxi-mally vasodilated. The vasodilator response in PAD can also be impaired by endothelial dysfunction, as discussed below. In humans with coronary artery disease, these relationships have
Figure 1. Hemodynamic alterations in peripheral artery disease. Top, A healthy arterial bed with normal large vessel and microcirculatory flow characteristics. Bottom, A peripheral artery with atherosclerotic occlusive disease. ABI indicates ankle-brachial index. Reprinted from Hiatt and Brass.32
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

1530 Circulation Research April 24, 2015
been confirmed to have physiological significance for quanti-fying coronary ischemia.38 In the coronary circulation, clinical studies have shown that an FFR of <0.80 is physiologically significant and that this FFR value identifies a clinically sig-nificant cutoff point where symptomatic patients benefit from coronary revascularization.39 In patients with claudication, initial studies have shown that FFR measurements correlate with the lesion peak systolic velocity, a noninvasive measure-ment of lesion severity.40 Further studies will be necessary to correlate the clinical use of FFR measurements to potentially guide revascularization or other treatment strategies in PAD.
A complementary approach to determining the physiologi-cal significance of flow limitations in patients with PAD is the assessment of tissue oxygenation. Blood-oxygen-level–dependent MRI imaging techniques can measure the extent of tissue deoxygenation during postocclusive reactive hyper-emia.41 Near-infrared spectroscopy has also been used to make dynamic assessments of tissue oxygenation in patients with PAD. For example, the phosphodiestersase-5 inhibitor silde-nafil improved muscle oxygenation as assessed by near-infra-red spectroscopy without improving walking performance in a small study of patients with PAD.42 These approaches have the potential to differentiate the effect of oxygen delivery versus oxygen use on muscle dysfunction.
Endothelial and Microcirculatory DysfunctionAs described above, optimizing muscle blood flow during ex-ercise is dependent on vasodilation in the limb to minimize the overall resistance to flow delivery to active muscle. This vasodilation is an active process with several important vaso-active mediators, including nitric oxide.43 Patients with PAD have significant abnormalities in endothelium-dependent va-sodilation.44,45 Oxidant stress leads to generation of superox-ide anion and other mediators of endothelial dysfunction.10,46 Exercise-induced release of endothelin-1, a potent vasocon-strictor, can also antagonize exercise-induced skeletal muscle vasodilation.47,48 Through these mechanisms, impaired endo-thelial function as assessed by flow-mediated dilation has been correlated with the clinical severity of PAD.49,50 Furthermore, in studies where leg blood flow was measured by using a thermodilution catheter, there was a correlation (r=0.71) be-tween maximal leg blood flow and performance on a bicycle ergometer.31
Interestingly, endothelial dysfunction was recently associat-ed with walking impairment independent of the ABI, suggest-ing that endothelial dysfunction may contribute to the exercise impairment in PAD.49 Other studies have suggested a correla-tion between ABI and endothelial dysfunction as assessed by flow-mediated dilation.51 Exercise training, which improves functional status in patients with PAD, also improves flow-mediated dilation.52 A recent study of patients undergoing a 12-week exercise training program demonstrated an improve-ment in flow-mediated dilation compared with baseline, sug-gesting that improvements in endothelial function may be one mechanism mediating reduced symptoms of claudication after exercise training.53 In addition, in an animal model of chronic atherosclerosis that simulated some features of PAD, a phar-macological intervention that improved exercise-induced blood flow also improved the animals’ functional status.54 The
impaired vasodilation in patients with PAD is likely a sequela of the obstruction, and improvement in physiological vasodi-lation with exercise offers a potential therapeutic target.
Microcirculatory dysfunction and local skeletal muscle flow can also be assessed by novel noninvasive imaging tech-niques, including arterial spin–labeling MRI and contrast-en-hanced ultrasound. In a pilot study, arterial spin–labeling MRI demonstrated that microvascular flow was relatively preserved among patients with mild PAD (ABI>0.50), but more severe PAD (ABI<0.50) was associated with a significant decrement in microvascular blood flow.55 This technique can also be used to image calf muscle flow at peak exercise and may be a useful tool to assess changes in calf blood flow after therapeutic in-terventions.56 In another small study, perfusion imaging of the skeletal muscle microcirculation was performed by contrast-enhanced ultrasound at rest and with exercise. In a multivari-ate model, the treadmill time to the onset of claudication was correlated with microcirculatory exercise flow and the differ-ence between resting and exercise microcirculatory flow.57 Contrast-enhanced MRI measures of peak exercise blood flow have also been shown to correlate with exercise performance and 6-minute walk times.58
Rheological FactorsAlterations in blood hemorheology can also impair arte-rial flow. Changes in the blood concentration of fibrinogen and von Willebrand factor can increase blood viscosity, par-ticularly at the microcirculatory level, which according to Pousseille law could contribute to reduced arterial flow—but less so than a change of equal magnitude in the percent steno-sis.59,60 Activated leukocytes may also promote microvascular plugging and thrombosis, thereby further increasing the re-sistance to arterial flow. In a large cohort of patients from the Edinburgh Artery Study, blood viscosity and fibrinogen were independently associated with hemodynamic disease severity of PAD, and fibrin degradation products were also associated with progression of PAD.61,62 These findings suggest that in-creased blood viscosity may be a component of the functional limitation or simply secondary to the systemic atherosclerotic disease process.
Existing Medical Therapy for the Exercise Limitation in PAD
Current medical therapy for the exercise limitation in PAD is limited. Reasonable evidence exists for the use of phospho-diesterase type 3 inhibition, particularly cilostazol. Several meta-analyses have demonstrated a consistent clinical benefit of this medication despite a lack of detailed understanding of its mechanism of disease benefit.63 Specifically, it is not clear why either the inhibition of platelet aggregation or the stimu-lation of vasodilation—both mediated by phosphodiesterase type 3 inhibition—would translate into functional benefit in patients with PAD. As noted above, a nonspecific vasodilator, such as cilostazol, has the potential for steal of flow by health-ier, more responsive vessels. Also, no convincing explanation exists for why the clinical benefits of phosphodiesterase type 3 inhibition continue to increase during 24 weeks of treat-ment when the direct pharmacological effects—vasodilation and inhibition of platelet aggregation—are immediate.64 This
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

Hiatt et al Exercise Limitation in Peripheral Artery Disease 1531
time-dependent improvement suggests a complex physiologi-cal response to treatment. Although modest improvements in ABI have been observed with phosphodiesterase inhibition, it is unlikely that this effect alone accounts for the mechanism of benefit.65 The efficacy signals from 2 additional phosphodies-terase type 3 inhibitors support a disease benefit for the class, albeit one that is not completely understood.66,67
Older medications, such as pentoxifylline and naftidrofuryl, are approved for use in patients with PAD within and outside of the United States, respectively. The overall data supporting any functional benefit for treatment of patients with PAD with pentoxifylline are weak.68,69 The limited benefit of naftidro-furyl in patients with PAD also cannot be linked to any well-defined mechanism of action.69–71
Exercise training has been a mainstay of treatment for PAD, with a well-established benefit during a typical 12-week train-ing program.72 Exercise training may affect several pathways associated with clinical benefit, including improved skeletal muscle metabolism, endothelial function, and the biomechan-ics of gait.73,74 Given the established efficacy of exercise train-ing, it would be logical to use pharmacotherapy as an adjunct to structured exercise rehabilitation in patients with PAD. Candidates for pharmacotherapy might include drugs with mechanisms that augment or complement the beneficial ef-fects of training. In part to due to lack of good candidates and the complexity of studying drug therapy against a background of exercise training, there is a paucity of data addressing this hypothesis. A randomized trial of exercise training added to optimal medical therapy, including cilostazol, demonstrated a clear additive benefit of training, but the design did not address if cilostazol added benefit compared with exercise training without the drug.75 In addition, a study combining treatment with propionyl-l-carnitine and exercise training failed to show significantly better improvement in walking performance when compared with exercise training alone.76
Endovascular revascularization is a commonly used inter-vention to improve skeletal muscle blood flow. When provided on a background of best medical therapy, revascularization of aortoiliac disease results in improved peak walking time and associated parameters of quality of life, and the magnitude of benefit is similar to that achieved with supervised exercise.75
Cellular and Molecular Pathophysiology of the Exercise Impairment in PAD
Although the primary pathophysiology of the exercise limita-tion in PAD is initiated by the underlying arterial occlusive disease and associated reduction in exercise blood flow and oxygen delivery, the correlation is not strong between the flow limitation versus the observed decrease in exercise perfor-mance. Studies examining the resting ABI showed a weak to no correlation with peak treadmill exercise performance.22,77,78 In addition, interventions, such as exercise training, that lead to a large increase in peak exercise performance have little ef-fect on skeletal muscle blood flow or ABI.79 Thus, although the occlusive atherosclerotic disease process is associated with a well-defined limitation of blood flow and oxygen delivery to exercising skeletal muscle, the absence of a strong correla-tion between the arterial obstruction and exercise performance
indicates that factors other than changes in limb vascular re-sistance contribute to the exercise impairment in patients with PAD. Underlying mechanisms that may induce factors that are linked to the functional impairment include inflammation and oxidant stress with subsequent endothelial and microcir-culatory dysfunction, skeletal muscle structural abnormalities, altered oxygen coupling and mitochondrial respiration, and skeletal muscle metabolic abnormalities. A better understand-ing of these pathways may help guide novel medical therapies for the treatment of PAD and improve functional outcomes in patients with claudication.
Endothelial and Microcirculatory DysfunctionAs described above, patients with PAD have significant ab-normalities in endothelium-dependent vasodilation.44,45 A potential therapeutic strategy with respect to endothelial and microcirculatory dysfunction is antagonism of the release or action of endothelin. Endothelin can bind to either endothelin receptor A (ETA) or endothelin receptor B (ETB) subtypes 1 and 2. ETA receptors are located on the smooth muscle cells of vascular tissue, and endothelin binding causes vaso-constriction through agonist-induced receptor-mediated sig-naling.80 ETB receptor action is more complex, with ETB1 mediating vasodilation through nitric oxide release, whereas ETB2 causes vasoconstriction. Thus, antagonism of vasocon-striction mediated by ETA represents a potential therapeutic strategy to improve microcirculatory flow in PAD. However, the resultant vasodilator effect will be of benefit only if it im-proves microvascular flow to ischemic muscle and does not induce a steal phenomenon. Several selective ETA receptor antagonists are available for clinical testing. Ambrisentan is an ETA selective antagonist approved in the United States and Europe for the treatment of pulmonary arterial hypertension.81 Two other candidates for testing would be the ETA and ETB dual antagonists macitentan and bosentan, which are both also approved for the treatment of pulmonary artery hypertension. Macitentan represents an intermediate pharmacological pro-file between bosentan and ambrisentan, with a 50-fold selec-tivity for the ETA subtype compared with the ETB subtype.82,83
Given the high prevalence of diabetes mellitus in patients with PAD, it is interesting to note that studies have also sug-gested that pioglitazone could improve vascular function.84–86 The relevance of these changes to functional status in patients with PAD remains unknown.
Inflammation and Oxidant StressInflammation is a key mediator of the atherosclerotic process and likely contributes to the limb manifestations of PAD as well.9,10 In addition, the mismatch between oxygen demand and oxygen delivery during exercise in patients with PAD induces an inflammatory response.10 In PAD, exercise is as-sociated with an increase in plasma levels of numerous in-flammatory mediators, including thiobarbituric acid–reactive substances (formed as a byproduct of lipid peroxidation), thromboxane, interleukin-8, tumor necrosis factor-α, soluble intercellular adhesion molecule-1, vascular cell adhesion mol-ecule-1, von Willebrand factor, E-selectin, and thrombomodu-lin.87–93 Inflammatory mediators can aggravate endothelial dysfunction, and markers, such as interleukin-6, are inversely
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

1532 Circulation Research April 24, 2015
correlated with maximum treadmill performance.94 When ex-ercise impairment was evaluated by a series of walking tests, higher serum C-reactive protein and serum amyloid A concen-trations were associated with reductions in 6-minute-walk dis-tance, 4-meter walking velocity, and a summary performance score that combined performance in walking speed, stand-ing balance, and time for 5 repeated chair rises.95 Elevated C-reactive protein levels were also associated with a greater annual decline in 6-minute walk performance for a period of 3 years and peak walking time.96,97
During ischemia, skeletal muscle mitochondria release free radicals, including superoxide and other reactive oxygen spe-cies, that are derived from the oxidation–reduction cascade.98 Reperfusion of ischemic muscle after exercise may also lead to an increase in oxidant stress.99,100 These reactive oxygen species have the potential to trigger numerous pathophysi-ologic pathways, including endothelial dysfunction and cova-lent modification of muscle macromolecules. Over time, this oxidant stress can also lead to mitochondrial DNA injury as demonstrated in patients with PAD.101,102 Mitochondrial DNA injury can also be detected in the less affected limbs of pa-tients with unilateral PAD, suggesting that the mitochondrial injury may reflect systemic inflammation and not simply local skeletal muscle ischemia. Although exercise acutely induces oxidant stress in patients with PAD, exercise training has con-sistently been shown to improve symptoms among patients with PAD. Although this may seem to be contradictory, it is important to differentiate the effects of acute versus training exercise paradigms.103 For example, in model systems, exercise training has been shown to upregulate modulators of oxidative stress, including superoxide dismutase, inducible nitric oxide synthase, and thioredoxin.104–106 This modulation of oxidative stress defense mechanisms may be an important mechanism for the benefit of exercise training in patients with PAD.
Inflammatory mediators may also have proangiogenic and antiangiogenic effects, potentially modulating the endogenous response to ischemia.107 For example, circulating concentra-tions of vascular endothelial growth factor are decreased in patients with PAD when compared with controls with other comorbid conditions.93
Innovative anti-inflammatory therapies developed for other indications may have relevance for PAD. For example, inter-cellular adhesion molecules and vascular cell adhesion mol-ecules play important roles in intracellular signaling and the immune and inflammatory responses and are elevated in pa-tients with PAD.108 Antagonists of vascular cell adhesion mol-ecule and intercellular adhesion molecule function have been developed that could be tested for efficacy in PAD. In particu-lar, antagonists of very late antigen-4 have shown promise in treating inflammatory disorders in several animal models and could be advanced into clinical trials for this indication.109–112
Selectins, also elevated in PAD populations, are a set of cell adhesion molecules consisting of 3 subsets: E-selectins expressed on endothelial cells in skin microvessels after ex-posure to cytokines, L-selectins basally expressed on leuko-cytes, such as granulocytes and monocytes, and P-selectins basally expressed on platelets and endothelial cells. Recently, inclacumab, a potent and selective P-selectin–neutralizing
antibody, has completed safety, tolerability, pharmacokinetic, and pharmacodynamic studies showing reduction in myo-cardial damage after percutaneous coronary intervention for non–ST-segment–elevation myocardial infarction.113 Whether modulating P-selectin in PAD has longer term clinical benefit has not yet been studied. In addition, inclacumab has been demonstrated to reduce elevated circulating platelet–leuko-cyte aggregate levels in patients with PAD, thus providing pharmacodynamic data useful for hypothesis generation.114
The angiotensin-converting enzyme inhibitor ramipril re-cently has been reported to improve placebo-corrected walk-ing distance.115 However, the placebo group in this study did not show the usual walking performance improvements typically seen in these trials, which may have inflated the net benefit of the drug over placebo. Potential mechanisms of ramipril-mediated improvement in walking performance include associations with an increase in angiogenic biomark-ers and reduction in the markers of thrombosis, inflammation, and leukocyte adhesion.116 These biomarker changes may re-flect modulation of more fundamental processes. As a meta-analysis of angiotensin-converting inhibition did not find any benefit on exercise performance recently,117 it seems unlikely that renin–angiotensin–aldosterone system pathway interven-tion provides consistent functional benefit.
Metabolic agents, such as propionyl-l-carnitine, have also shown a signal of benefit but have not been fully developed as an approved pharmacological therapy.118 Although several large studies have demonstrated the atherosclerotic disease–modifying benefit of statin treatment, which may include actions through anti-inflammatory pathways, inconsistent benefits on exercise performance have been observed in PAD.119–121
Skeletal Muscle Structural AbnormalitiesNumerous pathological changes have been identified in the skeletal muscle of patients with PAD, including muscle apop-tosis and atrophy, increased fiber type switching, altered myosin heavy-chain expression, and muscle fiber denerva-tion.122–125 These structural changes may be mediated, in part, by higher levels of inflammatory mediators in PAD.126 On the basis of biopsy specimens from the gastrocnemius muscles of patients with PAD, ≈4% of gastrocnemius cells are apoptotic, and caspase-3 levels are twice as high as in patients without PAD.125 Selective fiber type switching from type I (aerobic) to type II (glycolytic) fibers may impair skeletal muscle per-formance and has been associated with decreased exercise tolerance.123 Decreased expression of myosin heavy-chain iso-form II in patients with PAD may also result in altered muscle contraction kinetics and decreased cellular efficiency.127 The observation of muscle fiber denervation among patients with PAD has also led to the hypothesis that arterial insufficiency coexists with a distal motor neuron neuropathy that worsens muscle weakness independent of arterial flow.128 Consistent with this hypothesis, impaired peroneal nerve conduction velocity was associated with decreased calf muscle area and lower 6-minute walk distance among patients with PAD.129
Numerous studies have correlated changes in calf muscle ultrastructure and overall muscle strength with subsequent car-diovascular outcomes in patients with claudication. Computed
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

Hiatt et al Exercise Limitation in Peripheral Artery Disease 1533
tomographic measurements of the content of muscle and fat in the calf have shown that calf muscle content is inversely associated with loss of mobility, even after adjusting for other risk factors and comorbidities.130 During long-term follow-up, a reduced calf muscle content was associated with increased all-cause and cardiovascular mortality independent of the ABI.131 Overall leg strength has also been shown to associate with mortality in men, but not women, with PAD.132 Taken to-gether, these findings suggest that the morphological changes in calf muscle predispose to significant functional decline and may be an additional marker for increased risk among patients with symptomatic PAD.
One approach for modulating muscle apoptosis and atrophy is through exploitation of the myostatin pathway. Multiple new pharmacological agents that target this pathway are al-ready in clinical development, including the soluble ActRIIB-Fc fusion decoy receptor ramatercept,133,134 antimyostatin antibody MYO-029, and the ActRIIB antibody BYM338.135–137 However, previous studies have shown that although endur-ance training improves function in patients with PAD, strength training does not result in the same degree of improvement. This discordance between the strong predictive value of en-dogenous muscle mass and the poor response to interven-tion may mean that endogenous muscle mass is an integrated marker of the complex limb changes occurring with chronic PAD. Thus, the likelihood of success of a muscle mass–based strategy alone may be low.74 Furthermore, this strategy is like-ly to be associated with systemic adverse events as exempli-fied by the epistaxis, gum bleeding, and skin vessel dilation observed in patients treated with ramatercept.133
Alterations in Oxygen Coupling and Mitochondrial RespirationThere is a tight coupling between pulmonary oxygen uptake, circulatory delivery of oxygen, and muscle mitochondrial respiration in healthy subjects during steady-state exercise. The transition from rest-to-exercise causes a rapid increase in the cellular degradation of ATP to ADP to support mus-cle contraction. Regeneration of ATP is initially supported by nonoxidative mechanisms, including a rapid depletion of phosphocreatine. Oxidative resynthesis of ATP occurs more slowly and requires delivery of oxygen to exercising skeletal muscle. The delay in oxidative adjustment to a new metabolic demand has been termed metabolic inertia.138
The transition to increased oxygen consumption can be characterized by several noninvasive measurements, including the kinetics of pulmonary oxygen consumption at the onset of exercise and the rate of hemoglobin desaturation in exercising skeletal muscle. In healthy subjects at the onset of exercise, these kinetic assessments are an attempt to characterize rates of mitochondrial oxidative metabolism rather than overall oxygen delivery.138 In patients with PAD, a profound prolon-gation of the kinetic rates of pulmonary oxygen consumption and tissue hemoglobin desaturation have been described at the onset of exercise relative to healthy, age-matched con-trols.139,140 This prolonged kinetic response associated with the reduced exercise performance in subjects with PAD sug-gests that alterations in skeletal muscle mitochondrial respira-tion may contribute to the decreased exercise performance in
PAD.141 Studies have also been performed using 31P magnetic resonance spectroscopy in PAD. When assessed at the onset of exercise, changes in muscle pH and phosphocreatine con-centration suggested inefficient oxidative metabolism neces-sitating a higher rate of ATP turnover for given power output as observed in control muscle.142 Taken together, these obser-vations demonstrate increased metabolic inertia in patients with PAD and provide evidence of impaired muscle metabolic function in PAD.
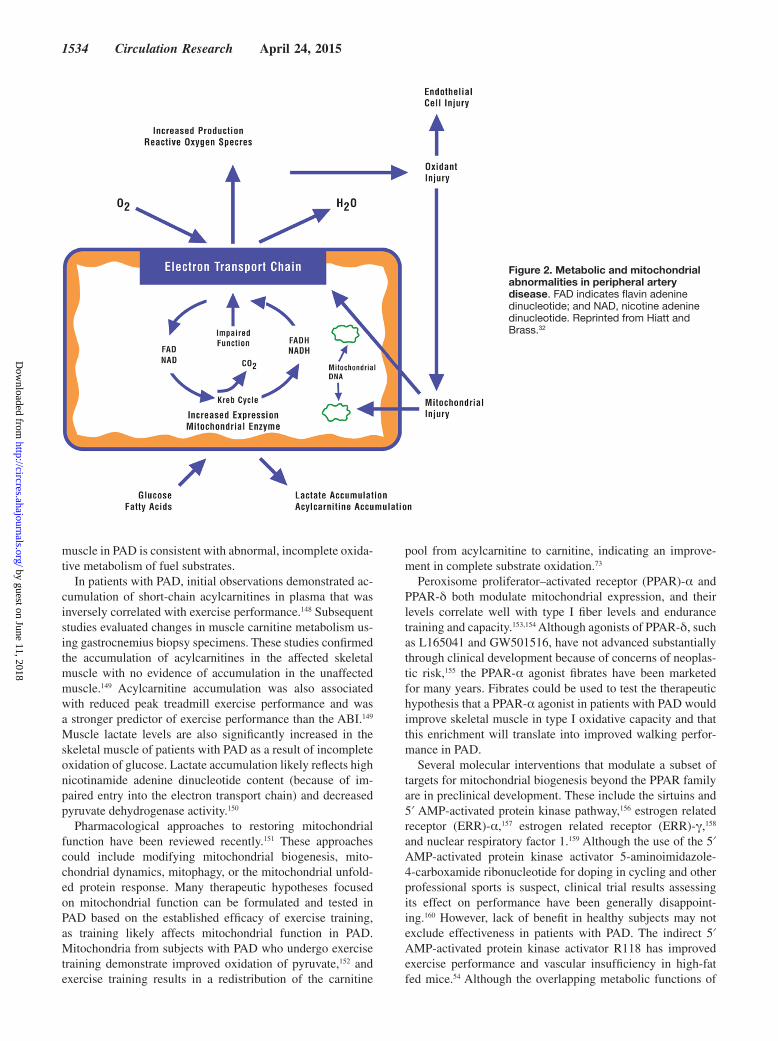
Other evidence supports impaired mitochondrial function as an important factor in functional impairment in PAD. The electron transport chain in mitochondria oxidizes nicotinamide adenine dinucleotide in a series of enzymatic steps that trans-fer electrons to oxygen (Figure 2). Key mitochondrial path-ways, including the electron transport chain, are vulnerable to free-radical injury.143 Skeletal muscle from the affected leg in patients with PAD has reduced the activities of mitochondrial nicotinamide adenine dinucleotide dehydrogenase of complex I and ubiquinol-cytochrome c oxidoreductase (complex III).144 The impairment in complex III of the electron transport chain may result in a higher redox potential to maintain electron flux, which may in turn lead to free-radical leakage in the mi-tochondria. Catalase and superoxide dismutase minimize the deleterious effects of hydrogen peroxide and superoxide, re-spectively, by catalyzing the conversion of these species into oxygen and hydrogen peroxide, which is subsequently con-verted to water. Damage ensues when reactive oxygen species levels exceed the reductive capacity of the cell.145 These ob-servations suggest that electron transport chain activity is im-paired, likely due to the ischemia-reperfusion injury in PAD, which may contribute to propagation of oxidative injury and metabolic dysfunction. Future strategies to modulate mito-chondrial respiratory function and efficiency could represent novel therapeutic targets for patients with PAD.
Skeletal Muscle Metabolic AbnormalitiesNumerous alterations in metabolic pathways have been stud-ied in the skeletal muscle of patients with PAD. A commonly used experimental paradigm has been used to identify patients with predominant evidence of hemodynamic abnormalities in one leg with no ABI abnormality or claudication symptoms in the contralateral leg. This allowed comparisons between the affected leg, an apparently unaffected leg in the same patient, and an age-matched control population. These studies have identified many key metabolic abnormalities in PAD.
Early observations focused on alterations in muscle car-nitine metabolism. Under normal metabolic conditions, fuel substrates, such as fatty acids, proteins, and carbohydrates, are converted into acyl-CoAs as intermediates in their com-plete oxidation. These coenzyme A–coupled intermediates are linked to the cellular carnitine pool through the reversible transfer of acyl groups between carnitine and coenzyme A.146 One of the functions of carnitine is to serve as a buffer for the acyl-CoA pool through the formation of acylcarnitines. Under conditions of metabolic stress, incomplete oxidation or incom-plete use of acyl-CoAs leads to their accumulation. Transfer of the acyl group to carnitine results in the accumulation of the corresponding acylcarnitine, which can be measured.147 Thus, an increase in the concentration of acylcarnitines in plasma or
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from
1534 Circulation Research April 24, 2015
muscle in PAD is consistent with abnormal, incomplete oxida-tive metabolism of fuel substrates.
In patients with PAD, initial observations demonstrated ac-cumulation of short-chain acylcarnitines in plasma that was inversely correlated with exercise performance.148 Subsequent studies evaluated changes in muscle carnitine metabolism us-ing gastrocnemius biopsy specimens. These studies confirmed the accumulation of acylcarnitines in the affected skeletal muscle with no evidence of accumulation in the unaffected muscle.149 Acylcarnitine accumulation was also associated with reduced peak treadmill exercise performance and was a stronger predictor of exercise performance than the ABI.149 Muscle lactate levels are also significantly increased in the skeletal muscle of patients with PAD as a result of incomplete oxidation of glucose. Lactate accumulation likely reflects high nicotinamide adenine dinucleotide content (because of im-paired entry into the electron transport chain) and decreased pyruvate dehydrogenase activity.150
Pharmacological approaches to restoring mitochondrial function have been reviewed recently.151 These approaches could include modifying mitochondrial biogenesis, mito-chondrial dynamics, mitophagy, or the mitochondrial unfold-ed protein response. Many therapeutic hypotheses focused on mitochondrial function can be formulated and tested in PAD based on the established efficacy of exercise training, as training likely affects mitochondrial function in PAD. Mitochondria from subjects with PAD who undergo exercise training demonstrate improved oxidation of pyruvate,152 and exercise training results in a redistribution of the carnitine
pool from acylcarnitine to carnitine, indicating an improve-ment in complete substrate oxidation.73
Peroxisome proliferator–activated receptor (PPAR)-α and PPAR-δ both modulate mitochondrial expression, and their levels correlate well with type I fiber levels and endurance training and capacity.153,154 Although agonists of PPAR-δ, such as L165041 and GW501516, have not advanced substantially through clinical development because of concerns of neoplas-tic risk,155 the PPAR-α agonist fibrates have been marketed for many years. Fibrates could be used to test the therapeutic hypothesis that a PPAR-α agonist in patients with PAD would improve skeletal muscle in type I oxidative capacity and that this enrichment will translate into improved walking perfor-mance in PAD.
Several molecular interventions that modulate a subset of targets for mitochondrial biogenesis beyond the PPAR family are in preclinical development. These include the sirtuins and 5′ AMP-activated protein kinase pathway,156 estrogen related receptor (ERR)-α,157 estrogen related receptor (ERR)-γ,158 and nuclear respiratory factor 1.159 Although the use of the 5′ AMP-activated protein kinase activator 5-aminoimidazole-4-carboxamide ribonucleotide for doping in cycling and other professional sports is suspect, clinical trial results assessing its effect on performance have been generally disappoint-ing.160 However, lack of benefit in healthy subjects may not exclude effectiveness in patients with PAD. The indirect 5′ AMP-activated protein kinase activator R118 has improved exercise performance and vascular insufficiency in high-fat fed mice.54 Although the overlapping metabolic functions of
Figure 2. Metabolic and mitochondrial abnormalities in peripheral artery disease. FAD indicates flavin adenine dinucleotide; and NAD, nicotine adenine dinucleotide. Reprinted from Hiatt and Brass.32
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

Hiatt et al Exercise Limitation in Peripheral Artery Disease 1535
ERRα and ERRγ suggest potential benefit for patients with PAD, breast cancer association studies suggest that ERRα and ERRγ have differing effects on cancer progression, with high levels of ERRα associated with expression of ErbB2, in-creased risk of recurrence, and adverse clinical outcomes.161,162 Thus, careful choices of pharmacological agents will need to be made if mitochondrial biogenesis in patients with PAD will be attempted through ERR modulation. At this time, there is minimal literature reporting ERRγ modulators likely to be useful for experimental medicine hypothesis testing, leaving only small molecules associated with the unclear benefit/risk ratio of ERRα modulation available for use in the near future. Likewise, no facile methods to clinically modulate the impor-tant regulator of mitochondrial expression nuclear respiratory factor 1 exist at this time. Thus, both basic research and drug discovery in the area of mitochondrial biogenesis are newly needed to generate hypotheses and new targets for clinical testing.
ConclusionsPAD represents a complex pathophysiology that results in significant functional limitations in exercise performance. A dominant mechanism in the initiation of the exercise limita-tion is a reduction in exercise blood flow and oxygen delivery to exercising skeletal muscle in the lower extremity. This flow limitation is also associated with skeletal muscle ischemia with walking exercise and reperfusion with rest that set up a cas-cade of pathophysiological responses leading to further tissue injury, endothelial dysfunction, muscle metabolic abnormali-ties, and other changes that further reduce exercise capacity. Understanding these sequelae offers insights into mechanisms
underlying the reduced exercise performance in these patients and potential new targets for therapeutic interventions.
DisclosuresDr Hiatt reports grant awards in the past 2 years to CPC Clinical Research (a nonprofit academic research organization and affiliated to the University of Colorado) from the following sponsors: Aastrom, AstraZeneca, Bayer, National Institutes of Health, CSI, Cytokinetics, DNAVEC, Kowa, Kyushu University, Merck, Pluristem, Regeneron, Rigel, and Takeda. Dr Armstrong reports being a consultant in the past 2 years to Pfizer, Abbott Vascular, and Spectranetics. Dr Larson is an employee of Takeda Pharmaceuticals Company, Inc. Dr Brass reports being a consultant in the past 2 years to GlaxoSmithKline, Novartis, McNeil Consumer Pharmaceuticals, Novo Nordisk, 3D Communications, Catabasis Pharmaceuticals, Allergan, NovaDigm Therapeutics, Bayer, Endo Pharmaceuticals, Amgen, Boston Scientific, World Self-Medication Institute, Merck, NPS Pharmaceuticals, HeartWare International, Takeda Pharmaceuticals, Genzyme, Consumer Healthcare Products Association, DepoMed, Cangene, Aveo Oncology, BioMarin, Galderma, QRx Pharma, University of Washington, Amarin, EnteroMedics, Acerta, Cerexa, Kythera Biopharmaceuticals, and Trius Therapeutics. Dr Brass has equity in Calistoga Pharmaceuticals and Catabasis Pharmaceuticals. None of the authors received financial support for this article.
References 1. Libby P. Mechanisms of acute coronary syndromes and their implica-
tions for therapy. N Engl J Med. 2013;368:2004–2013. doi: 10.1056/NEJMra1216063.
2. Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ, Mensah GA, Criqui MH. Comparison of global estimates of prevalence and risk factors for periph-eral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329–1340. doi: 10.1016/S0140-6736(13)61249-0.
3. McDermott MM, Greenland P, Liu K, Guralnik JM, Criqui MH, Dolan NC, Chan C, Celic L, Pearce WH, Schneider JR, Sharma L, Clark E, Gibson D, Martin GJ. Leg symptoms in peripheral arterial disease: as-sociated clinical characteristics and functional impairment. JAMA. 2001;286:1599–1606.
4. Golomb BA, Dang TT, Criqui MH. Peripheral arterial disease: morbidity and mortality implications. Circulation. 2006;114:688–699. doi: 10.1161/CIRCULATIONAHA.105.593442.
5. Hirsch AT, Allison MA, Gomes AS, Corriere MA, Duval S, Ershow AG, Hiatt WR, Karas RH, Lovell MB, McDermott MM, Mendes DM, Nussmeier NA, Treat-Jacobson D; American Heart Association Council on Peripheral Vascular Disease; Council on Cardiovascular Nursing; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology; Council on Epidemiology and Prevention. A call to action: women and peripheral ar-tery disease: a scientific statement from the American Heart Association. Circulation. 2012;125:1449–1472. doi: 10.1161/CIR.0b013e31824c39ba.
6. Goldschmidt-Clermont PJ, Creager MA, Losordo DW, Lorsordo DW, Lam GK, Wassef M, Dzau VJ. Atherosclerosis 2005: recent discoveries and novel hypotheses. Circulation. 2005;112:3348–3353. doi: 10.1161/CIRCULATIONAHA.105.577460.
7. Bhatt DL, Steg PG, Ohman EM, Hirsch AT, Ikeda Y, Mas JL, Goto S, Liau CS, Richard AJ, Röther J, Wilson PW; REACH Registry Investigators. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006;295:180–189. doi: 10.1001/jama.295.2.180.
8. Berger JS, Hochman J, Lobach I, Adelman MA, Riles TS, Rockman CB. Modifiable risk factor burden and the prevalence of peripheral artery dis-ease in different vascular territories. J Vasc Surg. 2013;58:673–81.e1. doi: 10.1016/j.jvs.2013.01.053.
9. Grenon SM, Vittinghoff E, Owens CD, Conte MS, Whooley M, Cohen BE. Peripheral artery disease and risk of cardiovascular events in patients with coronary artery disease: insights from the Heart and Soul Study. Vasc Med. 2013;18:176–184. doi: 10.1177/1358863X13493825.
10. Brevetti G, Giugliano G, Brevetti L, Hiatt WR. Inflammation in periph-eral artery disease. Circulation. 2010;122:1862–1875. doi: 10.1161/CIRCULATIONAHA.109.918417.
Table 1. Mechanisms of Exercise Impairment in PAD
Healthy Physiology PAD Pathophysiology
Arterial flow Normal at rest, inadequate increment with exercise to meet metabolic demand
Endothelial and microvasculature dysfunction
Impaired endothelium-dependent vasodilation on exercise challenge
Inflammation Increase in plasma levels of numerous inflammatory mediators; inflammation-impaired actions of progenitor/satellite cell differentiation and responses and growth factors
Reactive oxygen species and oxidative/reductive stress
During ischemia, skeletal muscle mitochondria release free radicals, including superoxide and other reactive oxygen species that are derived from the oxidation–reduction cascade
Muscle structural abnormalities Muscle apoptosis and atrophy; fiber type switching; altered myosin heavy chain expression; fiber denervation
Muscle metabolic abnormalities Altered oxygen coupling and mitochondrial respiration: in patients with PAD, prolongation of the kinetic rates of oxygen consumption, and tissue hemoglobin desaturation has been described at the onset of exercise
PAD indicates peripheral artery disease.
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

1536 Circulation Research April 24, 2015
11. Steg PG, Bhatt DL, Wilson PW, D’Agostino R Sr, Ohman EM, Röther J, Liau CS, Hirsch AT, Mas JL, Ikeda Y, Pencina MJ, Goto S; REACH Registry Investigators. One-year cardiovascular event rates in outpa-tients with atherothrombosis. JAMA. 2007;297:1197–1206. doi: 10.1001/jama.297.11.1197.
12. Pande RL, Perlstein TS, Beckman JA, Creager MA. Secondary prevention and mortality in peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004. Circulation. 2011;124:17–23. doi: 10.1161/CIRCULATIONAHA.110.003954.
13. Hirsch AT, Criqui MH, Treat-Jacobson D, Regensteiner JG, Creager MA, Olin JW, Krook SH, Hunninghake DB, Comerota AJ, Walsh ME, McDermott MM, Hiatt WR. Peripheral arterial disease detection, aware-ness, and treatment in primary care. JAMA. 2001;286:1317–1324.
14. 2011 Writing Group Members; 2005 Writing Committee Members; ACCF/AHA Task Force Members. 2011 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Peripheral Artery Disease (Updating the 2005 Guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011;124:2020–2045. doi: 10.1161/CIR.0b013e31822e80c3.
15. Armstrong EJ, Chen DC, Westin GG, Singh S, McCoach CE, Bang H, Yeo KK, Anderson D, Amsterdam EA, Laird JR. Adherence to guide-line-recommended therapy is associated with decreased major adverse cardiovascular events and major adverse limb events among patients with peripheral arterial disease. J Am Heart Assoc. 2014;3:e000697. doi: 10.1161/JAHA.113.000697.
16. Aboyans V, Criqui MH, Abraham P, et al; American Heart Association Council on Peripheral Vascular Disease; Council on Epidemiology and Prevention; Council on Clinical Cardiology; Council on Cardiovascular Nursing; Council on Cardiovascular Radiology and Intervention, and Council on Cardiovascular Surgery and Anesthesia. Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association. Circulation. 2012;126:2890–2909. doi: 10.1161/CIR.0b013e318276fbcb.
17. von Ziegler F, Costa MA. The role of CT and MRI in the assessment of peripheral vascular disease. Curr Cardiol Rep. 2007;9:412–419.
18. McDermott MM, Mehta S, Greenland P. Exertional leg symptoms other than intermittent claudication are common in peripheral arterial disease. Arch Intern Med. 1999;159:387–392.
19. Smith GD, Shipley MJ, Rose G. Intermittent claudication, heart disease risk factors, and mortality. The Whitehall Study. Circulation. 1990;82:1925–1931.
20. McDermott MM, Guralnik JM, Ferrucci L, Tian L, Liu K, Liao Y, Green D, Sufit R, Hoff F, Nishida T, Sharma L, Pearce WH, Schneider JR, Criqui MH. Asymptomatic peripheral arterial disease is associ-ated with more adverse lower extremity characteristics than intermit-tent claudication. Circulation. 2008;117:2484–2491. doi: 10.1161/CIRCULATIONAHA.107.736108.
21. Hiatt WR, Nawaz D, Regensteiner JG, Hossack KF. The evaluation of exercise performance in patients with peripheral vascular disease. J Cardiopulmonary Rehabil. 1988;12:525–532.
22. Gardner AW. Claudication pain and hemodynamic responses to exercise in younger and older peripheral arterial disease patients. J Gerontol. 1993;48:M231–M236.
23. Gardner AW, Killewich LA, Katzel LI, Womack CJ, Montgomery PS, Otis RB, Fonong T. Relationship between free-living daily physical activ-ity and peripheral circulation in patients with intermittent claudication. Angiology. 1999;50:289–297.
24. Gardner AW, Poehlman ET. Assessment of free-living daily physical activ-ity in older claudicants: validation against the doubly labeled water tech-nique. J Gerontol A Biol Sci Med Sci. 1998;53:M275–M280.
25. McDermott MM, Greenland P, Ferrucci L, Criqui MH, Liu K, Sharma L, Chan C, Celic L, Priyanath A, Guralnik JM. Lower extremity performance is associated with daily life physical activity in individuals with and with-out peripheral arterial disease. J Am Geriatr Soc. 2002;50:247–255.
26. McDermott MM, Liu K, Greenland P, Guralnik JM, Criqui MH, Chan C, Pearce WH, Schneider JR, Ferrucci L, Celic L, Taylor LM, Vonesh E, Martin GJ, Clark E. Functional decline in peripheral arterial disease: associations with the ankle brachial index and leg symptoms. JAMA. 2004;292:453–461. doi: 10.1001/jama.292.4.453.
27. Wheeler EC, Brenner ZR. Peripheral vascular anatomy, physiology, and pathophysiology. AACN Clin Issues. 1995;6:505–514.
28. Pfitzner J. Poiseuille and his law. Anaesthesia. 1976;31:273–275. 29. Hlavová J, Linhart J, Prerovský I, Ganz V, Fronĕk A. Leg blood flow at
rest, during and after exercise in normal subjects and in patients with fem-oral artery occlusion. Clin Sci. 1965;29:555–564.
30. Karayannacos PE, Talukder N, Nerem RM, Roshon S, Vasko JS. The role of multiple noncritical arterial stenoses in the pathogenesis of ischemia. J Thorac Cardiovasc Surg. 1977;73:458–469.
31. Sørlie D, Myhre K. Lower leg blood flow in intermittent claudication. Scand J Clin Lab Invest. 1978;38:171–179.
32. Hiatt WR, Brass EP. Pathophysiology of intermittent claudication. In: Creager MA, Dzau VJ, Loscalzo J, eds. Vascular Medicine: A Companion to Braunwald’s Heart Disease. 2nd ed. Philadelphia: Saunders Elsevier; 2013;223–230.
33. Hansen JE, Sue DY, Oren A, Wasserman K. Relation of oxygen uptake to work rate in normal men and men with circulatory disorders. Am J Cardiol. 1987;59:669–674.
34. Hiatt WR, Marsh RC, Brammell HL, Fee C, Horwitz LD. Effect of aerobic conditioning on the peripheral circulation during chronic beta-adrenergic blockade. J Am Coll Cardiol. 1984;4:958–963.
35. Wasserman K. Coupling of external to cellular respiration during exercise: the wisdom of the body revisited. Am J Physiol. 1994;266:E519–E539.
36. Bragadeesh T, Sari I, Pascotto M, Micari A, Kaul S, Lindner JR. Detection of peripheral vascular stenosis by assessing skeletal muscle flow reserve. J Am Coll Cardiol. 2005;45:780–785. doi: 10.1016/j.jacc.2004.11.045.
37. Young DF, Cholvin NR, Kirkeeide RL, Roth AC. Hemodynamics of arte-rial stenoses at elevated flow rates. Circ Res. 1977;41:99–107.
38. Opolski MP, Pregowski J, Kruk M, Kepka C, Staruch AD, Witkowski A. Advanced 2-dimensional quantitative coronary angiographic analy-sis for prediction of fractional flow reserve in intermediate coro-nary stenoses. J Thorac Imaging. 2014;29:217–223. doi: 10.1097/RTI.0000000000000058.
39. Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van’ t Veer M, Klauss V, Manoharan G, Engstrøm T, Oldroyd KG, Ver Lee PN, MacCarthy PA, Fearon WF; FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary interven-tion. N Engl J Med. 2009;360:213–224. doi: 10.1056/NEJMoa0807611.
40. Lotfi AS, Sivalingam SK, Giugliano GR, Ashraf J, Visintainer P. Use of fraction flow reserve to predict changes over time in management of superficial femoral artery. J Interv Cardiol. 2012;25:71–77. doi: 10.1111/j.1540-8183.2011.00691.x.
41. Ledermann HP, Schulte AC, Heidecker HG, Aschwanden M, Jäger KA, Scheffler K, Steinbrich W, Bilecen D. Blood oxygenation level-dependent magnetic resonance imaging of the skeletal muscle in patients with pe-ripheral arterial occlusive disease. Circulation. 2006;113:2929–2935. doi: 10.1161/CIRCULATIONAHA.105.605717.
42. Roseguini BT, Hirai DM, Alencar MC, Ramos RP, Silva BM, Wolosker N, Neder JA, Nery LE. Sildenafil improves skeletal muscle oxygenation during exercise in men with intermittent claudication. Am J Physiol Regul Integr Comp Physiol. 2014;307:R396–R404. doi: 10.1152/ajpregu.00183.2014.
43. Hickner RC, Fisher JS, Ehsani AA, Kohrt WM. Role of nitric oxide in skeletal muscle blood flow at rest and during dynamic exercise in humans. Am J Physiol. 1997;273:H405–H410.
44. Liao JK, Bettmann MA, Sandor T, Tucker JI, Coleman SM, Creager MA. Differential impairment of vasodilator responsiveness of peripheral resistance and conduit vessels in humans with atherosclerosis. Circ Res. 1991;68:1027–1034.
45. Schellong SM, Böger RH, Burchert W, Bode-Böger SM, Galland A, Frölich JC, Hundeshagen H, Alexander K. Dose-related effect of intrave-nous L-arginine on muscular blood flow of the calf in patients with periph-eral vascular disease: a H215O positron emission tomography study. Clin Sci (Lond). 1997;93:159–165.
46. Tsao PS, Buitrago R, Chang H, Chen UDI, Reaven GM. Effects of dia-betes on monocyte-endothelial interactions and endothelial superoxide production in fructose-induced insulin-resistant and hypertensive rats. Circulation. 1995;92:A2666.
47. Mangiafico RA, Malatino LS, Spada RS, Santonocito M, Messina R, Dell’Arte S, Attinà T. Treadmill exercise-induced release of endothelin-1 in patients with peripheral arterial occlusive disease at Fontaine stage IIb. Int Angiol. 2000;19:14–17.
48. Brevetti G, Silvestro A, Di Giacomo S, Bucur R, Di Donato A, Schiano V, Scopacasa F. Endothelial dysfunction in peripheral arterial disease is related to increase in plasma markers of inflammation and severity of pe-ripheral circulatory impairment but not to classic risk factors and athero-sclerotic burden. J Vasc Surg. 2003;38:374–379.
49. Grenon SM, Chong K, Alley H, Nosova E, Gasper W, Hiramoto J, Boscardin WJ, Owens CD. Walking disability in patients with peripheral artery disease is associated with arterial endothelial function. J Vasc Surg. 2014;59:1025–1034. doi: 10.1016/j.jvs.2013.10.084.
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from

Hiatt et al Exercise Limitation in Peripheral Artery Disease 1537
50. Coutinho T, Rooke TW, Kullo IJ. Arterial dysfunction and functional per-formance in patients with peripheral artery disease: a review. Vasc Med. 2011;16:203–211. doi: 10.1177/1358863X11400935.
51. Silvestro A, Scopacasa F, Ruocco A, Oliva G, Schiano V, Zincarelli C, Brevetti G. Inflammatory status and endothelial function in asymptomatic and symptomatic peripheral arterial disease. Vasc Med. 2003;8:225–232.
52. Brendle DC, Joseph LJ, Corretti MC, Gardner AW, Katzel LI. Effects of exercise rehabilitation on endothelial reactivity in older patients with pe-ripheral arterial disease. Am J Cardiol. 2001;87:324–329.
53. Januszek R, Mika P, Konik A, Petriczek T, Nowobilski R, Niżankowski R. Effect of treadmill training on endothelial function and walking abilities in patients with peripheral arterial disease. J Cardiol. 2014;64:145–151. doi: 10.1016/j.jjcc.2013.12.002.
54. Baltgalvis KA, White K, Li W, et al. Exercise performance and peripheral vascular insufficiency improve with AMPK activation in high-fat diet-fed mice. Am J Physiol Heart Circ Physiol. 2014;306:H1128–H1145. doi: 10.1152/ajpheart.00839.2013.
55. Wu WC, Mohler E 3rd, Ratcliffe SJ, Wehrli FW, Detre JA, Floyd TF. Skeletal muscle microvascular flow in progressive peripheral artery disease: assessment with continuous arterial spin-labeling perfusion magnetic resonance imaging. J Am Coll Cardiol. 2009;53:2372–2377. doi: 10.1016/j.jacc.2009.03.033.
56. Pollak AW, Meyer CH, Epstein FH, Jiji RS, Hunter JR, Dimaria JM, Christopher JM, Kramer CM. Arterial spin labeling MR imaging repro-ducibly measures peak-exercise calf muscle perfusion: a study in patients with peripheral arterial disease and healthy volunteers. JACC Cardiovasc Imaging. 2012;5:1224–1230. doi: 10.1016/j.jcmg.2012.03.022.
57. Lindner JR, Womack L, Barrett EJ, Weltman J, Price W, Harthun NL, Kaul S, Patrie JT. Limb stress-rest perfusion imaging with contrast ultrasound for the assessment of peripheral arterial disease severity. JACC Cardiovasc Imaging. 2008;1:343–350. doi: 10.1016/j.jcmg.2008.04.001.
58. Anderson JD, Epstein FH, Meyer CH, Hagspiel KD, Wang H, Berr SS, Harthun NL, Weltman A, Dimaria JM, West AM, Kramer CM. Multifactorial determinants of functional capacity in peripheral arterial disease: uncoupling of calf muscle perfusion and metabolism. J Am Coll Cardiol. 2009;54:628–635. doi: 10.1016/j.jacc.2009.01.080.
59. Woodburn KR, Lowe GD, Rumley A, Love J, Pollock JG. Relation of hae-mostatic, fibrinolytic, and rheological variables to the angiographic extent of peripheral arterial occlusive disease. Int Angiol. 1995;14:346–352.
60. Dormandy JA, Hoare E, Colley J, Arrowsmith DE, Dormandy TL. Clinical, haemodynamic, rheological, and biochemical findings in 126 patients with intermittent claudication. Br Med J. 1973;4:576–581.
61. Lowe GD, Fowkes FG, Dawes J, Donnan PT, Lennie SE, Housley E. Blood viscosity, fibrinogen, and activation of coagulation and leukocytes in peripheral arterial disease and the normal population in the Edinburgh Artery Study. Circulation. 1993;87:1915–1920.
62. Fowkes FG, Lowe GD, Housley E, Rattray A, Rumley A, Elton RA, MacGregor IR, Dawes J. Cross-linked fibrin degradation products, progres-sion of peripheral arterial disease, and risk of coronary heart disease. Lancet. 1993;342:84–86.
63. Pande RL, Hiatt WR, Zhang P, Hittel N, Creager MA. A pooled analy-sis of the durability and predictors of treatment response of cilostazol in patients with intermittent claudication. Vasc Med. 2010;15:181–188. doi: 10.1177/1358863X10361545.
64. Brass EP. Intermittent claudication: new targets for drug development. Drugs. 2013;73:999–1014. doi: 10.1007/s40265-013-0078-3.
65. Money SR, Herd JA, Isaacsohn JL, Davidson M, Cutler B, Heckman J, Forbes WP. Effect of cilostazol on walking distances in patients with in-termittent claudication caused by peripheral vascular disease. J Vasc Surg. 1998;27:267–74; discussion 274.
66. Brass EP, Anthony R, Cobb FR, Koda I, Jiao J, Hiatt WR. The novel phosphodiesterase inhibitor NM-702 improves claudication-limited exer-cise performance in patients with peripheral arterial disease. J Am Coll Cardiol. 2006;48:2539–2545. doi: 10.1016/j.jacc.2006.07.064.
67. Brass EP, Cooper LT, Morgan RE, Hiatt WR. A phase II dose-ranging study of the phosphodiesterase inhibitor K-134 in patients with peripheral artery disease and claudication. J Vasc Surg. 2012;55:381–389.e1. doi: 10.1016/j.jvs.2011.09.004.
68. Salhiyyah K, Senanayake E, Abdel-Hadi M, Booth A, Michaels JA. Pentoxifylline for intermittent claudication. Cochrane Database Syst Rev. 2012;1:CD005262. doi: 10.1002/14651858.CD005262.pub2.
69. Stevens JW, Simpson E, Harnan S, Squires H, Meng Y, Thomas S, Michaels J, Stansby G. Systematic review of the efficacy of cilostazol, naftidrofuryl oxalate and pentoxifylline for the treatment of intermittent claudication. Br J Surg. 2012;99:1630–1638. doi: 10.1002/bjs.8895.
70. de Backer TL, Vander Stichele R, Lehert P, Van Bortel L. Naftidrofuryl for intermittent claudication. Cochrane Database Syst Rev. 2012;12:CD001368. doi: 10.1002/14651858.CD001368.pub4.
71. Barradell LB, Brogden RN. Oral naftidrofuryl. A review of its pharmacol-ogy and therapeutic use in the management of peripheral occlusive arterial disease. Drugs Aging. 1996;8:299–322.
72. Bendermacher BL, Willigendael EM, Teijink JA, Prins MH. Supervised exercise therapy versus non-supervised exercise therapy for intermittent claudication. Cochrane Database Syst Rev. 2006;2:CD005263.
73. Hiatt WR, Regensteiner JG, Wolfel EE, Carry MR, Brass EP. Effect of ex-ercise training on skeletal muscle histology and metabolism in peripheral arterial disease. J Appl Physiol (1985). 1996;81:780–788.
74. Hiatt WR, Wolfel EE, Meier RH, Regensteiner JG. Superiority of tread-mill walking exercise versus strength training for patients with peripheral arterial disease. Implications for the mechanism of the training response. Circulation. 1994;90:1866–1874.
75. Murphy TP, Cutlip DE, Regensteiner JG, et al; CLEVER Study Investigators. Supervised exercise versus primary stenting for claudication resulting from aortoiliac peripheral artery disease: six-month outcomes from the claudication: exercise versus endoluminal revascularization (CLEVER) study. Circulation. 2012;125:130–139. doi: 10.1161/CIRCULATIONAHA.111.075770.
76. Hiatt WR, Creager MA, Amato A, Brass EP. Effect of propionyl-L-car-nitine on a background of monitored exercise in patients with claudica-tion secondary to peripheral artery disease. J Cardiopulm Rehabil Prev. 2011;31:125–132. doi: 10.1097/HCR.0b013e3181f1fd65.
77. Pernow B, Zetterquist S. Metabolic evaluation of the leg blood flow in claudicating patients with arterial obstructions at different levels. Scand J Clin Lab Invest. 1968;21:277–287.
78. Szuba A, Oka RK, Harada R, Cooke JP. Limb hemodynamics are not predic-tive of functional capacity in patients with PAD. Vasc Med. 2006;11:155–163.
79. Hiatt WR, Regensteiner JG, Hargarten ME, Wolfel EE, Brass EP. Benefit of exercise conditioning for patients with peripheral arterial disease. Circulation. 1990;81:602–609.
80. Hynynen MM, Khalil RA. The vascular endothelin system in hyperten-sion–recent patents and discoveries. Recent Pat Cardiovasc Drug Discov. 2006;1:95–108.
81. Vatter H, Seifert V. Ambrisentan, a non-peptide endothelin receptor antagonist. Cardiovasc Drug Rev. 2006;24:63–76. doi: 10.1111/j.1527-3466.2006.00063.x.
82. Hong IS, Coe HV, Catanzaro LM. Macitentan for the treatment of pul-monary arterial hypertension. Ann Pharmacother. 2014;48:538–547. doi: 10.1177/1060028013518900.
83. Iglarz M, Binkert C, Morrison K, Fischli W, Gatfield J, Treiber A, Weller T, Bolli MH, Boss C, Buchmann S, Capeleto B, Hess P, Qiu C, Clozel M. Pharmacology of macitentan, an orally active tissue-targeting dual endo-thelin receptor antagonist. J Pharmacol Exp Ther. 2008;327:736–745. doi: 10.1124/jpet.108.142976.
84. Forst T, Lübben G, Hohberg C, Kann P, Sachara C, Gottschall V, Friedrich C, Rosskopf R, Pfützner A. Influence of glucose control and improvement of insulin resistance on microvascular blood flow and endothelial function in patients with diabetes mellitus type 2. Microcirculation. 2005;12:543–550. doi: 10.1080/10739680500253402.
85. Martens FM, Visseren FL, de Koning EJ, Rabelink TJ. Short-term piogli-tazone treatment improves vascular function irrespective of metabolic changes in patients with type 2 diabetes. J Cardiovasc Pharmacol. 2005;46:773–778.
86. Tsuchiya K, Akaza I, Yoshimoto T, Hirata Y. Pioglitazone improves endo-thelial function with increased adiponectin and high-density lipoprotein cholesterol levels in type 2 diabetes. Endocr J. 2009;56:691–698.
87. Edwards AT, Blann AD, Suarez-Mendez VJ, Lardi AM, McCollum CN. Systemic responses in patients with intermittent claudication after tread-mill exercise. Br J Surg. 1994;81:1738–1741.
88. Belch JJ, McLaren M, Khan F, Hickman P, Muir AH, Stonebridge PA. The inflammatory process in intermittent claudication. Eur Heart J. 2002;4:B31–B34. doi: 10.1016/S1520-765X(02)90014-3.
89. Belch JJ, Mackay IR, Hill A, Jennings P, McCollum P. Oxidative stress is present in atherosclerotic peripheral arterial disease and further increased by diabetes mellitus. Int Angiol. 1995;14:385–388.
90. Brevetti G, De Caterina M, Martone VD, Ungaro B, Corrado F, Silvestro A, de Cristofaro T, Scopacasa F. Exercise increases soluble adhesion mol-ecules ICAM-1 and VCAM-1 in patients with intermittent claudication. Clin Hemorheol Microcirc. 2001;24:193–199.
91. Signorelli SS, Mazzarino MC, Di Pino L, Malaponte G, Porto C, Pennisi G, Marchese G, Costa MP, Digrandi D, Celotta G, Virgilio V. High cir-culating levels of cytokines (IL-6 and TNFalpha), adhesion molecules (VCAM-1 and ICAM-1) and selectins in patients with peripheral arterial disease at rest and after a treadmill test. Vasc Med. 2003;8:15–19.
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from
1538 Circulation Research April 24, 2015
92. Blann AD, Dobrotova M, Kubisz P, McCollum CN. von Willebrand fac-tor, soluble P-selectin, tissue plasminogen activator and plasminogen ac-tivator inhibitor in atherosclerosis. Thromb Haemost. 1995;74:626–630.
93. Gardner AW, Parker DE, Montgomery PS, Sosnowska D, Casanegra AI, Esponda OL, Ungvari Z, Csiszar A, Sonntag WE. Impaired vas-cular endothelial growth factor A and inflammation in patients with peripheral artery disease. Angiology. 2014;65:683–690. doi: 10.1177/0003319713501376.
94. Nylaende M, Kroese A, Stranden E, Morken B, Sandbaek G, Lindahl AK, Arnesen H, Seljeflot I. Markers of vascular inflammation are associ-ated with the extent of atherosclerosis assessed as angiographic score and treadmill walking distances in patients with peripheral arterial occlusive disease. Vasc Med. 2006;11:21–28.
95. McDermott MM, Greenland P, Green D, Guralnik JM, Criqui MH, Liu K, Chan C, Pearce WH, Taylor L, Ridker PM, Schneider JR, Martin G, Rifai N, Quann M, Fornage M. D-dimer, inflammatory markers, and lower extremity functioning in patients with and without periph-eral arterial disease. Circulation. 2003;107:3191–3198. doi: 10.1161/01.CIR.0000074227.53616.CC.
96. McDermott MM, Liu K, Guralnik JM, Ferrucci L, Green D, Greenland P, Tian L, Criqui MH, Lo C, Rifai N, Ridker PM, Zheng J, Pearce W. Functional decline in patients with and without peripheral arterial dis-ease: predictive value of annual changes in levels of C-reactive protein and D-dimer. J Gerontol A Biol Sci Med Sci. 2006;61:374–379.
97. Brass EP, Cooper LT, Hanson P, Hiatt WR. Association of clinical at-tributes and treadmill walking performance in patients with claudication due to peripheral artery disease. J Vasc Surg. 2013;58:396–403. doi: 10.1016/j.jvs.2012.12.077.
98. Dröse S, Brandt U. Molecular mechanisms of superoxide production by the mitochondrial respiratory chain. Adv Exp Med Biol. 2012;748:145–169. doi: 10.1007/978-1-4614-3573-0_6.
99. Hickman P, Harrison DK, Hill A, McLaren M, Tamei H, McCollum PT, Belch JJ. Exercise in patients with intermittent claudication results in the generation of oxygen derived free radicals and endothelial damage. Adv Exp Med Biol. 1994;361:565–570.
100. Ciuffetti G, Mercuri M, Mannarino E, Ott C, Lombardini R, Pasqualini L, Lupattelli G, Santambrogio L. Free radical production in peripheral vas-cular disease. A risk for critical ischaemia? Int Angiol. 1991;10:81–87.
101. Melov S, Shoffner JM, Kaufman A, Wallace DC. Marked increase in the number and variety of mitochondrial DNA rearrangements in aging hu-man skeletal muscle. Nucleic Acids Res. 1995;23:4122–4126.
102. Bhat HK, Hiatt WR, Hoppel CL, Brass EP. Skeletal muscle mitochon-drial DNA injury in patients with unilateral peripheral arterial disease. Circulation. 1999;99:807–812.
103. Ji LL. Modulation of skeletal muscle antioxidant defense by exercise: role of redox signaling. Free Radic Biol Med. 2008;44:142–152. doi: 10.1016/j.freeradbiomed.2007.02.031.
104. Oh-ishi S, Kizaki T, Nagasawa J, Izawa T, Komabayashi T, Nagata N, Suzuki K, Taniguchi N, Ohno H. Effects of endurance training on super-oxide dismutase activity, content and mRNA expression in rat muscle. Clin Exp Pharmacol Physiol. 1997;24:326–332.
105. Vassilakopoulos T, Deckman G, Kebbewar M, Rallis G, Harfouche R, Hussain SN. Regulation of nitric oxide production in limb and ventila-tory muscles during chronic exercise training. Am J Physiol Lung Cell Mol Physiol. 2003;284:L452–L457. doi: 10.1152/ajplung.00270.2002.
106. Sumida S, Nakamura H, Yodoi J. Thioredoxin induction of peripheral blood mononuclear cells in mice in response to a single bout of swim-ming exercise. Gen Physiol Biophys. 2004;23:241–249.
107. Naldini A, Carraro F. Role of inflammatory mediators in angiogenesis. Curr Drug Targets Inflamm Allergy. 2005;4:3–8.
108. Gahmberg CG, Tolvanen M, Kotovuori P. Leukocyte adhesion–structure and function of human leukocyte beta2-integrins and their cellular li-gands. Eur J Biochem. 1997;245:215–232.
109. Comi G. Treatment of multiple sclerosis: role of natalizumab. Neurol Sci. 2009;30 Suppl 2:S155–S158. doi: 10.1007/s10072-009-0147-2.
110. Schmidt KJ, Büning J, Jankowiak C, Lehnert H, Fellermann K. Crohn’s targeted therapy: myth or real goal? Curr Drug Discov Technol. 2009;6:290–298.
111. Enlinomab Acute Stroke Investigators. Use of anti-ICAM-1 therapy in ischemic stroke: results of the Enlimomab Acute Stroke Trial. Neurology. 2001;57:1428–1434.
112. Lin KC, Castro AC. Very late antigen 4 (VLA4) antagonists as anti-in-flammatory agents. Curr Opin Chem Biol. 1998;2:453–457.
113. Tardif JC, Tanguay JF, Wright SS, Duchatelle V, Petroni T, Grégoire JC, Ibrahim R, Heinonen TM, Robb S, Bertrand OF, Cournoyer D, Johnson
D, Mann J, Guertin MC, L’Allier PL. Effects of the P-selectin antago-nist inclacumab on myocardial damage after percutaneous coronary in-tervention for non-ST-segment elevation myocardial infarction: results of the SELECT-ACS trial. J Am Coll Cardiol. 2013;61:2048–2055. doi: 10.1016/j.jacc.2013.03.003.
114. Kling D, Stucki C, Kronenberg S, Tuerck D, Rhéaume E, Tardif JC, Gaudreault J, Schmitt C. Pharmacological control of platelet-leukocyte interactions by the human anti-P-selectin antibody inclacumab–preclini-cal and clinical studies. Thromb Res. 2013;131:401–410. doi: 10.1016/j.thromres.2013.02.020.
115. Ahimastos AA, Walker PJ, Askew C, Leicht A, Pappas E, Blombery P, Reid CM, Golledge J, Kingwell BA. Effect of ramipril on walking times and quality of life among patients with peripheral artery disease and intermittent claudication: a randomized controlled trial. JAMA. 2013;309:453–460. doi: 10.1001/jama.2012.216237.
116. Ahimastos AA, Latouche C, Natoli AK, Reddy-luthmoodoo M, Golledge J, Kingwell BA. Potential vascular mechanisms of ramipril induced increases in walking ability in patients with intermittent clau-dication. Circ Res. 2014;114:1144–1155. doi: 10.1161/CIRCRESAHA. 114.302420.
117. Shahin Y, Mazari F, Chetter I. Do angiotensin converting enzyme in-hibitors improve walking distance in patients with symptomatic lower limb arterial disease? A systematic review and meta-analysis of ran-domised controlled trials. Int J Surg. 2011;9:209–213. doi: 10.1016/j.ijsu.2010.12.006.
118. Brass EP, Koster D, Hiatt WR, Amato A. A systematic review and meta-analysis of propionyl-L-carnitine effects on exercise perfor-mance in patients with claudication. Vasc Med. 2013;18:3–12. doi: 10.1177/1358863X12467491.
119. LaRosa JC, He J, Vupputuri S. Effect of statins on risk of coronary disease: a meta-analysis of randomized controlled trials. JAMA. 1999;282:2340–2346.
120. Hiatt WR, Hirsch AT, Creager MA, Rajagopalan S, Mohler ER, Ballantyne CM, Regensteiner JG, Treat-Jacobson D, Dale RA, Rooke T. Effect of niacin ER/lovastatin on claudication symptoms in pa-tients with peripheral artery disease. Vasc Med. 2010;15:171–179. doi: 10.1177/1358863X09360579.
121. Mohler ER 3rd, Hiatt WR, Creager MA. Cholesterol reduction with atorvastatin improves walking distance in patients with peripheral ar-terial disease. Circulation. 2003;108:1481–1486. doi: 10.1161/01.CIR.0000090686.57897.F5.
122. Regensteiner JG, Wolfel EE, Brass EP, Carry MR, Ringel SP, Hargarten ME, Stamm ER, Hiatt WR. Chronic changes in skeletal muscle his-tology and function in peripheral arterial disease. Circulation. 1993;87:413–421.
123. Askew CD, Green S, Walker PJ, Kerr GK, Green AA, Williams AD, Febbraio MA. Skeletal muscle phenotype is associated with exer-cise tolerance in patients with peripheral arterial disease. J Vasc Surg. 2005;41:802–807. doi: 10.1016/j.jvs.2005.01.037.
124. McGuigan MR, Bronks R, Newton RU, Sharman MJ, Graham JC, Cody DV, Kraemer WJ. Muscle fiber characteristics in patients with peripheral arterial disease. Med Sci Sports Exerc. 2001;33:2016–2021.
125. Mitchell RG, Duscha BD, Robbins JL, Redfern SI, Chung J, Bensimhon DR, Kraus WE, Hiatt WR, Regensteiner JG, Annex BH. Increased levels of apoptosis in gastrocnemius skeletal muscle in patients with peripheral arterial disease. Vasc Med. 2007;12:285–290. doi: 10.1177/1358863X07084858.
126. McDermott MM, Ferrucci L, Guralnik JM, Tian L, Green D, Liu K, Tan J, Liao Y, Pearce WH, Schneider JR, Ridker P, Rifai N, Hoff F, Criqui MH. Elevated levels of inflammation, d-dimer, and homocysteine are associated with adverse calf muscle characteristics and reduced calf strength in peripheral arterial disease. J Am Coll Cardiol. 2007;50:897–905. doi: 10.1016/j.jacc.2007.05.017.
127. Steinacker JM, Opitz-Gress A, Baur S, Lormes W, Bolkart K, Sunder-Plassmann L, Liewald F, Lehmann M, Liu Y. Expression of myosin heavy chain isoforms in skeletal muscle of patients with peripheral arte-rial occlusive disease. J Vasc Surg. 2000;31:443–449.
128. England JD, Ferguson MA, Hiatt WR, Regensteiner JG. Progression of neuropathy in peripheral arterial disease. Muscle Nerve. 1995;18:380–387. doi: 10.1002/mus.880180403.
129. Garg PK, Liu K, Ferrucci L, Guralnik JM, Criqui MH, Tian L, Sufit R, Nishida T, Tao H, Liao Y, McDermott MM. Lower extremity nerve func-tion, calf skeletal muscle characteristics, and functional performance in peripheral arterial disease. J Am Geriatr Soc. 2011;59:1855–1863. doi: 10.1111/j.1532-5415.2011.03600.x.
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from
Hiatt et al Exercise Limitation in Peripheral Artery Disease 1539
130. McDermott MM, Ferrucci L, Guralnik J, Tian L, Liu K, Hoff F, Liao Y, Criqui MH. Pathophysiological changes in calf muscle predict mobility loss at 2-year follow-up in men and women with periph-eral arterial disease. Circulation. 2009;120:1048–1055. doi: 10.1161/CIRCULATIONAHA.108.842328.
131. McDermott MM, Liu K, Tian L, Guralnik JM, Criqui MH, Liao Y, Ferrucci L. Calf muscle characteristics, strength measures, and mortality in peripheral arterial disease: a longitudinal study. J Am Coll Cardiol. 2012;59:1159–1167. doi: 10.1016/j.jacc.2011.12.019.
132. Singh N, Liu K, Tian L, Criqui MH, Guralnik JM, Ferrucci L, Liao Y, McDermott MM. Leg strength predicts mortality in men but not in wom-en with peripheral arterial disease. J Vasc Surg. 2010;52:624–631. doi: 10.1016/j.jvs.2010.03.066.
133. Attie KM, Borgstein NG, Yang Y, Condon CH, Wilson DM, Pearsall AE, Kumar R, Willins DA, Seehra JS, Sherman ML. A single ascending-dose study of muscle regulator ACE-031 in healthy volunteers. Muscle Nerve. 2013;47:416–423. doi: 10.1002/mus.23539.
134. Campbell C, Escolar D, Mah J. A phase 2, randomized, placebo con-trolled, multiple ascending-dose study of ACE-031, a soluble activin receptor Type IIB, in boys with Duchenne muscular dystrophy (DMD). Neurology. 2012;78:P04.088.
135. Wagner KR, Fleckenstein JL, Amato AA, et al. A phase I/IItrial of MYO-029 in adult subjects with muscular dystrophy. Ann Neurol. 2008;63:561–571. doi: 10.1002/ana.21338.
136. Deleted in proof. 137. Lach-Trifilieff E, Minetti GC, Sheppard K, Ibebunjo C, Feige JN,
Hartmann S, Brachat S, Rivet H, Koelbing C, Morvan F, Hatakeyama S, Glass DJ. An antibody blocking activin type II receptors induces strong skeletal muscle hypertrophy and protects from atrophy. Mol Cell Biol. 2014;34:606–618. doi: 10.1128/MCB.01307-13.
138. Grassi B. Regulation of oxygen consumption at exercise onset: is it really controversial? Exerc Sport Sci Rev. 2001;29:134–138.
139. Bauer TA, Regensteiner JG, Brass EP, Hiatt WR. Oxygen uptake kinetics during exercise are slowed in patients with peripheral arterial disease. J Appl Physiol (1985). 1999;87:809–816.
140. Bauer TA, Brass EP, Barstow TJ, Hiatt WR. Skeletal muscle StO2 ki-netics are slowed during low work rate calf exercise in peripheral ar-terial disease. Eur J Appl Physiol. 2007;100:143–151. doi: 10.1007/s00421-007-0412-0.
141. Barker GA, Green S, Green AA, Walker PJ. Walking performance, oxy-gen uptake kinetics and resting muscle pyruvate dehydrogenase complex activity in peripheral arterial disease. Clin Sci (Lond). 2004;106:241–249. doi: 10.1042/CS20030244.
142. Kemp GJ, Hands LJ, Ramaswami G, Taylor DJ, Nicolaides A, Amato A, Radda GK. Calf muscle mitochondrial and glycogenolytic ATP syn-thesis in patients with claudication due to peripheral vascular disease analysed using 31P magnetic resonance spectroscopy. Clin Sci (Lond). 1995;89:581–590.
143. Rouslin W. Mitochondrial complexes I, II, III, IV, and V in myocardial ischemia and autolysis. Am J Physiol. 1983;244:H743–H748.
144. Brass EP, Hiatt WR, Gardner AW, Hoppel CL. Decreased NADH dehydrogenase and ubiquinol-cytochrome c oxidoreductase in peripheral arterial disease. Am J Physiol Heart Circ Physiol. 2001;280:H603–H609.
145. Patel RP, T Cornwell, Darley-Usmar VM. The biochemistry of nitric ox-ide and peroxynitrite: implications for mitochondrial function. In: Packer L, Cadenas E, eds. Understanding the Process of Aging: The Roles of Mitochondria, Free Radicals, and Antioxidants. New York, NY: Marcel Dekker. 1999;39–56.
146. Bieber LL. Carnitine. Annu Rev Biochem. 1988;57:261–283. doi: 10.1146/annurev.bi.57.070188.001401.
147. Brass EP, Hoppel CL. Relationship between acid-soluble carnitine and coenzyme A pools in vivo. Biochem J. 1980;190:495–504.
148. Hiatt WR, Nawaz D, Brass EP. Carnitine metabolism during exercise in patients with peripheral vascular disease. J Appl Physiol (1985). 1987;62:2383–2387.
149. Hiatt WR, Wolfel EE, Regensteiner JG, Brass EP. Skeletal muscle car-nitine metabolism in patients with unilateral peripheral arterial disease. J Appl Physiol (1985). 1992;73:346–353.
150. Barker GA, Green S, Green AA, Walker PJ. Walking performance, oxy-gen uptake kinetics and resting muscle pyruvate dehydrogenase complex activity in peripheral arterial disease. Clin Sci (Lond). 2004;106:241–249. doi: 10.1042/CS20030244.
151. Andreux PA, Houtkooper RH, Auwerx J. Pharmacological approaches to restore mitochondrial function. Nat Rev Drug Discov. 2013;12:465–483. doi: 10.1038/nrd4023.
152. Hou XY, Green S, Askew CD, Barker G, Green A, Walker PJ. Skeletal muscle mitochondrial ATP production rate and walking perfor-mance in peripheral arterial disease. Clin Physiol Funct Imaging. 2002;22:226–232.
153. Russell AP, Feilchenfeldt J, Schreiber S, Praz M, Crettenand A, Gobelet C, Meier CA, Bell DR, Kralli A, Giacobino JP, Dériaz O. Endurance training in humans leads to fiber type-specific increases in levels of per-oxisome proliferator-activated receptor-gamma coactivator-1 and peroxi-some proliferator-activated receptor-alpha in skeletal muscle. Diabetes. 2003;52:2874–2881.
154. Kramer DM, Ahlsen M, Norrbom J, Jansson E, Hjeltnes N, Gustafsson T, Krook A. Human skeletal muscle fibre type variations corre-late with PPARα, PPARd and PGC-1α mRNA. Acta Physiol (Oxf).. 2006;188:207–216.
155. Peters JM, Foreman JE, Gonzalez FJ. Dissecting the role of peroxisome proliferator-activated receptor-β/δ (PPARβ/δ) in colon, breast, and lung carcinogenesis. Cancer Metastasis Rev. 2011;30:619–640. doi: 10.1007/s10555-011-9320-1.
156. Kong X, Wang R, Xue Y, Liu X, Zhang H, Chen Y, Fang F, Chang Y. Sirtuin 3, a new target of PGC-1alpha, plays an important role in the suppression of ROS and mitochondrial biogenesis. PLoS One. 2010;5:e11707. doi: 10.1371/journal.pone.0011707.
157. Ranhotra HS. Estrogen-related receptor alpha and mitochondria: tale of the titans. J Recept Signal Transduct Res. 2014;15:1–5.
158. Procaccio V, Bris C, Chao de la Barca JM, Oca F, Chevrollier A, Amati-Bonneau P, Bonneau D, Reynier P. Perspectives of drug-based neuropro-tection targeting mitochondria. Rev Neurol (Paris). 2014;170:390–400. doi: 10.1016/j.neurol.2014.03.005.
159. Shao D, Liu Y, Liu X, Zhu L, Cui Y, Cui A, Qiao A, Kong X, Liu Y, Chen Q, Gupta N, Fang F, Chang Y. PGC-1 beta-regulated mito-chondrial biogenesis and function in myotubes is mediated by NRF-1 and ERR alpha. Mitochondrion. 2010;10:516–527. doi: 10.1016/j.mito.2010.05.012.
160. Pokrywka A, Cholbinski P, Kaliszewski P, Kowalczyk K, Konczak D, Zembron-Lacny A. Metabolic modulators of the exercise response: doping control analysis of an agonist of the peroxisome proliferator-activated receptor δ (GW501516) and 5-aminoimidazole-4-carboxamide ribonucleotide (AICAR). J Physiol Pharmacol. 2014;65:469–476.
161. Ariazi EA, Clark GM, Mertz JE. Estrogen-related receptor alpha and estrogen-related receptor gamma associate with unfavorable and fa-vorable biomarkers, respectively, in human breast cancer. Cancer Res. 2002;62:6510–6518.
162. Suzuki T, Miki Y, Moriya T, Shimada N, Ishida T, Hirakawa H, Ohuchi N, Sasano H. Estrogen-related receptor alpha in human breast carcino-ma as a potent prognostic factor. Cancer Res. 2004;64:4670–4676. doi: 10.1158/0008-5472.CAN-04-0250.
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from
William R. Hiatt, Ehrin J. Armstrong, Christopher J. Larson and Eric P. BrassDisease
Pathogenesis of the Limb Manifestations and Exercise Limitations in Peripheral Artery
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 2015 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/CIRCRESAHA.116.3035662015;116:1527-1539Circ Res.
http://circres.ahajournals.org/content/116/9/1527World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Researchin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 11, 2018http://circres.ahajournals.org/
Dow
nloaded from