Embed Size (px)
Citation preview

Pathophysiological Changes in the Lungs DuringExtracorporeal Circulation
By Robert S. Cartwright, M.D., Thomas P. K. Lim, M.D., Ph.D.,Ulrich C. Luft, M.D., and William E. Palich, D.V.M.
• Management of the lungs during heart-lung bypass for cardiac surgery should bedirected toward minimizing possible adverseeffects resulting from gross alterations of per-f'usion and ventilation of the organ, thus per-mitting normal gas exchange to be resumedimmediately after termination of bypass. Sofar the approach to this end has been mainlyempirical, and various forms of static infla-tion, intermittent ventilation, or passive de-flation have been employed without knowledgeof the merits of each. Kottmeier and asso-ciates' reported an increased incidence ofperibronchial hemorrhage and patchy atel.ee-tasis when pulmonary ventilation was omittedduring animal heart-lung bypass procedures.The detrimental effects of an elevated pul-monary venous pressure on the lungs duringand following bypass have been frequentlydemonstrated.2 Schramel et al.3 found pulmo-nary diffusion capacity to be decreased fol-lowing thoracic operations and believed thisdeficiency was greater when heart-lung bypasswas utilized. Recent data4 suggested a signifi-cant reduction in pulmonary compliance fol-lowing open-heart surgery due t;o disturbedmechanics of breathing.
The present study was undertaken (a) toascertain the physiological implications ofbypass to pulmonary function with regard tothe quantity and quality of bronchial collat-eral blood flow, metabolic requirements of thelung tissue, and alterations of pulmonarycompliance, and (b) to establish the most suit-able management for maintaining an adequatecondition in the lungs and the systemic cir-culation. Some of the observations gained inthe experimental series were extended to sev-eral clinical cases.
From the 'Departments of Surgical Eesonrch andPhysiology, Lovelace Foundation, Albuquerque, NewMexico.
Supported by IT. S. Public Health Service GrantTT-4G47.
'Received for publication August; 4, 1961.
Circulation Research, Volume X, February 196S
MethodsA total of 29 experimental and 6S donor dogs
was used. The experimental nnimnls were anes-thetized with pcntobarbital sodium (30 mg./Kg..I.V.) and tracheotomized. Following heparinization(2 mg./Kg.), the femoral vessels were exposedbilaterally to monitor arterial and venous pres-sures and also to return the oxygenated bloodfrom the pump. Room air (nonhumidified) wasused in artificial respiration. In all animals, thechest was opened by a vertical incision splittingthe sternum and entering both pleural spaces.
A modified Kay-Cross rotating disk oxygena-tor"' ° primed with blood from the donor dogs wasutilized. A gas mixture having 2.0 ± 0.2 percent CO2 in O2 was delivered to the oxygenator ata rate of 3 to 4 L./min. Total body pel-fusionwas conducted for 60 to 80 minutes at flow ratesof 80 to 100 ml./Kg./inin. maintaining a meanarterial pressure of SO to 110 mm. Hg and anaverage esophageal temperature of 37 C.
Two animal preparations were used. In the firstpreparation, systemic, arterial and caval bloodflows and pressures were continuously monitored,while the coronary circulation was excluded fromthe perfusion by a clamp across the aorta andpulmonary artery at the level of the semilunarvalves with resulting hypoxic arrest of the heart.In addition, the left atrial blood was allowed todrain into a container (preparation A) (fig. 1).The second preparation differed from the firstin that coronary flow was left intact. Caval bloodflow including azygos venous return was directedto the oxygenator. Thus, the heart maintained itssinus rhythm throughout bypass (preparation B).In both preparations, care was taken to maintainleft atrial pressure 1 to 4 cm. HoO greater thanright atrial pressure by manually adjusting theheight of the venous receiving reservoir locatedbetween the oxygenator and the venae cavae. Thiswas done to avoid a possible reversal of bloodflow from the superior vena cava into the pul-monary veins by way of azygos-bronchial venouscommunication when the caval pressure exceedsthe left atrial pressure.
During bypass, the lungs were either (1)statically inflated with the surface of the lungsreaching the upper margin of the chest walls(7 to 15 cm. H20 pressure), (2) ventilated at1 to 6 L./min., or (3) allowed to remain deflated,the sequence being varied at random. In eacliinstance, after a steady state of 20 minutes, blood
131
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from

132 CARTWBIGHT, LIM, LTJPT, PALICH
.SVC
Rt Atrial Pressure
U Alriol Pressure
Arterial Pressure
FIGURE 1
Schematic (line/ram showing the pressure and flowmonitoring si/s/f»i during heart-lung bi/pass withcardiac arrest (preparation A). Superior venaeuro (SVC); inferior vena cara (1VC); rightrentrirle (HT') ; left auricle (LA); left rentride(LV): pulmonary arterii (PA); aorta (Ao).
s;i in pies were taken anaerobically from the systemicartery, vena eava, and pulmonary vein and wereanalyzed for O2 saturation, pCO2, and pH. Theexpired air during artificial respiration was col-lected in a Douglas bap, and the respiratory andblood gases were analyzed according: to methodsdescribed previously." Tn those animals havingintact coronary flow, the right atrial blood wassimilarly analyzed. The total peripheral resistancewas calculated by Frank's formula in absoluteunits.s Tn addition, pulmonary compliance wasmeasured by stepwiso increases of lung1 volumefrom the passively deflated condition up to S00ml. and by concomitant measurement of statictranspulmonary pressure. The latter was obtainedby a water manometer. Statistical methods usedin this work follow Snedecor.1'
ResultsEFFECTS OF VARIED INSUFFLATION OFBYPASSED LUNGS ON BLOOD GASES
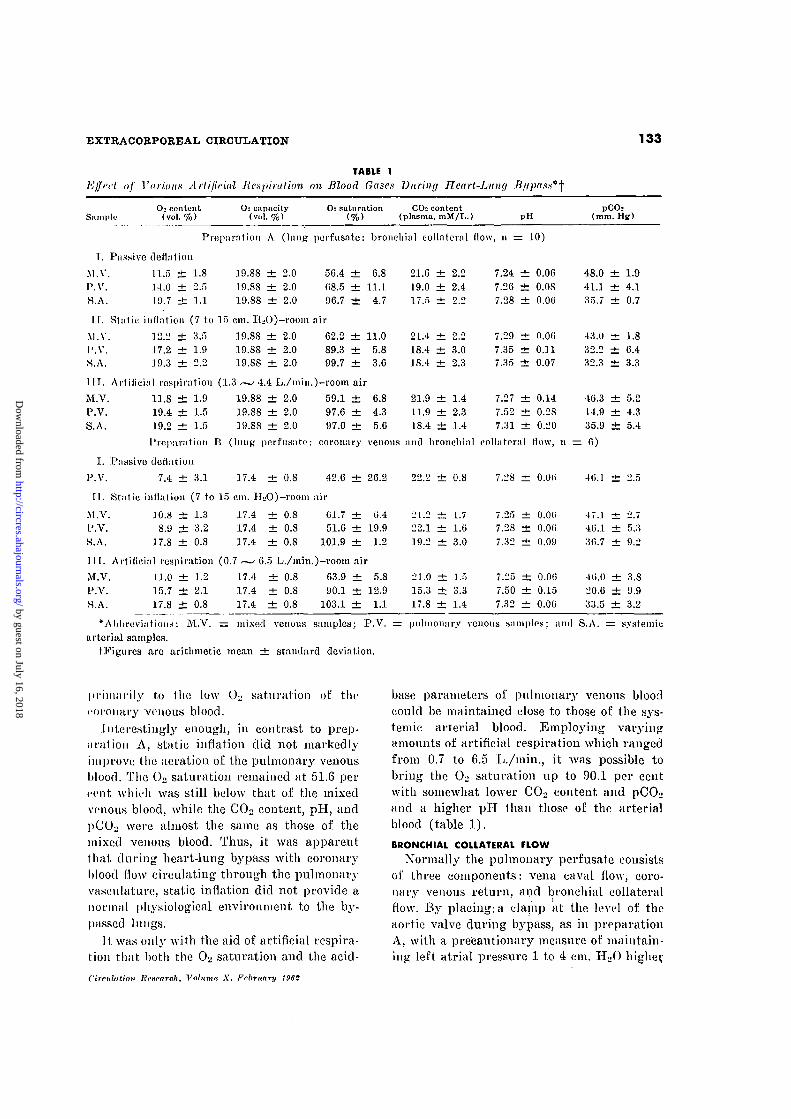
Three types of artificial lung insufflation,namely passive deflation, static inflation, andartificial respiration, were administered to 10animals of preparation A. Since the systemicand the coronary venous returns were pre-vented from entering the pulmonary vascularbeds in this preparation (see fig. 1), the bron-chial collateral flow constituted the sole per-fusate of the lungs. The data on the bloodgases during these maneuvers are summar-ized in table 1. When the pulmonary venous
FIGURE 2
Effect of controlled changes of superior vena carapressure on bronchial collateral flow (n — '>).Bronchial collateral flow (QI,.\)'I superior venacara pressure (Psrc)j left ('trial pressure (P,lA).
blood was compared with the systemic arterialblood during passive deflation, the formershowed consistently lower ()2 saturation andhigher CO2 tension and hydrogen ion concen-tration than the latter. These differencesamounted to 28 per cent of O2 saturation, 7mm. Hg of pCO2, and 0.02 units of pH andwere suggestive of appreciable exchanges of0;. and CO2 between the lung tissues and thepulinonary perfusate.
With static inflation of the bypassed lungswith room air, the ();> saturation, pCOo, andpll of the pulmonary venous blood approach-ed those noted in the systemic arterial blood,as shown in table 1. Except for O2 saturationwhich was still 89 per cent, static inflationrestored the chemical values (CO^ content,pCOL., and pll) of the pulmonary venousblood to practically the same levels as thesystemic arterial blood.
With artificial respiration, it was possibleto bring the O2 saturation of the pulmonaryvenous blood to the level of the systemic arte-rial blood. Nevertheless, this was achievedonly after considerable depletion of the CO-jreservoir as reflected in lowered COo andhigh pIT.
Tn preparation B, in which the lung per-fusate consisted of both coronary venous andbronchial collateral flow, O2 saturation ofpulmonary venous blood was markedly re-duced to 42.6 per cent during passive defla-tion of the lungs (table 1). This level wasmuch lower than that, of the mixed venousblood (approximately 20 per cent below) due
Circulation Research, Volume A*, Ffbrttary 1961
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from
EXTRACORPOREAL CIRCULATION 133
TABLE 1Effect of Various Artificial Respiration on Blood Gases During Heart-Lung
SampleO:< content
(vol. %)Ch capneity
(vol. %)O2 saturation CO: content
(plasma, mM/L.) pHpCOs
(mm. Hg)
Preparation A (lung perfusnto: bronchial eollnternl flow, 11 = 10)
T. Pnssivc deflation
M.V. 11.5 ± 1.8 1.9.88 ± 2.0 50.4 ± 6.8P.V. 14.0 ± 2.5 19.88 ± 2.0 08.5 ± 11.1.S.A. 19.7 ± 1.1 19.88 ± 2.0 96.7 ± 4.7
11. Static inflation (7 to 15 cm. H»0)-room air
M.V. 12.2 ± 3.5 19.88 ± 2.0 62.2 ± 11.0I'.V. 17.2 ± 1.9 .19.88 ± 2.0 89.3 ± 5.8S.A. 19.3 ± 2.2 19.88 ± 2.0 99.7 ± 3.6
111. Artificial respiration (1.3.— 4.4 L./inin.)—room air
M.V. 11.8 ± 1.9 19.88 ± 2.0 59.1 ± 6.8P.V. 19.4 ± 1.5 19.88 ± 2.0 97.6 ± 4.3S.A. 19.2 ± 1.5 19.88 ± 2.0 97.0 ± 5.6
I'reparation B (lung pcrfusate: coronary venous and bronchial collateral How, 11
I. Passive dodation
P.V. 7.4 ± 3.1 17.4 ± 0.8 42.6 ± 26.2
II. Static inflation (7 to 15 cm. H2O)-room air
M.V. .10.8 dz 1.3 17.4 ± 0.8 G1.7 ± C.4P.V. 8.9 ± 3.2 17.4 ± 0.8 51.6 ± 19.9S.A. 17.8 ± 0.8 17.4 ± 0.8 101.9 ± 1.2
111. Artificial respiration (0.7 —• 6.5 L./min.)-room air
M:.V. 11.0 ± 1.2 17.4 ± 0.8 63.9 ± 5.8P.V. 15.7 ± 2.1 17.4 ± 0.8 90.1 ± 12.9S.A. 17.8 ± 0.8 17.4 ± 0.8 103.1 ± 1.1
21.6 ± 2.219.0 ± 2.417.5 ± 2.2
21.4 ± 2.218.4 ± 3.018.4 ± 2.3
21.9 i t 1.411.9 ± 2.318.4 ± 1.4
22.2 ± 0.8
21.2 ± 1.722.1 ± 1.619.2 ± 3.0
21.0 ± 1.515.3 ± 3.317.8 dfc 1.4
7.24 ± 0.067.26 ± 0.087.28 ± 0.06
7.29 ± 0.067.35 ± 0.117.35 ± 0.07
7.27 ± 0.147.52 ± 0.287.31 ± 0.20
7.28 ± 0.01)
7.25 ± 0.007.28 ± O.Ofi7.32 ± 0.09
7.25 ± 0.0(57.50 ± 0.157.32 ± 0.06
48.0 ± 1.941.1 ± 4.135.7 ± 0.7
43.0 ± 1.832.2 ± 6.432.3 ± 3.3
46.3 ± 5.214.9 ± 4.3
35.9 ± 5.4
: 6)
46.1 ± 2.5
47.1 ± 2.746.1 ± 5.33(5.7 ± 9.2
46.0 ± 3.S20.6 ± 9.933.5 ± 3.2
•Abbreviations: M.V. = mixed venous samples; P.V. = pulmonary venous samples; and S.A. = systemicarterial samples.
tFiguros are arithmetic moan ± standard deviation.
primarily to the low OL. saturation of' thecoronary venous blood.
'Interestingly enough, in contrast to prep-aration A, static inflation did not markedlyimprove the aeration of the pulmonary venousblood. The O2 saturation remained at 51.6 percent which was still below that of the mixedvenous blood, while the CO2 content, pH, andpCOo were almost the same as those of themixed venous blood. Thus, it was apparentthat during heart-lung bypass with coronaryblood flow circulating through the pulmonaryvasculature, static inflation did not provide anormal physiological environment to the by-passed lungs.
It: was only with the aid of artificial respira-tion that; both the O2 saturation and the acid-
base parameters of pulmonary venous bloodcould be maintained close to those of the sys-temic arterial blood. Employing varyingamounts of artificial respiration which rangedfrom 0.7 to 6.5 L./min., it was possible tobring the O2 saturation up to 90.1 per centwith somewhat lower COo content and pCO^and a higher pll than those of the arterialblood (table 1).
BRONCHIAL COLLATERAL FLOW
Normally the pulmonary perfusate consistsof three components: vena naval flow, coro-nary venous return, and bronchial collateralflow. By placing; a clamp at the level of theaortic valve during bypass, as in preparationA, with a precautionary measure of maintain-ing left atrial pressure 1 to 4 cm. IIoO higher
Circulation lirxrarck. Volume, X, February 1962
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from

EXTRACOEPOREAL CIRCULATION 135
TABLE 3
Alteration of Lung ComjMance During Heart-Lung Bypass
CL (ml./cm. H:O), mean ± S.D.
1. EITect of ventilationStatic inflation (n = 13)Artificial inflation (n = 13)
2. KfToet of lung perfusate(after static inflation)Preparation A (n = 7)Preparation B (n =r 6)
•Significant difference.
36.0 ± 7.032.9 ± 4 . 9 t = 2.84* d.f. = 12
0.01 < P < 0.02
36.9 ± 6.435.0 ± 8 . 1 t = 0.47 d.f. = 11
0.6 < P < 0.7
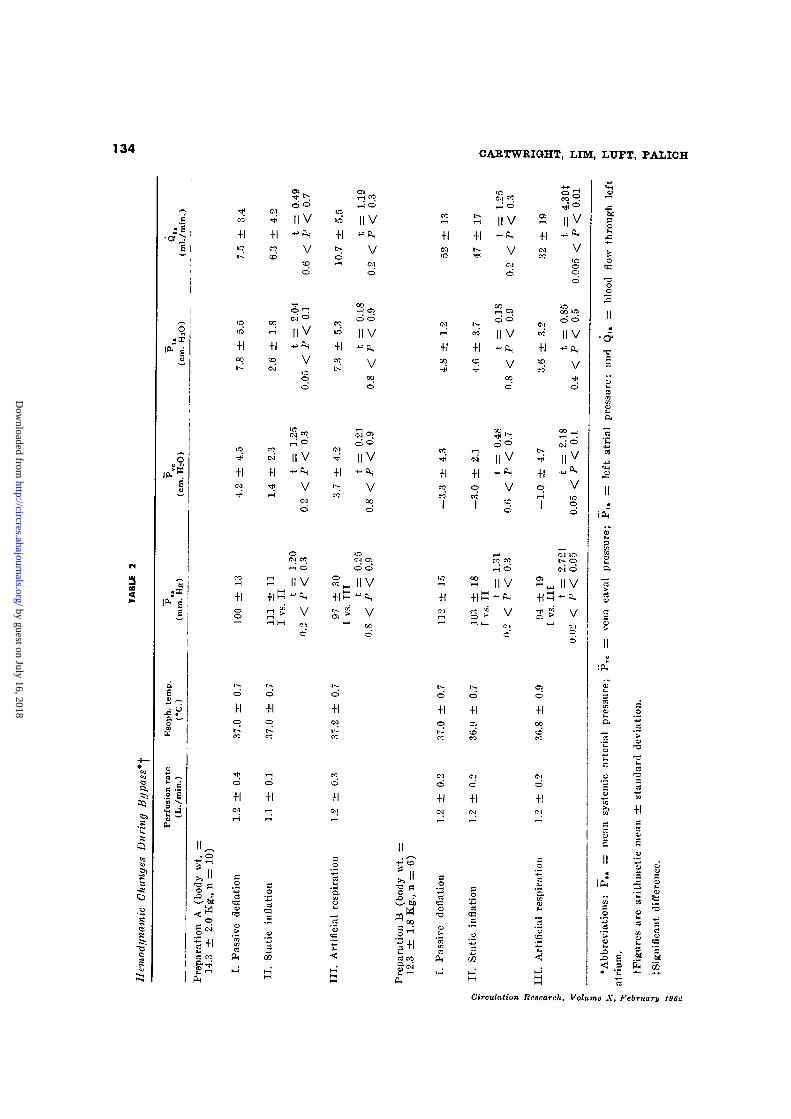
than right atrial pressui'o (to prevent back-flow through azygos-bronchial venous connec-t ions), it was possible to quantitatc the bron-chial collateral flow by continuously drainingthe blood from the left atrium by gravity.The data from 10 animals of preparation Aare shown in the last column of table 2. Theaverage body weight of the animals was 14.3± 2.0 Kg. (range: 11.4 to 17.3 Kg.) with cor-responding mean bronchial flow rates (Q,n)of 7.5, 6.3, and 10.7 ml./min. during passivedeflation, static inflation, and artificial res-piration, respectively. As indicated by thepaired comparison in table 2, the differencesbetween these values were not statisticallysignificant. Therefore, the data were pooledtogether yielding an average bronchial flowof 8.8 ± 4.9 ml./min. (range: 2.4 to 19.0 ml./min.), which was equivalent to 0.7 per cent:of the total systemic flow. An attempt to re-veal correlation between the gross bodyweight and the bronchial flow in these animalswas unsuccessful, perhaps due to the narrowrange of body weight studied and the accom-panying variations during the surgery. Fur-thermore, in subsequent studies in five otherdogs, varying the superior vena caval pres-sure from —10 to +40 cm. H2O relative tothe left atrial pressure did not significantlyaffect the bronchial flow as shown in figure 2.
METABOLIC RATE OF THE LUNG TISSUES
The experimental conditions of preparationA were particularly suited for the metabolicstudy of the lungs. Since the lungs were solelyperfused by fully oxygenated blood (i.e.,bronchial arterial blood) in this preparation,
Circulation Research, Volume X, February 1&SZ
it was possible to determine the O2 consump-tion of the lungs in situ by collecting andanalyzing the expired air during artificialventilation. The O2 consumption of the lungsmeasured in this fashion revealed an averagevalue of 1.6 ± 0.8 ml./min. (range: 0.4 to 3.3ml./min.), with the mean CO2 output of 4.3ml./min. (range: 2.7 to 6.0 ml./min.). Con-sidering an average body weight of 14.3 Kg.for the animals and a mean respiratory gasexchange prior to bypass of 99 ml./min. ofO2 and 81 ml./min. of CO2, it is concludedthat the metabolic requirement of the lungsis quite small, amounting to only 1 to 2 percent of the total metabolic rate.
HEMODYNAMIC CHANGES DURING BYPASS
The blood collected from the left atrium inpreparation B averaged 52, 47, and 32 ml./min, during passive deflation, static inflation,and artificial respiration, respectively, asshown in table 2. Although the greater amountof drainage seen in this preparation as com-pared to that in preparation A was undoubt-edly due to the large coronary veuous returnin the former, these volume figures in prep-aration B did not warrant accurate quantita-tion of the coronary venous return due toprobable escape of blood through the left ven-tricle into the aorta. _
The mean values of systemic arterial (PBn).vena caval (P~vc), and left atrial (P,a) pres-sures during bypass are also shown in table2. In preparation A, these pressures weremaintained at practically the same levels,whereas the systemic arterial pressure wassomewhat lower during artificial respiration
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from
136 CARTWEIGHT, LIM, LXTFT, PALtCH
Totol Peripherol Resistance During Heart-Lung Bypass
• — -
0
FIGURE 3
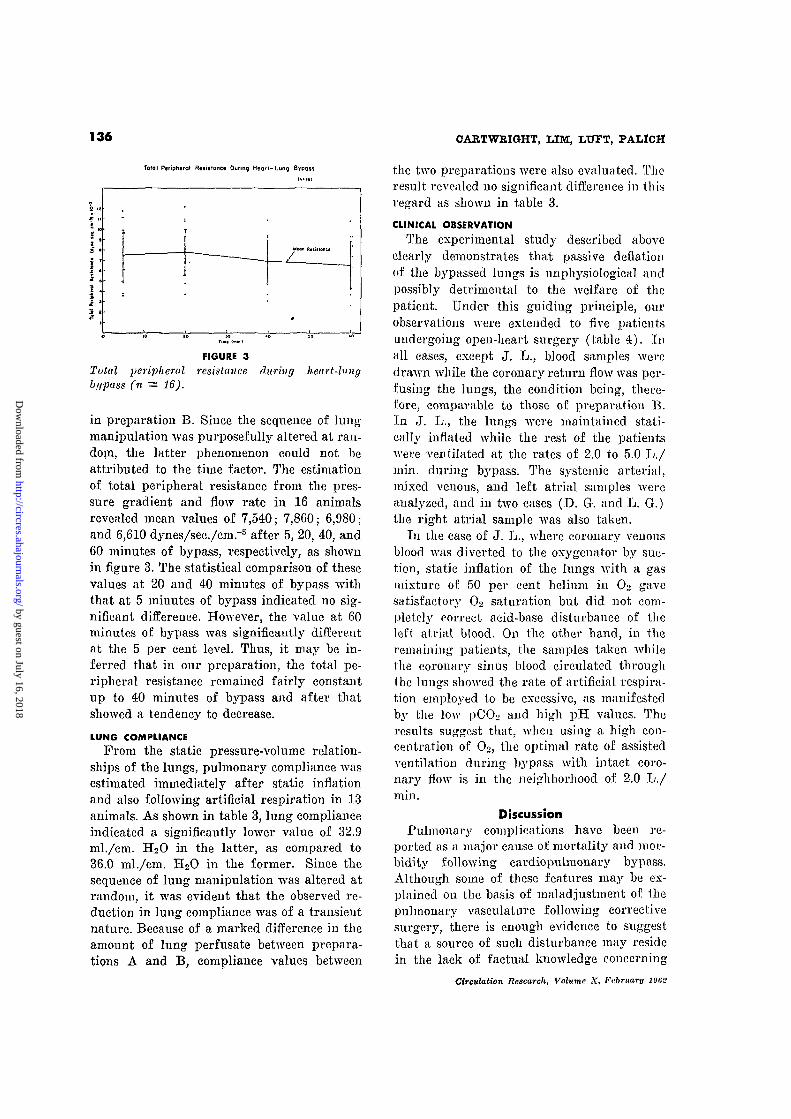
Total peripheral resistance during heart-lungbypass (n = 16).
in preparation B. Since the sequence of lungmanipulation was purposefully altered at ran-dom, the latter phenomenon could not beattributed to the time factor. The estimationof total peripheral resistance from the pres-sure gradient and flow rate in 16 animalsrevealed mean values of 7,540; 7,860; 6,980;and 6,610 dynes/sec./cmr5 after 5, 20, 40, and60 minutes of bypass, respectively, as shownin figure 3. The statistical comparison of thesevalues at 20 and 40 minutes of bypass withthat at 5 minutes of bypass indicated no sig-nificant difference. However, the value at 60minutes of bypass was significantly differentat the 5 per cent level. Thus, it may be in-ferred that in our preparation, the total pe-ripheral resistance remained fairly constantup to 40 minutes of bypass and after thatshowed a tendency to decrease.
LUNG COMPLIANCE
From the static pressure-volume relation-ships of the lungs, pulmonary compliance wasestimated immediately after static inflationand also following artificial respiration in 13animals. As shown in table 3, lung complianceindicated a significantly lower value of 32.9ml./cm. H2O in the latter, as compared to36.0 ml./cm. H2O in the former. Since thesequence of lung manipulation was altered atrandom, it was evident that the observed re-duction in lung compliance was of a transientnature. Because of a marked difference in theamount of lung perfusate between prepara-tions A and B, compliance values between
the two preparations were also evaluated. Theresult revealed no significant difference in thisregard as shown in table 3.
CLINICAL OBSERVATION
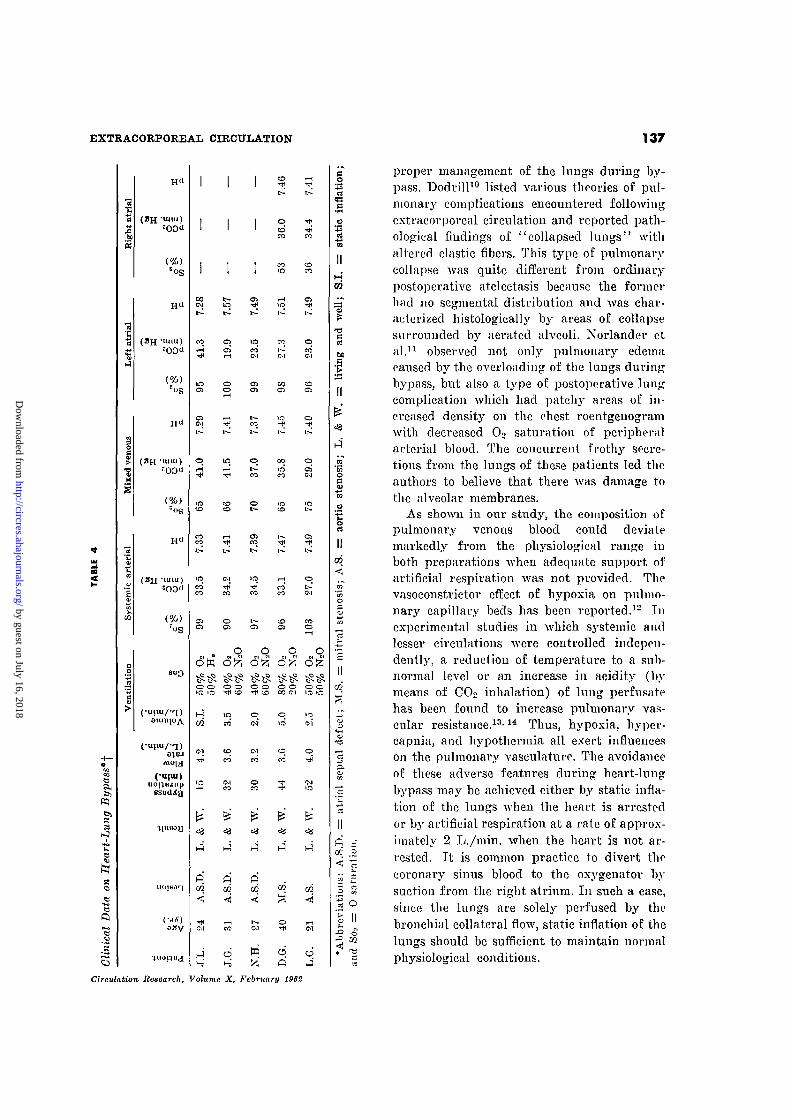
The experimental study described aboveclearly demonstrates that passive deflationof the bypassed lungs is unphysiological andpossibly detrimental to the welfare of thepatient. Under this guiding principle, ourobservations were extended to five patientsundergoing open-heart surgery (table 4). Inall cases, except J. L., blood samples weredrawn while the coronary return flow was per-fusing the lungs, the condition being, there-fore, comparable to those of preparation B.In J. L., the lungs M'ere maintained stati-cally inflated while the rest of the patientswere ventilated at the rates of 2.0 to 5.0 L./min. during bypass. The systemic arterial,mixed venous, and left atrial samples wereanalyzed, and in two cases (D. G. and L. G.)the right atrial sample was also taken.
In the ease of J. L., where coronary venousblood was diverted to the oxygenator by suc-tion, static inflation of the lungs with a gasmixture of 50 per cent helium in O2 gavesatisfactory O2 saturation but did not com-pletely correct acid-base disturbance of theleft atrial blood. On the other hand, in theremaining patients, the samples taken whilethe coronary sinus blood circulated throughthe lungs showed the rate of artificial respira-tion employed to be excessive, as manifestedby the low pCO? and high pH values. Theresults suggest that, when using a high con-centration of O2, the optimal rate of assistedventilation during bypass with intact coro-nary flow is in the neighborhood of 2.0 L./min.
DiscussionPulmonary complications have been re-
ported as a major cause of mortality and mor-bidity following cardiopulmonary bypass.Although some of these features may be ex-plained on the basis of maladjvistnient of thepulmonary vasculature following correctivesurgery, there is enough evidence to suggestthat a source of such disturbance may residein the lack of factual knowledge concerning
Circulation Research, Volume X, February 196!.'
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from
EXTRACORPOREAL CIRCULATION 137
PQ
)
)=00"
5og
H«
(2H "Uiui)
H«
-luiu)
roS
0}0J
( |uopiunp
(oily
COCO
l >
I O
co'CO
Oiat
i—1
CO
o
o>COL ^
ire-* 'CO
0 1
' ^
T—ICO*CO
t o
en• * .
0
oq
CO0
q q q qlzl 6>5 6^; dfe
CO
1MCO
S.D
.
CO
OCO
S.D
.
toCO
0
0 1ire
fc>'
ct
nl s
e;
II
p" =•cc 2
S S
H q'̂ P
m
proper management of the lungs during by-pass. Dodrill10 listed various theories of pul-monary complications encountered followingextracorporeal circulation and reported path-ological findings of "collapsed lungs" withaltered elastic fibers. This type of pulmonarycollapse was quite different from ordinarypostoperative atelectasis because the formerhad no segmental distribution and was char-acterized histologically by areas of collapsesurrounded by aerated alveoli. Norlander etal.11 observed not only pulmonary edemacaused by the overloading of the lungs duringbypass, but also a type of postoperative lungcomplication which had patchy areas of in-creased density on the chest roentgenogramwith decreased Oo saturation of peripheralarterial blood. The concurrent frothy secre-tions from the lungs of these patients led theauthors to believe that there was damage tothe alveolar membranes.
As shown in our study, the composition ofpulmonary venous blood could deviatemarkedly from the physiological range inboth preparations when adequate support ofartificial respiration Avas not provided. Thevasoconstrictor effect of hypoxia on pulmo-nary capillary beds has been reported.12 Tnexperimental studies in which systemic andlesser circulations were controlled indepen-dently, a reduction of temperature to a sub-normal level or an increase in acidity (bymeans of COo inhalation) of lung peivfusatehas been found to increase pulmonary vas-cular resistance.13'14 Thus, hypoxia, hyper-capnia, and hypothermia all exert influenceson the pulmonary vasculature. The avoidanceof these adverse features during heart-lungbypass may be achieved either by static infla-tion of the lungs when the heart: is arrestedor by artificial respiration at a rate of approx-imately 2 L./min. when the heart is not ar-rested. It is common practice to divert thecoronary sinus blood to the oxygenator bysuction from the right atrium. In such a case,since the lungs are solely perfused by thebronchial collateral flow, static inflation of thelungs should be sufficient to maintain normalphysiological conditions.
Circulation Research, Volume X, February 1962
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from

138 CARTWKIGHT, LIM, LUFT, PALICH
Several attempts have been made in thepast to measure the bronchial blood flow inexperimental animals and in man, utilizingeither direct or indirect methods. The indirectmethod is based on the simultaneous measure-ments of the right and left ventricular out-puts,15 and the direct measurement is neces-sarily marked by the excessive dissection andligation of the blood vessels. The employmentof extraeorporeal circulation seems to offerone of the best physiological conditions inwhich the bronchial flow can be quantitateddirectly. The elimination of caval and coro-nary venous returns leaves only the bronchialflow (and negligibly minute thebesian return)to empty into the left heart, and the averagevalue of 8.8 ml./min. under normal arterialpressure and body temperature compares wellwith the values reported by others.10"18 Al-though the anatomical complexity of thebronchial circulation is apparent, and thepossible anastomosis between mediastinal ves-sels and small bronchial veins is cited byHayek, the quantity of bronchial blood flowlost to the right heart through this route isassumed to be negligibly small.
Our findings of constant bronchial floMT
during three different types of lung manipu-lation with or without cardiac arrest tends tonegate the concept expressed by Muller andhis associates,20 who believed that the manualmovement of the lungs in open-chest prepara-tion increased the bronchial flow. In agree-ment with our observations, Horisbergcr andRodbard21 reported that the bronchial bloodflow did not change until the lung insufflationpressure reached an excessive level of 20 to 30cm. H2O in dogs.
The constancy of bronchial flow despite in-creased systemic venous pressure, as shownin figure 2, contrasts with the observationmade by State and his co-workers,18 who noteda positive relationship between systemicvenous pressure and bronchial collateral flow.The reason for this difference is unknown ex-cept that the pulmonary circulation was arti-ficially maintained by a pump in the latter,while it was devoid of main flow in our prep-aration.
In the past, oxygen consumption of the lunghas been estimated using either slices of lungtissue by Warburg's technique or isolatedlung preparations. Differing from these cus-tomary methods, our technique is unique inthat (1) it allows estimation of oxygen con-sumption of whole lungs, (2) it is done insitu, and (3) the lungs are perfused withoxygenated blood (bronchial arterial blood).Some technical aspects in our method whichdeserve further attention are (a) that thedifference in oxygen content of systemic arte-rial and pulmonary venous blood is practi-cally nil during artificial respiration of thebypassed lung (i.e., 19.4 versus 19.2 volumeper cent of Oo with no statistical difference) —this fact suggests that the oxygen consumedby the lung tissue is rapidly supplementedfrom the air by the diffusion process; (b)that the O2 content of expired air in theDouglas bag averaged 20.82 per cent (range:20.63^20.88 per cent) which indicates thatalthough the amount of oxygen consumptionis indeed small, its magnitude is sufficientlylarge to be detected by the standard methodof gas analysis (Scholander technique with=t 0.03 per cent of accuracy) ; and (c) in con-trast to the average 02 consumption of l.fiml./rain., the corresponding CO2 ontput was4.3 ml./min.. which gave a respiratoryquotient of 2.7. This was due to the"Auspumpung" of COo during the artificialrespiration Avhich ranged from 1 to 4 L./min.and was also perhaps due to higher COustorage capacity of the lungs relative tooxygen.
The mean value for oxygen consumptionof canine lung in this study (i.e., .1.6 ± 0.8ml./min. in 10 dogs having an average bodyweight of 14.3 Kg.) compares well with thatreported by Bostroem and Lochner.1- Duringperfusion of the pulmonary artery «of an iso-lated lung with arterial blood of tin1 donor'sdog, the latter found 1.4 ± 0.5 luL/min. ofO2 consumption of whole lungs in nine dogshaving an average body weight of" .1 1.4 Kg.Recent data by Aviado23 gives a n averagevalue of 0.64 ml./min./lOO Gin. of "we I lung-
Assuming the wet weight of the lunpi .in our
Circulation Research, Volume X, "Pf^ttt*' V ^962
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from

EXTRACORPOREAL CIRCULATION 139
preparation is 150 Gin., this provides approx-imately 1.0 ml./inin. of O2 uptake of wholecanine lung.
Among many factors which influence vaso-motor tone, arterial and venous pressures,perfusion rate, and circulating blood volumeare of prime importance. In addition, thetemperature, acidity, viscosity of perfusingblood, and the. depth of anesthesia contributesignificantly to the vasomotor regulation. Asa preliminary approach to the problem, thetotal peripheral resistance was calculatedover 00 minutes of bypass in our preparation.The result indicated a fairly constant resist-ance up to 40 minutes of bypass and a slightreduction at the end of one hour of bypassunder conditions of norinothermia and nor-motension (fig. 3, table 2).
Contrary to our findings, Moffitt ct a I.-4
reported a gradual increase in peripheral re-sistance during bypass in patients. Their rateof perfusion, however, was rather low, themean perfusion rate being 1.7 L./min./M.2 incontrast to the preoperative cardiac index of4.2 Tj./min./M.2. Furthermore, the mean arte-rial pressure during bypass ranged from 27to 50 mm. Tig, with an average reduction ofthe patient's rectal temperature of 1.7 C.Cordell and his associates-"' found a gradualincrease, in peripheral resistance in sevendogs during 30 minutes of bypass under nor-niotherniia and normotension. They also per-fused the animal at a low rate of approxi-mately 800 ml./min. In an extensive studyon vasomotor regulation during bypass inman, Sanger et a.l.2" observed a somewhatphasic alteration in peripheral resistance:namely, an initial reduction during 5 minutesof bypass, an increase during 10 to 40 min-utes, and a gradual decrease during 40 to 80minutes of bypass. Their rate of perfusionwas 50 ml./Kg./min. in adults and 70 to 100ml./Kg./min. in children. Thus, it appearsthat, other factors being kept constant, theperipheral resistance tends to increase whenthe low flow rate of perfusion is used, where-as the trend is reversed with the employmentof high flow rate. This conclusion is in agree-ment with that of Ankeney and his associates-
who showed that peripheral resistance pro-gressively declines as the pumping rate isincreased. Clowes28 suggests that this may bedue to the effect of "buffer" nerves.
In a previous investigation," pulmonarycompliance of anesthetized intact (closed-chest) dogs was found to be 34.1 ± 2.8 ml./cm. IT2O in 10 animals (mean body weight,15 Kg.). In the present study, the averagefigure in anesthetized open-chest dogs gave amean value of 36.0 ± 7.0 ml./ein. II2O in 13animals (average body weight, 13.4 Kg.) (ta-ble 3), revealing close agreement of valuesfor pulmonaiy compliance in the two groups.
Contrary to our findings, a much higherlung compliance was reported by (Inastavinoand his associates4 who found a value of 134ml./cm. H20 (range: 6!) to 240 ml ./cm. 11.01in 10 anesthetized open-chest dogs having anaverage body weight of 15.8 Kg. This figureis almost three times as great as our own.approaching values recorded in human be-ings. The reason for this discrepancy is notknown, the only apparent difference in thetwo studies being the use of air for lung in-sufflation in our work, while oxygen was usedin the other study. It must also be mentionedthat leakage of gas from the lungs due tosurgical trauma will reduce the static trans-pulmonary pressure, giving an erroneouslyhigh "pulmonary compliance."
SummaryAn attempt has been made to determine the
optimal method of managing the lungs duringcardiopulmonary bypass. The chemical bc-luwior (oxygen saturation, acid-base balance)of the pulmonary venous blood indicates (a)that static inflation of the lungs with eithera gas mixture of high oxygen content or am-bient air is sufficient to maintain a properinternal milieu for the pulmonary vaseulaturewhen the bronchial collateral flow is the solepulmonary perfusate, and (b) that in adulthuman beings artificial respiration up to 2L./min. is necessary when the pulmonaryperfusate consists of the coronary venousblood in addition to the bronchial collateralflow.
The effective application of the heart-lung
Circulation Research, Volume X, February J9G£
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from
140 CARTWRIGHT, LIM, LUFT, PALICH
bypass procedure in physiological investiga-tion is depicted by the studies on metabolicrate of the lung tissues and the measurementof bronchial flow. It is estimated that thebronchial collateral flow amounts to 8.8 ml./min. or 0.7 per cent of the total systemic flow,and that the oxygen consumption of the lungsaverages 1.6 nil./min. or 1 to 2 per cent ofthe total metabolic rate in the open-chest dogs.The pulmonary compliance did not changefollowing either passive deflation or static in-flation, but is transiently reduced after arti-ficial respiration.
AcknowledgmentE. Mary Mostyn, M.D., actively participated in
this study.The technical assistance of Mrs. Aicla Shero is
gratefully acknowledged.
References1. KOTTMEIEK, P . K. , ADAMSONS, .T., S T U C K E Y ,
J. H., NEWMAN, M. M., AND DENNIS, C :
Pathological changes after partial and totalcardiopulinonary bypass in humans and ani-mals. Surg. 'Forum 9: 184, 1959.
2. KOLFF, W. .!., EFFLER, D. B., GROVES, L. K.,
HUGHES, C. R., AND MCCORMACK, L. ,1".: Pul-
monary complications of open-heart operations:Their pathogencsis and avoidance. ClevelandClin. Quart. 25: 65, 1958.
3. SCHRAMEL, R. J., CAMERON, R., ZISKIND, M. M.,
ADAM, M., AND CREECH, 0.: Studies of pul-
monary diffusion after open heart surgery.J. Thoracic & Cardiovas. Surg. 38: 281, 1959.
4. GTJASTAVINO, G. N., WIKINSKI, J. A., ANDRES,
R. H . , DONABEI, C. A., AND QU1NTERN0, J . E . :Modification of lung compliance during perfu-sion with pump-oxygenator (experimental).Dis. Chest 38: 170, 1960.
5. CROSS, F. S., BERNE, R. M., HIROSE, Y., JONES,
R. D., AND KAY, E. B.: Evaluation of arotating disc type of rcservoir-oxygenator.Proc. Soc. Exper. Biol. & Med. 93: 210, 195G.
fi. CARTWRIGHT, R. S., PAUCH, W. E., LIM, T. P. K.,
PROPER, R., AND CARDUS, D. P.: Experiences
in extracorporeal circulation. Am. Surgeon 26:792, 1960.
7. LIM, T. P. K., H ' F T , V. C, AND GRODINS, F. S.:
Effects of cervical vagotomy on pulmonaryventilation and mechanics. J. Appl. Physiol.13: 317, 1958.
8. WlGQERS, C. .T.: Physiology in Health andDisease, ed. 4. Philadelphia, Lea & Febigor,1944.
9. SNEDECOR, G. \V.: Statistical Methods. Ames,Iowa, Iowa State College Press, 1946.
10. DODRILL, F. D.: Effects of total body perfnsionupon the lungs. In Extracorporeal Circulation,edited by .T. G. Allen. Springfield, TU., CharlesC Thomas, 195S, p. 327.
1 1 . XORLANDER, O., PlTZELE, S., E D L I N G , I . , NORBERG,
B., CRAFOORD, C, AND SENNINO, A.: Anes-
thesiological experience from intracardiac sur-gery with the Crafoord-Senning heart-lungmachine. Acta anaesth. scandinav. 2: 181, 195S.
12. VOXECLER, U. S., AND LILJESTRAND, G.: Obser-
vations on the1 pulmonary arterial blood pros-sure in the cat. Acta physiol. scandinav. 12:301, 3946.
13. GALLETTI, P. M., AND SALISBURY, P. F.: Influ-
ence of blood temperature on the pulmonarycirculation. Circulation Research 6: 275, 1958.
14. WEIL, P., SALISBURY, P. F., AND STATE, D.:
Physiological factors which influence pulmo-nary artery pressure during separate perfu-sion of systemic and of pulmonary circula-tion in the dog. Am. J. Physiol. 191: 453,1957.
15. FISHMAN, A. P., TURINO, G. M., BRANDFON-
BRENER, M., AND HIMMELSTEIN, A.: "Effec-
tive" pulmonary collateral blood flow in man.J. Clin. Invest. 37: 1071, 195S.
lfi. BRUNER, H. D., AND SCHMIDT, C. F.: Blood flowin the bronchial artery of the anesthetizeddog. Am. J. Physiol. 148: 64S, 1947.
17. CUDKOWICZ, L., CALABRESI, M., B U S , E. G.,
AND GRAY, F. D.: Simultaneous estimationof right and left ventricular outputs appliedto a study of the bronchial circulation in dogs.Am. Heart J. 58: 732, 1959.
18. STATE, D., SALISBURY, P. F., AND WEIL, P.:
Physiologic and pharmacologic studies ofcollateral pulmonary flow. J. Thoracic Surg.34: 599, 1957.
If). HAYEK, II. V.: Die Menschliche Lunge. Berlin,Springer-Verlag, 1953.
20. MULLER, W . H . , LlTTLEFIELD, .T. B . , ANDDAJIMANN, J. F.: Pulmonary parenchymalchanges associated with cardiopulinonarybj'pass. In Extracorporeal Circulation, editedby J. G. Allen. Springfield, Til., Charles CThomas, .1958, p. 330.
21. HORISBERGER, B., AND RODBARD, S.: Direct
measurement of bronchial arterial flow. Circu-lation Research 8: 1149, 3960.
22. BOSTROEM, B., AND LOCHNER, W.: Uber der
Sauerstoffverbraueh dor Lunge. Arch. gcs.Physiol. 260: 511, 1955.
23. AVIADO, D. M.: Therapy of experimental pul-monary edema in the dog. Circulation Research7: 1018, 1959.
24. MOFFITT, E. A., PATRICK, R. T., SWAN, H. J. C,
AND DONALD, D. E.: Study of blood flow,venous blood oxygen saturation, blood pres-
Circulalion Research, Volume A', February 196S
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from
EXTRACORPOREAL CIRCULATION 141
sure, iind peripheral resistance during totalbody porfusion. Anesthesiology 20: 18, 1959.
25. CORDELL, A. K., SPENCER, M. P., AND MEREDITH,
)'. H.: Studies of peripheral vascular resistanceassociated with total cardiopulmonary bypass:I. Peripheral resistance under condition ofnormothermia and normotension. J. Thoracic& Cnrdioviis. Surg. 40: 421, 1960.
120. SANGER, P. W., ROBICSEK, V., TAYLOR, F. H.,
HUES, T. T., AND STAM, R. E.: Vasomotor
regulation during extracorporeal circulationand open-heart surgery. J. Thoracic & Cardio-vas. Surg. 40: 355, 1960.
ANKENEY, J. L., VILES, P. H., AND LEONARDS,
J. E.: Study of changes in peripheral flowand resistance as associated with total bodyperfusion. Surg. Forum 9: 157, 1959.
CLOWES, G. H. A.: Extracorporeal maintenanceof circulation and respiration. Physiol. Rev.40: 826, 1960.
Circulation Rrnrnrch. Volume X, February J962
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from

Robert S. Cartwright, Thomas P. K. Lim, Ulrich C. Luft and William E. PalichPathophysiological Changes in the Lungs During Extracorporeal Circulation
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1962 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.10.2.1311962;10:131-141Circ Res.
http://circres.ahajournals.org/content/10/2/131World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Research Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 16, 2018http://circres.ahajournals.org/
Dow
nloaded from





























